mitral valve disease, when to intervene - fumed · mitral valve disease, when to intervene swedish...
TRANSCRIPT
Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease
Mitral Valve Disease, When to
Intervene
Swedish Heart and Vascular Institute
Structural Heart ProgramSwedish Heart & Vascular Institute
Conflict of Interest
None
Structural Heart ProgramSwedish Heart & Vascular Institute
3
• Current ACC/AHA guideline
• Stages of Heart Valve Disease
• Evaluation of Surgical and Interventional Risk
• Evidence based management of mitral valve disease
• The transcatheter valve therapy, MitraClip and valve implantation
Objective
Structural Heart ProgramSwedish Heart & Vascular Institute
Structural Heart ProgramSwedish Heart & Vascular Institute
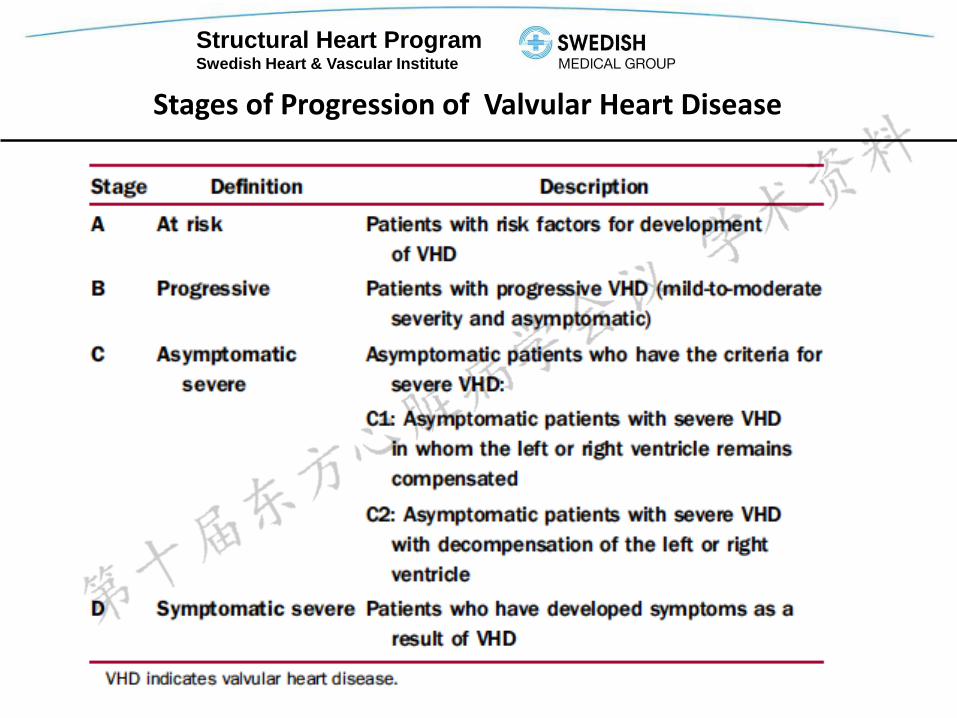
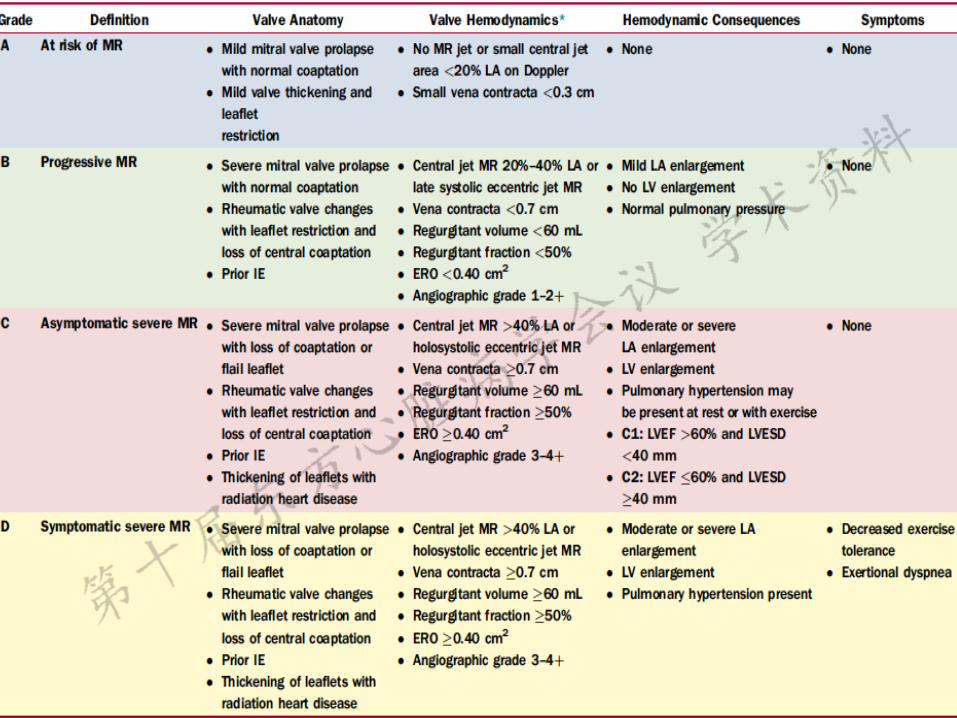
Stages of Progression of Valvular Heart Disease
Structural Heart ProgramSwedish Heart & Vascular Institute
Structural Heart ProgramSwedish Heart & Vascular Institute
7
Abnormal structure and/or function of 1 or more of
the 4 components of the mitral apparatus
Leaflets, annulus,
