microscopic tubal reversal
TRANSCRIPT
Constance Fleming, RN Anne D Jenks, RN
Microscopic tubal reversal
Technical advances and social changes have increased the likelihood of revers- ing a sterilization procedure. An esti- mated 80 million couples around the world now use sterilization for family planning. A woman who is certain she wants no more children is apt to choose tubal ligation as a form of permanent sterilization.'
Several factors contribute to the in- creased use of this contraceptive method. The development of laparos- copic sterilization resulting in a short hospital stay and minimal discomfort is a major contributing factor.2 Other fac- tors include a growing concern about possible complications from taking oral contraceptives and using intrauterine devices, the emphasis on population control, and the women's movement.
Various techniques are used for tubal occlusion sterilization. The most com- mon methods performed with laparos- copy are: cauterization, the use of Silas-
Constance Fleming, RN, CNOR, is the head nurse of the gynecology operating room at Brigham and Women's Hospital, Boston. She is a graduate of the Holyoke (Mass) Hospital School of Nursing.
Anne D Jenks, RN, BSN, is the assistant di- rector of nursing in the operating room and recovery room at Brigham and Women's Hos- pital. She is a graduate of Albany (NY) Medical Center School of Nursing and earned her BSN at Northeastern University, Boston.
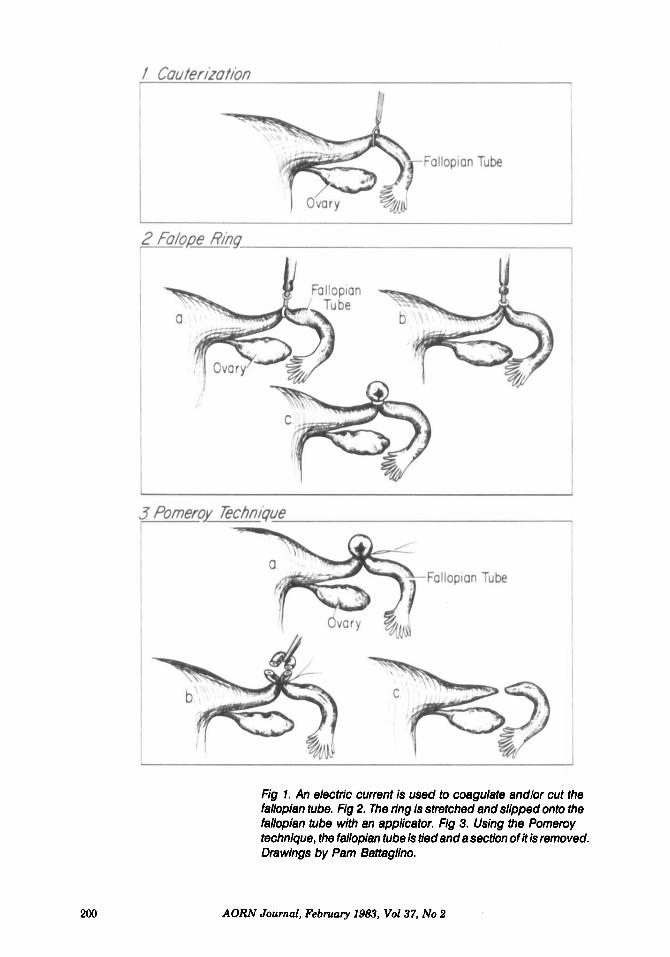
tic rings, and the use of clips. In the cauterization technique, a bipolar elec- trosurgical instrument is used to grasp and coagulate the tube; to cut and seal the ends of the tube by coagulation; or to cut a section of the tube and seal each end (Fig 1). The Silastic ring is a band that is stretched and slipped onto the fallopian tube with an applicator. The pinched section of the tube eventually becomes scar tissue (Fig 2). The clip method works in a similar way.
