mild children: associated with - jnnp.bmj.comjnnp.bmj.com/content/jnnp/59/4/375.full.pdf ·...
TRANSCRIPT

J7ournal ofNeurology, Neurosurgery, and Psychiatry 1995;59:375-380
Mild head injury in preschool children: evidencethat it can be associated with a persisting cognitivedefect
Philip Wrightson, Valerie McGinn, Dorothy Gronwall
AbstractThis study describes the effect of mildhead injury in preschool children onaspects of their cognitive performance inthe year after injury and at the age of 6*5years, with particular reference to thedevelopment of reading skills. Mild headinjury was defined by diagnosis at a hos-pital emergency department of a headinjury which was not severe enough toneed admission for observation. Seventyeight such children were compared with agroup of86 with a minor injury elsewhere.The groups had similar developmental,family, and socioeconomic status. Therewere no differences in cognitive tests soonafter the injury, but at six months and oneyear children with mild head injuryscored less than controls on one test, solv-ing a visual puzzle (visual closure); theywere also more likely to have had anothermild head injury. At 6-5 years of age theystill scored less than controls, readingability was related to their visual closurescore at one year, and they were morelikely to have needed help with reading.Mild head injury seems to be able to
produce subtle but significant changeswhich can affect school performance.
(7 Neurol Neurosurg Psychiatry 1995;59:375-380)
Keywords: preschool children; head injury; cognitiveimpairment
Department ofNeurosurgery,Auckland Hospital,Private Bag 92024,Auckland,New ZealandP WrightsonV McGinnD GronwallCorrespondence to:Mr Philip Wrightson,18 Crocus Place, Remuera,Auckland 1005,New Zealand.Received 25 November 1994and in revised form1 May 1995Accepted 17 May 1995
Some children who have a mild head injury dobadly at school afterwards, either because oftheir behaviour or because they cannot copewith the school work. Several studies have sug-gested that the head injury is not responsible.One view is that the sort of children who areinjured are more likely to have had behaviourproblems before the injury.'2 Another is thatalthough the children may show defects ofcognitive function, this is not proportional tothe apparent severity of the injury, and that thechanges do not show the pattern of loss andsubsequent recovery typical of CNS damage,so that it is more likely that the deficit wasthere before the injury.3 A long term follow upof children with various injuries suggested thatcognitive changes were common in all, andthat the children with head injuries were notspecially affected.4 It has also been suggestedthat parental overreaction and family dysfunc-tion may be a factor.5Our previous work had shown that in adults
the defects of cognitive function that followa mild head injury can persist for manymonths,67 and we saw no reason why childrenshould be different. In 1982, prompted bysuggestions from teachers and parents thatyoung children who had had head injurieswere slow in learning to read, a pilot study wascompleted comparing 10 preschool childrenwith mild head injury with 10 matched for thefactors known to affect learning. No differencebetween the groups was found immediatelyafter the injury, but eight months later thechildren with head injury were less able tocomplete visual puzzles. It seemed reasonableto suppose that children who found this diffi-cult might have problems in learning to read,and further investigation of this area wasclearly warranted.
There are, however, practical problems inshowing changes of cognitive function andtheir relation to injury in preschool children.Assessment of very young children is difficult.It may be complicated by factors such as shy-ness, distractability, and developmental delay,which are not related to the accident. Further,they belong to a group in which informationon academic achievement is absent, so that thechild's capacity before the head injury cannotbe estimated. On the other hand the familyand socioeconomic factors which affect learn-ing at this age have been well documented andcan be allowed for. Also, as this is a period ofintense learning activity loss of capacity mightbe expected to produce greater effects than inolder children.A more rigorous investigation was therefore
planned, with the hypothesis that mild headinjury in preschool children would affect theirlearning to read. The development of this skillhas been well studied and quantified, andwould provide a good endpoint. The childrenwould be followed up for a year from the dateof their accident, and then seen again at theage of 6'5 years when their school progressand particularly their reading skills would beassessed.
