morphological patterns of gestational …
TRANSCRIPT
i
MORPHOLOGICAL PATTERNS OF GESTATIONAL
TROPHOBLASTIC DISEASES AT THE JOS UNIVERSITY TEACHING
HOSPITAL; A RETROSPECTIVE STUDY BETWEEN 2004 AND 2013.
A DISSERTATION SUBMITTED TO THE NATIONAL
POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PARTIAL
FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE
PART TWO (FINAL) FELLOWSHIP OF THE COLLEGE IN
PATHOLOGY
BY
DR. AKPOR ISAAC ONAH,
HISTOPATHOLOGY DEPARTMENT, JOS UNIVERSITY TEACHING
HOSPITAL, JOS, NIGERIA
MAY 2016.

ii
CERTIFICATION
We hereby certify that, this dissertation was written by Dr. Akpor Isaac Onah at the Jos
University Teaching Hospital, Jos and supervised by us
1. Prof. Barnabas Mafala Mandong, MBBS, FMCPath
Consultant Pathologist,
Jos University Teaching Hospital,
Sign……………………………………
2. Dr. Madachi Dauda Ayuba, MBBS, FMCPath
Consultant Pathologist,
Jos University Teaching Hospital,
Sign……………………………………

iii
ATTESTATION
I hereby attest that this dissertation project was carried out by
DR AKPOR ISAAC ONAH
At the Histopathology Department of the
Jos University Teaching Hospital,
Jos.
__________________________________________________
DR MADACHI DAUDA AYUBA, FMCPath
HEAD OF DEPARTMENT
HISTOPATHOLOGY UNIT
JOS UNIVERSITY TEACHING HOSPITAL,
JOS

iv
DECLARATION
I hereby declare that this dissertation is an original work and it is the product of my personal
effort, and that this work has not been presented in part or whole, to any institution for a degree
or certificate nor has it been published in any form.
Dr Akpor Isaac Onah
Signature………………………. Date……………………….

v
TABLE OF CONTENTS
Title Page - - - - - - - - - - i
Certification - - - - - - - - - ii
Attestation- - - - - - - - - - iii
Declaration - - - - - - - - - iv
Table of Contents - - - - - - - - v
Dedication- - - - - - - - - - vii
Acknowledgement - - - - - - - - viii
List of Abbreviations used- - - - - - - - ix
List of Tables- - - - - - - - - - x
List of Figures- - - - - - - - - xi
Abstract- - - - - - - - - - xii
1.0 Chapter One:
Introduction - - - - - - - - 1
Aim- - - - - - - - - - 3
Objectives- - - - - - - - - 4
2.0 Chapter Two: Literature Review
Background- - - - - - - - - 5
Classification of patterns of Gestational Trophoblastic Diseases - 5
Pathology- - - - - - - - - 5
Complete Hydatidiform Mole - - - - - - 6
Partial Hydatidiform Mole- - - - - - - 6
Invasive Mole- - - - - - - - 7
Choriocarcinoma- - - - - - - - 7
Placental-Site Trophoblastic Tumour (PSTT)- - - - 8
Epithelioid Trophoblastic Tumour (ETT)- - - - - 8
Epidemiology of Gestational Trophoblastic Diseases - - 8
Distribution- - - - - - - - - 8
Determinants- - - - - - - - - 13
Deterrents- - - - - - - - - 15
Treatment Outcomes- - - - - - - - 16
3.0 Chapter Three: Materials and Method- - - - - - 18
4.0 Chapter Four: Results - - - - - - - 22

vi
5.0 Chapter Five: Discussion- - - - - - - - 34
6.0 References- - - - - - - - - 43
7.0 Appendix A: The Modified WHO Classification of Gestational
Trophoblastic Diseases (2002)- - - - - - - 49
8.0 Appendix B: Ethical clearance- - - - - - - 50

vii
DEDICATION
To our Source, The Almighty and Giver of opportunities to all souls, and to the souls who
desire to, and have chosen to make room for continuous improvement in our noble discipline
and in all realms of life.

viii
ACKNOWLEDGEMENT
By no means exhaustive, the following persons are duly appreciated for their invaluable, open
and sincere contributions to the success of this project. Professor Barnabas M Mandong, for
his objective and honest approach to our training, and for supervising this work at every stage
in a supportive manner. Dr MD Ayuba, for supervising this work in a most objective and
candidly meticulous way. His encouragement went a long way. Dr OA Silas is appreciated for
his occasional reproofs and inspiring encouragement at various points in time. Drs AN
Manasseh and Godwin Echejoh will not be forgotten for their constructive advice and
guidance.
Drs Emmanuel Bangams, BarkaVandi, and the residents of the Histopathology Unit, JUTH are
acknowledged and appreciated for their constructive criticisms and drive that kept me steady on
my feet. The selfless and professional inputs of Miss Ju Gye, always ready to help, as well as
Mrs. Rifkatu Bot in sectioning and staining the slides cannot be overlooked. All other staff
members of the JUTH Histopathology unit for their sundry helps at various times, and to Mr
Jared for assisting with aspects of data processing.
I can only say so much, to appreciate my ever loving and supportive parents, who are not just
parents, but friends indeed to their wards. My siblings, Eunice Edi, Joel, and Mercy were an
encouragement and positive challenge to me. Finally, the inputs of Joheobe Onah, and Mr
Livingstone will be remembered and indeed, many other friends and associates who space and
time will limit their mention here.

