microsurgical anatomy of the temporal stem: clinical ... · j neurosurg / volume 112 / may 2010 j...
TRANSCRIPT

J Neurosurg / Volume 112 / May 2010
J Neurosurg 112:1033–1038, 2010
1033
DescribeD by Ebeling and von Cramon6 in 1992, the temporal stem is a thin band of white matter concentrating long and short association fibers
that connects the frontal and temporal lobes. Our aim in this anatomical study was to describe the temporal stem and explain the spread of seizures originating from the mesial temporal structures to better understand malignant tumoral extension between adjacent temporal and frontal lobes over the temporal stem (such as gliomatosis).
MethodsSixteen hemispheres (8 brains) of formalin-fixed
normal adult human brains of both sexes were examined. The Klingler fiber dissection method10 was applied with the aid of a Zeiss operating microscope (magnification range 6–40). Each brain was removed from the cranium no longer than 12 hours postmortem, and fixed in a 10% formalin solution for at least 3 months, suspended by the
Microsurgical anatomy of the temporal stem: clinical relevance and correlations with diffusion tensor imaging fiber tracking
Laboratory investigation Johann Peltier, M.D.,1,3 SébaStien Verclytte, M.D.,2 chriStine DelMaire, M.D., Ph.D.,2 Jean-Pierre PruVo, M.D., Ph.D.,2 oliVier GoDefroy, M.D., Ph.D.,3 anD Daniel le GarS, M.D., Ph.D.1 1Laboratoire d’Anatomie et d’Organogenèse, Université de Picardie Jules Verne, Amiens; 2Service de Neuroradiologie, CHRU Lille; and 3Laboratoire Neurosciences Fonctionnelles et Pathologie UMR CNRS 8160, Université de Picardie Jules Verne, Amiens, France
Object. The authors used a fiber dissection technique to describe the temporal stem and explain the tendency of malignant tumors to spread within both the frontal and temporal lobes. The authors focused on the morphological characteristics and course of various fasciculi of the temporal stem, including the uncinate fascicle, occipitofrontal fascicle, anterior commissure, loop of the optic radiations (Meyer loop), and the ansa peduncularis.
Methods. Eight previously frozen, formalin-fixed human brains were dissected under an operating microscope using the fiber dissection technique described by Klingler. Lateral, inferior, and medial approaches were made. Cross-sectional 3D MR images obtained in 10 patients without brain lesions demonstrated that fibers of the temporal stem, which were intermingled together in various ways, curved laterally within the basal forebrain. Various pathological entities affecting the temporal stem are described and discussed.
Results. The uncinate fascicle has 3 portions: a ventral extension, an intermediary segment called the isthmus, and a dorsal segment. The inferior occipitofrontal fasciculus is a layer of more superficial white matter that appeared to be superior to the uncinate fasciculus. A short ventral portion of the radiations of the corpus callosum was some-times noted to run ventrally to enter the temporal stem and to reach both temporal lobes.
Conclusions. To the authors’ knowledge, a detailed anatomy of the temporal stem has not been previously described in the literature. The unique anatomy of the temporal stem provides a route for tumor spread between the frontal and temporal lobes. (DOI: 10.3171/2009.6.JNS08132)
Key WorDS • temporal stem • white matter • fiber dissection technique • uncinate fasciculus • anterior commissure • optic radiation • corpus callosum
1033
Abbreviations used in this paper: CC = corpus callosum; MCA = middle cerebral artery.
This article contains some figures that are displayed in color on line but in black and white in the print edition.
J. Peltier et al.
1034 J Neurosurg / Volume 112 / May 2010
basilar artery to avoid deformation. The specimens were washed under running water for several hours, and the arachnoid mater and vessels were completely removed. The brains were then refrigerated at temperatures ranging from −10 to −15°C for 15 days. Because water increases 10% in volume with the formation of ice, the fibers were somewhat spread apart after refrigeration. The primary dissection tools were handmade thin, wooden, and curved metallic spatulas with various tip sizes.