Chordae tendineae,
Papillary muscles
Left ventricular myocardium
Structural Heart ProgramSwedish Heart & Vascular Institute
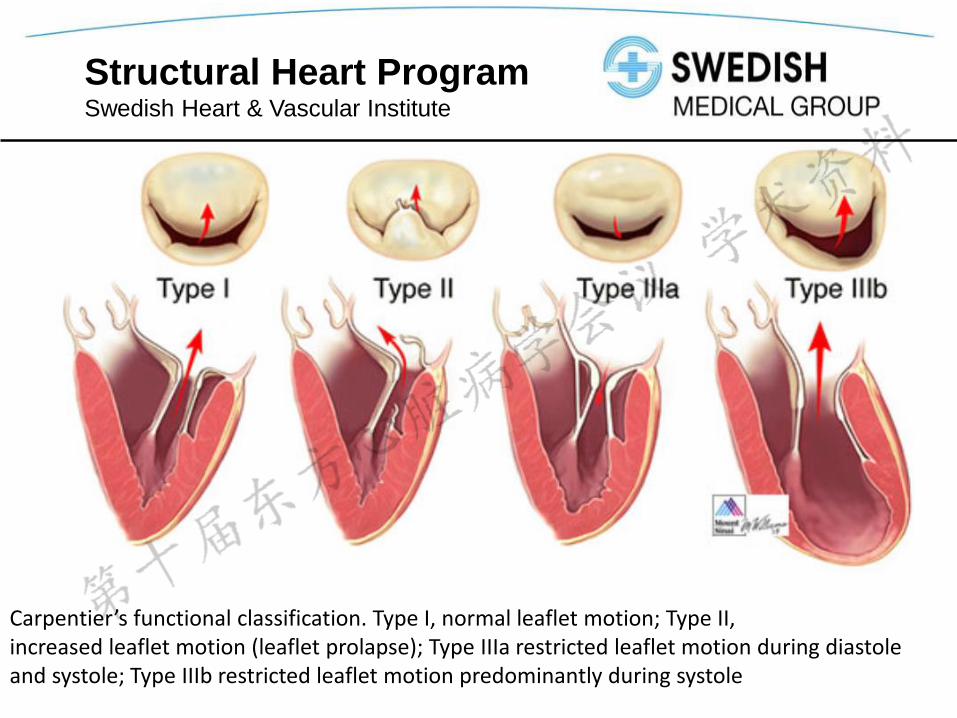
Carpentier’s functional classification. Type I, normal leaflet motion; Type II,increased leaflet motion (leaflet prolapse); Type IIIa restricted leaflet motion during diastoleand systole; Type IIIb restricted leaflet motion predominantly during systole
Structural Heart ProgramSwedish Heart & Vascular Institute
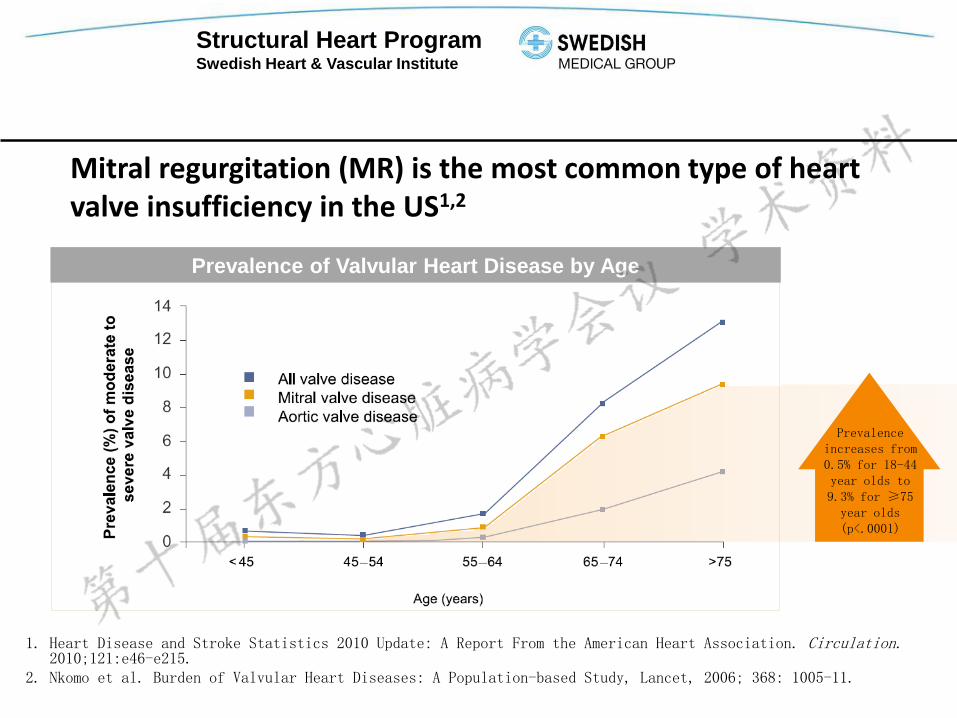
Mitral regurgitation (MR) is the most common type of heart valve insufficiency in the US1,2
1. Heart Disease and Stroke Statistics 2010 Update: A Report From the American Heart Association. Circulation.2010;121:e46-e215.
2. Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11.
12
Prevalence of Valvular Heart Disease by Age
Prevalence increases from 0.5% for 18-44 year olds to 9.3% for ≥75 year olds (p<.0001)
Structural Heart ProgramSwedish Heart & Vascular Institute
1. U.S. Census Bureau, Statistical Abstract of the U.S.
2. Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11.