ix
LIST OF ABBREVIATIONS USED
CHM Complete Hydatidiform Mole
D & C Dilatation and Curettage
ETT Epithelioid Trophoblastic Tumour
GTD Gestational Trophoblastic Disease
GTN Gestational Trophoblastic Neoplasia
H & E Haematoxylin and Eosin
hCG Human Chorionic Gonadotropin
hPL Human Placental Lactogen
HUC Hospital Universitario de Caracas, Venezuela
JUTH Jos University Teaching Hospital
PHM Partial Hydatidiform Mole
PSTT Placental-Site Trophoblastic Tumour
UAE United Arab Emirate
UK United Kingdom
USA United States of America
WHO World Health Organization
x
LIST OF TABLES
Table 1 The distribution of GTD into specific morphologic/ histologic
subtypes in JUTH, Jos.
Table 2 Age distribution of GTD and the histologic subtypes in JUTH, Jos.
Table 3 Frequencies of the histologic types of GTD in relation to total pregnancies and
deliveries in JUTH, Jos.

xi
LIST OF FIGURES
Figure 1 Age distribution of the study population
Figure 2 Distribution of gestational trophoblastic diseases in JUTH into the histologic subtypes.
Figure 3 Photomicrograph depicting partial hydatidiform mole with oedematous vascular,
villous cores. Haematoxylin and eosin.
Figure 4 Histological photomicrograph of complete hydatidiform mole showing stromal
oedema imparted by cisternae, and a rim of surrounding roughly uniform trophoblast.
Haematoxylin and eosin.
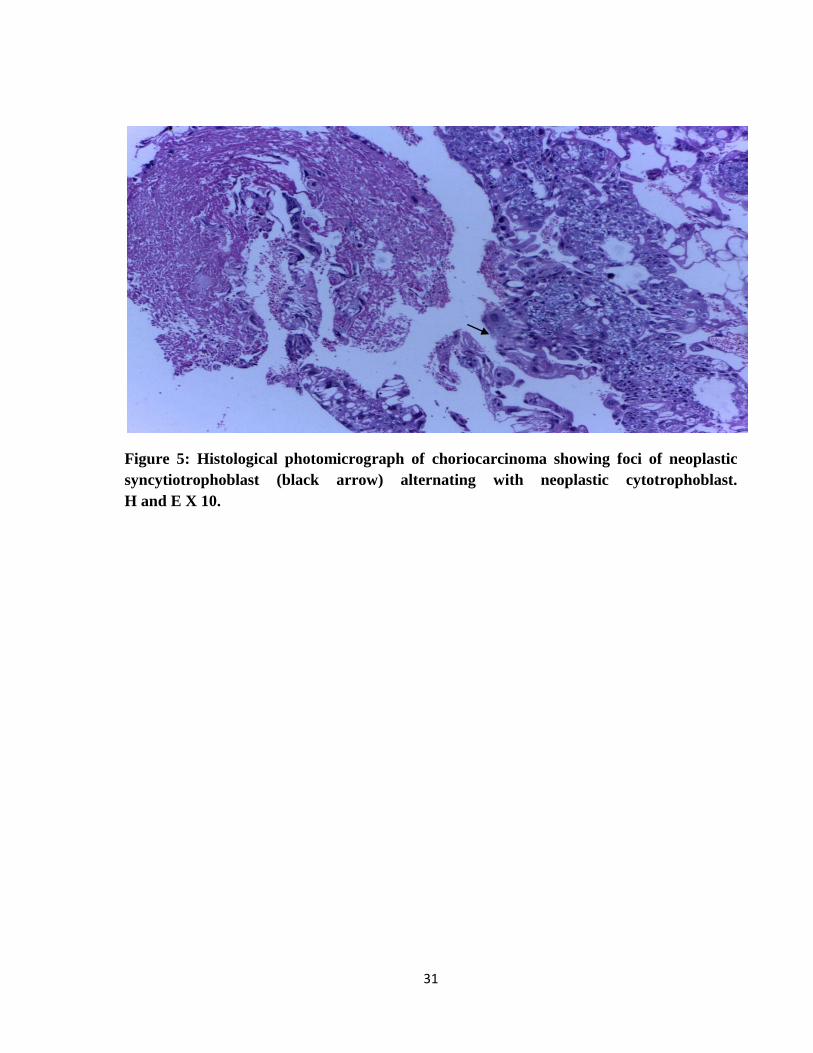
Figure 5 Histological photomicrograph of choriocarcinoma showing foci of neoplastic
syncytiotrophoblast alternating with neoplastic cytotrophoblast. Haematoxylin and eosin.
Figure 6 Histological photomicrograph of choriocarcinoma, showing foci of neoplastic
syncytiotrophoblast alternating with neoplastic cytotrophoblast, with a focus of necrosis and
haemorrhage at the left lower half. Haematoxylin and eosin.
Figure 7 Histological photomicrograph showing the large, polygonal intermediate trophoblastic
cells of PSTT. They have abundant eosinophilic cytoplasm. Haematoxylin and eosin.

