mmpi differences for renal, psychiatric, and general medical patients
TRANSCRIPT
178 Journal of Clinical Psychology, March 1990, Vol. 46, No. 2
DAVIS, W. E., & JONES, M. H. (1974). Negro versus Caucasian psychological test performance revisited. Journal of Consulting and Clinical Psychology, 42, 675-679.
FRY, F. D. (1949). A study of the personality traits of college students and of state prison inmates as measured by the Minnesota Multiphasic Personality Inventory. Journal of Psychology, 28, 439-449.
GYNTHER, M. D. (1972). White norms and black MMPIs: A prescription for discrimination? Psychological Bulletin, 78, 386-402.
GYNTHER, M. D., GREEN, S. B. (1980). Accuracy may make a difference, but does a difference make for accuracy? A response to Pritchard and Rosenblatt. Journal of Consulting and Clinical Psychology, 48,
GYNTHER, M. D., LACHAR, D., & DAHLSTROM, W. G. (1978). Are special norms for minorities needed? Development of an MMPI F scale for blacks. Journalof Consulting and Clinical Psychology, 46, 1403-1408.
MILLON, T. (1983). Millon Clinical Multiaxial Inventory. Minneapolis, MN: National Computer Systems. MILLON, T. (1984). Millon Clinical Multiaxial Inventory manual supplement. Minneapolis, MN: National
MILLON, T. (1985). The MCMI provides a good assessment of DSM-Ill disorders: The MCMI-I1 will prove
MILLON, T. (1987). Manual for the MCMI-II. Minneapolis: National Computer Systems. PRITCHARD, D. A., & ROSENBLATT, A. (1980). Racial bias in the MMPI: A methodological review. Journal
WIDIGER, T. A., WILLIAMS, J. B., SPITZER, R. L., & FRANCES, A. (1986). The MCMI and DSM-111: A brief
268-272.
Computer Systems.
even better. Journal of Personality Assessment, 49, 379-391.
of Consulting and Clinical Psychology, 48, 263-267.
rejoinder to Millon (1985). Journal of Personality Assessment, 50, 198-204.
MMPI DIFFERENCES FOR RENAL, PSYCHIATRIC, AND GENERAL MEDICAL PATIENTS
BRANDON DAVIS DAMON KRUG
Ball State University
RAYMOND S . DEAN
Ball State University and
Indiana University School of Medicine
BARRY A. HONG
Washington University School of Medicine
Renal failure has both medical and psychological implications. Indeed, various psychiatric problems related to end-stage renal disease have been reported in the literature; however, the focus has been on anxiety and depres- sion. While previous research has dealt with the comparisons of patients with renal failure, few studies have investigated the comparison of renal patients with psychiatric and general medical patients. The present study compared renal patients (N = 24) with a group of depressed psychiatric patients (N = 24) and a group of general medical patients (N = 24) on the MMPI. The results suggested that the renal group presented a psycho- logical profile that more closely resembled that of the depressed psychiatric group than that of patients with other chronic medical conditions.
This study was supported in part by grant IR15HD23154 from the National Institute of Child Health
Correspondence that concerns this article should be addressed to Brandon Davis, Neuropsychology and Human Development to R. S. Dean.
Laboratory, TC 517, Ball State University, Muncie, IN 47306.
MMPI DiTerences 179
It has been estimated that end-stage renal disease (ESRD) occurs at the rate of 20 per 100,OOO in the general population (Levy, 1981), and, although a number of ap- proaches exist, the treatment of choice is hemodialysis. However, hemodialysis patients suffer from numerous secondary physical and psychological conditions. Resulting in large part from the accumlation of toxins between dialysis runs, patients may develop hyper- thyroidism, hemolytic anemia, parathyroid disease, osteodystrophy, cardiovascular disorders, as well as a number of neurologic and psychiatric disorders (Bagdade, 1978; Glaser, 1974; Levy, 1981; Nadel& Wilson, 1979; Surman, 1981; Tyler, 1968). Psychiatric diagnosis of the ESRD patient often is complicated by the interaction of circulating toxins and an emotional response to a chronic disease.
Metabolic toxins clearly have been shown to lead to psychological disorders (Alfrey, 1976; Bergstrom & Furst, 1978; Harrison, 1979). Behavioral disturbances, including loss of memory, problems of concentration, lethargy, insomnia, and increased incidence of depression, have been reported as common psychological sequelae of ESRD (Surman, 198 1). While infrequently reported as such, psychotic reactions also have been observed as a psychiatric complication of ESRD and/or hemodialysis treatment (Steinman & Yager, 1978).