In addition, 10 patients without brain lesions were studied. Tractography was accomplished by placing ini-tiation and termination sites (seed and target points) in both frontal and temporal regions. All MR images were obtained using a 1.5-T whole-body unit with echo planar capabilities and a standard whole-head transmitter-receiv-er coil (Vision, Siemens, and Signa EchoSpeed, General Electric Medical Systems). Before calculating fractional anisotropy, the Philips Research Integrated Development Environment registration tool was used to remove eddy current distortions and head motion. Philips Fiber Track-ing 4.1V3 software was used to plot fiber tracts and deter-mine fractional anisotropy.
ResultsThe human adult temporal stem is completely en-
closed and concealed under the lateral orbital and supe-rior temporal gyri in the depths of the lateral fissure. The prominent caudatolenticular bridges of gray matter cross-ing the anterior limb of the internal capsule were easily visible and resected. We found the fibers of the temporal stem to be intermingled in various ways.
Anterior Commissure The anterior commissure constitutes a bundle of
white matter almost completely surrounded by gray mat-ter, found after removal of the head of the caudate nucle-us. This structure resembles bicycle handlebars crossing the midline just ventral to the supraoptic recess of the
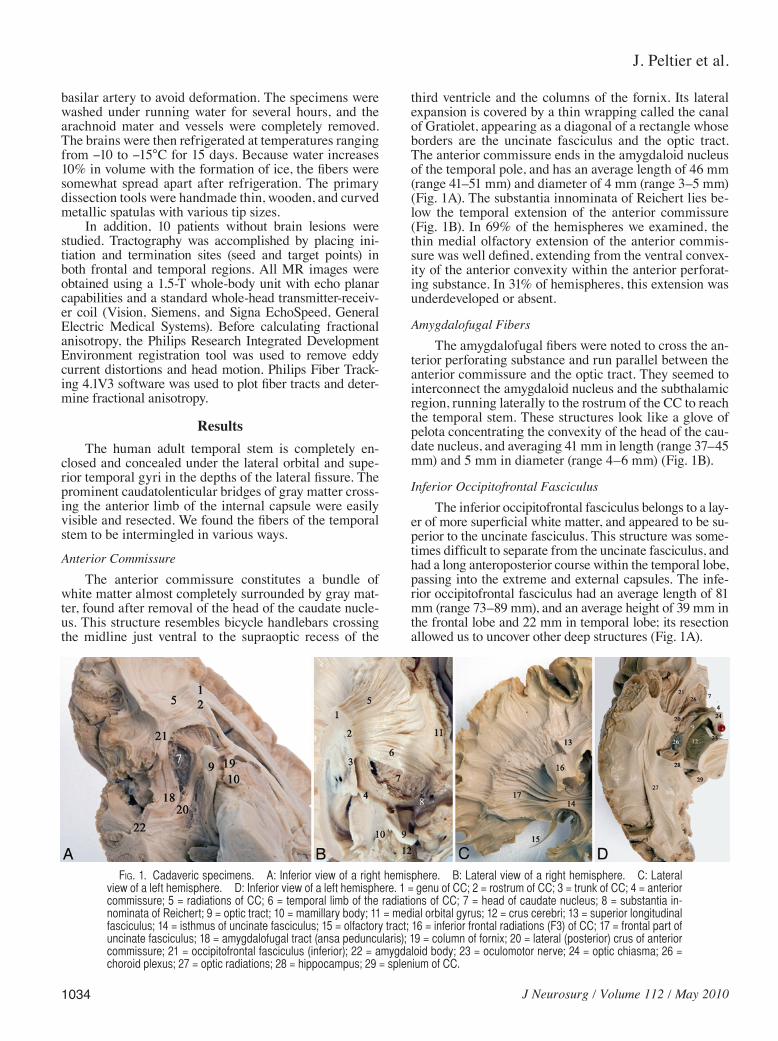
third ventricle and the columns of the fornix. Its lateral expansion is covered by a thin wrapping called the canal of Gratiolet, appearing as a diagonal of a rectangle whose borders are the uncinate fasciculus and the optic tract. The anterior commissure ends in the amygdaloid nucleus of the temporal pole, and has an average length of 46 mm (range 41–51 mm) and diameter of 4 mm (range 3–5 mm) (Fig. 1A). The substantia innominata of Reichert lies be-low the temporal extension of the anterior commissure (Fig. 1B). In 69% of the hemispheres we examined, the thin medial olfactory extension of the anterior commis-sure was well defined, extending from the ventral convex-ity of the anterior convexity within the anterior perforat-ing substance. In 31% of hemispheres, this extension was underdeveloped or absent.