3. Patel, et al. Mitral Regurgitation in Patients with Advanced Systolic Heart Failure, J of Cardiac Failure, 2004.
4. Rankin, et al, J of Thoracic and Cardiovascular Surgery, March 2006
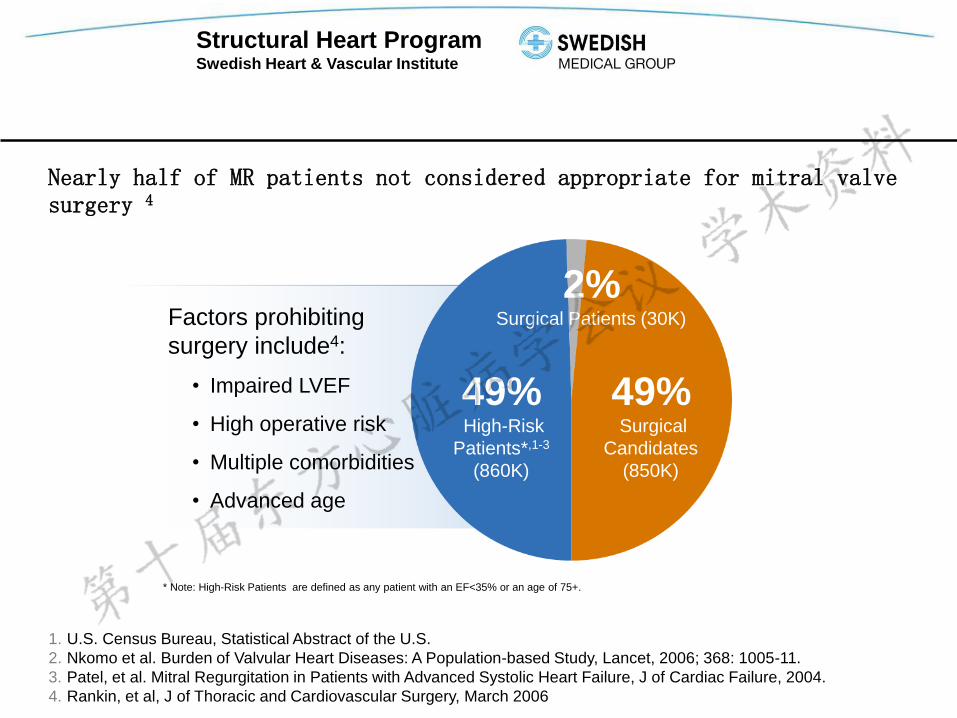
* Note: High-Risk Patients are defined as any patient with an EF<35% or an age of 75+.
49%High-Risk
Patients*,1-3
(860K)
49%Surgical
Candidates
(850K)
2%Surgical Patients (30K)Factors prohibiting
surgery include4:
• Impaired LVEF
• High operative risk
• Multiple comorbidities
• Advanced age
Nearly half of MR patients not considered appropriate for mitral valve surgery 4
Structural Heart ProgramSwedish Heart & Vascular Institute
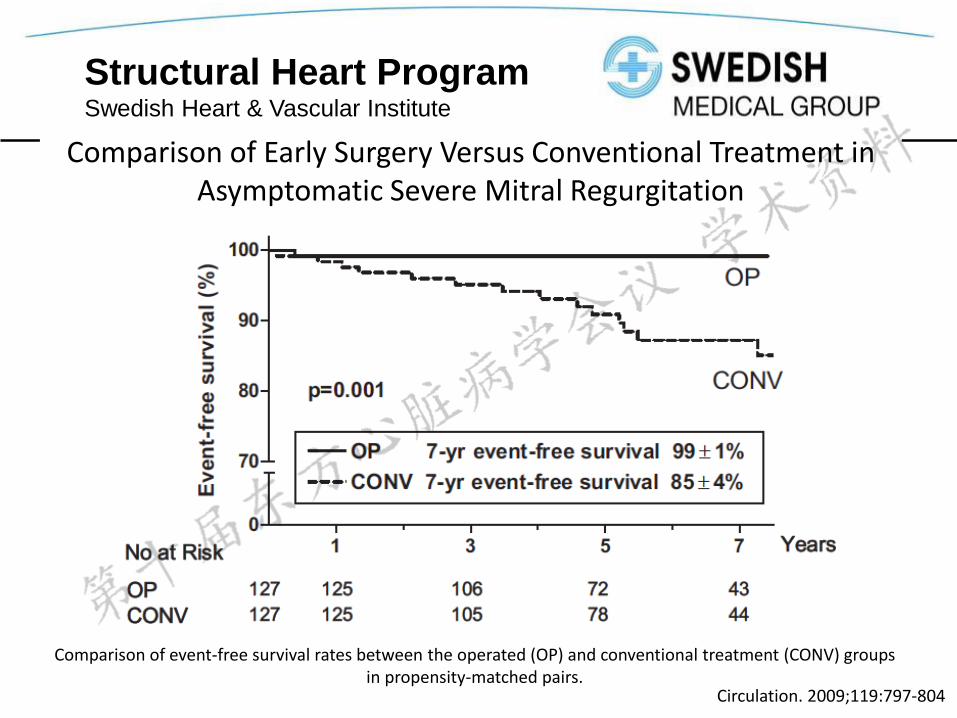
Comparison of Early Surgery Versus Conventional Treatment in Asymptomatic Severe Mitral Regurgitation
Comparison of event-free survival rates between the operated (OP) and conventional treatment (CONV) groups in propensity-matched pairs.
