models of rehabilitation research john whyte, md, phd moss rehabilitation research institute &...
TRANSCRIPT

MODELS OF REHABILITATION RESEARCH
John Whyte, MD, PhDMoss Rehabilitation Research Institute
&Thomas Jefferson University

The ICF & Related Models Body structure (disease) Body function (impairment) Activity (disability) Participation (handicap)

Biomedical Research Deals primarily with body structure &
function Assumes that functional ability is directly
related to resolution of body structure/ function abnormalities
What about….. Improvement in function w/o improvement in
pathology? Improvement in pathology w/o improvement
in function?

SustainedAttention
WorkingMemory
LanguageComprehen-
sionBalance
MotorCoordination
DiffuseAxonalInjury
ContusionSensori-neural
Hearing Loss
DiabeticNeuropathy
DrivingPublic
Speaking
ParentingEmploymentB
ody
Stru
ctu r
eB
ody
Func
tion
Act
ivit
yPa
rtic
ipat
ion
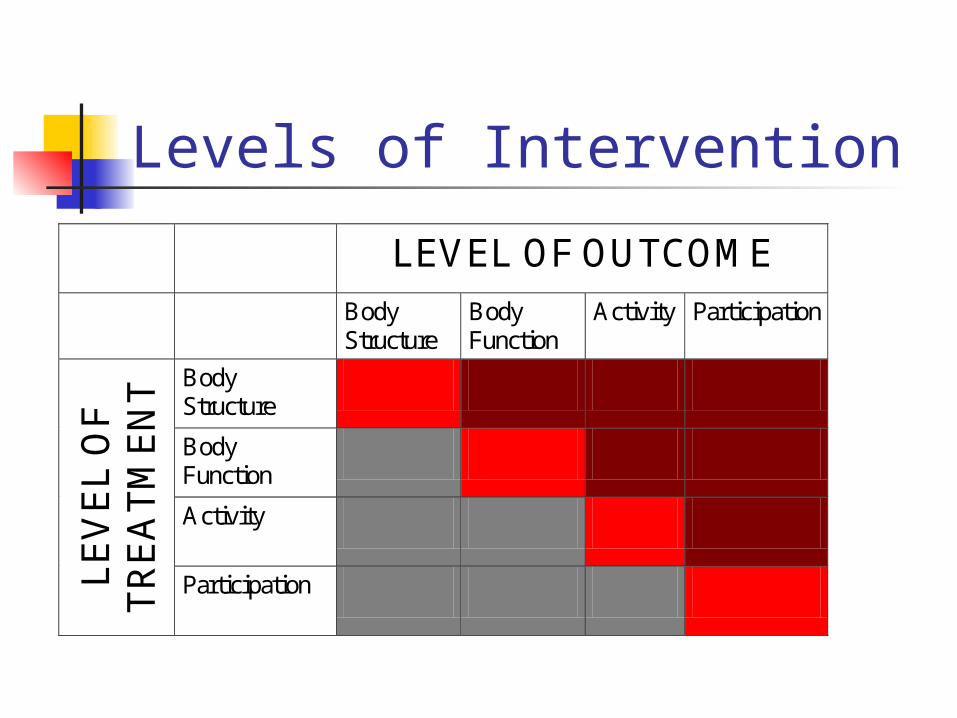
Levels of Intervention
LEVEL OF OUTCOME
Body Structure
Body Function
Activity Participation
Body Structure Body Function Activity
LE
VE
L O
F
TR
EA
TM
EN
T
Participation
Implications for Research Ideally, research should clarify the
causal links among levels in the enablement/disablement process
Most NIH-funded rehabilitation research to date stays primarily at one level (and mostly at body structure/function levels)
Distinction between enablement/ disablement research and rehabilitation research
2 Case Examples The effects of oral antispasticity
medications (Whyte & Robinson, 1990)
The effects of cognitive remediation (Carney, et al, 1999; Cicerone, et al, 2000)

Implications for Training Investigators will need to work in
interdisciplinary teams Having in-depth knowledge regarding a
level above or below the “target” level can be ideal
Researchers need to build quantitative and testable models of these interrelationships
Who mentors the linkages?
Using Theory In Rehabilitation Research Is there an overarching theoretical
framework for rehabilitation? What focused theories are useful
for focused domains? How can these theories be applied
specifically to treatment research?
Key Elements in Efficacy Study Design
Defining the appropriate study sample
Defining the “active ingredients” of treatment
Defining the study outcomes Determining the overall study design

What do we mean by “treatment theory”? A proposed specification of the
“active ingredients” of treatment A proposed specification of the
mechanism of action of those active ingredients

Why do we need a treatment theory? Many rehabilitation treatment
interventions are multifaceted and interactive – what elements or processes make a difference?
Candidate active ingredients are infinite; we need to constrain them for study
Results of theoretically-driven treatment studies not only provide an empirical result; they support theory development and refinement
Multifaceted Treatments May consist of a set of tasks and
activities delivered by specific disciplines in a particular dose or schedule and according to a particular protocol
Which of these are important determinants of treatment outcome?