Amygdalofugal FibersThe amygdalofugal fibers were noted to cross the an-
terior perforating substance and run parallel between the anterior commissure and the optic tract. They seemed to interconnect the amygdaloid nucleus and the subthalamic region, running laterally to the rostrum of the CC to reach the temporal stem. These structures look like a glove of pelota concentrating the convexity of the head of the cau-date nucleus, and averaging 41 mm in length (range 37–45 mm) and 5 mm in diameter (range 4–6 mm) (Fig. 1B).
Inferior Occipitofrontal FasciculusThe inferior occipitofrontal fasciculus belongs to a lay-
er of more superficial white matter, and appeared to be su-perior to the uncinate fasciculus. This structure was some-times difficult to separate from the uncinate fasciculus, and had a long anteroposterior course within the temporal lobe, passing into the extreme and external capsules. The infe-rior occipitofrontal fasciculus had an average length of 81 mm (range 73–89 mm), and an average height of 39 mm in the frontal lobe and 22 mm in temporal lobe; its resection allowed us to uncover other deep structures (Fig. 1A).
Fig. 1. Cadaveric specimens. A: Inferior view of a right hemisphere. B: Lateral view of a right hemisphere. C: Lateral view of a left hemisphere. D: Inferior view of a left hemisphere. 1 = genu of CC; 2 = rostrum of CC; 3 = trunk of CC; 4 = anterior commissure; 5 = radiations of CC; 6 = temporal limb of the radiations of CC; 7 = head of caudate nucleus; 8 = substantia in-nominata of Reichert; 9 = optic tract; 10 = mamillary body; 11 = medial orbital gyrus; 12 = crus cerebri; 13 = superior longitudinal fasciculus; 14 = isthmus of uncinate fasciculus; 15 = olfactory tract; 16 = inferior frontal radiations (F3) of CC; 17 = frontal part of uncinate fasciculus; 18 = amygdalofugal tract (ansa peduncularis); 19 = column of fornix; 20 = lateral (posterior) crus of anterior commissure; 21 = occipitofrontal fasciculus (inferior); 22 = amygdaloid body; 23 = oculomotor nerve; 24 = optic chiasma; 26 = choroid plexus; 27 = optic radiations; 28 = hippocampus; 29 = splenium of CC.

J Neurosurg / Volume 112 / May 2010
Microsurgical anatomy of the temporal stem
1035
Corpus CallosumA short ventral portion of the radiations of the CC
seemed to belong to the temporal stem; to our knowledge this has not been previously described in the literature. These radiations had an average length of 62 mm (range 56–68 mm) and diameter of 8 mm (range 6–11 mm).
Uncinate FascicleThe uncinate fascicle had 3 parts: a ventral or frontal
extension, an intermediary segment called the isthmus or insular segment that lies in the limen insulae area, and a temporal or dorsal segment. The posterosuperior margin was attached to the rostral border of the occipitofrontal fasciculus. The medial fibers seemed to reach the baso-lateral nucleus of the amygdala. The length of the unci-nate fasciculus averaged 45 mm (range 40–49 mm) in our specimens, and the average width of the frontal extension was 20 mm. This was interrupted in its dorsal part by several inferior callosal radiations emerging from the foot of inferior frontal gyrus or the pars opercularis of F3 (the Broca center or area 44) (Fig. 1C). The breadth of the temporal portion averaged 46 mm.
