micronutrient malnutrition iii - wordpress.com malnutrition iii ... anemia is commonly used to...
TRANSCRIPT
Micronutrient malnutrition III
Vanessa Velazquez-Ruiz, MD Emergency Medicine Global Health Fellow
St. Luke’s-Roosevelt Hospital

Agenda
Iron deficiency anemia
Overview and epidemiology
Discuss risk factors and food sources
Highlight the role or iron as a micronutrient and discuss some of the consequences of iron deficiency
Iron deficiency and anemia
Overview
One of the most common nutrition disorders worldwide
Only nutrient deficiency of significant prevalence in all develop countries
Play a key role in oxygen and energy metabolism
Anemia is commonly used to screen for iron deficiency
Anemia not specific for iron deficiency
Iron deficiency anemia represents the severe end of spectrum of iron deficiency
Iron deficiency without anemia represent a mild form of the deficiency

Anemia
Defined as hemoglobin concentration below -2 standard deviation of the age, sex specific reference
Most common cutoff in hemoglobin is below
110mg/L for children under 5 and pregnant
120mg/L for non pregnant women
130mg/L for men
Epidemiology
WHO estimated 4-5 billion people with iron deficiency
More than half preschool-aged children and women of reproductive age are anemic in many countries from South Asia and sub-Saharan Africa
High rates in countries like Peru, Bolivia and Haiti
Estimated 7-12% with iron deficiency in develop countries
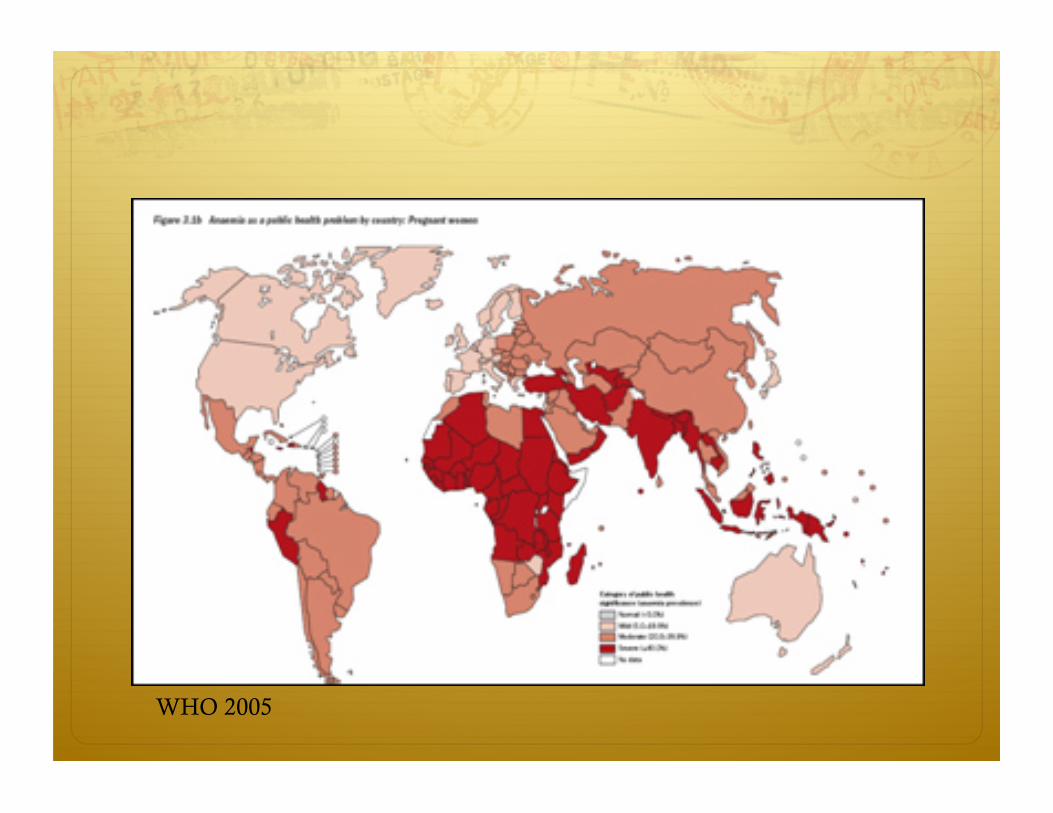
WHO 2005
Not all anemias are caused by iron deficiency
In areas where the prevalence of anemia in higher than 30-40%, most is caused by iron deficiency
Challenging in places like Sub-Saharan Africa where thalassemia and malaria are endemic.
Vit A, Folic Acid and Vit B 12 may contribute to etiology
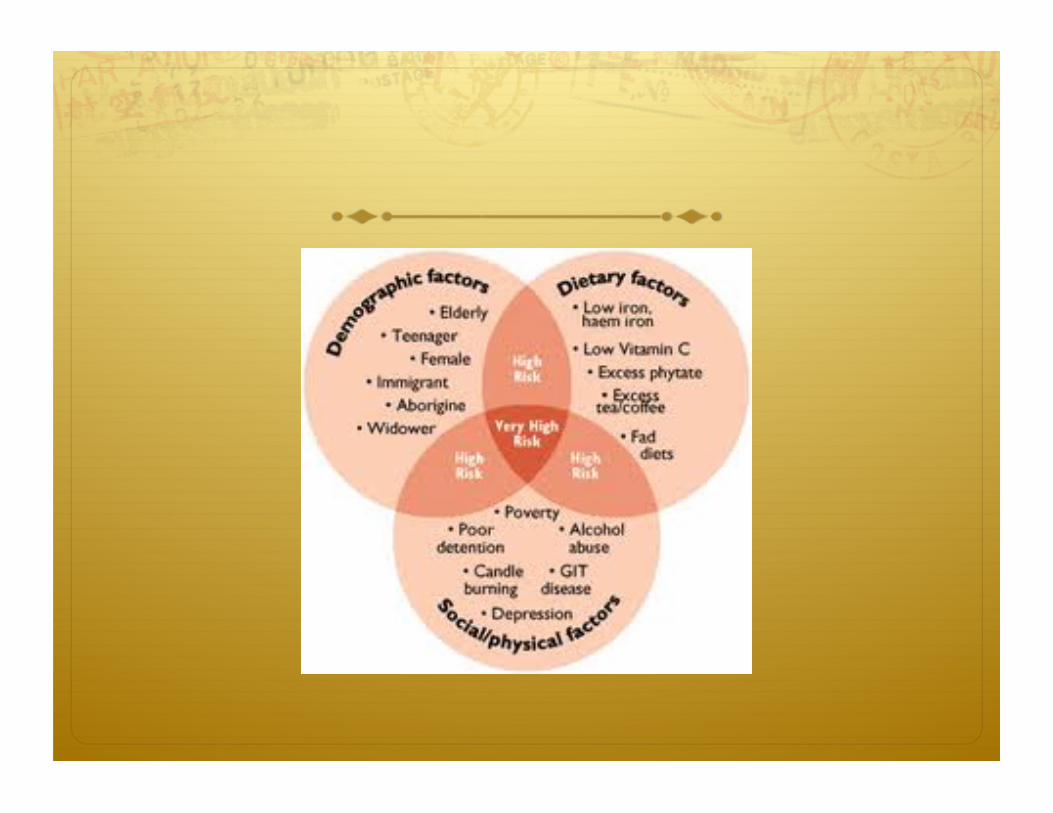
Risk factors
Pregnancy
Prematurity
Low birth weight
Rapid growth
Sensitivity to cow’s milk
Low consumption of meat
High consumption of phytates
Menstruation
Nematode infection in GI

