minimally invasive heart valve surgery technique … invasive heart valve surgery technique overview...
TRANSCRIPT
Innovating for life.
Minimally Invasive Heart Valve Surgery Technique OverviewTECHNIQUES FOR MINIMALLY INVASIVE MITRAL VALVE REPAIR/REPLACEMENTMichael Moront, MD
AcademiaMedical Education
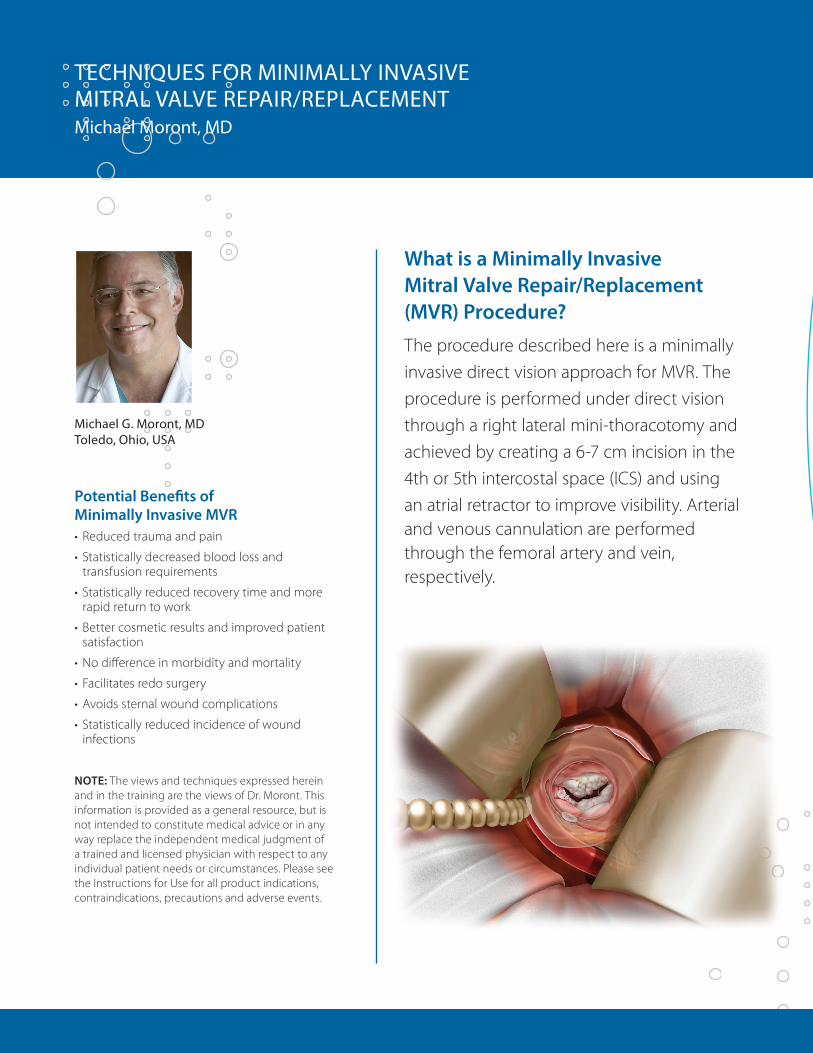
What is a Minimally Invasive Mitral Valve Repair/Replacement (MVR) Procedure?
The procedure described here is a minimally invasive direct vision approach for MVR. The procedure is performed under direct vision through a right lateral mini-thoracotomy and achieved by creating a 6-7 cm incision in the 4th or 5th intercostal space (ICS) and using an atrial retractor to improve visibility. Arterial and venous cannulation are performed through the femoral artery and vein, respectively.