Meyer LoopThe initial portion of the optic radiations, called the
Meyer loop, cover the extremities of the uncinate fascicu-lus and the lateral extension of the anterior commissure. More medially, the temporal tip of the choroid plexus constitutes a dorsomedial boundary of the temporal stem (Fig. 1D). More dorsally located is the hippocampus, with an average head height of 8 mm and a frontal diameter of 14 mm.
Cross-sectional 3D MR images showed that fibers of the temporal stem curved dorsally in a fan-shaped arrange-ment. We noted that the medial olfactory extension of the anterior commissure was never visible on MR images. The fact that the fibers of the temporal stem were intermingled in various directions to form a dense 3D network encom-passing all the white matter created too many artifacts for accurate tractography in this area (Fig. 2). A drawing sum-marizes these fasciculi within the temporal stem (Fig. 3).
DiscussionMorphological Characteristics of the Temporal Stem
Several fasciculi—including the Meyer loop of the optic radiation, the uncinate fasciculus, the occipitofrontal fasciculus, the anterior commissure, the inferior thalamic peduncle, the posterior thalamic peduncle, the extreme capsule, the temporopontine fibers, the corticotectal fi-bers, the corticotegmental fibers, and the occipitopontine fibers—are embedded in a dense network within the tem-poral stem.2,20,21,36,37
The anterior bundle of the optic radiation initially crosses ventrally over the roof of the inferior horn, then turns backward, forming the so-called Meyer loop or the temporal knee around the tip of the temporal horn. The optic radiations run below the inferior longitudinal fas-ciculus,1,20,21,31,32 and extend for a variable distance in the
temporal pole along 5 mm in front of the temporal horn, 15–30 mm behind the tip of the temporal pole, and 5 mm anterior to the hippocampus head.21,24 The Meyer loop has an anterior concavity and drapes behind the distal por-tion of the anterior commissure, whose lateral expansion appears to follow a counterclockwise rotation similar to the pattern of a hemp rope.20 Some fibers of the anterior commissure merge into the anterior loop.30,31 The Meyer loop extends anteriorly up to the lateral surface of the amygdaloid nucleus in the vicinity of the anterior com-missure.
The uncinate fascicle is a long ipsihemispheric asso-ciation fascicle with a hooklike shape that sharply curves ventrally at the limen insulae region underneath the puta-men and the claustrum. Its mean width and height in our specimens were 7 and 5 mm, respectively. This structure originates like a double fan from the ventral 3 temporal gyri (areas 20 and 38) in front of the tip of the inferior horn and the cortical nuclei of the amygdala (areas 28, 34, and 36) and joins the gyrus rectus (area 11), the medial retroorbital cortex (area 12), and subcallosal area (area 25), after passing underneath the MCA. The uncinate fas-ciculus has been reported to be asymmetrical in 80% of those examined, and is on average 27% larger and con-tains one-third more fibers in the right than the left hemi-
Fig. 2. Axial (upper) and sagittal (lower) MR images showing 3D re-construction of the temporal stem. 4 = anterior commissure; 17 = frontal part of uncinate fasciculus; 20 = lateral (posterior) crus of anterior com-missure; 21 = occipitofrontal fasciculus (inferior); 27 = optic radiations; 30 = Meyer loop.