Subjects and methodsSUBJECTSConsecutive names were taken from therecords of two general hospitals of childrenwho had attended the accident departmentsand had been diagnosed as having had either amild head injury (HI group) or a minor injuryto another part of the body (control group).Within a week of the accident the parents weretelephoned and their consent to enter the
375
on 22 July 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.4.375 on 1 October 1995. D
ownloaded from

Wrightson, McGinn, Gronwall
children into the study sought. The child wasincluded providing: (1) that hospital admis-sion had not been needed; (2) that the childwas between 2-5 and 4-5 years old; (3) thatthere was no history of previous head injury oranother condition which might confuse theissue; and (4) that the first language spoken athome was English.
Eighty nine children were identified as pos-sible subjects for each group (HI and control).11 of the HI group and three of the controlshad then to be excluded because of a previoushead injury, leaving 78 in the HI group and 86controls.As the investigation progressed head
injuries occurred in both the HI group and thecontrols. These children continued to beexamined but data obtained after the furtherinjury was not used for the present analysis.
METHODSPart 1Each child was seen within a month of theinjury, then six and 12 months later.
Assessments were all made in the child'shome, with the help of a parent. The first wasdone as soon as the parent considered that thechild was well enough to be tested, usuallywithin 14 days of the accident. The otherassessments were done six and 12 monthslater. Two sessions of an hour were needed foreach, both being completed within a week.The following information was obtained:
Clinical history-The parents were asked forthe details of the accident, the immediatesymptoms, and the child's progress after-wards. Note was taken of previous illnesses oraccidents which might affect development. Atthe second and third visits the occurrence ofsubsequent injuries, to the head or elsewhere,was recorded.
Family and socioeconomic status-The agesand education of the parents, the number andage of the siblings, and the child's position inthe family were noted. A measure of socioeco-nomic status designed for use in New Zealandwas recorded.8
Behavioural measures-The Vineland socialmaturity scale9 and the Connors parent ques-tionnaire'0 were used to assess social maturityand behaviour.
Cognitive tests-The Reynell developmentallanguage scales" were used as a broad mea-sure of expressive and receptive language abil-ity. The battery uses a collection of attractivetoys and everyday objects, and is designed forchildren from 1 to 5 years old.The Illinois test of psycholinguistic abilities
(ITPA),'2 which is suitable for children from2-5 to 10 years old, was used to provide anassessment of a wide range of language andrelated cognitive skills. Its 10 subtests are:(1) Auditory reception: deriving meaningfrom spoken questions such as "Do catsbark?"(2) Visual reception: finding the conceptuallyrelated response picture when presented witha stimulus picture.(3) Visual sequential memory: reproducingsequences of geometric figures from memory
after looking at them for five seconds.(4) Auditory association: completing sen-tences such as "I sit on a chair, I sleep ona-
(5) Auditory memory: rememberingsequences of digits.(6) Visual association: finding a responsepicture which goes with a stimulus picture.(7) Visual closure: finding partially concealedobjects embedded in pictures within a timelimit of thirty seconds.(8) Verbal expression: describing commonobjects.(9) Grammatical closure: using appropriategrammar to complete sentences in response topictures.(10) Manual expression: miming the use ofcommon objects.
Part 2The children were seen again when theyreached the age of 6-5 years. They were testedon two occasions, once at home with a parentpresent, and once at school with the coopera-tion of their teacher. The following tests werecarried out:
In the first session, at home, the Illinois testof psycholinguistic abilities, the Connorsparent behaviour questionnaire, and theVineland social maturity scale were given toassess the child's present capacity and to docu-ment change since the previous tests. Parentswere asked about general progress andwhether there had been further head injuries.
In the second session, at school, the testspresented were:(1) The Neale analysis of reading ability:'3 agraded series of illustrated stories with com-prehension questions.(2) Letter knowledge and writing: the child isasked to say the name and the sound of lowerand upper case letters of the alphabet andasked to write six words.(3) Coding subtest of the Wechsler intelli-gence scale for children: this is a timed atten-tion task.(4) Verbal memory passage: this is a measureof immediate and delayed recall using a pas-sage suitable to the child's age.(5) Visual memory test: immediate memoryof four geometric figures adapted from theWechsler memory scale to be suitable for chil-dren.(6) Paired associate learning: a measure ofability to learn verbal material adapted fromthe Wechsler memory scale.(7) Frostig developmental test of visual per-ception: tasks to assess various perceptualskills. 1'(8) Connors teacher's questionnaire: theteacher rates the child on items concerning itsbehaviour at school. It was also noted whetherproblems with reading which required specialtuition had been recognised by the teacher.