Food sources
red meat
Poultry
insects
lentils
beans
leafy vegetables
pistachios
tofu
chickpeas
black-eyed peas
fortified bread, and fortified breakfast cereals
Iron from plant sources is less easily absorbed than iron from animal sources
Vegetarians and vegans should have a higher total daily iron intake than those who eat meat, fish or poultry
Legumes and dark-green leafy vegetables like broccoli, are especially good sources of iron for vegetarians and vegans
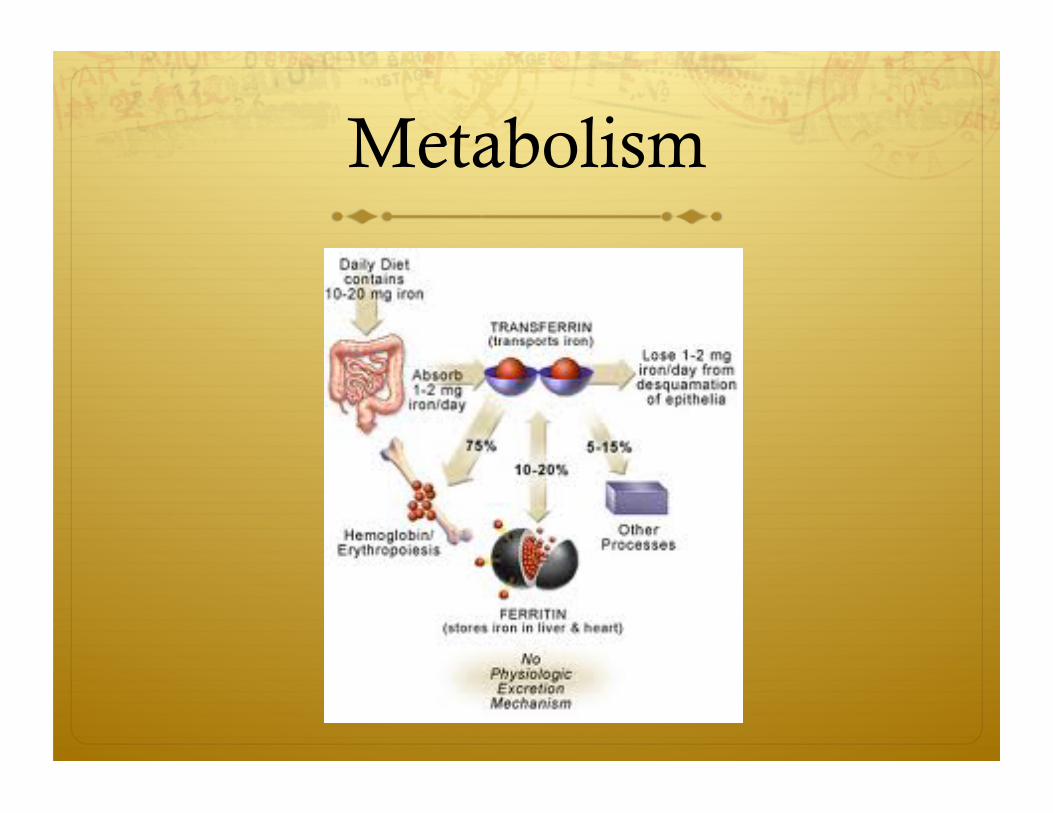
Metabolism
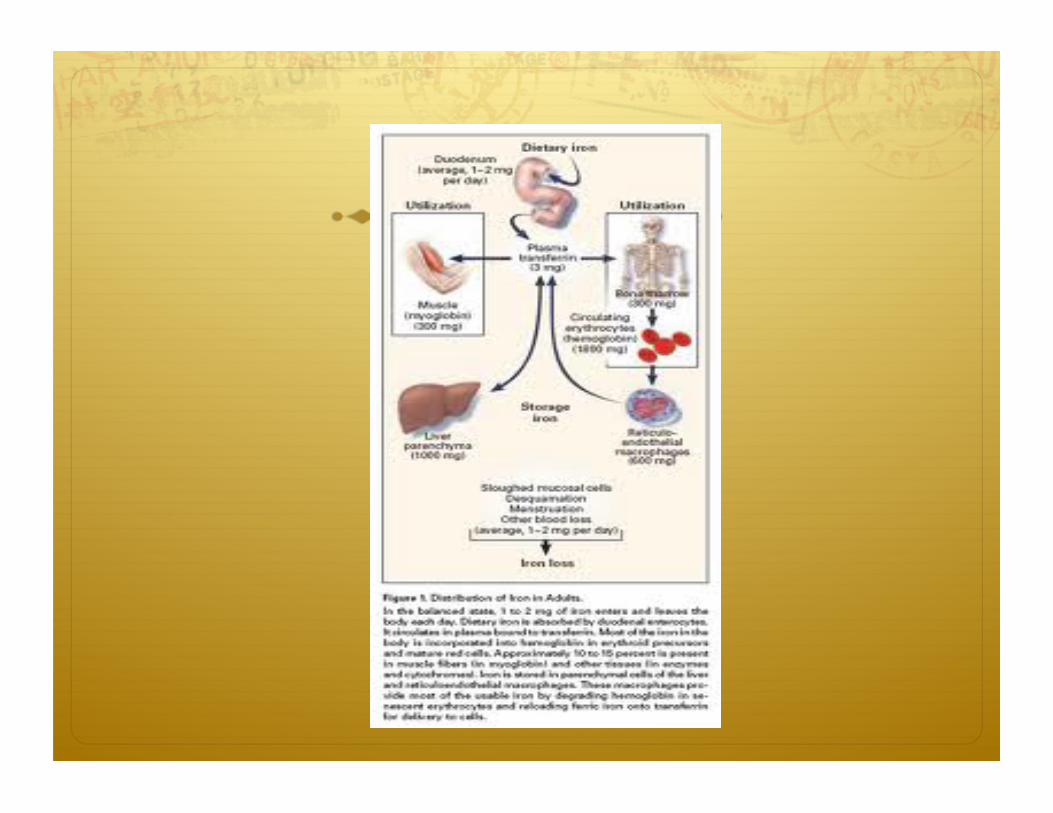

