minor ailments
TRANSCRIPT

Patient Self CareCondensed
Niamh MonePEBC NO: 100644
PEBC Qualifying Exam ISUMMER 2014
1

Contents
Insomnia 3Depression 5Smoking Cessation 7Headache 11Fever 15Heat Related Disorders 17Vertigo 19Tinnitus 21
2

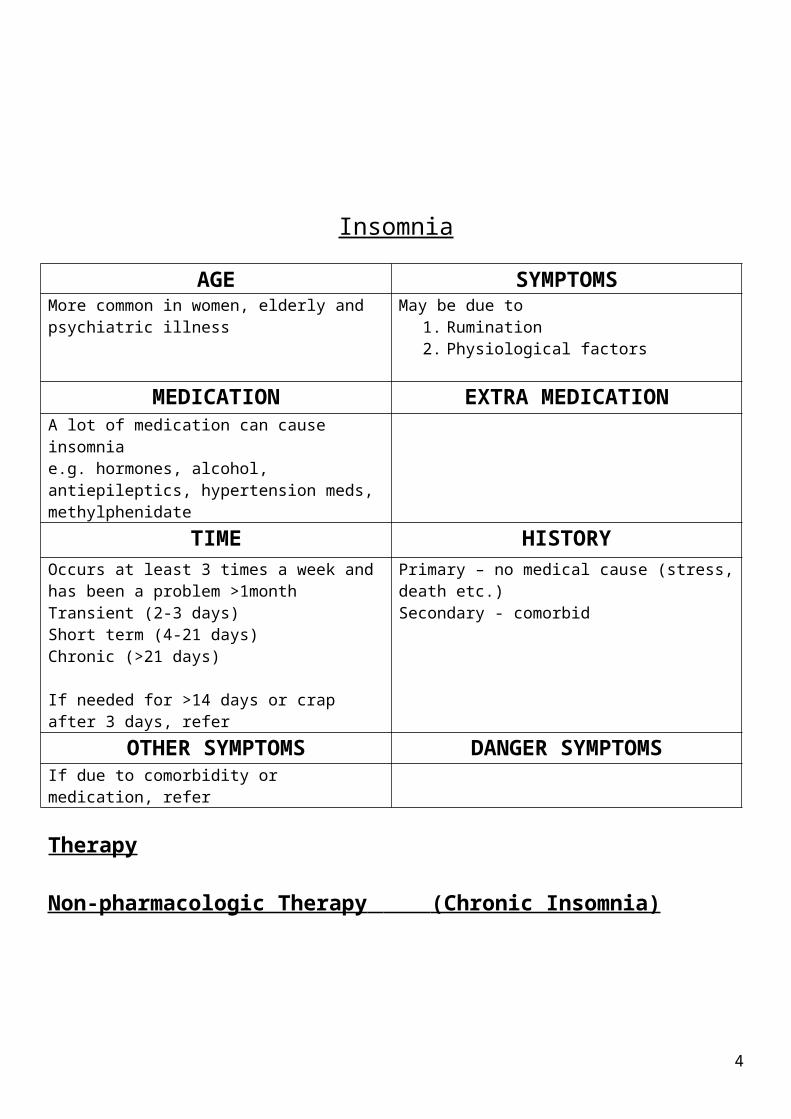
Insomnia
AGE SYMPTOMSMore common in women, elderly and psychiatric illness
May be due to1. Rumination2. Physiological factors
MEDICATION EXTRA MEDICATIONA lot of medication can cause insomniae.g. hormones, alcohol, antiepileptics, hypertension meds, methylphenidate
TIME HISTORYOccurs at least 3 times a week and has been a problem >1monthTransient (2-3 days)Short term (4-21 days)Chronic (>21 days)
If needed for >14 days or crap after 3 days, refer
Primary – no medical cause (stress, death etc.)Secondary - comorbid
OTHER SYMPTOMS DANGER SYMPTOMSIf due to comorbidity or medication, refer
Therapy
Non-pharmacologic Therapy (Chronic Insomnia)
Sleep hygiene
Personal habits
1. fix a bedtime and an awakening time
2. exercise regularly, but not right before bead
3. avoid nicotine before sleep and awakening
4. avoid caffeine, alcohol, sugar and spice 4-6 hours before bed
Sleeping Environment
1. comfortable bed2. temperature and
ventilation are good3. block all noise
Getting ready for bed
1. light snack such as warm milk or tryptophan
2. pre-sleep ritual3. relaxation techniques4. get into fav sleeping position5. don’t take worries to bed
stimulus control therapy, relaxation
training, CBT
sleep restriction therapy,
multicomponent therapy, biofeedback, paradoxical intention
Sleep hygiene (not as effective as
monotherapy)
3
Stimulus Control TherapyAssociate the bedroom with sleep1. go to bed only when tired2. use bedroom only for sleep3. get up at same time q am4. avoid napping5. if still not tired, read a
book in a different room for 15-20mins
Relaxation techniquesGood where hyper arousal the cause of insomnia1. progressive muscle
relaxation(muscles tightened and relaxed in certain order)2. biofeedbackincrease slow brain wave activity using EEG3. imagery trainingsubstitute pleasant thoughts with worrying ones
Paradoxical IntentionReduces performance anxiety by forcing patient to stay awake with eyes open in dark room
Sleep RestrictionControlling amount of time in bed but increasing time asleep
MulticomponentMay combine cognitive behavioral and sleep hygiene components
CBTAimed at creating at new attitude towards sleep
Pharmacologic therapy
Drug Dose Side Effects CIsValerian 400-900mg 30-60mins
before bedDizziness, nausea, headache, GI, high doses cause hangover.Hepatotoxicity and withdrawal reported.
Pregnancy
Melatonin Fatigue, headache, dizziness, irritability and abdominal cramps
Diphenhydramine
12,5-50mg 30-60mins before bedtime
Morning drowsiness, dizziness, grogginess, AC side effects
May lower seizure threshold, glaucoma, prostate, heart disease, AC problems
Doxylamine 25mg, 30 mins before bedtime
Tired in morning, hangover, AC May lower seizure threshold
On these meds….1. sleep hygiene2. avoid alcohol3. avoid operating machinery and driving4. keep a sleep diary
4

Depression
AGE SYMPTOMS1/3 suffer from bipolar – so see if they have had any manic episodes in the past
Major depressive disorder: >5 or more symptoms with at least one of first 2:
1. depressed mood2. markedly decreased interest/pleasure3. weight loss/gain4. insomnia/hypersomnia5. restlessness/lethargy6. fatigue7. worthlessness or guilt8. cant conc or make decisions9. suicidal thoughts, plans, actions
Dysthymia: 2y of depressed mood plus 2 or more of:1. increased/decreased appetite2. insomnia/hypersomnia3. low energy4. low self esteem5. poor conc6. hopelessness
MEDICATION EXTRA MEDICATIONBeta blockers, steroids, oral contraceptives
TIME HISTORYBidirectional with CV disease poorer outcomesMore likely with a first degree relative (1.5-3X)Reoccurrence1- 60% 2 – 70% 3 – 90%Edinburgh Postnatal Depression Scale for postpartum
OTHER SYMPTOMS DANGER SYMPTOMSPHQ-9: if yes to either, refer
1. over past month, have you been feeling down, depressed or hopeless
2. over past month, have you had little interest in doing things?
Non-Pharmacological Therapy
PsychotherapyGood for mild to moderate, but not for crazy or suicidal people.Counseling, CBT, IBT, self help books etc.
Exercise Light therapy10,000n lux light pointed at face for 30 mins. Difference seen in 1-3 weeks. Good for “SAD” may cause irritability, eye strain, headache, insomnia. Can start with 15 minutes and work up if bad side effects.
Electroconvulsive therapyReserved for more severe. Induced seizures in anaesthetized patient.
rTMSSofter than ECT, non invasive.
5