J. Peltier et al.
1036 J Neurosurg / Volume 112 / May 2010
sphere.6,7,23,29–32 Nevertheless, there were no significant differences for age or sex.23
The occipitofrontal fasciculus is a long association bundle that goes through the basal portion of the insula, immediately rostral to the uncinate fasciculus.32 It appears to include fibers connecting the auditory (area 22) and vi-sual association cortex (areas 20 and 21) in the temporal lobe with the prefrontal cortex (areas 54 and 55).9
The anterior commissure belongs to the interhemi-spheric commissural system. It is almost completely sur-rounded by gray matter, resembles bicycle handlebars, and crosses the midline just anterior to the anterior col-umns of the fornices.17 The medial extension (or anterior crus) connects both olfactory systems, creating a real ol-factive commissure.19 The lateral extension of the anterior commissure passes through the basal portion of the glo-bus pallidus—perpendicular to the optic tract and medial to the uncinate fasciculus—to the temporal region.4,29 Its lateral relationships are the fasciculus olfactorius, the nu-cleus accumbens septae, the head of the caudate nucleus, the anterior limb of the internal capsule, and the puta-men.17,22
More medially, after removal of the lateral extension of the anterior commissure, we can see the ansa pedun-
cularis, which is composed of amygdaloseptal (diagonal band of Broca), amygdalohippocampic, and amygdalo-thalamic fibers (or pedunculus thalami extracapsularis).32
The sagittal stratum is made of these 2 last fasciculi (the inferior longitudinal fasciculus and the optic radia-tions) and the posterior thalamic peduncle (which con-tains the optic radiations). It is a large white matter tract that is oriented in a sagittal plane and passes from the temporal to the occipital lobe.31
Temporal Stem, Epilepsy, and Brain TumorsThe temporal stem—including the uncinate fascicu-
lus, the stria terminalis, the fornix and the amydgdalofugal fibers—seems to be the preferential pathway for seizure spread. The main sites of seizure origin are the hippocam-pal formation more than the amygdala.11,13 In addition, the inferior occipitofrontal fasciculus seems to produce the vi-sual hallucinations that can accompany epilepsy.25
Tumors of the temporal stem represent 13% of tu-mors of the limbic and paralimbic system. Tumors in this region average > 5 cm in diameter.36 The temporal stem, a well-myelinated structure, constitutes a pathway of glio-ma dissemination and helps to explain the phenomena of gliomatosis cerebri and multicentricity. In addition, tu-mors can spread within the confines of the allocortical/mesocortical zones while sparing adjacent neocortical areas and medial structures such as the claustrum, puta-men, pallidum, and capsules.35,37 An infiltrating insular glioma involving the frontal opercula and the frontoor-bital gyrus via the temporal stem is shown in Fig. 4. This rostrocaudal tumoral spread is in contrast with the frontal spread across the CC. Slow growing, low-grade temporal tumors are one of the most common causes of epilepsy of children.3
Fig. 4. Representative axial T1-weighted MR image showing a right high-grade glioma involving the ventral portion of the insula, the frontal opercula, and the frontoorbital gyrus via the temporal stem.
Fig. 3. Drawing of the different components within the temporal stem. 1 = genu of CC; 7 = head of caudate nucleus; 8 = substantia in-nominata of Reichert; 14 = isthmus of uncinate fasciculus; 19 = column of fornix; 20 = lateral (posterior) crus of anterior commissure; 21 = oc-cipitofrontal fasciculus (inferior); 24 = optic chiasma; 30 = Meyer loop; 31 = caudatolenticular bridges; 32 = anterior limb of internal capsule; 33 = supraoptic recess of third ventricle (of Vieussens); 34 = cells of Calleja; 35 = nucleus of stria terminalis; 36 = ventral pallidum; 37 = diagonal band of Broca; 38 = nuclei septum (with nucleus basalis of Meynert).