Roles of iron in biological functions
Hemoglobin
Transfer of oxygen from lungs to tissue in erythrocytes
In anemia,
Hgb content of erythrocytes is reduced -> decreasing oxygen delivery to tissue -> leading to chronic tissue hypoxia

Myoglobin
Found in muscle
Transport and storages oxygen needed for muscle contraction
10% of total body iron
Single heme group with single globin chain
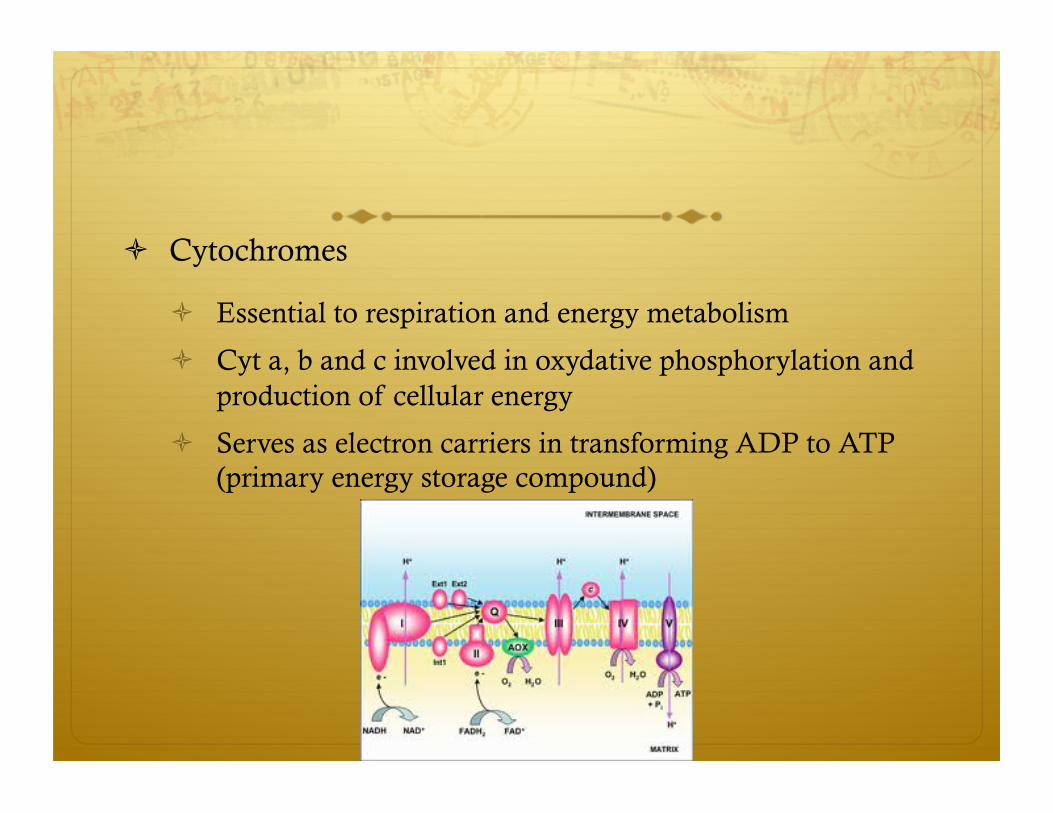
Cytochromes
Essential to respiration and energy metabolism
Cyt a, b and c involved in oxydative phosphorylation and production of cellular energy
Serves as electron carriers in transforming ADP to ATP (primary energy storage compound)
Other iron containing enzymes
NADH (Nicotinamide adenine dinucleotide phosphate) dehydrogenase
Catalase
Peroxidase
Among other
Iron and immune system
Animal studies suggested some role in immune system
No convincing evidence for humans