OTC medications
Drug Dose Side effects CIsSt johns wort 300mg TID Photosensitivity, GI, dizziness,
insomnia, restlessness, agitation, mania and hypomania
Inducer; Reduce effectiveness of drugs, can cause serotonin syndrome with SSRIsPregnancy, breastfeeding
SAMe 400-1600mg dy in divided doses
Insomnia, AC effects Serotonin syndrome, pregnancy and lactation
Omega 3 1-2g day Fishy aftertaste, nausea Additive bleeding risk with anticoagulants,Pregnancy and lactation
Prescription Meds
Symptom improvement in 2-4 weeks. If no improvement after 6-8 weeks, see doctor.Overall good outcome in 2 months.Patient should stay on meds for 6-9 months after remission if first episode. Longer than 1 year is not unreasonable.
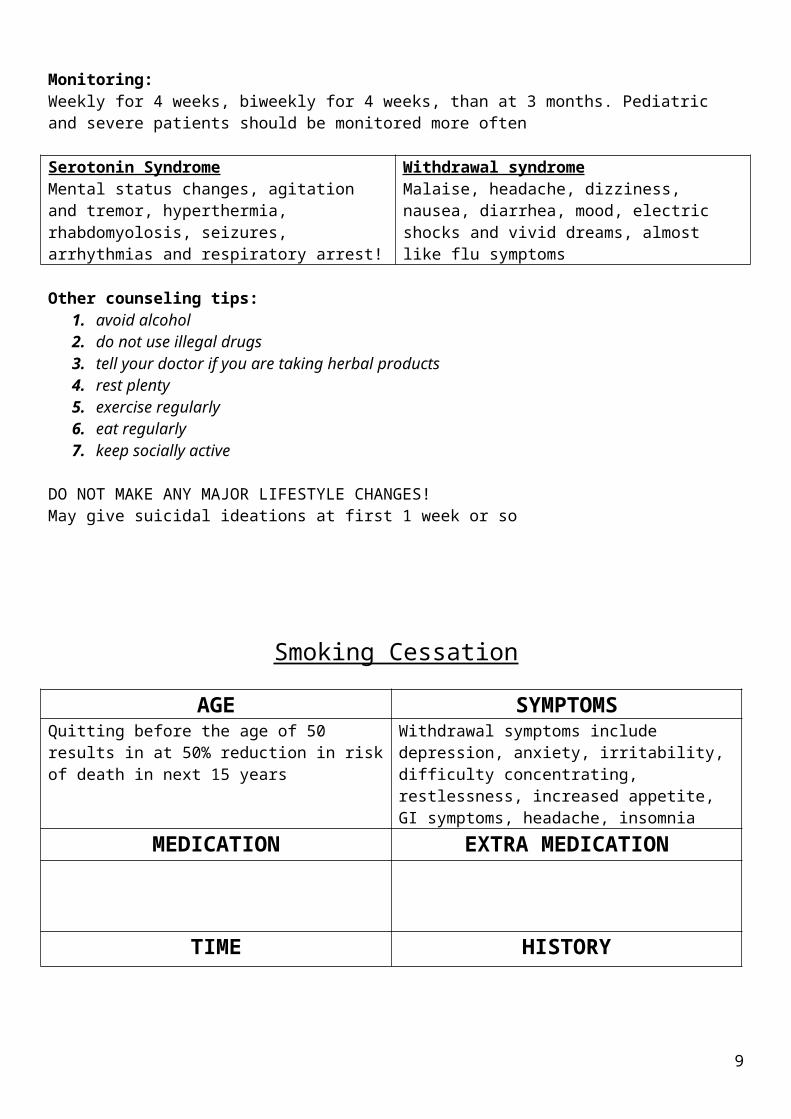
Monitoring:Weekly for 4 weeks, biweekly for 4 weeks, than at 3 months. Pediatric and severe patients should be monitored more often
Serotonin SyndromeMental status changes, agitation and tremor, hyperthermia, rhabdomyolosis, seizures, arrhythmias and respiratory arrest!
Withdrawal syndromeMalaise, headache, dizziness, nausea, diarrhea, mood, electric shocks and vivid dreams, almost like flu symptoms
Other counseling tips:1. avoid alcohol2. do not use illegal drugs3. tell your doctor if you are taking herbal products4. rest plenty5. exercise regularly6. eat regularly7. keep socially active
DO NOT MAKE ANY MAJOR LIFESTYLE CHANGES!May give suicidal ideations at first 1 week or so
bupropion, mirtazepine, moclobemide, SNRIs,
SSRIs
quetiapine, trazodone, tcas maois
6

Smoking Cessation
AGE SYMPTOMSQuitting before the age of 50 results in at 50% reduction in risk of death in next 15 years
Withdrawal symptoms include depression, anxiety, irritability, difficulty concentrating, restlessness, increased appetite, GI symptoms, headache, insomnia
MEDICATION EXTRA MEDICATION
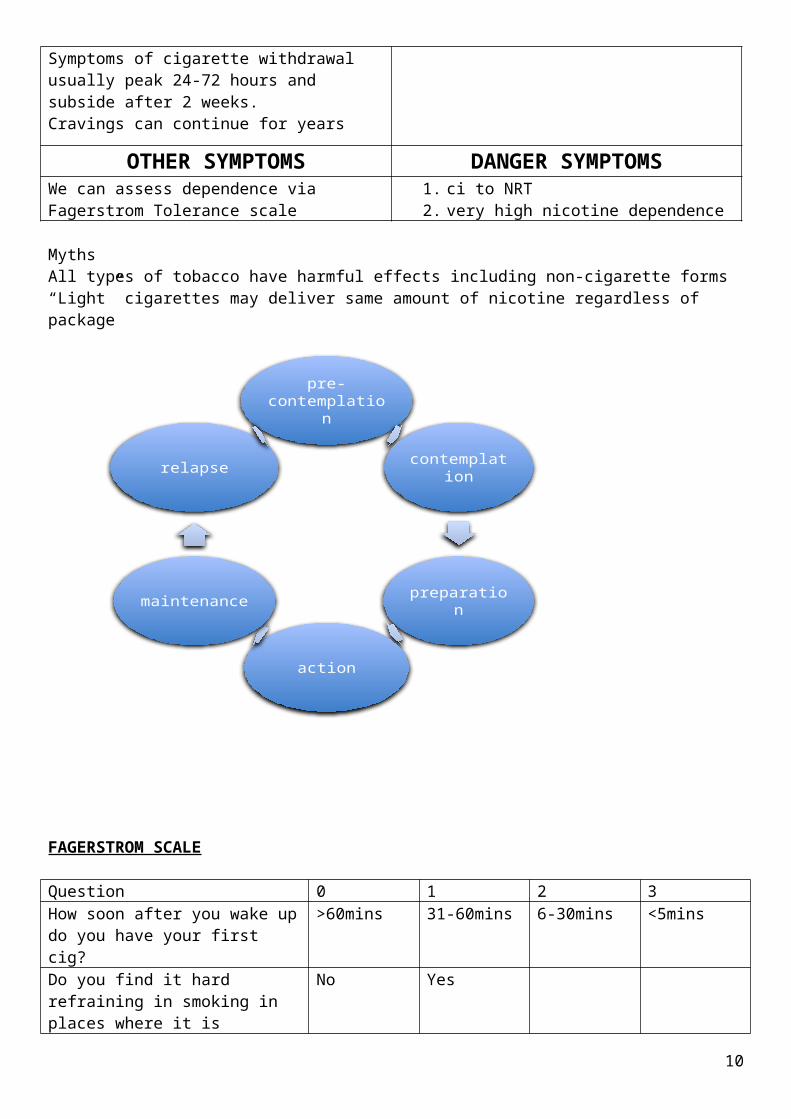
TIME HISTORYSymptoms of cigarette withdrawal usually peak 24-72 hours and subside after 2 weeks.Cravings can continue for years
OTHER SYMPTOMS DANGER SYMPTOMSWe can assess dependence via Fagerstrom Tolerance scale
1. ci to NRT2. very high nicotine dependence
MythsAll types of tobacco have harmful effects including non-cigarette forms“Light” cigarettes may deliver same amount of nicotine regardless of package
pre- contemplation
contemplation
preparation
action
maintenance
relapse
7