Circulation. 2009;119:797-804
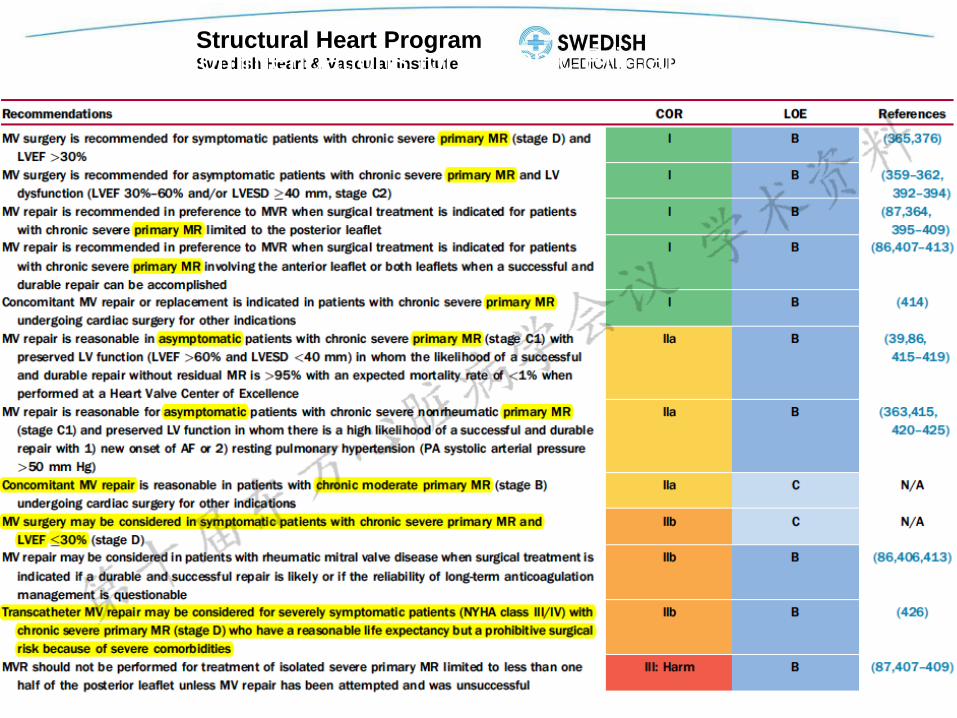
Structural Heart ProgramSwedish Heart & Vascular InstituteRecommendations for Chronic Primary MR
Structural Heart ProgramSwedish Heart & Vascular Institute
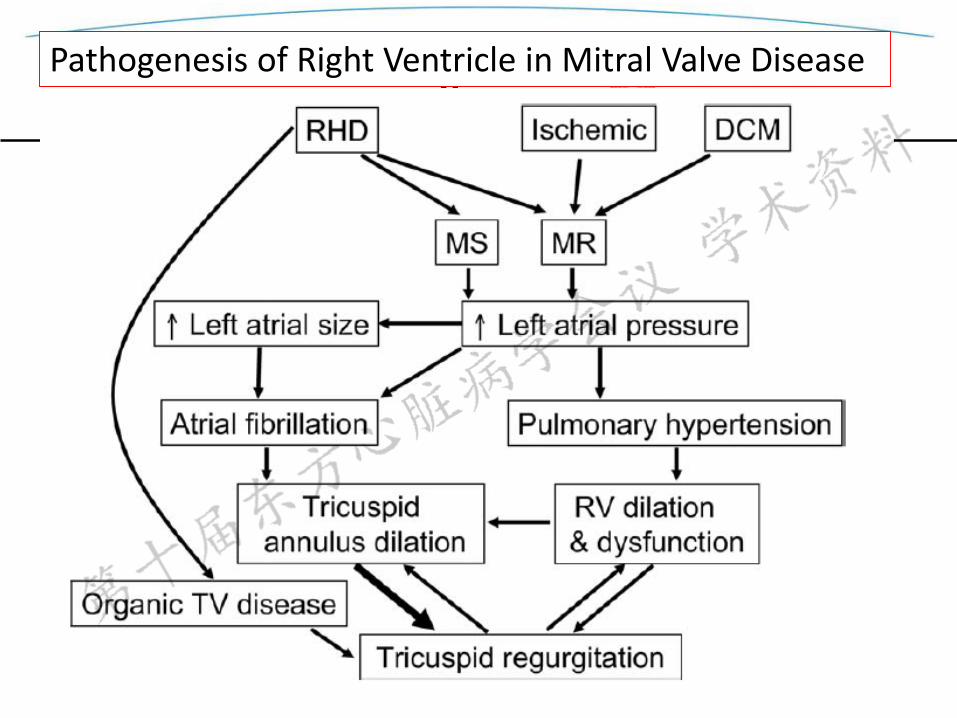
Pathogenesis of Right Ventricle in Mitral Valve Disease
Structural Heart ProgramSwedish Heart & Vascular Institute
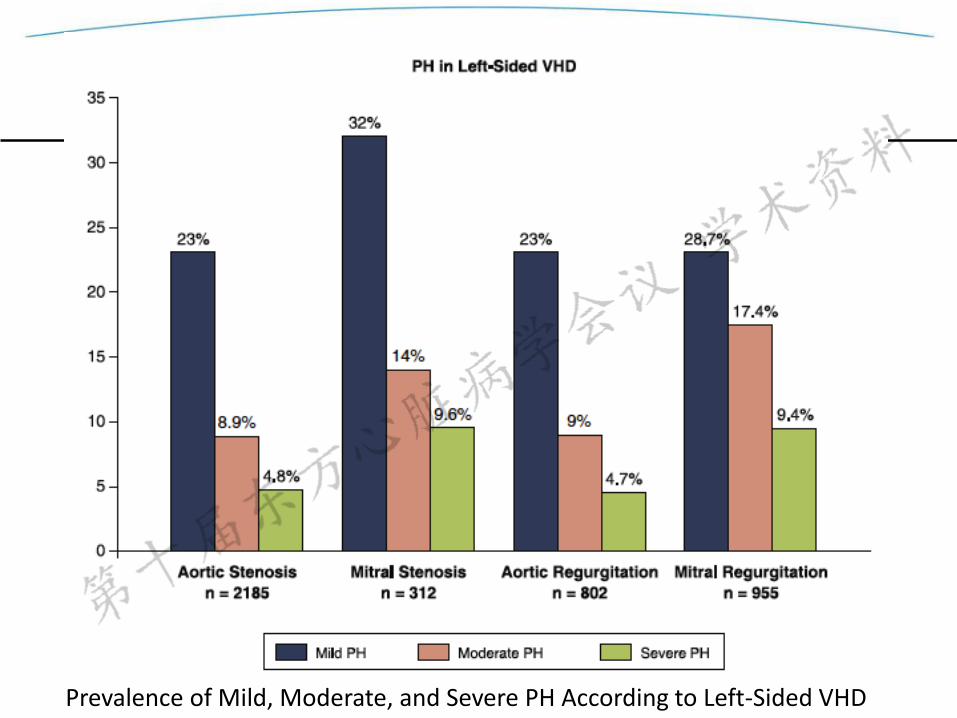
Prevalence of Mild, Moderate, and Severe PH According to Left-Sided VHD
Structural Heart ProgramSwedish Heart & Vascular Institute
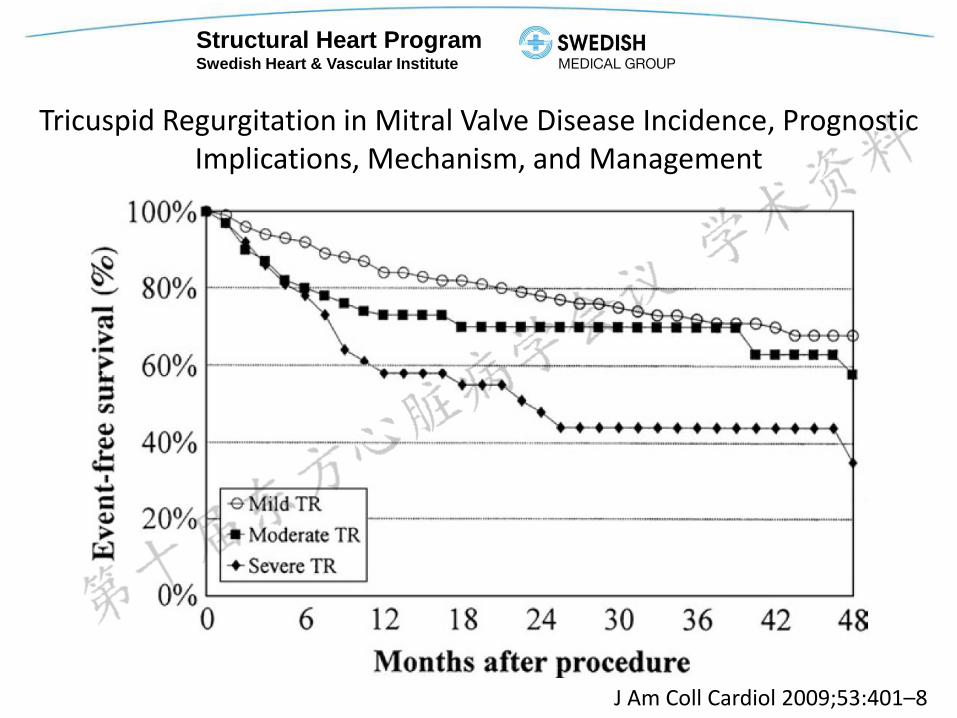
Tricuspid Regurgitation in Mitral Valve Disease Incidence, Prognostic Implications, Mechanism, and Management
J Am Coll Cardiol 2009;53:401–8
Structural Heart ProgramSwedish Heart & Vascular Institute
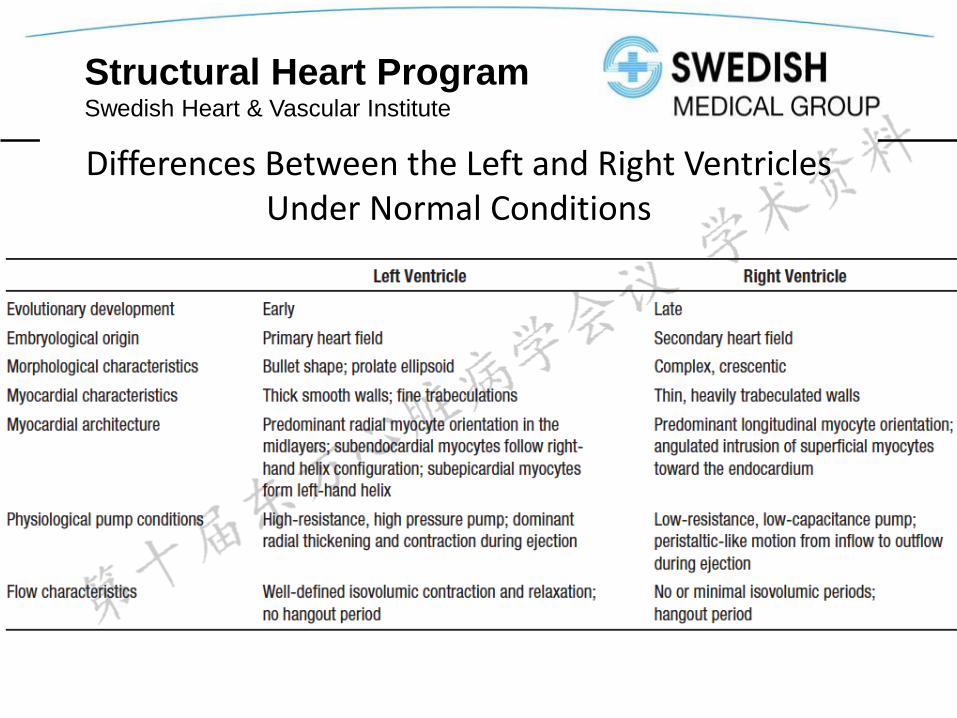
Right Versus Left Ventricular Failure Differences, Similarities, and Interactions
