monitoring bacterial resistance using selected … bacterial resistance using selected reaction...
TRANSCRIPT

Monitoring bacterial resistance using selected reaction monitoring
Anthony M. Haag*,1,2, Norbert K. Herzog1,3 and David W. Niesel1 1Department of Microbiology and Immunology, University of Texas Medical Branch, Galveston, TX 77555, USA 2Biomolecular Resource Facility, University of Texas Medical Branch, Galveston, TX 77555, USA 3Department of Medical Sciences, Quinnipiac University, Hamden, CT 06518, USA
Antibiotic resistance among pathogenic bacteria continues to be a major growing public health problem worldwide. It is well documented that the overuse of antibiotics also leads to new resistant strains, thus decreasing the effectiveness of “front line” antibiotics. Therefore, the detection of the antibiotics to which a bacterium is resistant is critical in designing an effective medical treatment plan and in minimizing the chances of increasing antibiotic resistance. Clinical treatment of an infection with ineffective antibiotics can lead to increased pathogen growth and spread, and cause serious medical complications and death. For this reason, clinical laboratories often determine the susceptibility of the bacterial isolate to a number of different antibiotics in order to establish the most effective antibiotic for treatment. Unfortunately, current clinical procedures for antimicrobial susceptibility assays remain based on time consuming culturing methods. Since antibiotic resistance often involves the chemical modification of an antibiotic to an inactive form by a bacterial enzyme, selected reaction monitoring (SRM) has the ability to quickly monitor and identify these chemical changes in an unprecedented time scale. Because SRM is highly selective and can identify chemical changes in a multitude of antibiotics, SRM has the ability to detect organisms that are resistant to one or more antibiotics in a single assay. The use of SRM greatly reduces the time it takes to determine the susceptibility or resistance of an organism to many antibiotics by eliminating the time consuming process of current culturing methods.
Keywords resistance detection; antibiotics; SRM
1. Antibiotic resistance
Antibiotic resistance among pathogenic bacteria is a major growing health problem [1,2]. The overuse of antibiotics and the adaptability of bacteria have created a growing number of resistant bacterial strains. This number has been continuously increasing [3-6]. In 2008, 25% of Salmonella and >12% of E. coli strains were resistant to three or more antibiotics and thus adding to the length of hospitalization and increases in morbidity and mortality [7,8]. In addition, there is increasing concern over “super bugs” that are resistant to multiple antibiotics. These Gram positive and Gram negative pathogens include methicillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile, Acinetobater calcoaceticus-baumanii complex and Pseudomonas sp. among others. It is clear that the overuse of antibiotics creates new resistant strains, thus decreasing the effectiveness of antibiotics [9]. Therefore, the detection of the antibiotics to which a bacterium is resistant is critical in designing an effective treatment plan and in minimizing the chances of increasing antibiotic resistance. Clinical treatment of an infection with ineffective antibiotics can lead to increased pathogen growth and spread, disruption of the protective “microbiome”, and cause serious medical complications including unnecessary amputation (particularly among wounded soldiers) and death. Nosocomial infections from antibiotic resistant bacteria are not only of major concern to local hospitals but also for military personnel at medical facilities in the US and as of a result of injuries in the Iraq and Afghanistan theaters [10-13]. Wound, skin, soft tissue, and systemic infections mediated by S. aureus and Gram negative pathogens (Klebsiella pneumonia, Pseudomonas sp. and Acinetobacter calcoaceticus-baumannii complex) represent serious concerns for soldiers injured on the battlefield. While S. aureus and Pseudomonas sp. wound and burn infections are well known, the CDC reports the increasing occurrence of multi-drug resistant A. baumannnii bacteremia at military hospitals and centers [14]. Also of concern is that A. baumannii is extremely resistant to drying and persists for long periods in the environment [15]. Multiple drug resistant A. baumannii is routinely recovered from US soldiers at military hospitals [16]. These infections are serious in that a large number of A. baumannii strains are reported to be resistant to β-lactam antibiotics, aminoglycosides, fluoroquinolones and chloramphenicols [17]. A. baumannii isolates are commonly co-treated with a β-lactamase inhibitor and a carbapenem, the drug of last resort [18,19]. The ability to rapidly determine the antibiotic resistance profile of A. baumannii and other commonly antibiotic-resistant bacteria will improve the treatment and clinical outcome of infected patients.