FAGERSTROM SCALE
Question 0 1 2 3How soon after you wake up do you have your first cig?
>60mins 31-60mins 6-30mins <5mins
Do you find it hard refraining in smoking in places where it is forbidden?
No Yes
Which cig would be the hardest to give up?
Any other than first in the morning
First in the morning
How many cigarettes do you smoke? <10 11-20 21-30 >31Do you smoke more in the morning than rest of day?
No Yes
Do you smoke even when ill? No Yes
<5 = low5 = moderate>6= high – REFER
Non-pharmacologic therapy
Refer everyone to behavioral modification programs. Light smokers may be able to do this alone.e.g. smokershelpline.ca, cancer.ca, camh.net “on the road to quitting” is a 40 page self help guide
AcupunctureNeedles in nose and ear, no evidence
Laser therapySimilar to acupuncture. No evidence.
HypnotherapyNo evidence
Aversion TherapyAssociation with an unpleasant sensation with smoking. E.g., electric shocks. Rapid smoking has shown most promise but not recommended due to heart and lung problems!
Clove and herbal cigarettesMay contain up to 70% tobacco. Also tar, CO and other toxins.
Pharmacological therapy
In order of best to worst:1. Champix2. Nicotine patch plus PRN3. bupropion and patch4. inhaler5. bupropion6. patch7. lozenge8. gum
8
Drug Dose Side effects Contraindications CommentsGum Nicorette
2mg if <64mg if >7
Thrive2mg if <254mg if >25
10-12 pieces per day, up to 20. May decrease by 1 gum per day each week over 3 months, up to 6 months max
Jaw throat and mouth soreness
1. depression, insomnia, dizziness, headache
2. Taste disturbances, nausea and vom
3. hypertension4. rash5. cough
6. life threatening arrhythmia
7. severe angina8. history of recent
stroke9. 2ks following MI
relative ci:1. pregnancy2. smoking while
using3. <18 yrs
Do not chew like normal gum!!
Bite one piece in the mouth, and park between teeth and gums for 1 mins, repeat when desire arise again, up to once a min for 30 mins then discard piece.
Avoid acidic beverages and foods while chewing and 15 mins before.
Lozenges Thrive1mg if <20 (max 25 per day)2mg >20 (max 15 per day)Nicorette2mg if >30mins4mg if <30mins
weeks 1-6: q1-2hweeks 7-9: q2-4hweeks 10-12: 4-8
discontinue when loz are 1-2 times per day, do not use for >6months
Same as above Same as above DO NOT SWALLOW OR CHEW! Suck only. Move from one side of mouth to other periodically
Same as above w/ acidic foods and drinks
Inhaler Initial: use 6-12 per day for 3-6 weeks and taper over next 6-12 weeksD/C if use is down to 1-2 times per day. Not >6months
Transient and decrease with use. Irritation, cough, headache, nausea
same as above Puff like cig (5-10 mins at a time)
Cartridges can be used for 24h once punctured
Patch Apply to non-hairy, clean, dry site in upper arm or hip. Don’t use the same site >1 per week
6wks>2wks>2wks
Same as above and rash
generalized skin problems – severe eczema or psoriasis
If patient still smoking in first 2 weeks, referCheck monograph with strenuous exerciseDo not cut patches
9
21-40 cigs per day can use 35mg nicotine>40 cigs per days can use 40mg nicotine
with insomnia, remove patch at night and use immediate release product first thing in the morning.
Prescription Therapy
Drug Side effects CIBupropion Dry mouth, insomnia
Hypertension, muscle/joint pain, dizziness, tremor, sleepy, rash, taste
Can cause agitation – caution in psychiatric patients
SeizuresAnorexia/bulimiaConcurrent MAOI therapy
Can be used in combination and pregnancy
Varenicline Nausea, vomiting, headache, insomnia, abnormal dreams and dizziness
Psychological assessment important
Pregnancy
Do not use in combo as increased side effects and no increased efficacy
Clonidine can also be used but is generally not due to side effects
Special Considerations
1. PregnancyUse non-pharmacologic methods where possible. If moderate to heavy smoker, use NRT. Start within first 16 weeks. Use IR products, and if not, use 16-hour patch. Should involve patient’s physician.
2. LactationUse IR products. Breastfeed before using the product to minimize exposure.
3. CV diseaseSafe with stable CV disease. Transdermal patch preferable as it is consistent.
4. ChildrenCounseling best. No evidence that NRT works best, should be done under physicians care.
5. Smokeless tobaccono conversion for NRT products. Counseling best or refer.
DRUG INTERACTIONSEnzyme inducer – so increases clearance of drugs in smokers.
FluvoxamineRasagilineOlanzapineWarfarinNifedipineEstrogensDiazepamTheophyllineTrifluoperazineMethadoneClozapineCaffeine
Reduce caffeine intake to reduce side effects
10

Headache
AGE SYMPTOMSTemporal arteritis >50 years, fatal
Refer if onset >40 years
Tension – mild- moderate tight band in both sides of the head. May have photo/phonophobia (1 or the other)Migraine – moderate/severe pulsating headache, usually on one side of the head. May have aura with photo/phonophobia with nausea or vomiting.Cluster – excruciating penetrating, usually unilateral at temple/above eyebrow. May have, at same side of headache, NO VOMITING
1. lacrimation2. red eyes3. nasal congestion or running4. constriction of pupil “miosis”5. dropping of eyelid “ptosis”6. facial sweating7. eyelid edema8. some photophobia (mild)
MEDICATION EXTRA MEDICATIONIntracranial hypertensionAntibioticsCorticosteroidsCimetidine, isotrenitoin, tamoxifenHeadacheHypertensivesH2 antagonistsNitratesNSAIDSHRT, Oral contraceptivesSSRIS
TIME HISTORYTension – can last 30 mins to 7 daysMigraine – 4-72hCluster – 15-180mins
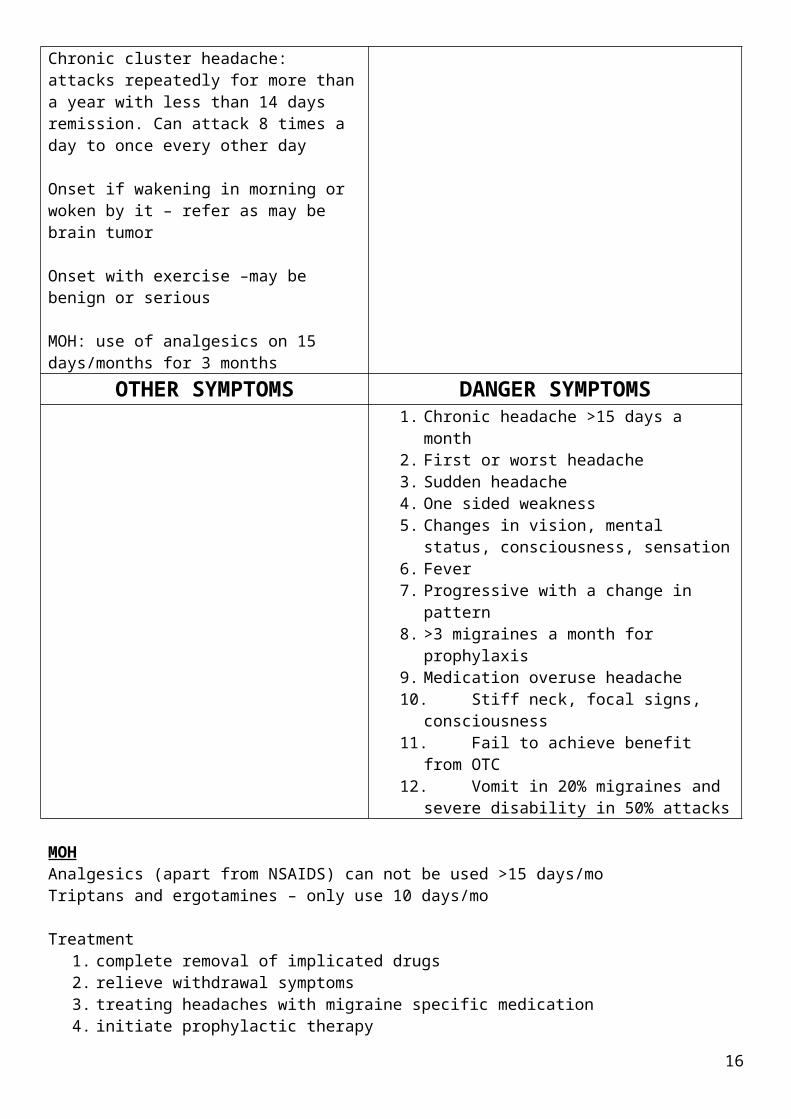
Chronic - >15 days a monthChronic cluster headache: attacks repeatedly for more than a year with less than 14 days remission. Can attack 8 times a day to once every other day
Onset if wakening in morning or woken by it – refer as may be brain tumor
Onset with exercise –may be benign or serious
MOH: use of analgesics on 15 days/months for 3 months
Pregnant?Any medical conditions? E.g. diabetes, epilepsyHave you had this before?
11