1. Embryological and Physiological Differences
2. Does the RV Differ From the LV in Its (Mal) Adaptation to Adverse Loading
3. How Does the RV Adapt to Chronically Increased Afterload
4. Mechanical and Functional Interdependence Between the RV and LV
Structural Heart ProgramSwedish Heart & Vascular Institute
Differences Between the Left and Right Ventricles Under Normal Conditions
Structural Heart ProgramSwedish Heart & Vascular Institute
18
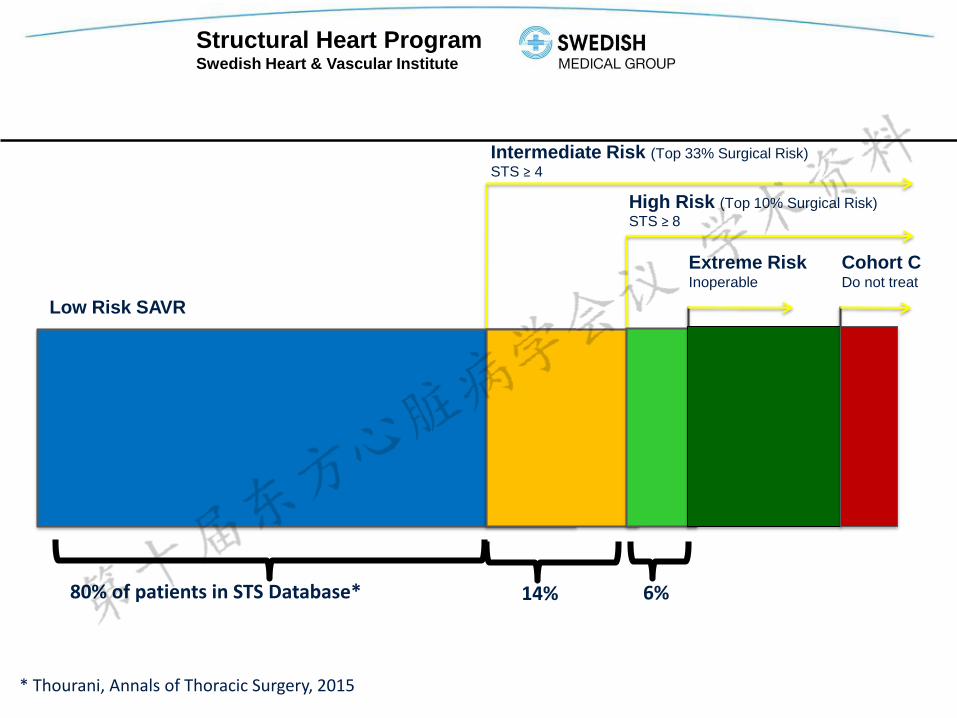
Intermediate Risk (Top 33% Surgical Risk)
STS ≥ 4
High Risk (Top 10% Surgical Risk)
STS ≥ 8
Cohort CDo not treat
Extreme RiskInoperable
Low Risk SAVR
80% of patients in STS Database* 14% 6%
* Thourani, Annals of Thoracic Surgery, 2015
Structural Heart ProgramSwedish Heart & Vascular Institute
ACCESS TO ABBOTT'S MITRACLIP® SYSTEM EXPANDS IN THE U.S. WITH MEDICARE NATIONAL COVERAGE DETERMINATION