2. Antibiotic resistance mechanisms involving chemical modification
2.1. β-lactamase
β-lactam antibiotics have become the most common antibiotics in use today with half of all antibiotics belonging to the β-lactam class [20]. They consist of any antibiotic that contains a β-lactam ring within its molecular structure. This includes such antibiotics as penicillins, cephalosporins, monobactams, and carbapenems. All β-lactam antibiotics
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
535

exhibit their antibacterial action by binding to and inactivating penicillin binding protein (PBP). PBP is necessary for bacterial cell wall synthesis and inactivation by β-lactam antibiotics results in cell death. Although resistance can occur by other mechanisms in which the antibiotic is left intact, such as by changes in PBP, β-lactamase remains the most common mechanism bacteria use to become resistant to β-lactam antibiotics. Bacteria use a number of mechanisms to become resistant to β-lactam antibiotics. One of the most common mechanisms is via the expression of β-lactamase by the organism. β-lactamase hydrolyzes the β-lactam ring of the antibiotic via ring opening (Figure 1). The resulting hydrolyzed antibiotic is unable to bind to PBP and therefore has no antimicrobial activity. In order to overcome the hydrolyzing effects of β-lactamase, inhibitors such as clavulanic acid and sulbactam, have been developed in order to inhibit the hydrolysis of β-lactam antibiotics. Later generation antibiotics have also been developed in an attempt to prevent the hydrolytic action of β-lactamases.
β-lactamase
Fig. 1 β-lactam antibiotics, such as cephalosporins, are hydrolyzed by the enzyme β-lactamase. This causes ring opening of the antibiotic. The hydrolyzed antibiotic has no antibacterial activity.
2.2. Chloramphenicol acetyltransferase
First isolated and characterized in 1947, chloramphenicol was one of the first antibiotics to be used clinically [21]. Since then several different analogs of chloramphenicol have been synthesized including thiamphenicol, florfenicol and azidamphenicol. Chloramphenicol has since fallen out of favor because of its potential to cause aplastic anemia, an often fatal bone marrow disease [22]. However, the drug is still used in many countries to treat a variety of different bacterial infections due to the low cost of the drug and its ease of manufacture [23]. Bacterial resistance to chloramphenicol arose as early as the 1950s [24]. This resistance results from the acetylation of the hydroxyl moieties of chloramphenicol via chloramphenicol acetyl transferase, which thereby prevents the binding of chloramphenicol to the bacterial ribosomes [25]. The acetylation of chloramphenicol occurs in a three-step process (Figure 2). First, chloramphenicol acetyl transferase acetylates the C-3 hydroxyl group to form 3-O-acetylchloramphenicol. Second, a non-enzymatic rearrangement then occurs whereby the acetyl group shifts to the C-1 hydroxyl group. Third, the C-3 hydroxyl moiety is then acetylated to form the compound 1,3-O-O-diacetyl chloramphenicol. Neither the monoacetylated nor diacetylated form of chloramphenicol exhibit antibacterial activity [26].
2.3. Other modifying enzymes
A number of other chemically modifying enzymes are used by bacteria in order to confer antibiotic resistance. Erythromycin esterase has been observed in E. coli which hydrolyzes the lactam ring of erythromycin [27]. The enzyme aminoglycoside acetyltransferase has been observed in E. coli and is known to acetylate the piperazine ring of the fluoroquinolone drug ciprofloxacin [28]. This enzyme is also known to acetylate kanamycin, an aminoglycoside antibiotic [29]. The plasmid pBR4, originally found on B. fragilis, confers resistance to tetracycline when the organism is grown anerobically [30]. The resistance mechanism was determined to be by chemical modification of tetracycline as opposed to efflux pumps which bacteria typically use to become resistant to tetracycline.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
536

non-enzymaticrearrangement
chloramphenicolacetyltransferase
chloramphenicolacetyltransferase
NH
Cl
Cl
O
O HO H O H O O
NH
O
Cl
Cl
O H
NH
O
Cl
Cl
OOOO
NH
O
Cl
Cl
OO
O2N O2N
CH3
O2N
CH3CH3
O2N
CH3
3. Selected reaction monitoring
3.1. Description
Selected Reaction Monitoring (SRM) is a mass spectrometric technique that allows one to selectively monitor and quantitate one or more compounds in a complex mixture. Triple quadrupole mass spectrometers are often used to accomplish this due to their mass filtering capabilities. The technique dates back more than 30 years as a way to quantitate small molecule compounds [31]. In SRM, ions are introduced into the mass spectrometer and the first quadrupole selects ions of a particular mass-to-charge ratio (m/z), known as the precursor ion, while excluding all others. The second quadrupole then acts as a collision cell to fragment the selected precursor ion by collision-induced dissociation. Finally, the third quadrupole selects a particular product ion indicative to the compound of interest (Figure 3).