OTHER SYMPTOMS DANGER SYMPTOMS1. Chronic headache >15 days a month2. First or worst headache3. Sudden headache4. One sided weakness5. Changes in vision, mental status,
consciousness, sensation6. Fever7. Progressive with a change in pattern8. >3 migraines a month for prophylaxis9. Medication overuse headache10. Stiff neck, focal signs, consciousness11. Fail to achieve benefit from OTC12. Vomit in 20% migraines and severe disability
in 50% attacks
MOHAnalgesics (apart from NSAIDS) can not be used >15 days/moTriptans and ergotamines – only use 10 days/mo
Treatment1. complete removal of implicated drugs2. relieve withdrawal symptoms3. treating headaches with migraine specific medication4. initiate prophylactic therapy
Triggers
Foods that contain nitrites MSG Aspartame or
neurotransmitter precursorsE.g. cheeses, cured meats, chocolate, alcohol, caffeineALSO MISSED/DELAYED MEALS
Environmental Weather Loud noises Flickering lights Strong odors Cig smoke Travel across time zones
Chemical Benzene Insecticides perfumes
Hormonale.g. periods, menopause
Stress, anxiety, sex, sleep cycle
TREATMENT OF HEADACHE
Drug Dose Side effects Interactions Pregnancy CommentsAcetaminophen
1000mg Q4H prn x2 doses (no more than 4g daily)Child: 10-15 mg/kg q4h prn
Liver or kidney dysfunction
Warfarin – increased bleeding (1.3g dy for >1 week more likely)
First choice Less effective than NSAIDs
ASA Same as aboveChild (>12 y) 500-650mg single dose
GI upset, ulceration or bleed
Warfarin Safe in first and second trimesters, NOT 3RD! – hypertension
Do not use in viral or fever in children. Avoid EC as this prolongs
12

of newborn, prolonged preg and labor
onset. Effervescent 100mg ASA similar to sumatriptan 50mg for migraine.
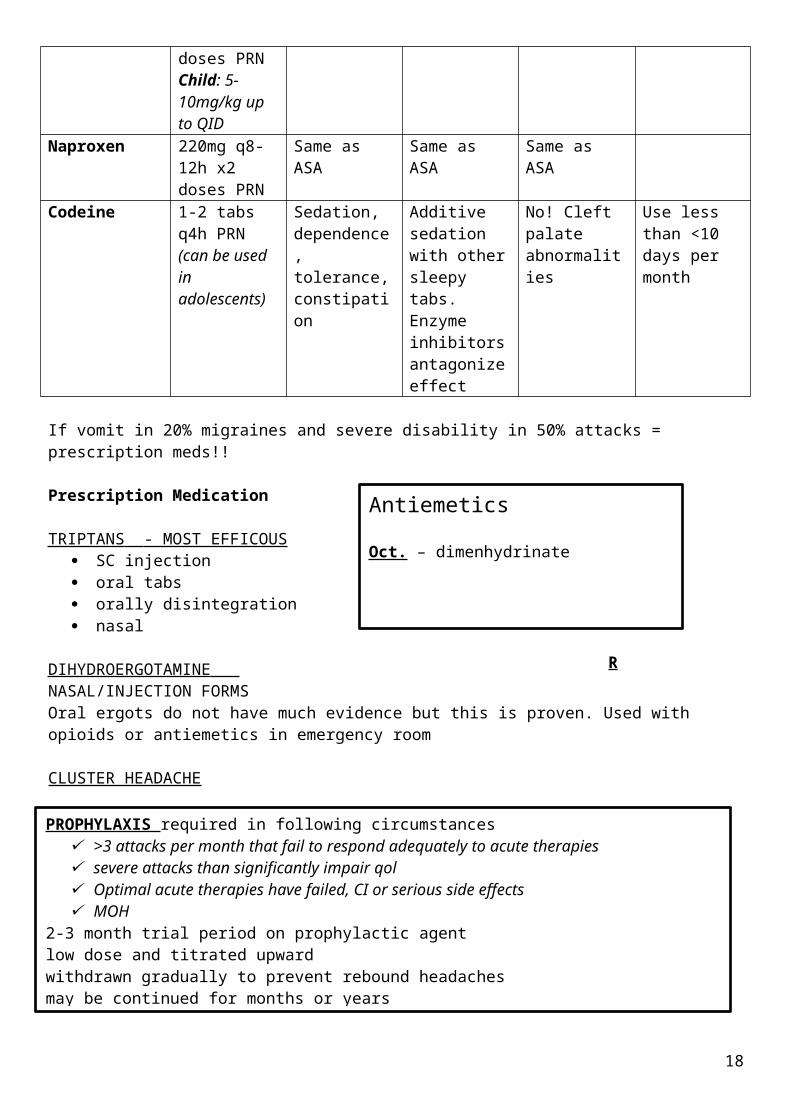
Ibuprofen 200-400mg Q6H x2 doses PRNChild: 5-10mg/kg up to QID
Same as ASA Same as ASA Same as ASA Pain free at 2h
Naproxen 220mg q8-12h x2 doses PRN
Same as ASA Same as ASA Same as ASA
Codeine 1-2 tabs q4h PRN (can be used in adolescents)
Sedation, dependence, tolerance, constipation
Additive sedation with other sleepy tabs.Enzyme inhibitors antagonize effect
No! Cleft palate abnormalities
Use less than <10 days per month
If vomit in 20% migraines and severe disability in 50% attacks = prescription meds!!
Prescription Medication
TRIPTANS - MOST EFFICOUS SC injection oral tabs orally disintegration nasal
DIHYDROERGOTAMINE NASAL/INJECTION FORMSOral ergots do not have much evidence but this is proven. Used with opioids or antiemetics in emergency room
CLUSTER HEADACHERequires O2 and rapid onset triptans e.g. nasal, subcutaneous triptans or DHE
Antiemetics
Oct. – dimenhydrinate
RX- domperidone, metoclopramide and prochlorperazine
PROPHYLAXIS required in following circumstances >3 attacks per month that fail to respond adequately to acute therapies severe attacks than significantly impair qol Optimal acute therapies have failed, CI or serious side effects MOH
2-3 month trial period on prophylactic agentlow dose and titrated upwardwithdrawn gradually to prevent rebound headachesmay be continued for months or years
13

Drug Dose Side effects
Interactions Pregnancy Comments
Feverfew 125mg per day
Mouth ulcers
Anticoagulants Avoid – uterine contractions
Avoid if contact dermatitis from plants in Asteraceae family
butterbur 75mg BID GI – burping
None ? Good evidence. Do not use unless commercially prepared as a carcinogenic
Coenzyme q10
100mg tid GI <1% Additive blood pressure lowering effects, may reduce AC effects of warfarin, may lower efficacy of chemo
? May take up to 3 months for benefit
Magnesium 300mg BID Diarrhea, GI
Separate doses by 2h for doxy ETC
Safe Conflicting evidence
Riboflavin 400mg/day
Yellow urine
None High doses teratogenic
Small trial in adults show efficacy
Prescription
Migraine
Bblockers w/o intrinsic sympathomimetic activity e.g. propranolol, metoprololTCAsCCBsSerotonin receptor antagonists e.g. pizotifenValproic acid/divalproexTopiramateNSAIDS
Cluster
Verapamil/Lithium/Valproic acid at onset&Steroids (e.g. prednisolone 60-80mg/day for 2-3 days, then reduce)ORErgotamines (not within 24 hours of triptan)
A 50% reduction in migraines is considered good! Keep a diary and record migraines
14

Fever
AGE SYMPTOMSFever in children is rectal temperature >38Adults – circadian highest between 4-6pm, lowest at 6am.>37.2 morning>37.8 any time define feverHigh fever >40.5
Refer<6moRefer >40.5 everyone elseRefer – distressed child
MEDICATION EXTRA MEDICATIONNew drug that causes hypersensitivity?
TIME HISTORYFEVER LONGER THAN 3 DAYS – refer24h with no cause - refer
Travelled abroad?Surgery?Raw food?
OTHER SYMPTOMS DANGER SYMPTOMS1. Stiff neck, seizures, localized pain,
redness, swelling or heat2. Wheezing and cough3. Rash
Temperatures
Rectal 0.6 higher than…OralArmpit 0.5-1 lower than…
Mercury thermometers no longer recommended as they may break, up to 10 minutes for glass thermometers. Digital only need 10 seconds.
Rectal is most accurate, good for <4-5 years oldOral >5yrs. Do not bite thermometer. No hot food or bev 10 mins before.Auxiliary less reliable. Confirm via another route if >37.2
Non-pharmacological Therapy Removal of excess clothing and bedding Increased fluid intake Avoid physical exertion Ambient temps around 20-21 degrees
Sponging – no additional benefit. But take antipyretics 30 mins before. ONLY DO WITH WATER!
15
Pharmacological TherapyReduce hypothalamic set point.Use at regular intervals to avoid shivering
Ibuprofen – avoid in diarrhea and vomiting
Combination of paracetamol and ibuprofen NOT GOOD – one or the other
16