The incidence and nature of depression in dialysis patients continue to be signifi- cant concerns in treatment (Kutner, Fair, & Kutner, 1985). Although De-Nour (1982) has argued that depression and anxiety are characteristic of only a small percentage of dialysis patients, research with the MMPI suggests that the three neurotic scales of this measure (Hypochondrias, Depression, and Hysteria) frequently have characterized ESRD patients (Burke, 1979; Trieschmann & Sand, 1971; Ziarnik, Freeman, Sherrard, & Calsyn, 1977). However, much of this research has centered around a comparison of various renal subgroups and not as an aid to differential diagnosis of psychiatric problems.
Disparate results in the study of the psychological effects of ESRD are due in part to a lack of control for patients’ age and gender. For example, Moore (1976) reported that young males were less likely to have satisfactory acceptance of their diagnosed renal disease than were young females. Recent research also has suggested that the Psychopathic Deviate (PD) scale of the MMPI is higher for younger adults (19 years to 34 years) than older adults (35 years to 79 years) on hemodialysis (Gonsalves-Ebrahim, Sterin, Gulledge, Gipson, & Rodgers, 1987). These investigators also describe younger ESRD patients as reporting more somatic complaints than do older patients.
The present investigation examined the similarities and differences in psychological profiles for patients with ESRD and groups of chronic medical and depressed psychiatric patients while controlling for age and gender. Specifically, interest was directed to a comparison of profiles of the MMPI. Such comparisons were seen as important in understanding the underlying emotional frustrations of ESRD patients.
METHOD Subjects
The subjects were 72 patients (24 in each of the three groups) from a large university- affiliated medical center. Each subject in a Renal Group (Group 1) was matched for age ( f 3 years), and gender (12 males and 12 females in each group) with subjects in a Medical (Group 2) and a Depressed Psychiatric Group (Group 3). The 24 subjects in the ESRD Group had all been on a dialysis regimen for longer than 6 months and less than 2 years. Patients in the Psychiatric Group reported having had depressed symp- toms for more than 6 months and less than 2 years and met the criteria for primary affective disorders (DSM-111-R; American Psychiatric Association, 1987). Subjects in the Medical Group were patients with chronic disorders other than renal or psychiatric illnesses. Subjects were selected randomly from those patients who matched with renal patients. The three groups did not differ significantly (p < .05) in socioeconomic status (as determined by premorbid occupation) or chronological age.
180 Journal of Clinical Psychology, March 1990, Vol. 46, No. 2
Procedure Each subject completed the MMPI-Form R. The MMPI has been demonstrated
to have predictive validity with psychiatric inpatients (Graham, Smith, & Swartz, 1986; Heinrichs, 1964; Payne & Wiggins, 1972); normal populations (Bernstein, 1980; Fowler & Coyle, 1969; Lachar, Klinge, & Grisell, 1976); and diverse medical patients (Heinrichs, 1981; Heinrichs & Waters, 1972; Sobel& Warden, 1979). The MMPI also has been shown to have utility in the diagnosis and treatment of psychiatric disorders with ESRD pa- tients (Campbell & Sinha, 1983; Osberg, Meares, McKee, & Burnett, 1982; Willcockson, Bolton, & Dana, 1983; Ziarnik et al., 1977).