Fig. 3 Ions of different m/z values (masses) are introduced into quadrupole mass filter Q1. Q1 selects ions of a specific m/z and passes them to the collision cell Q2. Ions are fragmented and product ions of a specific m/z are passed through and allowed to exit quandrupole Q3. Exiting ions are counted with respect to time and an ion chromatogram is generated. The selected product ion is monitored over time to yield a trace of ion intensity versus time. The intensity of the monitored ions is proportional to the concentration of the compound of interest. A linear regression is performed from sample standards of known concentration. Because the mass spectrometer is often used as the detector from an HPLC system, the chromatographic trace yields a chromatographic trace of retention time of the compound of interest and its concentration. Several compounds can be monitored simultaneously by continuously cycling through different transitions (precursor/product ion pairs) and monitoring the ion count for each pair over time. The selectivity of this method allows the exclusion of co-eluting compounds. Because this is a non-scanning technique and only specific ions of interest are monitored, the technique translates into high sensitivity for the compounds of interest. The linear response of this technique is over 5 orders of magnitude [32].
3.2. SRM of antibiotics
Quantitating antibiotics by SRM has been previously reported. SRM has been used to monitor the level of β-lactam antibiotics in kidney tissue [33,34]. It has also been used to determine the amount of tetracycline and penicillin in
Fig. 2 Acetylation of chloramphenicol occurs via the enzyme chloramphenicol acetyltransferase by first acetylating the C-3 hydroxyl moiety to form 3-O-acetylchloramphenicol. A non-enzymatic rearrangement then shifts the acetyl group to the C-1 hydroxyl moiety to form 1-O-acetylchloramphenicol. Finally, the C-3 hydroxyl moiety is again acetylated by chloramphenicol acetyltransferase to form 1,3-O,O-diacetylchloramphenicol. Both monoacetylated and diacetylated chloramphenicol exhibit no antibacterial activity.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
537
animal tissue and food products [35, 36]. Because of the concern of a build-up of pharmaceutical drugs in the environment, SRM has been used as a method to detect low levels of antibiotics in wastewater and soils [37, 38].
4. Detecting antibiotic resistance by SRM
4.1. Monitoring resistance to ampicillin and chloramphenicol
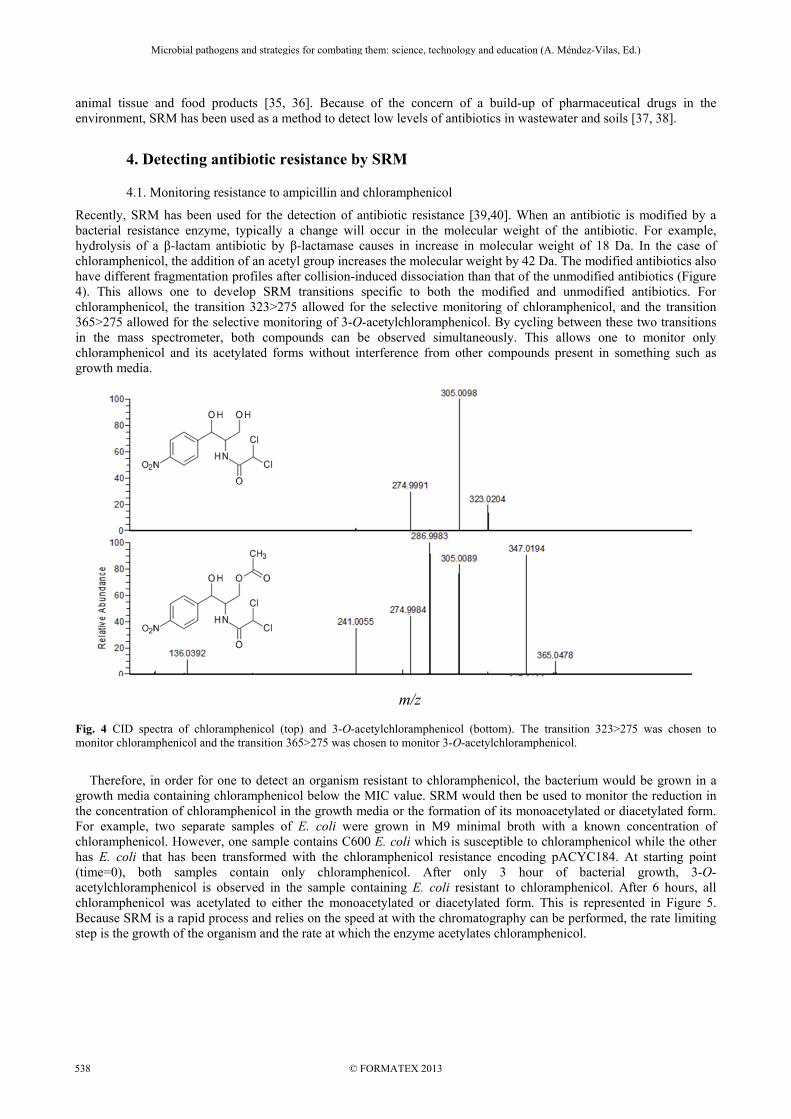