- MEDICARE WILL PROVIDE NATIONAL COVERAGE FOR PEOPLE WITH SEVERE DEGENERATIVE MITRAL REGURGITATION DEEMED TOO SICK FOR SURGERY
- IN ADDITION, APPROVAL OF NEW TECHNOLOGY ADD-ON PAYMENT RECOGNIZES THE SUBSTANTIAL CLINICAL BENEFITS OF MITRACLIP THERAPY
ABBOTT PARK, Ill., Aug. 12, 2014 /
Structural Heart ProgramSwedish Heart & Vascular Institute
20
The surgical mitral repair procedure introduced in 1991 by the Italian
surgeon Ottavio Alfieri who successfully treated a patient with anterior
leaflet prolapse.
In the largest surgical series from this same group, including 260
patients who underwent such repair, 80% of the cohort had
additional MV annuloplasty that was associated with reduced
reoperation at a mean follow-up of 5 years.
J Thorac Cardiovasc Surg 2001;122:674–81
Structural Heart ProgramSwedish Heart & Vascular Institute
21
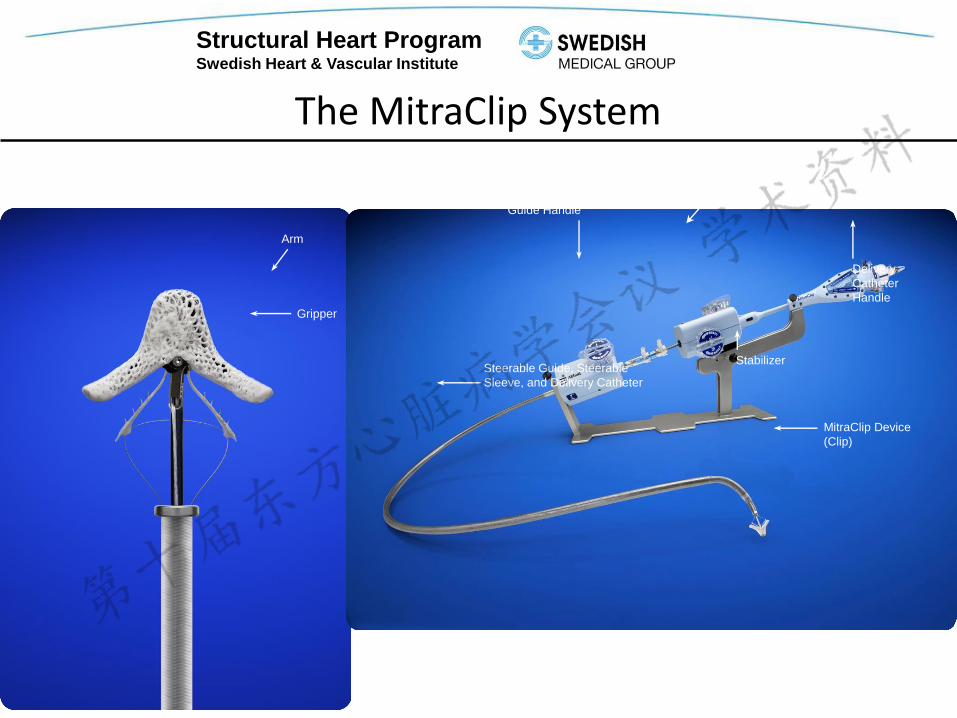
The MitraClip System
Gripper
Arm