STATISTICAL METHODSThe methods used are given with each finding.In analysing the results of the cognitive teststhe raw scores were used as dependent vari-ables. This allowed direct comparison of indi-
376 on 22 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.4.375 on 1 O
ctober 1995. Dow
nloaded from
Mild head injury in preschool children: evidence that it can be associated with a persisting cognitive defect
vidual subjects over time, and avoided theuncertainty of using scores scaled for age someyears before and in a different population.
ETHICAL ISSUESBoth parts of the study were approved by theAuckland Hospital ethics committee. The par-ents were told in detail about the aims of theinvestigation before being asked for consent.In the second part informed consent was alsoobtained from both the Auckland EducationBoard and the principals of the schools visited.
ResultsPART 1Comparability ofgroupsThere was no significant difference betweenthe groups in sex, pre-accident developmentand behaviour, socioeconomic state, ormother's or father's age or education levels. Inthe subjects available for study at one yearthere was a slightly higher proportion ofyounger children in the HI group, the meanand median ages being 3-38 and 3-25 years
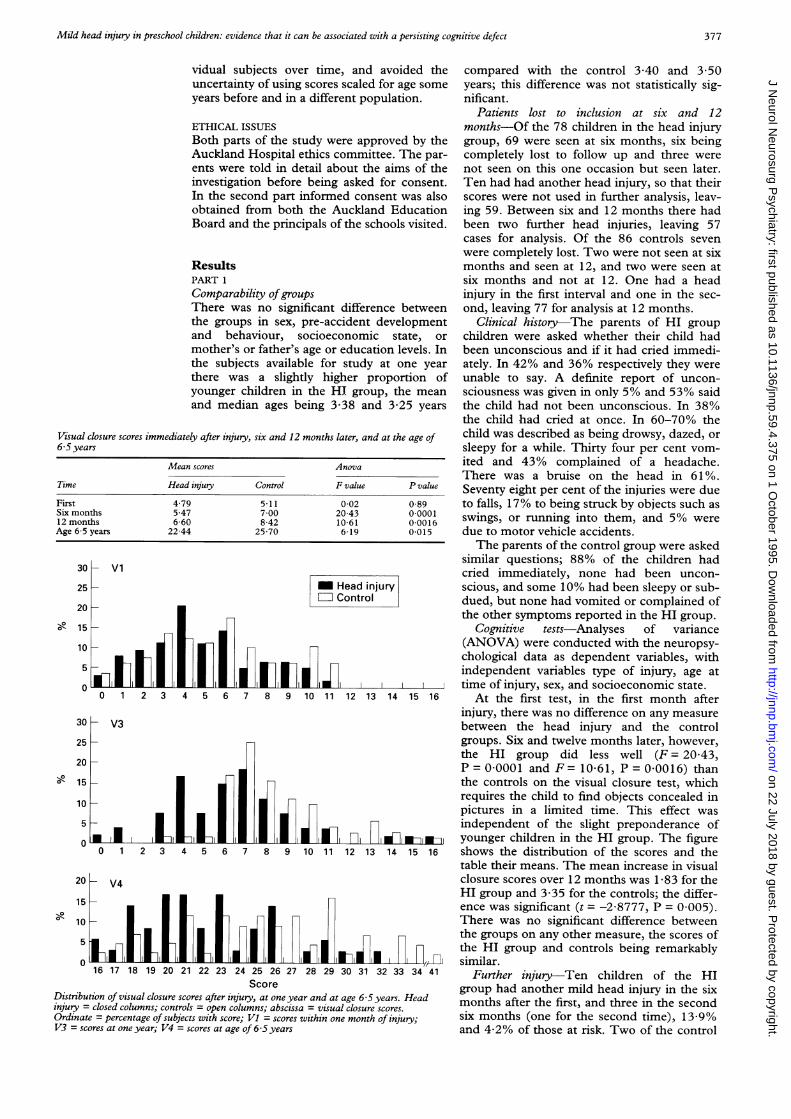
Visual closure scores immediately after injury, six and 12 months later, and at the age of6-5years
Mean scores Anova
Time Head injury Control F value P value
First 479 511 002 0-89Six months 5-47 7 00 20-43 0 000112 months 6-60 8-42 10-61 0-0016Age 6-5 years 22-44 25-70 6-19 0-015
30- Vl
25 m Head injuryControl
20-
X 15
10
5-
0
o 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
30 - V3
25-
20 -
15-
10
5-
01
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
20 -V
15
16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 41Score
Distribution of visual closure scores after injury, at one year and at age 6-5 years. Headinjury = closed columns; controls = open columns; abscissa = visual closure scores.Ordinate = percentage of subjects with score; Vl = scores within one month of injury;V3 = scores at one year; V4 = scores at age of 6-5 years
compared with the control 3 40 and 3 50years; this difference was not statistically sig-nificant.