J Neurosurg / Volume 112 / May 2010
Microsurgical anatomy of the temporal stem
1037
The uncinate fascicle allows seizure propagation, and its partial interruption can decrease the number and inten-sity of seizures. Because the temporal stem is very deep and contains critical structures that must be preserved, complete resection of lesions in this region is not always possible due to the decreasing volume of the critical epi-leptogenic mass.38
Temporal Stem and Surgical ApproachesOrbitofrontal insular temporal pole tumors can be re-
moved with a special attention to the origin and course of the lenticulostriate vessels as the neurosurgeon enters the anterior perforating substance in the region of the unci-nate fasciculus. It is important to note that the uncinate fasciculus underlies the MCA. This knowledge is critical so that the surgeon can avoid injury to the M1 segment of the MCA during removal of insular gliomas.35,36
To avoid retraction of the temporal lobe and dam-age to the temporal stem, especially the optic radiations, some authors have proposed the anterior transsylvian and subtemporal transfusiform approaches.37
The anterior transsylvian route opens the insular cis-tern along the gyrus of Heschl and provides an “inside-out” orientation with a circumferential handling of the anatomy of the mesial temporal lobe. The inferior (tem-poral) horn is entered via a corticectomy through the su-perior temporal gyrus at the level of the limen insulae. Thus it allows the surgeon to avoid possible harm to the optic radiation, the anterior commissure, and the main components of the temporal stem, except the anterior part of the uncinate fasciculus, which will be transected. Ad-vantages to this approach are both the preservation of the language area and visual pathways, avoiding sacrifice of normal cortical tissue.14,16,26,37
More recently, a transsylvian, transcisternal, mesial en bloc resection has been proposed for hippocampal scle-rosis. A semicircular opening of the dura is made above the sylvian fissure, and the arachnoid of the interpedun-cular cistern is opened, exposing the basal arteries. The medial face of the parahippocampal gyrus rhinal sulcus is then visible. Resection of the anterior hippocampus and amygdala is made en bloc up to the midmesencephalic level, and facilitated by following the medial wall of the opened inferior horn of the lateral ventricle. This approach preserves the lateral and laterobasal temporal lobe. How-ever, this route can cause temporary mechanical irritation of the oculomotor nerve in 9% of patients explained by an arachnoid tunnel, which represents the lateral duplicate extension of the Liliequist membrane. From 3 to 13% of patients present with contralateral superior quadranopia, which is never perceived in daily life.3,33
The subtemporal transfusiform gyrus approach to the parahippocampal gyrus spares the lateral temporal neocortex with its higher cortical functions but can cause injury to the vein of Labbé or to a well-developed basal temporal bridging vein, and gives direct or retraction-related injury to the inferior temporal gyrus, as demon-strated on postoperative MR images. These approaches through T-4 can be facilitated by removing the zygomatic arch.5,15,28
During frontal lobectomy, care must be taken to pre-
serve a part of the basifrontal cortex including the gyrus rectus to maintain the connections between Brodmann area 11 and the amygdala.
Temporal Stem, Functional Significance, and Cognitive Pathology
The temporal stem plays an important role in numer-ous of disorders, including amnesia, Klüver-Bucy syn-drome, traumatic brain injury, and Alzheimer disease.9 Surgical approaches in the temporal lobe often generate behavior changes that can be better understood if the ef-fects on the white matter structures are considered, espe-cially connections with the orbitofrontal region and lim-bic system. The anterior commissure plays a role in the interhemispheric transfer of visual, auditory, and olfac-tory information between temporal lobes in humans.34
Fortunately, during severe diffuse axonal injury, the temporal stem is only involved in 6–8% of vegetative pa-tients in comparison to the posterior part of the CC, which is involved in 100% of patients, or the rostral brainstem, which is involved in 74%.8 The uncinate fasciculus carries cholinergic fibers from the basal nucleus of Meynert, in-nervating the anterior temporal lobe.27
The temporal stem and the superior temporal gyrus play an important role in social cognition, social impair-ment, regulation of behavior, and neuromechanism of im-itation. The authors of several analyses have shown that a reduction in the white matter of the temporal stem area may occur in individuals with autism.12,18 However, there are no significant differences in either the mean age or any of the diffusion tensor imaging measures in patients with autism who are taking psychotropic medications versus those who are not.12
ConclusionsAlthough many fasciculi developed in our cadavers
and were also visualized separately using diffusion tensor imaging in living patients, this radiological method has the limitation of being unable to resolve detail of cross-ing and intermingled bundles. Our data provide detailed information regarding all white matter structures and should assist the surgeon in proper preoperative planning and intraoperative decision making, leading to a reduc-tion in perioperative morbidity and death, especially in glioma resections.
Disclaimer
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Acknowledgment
The authors are grateful to Jean-Noel Gobeaut of Laboratory Achrome Photo for preparing the illustrations.