Michael G. Moront, MD Toledo, Ohio, USA
Potential Benefits of Minimally Invasive MVR• Reducedtraumaandpain
• Statisticallydecreasedbloodlossand transfusion requirements
• Statisticallyreducedrecoverytimeandmorerapid return to work
• Bettercosmeticresultsandimprovedpatientsatisfaction
•Nodifferenceinmorbidityandmortality
• Facilitatesredosurgery
•Avoidssternalwoundcomplications
• Statisticallyreducedincidenceofwoundinfections
NOTE: The views and techniques expressed herein and in the training are the views of Dr. Moront. This information is provided as a general resource, but is not intended to constitute medical advice or in any way replace the independent medical judgment of a trained and licensed physician with respect to any individual patient needs or circumstances. Please see the Instructions for Use for all product indications, contraindications, precautions and adverse events.
TECHNIQUES FOR MINIMALLY INVASIVE MITRAL VALVE REPAIR/REPLACEMENTMichael Moront, MD
1. PATIENT SELECTIONExclusion criteria •Severelycalcifiedascendingaorta•Severelycalcifiedorobstructedfemoralarteries•Priorsurgeryorinflammatoryprocessinrightchest•Presenceofaninferiorvenacavalumbrella•Presenceofknownfemoralchronicdeepvenousthrombosis•Severepectusdeformityofthechest
Alternative approach:Redowithpriorcoronaryarterybypassgraftingcanbeperformedwithheartfibrillating.
2. ANESTHESIA TECHNIQUE•Doublelumenendobronchialtubeorbronchialblockerendotrachealtube•Swan-Ganz®pulmonaryarterycatheter•Transesophagealechocardiography(TEE)•MeasureleftatriumdimensionsforsizingofMitraX®retractor•Radialandfemoralarteriallines
3. PATIENT POSITIONING•Modifiedleftlateraldecubitusposition•Placerollbehindthetipofscapula,elevatingtherightchest•Positionrightarmata45°angleofftothesideofthebed•Infemalepatientstheincisionismarkedintherightinframammaryfoldbutthebreastismovedsuperiorlyfollowing
topical prep and secured in place by a second steri-drape (this moves the inframammary fold into the 4th and 5th ICS)•Prepanddrapeinusualfashion
4. CANNULATION•Performedpriortothoracotomy•LeftfemoralarteryandveincannulationareperformedutilizingaSeldingertechnique(onlylimitedexposureisrequiredto
identify the anterior aspect of the vessels) •Performarterialcannulationfirst,thecannulashouldneverbeforcedandshouldadvanceeasily•Insertfemoralvenousguidewarefromthefemoralveinintothesuperiorvenacava(SVC)utilizingtransesophagealechocardiography(TEE)guidance•VerifywirelocationinSVCpriortopassingcannula(veryimportant)•Ultimately,thefemoralvenouscannulatipshouldbeinthelowerrightatrium•AnadditionalvenouslineisaddedfortransthoracicSVCcannulation
If there is resistance while passing the cannula, immediately abandon and insert via a right percutaneous approach.LeftatrialsizesandmitralvalveannulardiameterisassessedpriortocardiopulmonarybypassandtheappropriatesizeMitraXintra-atrialretractorisselectedandprepared.