Patients lost to inclusion at six and 12months-Of the 78 children in the head injurygroup, 69 were seen at six months, six beingcompletely lost to follow up and three werenot seen on this one occasion but seen later.Ten had had another head injury, so that theirscores were not used in further analysis, leav-ing 59. Between six and 12 months there hadbeen two further head injuries, leaving 57cases for analysis. Of the 86 controls sevenwere completely lost. Two were not seen at sixmonths and seen at 12, and two were seen atsix months and not at 12. One had a headinjury in the first interval and one in the sec-ond, leaving 77 for analysis at 12 months.
Clinical history-The parents of HI groupchildren were asked whether their child hadbeen unconscious and if it had cried immedi-ately. In 42% and 36% respectively they wereunable to say. A definite report of uncon-sciousness was given in only 5% and 53% saidthe child had not been unconscious. In 38%the child had cried at once. In 60-70% thechild was described as being drowsy, dazed, orsleepy for a while. Thirty four per cent vom-ited and 43% complained of a headache.There was a bruise on the head in 61 %.Seventy eight per cent of the injuries were dueto falls, 17% to being struck by objects such asswings, or running into them, and 5% weredue to motor vehicle accidents.The parents of the control group were asked
similar questions; 88% of the children hadcried immediately, none had been uncon-scious, and some 10% had been sleepy or sub-dued, but none had vomited or complained ofthe other symptoms reported in the HI group.
Cognitive tests-Analyses of variance(ANOVA) were conducted with the neuropsy-chological data as dependent variables, withindependent variables type of injury, age attime of injury, sex, and socioeconomic state.
At the first test, in the first month afterinjury, there was no difference on any measurebetween the head injury and the controlgroups. Six and twelve months later, however,the HI group did less well (F = 20-43,P = 0-0001 and F = 10-61, P = 0-0016) thanthe controls on the visual closure test, whichrequires the child to find objects concealed inpictures in a limited time. This effect wasindependent of the slight preponderance ofyounger children in the HI group. The figureshows the distribution of the scores and thetable their means. The mean increase in visualclosure scores over 12 months was 1-83 for theHI group and 3-35 for the controls; the differ-ence was significant (t = -2-8777, P = 0 005).There was no significant difference betweenthe groups on any other measure, the scores ofthe HI group and controls being remarkablysimilar.
Further injury-Ten children of the HIgroup had another mild head injury in the sixmonths after the first, and three in the secondsix months (one for the second time), 13-9%and 4-2% of those at risk. Two of the control
377
on 22 July 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.4.375 on 1 October 1995. D
ownloaded from

Wrightson, McGinn, Gronwall378
group also had a mild head injury, one in thefirst six months, and one in the second (1-3%).The difference in incidence between the HIand control groups in the first six months was
significant (P = 0-0023 (Fisher's exact test)).In both groups parents reported injuries otherthan those to the head, five in the HI group
and 18 in the control group. The number ofinjuries of all sorts was therefore similar in thetwo groups (25% and 25-3%).