xii
ABSTRACT
A group of diseases related to normal or abnormal gestation, that have a common
denominator, the abnormal proliferation of trophoblast tissue, are generically designated
gestational trophoblastic diseases. Individual disorders differ remarkably in their appearance
(morphology) and clinical significance.
Aim and Objectives
The study was aimed at characterizing all cases of histologically diagnosed gestational
trophoblastic diseases, seen at the histopathology department of the Jos University
Teaching Hospital (JUTH), between the years 2004 and 2013, all inclusive .
Materials and Method
The study was a 10-year hospital based retrospective study employing slides and tissue blocks
of specimens from uterine evacuation products of gestation of all females diagnosed with GTD
in the histopathology department of Jos University Teaching Hospital (JUTH) from January
2004 to December 2013. The materials used in the study included records from the
departmental registry and archival slides and tissue blocks from the archives of the
histopathology department of the hospital.

xiii
Results
A total of one hundred and fifty five (155) cases were diagnosed histologically as Gestational
Trophoblastic Diseases (GTD), during the period under review. These accounted for 0.8% of
all the surgical pathology specimens received.
One hundred and fifty one (97.4%) of the histologically diagnosed cases of GTD translated to a
frequency of 5.7 cases per 1,000 pregnancies. The following histological subtypes were seen:
sixty three cases (41.7%) were diagnosed as partial hydatidiform mole, forty-two cases (27.8%)
were choriocarcinoma, thirty-five cases (25.8%) were diagnosed as complete hydatidiform
mole. Four cases diagnosed as invasive mole accounted for 2.7%, which is closely followed by
3 cases of placental site trophoblastic tumour (PSTT), accounting for approximately 2% of
GTDs. However, no case of epithelioid trophoblastic tumour (ETT) was seen.
Conclusion
GTD was found to be common in Jos and had a frequency of 5.7 cases per 1000 pregnancies in
our series. The most common histological subtype was partial hydatidiform mole, closely
followed by choriocarcinoma. The molar lesions peaked in the third and fourth decades, while
choriocarcinoma peaked in the third decade of life.

1
CHAPTER ONE
INTRODUCTION
1.1 Introduction
A group of diseases related to normal or abnormal gestation, that have a common
denominator, the abnormal proliferation of trophoblast tissue, are generically designated
gestational trophoblastic diseases. Individual disorders differ remarkably in their
appearance (morphology) and clinical significance.1,2
This presents the importance of undertaking a study to characterize and essentially, contribute
to the available data on morphological patterns of gestational trophoblastic diseases in our
centre, as similar studies have been done in other places, with assessments of the
clinical characteristics and management outcomes.
The spectrum includes interrelated tumours, viz- complete hydatidiform mole, partial
hydatidiform mole, invasive mole, choriocarcinoma, and placental site trophoblastic
tumour. Variation in the frequency of complete mole for instance, is said to be striking.
In a study carried out by Hertig, the average incidence for young women in the United
States of America (USA) was 1 in 2000 deliveries3, whereas, the reported incidence in
South East Asia was four to five times greater than the USA average. Higher
incidences have also been reported from Mexico, the Philippines, India, Taiwan, and
Indonesia4,5.
Although, on a global scale, particularly in the developed nations, gestational
trophoblastic diseases are not very common, four separate studies have demonstrated
that they are relatively common among women of African descent, especially during