Heat Related Disorders
AGE SYMPTOMSYounger patients – exertional heat strokeOlder patients – classical heat stroke
Infants and elderly at risk
Heatstroke – body temp >40 and changes in mental status. Two types
1. Classical – poor environment. Hot dry skin and less pronounced increase in core body temp. occurs over several days
2. Exertional – physical activity. Occurs over few hours
MEDICATION EXTRA MEDICATION1. Blockage of sweat production
alcohol, anticholinergics, antihistamines, hypertension drugs
2. Vasoconstrictionalpha agonists, MAOIs, sympathomimetics
3. Disrupted hypothalamusantipsychotics, amphetamines
4. Increase in heat productionexcessive thyroid, sympathomimetics
Also any meds that alter a person’s perception to stay hydrated
TIME HISTORYFew hours – exertionalFew days – classical
If recovery does not occur within 20-30mins refer
Outdoor laborers and athletes at riskDehydration
OTHER SYMPTOMS DANGER SYMPTOMS1. Loss of consciousness2. Confusion/hallucinations3. Convulsions4. Altered mental status5. Sob6. Vomiting7. Little or no urine8. Skin that is hot and dry with no sweat9. If recovery does not occur within 20-
30mins10.Heat stroke
The hypothalamus regulates heat. Body eliminates heat by four different mechanisms:1. EVAPORATION e.g. sweating2. RADIATION – electromagnetic waves. 65%3. CONDUCTION – physical contact with a cooler object. Least effective4. CONVECTION – transfer to air. E.g. vasodilation
Reduction in these can increase risk of heat related illness. CV system can collapse with multiple organ failure.
17
Prevention Methods
1. Move at risk individuals to air conditioned location to partake in social activities (FIRST LINE) 2. Be hydrated before activity and during (500ml to IL per hour of activity)3. 10 to 20 mins break from sun per hour4. Avoid strenuous activity from 10am-3pm5. Wear light coloured, light weight clothing including wide brimmed hat6. Acclimatize. 10-14 days!
Heat Rash Heat edema Heat Cramps Heat Syncope Heat Exhaustion
Heat Stroke
Prickly heat due to increased sweatingBreasts (under)Elbow creasesGroinUpper ChestNeck
Vasodilation of blood vessels, sodium and water retentions and prolonged standing
Water and sodium depletion.Stomach, arms and legs.Common in athletes – warning sign of heat exhaustion.
Dizziness and fainting
Weakness , n&v, hypotension, fatigue, dizziness, headache, increased body temp
Similar to heat exhaustion but with altered mental status
Go to cooler area and keep dry
Elevate feet or handsPrevent with acclimatization
Stop activity! And rest for a few hours- see physician if not better in 1 hourORSStretch and massage
Stop and rest – get up slowly
AcclimatizationCan lead to heat stroke if untreated.
Stop and rest.ORS.recovery in 2-3 hif no improvement in 20-30 mins - refer
Call 911Stop and rest.ORSRemove excessive clothingIce packs
Pharmacologic Therapy
Acetaminophen won’t workBenzos and barbiturates for seizuresMannitol promotes osmotic diuresis and prevents or treats renal failure
18

Vertigo
AGE SYMPTOMSDizziness – light headednessVertigo – sense of movement when there is none
Can include nausea, vomiting, pallor and sweating
MEDICATION EXTRA MEDICATIONOtotoxic drugs
TIME HISTORYCan be acute, chronic and recurrent CV
Endocrine – anemia, diabetesMigraine, head injury
OTHER SYMPTOMS DANGER SYMPTOMSRefer everyoneNumbness, tingling, weakness, visual disturbances, difficulty speaking – 911!
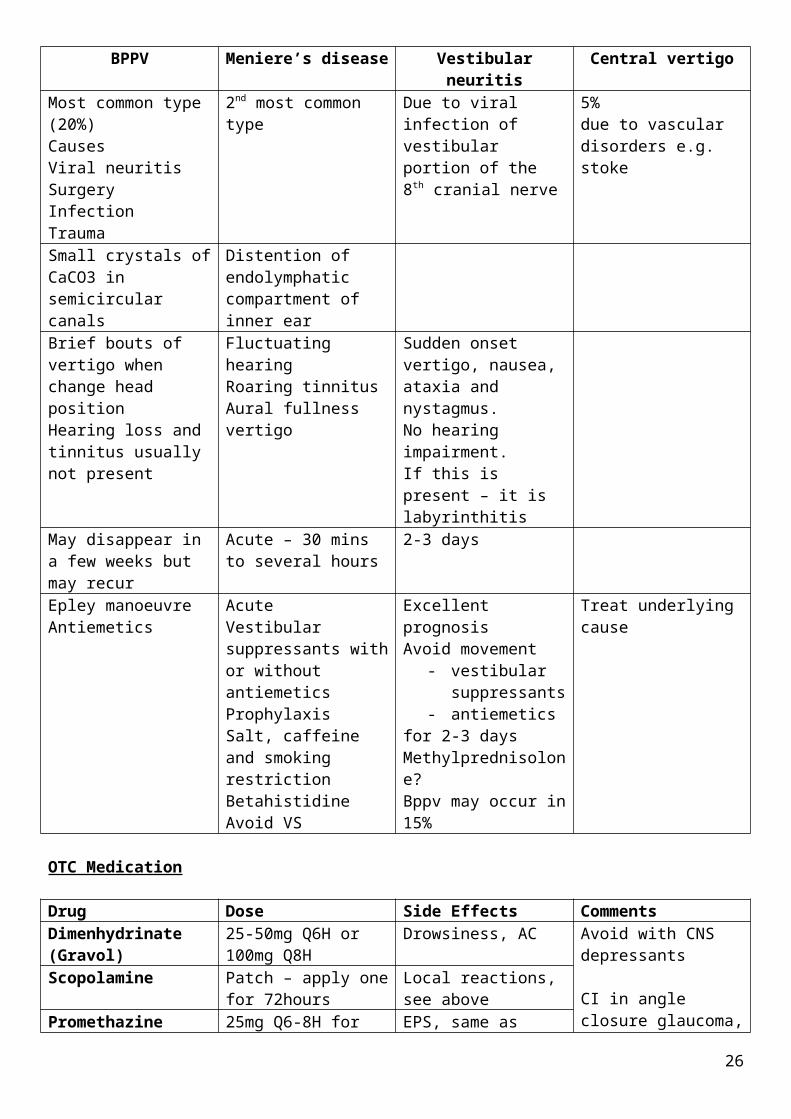
BPPV Meniere’s disease Vestibular neuritis Central vertigoMost common type (20%)CausesViral neuritisSurgeryInfectionTrauma
2nd most common type Due to viral infection of vestibular portion of the 8th cranial nerve
5%due to vascular disorders e.g. stoke
Small crystals of CaCO3 in semicircular canals
Distention of endolymphatic compartment of inner ear
Brief bouts of vertigo when change head positionHearing loss and tinnitus usually not present
Fluctuating hearingRoaring tinnitusAural fullnessvertigo
Sudden onset vertigo, nausea, ataxia and nystagmus.No hearing impairment.If this is present – it is labyrinthitis
May disappear in a few weeks but may recur
Acute – 30 mins to several hours
2-3 days
Epley manoeuvreAntiemetics
AcuteVestibular suppressants with or without antiemeticsProphylaxisSalt, caffeine and smoking restrictionBetahistidineAvoid VS
Excellent prognosisAvoid movement
- vestibular suppressants
- antiemeticsfor 2-3 daysMethylprednisolone?Bppv may occur in 15%
Treat underlying cause
19

OTC Medication
Drug Dose Side Effects CommentsDimenhydrinate (Gravol)
25-50mg Q6H or 100mg Q8H
Drowsiness, AC Avoid with CNS depressants
CI in angle closure glaucoma, prostatic hypertrophy and urinary retention
Scopolamine Patch – apply one for 72hours
Local reactions, see above
Promethazine 25mg Q6-8H for nausea only
EPS, same as above
Prescription therapy
Benzodiazepines, betahistine, flunarizine. Only treat for a week or less
Other points:Avoid drivingAvoid alcohol with therapy
20