Recently, SRM has been used for the detection of antibiotic resistance [39,40]. When an antibiotic is modified by a bacterial resistance enzyme, typically a change will occur in the molecular weight of the antibiotic. For example, hydrolysis of a β-lactam antibiotic by β-lactamase causes in increase in molecular weight of 18 Da. In the case of chloramphenicol, the addition of an acetyl group increases the molecular weight by 42 Da. The modified antibiotics also have different fragmentation profiles after collision-induced dissociation than that of the unmodified antibiotics (Figure 4). This allows one to develop SRM transitions specific to both the modified and unmodified antibiotics. For chloramphenicol, the transition 323>275 allowed for the selective monitoring of chloramphenicol, and the transition 365>275 allowed for the selective monitoring of 3-O-acetylchloramphenicol. By cycling between these two transitions in the mass spectrometer, both compounds can be observed simultaneously. This allows one to monitor only chloramphenicol and its acetylated forms without interference from other compounds present in something such as growth media.
Fig. 4 CID spectra of chloramphenicol (top) and 3-O-acetylchloramphenicol (bottom). The transition 323>275 was chosen to monitor chloramphenicol and the transition 365>275 was chosen to monitor 3-O-acetylchloramphenicol.
Therefore, in order for one to detect an organism resistant to chloramphenicol, the bacterium would be grown in a growth media containing chloramphenicol below the MIC value. SRM would then be used to monitor the reduction in the concentration of chloramphenicol in the growth media or the formation of its monoacetylated or diacetylated form. For example, two separate samples of E. coli were grown in M9 minimal broth with a known concentration of chloramphenicol. However, one sample contains C600 E. coli which is susceptible to chloramphenicol while the other has E. coli that has been transformed with the chloramphenicol resistance encoding pACYC184. At starting point (time=0), both samples contain only chloramphenicol. After only 3 hour of bacterial growth, 3-O-acetylchloramphenicol is observed in the sample containing E. coli resistant to chloramphenicol. After 6 hours, all chloramphenicol was acetylated to either the monoacetylated or diacetylated form. This is represented in Figure 5. Because SRM is a rapid process and relies on the speed at with the chromatography can be performed, the rate limiting step is the growth of the organism and the rate at which the enzyme acetylates chloramphenicol.
m/z
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
538

a) b)
Fig. 5 SRM spectra of media containing chloramphenicol and analyzed at different times during bacterial growth. In both samples, chloramphenicol is observed at a retention time of 12 min (time=0). Chloramphenicol resistant E. coli in a) acetylated chloramphenicol after 3 hrs (peak at 14 min). After 6 hrs of growth, nearly all of the chloramphenicol has been depleted with nearly all of it having been acetylated. Susceptible E. coli in b) did not convert chloramphenicol to its acetylated form at any time period.