MitraClip Device
(Clip)
Clip Delivery SystemMitraClip System
Delivery
Catheter
Handle
Stabilizer
Steerable
Guide Handle
Steerable Guide, Steerable
Sleeve, and Delivery Catheter
MitraClip Device
(Clip)
Structural Heart ProgramSwedish Heart & Vascular Institute
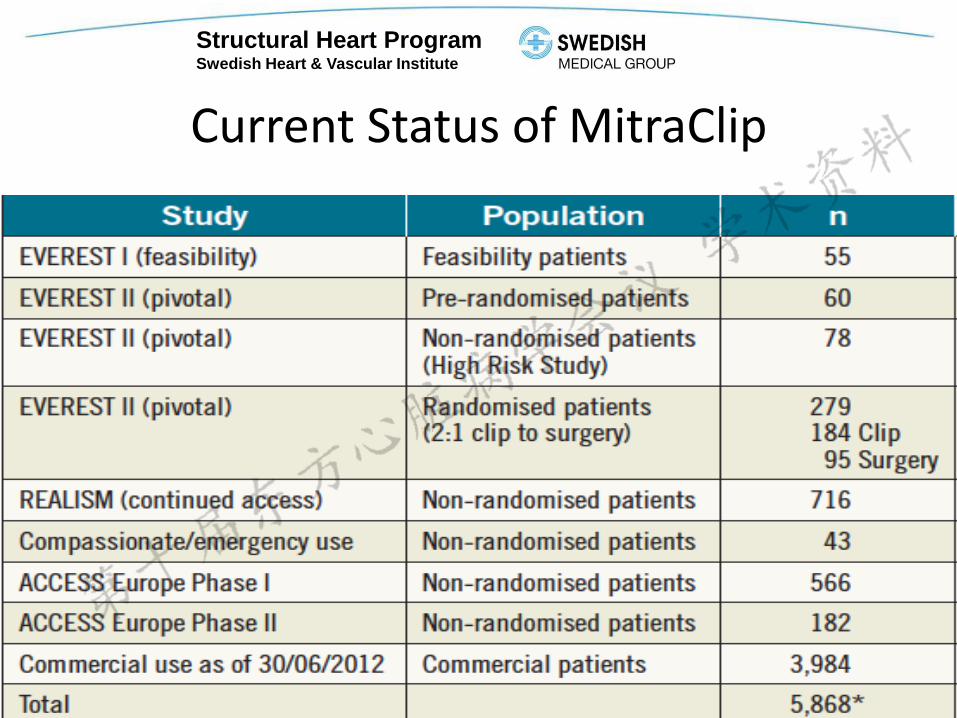
Current Status of MitraClip
22
Structural Heart ProgramSwedish Heart & Vascular Institute
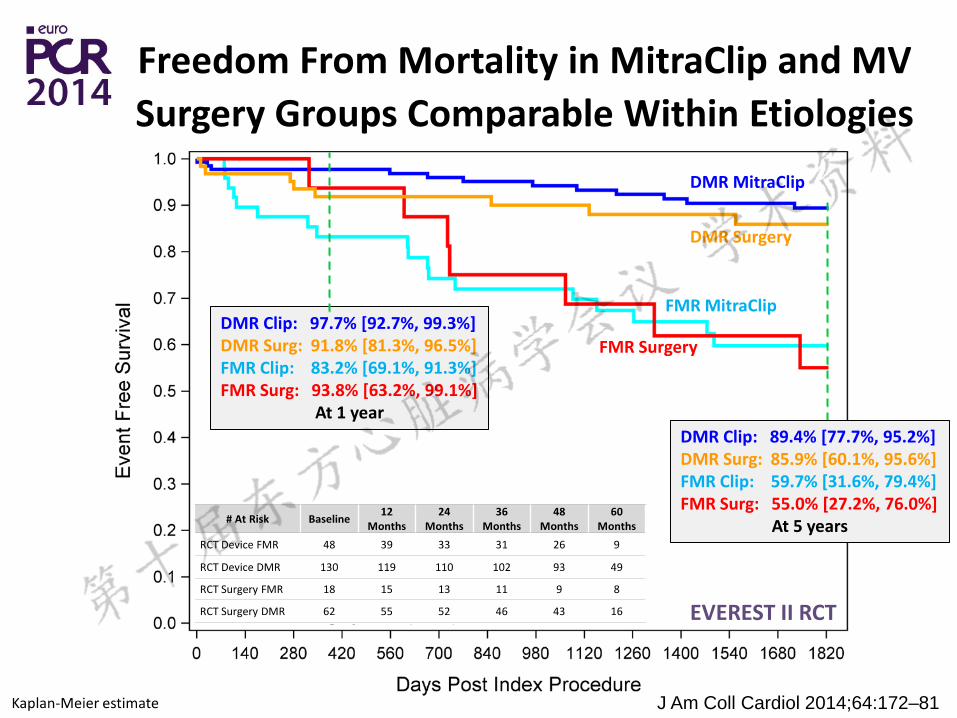
J Am Coll Cardiol 2014;64:172–81
Structural Heart ProgramSwedish Heart & Vascular Institute
Outcomes of the Initial Experience with Commercial TranscatheterMitral Valve Repair in the United States study,
The U.S. National TVT Registry 2015
This study included data from 564 high-risk patients with primary mitral regurgitation (MR)
Procedural success rate of 91.8% and a procedural complication rate of 7.8%. Procedural stroke rate was 1.8% The major bleeding rate was 3.9%.