Part 2Number of subjects At the age of 6-5 years
complete results were available for 49 childrenwithout a second injury in the first year; two ofthese had mild head injuries subsequently,leaving 47 for analysis. Of 56 controls withouthead injury in the first year four had a headinjury subsequently, leaving 52 for analysis.
Cases lost to follow up at 6 5 years-Themeans, medians, and ranges of visual closurescores at one year did not differ significantly inthe available HI, available control, and lostcontrol groups. The scores were significantlylower in the lost HI group (P = 0 005, mediantest).
Cognitive tests-Analyses of variance were
again conducted with the neuropsychologicaldata as dependent variables, with type ofinjury, time since the injury, sex, and socio-economic state as independent variables.
Again the only difference between the HIand control groups was in the visual closurescores (F = 6-19, P = 0-015), the controlsagain scoring higher (table and figure). Therewas no dependence on the time elapsed sinceinjury or on sex.
Tests of reading ability-For the HI group
there were significant (Pearson) correlationsbetween the visual closure scores at six months(r = 0 35, P < 0 05) and 12 months (r = 0 45,P < 0-01) after injury and the reading scores at
6-5 years, low visual closure scores being asso-
ciated with low reading scores. By contrast, inthe control children the visual closure scores
did not relate significantly to reading scores.
The relation to the visual closure score at 6 5years was not significant.
Reading recovery had been provided for 13of the 45 children in the HI group (29%) andeight of 58 children of the control group
(14%) (,2 = 3-56, P - 0 06). As the differ-ence is in the direction predicted by the originalhypothesis, a one tailed test can be appropri-ate, with P < 0 05.Behaviour-On the teacher's questionnaire
there was no overall difference between thescores of the HI and control groups (t = 1-31,P > 0 05). Scores were higher, however, forchildren who had had reading recovery (means7.39 and 3-32, t = 3.95, P < 0-01). This was
true for the HI and control groups separately,but the difference was greater in the HI group.
DiscussionThe major finding was that in preschool chil-dren who had had a mild head injury there wasa significant chance that their ability to inter-pret visual puzzles, expressed as their score on
the visual closure test, would be impaired. Theimpairment was not present immediately afterthe accident, but was evident six months later,and persisted to the age of 6-5 years. More ofthe HI group had difficulties with reading intheir first year of school and needed specialtuition, and within this group the reading abil-ity at 6-5 years was significantly related to thevisual closure score six and 12 months afterinjury.Some points in the methodology need com-
ment. Strict definition of the severity of theinjury presented problems. In most cases thechild was not being watched at the time of theaccident and often it was difficult for the parentto know whether the child had actually beenunconscious, or had cried at once. In the eventthey were only able to answer this question insome 60% of cases, and in only 5% of thesewere the parents certain that there had been adefinite loss of consciousness. This pattern ofmild head injury in younger children has beenwell documented, with a similar incidence ofclinical findings."5
In fact the range of severity was determinedby management decisions. Children wereincluded in the HI group if they had been suf-ficiently affected by the head injury for theirparents to take them to hospital and for a diag-nosis of head injury to be made, but not if theythen needed to be admitted. Children whohad skull fractures or who still had definitesymptoms after four hours of observation weretherefore excluded.
It would have been satisfying if a furthermeasure of the severity of the head injury hadbeen possible. In adults the duration of post-traumatic amnesia is conventionally used forthis purpose, and it is possible to make someestimate of post-traumatic amnesia in evensmall children.'6 We have, however, shown inadults that the estimates of post-traumaticamnesia of duration up to an hour are nothelpful in grading the severity of mild injury,both because they are unreliable and becausethey do not relate well to the incidence of cog-nitive and other problems later. 7 In the event itwas decided that to use this measure would bea fruitless complication.The children of the control group had
injuries which seemed to be very similar interms of the stresses of treatment needed inthe accident department and later. Thesocioeconomic and development factors wereclosely comparable, and the children of thetwo groups performed in the tests in a virtuallyidentical way except for the visual closurescores at the second and subsequent occa-sions, and for those of reading ability.Many observations and tests were made on
each child, and it could be held that by chanceat least one would show a difference betweenthe groups. It was, however, the originalhypothesis derived from the pilot study thatthe anomaly of visual perception and associ-ated reading problems would be found, andthe other investigations were accessory to this.The changes in visual closure were seen onthree occasions over periods of two to fouryears, the differences in scores of individual
on 22 July 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.4.375 on 1 October 1995. D
ownloaded from

Mild head injury in preschool children: evidence that it can be associated with a persisting cognitive defect
patients over time were consistent, and scoreson the reading test, an independent measure,were related to visual closure. Under these cir-cumstances it is reasonable to dismiss this sta-tistical objection.The investigator carrying out the tests knew
the history of the child and an expectancyeffect could have been introduced. The singleinvestigator was aware of the problem, but analternative was not possible with the resourcesavailable. The limitation has to be acknowl-edged.