Incision
AcademiaMedical Education
5. INCISION AND EXPOSURE•Lateraltotheanterioraxillaryline,chestincision
in 4th or 5th ICS, 5-6 cm long
In female patients, the right inframammary line is entered
•Usesofttissueretractorandribretractortoobtainfurther exposure
•Makeachesttubeincisionandpassthrough the following:
1. Carbondioxideblower(infuseat2L/minthroughout the operation)
2. Cardiotomy suction
3. Diaphragmatic suture (placed and tied on the tendinous portion of the diaphragm)
4. Pericardial tacking suture on right lower aspect of the pericardium
•Openthepericardiumapproximately2-3cmabovethephrenicnerve
•Placeapericardiumretractionsutureonthelowermostportionofthepericardiumandexitthroughthechest tube incision (as previously described)
•Placeadditionalpericardialsuturesandtacktoskintohelpretractthehearttowardstheincision
6. SVC CANNULATION AND CARDIOPLEGIA•SVCiscannulateddirectlywitha18-22Frflexiblevenouscannulaforadditionalexposureandimproved
venous drainage
•InsertretrogradecardioplegiacannulaintothecoronarysinusutilizingTEEguidance
•Institutecardiopulmonarybypass
•Developaplanebetweentheinferioraspectoftheaortaandthesuperioraspectoftherightpulmonaryartery with electrocautery
•Acardioplegia-aorticventcannulaisplacedintheascendingaorta
•Crossclamptheascendingaortadirectlythroughtheincisionutilizingaflexiblecrossclampinthepreviouslydeveloped plane
•Antegradeandretrogradecardioplegiaareadministeredinastandardfashion
•Thepatient’sbodytemperatureiskeptat36°centigrade

7. ATRIOTOMY•Developtherightintra-atrialgroove
•Opentheleftatrium
•InsertMitraX®(self-adjustingretractor)andaccessmitralvalve
8. VALVE REPAIR OR REPLACEMENT•Inspectthemitralvalveleafletsandtestthevalvewithsalineinfusiontodeterminerepairorreplacement
•Placealloftheannularsuturestoaidinexposureandvisualizationofthevalvepriortoperformingyourvalverepairorreplacement technique of choice
•Utilizestandardrepairandreplacementtechniques
Refer to the “Instructions for Use” which accompany Medtronic heart valve repair and replacement products. Use only thosesizers/obturatorsdesignedfortheproductbeingimplanted.Productimplantguidesavailableuponrequest.
9. CLOSING•Closetheatriotomyusingrunningsutureline
•Placeasingleintramyocardialpacingwireintheanteriorrightventricularfreewallpriortoremovingtheaortic cross clamp
- Tunnel this pacing wire subcutaneously out the medial aspect of the thoractomy wound
- Place a grounding wire
•PlacepatientinsteepTrendelenburgpositionandinflatethelungs
•Removecrossclamp
•Placeade-airingneedleintherootoftheaortaandde-airtheheartintheusualfashionutilizingTEEguidance
- Shake patient or compress the chest if needed for de-airing (avoid direct manipulation of the heart)
•Placetwoatrialpacingwiresontherightatrium
•Weanpatientfromcardiopulmonarybypass
•Afterprotamineadministrationiscompleteremovefemoralvenousarterialcannula
•Placeonlyonechesttubeintherightpleuralspace,leavingpericardiumopenfordrainage
•GiveabolusoflocalanesthesiaintotheICS
10. END OF PROCEDURE•Twopericostalsuturesof#2Vicryl™areplacedtoclosethemini-thoracotomyincision
•AnOn-Q®painpumpsystemisinsertedintothesubpleuralspaceatthelateralaspectofthethoracotomyandasecond catheter is inserted into the neurovascular bundle of the upper rib of the thoracotomy
•Theendobronchialtubeisreplacedwithastandardendotrachealtube

Mosaic®Valve
CGFuture®Band
CGFuture®Ring Profile3D®
Annuloplasty System
Bio-Medicus®Multi-StageFemoralVenousCannula
*Theinstruments/disposableslistedareinadditiontoessentialinstrumentsnecessarytoperformsurgery.Over 35 years of scientific innovation, resulting in more options for minimally invasive heart valve repair and replacement.