Pre-implantation MR grade was 3 in 94% of patientsPost-implantation MR grade was 2 in 93% of patients and 1 in 63.7% of patients.
In hospital mortality was 2.3% and 30-day mortality was 5.8%.
Structural Heart ProgramSwedish Heart & Vascular Institute
Q&A
Structural Heart ProgramSwedish Heart & Vascular Institute
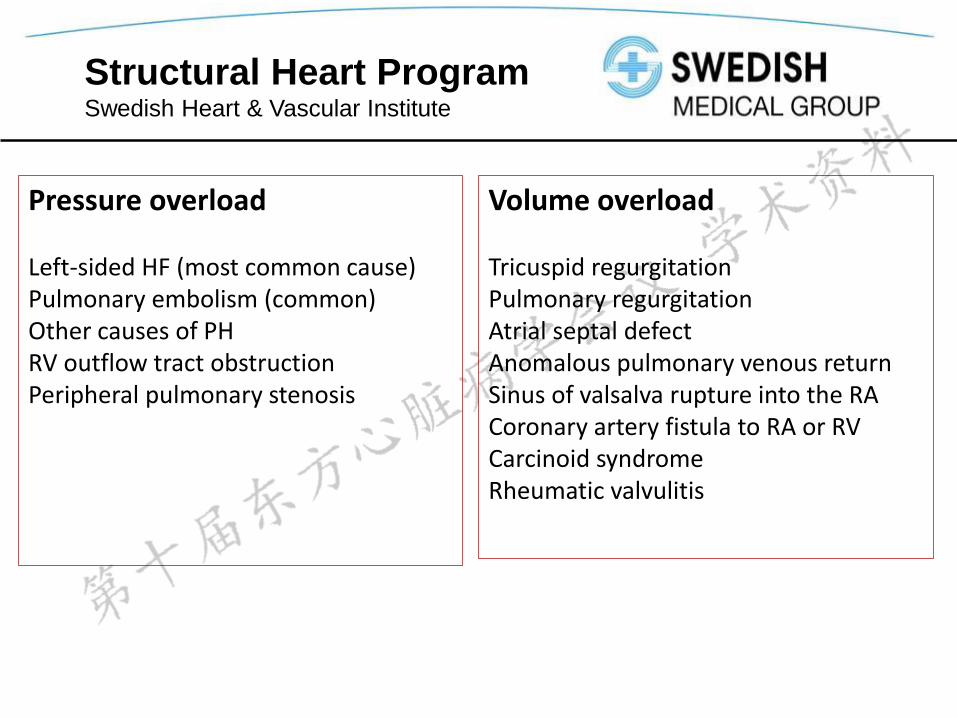
Pressure overload
Left-sided HF (most common cause)Pulmonary embolism (common)Other causes of PHRV outflow tract obstructionPeripheral pulmonary stenosis
Volume overload
Tricuspid regurgitationPulmonary regurgitationAtrial septal defectAnomalous pulmonary venous returnSinus of valsalva rupture into the RACoronary artery fistula to RA or RVCarcinoid syndromeRheumatic valvulitis
Structural Heart ProgramSwedish Heart & Vascular Institute
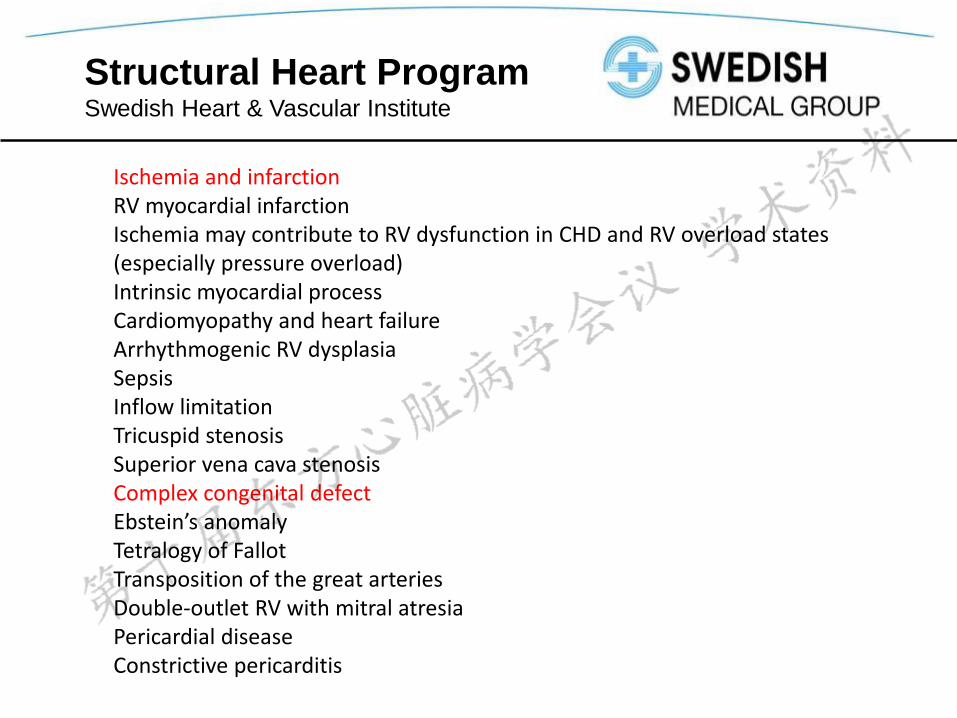
Ischemia and infarctionRV myocardial infarctionIschemia may contribute to RV dysfunction in CHD and RV overload states(especially pressure overload)Intrinsic myocardial processCardiomyopathy and heart failureArrhythmogenic RV dysplasiaSepsisInflow limitationTricuspid stenosisSuperior vena cava stenosisComplex congenital defectEbstein’s anomalyTetralogy of FallotTransposition of the great arteriesDouble-outlet RV with mitral atresiaPericardial diseaseConstrictive pericarditis