Tuba1 ligation can also be performed using a minilaparotomy incision. This procedure is performed most often on patients sterilized immediately post- partum when laparoscopy is not indi- cated. When the Pomeroy technique is used, the tube is tied with suture and a section of it is removed. As the suture dissolves, the tube pulls apart and is no longer a passageway between the ovary and uterus3 (Fig 3).
Corresponding to the rise in the number of occlusions, there has been a rise in the number of women seeking reversals. The American Association of Gynecologic Laparoscopists estimates that 1% of all women having steriliza- tions will seek reversals. In the United States, that amounts to 6,000 requests for reversals a year.4 Results of tubal reversals are significantly better since the advent of microsurgery, introduc- tion of fine suture material, and im- provements in reconstructive surgical techniques. That the success rate has
AORN Journal, February 1983, Vol37, No 2 199
200
Fig 1. An electric current is used to coagulate andlor cut the fallopian tube. Fig 2. The ring is stretched and slipped onto the fallopian tube with an applicator. Fig 3. Using the Pomeroy technique, the fallopian tube is tied and a section of it is removed. Drawings by Pam Baitaglino.
AORN Journal, February 1983, Vol37, No 2

increased, however, does not suggest that a woman contemplating steriliza- tion should take the procedure any less seriously. Thorough counseling is necessary to screen out women who are likely to request a reversal. If the woman has any doubts, she should use alternate forms of contraception.
A woman who chooses sterilization may seek a tubal reversal after an un- predicted event. Common reasons for requesting a tubal reversal are death of a child or a second marriage. Steriliza- tion before age 30, an unhappy mar- riage at the time of sterilization, and sterilization immediately after preg- nancy or after a contraceptive failure are often factors resulting in a request for a tubal r e ~ e r s a l . ~ Interview. When a woman seeks a re-
versal, an initial interview should be done to determine her reasons for re- questing it and her degree of motiva- tion. If possible or appropriate, the woman’s partner should be included in the interview session.
During the interview, the preopera- tive tests and the nature, extent, and implications of the surgery are ex- plained. Many women choose not to have surgery because they gain a more realistic understanding of the surgical procedure during the interview. Before the interview, women often have not considered that because of their age, their fertility may be decreased, and their chance of bearing a child with ab- normalities is increased. Women also may choose not to have a reversal be- cause the chances of success are below their expectations.6
If a woman wants to proceed with the surgery after the interview, a preopera- tive investigation is done to determine if either partner is infertile. This in- cludes a semen analysis, postcoital tests, and charting of basal body tem- peratures. A hystedpingogram and/ or laparoscopy may be recommended..
Hysterosalpingography provides in- formation as to the length and patency of the tubal segments. Laparoscopy permits visualization of the pelvis and oviducts to assess the likelihood of a successful reversal. Findings at laparoscopy can be at a variance with the operative note at sterilization.’
The OR nurse caring for the patient who chooses tubal ligation reversal must thoroughly review the patient’s chart. She should understand the interview- ing, screening, and decision-making process.
Often nurses are not as sensitive to a patient who wants a sterilization re- versed as they are to a n infertile patient who has not been sterilized. Unexpected life events usually precipitate the deci- sion to have a reversal. Nurses must examine and evaluate their personal opinions regarding both sterilization and surgery for a reversal.
The perioperative nurse will face a healthy woman who has come for surgery after a lengthy decision- making process. The patient has coped with her own feelings and the feelings of others, shared the decision with her partner, and has been counseled by her physician and perhaps a social worker.
Women often ask for reversals after unpredicted events.
She has had many tests. The nurse should be sure the patient understands that although the success of tubal re- versals has increased, there is a chance of no subsequent pregnancy. If the pa- tient has understood the counseling, she should not have unrealistic expecta- tions. The unit nurse may help the pa-
AORN Journal, February 1983, Vol37, No 2 201

tient by talking with her about her feel- ings.