Tinnitus
AGE SYMPTOMSLess common in children and more in the elderly Objective – vascular, mechanical or spontaneous
Subjective – otologic, neurologic, infectious, drug
MEDICATION EXTRA MEDICATIONLoop diuretics, salicylates, aminoglycosides
TIME HISTORYRefer if >24 hours
OTHER SYMPTOMS DANGER SYMPTOMSRefer if >24 hours
Non-pharmacologic therapy
1. Avoid loud noises or use noise protectors2. Avoid caffeine or smoking3. Use masking techniques or devices4. Hearing aids in hearing loss5. Stress management and biofeedback6. Tinnitus retaining therapy
Acupuncture not found to be a benefit
Pharmacologic Therapy
Antidepressants – no evidenceGingko biloba –evidence is lacking.
Drug Side Effects CommentsGingko GI
HeadacheDizzinessPalpitationsAllergic skin reactions
Bleeding and seizures!
Avoid in warfarin or antiplatelets
Vitamin A and zinc have been used, but no evidence.
21

Eyelid Conditions
Hordeolum Chalazion BlepharitisPathophys Stye (most common)
Glands of ZeisSmall/superficialExternal – towards the skin
Meibomian GlandsLargerInternalPoint to skin or conjunctivaMore prolonged courseUsually staph aureus
Chronic inflammation of meibomian gland. Painless, localized swelling.
Most point towards conjunctiva.
More common in- blepharitis- rosacea- seb dermatitis
With recurrent, refer.
ChronicBilateral eyelidsCan be mixed, anterior and posteriorCan be associated with skin conditions.Can result in permanent damage e.g. scarring and damage to cornea
See next page
Assessment Unilateral, localized lid swelling, tenderness and redness. May occur with blepharitis.
May resemble stye, but without acute inflammatory signs. May press on eyeball for visual distortion
Irritation, burning and itching of the lid margins. Foreign body sensation, worst in mornings.
Time 48h Improvement – a few days. Complete can take weeks to months
Chronic
Prevention Avoid touching the eye and rash hands afterwardsChange compresses and towels after each useDo not let eye drops touch eye/lashes
Good eyelid hygiene Lid hygiene
Lifestyle Warm compresses 10-15 mins, tid/qid.Massage afterwards.Hard boiled eggsUsually drains in 2 days. If longer, refer.
Same 1. warm compresses2. eyelid scrub with baby
shampoo3. mechanical expression
my ophthalmologistUse once or twice daily at outbreak, or twice weekly when under control
OTC Not recommended Same NonePrescription After incision –
Antibacterial e.g. bacitracin or erythromycinIf cellulitis, erythromycin, cloxacillin or tetracycline
Steroid injections in lesion or incision. Topical steroids or antibacterials good.
Ointments after eyelid cleaning – bacitracin and erthyromycinSteroids and antibacterials at breakoutPosterior – systemic tetra, doxy or minocycline. Erthyromycin when CI
Refer If >2 days If recurrentIf large/painfulNo improvement within a few days
Eye painPhotophobiaImpaired visionTraumaChemical exposure
Foreign bodyHeat exposureEye protrusionContact lens wearer>48 hours and no improvement
22

Blepharitis
ANTERIOR POSTERIORSTAPYLOCOCCAL BLEPHARITISs. aureus and s. epidermitisinflammation and redness along anterior portion of eyelid. Scaly, crusts and ulceration in eyelids. Loss of lashes in chronic, recurrent styes
MEIBOMIAN SEBORRHEAExcessive glandular secretions.Photophobia, burning, oily and frothy tear film. Few signs of inflammations.
SEBORRHEIC BLEPHARITISNon-ulcerativeMore oily and greasy, less scaly.Will have sebborrheic dermatitis in other areas.
MEIBOMIANITISInflammation and obstruction of glands.Can be diffused or localized.Soft cheesy substance expressed
CHALAZION ARE1. LARGER2. MAY NOT HURT
Compared to styes
SEE MINOR AILMENTS BOOK REGARDING PUTTING IN EYE DROPS
23

Conjunctivitis
SymptomsForeign body sensation, scratching or burning sensation, fullness around the eyes and mild photophobia. Redness, crusty after sleeping.
Viral Bacterial AllergicItching Minimal Severe
Redness GeneralizedDischarge Profuse, serous Moderate, white Moderate, serous or
white
Acute Bacterial Hyperacute Bacterial
Chronic bacterial
Viral Allergic
Self limiting, resolves in 2 weeks. Can be reduced to 1-3 days.S aureusS pneumoniaeH influenzae
Neonates/sexually active young people. V serious, sight threatening.Neiserria G and MYellow green discharge. Bilateral in neonates
4 weeksusually with other condition e.g. blepharitiss aureusMoraxella lacunata (makeup)
Subconjunctical haem.UrtiWatery dischargeMay spread from one eye to the other.AdenovirusHerpes (keratitis)2-4 weeks
Itching, tearing, red eye
HandwashingWarm compressSaline irrigationReplace eye drops
Refer Lid hygieneWarm compresses
Infectious 2 weeks after 2nd eye infectedChildren out of school for 1 week
Avoidance strategies, cold compresses
Polysporin QID for 5-7 days, treat 2 days after it has resolved
Refer immediately Refer Antihistamines, lubricants
Oral antihistamines
Trimethoprim / polymixin BErythromycinBacitracinSylfacetamide sodium – cheap and toleratedAminoglycosides good for gram neg – toxicity and allergic reactionsChloram – aplastic anaemiaFluoroquinolones (oxacins” for more serious infections e.g. keratitis
Antibacterials (after gram staining) and irrigation.
Ceftriaxone 1-2g IM in adultsSpectinomycin or oral cipro can be used in penicillin allergic
Topical antibacterials.
Doxy/erythro for meb gland dysfunction or severe acne rosacea.
Topical metronidazole for rosacea
NOT antivirals or steroids in adenovirus
Herpes zoster – topical trifluridine and oral antivirals
Levocabastine and emedastine – rapid onset.OlopatadineNedocromin and lodoxamide.
Ketorolac can decrease itching and redness
Severe may need steroids
Contact lens wearersIf symptoms have not improved after 2 days with treatmentChildren
Refer all Refer all Refer all Refer moderate to severeThose who do not respond in 72h
24

Dry Eye
AGE SYMPTOMSFemales Discomfort, visual disturbance, tear film
instability with potential damage to ocular surface. Increased osmolarity of tear film and inflammation of ocular surface
1. aqueous tear deficient DE2. Evapourative dry eye
May overlapHard to diagnose – signs and symptoms may not concordSandy foreign body experience. Worsens over day. Tired, difficulty moving lids, photophobiaIncreased tearing in some circumstances e.g. reading
MEDICATION EXTRA MEDICATIONAnticholinergic drugsAmiodoroneAntiandrogenicB blockersDiureticsinterferonIsotrenitonHRTBenzalkonium chloride as a preservative in drops
TIME HISTORYWorsens over course of the dayRefer if last more than 3-5 days
Environmental – keeping eyes openDiet low in Vitamin A or omega 3 fatty acidsParkinsons
OTHER SYMPTOMS DANGER SYMPTOMSComplications:
1. ocular surface erosions2. epithelial damage3. ocular surface keratinization4. ulceration5. perforation6. scarring7. reduced vision
Refer anyone with autoimmune diseaseSymptoms to do resolve in 3-5 days or worsenComplicationsIf preservative burn patients eyes
Prevention
Remind patients about AC drugsContact lens wearers – clean lensesBlink more during concentrated tasksBlepharitis – lid hygiene
25
Non Pharmacologic OTC RXAvoid smoking and smoky roomsHumidifiersMoisture chamber spectacles, ski masksMoist washcloth over closed lids
Tear duct occlusion (by eye care practicioner)
Trial and error approach1-2 week trial of everything
with meibomian gland dysfunction, use omega 3
for factors to think about, see below
Opthalamic cyclosporine and loteprednolSjogren – oral pilocarpine
OthersTopical acetylcysteine, methylprednisolone, estradiol, periorbital IM injections of botulium toxin
Factors for OTC choice
1. ELECTROLYTE COMPOSITION Potassium – maintains corneal thicknessBicarbonate – aids recovery of epithelia barrier function in damaged cornea. May also maintain mucous layer of tear film
2. CRYSTALLOID OSMOLARITY Hypo-osmotic tears used to counteract increased ions with people who have DED
3. COLLOIDAL OSMOLALITY High osmolality stabilizes the volume of corneal epithelial cells. Solutes are taken up by cells so they don’t have to do this internally
4. VISCOSITY AGENTS High viscosity is good – carboxymethylcellulose, hypromellose, PVA, PEG, glycol 400 and propyleytylene glycol.HP-Guar forms bioadhesive gelCastor/mineral oil restore lipid layerSodium hyaluronate – viscosity 500,000x salineCarbomer – 940 resembles an ointment, but less blurred vision than petroleum
5. CYTOTOXIC AGENTS EDTA – can damage corneal epithelial cellsLanolin – irritation to those intolerant to sheeps wool
6. PRESERVATIVES If application more than 4x day then use preservative freeBenzalkonium chloride- toxic to corneal epitheliumOxidative preservative better e.g. polyquad, purite or sodium chlorite (‘vanishing”)OINTMENTS USUALLY DO NOT REQUIRE PRESERVATIVES
26