2
their reproductive age bracket9-13. Importantly too, they present a unique opportunity for
early detection and cure. Hence, the importance is emphasized, of increased patronage of
histopathological diagnosis, and ancillary investigations to enhance patient follow up,
treatment monitoring, as well as improved prognosis. Complete mole is the most
common form of gestational trophoblastic diseases, and presenting in the second
trimester, it is said to be more common in Asia, Africa, and Latin America14. Patients
with complete mole, usually tend to be above thirty (30) years of age, and more likely
have diets deficient in vitamin A precursors. The risk is however reduced by increased
carotene consumption, as well as a history of previous term delivery which also confers
less risk. On the other hand, history of a previous mole greatly increases the probability of
developing another molar pregnancy. An increased incidence of choriocarcinoma
reportedly follows a past history of complete mole, as well as older age (greater than
forty years) which is also a risk factor for choriocarcinoma 14. Choriocarcinoma is a curable
disease and early diagnosis becomes imperative.
1.2 Statement of the Problem
Globally, the highest reports of gestational trophoblastic diseases are from Asian
countries, and a relatively higher risk is also documented for black women15. Being at
extremes of the reproductive age group is an important risk factor associated with
molar pregnancy 15. Low literacy levels, poor socioeconomic status, and lack of antenatal
care have been documented as major contributory factors to late presentation, as well
as the inability to understand the importance of follow up in the Asian region of
Pakistan15. This may not be far from the situation in our own environment, which
would have informed the need for the index study to a large extent.

3
GTDs have been found to be quite common in our environment and owing to the unique
challenges of our health care system, they mostly present late. However, they are quite
potentially curable.
1.3 Justification for the Study
The importance of early diagnosis, prompt institution of treatment, and monitoring the
effects of therapy, by using serial determination of serum beta subunit of human chorionic
gonadotropin (β-hCG) are advocated as GTDs are curable. However, β-hCG secretion is
by no means restricted to gestational choriocarcinoma, or other forms of trophoblastic
diseases. It can occur also in non-trophoblastic disorders such as non-gestational
choriocarcinoma, other ovarian and testicular germ cell tumours, melanoma, lymphoma;
carcinomas of the oesophagus, stomach, pancreas, kidney, liver, lung, urinary bladder, the
uterus, adrenal glands, the breast, and other sites.
GTDs are a common health problem among Black and Asian women. They present late due to
the unique challenges of our health care delivery system, although they are potentially curable.
It is therefore important to undertake this study as it can also form the basis for
clinicopathological studies as a collaboration between the clinicians and pathologists.
It is expected to supply an important addition to the already existing body of data on gestational
trophoblastic disorders.
1.4 Aim
To review and characterize all cases of histologically confirmed or diagnosed gestational
trophoblastic diseases, seen at the histopathology department of the Jos University
Teaching Hospital (JUTH), between the years 2004 and 2013, all inclusive.

4
1.5 Objectives
(i) To determine the relative frequency of gestational trophoblastic diseases in JUTH.
(ii) To characterize GTDs according to the morphological/histopathological types.
(iii) To compare and contrast findings with relevant studies done in other centres

5
CHAPTER TWO
LITERATURE REVIEW
2.1 Background
Gestational trophoblastic diseases (GTD) as a group are a relatively rare condition,
especially in the western world, where a modest amount of work has been done and
documented on it. Again , as with most other conditions, data from Africa on GTD has
been relatively scarce16, but from available studies, it is found to be more common or
prevalent among Asian and black women. To confirm diagnosis, or make primary diagnosis
of unsuspected cases of molar gestation, histopathological examination of uterine evacuation
specimens is important, but in a particular study done in this centre (JUTH), by Ocheke
and coworkers, only 28.0% of patients seen had histopathology reports on their
specimens28.
2.2 Classification/Stratification of Patterns of Gestational Trophoblastic Diseases
There are both clinical and histopathological modes of classification. The system of classifying
gestational trophoblastic diseases adopted here is the modified world health organization
histopathological classification of gestational trophoblastic diseases, 200218. See appendix A.
2.3 Pathology
Molar pregnancies and gestational trophoblastic neoplasms all take their origin from placental
tissue. Normal placental trophoblast is composed of three types: syncytiotrophoblast,
cytotrophoblast and intermediate trophoblast.
6
The syncytiotrophoblast invades the endometrial stroma with implantation of the blastocyst19.
The cytotrophoblast functions to supply the syncytium with cells, in addition to forming
outpouchings that become the chorionic villi covering the chorionic sac. The intermediate
trophoblast is located in the villi, the implantation site and chorionic sac. GTDs may result
when all three types of trophoblastic tissue proliferate19.
Complete and partial hydatidiform moles are two separate variants of hydatidiform mole
described based on morphologic and cytologic criteria or differences.
2.3.1 Complete Hydatidiform Mole
Complete hydatidiform mole is usually diploid, and androgenetic in origin, having the 46XX
and 46XY karyotypes constituting 90% and 10% approximately, of these karyotypes
respectively. At the fertilization of the ovum, the maternal chromosomes are either inactive or
absent19. This implies that the chromosomes are purely paternal in a complete hydatidiform
mole.
For the histological features or morphological appearance, the trophoblast around the chorionic
villi is consistently hyperplastic with varying degrees of atypia. Villous capillaries are absent in
the core of the chorionic villi, unlike for partial hydatidiform mole.
2.3.2 Partial Hydatidiform Mole
Most partial hydatidiform moles (PHM) have a triploid karyotype (usually 69 XXY) resulting
from the fertilization of an apparently normal ovum by two sperms. The chromosomes are both
paternally and maternally derived.
Histopathologically, partial hydatidiform moles demonstrate identifiable foetal or embryonic
tissue, chorionic villi of varying sizes and shapes with focal oedema and scalloping,stromal