During the preoperative phase, the OR nurse should explain what will hap- pen the day of surgery. Since all of these patients have had surgery at least once, it is helpful to inquire about previous surgical experiences. Determine which experiences were negative and which were positive to plan intraoperative care. If the patient has had only a laparowopy, she should be reminded that the operative course is different.
The patient remains in the hospital five to seven days, and will have a Foley catheter and intravenous tube in place immediately postoperatively. Em- phasize the importance of turning, coughing, deep breathing, and early ambulation to prevent respiratory and vascular complications. Tell the patient she will probably need pain medication, and that it will facilitate movement. Answer the patient’s questions or refer them to her physician. A preoperative assessment and nursing care plan should be written.
The day of surgery, the nurse checks the hemoglobin or hematocrit, and de- termines if blood is available for trans- fusion. A clot for crossmatch may have
Counseled patients should not have unrealistic hopes.
~~ ~
been sent to the blood bank in case of unexpected blood loss. The patient’s name band and operative permit are checked. Length of NPO status is ver- ified along with absence of dentures, candy, or gum. Instrumentation and equipment are checked for readiness.
Surgical procedure. The surgical pro-
cedure is described as performed by the gynecologists of the Fertility and En- docrine Clinic at the Brigham and Women’s Hospital, Boston.
General anesthesia with an endo- tracheal tube is usually employed. The skin preparation is performed following proper procedures. The bladder is routinely catheterized with an indwell- ing Foley catheter. A pediatric Foley catheter is inserted vaginally through the cervix into the uterus for later injec- tion of methylene blue dye. The nurse is aware of potential injury from the pediatric Foley while the patient is in the lithotomy position. For the laparotomy, the Trendelenburg’s posi- tion is needed. When the patient is cor- rectly positioned for laparotomy, the nurse places a safety strap two inches above the patient’s knees. The elec- troaurgical pad is applied to the anterior thigh. The incision is made, and a self- retaining retractor is applied.
Intraoperatively, the nurse main- tains the patient’s body in correct alignment, and checks potential pres- sure areas. Blood loss is assessed, and sponge, needle, and instrument counts are done.
The operative area is irrigated con- tinually with Ringer’s lactate solution to moisten tissues and prevent post- operative adhesions. Small, pointed, straight scissors are used to excise the occluded ends of the tube. Methylene blue dye is injected into the uterus through the pediatric Foley catheter to determine the patency of the tubes.
Surgery is accomplished with the use of magnification and atraumatic tech- nique. Tissues are handled gently. Hemostasis and excision of adhesions are accomplished with finger-tip control electrocautery. High magnification (20X), achieved with a microscope, is used to examine the cut surfaces, ascer- tain excision of all abnormal tissue, and to complete the anastomosis. (A frozen
202 AORN Journal, February 1983, Vol37, No 2

section may be required to show that the ends to be approximated are perfectly normal.
A suture is placed in the mesosalpinx adjacent to the oviduct to take up ten- sion and facilitate anastomosis (Fig 4). A two-layer anastomosis is then per- formed. The lumens are approximated by placing 8-0 interrupted sutures through the muscularis (Fig 5). The anastomosis is completed by approxi- mation of the mesosalpinx and serosa with interrupted 8-0 suture (Fig 6). There should be no tension on the su- ture line. When the anastomosis is com- plete, the pelvis is lavaged to remove debris and blood clots. A routine laparotomy closure is then performed.
Postoperatively, the nurse removes the electrosurgical pad and checks the site for skin integrity. The pediatric Foley catheter is removed from the uterus, and the patient is cleaned of blood and dye. The nurse sees that the patient is safe and properly aligned dur- ing transfer to the recovery room stretcher. The OR nurse reports the pa- tient’s status to the recovery room nurse.