HOW DO I BEGIN?Medtronicofferspeer-to-peereducationforthoseinterestedinlearninghowtodoanMVRprocedure.Please contact your CardioVascular sales representative for more information. Instruments and Disposables* as typically used by Dr. Moront
1. ProstheticValve–MedtronicMosaic®Bioprosthesis2. RepairProducts–CGFuture®COMPOSITERingorCGFuture®Band,
Profile3-DAnnuloplastyRing.3. Reusable Instruments a. Minimally Invasive Rib Retractor System b. MinimallyInvasiveAtrialRetractorSet,LargeBlades c. MinimallyInvasiveFlexibleAorticClamp d. Minimally Invasive Knot Pusher e. Minimally Invasive Scissors, Curved f. MinimallyInvasiveScissors,30° g. MinimallyInvasiveNeedleDrivers,CurvedLocking(Qty.x2) h. MinimallyInvasiveForcepsStraight,DoubleAction(Qty.x2) i. ForcepsNarrowStraight,DoubleAction j. MinimallyInvasiveHook(Qty.x2)
3. Reusable Instruments (continued) k. MinimallyInvasiveFlushPortAdapter l. Minimally Invasive Instrument Tray4. Disposable Supplies a. Alexis®SoftTissueRetractor,Medium b. MitraX®AtrialRetractor–SizesA,A+,B,B+ c. Minimally Invasive Aortic Clamp Inserts d. Cannulae: -MedtronicBio-Medicus®Multi-StageFemoralVenousCannulae,
21and25Fr. -MedtronicBio-MedicusFemoralArterialCannula17,19,and21Fr. -Gundry®SiliconeRCSPCannulawithManual-InflateCuff,15Fr. -DLP®MalleableSingleStageVenousCannula -DLP®AorticRootCannula,14ga. e. On-Q®painpumpsystem
Mosaic® Porcine Bioprosthesis Indications: Forthereplacementofmalfunctioningnativeorprostheticaorticand/ormitralheartvalves.Contraindications:Noneknown.Warnings/Precautions/Adverse Events:Accelerateddeteriorationduetocalcificdegenerationofbioprosthesismayoccurin:children,adolescents,youngadults,andpatients with altered calcium metabolism (e.g., chronic renal failure, hyperparathyroidism). Adverse events can include: angina, cardiac arrhythmia, cardiac dysrhythmias, death, endocarditis, heart failure, hemolysis, hemolytic anemia, hemorrhage, transvalvular or paravalvular leak, myocardial infarction, nonstructural dysfunction, stroke, structural deterioration, thromboembolism, or valve thrombosis.Foradditionalinformation,pleaserefertotheInstructionsForUseprovidedwiththeproduct.CAUTION: Federallaw(USA)restrictsthisdevicetosalebyorontheorderofaphysician.
CG Future® Annuloplasty System, Profile 3D® Annuloplasty System Indications:Thisdeviceisindicatedforthereconstructionand/orremodelingofpathologicalmitralvalves.Valvularinsufficiencyand/orstenosismaybecorrected by appropriate repair and annular remodeling. Contraindications:Heavilycalcifiedvalves,valvularretractionwithseverelyreducedmobility,activebacterial endocarditis. Warnings/Precautions/Adverse Events: Onlyphysicianswhohavereceivedpropertraininginvalverepairshouldusethisdevice.Adverse events can include: thromboembolic events, dehiscence, hemolysis, stenosis, residual incompetence, heart block, endocarditis, systolic anterior motion,leftventricularoutflowtractobstruction,anticoagulant-relatedbleedingorhemorrhage.ForadditionalinformationpleaserefertotheInstructionsfor Use provided with the product or contact your local Medtronic representative. CAUTION:Federallaw(USA)restrictsthisdevicetosalebyorontheorderofaphysician.ForadditionalinformationpleaserefertotheInstructionsForUseprovidedwiththeproductorcontactyourlocalMedtronicrepresentative.CAUTION:Federallaw(USA)restrictsthisdevicetosalebyoron the order of a physician.
Bio-Medicus® Femoral Arterial Cannula Indication:Thesedevicesaretobeusedbyatrainedphysicianonly.Cannulaeareusedtocannulatevessels,perfusevesselsororgansand/orconnectwithaccessoryextracorporealequipment.Thecannulaobturatorisintendedtofacilitateproperinsertionandplacementoftheappropriatesizedcannulawithin the vessel for cardiopulmonary bypass. Contraindication: Alone, the cannula and obturator are not medical treatment devices. There are no known contraindications for the use of the cannula other than those generally contraindicated for cardiopulmonary bypass. The cannula obtruator is to be used only withtheappropriatesizedBio-MedicusCannula.Thesedevicesarenotintendedforuseexceptasindicatedabove.