RESULTS An individual analysis of each patient’s MMPI protocol showed a valid administra-
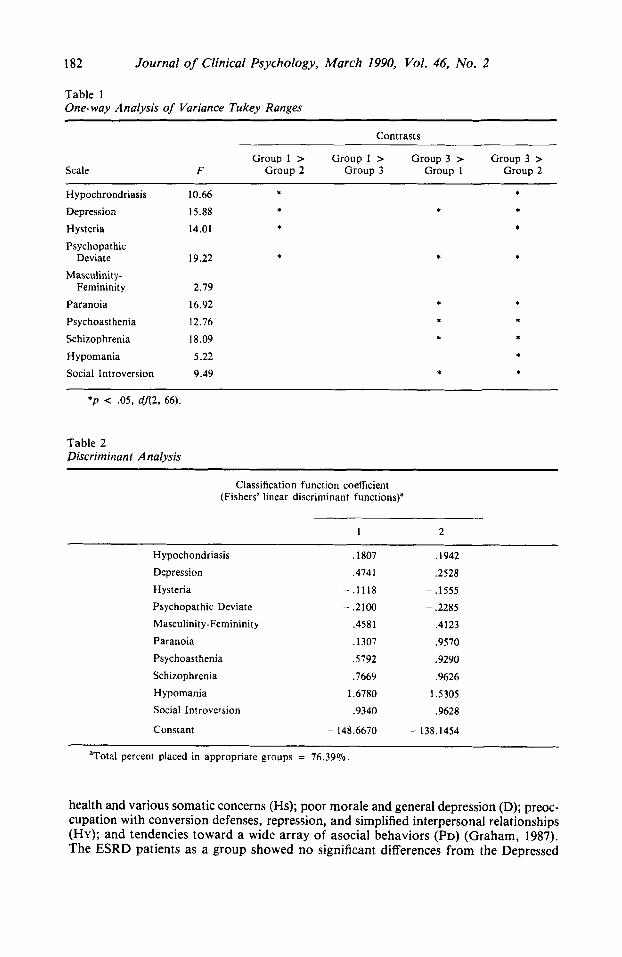
tion (as determined by scales L, F, and K). The MMPI raw scores were K corrected and transformed to standard scores in the normal fashion. The standard score means for each scale of the MMPI are presented by group in Figure 1 . Group differences on the 10 scales of the MMPI were tested in a one-way multivariate analysis of variance (MANOVA). This analysis showed a significant difference among groups on the MMPI, F(20, 120) = 5 . 1 3 , ~ < .001. This finding was simplified via univariate analysis followed by Tukey’s HSD for each significant finding. As shown in Table 1, the Depressed Psychiatric Group was significantly more elevated than the Medical Group on all measures except Masculinity-Femininity (MF) (p > .05), in which there were no significant differences among the three groups. Other contrasts showed the Renal Group to be significantly more elevated than the Medical Group on Hypochondriasis (Hs), Depres- sion (D), Hysteria (HY), and Psychopathic Deviate (PD) (p < .05) scales of the MMPI. However, there was no significant difference between the Renal Group and the Medical Group on Paranoia (PA), Psychasthenia (PT), Schizophrenia (Sc), Hypomania (MA), and Social Introversion (SI). In addition, the Renal Group was significantly less elevated than the Depressed Psychiatric Group on D, PD, PA, PT, Sc, and SI scales of the MMPI. Interestingly, the Renal Group and the Depressed Psychiatric Group were not significantly different on the Hs, HY, and MA scales.
In an attempt to examine the MMPI scales in a combination that would best characterize the three groups, a discriminant analysis that used Fisher’s linear discrimi- nant functions was performed. Two significant discriminant functions resulted, which significantly separated groups. The first disciminant function ( ’ [22] = 8 1.18, p < .001) accounted for some 64% of the variance, while the second, x [lo] = 21.04, p < .004, accounted for more than 36% of the variance. Group centroids for the two discrimi- nant functions were, respectively: Group 1 (Renal) .69, - .74; Group 2 (Medical) - 1.51, - .38; and, Group 3 (Psychiatric) 3 2 , 1.12. In sum, these two functions correctly placed more than 76% of the cases. The discriminant function coefficients for each MMPI scale are presented in Table 2.
The results from the discriminant analysis suggest that the three groups of patients could be characterized by their profiles on the MMPI. The first discriminant function, which seemed to discriminate between ESRD and other patients, showed the highest loadings on Depression (D), Psychopathic Deviate (PD), Masculinity/Femininity (MF), Paranoia (PA), Psychasthenia (PT), Schizophrenia (Sc), Hypomania (MA), and Social Introversion (SI).
3
DISCUSSION The results of the univariate analysis indicated that the renal patients in this study
were significantly different than the Medical Group. These differences were characterized on the part of the Renal Group by a preoccupation with bodily illnesses, denial of good

MMPI Diflerences 181
\ \ \ \
0 I I I
d I
I I
d \ \ \ \
\ 0
\ \ \
0
I 1 I I I I 1 I
182 Journal of Clinical Psychology, March 1990, Vol. 46, No. 2
Table 1 One-way Analysis of Variance Tukey Ranges
Contrasts
Scale Group 1 > Group 1 > Group 3 > Group 3 >
F Group 2 Group 3 Group 1 Group 2
Hypochrondriasis Depression Hysteria Psychopathic
Deviate Masculinity-
Femininity Paranoia Psychoasthenia Schizophrenia Hypomania Social Introversion
10.66 15.88 14.01
19.22
2.79
16.92 12.76
18.09
5.22 9.49
* * *
*
* *
* * * * * *
* * *
*P < .05, df2, 66).