Pathogenesis of Iron deficiency
Increase requirement for iron
Negative balance between intake and loss
Rapid growth (infancy, adolescence, pregnancy)
Iron loss (menstrual period, transfer to fetus)
Poor dietary intake
For infants, iron content of milk is a major determinant
Iron content of breast milk is low compared to cow milk, however
50% of breast milk iron can be absorbed and only 10% of cow milk can
After 6 months, breast feeding infants need another source of iron besides breast milk
Abnormal iron loss
Menstrual blood
Occult GI blood due to sensitivity to proteins in cow milk
Hookworm infection
Necator americanus (greater bleeding) and Ancyclostoma duodenale
Functional consequences of iron deficiency
Mild anemia (10-20gm/L below cutoff) : no health impairment
Moderate anemia: reduce oxygen carrying capacity and interferes with aerobic function
Very Severe (<50gm/L) : increase childhood and maternal mortality
Child behavior and development
Better Birth Outcomes
Child behavior and development
Children with iron deficiency anemia test less well in psychomotor development
Moderately severe iron deficiency can lead to irreversible development disadvantage
Iron-deficiency women are at increase risk of depression

Work performance and productivity
Reduce work performance
Linear dose response relationship between hemoglobin concentration and performance
Supplementation of iron in workers increases productivity
In developing countries, a major reduction in work capacity can be of great economic consequence
In a country where 50% of women and 20% of men are affected, the impact equals 5-7% of the national economic output.

Heavy metal absorption
Iron deficiency children in USA have 3-4 times higher prevalence of lead poisoning
Strong evidence of direct association between iron deficiency and increase efficiency of lead absorption
Assessment of nutritional status
Test for iron deficiency
One or more abnormal iron biochemical test:
Serum ferritin
Transferrin saturation
Transferrin receptor
Erythrocyte protoporphyrin
Ferritin
Serum Ferritin is a well accepted marker of body iron
Pros: ability to measure level form blood spots
Contras:
Infection and inflammation can falsely elevate levels
Expensive for field base settings
Hemoglobin
Field testing of anemia
Portable photometer or standard methods
Detection of anemia by clinical examination
Pallor of skin, conjunctive, tongue and palms

Physical exam

Symptoms of iron deficiency
Fatigue
Pallor
hair loss
Irritability
Weakness
Pica
brittle or grooved nails
Plummer-Vinson Syndrome
Painful atrophy of mucous membrane of the tongue, pharynx and esophagus
Among other


Primary Health Care approaches

Iron supplementation
1st approach
If Prevalence of iron deficiency anemia is low (10-15%)
Screen for anemia and supplement those found anemic
Dosage 3mg/kg elemental iron for children under 5
60mg elemental iron daily for adults for 3 months
2nd approach
Universal supplementation where the prevalence is high and where the majority are iron deficient
Most suitable in developing countries
UNICEF recommends a daily dose of 12.5mg of elemental iron for infants 6-12 months old
In pregnancy WHO recommends
6-month regimen of daily supplements containing 60mg of elemental iron +folic acid
If the prevalence of anemia is >40%, an additional 3 month tx in postpartum periods is recommended

Limitations
Strategy is needed to establish a system for supply and distribution of iron tablets
Supply and distribution is not always reliable
Poor compliance
At higher doses (>60mg) many GI side effects
Control of intestinal Helminth infection
Routine de-worming
Nutrition education and promotion
Promotion of exclusive breast-feeding (higher absorption)
Education to delay the tea introduction to kids
Fortification
Ferrous sulfate is usually used to fortify infant formula and bread
Example:
Fortification of milk powder with Iron and Vit C in Chile
Fortified cookies in school
Flour fortification
THE END

References
WHO website