Because β-lactamase can hydrolyze β-lactam susceptible antibiotics at an extremely fast rate, only a small amount of bacterial growth is needed to express enough β-lactamase to quickly hydrolyze the susceptible antibiotic. When E. coli containing the ampicillin resistance encoding plasmid-pUC18 is grown in a broth containing ampicillin, antibiotic resistance can be easily observed after only 1 hour of growth. This is illustrated in figure 6.
a) b)
Fig. 6 SRM of media containing ampicillin analyzed at different times during bacterial growth. In both samples, ampicillin is observed at a retention time of 14 min (time=0). Ampicillin resistant E. coli in a) completely hydrolyze ampicillin after 1 hr. However, no hydrolysis of ampicillin was observed in b) when ampicillin susceptible E. coli are grown for 1hr.
4.2. Monitoring the effects of β-lactamase on multiple antibiotics in a single assay
Because SRM has the ability to monitor chemical changes in a variety of different antibiotics simultaneously, they can also be monitored in a single assay. Often a β-lactamase has the ability to hydrolyze a variety of different β-lactam antibiotics. Later generation β-lactam antibiotics are often more resistant to hydrolysis. To determine which antibiotics a particular β-lactamase will hydrolyze, multiple antibiotics can be screened in a single SRM assay. Observing the disappearance of an antibiotic in an SRM trace indicates that the antibiotic has been modified. For example, a well characterized β-lactamase from B. cereus is known to hydrolyze first generation penicillins such as ampicillin and nafcillin. However, second generation penicillins such as cloxacillin are known to resist the hydrolyzing effects of this enzyme. Figure 7 shows the effect of the B. cereus β-lactamase when incubated for 2 hrs with these three antibiotics.
0.0
1.0e+5
2.0e+5
3.0e+5
4.0e+5
10 12 14 16 18 20
0
3
6
Ion
inte
nsity
(cou
nts/
sec)
HPLC retention time (min)G
row
th ti
me
(hrs
)
0
1e+5
2e+5
3e+5
4e+5
10 12 14 16 18 20
0
3
6
Ion
inte
nsity
(cou
nts/
sec)
HPLC retention time (min)
Gro
wth
tim
e (h
rs)
0.0
2.0e+3
4.0e+3
6.0e+3
8.0e+3
1.0e+4
1.2e+4
1.4e+4
10 12 14 16 18 20
0.0
1.0
Ion
inte
nsity
(cou
nts/
sec)
HPLC retention time (min)
Gro
wth
tim
e (h
rs)
0.0
2.0e+3
4.0e+3
6.0e+3
8.0e+3
1.0e+4
1.2e+4
1.4e+4
10 12 14 16 18 20
0.0
1.0
Ion
inte
nsity
(cou
nts/
sec)
HPLC retention time (min)
Gro
wth
tim
e (h
rs)
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
539

a) b)
Fig. 7 SRM of media containing the antibiotics ampicillin, cloxacillin, and nafcillin. a) All three antibiotics are observed in media prior to exposure to a β-lactamase. b) Only cloxacillin remains unhydrolyzed after exposure to a β-lactamase from B. cereus.
4.3. Advantages of SRM compared to other analytical techniques to monitor antibiotic resistance.
A rapid colorimetric assay for determining whether an organism produces β-lactamase was developed over twenty years ago [41]. However, this assay only determines whether an organism expresses β-lactamase. Because many later generation cephalosporins are stable to certain β-lactamases, the assay does not provide any information as to which generation of cephalosporins the enzyme will hydrolyze. With this in mind, it is important to have an assay that can determine which antibiotic a specific β-lactamase will hydrolyze. Also, the assay only measures a single chemical pathway, in this case hydrolysis of certain β-lactams, and does not detect other chemical modification pathways such as acetylation, methylation, etc., that a bacterium may use to overcome antibiotic activity. Therefore, a method such as SRM that incorporates a single assay to monitor many chemical modification pathways simultaneously could greatly reduce the time, cost and complexity of antibiotic resistance testing. Current methods to determine the susceptibility or resistance of bacteria to a particular antibiotic typically involves isolating the organism from an individual specimen (blood, spinal fluid, tissue, etc.). The isolated bacteria is then grown on culture media. Two methods for analyzing antibiotic resistance, Kirby-Bauer and the Minimal Inhibitory concentration (MIC) dilution method, are usually employed. Kirby Bauer is a qualitative method whereby the bacteria to be tested is inoculated over the entire surface of an agar plate followed by the placement of a disk containing a standardized concentration of antibiotic. Susceptibility is determined from a standardized range of the resulting diameter of inhibition of bacterial growth around the disk. The MIC dilution method is a quantitative method whereby the lowest concentration of an antibiotic that inhibits visible growth of a microorganism is determined. Although these two methods are effective, susceptibility testing is slow, often requiring days to perform [42]. Because of this delay, a physician may treat the patient with antibiotics until the susceptibility results are known. Unfortunately, treating with an ineffective antibiotic may not only compromise the health of the patient but can contribute to the selection of antibiotic resistant organisms [43]. Also, a broader spectrum antibiotic may be used instead of a more specific one. Therefore, methods to determine the organism’s susceptibility to a variety of antibiotics in as short of a time span as possible prevents the development of resistance and can also increase the patient survival rate.