7
trophoblastic inclusions, functioning villous circulation, as well as focal trophoblast hyperplasia
with only mild atypia19.
2.3.3 Invasive Mole
The invasive mole is a benign tumour which arises from myometrial invasion of a hydatidiform
mole via direct extension through tissue or venous channels. It is most often diagnosed
clinically, rather than pathologically, based on persistent human chorionic gonadotropin
(β-hCG) elevation following molar evacuation. Invasive moles are frequently treated with
chemotherapy, even without making histopathological diagnosis.
Histologically, it is seen as direct extension of molar tissue, including hydropic villi with the
covering hyperplastic trophoblast into the myometrium.
2.3.4 Choriocarcinoma
Choriocarcinoma is a malignant disease characterized by abnormal trophoblastic hyperplasia
and anaplasia, absence of chorionic villi, haemorrhage and necrosis, with direct invasion into
the myometrium, vascular invasion and spread to distant sites. Approximately 25% of
choriocarcinomas follow abortion or tubal pregnancy, and another 25% are associated with
term or preterm gestation. The remaining 50% are said to arise from hydatidiform moles,
although only 2-3% of the moles progress to choriocarcinoma 19. Histopathological features are
as described, characterized by large syncytial cells with prominent nucleoli, severe nuclear and
cytologic pleomorphism, and some giant cells; the background is seen as neoplastic cells
alternating with intervening areas of necrosis and haemorrhage.
8
2.3.5 Placental-Site Trophoblastic Tumour (PSTT)
This is an extremely rare disease which arises from the placental implantation site, and consists
predominantly of mononuclear intermediate trophoblast (without chorionic villi formation)
infiltrating in sheets or cords between myometrial fibres. PSTT is associated with less vascular
invasion, necrosis, and haemorrhage than is choriocarcinoma, but is said to have propensity for
lymphatic spread19. Immunohistochemically, diffuse presence of cytokeratin and human
placental lactogen (hPL) staining is demonstrated, while the hCG staining is only focal19.
2.3.6 Epithelioid Trophoblastic Tumour (ETT)
Epithelioid trophoblastic tumour is a rare variant of PSTT that simulates carcinoma. It appears
to develop from neoplastic transformation of chorionic-type intermediate trophoblast, based on
morphological and histochemical features19. Most ETTs are said to present many years
following a full-term delivery.
2.4 Epidemiology of Gestational Trophoblastic Diseases
2.4.1 Distribution
Although a wide geographical variation is observed in the frequency, and reported
incidences of gestational trophoblastic diseases, the highest number of incidents are
reported from the Asian continent. There is a relatively high risk reported for black
women as well, e.g. African American women20.
There are three main forms in which gestational trophoblastic diseases occur, viz:
hydatidiform moles (in 80% of cases, complete mole being the most common form of
GTD), locally invasive moles (in 15% of cases), and metastatic trophoblastic disease
(choriocarcinoma, in 5% of cases)22,23. In a review of cases of hydatidiform mole by
9
Moore and Hernandez24, reported frequencies range from 1 in 100 pregnancies in
Indonesia to 1 in 200 pregnancies in Mexico, and 1 in 5000 pregnancies in Paraguay.
Frequency of complete and partial moles in Ireland was established at 1 per 1945 and 1
per 695 pregnancies respectively, based on a study of pathological material from first
and second trimester abortions.
In a study conducted much earlier, the incidence from the Far East (the Orient) was as
high as 1 in 120 pregnancies, and a separate study in Indonesia reported an incidence of
molar lesions to be 1 in 77 pregnancies20,24. The incidence of malignant trophoblastic
disease (choriocarcinoma) was 1 in 185 pregnancies, and spontaneous remission was
reported in 80% to 85% of all patients with hydatidiform mole. In another review, the
incidence of hydatidiform mole in the USA was about 1 in 2000 deliveries or 1 in 1200
pregnancies, which was said to be influenced by socioeconomic status and race 21. The
incidence in the UK was 1.5 per 1000 pregnancies, in Japan it was 2 per 1000
pregnancies, and in Nigeria it was 2.4 per 1000 pregnancies 20,21.Thus, GTDs are more
common in the Orient (Far East) and in Mexican Americans living in southern
California, and among Africans. Additionally, while a prevalence study in Nigeria has
reported a prevalence ranging from 99 to 335 cases of molar gestation per 100,000
pregnancies, a study in South Africa estimated the incidence of molar pregnancy to be
1.2 and of choriocarcinoma to be 0.5 cases per 1000 deliveries.
2.4.1.1 Complete Hydatidiform Mole
As was earlier highlighted from published literature, complete hydatidiform mole is the most
common form of GTD. A study by Moore and Hernandez24, found out that tissue
examination by histology may reveal hydatidiform mole (complete or partial) or a