References
1. Archambault L: Le faisceau longitudinal inférieur et le fais-ceau optique central: quelques considérations sur les fibres
J. Peltier et al.
1038 J Neurosurg / Volume 112 / May 2010
d’association du cerveau. Rev Neurol (Paris) 4:1206–1222, 1906
2. Bailey P, von Bonin G, Garol HW, McCulloch WS: Long association fibers in cerebral hemispheres of Monkey and Chimpanzee. J Neurophysiol 6:129–146, 1943
3. Cataltepe O, Turanli G, Yalnizoglu D, Topçu M, Akalan N: Surgical management of temporal lobe tumor-related epilepsy in children. J Neurosurg 102 (3 Suppl):280–287, 2005
4. Chabardès S, Kahane P, Minotti L, Hoffmann D, Benabid AL: Anatomy of the temporal pole region. Epileptic Disord 4 (1 Suppl):S9–S15, 2002
5. D’Angelo VA, Galarza M, Catapano D, Monte V, Bisceglia M, Carosi I: Lateral Ventricle Tumors: Surgical strategies ac-cording to tumor origin and development: a series of 72 cases. Neurosurgery 56 (1 Suppl):36–45, 2005
6. Ebeling U, Cramon DV: Topography of the uncinate fascicle and adjacent temporal fiber tracts. Acta Neurochir (Wien) 115:143–148, 1992
7. Ebeling U, Reulen HJ: Neurosurgical topography of the optic radiation in the temporal lobe. Acta Neurochir (Wien) 92: 29–36, 1988
8. Kampfl A, Franz G, Aichner F, Pfausler B, Haring HP, Felber S, et al: The persistent vegetative state after closed head in-jury: clinical and magnetic resonance imaging findings in 42 patients. J Neurosurg 88:809–816, 1998
9. Kier EL, Staib LH, Davis LM, Bronen RA: MR Imaging of the temporal stem: anatomic dissection tractography of the uncinate fasciculus, inferior occipitofrontal fasciculus, and Meyer’s loop of the optic radiation. AJNR Am J Neurora-diol 25:677–691, 2004
10. Klingler J: Erleichterung der makroskopischen Praeparation des Gehirns durch den Gefrierprozess. Schweiz Arch Neurol Psychiat 36:247–256, 1935
11. Klingler J, Gloor P: The connections of the amygdala and the anterior temporal cortex in the human brain. J Comp Neurol 115:333–369, 1960
12. Lee JE, Bigler ED, Alexander AL, Lazar M, DuBray MB, Chung MK, et al: Diffusion tensor imaging of white matter in the superior temporal gyrus and temporal stem in autism. Neurosci Lett 424:127–132, 2007
13. Mayanagi Y, Watanabe E, Kaneko Y: Mesial temporal lobe epilepsy: clinical features and seizure mechanism. Epilepsia 37 (3 Suppl):57–60, 1996
14. Miyagi Y, Shima F, Ishido K, Araki T, Taniwaki Y, Okamoto I, et al: Inferior temporal sulcus approach for amygdalohip-pocampectomy guided by a laser beam of stereotactic naviga-tor. Neurosurgery 52:1117–1124, 2003
15. Miyamoto S, Kataoka H, Ikeda A, Takahashi J, Mikuni N, Usui K, et al: A combined subtemporal and transventricular/transchoroidal fissure approach to medial temporal lesions. Neurosurgery 54:1162–1169, 2004
16. Nagata S, Sasaki T: Lateral transsulcal approach to asymp-tomatic trigonal meningiomas with correlative microsurgical anatomy: technical case report. Neurosurgery 56 (2 Suppl): E438, 2005
17. Naidich TP, Daniels DL, Pech P, Haughton VM, Williams A, Pojunas K: Anterior commissure: anatomic-MR correlation and use as a landmark in three orthogonal planes. Radiology 158:421–429, 1986
18. Neeley ES, Bigler ED, Krasny S, Ozonoff S, McMahon W, Lainhart JE: Quantitative temporal lobe differences: autism distinguished from controls using classification and regres-sion tree analysis. Brain Dev 29:389–399, 2007