5. Conclusions
SRM allows the direct detection of antibiotic resistance by observing the presence of a known chemically modified form of each antibiotic. However, observing the decrease in the concentration of any antibiotic is enough to determine that the organism may be resistant to that antibiotic. This would be advantageous if a new and unknown chemical modification pathway is developed by the organism to a given antibiotic. Current susceptibility testing only allows a single antibiotic to be screened in a single assay. This requires multiple assays to be performed in parallel to maximize the number of antibiotics that can be screened and thus becomes a time consuming process. Because of the fast duty cycle of current mass spectrometers, SRM can screen multiple antibiotics in a single assay. SRM has already been reported to be capable of screening dozens of pharmaceutical compounds in the environment simultaneously. Also, because bacterial resistance is determined by observing the presence or absence of an antibiotic in the SRM spectrum, one can determine in a single assay not only which antibiotics an organism is resistant to but also which antibiotics are effective.
HPLC retention time (min)
5 10 15 20 25
Ion
inte
nsity
(cou
nts/
sec)
0.0
2.0e+5
4.0e+5
6.0e+5
8.0e+5
1.0e+6
1.2e+6
ampicillincloxacillinnafcillin
HPLC retention time
5 10 15 20 25
Ion
inte
nsity
(cou
nts/
sec)
0.0
2.0e+5
4.0e+5
6.0e+5
8.0e+5
1.0e+6
1.2e+6
ampicillincloxacillinnafcillin
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
540

Current software allows the data acquisition computer to make data dependant decisions as to the state of all antibiotics in the assay. This process can easily be developed commercially using kits. Collection vials would contain both growth media and a number of different antibiotics. After incubation of a microbe with sub-inhibitory levels of antibiotics in the collection vials, analysis by SRM would be performed and a report generated by the software. Similar technology is already in use for the identification and quantification of steroids in athletes and the detection of drugs of abuse in serum and urine by law enforcement. The application of SRM also has advantages of sensitivity. The sample size needed per injection can be as small as 1µL. For this reason, small quantities of biological samples can be analyzed. A sample containing only a few organisms may be sufficient to detect antibiotic resistance. This is highly advantageous when only a small amount of biological sample is available or if only small amounts of bacteria are present in the medical sample. Another benefit of this improved sensitivity of SRM is that the organism can be grown in a broth with an antibiotic concentration far below the MIC. This allows for the organisms to be unaffected by the antibiotics during their growth stage. The organism will continue to chemically modify those antibiotics that it is resistant to while leaving intact those that it is susceptible to. Unfortunately, performing an SRM analysis does require an experienced user. Manufacturers of mass spectrometry equipment have taken great steps in recent years in developing a simplified interface for the equipment and software. The initial cost of a mass spectrometer required for SRM analysis would eventually be offset by alleviating the need for the other chemical protocols.
References [1] Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA, Fridkin SK. Antimicrobial-resistant pathogens associated
with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the CDC, 2006-2007. Inf. Con. Hosp. Epidem. 2008;29:996-1011.
[2] Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial Bloodstream Infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Inf. Dis. 2004;39:309-317.
[3] Hujer KM, Hujer AM, Hulten EA, Bajaksouzian S, Adams JM, Donskey CJ, Ecker DJ, Massire C, Eshoo MW, Sampath R, Thomson JM, Rather PN, Craft DW, Fishbain JT, Ewell AJ, Jacobs MR, Paterson DL, Bonomo RA. Analysis of antibiotic resistance genes in multidrug-resistant Acinetobacter sp. Isolates from military and civilian patients treated at the Walther Reed Army Medical Center. Antimicrob Agents Chemother. 2006;50(12):4114-4123.