10
choriocarcinoma, but rarely is the histopathological diagnosis of an invasive mole or placental-
site trophoblastic tumour (PSTT) made on dilatation and curettage (D&C) specimens.
A study in the Asian region by Graham et al, in Abu Dhabi reported that Gulf Arabs have the
highest risk of developing complete hydatidiform mole25. Maternal ethnic-specific incidences
per 1000 births in different regions, for complete hydatidiform mole are as follows: Gulf Arabs
3.29, UAE Arabs 1.90, other Arabs 1.28, Asians 1.58, British women 0.55, and for African
women, 1.1025.
The reported prevalence of complete hydatidiform mole from an East African review in
Mulago hospital, Kampala Uganda was 3.42 per 1000 deliveries (or 342 per 100,000
pregnancies) and patients’ mean age was 29.6±8.5 years. The conclusion from this study was
that complete hydatidiform mole is a common condition in the region26. A North African
experience from a Moroccan study revealed an incidence of complete mole to be 4.3 per
1000 pregnancies, or 0.43%, with the mean age being 25years (age range of 16-55 years). In a
Tunisian study of sixty (60) cases or patients, whose mean age was 31.7years, thirty-three (33)
cases were found to be complete hydatidiform mole (55%)27.The study in Zaria, Nigeria by
Mayun et al35, revealed that complete hydatidiform mole occurs more frequently than the
partial hydatidiform mole, with thirty-four (34) cases reported as CHM out of fifty-six (56)
molar lesions (60.7% of cases studied were CHM), and patients’ mean age was 25.7years. The
findings in the foregoing studies are consistent with what obtains in already published
literature14, but a contrast is noted in two other Nigerian studies.32,37

11
2.4.1.2 Partial Hydatidiform Mole
In Ireland, the frequency of PHM was established to be 1 per 695 pregnancies (0.14%) based
on a study of pathological material from first and second trimester abortions. The North
African scenario shows that the Tunisian study reported twenty-seven (27) cases as partial
hydatidiform mole (45.0%) out of sixty (60) cases studied retrospectively27. From Morocco, the
frequency reported was 0.4 per 1000 pregnancies (i.e. 0.04%, much lower than that of complete
mole in the same series: University hospital, Casablanca; 2000 to 2010).46,47
In the multicenter study by Nggada et al 37, which analyzed cases drawn from three tertiary
hospitals in Maiduguri, Ilorin and Nnewi, the conclusion reached was that partial hydatidiform
mole was the most frequent (64.50% of total cases) histopathological pattern of gestational
trophoblastic diseases. The peak age group of patients affected was in the third decade of life
with a mean age of 27.65years (±7.6). Whereas twenty cases (35.70%) were reported as PHM
out of the 56 cases of molar gestations studied in Zaria Nigeria, making it less frequent than
complete hydatidiform mole, this is in keeping with data of published literature14,31,35. The
converse however was obtained in the Benin and multicenter studies by Aligbe et al32, and
Nggada et al37 respectively.
2.4.1.3 Invasive Mole
In Latin America, an eight-year study at the Hospital Universitario de Caracas (HUC) revealed
the mean age of patients to be 29.20 years, and out of twenty five (25) patients diagnosed with
and characterized as cases of gestational trophoblastic neoplasia (GTN), 4.0% had invasive
mole. Of the GTD cases studied in East Africa, from two teaching hospitals in Addis Ababa,
Ethiopia 12.90% were invasive mole33. Cases of invasive mole encountered in the multicenter
study by Nggada et al37, accounted for just around 1.10% of all GTD lesions characterized.