Contact Lens Care
Rigid Glass Permeable (RGP) and softLongetivity:
1. conventional >1 year2. planned replacement (2 weeks, 1 month or every 3 months)3. daily disposable
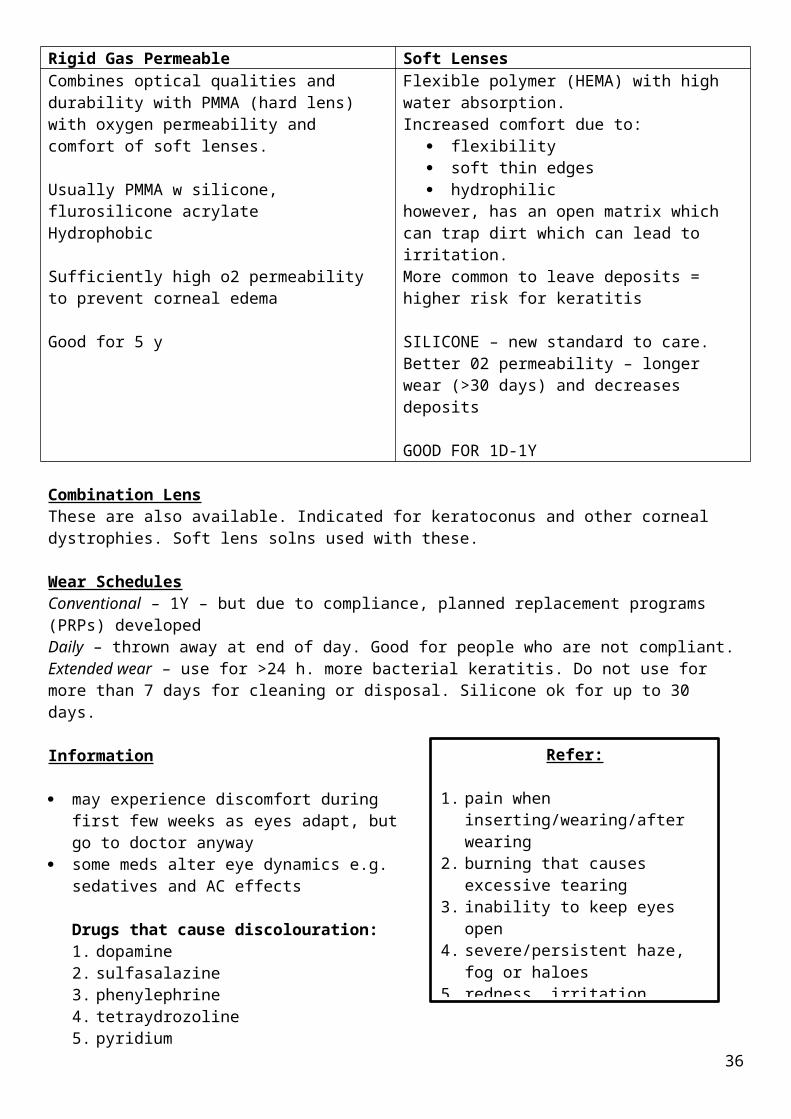
Rigid Gas Permeable Soft LensesCombines optical qualities and durability with PMMA (hard lens) with oxygen permeability and comfort of soft lenses.
Usually PMMA w silicone, flurosilicone acrylateHydrophobic
Sufficiently high o2 permeability to prevent corneal edema
Good for 5 y
Flexible polymer (HEMA) with high water absorption.Increased comfort due to:
flexibility soft thin edges hydrophilic
however, has an open matrix which can trap dirt which can lead to irritation.More common to leave deposits = higher risk for keratitis
SILICONE – new standard to care. Better 02 permeability – longer wear (>30 days) and decreases deposits
GOOD FOR 1D-1Y
Combination LensThese are also available. Indicated for keratoconus and other corneal dystrophies. Soft lens solns used with these.
Wear SchedulesConventional – 1Y – but due to compliance, planned replacement programs (PRPs) developedDaily – thrown away at end of day. Good for people who are not compliant.Extended wear – use for >24 h. more bacterial keratitis. Do not use for more than 7 days for cleaning or disposal. Silicone ok for up to 30 days.
Information
may experience discomfort during first few weeks as eyes adapt, but go to doctor anyway
some meds alter eye dynamics e.g. sedatives and AC effects
Drugs that cause discolouration:1. dopamine2. sulfasalazine3. phenylephrine4. tetraydrozoline5. pyridium6. nitrofurantoin7. rifampicin8. tetracycline
Refer:
1. pain when inserting/wearing/after wearing
2. burning that causes excessive tearing
3. inability to keep eyes open4. severe/persistent haze, fog or
haloes5. redness, irritation, itching6. poor vision 7. painful lid swelling8. photophobia
27

There are 2 forms of chemical disinfection: oxidizing agents (hydrogen peroxide) disinfecting
Eye doctor would have recommended one.
Should always be rinsed after dropping them
Always ask about compliance – soft lenses can be recommended
RGP SOFT
Remove lens from eye Remove lens from eye
Clean with surfactant cleaner Clean with surfactant cleaner
Rinse with soaking soln/saline Rinse with rinsing soln
Clean with enzyme cleaner every week then
rinsing soln afterwards
Store overnight in soaking soln Store overnight in disinfectant (look at product
for times)
Rinse with soaking soln Rinse with rinsing soln
Add a few drops of wetting soln to concave lens
Place on eye, rewet if required and discard used
solutionsPlace on eye, rewet if required and discard used
solutions
DO NOT SWITCH BETWEEN BRANDS, can only recommend what eye professional has given. Usually a trial and error approach.
Unpreserved aerosol saline is the only product that can be substituted by the wearer.
Ear Pain28

Condition Pain Itch Discharge Hearing loss
Other comments
Ruptured tympanic membrane
Yes (sudden and sharp)
No Yes Yes (abrupt) Can happen with acute OM and barotrauma
Earwax No (unless infected)
Frequently No (unless infected)
Yes (gradual)
Fulness or pressure
Acute bacterial OE
Yes (acute) Sometimes Frequent Sometimes Pain when chewing, movement of auricle.Excessive moisture, trauma, scratching
Eczemateous otitis externa
Sometimes Yes Sometimes (oozing, crusting)
Sometimes Will have other condition.May become infected
Otitis media Yes (abrupt) No Yes (if TM ruptures)
Sometimes ChildrenURTI to followRelieved with rupture of TM
Foreign Body Yes Sometimes If becomes infected
Yes Fullness and pressure in ear
Barotrauma Yes No Yes if TM Ruptures
Yes Aire travel and diving. Tinnitus and vertigo may be present
Refer: ear surgery in past 6 weeks ruptured TM (acute onset hearing loss with pain) Tympanostomy tubes Ear drainage (except definite EOM) Otitis media Foreign body When flying/scuba diving >24h Other symptoms >2-3days Hearing loss with no reason If hearing loss doesn’t improve following resolution of nasal congestion
Drug Related Ototoxicity
Cisplatin Loop diuretics Quinine AminoglycosidesASA Phosph type 5 Minocycline Macrolides
Otitis Media
Otalgia – ear painOtorrhea – ear drainage
29

AGE SYMPTOMSOM most common in children (75% <1 yr)Refer if <6months
Middle ear inflammation (acute ear pain, unilateral and developing over a few hours. Fever and reduced hearing)May occur with URTIPresence of middle ear effusionAcute onset
MEDICATION EXTRA MEDICATION
TIME HISTORYMore present during winter monthsRefer if >72hRefer if chronic or reccurrent
OTHER SYMPTOMS DANGER SYMPTOMSALL CASESOtorrhea<6monthshistory of chronic or reccurentcraniofacial abnormalitiesif lasts longer than 72 hours
“Wait and see” approachUse analgesia for first 48-72 hours, including child >6 months. Oral preferably, topical can cause irritation and hypersensitivity.if antibiotics are used, systemic only.Do not use decongestants or antihistamines.If using warm oils, only warm in palms due to burns. Never use in ruptured TM. Never sleep with hot water bottle.
Otitis Externa
30