DLP® Malleable Single Stage Venous Cannula Indication: These cannulae are intended for collection of venous blood from the right side of the heart via the superior and inferior vena cava during cardiopulmonary bypass surgery up to six hours or less. Contraindication: This device is not intended for use except as indicated above.
Bio-Medicus® Multi-Stage Femoral Cannula and Introducer Product Description: FemoralCannulaandIntroducer(allcontentsareSTERILE/singleuseonly). Indications for Use: These devices are to be used by a trainedphysicianonly.Cannulaeareusedtocannulatevessels,perfusevesselsororgansand/orconnectwithaccessoryextracorporealequipment.TheCannulaObturatorisintendedtofacilitateproperinsertionandplacementoftheappropriatesizedcannulawithinthevesselforcardiopulmonarybypass.Contraindications: Alone, the cannula and obturator are not medical treatment devices. There are no known contraindications for the use of the cannula other thanthosegenerallycontraindicatedforcardiopulmonarybypass.ThecannulaobturatoristobeusedonlywiththeappropriatesizedBio-Medicus®Cannula.These devices are not intended for use except as indicated above.
DLP® Aortic Root Cannula Product Description: TheAorticRootCannulaconsistsofflexibletubingpermanentlyattachedtoboththeinletandtip.Theinletfittingisafemaleluerfitting.The introducer is packaged within the cannula body. Sterile, nonpyrogenic, single use. Indications for Use: This cannula is intended for short term use (six hours or less) in conjunction with cardiopulmonary bypass surgery for delivering cardioplegia solutions. The cannula may also be used to aspirate air from the aorta at the conclusion of the bypass procedure. Contraindications: This device is not intended for use except as indicated above.
DLP®/Gundry®Retrograde Coronary Sinus Perfusion Cannula with Manual-Inflate Cuff Product Description: Thecannulaconsistsofawirewoundsiliconecannulabodywithabeveledtip(6-Frmodelshaveanon-wirewoundcannulabody).Twosideholes are present near the tip. The back of the cannula body terminates in a locking female luer. A pressure monitoring line is an integral part of the cannula body, beginningatthetipandterminatinginalockingfemaleluerfittingor3-waystopcockwithalockingfemaleluerfitting.Aninflatableballoonislocatedatthedistalbeveledtip.Models94006,94010,and94015donothaveastylet.Theinflationassemblyislocatedatthebackofthecannulabodyandcontainsafemalesliplueranda one-way valve assembly. Sterile, nonpyrogenic, single use. Indications for Use: The cannula is intended for use during cardiopulmonary bypass surgery up to six hours or less for the delivery of cardioplegia retrogradely through the coronary sinus. Contraindications: This device is not intended for use except as indicated above.
Mosaic,CGFutureandBio-MedicusareregisteredtrademarksofMedtronic,Inc.MitraXsisaregisteredtrademarkofCardioLifeResearch.(St.JudeMedical)On-QisaregisteredtrademarkofI-Flow.Swan-GanzisaregisteredtrademarkofEdwardsLifesciences.AlexisisaregisteredtrademarkofAppliedMedical.VicrylisaregisteredtrademarkofEthicon.

World Headquarters Medtronic, Inc. 710 Medtronic Parkway Minneapolis, MN 55432-5604 USA Tel: (763) 514-4000 Fax: (763) 514-4879
Medtronic USA, Inc. Toll-free: 1 (800) 328-2518 (24-hour technical support for physicians and medical professionals)
LifeLine CardioVascular Technical Support Tel: (877) 526-7890 Tel: (763) 526-7890 Fax: (763) 526-7888 E-mail: [email protected]
www.medtronic.com
UC201205682EN©Medtronic,Inc.2013.AllRightsReserved.PrintedinUSA