[4] Keen III EF, Robinson BJ, Hospenthal DR, Aldous WK, Wolf SE, Chung KK, Murray CK. Prevalence of multidrug-resistant organisms recovered at a military burn center. Burns. 2010;36(6):818-825.
[5] Rahal JJ. Novel Antibiotic combinations against infections with almost completely resistant Pseudomonas aeruginosa and Acinetobacter species. Clin. Infect. Dis. 43;S2:S95-S99.
[6] Ressner RA, Murray CK, Griffith ME, Rasnake MS, Hospenthal DR, Wolf SE. Outcomes of bacteremia in burn patients involved in combat operations overseas. J. Am. Coll. Surg. 2008;206:439-444.
[7] Cohen ML. Epidemiology of drug resistance: implications for a post-antimicrobial era. Science. 1992;257:1050-1055. [8] Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in the United
States hospitals: a three-year analysis. Clin. Infect. Dis. 1999;29(2):239-244. [9] Belongia EA, Schwartz B. Strategies for promoting judicious use of antibiotics by doctors and patients. BMJ. 1988;317:668-
671. [10] Braun L, Craft, D, Williams R, Tuamokumo F, Ottolini M. Increasing clindamycin resistance among methicillin-resistant
Staphylococcus aureus in 57 Northeast United States military treatment facilities. Ped. Infect. Dis. J. 2005;24:622-626. [11] Centers for Disease Control and Prevention (CDC). Acinetobacter baumannii infections among patients at military medical
facilities treating injured U.S. service members, 2002-2004. MMWR Morb. Mortal. Wkly. Rep. 2004;53(45):1063-1066. [12] Ellis MW, Hospenthal DR, Dooley DP, Gray PJ, Murray CK. Natural history of community-acquired methicillin-resistant
Staphylococcus aureus colonization and infection in soldiers. Clin. Infect. Dis. 2004;39(7):971-979. [13] Petersen K, Cannegieter SC, van der Reijden TJ, van Strijen B, You DM, Babel BS, Philip AI, Dijkshoorn L. Diversity and
clinical impact of Acinetobacter baumannii colonization and infection at a military medical center. J. Clin. Microbiol. 2011;49(1):159-166.
[14] Posluszny JA Jr, Conrad P, Halerz M, Shankar R, Gamelli RL. Surgical burn wound infections and their clinical implications. J. Burn Care Res. 2011;32(3);324-333.
[15] Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin. Micro. Rev. 2008;21:538-582.
[16] Davis KA, Moran KA, McAllister CK, Gray PJ. Multidrug-resistant Acinetobacter extremity infections in soldiers. Emerg. Infect. Dis. 2005;11(8):1218-1224.
[17] Perez F, Hujer AM, Hujer KM, Decker BK, Rather PN, Bonomo RA. Global Challenge of multidrug-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2007;51(10):3471-3484.
[18] Kiffer CR, Sampaio JL, Sinto S, Oplustil CP, Koga PC, Arrunda AC, Turner PJ, Mendes C. In-vitro synergy test of meropenem and sulbactam against clinical isolates of Acinetobacter baumannii. Diagn. Microbiol Infect. Dis. 2005;52(4):317-322.
[19] Choi JY, Park YS, Cho CH, Park YS, Shin SY, Song YG, Yong D, Lee K, Kim JM. Synergic in-vitro activity of imipenem and sulbactam against Acenitobacter baumannii. Clin Microbiol. Infect. 2004;10(12);1098-1101.
[20] Elander RP. Indusrtrial production of β-lactam antibiotics. Appl. Microbiol. Biotechnol. 2003;61:385-392. [21] Rebstock MC, Crooks HM, Controulis J, Bartz QR. Chloramphenicol (chloromycetin). IV. chemical studies. J. Am. Chem. Soc.
1949;71:2458-2462.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
541
[22] Rich M, Ritterhoff R, Hoffmann R. A fatal case of aplastic anemia following chloramphenicol (chloromycetin) therapy. Annals of Internal Medicine. 1950;33(6):1459–1467.