Table 2 Discriminant Analysis
Classification function coefficient (Fishers' linear discriminant functions)"
~
1 2
Hypochondriasis .1807 .1942 Depression ,4741 ,2528 Hysteria -.1118 - .I555 Psychopathic Deviate - .2100 - ,2285 Masculinity-Femininity ,4581 ,4123 Paranoia ,1307 .9570 Psychoasthenia ,5792 .9290 Schizophrenia Hypomania Social Introversion
,7669 .9626 1.6780 1.5305 .9340 .9628
Constant - 148.6670 - 138.1454
"Total percent placed in appropriate groups = 76.39%.
health and various somatic concerns (Hs); poor morale and general depression (D); preoc- cupation with conversion defenses, repression, and simplified interpersonal relationships (HY); and tendencies toward a wide array of asocial behaviors (PD) (Graham, 1987). The ESRD patients as a group showed no significant differences from the Depressed
MMPI Diflereences 183
Group on the Hypochondriasis (Hs), Hysteria (HY), and Hypomania (MA) scales. This suggests that the Renal group may be suffering from a psychiatric disturbance similar to that of the depressed population.
In a previous study, Ziarnik et al. (1977) looked at the scales of the MMPI with three groups of renal patients who differed with respect to the length of survival time on dialysis. They found that the group of patients who failed to survive beyond 1 year had significantly higher scores on the same three scales that significantly separated the Renal Group from the Medical Group (Lea, HY, Hs, and D) in the present study. While we found that the Renal Group had significantly lower Depression (D) scores than did the Depressed Group, the Renal patients were, nevertheless, distinguished from the general medical patients on general issues of neuroticism and depression.
In 15 of 22 studies surveyed by Osberg et al. (1982), at least one, and generally two, of the scales of the neurotic triad (i.e., Hypochondriasis [Hs], Hysteria [HY], and Depression [D] scales) on the MMPI were found to be elevated for ESRD patients. In- deed, the profile of the hemodialysis patient appears to be one that reflects depression and a diminished ability to react to the stresses of the disorder. This, in fact, may be the case for patients in the present study in that there were no differences between the Renal and Depressed Groups on Hypochondriasis (Hs), Hysteria (HY), or Hypomania (MA) even when age, length of treatment, and sex were controlled. Kutner et al. (1985), in a study that employed three separate psychological measures, found that more than half of their ESRD patients manifested symptoms of depression; 50% of these fell within clinical levels. Further supporting evidence of renal patients with clinical levels of anxiety is suggested from the present data, in which Renal and Depressed Groups were similar on the Hypomania Scale (MA). This scale is said to reflect elevation of mood, accelerated speech, irritability, and brief periods of depression (Graham, 1987).
To consider the discriminant analysis in the present study, the greatest percentage (i.e., 59%) of misdiagnosis when the MMPI was used came between the Renal and Depressed Groups. This finding suggests that these two groups shared more aspects of emotional functioning with each other than they did with a group of medical patients. While our sample size necessitates some caution, the present research suggests that the ESRD patient should be expected to look much like the depressed psychiatric patient on the MMPI.
REFERENCES ALFREY, A. C. (1976). AMERICAN PSYCHMTRIC ASSOCIATION. (1987).
BAGDADE, J . D. (1978).
Dialysis encephalopathy syndrome. Annual Review of Medicine, 29, 93-98. Diagnostic and statistical manual of mental disorders (3rd
ed., rev.). Washington: Author. Hyperlipdemia and atherosclerosis in chronic dialysis patients. In W. Drukker, F.M.
Parsons, & J . F. Maher (Eds.), Replacement of renal function by dialysis (pp. 538-539). Boston: Martinus Nishoff Medical Division.
BERGSTROM, J . , & FURST, P . (1978). Uremic toxins. In W. Drukker, F. M. Parsons, & J . F. Maher (Eds.), Replacement of renal function by dialysis (pp. 334-368). Boston: Martinus Nischoff Medical Division.
BERNSTEIN, I . H. (1980). Security guards’ MMPI profiles: Some normative data. Journal ofPersonality Assess- ment, 44, 377-380.
BURKE, H . R . (1979). Renal patients and their MMPI profiles. Journal of Psychology, 101, 229-236. CAMPBELL, D. R. , & SINHA, B . K . (1983).
for the Advancement of Counselling, 6, 47-60. DE-NOUR, A. K . (1982).
patients. Journal of Psychosomalic Research, 26, 11-22. FOWLER, R . D. , & COYLE, F. A. (1969).