Follow up was incomplete in both parts ofthe study. This was due to movement of fami-lies outside the area, and in only one case torefusal by the parents. The visual closurescores and the socioeconomic state of parentsof the lost and remaining cases were com-pared. There was no significant difference inpart 1. In part 2 the visual closure scores of thelost HI group children were lower than thoseof the remaining HI group; the scores of theremaining HI group children and of the lostand remaining controls were all similar.Retention of cases with a lower visual closurescore would be likely to increase the effectobserved, so that their loss does not diminishthe relevance of the major findings.Why was it that the visual closure and no
other scores were affected? Why at first did thevisual closure scores not differ from controlsbut later fail to increase normally with age sothat there was a persistent deficit?The Illinois test of psycholinguistic abilities
contains several visual tests, but only visualclosure was affected. The test presents a linedrawing and requires the child to search forone or two objects shown in the margin-forexample, a hammer and a saw. These arepartly concealed, showing perhaps only theserrated edge of the saw or the head of thehammer, and placed at different angles. Thechild therefore has to recognise the whole fromthe part and allow for rotation and differingviewpoints, and also to form a strategy to dothis within a limited time. Part of the processwould be expected to depend on what inadults would be minor hemispheric temporallobe function, but an important componentmay be the planning and execution, whichwould depend on function of the frontal lobes.Of the other tests that the children did, theone most comparable with visual closure waspart 2 of the Frostig developmental test ofvisual perception, but scores on this did notdiscriminate between the two groups, perhapsbecause there is no time limit on this task and itis made easier by allowing the child to outlinethe figures with coloured pencils.
There is good evidence that in children testsof the "performance" group such as visual clo-sure are more affected by head injury thanthose of the "verbal" group.'8-2' The reason forthis is not clear. Some performance tests aretime limited, so that low scores could be dueto the slowing of cognitive function that occursafter head injury in children as it does inadults.'8 This may be a factor in general, butdoes not apply in the present situation, asthere was no impairment of the visual closure
scores in the first test shortly after injury, whenslowing of function would be expected to be atits peak. Also no difference was found betweengroups in the visual sequential memory test,which is also time limited.No brain CT or MRI, were done on the
children in this study. Good evidence exists,however, that even in mild head injury MRIshows changes, usually in the temporal andfrontal regions and often in both, whichrelate to neuropsychological impairments.22Although in children of this age hemisphericdifferences are not well established, if lesionsof one temporal lobe were to be the cause ofdifficulty with visual closure, it would beexpected that in a group of cases lesions of theother lobe would occur and that some verbaldefects would also be found. This was not thecase. This could suggest that the frontal lobecomponent of the lesions was more likely to beresponsible for the changes seen. It certainlyseems likely that this is the cause of somefacets of cognitive impairment in rather moresevere head injuries in childhood.2'The selective effect on visual closure could
also occur because it depended on a functionwhich was developing particularly rapidly atthe time of the accident. Although the devel-opment of "verbal skills" probably precedesthat of the "performance skills", both are likelyto be in active growth in the 2-5 to 6 5 year agerange, and it is surprising that there should besufficient difference in growth rates to producea relative defect of this size.The finding that visual closure scores were
normal at the first test but then failed toincrease at the same rate as controls suggeststhat it was not an established visual skill thatwas damaged, but that further development ofthis skill was impaired, so that the affectedchildren were still not performing as well ascontrols two to four years later. This pattern ofincreasing defect is likely to be typical of thedeveloping brain, and is the reverse of thatseen in adult neurology when the maximumeffect is seen at once and diminishes with time.