[23] Pécoul B, Chirac P, Trouiller P, Pinel J. Access to essential drugs in poor countries a lost battle? JAMA. 1999;281(4):361-367. [24] Watanabe T. Ineffective heredity of multiple drug resistance in bacteria. Bacteriol. Rev. 1963;27:87-115. [25] Shaw WV, Leslie AGW. Chloramphenicol acetyltransferase. Annu. Rev. Biophys. Biophys. Chem. 1991;20:363-386. [26] Pongs O. Chloramphenicol. Chemical formula and history of discovery. In: Hahn FE. eds. Mechanism of action of antibacterial
agents. City: Springer-Verlag, Berlin Heidelberg; 1979:26-42. [27] Barthélémy P, Autissier D, Gerbaud G, Courvalin P. Enzymic Hydrolysis of Erythromycin by a Strain of Escherichia coli. J.
Antibiot. 1984;37:1692-1696. [28] Robicsek A, Strahilevitz J, Jacoby GA, Macielag M, Abbanat D, Park CH, Bush K, Hooper DC. Fluoroquinolone-Modifying
Enzyme: A New Adaptation of a Common Aminoglycoside Acetyltransferase. Nat. Med. 2006;12;83-88. [29] Le Goffic F, Martel A. Resistance to aminosides induced by an isoenzyme, kanamycin acetyltransferase. Biochimie.
1974;56:893-897. [30] Speer BS, Salyers AA. Novel aerobic tetracycline resistance gene that chemically modifies tetracycline. J. Bacteriol.
1989;171(1):148-153. [31] Baty JD, Robinson PR. Single and multiple ion recording techniques for the analysis of diphenylhydantoin and its major
metabolite in plasma. Biomed. Mass Spectrom. 1977;4:36-41. [32] Lange V, Picotti P, Domon B, Aebersold R. Selected reaction monitoring for quantitative proteomics: a tutorial. Mol. Syst. Biol.
2008;4:1-14. [33] Viberg A, Sandström M, Jansson B. Determination of cefuroxime in human serum or plasma by liquid chromatography with
electrospray tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2004;18:707-710. [34] Fagerquist CK, Lightfield AR. Confirmatory analysis of β-lactam antibiotics in kidney tissue by liquid
chromatography/electrospray ionization selective reaction monitoring ion trap mass spectrometry. Rapid Commun. Mass Spectrom. 2003;17:660-671.
[35] Goto T, Ito Y, Yamada S, Matsumoto H, oka H. High-throughput analysis of tetracycline and penicillin antibiotics in animal tissues using electrospray tandem mass spectrometry with selected reaction monitoring transition. J. Chromatogr. A. 2005;1100:193-199.
[36] Nakazawa H, Ino S, Kato K, Watanabe T, Ito Y, Oka H. Simultaneous determination of residual tetracyclines in foods by high-performance liquid chromatography with atmospheric pressure chemical ionization tandem mass spectrometry. J. Chromatogr. B. 1999;732:55-64.
[37] Martínez-Carballo E, González-Barreiro C, Scharf S, Gans O. Environmental monitoring study of selected veterinary antibiotics in animal manure and soils in Austria. Environ. Pollut. 2007;148:570-579.
[37] Pozo OJ, Guerrero JV, Sancho JV, Ibáñez M, Pitarch E, Hogendoorn E, Hernández F. Effiecient approach for the reliable quantification and confirmation of antibiotics in water using on-line solid-phase extraction liquid chromatography/tandem mass spectrometry. J. Chromatogr. A. 2006;1103:83-93.
[39] Haag AM, Medina AM, Royall AE, Herzog NK, Niesel DW. Monitoring bacterial resistance to chloramphenicol and other antibiotics by liquid chrmoatography electrospray ionization tandem mass spectrometry using selected reaction monitoring. J. Mass Spectrom. 2013; 48(6):732-739.
[40] Grundt A, Findesin P, Miethke T, Jäger E, Ahmad-Nejad P, Neumaier M. Rapid detection of ampicillin resistance in Escherichia coli by quantitative mass spectrometry. J. Clin. Microbiol. 2022;50(5):1727-1729.
[41] Cohenford MA, Abraham J, Medeiros AA. A Colorimetric Procedure for Measuring β-Lactamase Activity. Anal. Biochem. 1988;168:252-258.
[42] Bauer AW, Kirby WMM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966;36:493-496.
[43] Counts GW. Review and Control of Antimicrobial Usage in Hospitalized Patients. JAMA. 1977;238:2170-2172.
Microbial pathogens and strategies for combating them: science, technology and education (A. Méndez-Vilas, Ed.)
© FORMATEX 2013
____________________________________________________________________________________________
542