Clinical Psychology, 25, 62-63. GLASER, G. H. (1974).
Psychotherapy and chronic hemodialysis. International Journal
Psychological adjustment to illness scale (PAIS): A study of chronic hernodialysis
Collegiate normative data on MMPI content scales. Journal of
Brain dysfunction in uremia. In F. Plum (Ed.), Brain dysfunction in metabolicdisorders (pp. 173-197). New York: Raven Press.
184 Journal of Clinical Psychology, March 1990, Vol. 46, No. 2
GONSALVES-EBRAHIM, L., STERIN, G., GULLEDGE, A. D., GIPSON, W. T., & RODGERS, D. A. (1987).
GRAHAM, J. R. (1987). GRAHAM, J. R., SMITH, R. C., SWARTZ, G. F. (1986). Stability of MMPI configurations for psychiatric
HARRISON, H. E. (1979). Vitamin D, the parathyroid and the kidney. Johns Hopkins Medical Journal, 144,
HEINRICHS, T. F. (1964). Objective configural rules for discriminating MMPI profiles in a psychiatric popula- tion. Journal of Abnormal Psychology, 79, 1-8.
HEINRICHS, T. F. (1981). Using the MMPI in medical consultation. Clinical Notes on the MMPI No. 6. Minneapolis: National Computer Systems.
HEINRICHS, T. F., & WATERS, W. F. (1972). Psychological adjustment and response to open heart surgery: Some methodological considerations. British Journal of Psychiatry, 120, 491-496.
KUTNER, N. G., FAIR, P. L., & KUTNER, M. H. (1985). Assessing depression and anxiety in chronic dialysis patients. Journal of Psychosomatic Research, 29, 23-31.
LACHAR, D., KLINGE, V., & GRISELL, J. L. (1976). Relative accuracy of automated MMPI narratives generated from adult norms and adolescent norm profiles. Journal of Consulting and Clinical Psychology, 44. 20-24.
LEVY, N. B. (1981). Psychological reactions to machine dependency hemodialysis. Psychiatric Clinics of North America, 4, 351-363.
MOORE, G. L. (1976). Psychiatric aspects of chronic renal disease. Postgraduate Medicine, 60, 140-146. NADEL, A. M., Dialysis encephalopathy: A possible seizure disorder. Neurology,
OSBERC, J. W., MEARES, G. J., MCKEE, D. C., & BURNETT, G. B. (1982). The MMPI as a measure of the emotional correlates of chronic hemodialysis: A review. Journal of Personality Assessment, 46, 268-278.
PAYNE, F. D., & WIGGINS, J. S. (1972). MMPI profile types and the self-report of psychiatric patients. Jour- nal of Consulting and Clinical Psychology, 79, 1-8.
SOBEL, H. J., &WARDEN, W. (1979). The MMPI as a predictor of psychological adaptation to cancer. Journal of Consulting and Clinical Psychology, 47, 7 16-724.
STEINMAN, T. I., & YAGER, H. M. (1978). SUMAN, 0. S. (1981). Renal transplantation and the current treatment of end stage renal disease: A psychiatric
medicine perspective. In T. C. Manschreck (Ed.), Massachusetts General Hospital reviews for physicians (155-176). New York: Elsevier.
TRIESCHMANN, R. B., &SAND, R. L. (1971). WAIS and MMPI correlates of increasing renal failure in adult medical patients. Psychological Reports, 29, 1251-1262.
TYLER, R. H. (1968). Neurologic disorders in renal failure. American Journal of Medicine, 44, 734-748. WILLCOCKSON, J. C., BOLTON, B., DANA, R. H. (1983). A comparison of six MMPI short forms: Code type
ZIARNIK, J. P., FREEMAN, C. W., SHERRARD, D. J., & CALSYN, D. A. (1977). Psychological correlates of
Non- compliance in younger adults on hemodialysis. Psychosomatics, 28, 34-41.
The MMPI: A practical guide. New York: Oxford University Press.
inpatients. Journal of Consulting and Clinical Psychology, 54, 375-380.
180- 191.
WnsoN, W. P. (1979). 26, 1130-1 134.
Catatonia in uremia. Annual Intern Medicine, 89, 74-75.
correspondence and indices of psychopathology. Journal of Clinical Psychology, 39, 968-969.
survival on renal dialysis. Journal of Nervous and Mental Diseases, 164. 210-213.