Intuitively it was to be expected that defectsof visual interpretation would be associatedwith reduction of reading ability. In the HIgroup the visual closure scores one year afterthe injury were related to the reading scoreswhen the children were tested at 6-5 years ofage, and the HI group children needed specialhelp with their reading more often than con-trols. The relation of visual closure at 6-5 yearsto reading scores was not significant, suggest-ing that alternative stratagems for reading mayhave developed, perhaps as a result of the spe-cial tuition given to some of the subjects.
There was a relation between the need forspecial help with reading and general behav-iour in school as represented by the score onthe teacher's questionnaire. Although this wasstronger in the children with head injury, itaffected the controls as well. This could betaken to support the contention that childrenwho have accidents belong to a group whichcan be expected to behave badly,'-3 althoughthis is not supported by other authors.5 25Equally, it may indicate that children who fail
379 on 22 July 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.4.375 on 1 O
ctober 1995. Dow
nloaded from

Wrightson, McGinn, Gronwall
to achieve find difficulty in social adjustment.The incidence of further accidents was
much the same in both groups. In the first sixmonths, however, in the children in the HIgroup these resulted in further head injurysymptoms. After this they had accidents similarin frequency and resulting symptoms to thoseof the control group. This resembles our expe-rience with mild head injury in adults, whooften find that for a month or two after theinjury even a slight blow to their head resultsin a degree of headache and perhaps drowsi-ness that would not have been expected. Inchildren parenchymal lesions seen on MRIpersist, although reducing in size, for threemonths or more,22 and it is reasonable to pos-tulate that such lesions may make the brainmore sensitive to injury.
Despite the positive findings we presenthere there is little support in other studies ofinjured children for persisting cognitiveimpairment specific to mild head injury.Earlier work ascribed continuing problems topre-existing deficits, behavioural problems, orparental overreaction.' 35 In Gulbrandsen'sstudy of children aged 9-13 years,20 impair-ment of performance skills evident at four toeight months after mild injury was notdetectable at two years (personal communica-tion, quoted in Levin et a?4). Bijur and her col-leagues carried out a carefully controlled studyin which children aged 5 to 9 with mild headinjury were compared with children with otherinjuries and with uninjured children.4Children injured in any way tended moreoften to be aggressive and hyperactive thanuninjured children and to show lower acade-mic achievement, but the head injured differedlittle from those with other injuries. They con-cluded that head injury had no discernableeffect on general measures of intelligence,achievement, and aggression one to five yearsafter the injury. They did not, however, use atest comparable with the visual closure testand the children were older (only five of 114subjects were under 6 years old) and may havepassed the critical age for the development ofsome of the skills measured. They did, how-ever, find that the achievement in mathematicsat 10 years depended closely (P = 0 006) onthe age at which the head injury had occurred,scores varying from 93-5 for injuries at 5 yearsto 104-3 at 9 years of age. The authors did notthink that the impairment was a consequenceof injury, expecting that the more recentinjuries would have more pronounced residualeffects, the picture seen in adult neurology. Infact the finding would support the conceptthat the earlier years are important for devel-oping mathematical skills, and that in youngerchildren the development is more affected byinjury.
In conclusion it seems reasonable to saythat although in children a mild head injurymay not have a long term effect on cognitivefunction in general, there is good evidence thatif it occurs at an age which is critical for thedevelopment of a certain skill there may be a
persistinlg deficit. In this way injury in thepreschool years seems able to affect theprocess of learning to read.
As a practical measure, it should be possiblefor primary school teachers to pay particularattention to children known to have had ahead injury, so that help may be given as soonas possible. In more general terms., the possi-bility should be more widely recognised thatmild head injury in children of any age canhave subtle effects on school progress andbehaviour. Difficulties at school which becomeevident after a mild head injury are not neces-sarily or entirely due to pre-existing behav-ioural traits as has been suggested. Teachersought to be aware of this and resources fordiagnosis and remedial teaching should bemade available.We are much indebted to Dr Philip Voss for statistical advice.The investigation was funded by the New ZealandNeurological Foundation.