12
Whereas in the Nnewi, South-eastern Nigeria scenario, no case of invasive mole or PSTT was
identified, two cases of invasive mole, accounting for 3.60% of the 56 molar lesions analysed
in Zaria were reported by Mayun et al31,35 and in Benin city, 2.10% of the GTD cases analyzed
were identified as invasive mole, all corresponding to the least reported morphological
form/pattern of gestational trophoblastic diseases.
2.4.1.4 Choriocarcinoma
It is reported that in Europe and North America, choriocarcinoma affects approximately 1 in
40,000 pregnancies, and 1 in 40 hydatidiform moles, while in South-east Asia and Japan, the
rates are higher at 9.20 and 3.30 per 40,000 pregnancies respectively. The incidence rates for
both hydatidiform moles and choriocarcinoma are said to have declined in all populations over
the past thirty (30) years. The Venezuelan series in the HUC, revealed that, of the twenty-five
(25) patients diagnosed with GTN, 36% had choriocarcinoma. From East Africa, in the Addis
Ababa, Ethiopia series, choriocarcinoma was the second most common morphological pattern
of GTD, accounting for 15.0%34.
The Zaria, Nigeria series reported by Mayun et al, showed that out of 56 molar gestations,
37.0% (43 cases) of the GTDs were choriocarcinoma35. Choriocarcinoma also accounted for
57.7% of malignant tumours of the female genital tract, in a separate series in Zaria, North-
Western Nigeria36. In the multicenter study by Nggada et al37, choriocarcinoma was the second
most common type of GTD and accounted for 21.5%. In the Nnewi, South-eastern Nigeria
series, the conclusion reached was that a high prevalence of GTD exists, notably of
choriocarcinoma, with associated high mortality. It accounted for 66.7% of the cases of GTD
studied9.
13
2.4.1.5 Placental-Site Trophoblastic Tumour
In all the series cited, there were no reports of the PSTT variant of gestational trophoblastic
disease, hence confirming its rarity.
2.4.2 Determinants
A case-controlled study from Baltimore (USA), shows that the factors associated with
gestational trophoblastic diseases included, professional occupations, history of prior
spontaneous abortions, and the mean number of months from the last pregnancy to the
index pregnancy20. Furthermore, the highest incidences of GTD are observed among
women with the following demographic characteristics;
Extremes of reproductive age, i.e. greater than 45 years, and less than 15 years,
whereas a significantly lower incidence was seen in women at 20 to 29 years of age
in a study by the Duke group20,41.
Absence or deficiency of dietary carotene and animal fat
History of spontaneous abortions and previous molar gestation (the risk of recurrence
is 1- 2%)
Women whose husbands are exposed to soil and dust ( consistent with the findings
reported in the Morocco, North African experience, where the most incidences are among
women of low socioeconomic status, and whose husbands engage in agricultural
activities)38-42.

14
Interestingly, when a female with blood type A marries a man of blood type B or blood
type O, from a particular review, it shows there is a 10-fold increase in the incidence of
molar disease (GTD) in the event of subsequent pregnancies30.
The following are certain specific risk factors for chariocarcinoma ;
Prior complete hydatidiform mole. Choriocarcinoma is approximately one thousand
times more likely after a complete mole than after another normal pregnancy event.
Ethnicity and advancing maternal age: The risk is increased in women of Asian,
American-Indian, and those of African-American descent 4,5.
Women on long term oral contraceptives and those who are of blood group-A.
In another USA study, malignancy is diagnosed in 15 to 20% of patients with prior complete
hydatidiform mole and in 2 to 3% of patients with partial hydatidiform mole, while lung
metastases were found in 4 to 5% of patients with a CHM24. Hydatidiform mole is more
common at the extremes of reproductive age; the most at-risk women are in their early teenage
and/or perimenopausal years. Women older than thirty-five (35) years have a 2-fold increase in
risk and those older than forty (40) years have a 5 to 10-fold increase in risk compared to
younger women. With frequent pregnancies, and in women above forty (40) years of age,
the incidence of malignant GTD increases22,24,42. Though most choriocarcinomas follow
the evacuation of a hydatidiform mole, 25% accompany spontaneous miscarriages or
ectopic pregnancies; the remaining quarter (25%) occur, following term delivery, and
any GTD that occurs following a normal (uneventful) pregnancy and delivery is
invariably a choriocarcinoma22,42.

15
Hertz had demonstrated in the late 1940s that foetal tissue (or gestational trophoblast
tissue, as the case may be) requires a large amount of folic acid, and could be
inhibited by the anti-folate compound, methotrexate (hence, its role in chemotherapy)22,43.
Other determinants which can influence the development of GTD border on the sizes of
the uterus and ovaries at the time of diagnosis. For many years, the uterine size at the
time of diagnosis has been considered a significant factor with regards to the
development of malignant sequelae. In a review of 347 patients with hydatidiform mole
by Curry et al43,it was noted that those with normal sized and large for date uteri had
a 25% chance of developing gestational trophoblastic neoplasia or GTD, compared with
only 11% chance in patients with small for date uteri. Patients with enlarged ovaries
irrespective of the uterine size had a 49% chance of gestational trophoblastic neoplasia
(GTN) appearing in the future. Those with both enlarged ovaries and large for date
uteri developed GTN in 57% of cases, compared with only 16% if the uteri and
ovaries were not enlarged. In addition, an increased incidence of malignant sequelae was
observed in 29% of cases in patients for whom the time of evacuation was between 11 and
15 weeks, compared with just 4% in those whose time of evacuation was less than 10
weeks (of gestational age).
2.4.3 Deterrents
A history of previous term delivery confers less risk, as well as increased consumption
of carotene reduces the risk for gestational trophoblastic diseases in general.