Reducing the Infinite Given multifactorial treatments, how do
we select which aspects to “manualize” in defining the treatment of interest? The color of the walls? The gender of the therapist?
Theory, rightly or wrongly, points to the indispensable, defining aspects of the treatment
We always have at least covert theories
Theory Development An empirical comparison of 2 treatments
simply establishes that one is better than the other; it provides no guidance how the better treatment could be improved upon, or what components of it could be sacrificed without losing potency.
A theory-based comparison eliminates a whole family of unsuccessful treatments and provides a dimension along which the better treatment can be tuned (e.g., reaching training in motor-lesioned monkeys)

Treatment Theory Can Inform Other Aspects of Study Design
Selection of appropriate study participants
Selection of appropriate outcome measures
Selection of the optimal experimental design

Study Participants
Given the proposed mechanism of action, who can realistically benefit? Ability to understand and participate in
the critical aspects of treatment (e.g., learn to use an assistive device)
Requirement for preserved cognitive or motor capacities (e.g., ability to dorsiflex on command)
Requirement for social support (e.g., if treatment primarily targets family support skills, employer acceptance)

Study Participants (cont.) Choose participants that vary in the the
hypothesized “treatment responsive” characteristics to clarify the mechanism? individuals with and without declarative
memory deficits in a study of errorless learning
Individuals with different degrees of social support in a study of telephone care management
Characterizing the Participants Once selected, one must ask
whether the participants in different treatment groups are “comparable” – comparable in what way(s)? Balance achieved between randomized
groups Statistical adjustment of differences in
observational studies Need prior data on prognostic factors

Comparability & Adjustment Comparability and adjustment in
terms of prognosis on the outcome measures chosen (will discuss later)
Comparability and adjustment in terms of the characteristics that predict responsiveness to the treatment under study

Outcome Measures Given the proposed mechanism of
action of the treatment, where would you expect to see treatment impact? The most “proximal” impact (as
evidence for the proposed mechanism) A more “distal” impact (as evidence
that the change achieved has clinical meaning, ecological validity)
What other factors are likely to modify the chosen outcomes?
Outcome Measures (cont.) The same treatment may be
judged effective or ineffective, depending on the outcomes chosen, e.g. case examples mentioned earlier: Oral antispasticity medications Memory remediation treatments

Outcome Measures (cont.) Should a cognitive rehabilitation
intervention have impact on: Patterns of brain imaging associated
with specific tasks? Neuropsychological test scores? Real-world activities similar to those
used in treatment? Real-world activities different from
those used in treatment? Real-world activities, performed under
distraction?

Overall Study Design Does the proposed mechanism of action
suggest a permanent effect of intervention? (parallel group vs. crossover design)
Does the proposed mechanism of action suggest “localized” or “generalized” treatment impacts? (feasibility of multiple baseline across behaviors design; utility of multiple outcomes)

Study Design (cont.) Does the proposed treatment
capitalize on neurologic recovery (early vs. late enrollment)?
Are there important covariates that might affect treatment response that should be measured?
Summary Published rehabilitation research
frequently fails to clearly describe who should benefit from which treatment ingredients, with respect to what outcomes
Theory-based treatment research has many benefits, but among them is the ability to optimize the selection of participants, outcomes, and study design
Specifying the mechanism also leads the way toward conceptualizing interrelationships among treatment outcomes
Summary (cont.) ICF provides a “meta-theory” for all
treatment research, though this theory needs to be refined into a quantitative model.
ICF predicts where we will see impact of treatments that are effective but it doesn’t give us effective treatments.

Summary (cont.) Focused domain-specific theories
provide tools for implementing change at the organ, person, or societal level.
Only programmatic research can refine the interrelationships among measurement of patient characteristics, therapy ingredients, and meaningful outcomes.