AGE SYMPTOMSChildren 7-12, declines >50yrs Pain and discharge present. Normally unilateral
Bactererial OE- otalgia, pruritis and tenderness. Especially on movement of ear. Cellulitis of pinna and regional lymphadenopathy may be present.Fungal OE- pruritis and fullness in the ear, usually after antibiotic treatment. May have black, grey, blueish green, yellow or white fungal elements in EACAcute localized: Due to a boil by S aureus. Pain, itch, redness, edema, absessChronic – thickening of skin due to infection and inflammation. Itch and dry flaky skin – allergic contact dermatitisEcsemateous OENecrotizing – diabetic or immunocompromized. Extends to mastoid or temporal bone. Systemic antibiotics required
MEDICATION EXTRA MEDICATION
TIME HISTORY
OTHER SYMPTOMS DANGER SYMPTOMSEdema and debis in EAC – cleansing must be done first by physicianIf no improvement in 3-5 days. May take 1-2 weeks for full resolution
Therapy
Topical acidifying agents, antibiotics alone or antibiotic/steroid combo.
Eye products can be used as less acidic
Topical aminoglycosides can cause ototoxicity, if used for >1 week and after infection has subsided
Instill 3-4 drops 3-4 times daily. Treat for 1 week. Symptoms may last 6 days after treatment begins. If symptoms not completely gone, then treat for up to 2 weeks.
Fungal can be treated by cleansing and acidification alone. If not, compounded topical antifungals can be used.
Also – analgesia can be used. Topical analgesia not recommended.
Polysporin OTC is besEczematiousAvoid offending product
31

Apply aluminium acetate solutionre-acidifying with topical steroid
Prevention of re-occurance1. after swimming or bathing, dry EAC with hairdryer on low/instill with acidifying or alcohol drops2. avoid over cleaning and scratching3. avoid cotton swabs4. avoid water sports 7-10days after treatment
Impacted Earwax32

AGE SYMPTOMSMore common in older aged people with hearing aidsRefer if a child
Sensation of fullness in the ear, hearing loss and discomfort
MEDICATION EXTRA MEDICATION
TIME HISTORYHistory of cleaning with cotton swabs
OTHER SYMPTOMS DANGER SYMPTOMSInjuried earPerforated TMRecent ear surgeryTM tubesDrainage from earHearing lossTinnitus or dizzinessChild3-4 days or 5-7 days with oil based product. Should get relief straight after syringing.
PreventionOlive oil, light mineral oil, hydrogen peroxide, glycerin and sodium biocarbonate
TreatmentSyringing (can se eardrops of soften the wax) at physicians office, emergency department or at home with a caregiver. DO Not TRY TO DO THIS ON ONESELFContraindicated in:
if TM has been perforated in the past or now TM tubes present Ear surgery history Only hearing ear that in affected Children are uncooperative
Water based, oil based and carbamide peroxide equally effective. Instill 15 mins prior to syringing, or use for 3 nights prior to syringing.
URTI
Symptom Cold Allergic Flu Sinusitis Pharyngitis
33

rhinitisNasal discharge & congestion
Clear, then mucopurulentCongestion is common
Loads – clear.Congestion aswell
Clear, then mucopurulentCONGESTION IS RARE
Persistent rhinorrheaYellow/green
Rare
Fever Rare no Yes – sudden onset
possible Yes
Sore throat Common(mild) dry, scratchy
no Sometimes no Severe, sudden onset
Cough Mod to moderateDry -> prod
Yes – if postnasal drip
Non-productive
Yes – if postnasal drip
rare
Headache Rare, via sinus congestion
via sinus congestion
Yes via sinus congestion
no
Aches & pain Mild Earaches (in children)
Common Rare possible
Other Sneezing in first few days
Itchiness, watery eyes, sneezing
Fatigue, weakness, n&V
Facial tenderness, toothache
no
Duration 5-7 days, up to 14 days
As long as exposed
10 days Days to weeks 3 days
Etiology Viral Not infectious Viral All Viral>bacterial
Croup is a barking cough, usually unproductive. Inspiratory stridor, dyspnea and fever= refer
REFER:1. Difficulty breathing, wheezing, stridor, chest pain2. History of respiratory disease3. Difficulty swallowing4. Fever >38.5 for >72h5. Cough>3wks6. Severe throat pain7. Severe headache, neck pain8. Prolonged nasal congestion with mucopurulent
discharge
Child:1. Symptoms of croup/ear infection2. Excessive lethargy/irritability3. Skin rash4. Cough with vomiting5. Dehydration in infant6. <3months with fever
Severe symptoms with reduced fluids intake
Allergic Rhinitis
AGE SYMPTOMS34
Children have 30% chance if one parent affected and 50% if bothUsually peaks in early twenties/later teens and decreases >45yrs
Refer <2 yrs
Seasonal – spring to fallPerennial – all yearNon-Allergic – acute and chronic
MEDICATION EXTRA MEDICATIONOveruse of topical decongestantsACENSAIDsBblockersChlorpromazine
SildenafilPhentolaminePrazosinReserpineOral contraceptivesCocaineMethyldopa
Overuse of topical decongestants!!!
TIME HISTORYRefer if tried OTC >2weeks and no response Hypothyroidism and pregnancy can cause it as
well as menustrationRefer if comorbid illnessRefer if allergen not identified
OTHER SYMPTOMS DANGER SYMPTOMSTearing, stuffy or runny nose, itchy face, sneezing Refer if tried OTC >2weeks and no response
If allergen not identifiedFeverPurulent discharge<2yrs oldco-morbid illness e.g. asthmacan not sleep, very dehabilitated
Prevention
Measures can take weeks or months to help.
Avoid smoking, insect sprays, air pollution and fresh tar or paint
Surgery may be required
Prevention
Pollen Outdoor Molds Indoor molds House dust mites AnimalKeep windows Remain in closed Use fungiside on Avoid carpet Remove pet – trial
35
and doors closed
Keep air conditioning on indoor cycle
Do not use window or attic fans
Avoid outdoors at high pollen counts
Do not dry clothing outside
Shower or bathe after being outside
environment for as much as poss
Keep air conditioning on indoor cycle (can still be v contaminated)
Use face masks when raking leaves etc
sinks, showers, veg storage areas and garbage pails – or 50:50 bleach in water
Avoid colsole humidifiers and cool mist vapourisers – if used keep clean
Install plastic vapor barrier over exposed soil and keep foundation vents open if crawl space
Remove houseplants
Avoid carpet or furnish the basement if damp or floods
Plastic, leather or wood furniture good
Acarasides – no proven use
Avoid vacuuming or making beds – if so use mask for that and 15 mins afterwards
Vaccum cleaner – double filtration system
Clean while patient not at home
Indoor humidity between 40-50%
Avoid humidifiers
Incase all matresses and pillows
Replace old matresses
Wash bedding at 60 q2w
Avoid stuffed toys that connot be washed
Do not store items under bed
Use window shades – not venetian blinds
not good. Can take 20 weeks for cat allergens to be gone
If not:Put pet in non carpeted area, use heap filter or air purifier or not do put animal in bedroom
Wash cat weekly and dog twice weekly
Eliminate litter boxes or put them in abandoned place
Treatment
AntihistaminesGenerally do not relieve nasal congestion.
36

Desloratadine, fexofenadine and cetirizine have modest effects, but only desloratadine is licensed.
Cetirizine most drowsy of 2nd gen.
If tolerance occurs – change to different class. Take for as long as exposed!
Avoid in narrow angle glaucoma, CV disease, chronic lung disease, stenosing peptic ulcer, prostatic hypertrophy
Mast Cell Stabilizers – Sodium CromoglicateDelayed for up to 4 weeks. Less effective
DecongestantsOral have a weaker effect on obstruction. May increase BP. MAOIs – hypertensive crisis!
RX therapy
Steroids – work best. May take a week weeks for max benefit, but 6-8 hours.
Montelukast
Immunotherapy recommended for unavoidable patients
Intranasal ipratropium bromide for rhinnorhea only
Butterbur – natural remedy
ChildrenPediatric 1st gen antihistamines - >6monthsNasal steroids >4yrsDecongestants>6years
PregnancyNasal steroids okAntihistamines okAvoid oral decongestants in 1st trimesterTopical decongestant ok
37