The success of the reversal of the tubal ligation depends somewhat on the extent of tubal destruction. Cauteriza- tion destroys much of the tube so the potential for a successful reversal is low. With the Pomeroy method, the destruc- tion is minimal, and the ends of the tubes can be brought together with lit- tle tension. During reversal after ring application, the ring and any blocked tube are removed before bringing the
Fig 4. A suture is placed in the mesosalpinx adjacent to the oviduct to take up tension and facilitate anastomosis. Fig 5. The lumens are approximated by placing 8-0 interrupted sutures through the muscularis. Fig 6. The anastomosis is completed by approximation of the mesosalpinx and serosa with interrupted 8-0 suture.
AORN Journal, February 1983, Vol37, No 2 203
two ends together. Both the Pomeroy and ring method have a higher poten- tial for successful reversal than the cauterization method.8
The site of the tubal ligation also af- fects the outcome. Ligation of a segment at the midisthmus of the fallopian tube offers the best opportunity for reversal. If fimbriectomies have been performed, there is minimal chance for success.B
Requests for reversal procedures seem to be a growing trend. It is the responsibility of the nurses caring for these patients to familiarize themselves with these surgical interventions and the nursing care requirements. , 0 Notes
1. Jordan M Phillips, “Gynecologic mi- crosurgery- a deja vu of laparoscopy,” Journal of Reproductive Medicine 22 (March 1979) 135-1 37.
2. Ibid, 137. 3. Paulette Bouchard, “Another chance-tuba1
ligation reversals offer hope for many couples,” News from Brigham and Women‘s Hospital (Spring
4. Phillips, ”Gynecologic microsurgery,” 137. 5. Victor Gomel, “Microsurgical reversal of
female sterilization-a reappraisal,” Fertility and Sterility 33 (March 1979) 135143.
1982) 2-3.
6. Ibid. 7. lbid. 8. Bouchard, “Another chance.” 2-3. 9. Gomel, “Microsurgical reversal,” 138.
Suggested reading Fazez. Jamil A; Suleman, 0 S. “Infertility surgery of
the oviduct: Comparison between macrosurgery and microsurgery.” Fertility and Sterility 37 (January 1982).
Gomel, Victor. “Causes of failed reconstructive tubal microsurgery .” Journal of Reproductive Medicine 24 (June 1980) 239-243.
Gomel, Victor. “Laparoscopy prior to tubal surgery for infertility.” Journal of Reproductive Medicine 18 (May 1977) 251-253.
Winston, R M L. “Microsurgical tubocornual anas- tomosis for reversal of sterilization.” Lancet 1 (Feb 5. 1977) 284.
Thorough testing needed to treat sleep disorders Patients complaining of fatigue or an inability to sleep may be suffering from sleep apnea. Reporting at the 68th Annual Clinical Congress of the American College of Surgeons, Nancy L Snyderman, MD, said that while sleep apnea is rare, it is not known how many cases are missed or improperly treated.
At the Western Psychiatric Institute, Pittsburgh, Dr Snyderman and her associates tested 27 patients who had been referred to the institute’s sleep disorder laboratory. All patients underwent tests to determine the activity of their brain, heart, and muscles while sleeping. Physical and psychological examinations were also conducted. Air flow and respiratory activity were monitored. Patients who had more than 30 apneic episodes lasting more than 30 seconds were considered to have sleep apnea.
There are two types of apnea. In obstructive apnea, the airflow past the person’s nose and mouth stops, but his breathing is normal. Central apnea differs in that the area of brain that controls breathing malfunctions. In this study, half of the 27 patients had obstructive apnea, one fourth had central sleep apnea, and the remaining patients had a combination of obstructive apnea and central sleep apnea.
The usual treatment for obstructive apnea is a tracheostomy. Dr Snyderman suggests weight loss or use of a nasophatyngeal airway before surgical intervention. Most patients who suffer from sleep apnea are obese.
For patients with central or mixed apnea, a tracheostomy would not help to relieve the patient’s condition. Treatment for these patients is unclear. Dr Snyderman said the patients should avoid drinking alcoholic beverages and should not use other drugs. Antidepressant therapy has been helpful for some patients.
204 AORN Journal, February 1983, Vol37, No 2