1 Rune V. Acute head injuries in children: a retrospectiveepidemiological, child psychiatric and electroencephalo-graphic study on primary school children in UmeA. ActaPaediatr Scand Suppl 1970, 209.
2 Craft AW, Shaw DW, Cartlidge NEF. Head injuries inchildren. BM3' 1972;4:200-3.
3 Rutter M, Chadwick 0, Shaffer D, Brown G. A prospectivestudy of children with head injuries: I. Design and meth-ods. Psychol Med 1980;10:633-45.
4 Bijur PE, Maslum M, Golding J. Cognitive and behav-ioural sequelae of mild head injury in children. Pediatrics1990;86:337-44.
5 Casey R, Ludwig S, McCormick MC. Morbidity followingminor head trauma in children. Pediatrics 1986;78:497-502.
6 Gronwall D, Wrightson P. Delayed recovery of intellectualfunction after minor head injury. Lancet 1974;2:605-9.
7 Wrightson P, Gronwall D. Time off work and symptomsafter minor head injury. Injury 198 1;12:445-54.
8 Elley WB, Irving JC. Revised socio-economic index forNew Zealand. NZ Journal of Educational Studies 1976;11:25-36.
9 Doll AE. The measurement of social competence. Minneapolis:Educational Publishers, 1953.
10 Connors C. Connors parent's questionnaire. Psycho-pharmacol Bull 1973;9(suppl) :231-4.
11 Reynell J. Developmental language scales. Windsor: NSERPublishing Co, 1969.
12 Kirk SA, McCarthy JJ, Kirk WD. The Illinois test of psy-cholinguistic abilities. Urbana: University of Illinois Press,1968.
13 Neale MD. Neale analysis of reading ability (2nd ed).London: Macmillan Education, 1966.
14 Frostig M. Marianne Frostig developmental test of visualperception. 3rd ed. Palo Alto: Consulting PsychologistsPress Inc, 1951.
15 Jamison DL, Kaye HH. Accidental head injury in child-hood. Arch Dis Child 1974;49:376-81.
16 Ruijs MBM, Keyder A, Gabreels FJM. Assessment of post-traumatic amnesia in young children. Dev Med ChildNeurol 1992;34:885-92.
17 Gronwall D, Wrightson P. Duration of post-traumaticamnesia after mild head injury. J7ournal of ClinicalNeuropsychology 1980;2:51-60.
18 Bawden HN, Knights RM, Winogron HW. Speeded per-formance following head injury in children. J Clin ExpNeuropsychol 1985;7:39-54.
19 Filley CM, Cranberg LD, Alexander MP, Hart EJ.Neurobehavioural outcome after closed head injury inchildhood and adolescence. Arch Neurol 1987;44:194-8.
20 Gulbrandsen GB. Neuropsychological sequelae of lighthead injuries in older children 6 months after trauma.Jrournal of Clinical Neuropsychology 1984;6:257-68.
21 Levin HS, Eisenberg HM, Wigg NR, Kobayashi K.Memory and intellectual ability after head injury in chil-dren and adolescents. Neurosurgery 1982;11:668-73.
22 Levin HS, Williams DH, Eisenberg HM, High WM Jr,Guinto FC Jr. Serial MRI and neurobehavioural findingsafter mild and moderate head injury. J Neurol NeurosurgPsychiatry 1992;33:255-62.
23 Levin HS, Culhane KA, Mendelsohn D, et al. Cognition inrelation to magnetic resonance imaging in head injuredchildren and adolescents. Arch Neurol 1-993;50:897-905.
24 Levin HS, Ewing-Cobbs L, Fletcher JM. Neurobehaviouraloutcome in mild head injury in children. In: Levin HS,Eisenberg HM, Benton AL, eds. Mild head injury.Oxford: Oxford University Press, 1989:189-213.
25 Partington MW. The importance of accident proneness inthe aetiology of head injuries in childhood. Arch Dis Child1960;35:215-23.
380
on 22 July 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.4.375 on 1 October 1995. D
ownloaded from