19. Nieuwenhuys R, Voogd J, Huijzen C: The Human Central Nervous System: A Synopsis and Atlas, ed 3. Berlin: Spring-er, 1988
20. Peltier J, Travers N, Destrieux C, Velut S: Optic radiations: a
microsurgical anatomical study. J Neurosurg 105:294–300, 2006
21. Peuskens D, Van Loon J, Van Calenberg F, Van den Bergh R, Goffin J, Plets C: Anatomy of the anterior temporal lobe and the frontotemporal region demonstated by fiber dissection. Neurosurgery 55:1174–1184, 2004
22. Powell TPS, Cowan WM, Raisman G: Olfactory relationships of the diencephalon. Nature 199:710–712, 1963
23. Rodrigo S, Oppenheim C, Chassoux F, Golestani N, Cointepas Y, Poupon C, et al: Uncinate fasciculus fiber tracking in mesial temporal lobe epilepsy. Initial finding. Eur Radiol 17:1663–1668, 2007
24. Rubino PA, Rhoton AL, Tong X, de Oliveira E: Three-dimen-sional relationships of the optic radiation. Neurosurgery 57 (3 Suppl):219–227, 2005
25. Schneider RC, Crosby EC, Farhat SM: Extratemporal lesions triggering the temporal lobe syndrome. J Neurosurg 22:246–253, 1965
26. Schramm J, Kral T, Clusmann H: Transsylvian keyhole func-tional hemispherectomy. Neurosurgery 49:891–901, 2001
27. Selden NR, Gitelman DR, Salamon-Muryama N, Parrish TB, Mesulam MM: Trajectories of cholinergic pathways within cerebral hemispheres in the human brain. Brain 121:2249–2257, 1998
28. Sincoff EH, Tan Y, Saleem IA: White matter fiber dissection of the optic radiations of the temporal lobe and implications for surgical approaches to the temporal horn. J Neurosurg 101:739–746, 2004
29. Sindou M, Guenot M: Surgical anatomy of the temporal lobe of epilepsy surgery. Adv Tech Stand Neurosurg 28:315–343, 2003
30. Türe U, Yaşargil DCH, Al-Mefty O, Yaşargil MG: Topo-graphic anatomy of the insular region. J Neurosurg 90:720–733, 1999
31. Türe U, Yaşargil MG, Friedman AH, Al-Mefty O: Fiber dis-section technique: lateral aspect of the brain. Neurosurgery 47:417–426, 2000
32. Türe U, Yaşargil MG, Pait TG: Is there a superior occipito-frontal fasciculus? A microsurgical anatomic study. Neuro-surgery 40:1226–1232, 1997
33. Vajkoczy P, Krakow K, Stodieck S, Pohlmann-Eden B, Schmie-dek P: Modified approach for selective treatment of temporal lobe epilepsy: transsylvian-transcisternal mesial en bloc resec-tion. J Neurosurg 88:855–862, 1998
34. Wilde EA, Bigler ED, Haider JM, Chu Z, Levin HS, Li X, et al: Vulnerability of the anterior commissure in moderate to severe pediatric traumatic brain injury. J Child Neurol 21: 769–776, 2006
35. Yakovlev PI: Pathoarchitectonic studies of cerebral malforma-tions. J Neuropathol Exp Neurol 18:22–55, 1959
36. Yaşargil MG, von Ammon K, Cazavos E, Doczi T, Reeves JD, Roth P: Tumours of the limbic and paralimbic systems. Acta Neurochir (Wien) 118:40–52, 1992
37. Yaşargil MG, Yaşargil DCH: Impact of temporal lobe surgery. J Neurosurg 101:725–738, 2004
38. Zaatreh MM, Firlick KS, Spencer DD, Spencer SS: Temporal lobe tumoral epilepsy: characteristics and predictors of surgi-cal outcome. Neurology 61:636–641, 2003
Manuscript received March 14, 2008.Accepted June 3, 2009.Please include this information when citing this paper: pub-
lished online July 17, 2009; DOI: 10.3171/2009.6.JNS08132.Address correspondence to: Johann Peltier, M.D., Service de Neu -
rochirurgie, Centre Hospitalier Universitaire d’Amiens, Place Victor Pauchet, 80054 Amiens, cedex 1, France. email: [email protected].