16
2.5 Treatment Outcomes
For all patients with molar pregnancy, the standard treatment is cervical dilatation and suction
curettage (D&C)44.
In a South African hospital-based study, an audit of 112 patients, the main treatment modality
for patients with molar pregnancy was suction curettage, while choriocarcinoma was treated
primarily with chemotherapy. A total of 72% of patients with molar pregnancy, and 28% of
patients with choriocarcinoma had complete remission after initial therapy. Twelve (12)
patients were said to have died in the course of treatment, mainly due to late presentation and
advanced metastatic disease. Complete cure was achieved in 89% of patients overall, while
spontaneous remission was achieved in 60% of the patients with molar pregnancy45.
A retrospective study of sixty (60) cases in Tunisia revealed that thirty-three (33) cases were
histopathologically confirmed to be complete hydatidiform mole, while twenty-seven (27)
cases were PHM. Six (6) of the 33 patients with CHM developed persistent GTD, while
actinomycin-D induced complete remission in all cases. In a selective review of twenty-four
(24) cases of partial hydatidiform mole, out of 60,748 births in Morocco, the treatment was
endo-uterine aspiration (or suction curettage), while neoplastic drift was observed in one case
(4.2%) which went into remission with chemotherapy27,46. In a separate study of complete

17
hydatidiform mole in the same centre in Casablanca Morocco, 6.3% of cases had neoplastic
progression, and they all evolved into remission with chemotherapy 47.
In the Nigerian scenario, beginning with a gynaecological study in the Jos University Teaching
Hospital (JUTH), thirty-four (34) cases of hydatidiform mole were reviewed out of 12,129
deliveries taken between the years, 2001 and 2005. Suction curettage was the main mode of
treatment for all patients in this review, and only 7 patients (28%) had histopathological
confirmation done. After 3 months from diagnosis, no patient presented for follow up, while 17
patients (68%) came for at least one follow up visit within the first three (3) months of
treatment. Three (12%) of the patients lost to follow up, presented in the gynaecological
emergency unit with persistent gestational trophoblastic disease (i.e with features of malignant
disease) within six months.

18
CHAPTER THREE
3.1 MATERIALS AND METHOD
The study was a 10-year hospital based retrospective study employing slides and tissue blocks
of specimens from uterine evacuation products of gestation of all women diagnosed with GTD
in the histopathology department of Jos University Teaching Hospital (JUTH) from January
2004 to December 2013. JUTH is a referral tertiary health centre in North central Nigeria. The
materials used in the study included records from the departmental registry and archival slides
and tissue blocks from the archives of the histopathology department of the hospital. The
specimens studied included those obtained through uterine evacuation and hysterectomy
specimens received and diagnosed as GTD, in the department. Records of histologically
diagnosed GTD were retrieved from the departmental registry of the hospital and were
compared with fresh diagnoses made from sections of archival paraffin embedded formalin
fixed blocks. The slides were read by supervising consultants and the modified WHO
classification of GTD (Appendix A) in combination with specified diagnostic criteria was used
to classify the diseases as presented.
All GTD histologically diagnosed between January 2004 and December 2013 in the
histopathology department of JUTH with traceable archival slides or tissue blocks and clinical
data including age, were included in the study while clinically diagnosed GTDs using imaging
and not subjected to histological diagnosis were excluded.
19
3.2 DIAGNOSTIC CRITERIA
The criteria employed to diagnose and characterize the variants of GTD in this study are the
histopathological features seen on microscopic examination of H & E stained tissue sections.
They are stated as follows;
Complete Hydatidiform Mole
Lesions or cases will be diagnosed as CHM if they meet the following criteria:
i. Marked variation in sizes of the villi, with many abnormally, and markedly
distended (enlarged) chorionic villi, due to the oedema.
ii. Hydropic changes in the core of the villi, imparted by distended cisternae
iii. Absence of villous capillaries in the core of the chorionic villi.
iv. Consistent or almost continuous (circular) trophoblast hyperplasia around the villi,
with varying degrees of possible atypia.
Partial Hydatiform Mole
Lesions or cases will be diagnosed as PHM if they meet or satisfy the following criteria:
i. Presence of variable sizes and shape of chorionic villi
ii. Focal oedema, and scalloping in the villous cores, but absent cisterns.
iii. Functioning villous circulation (villous capillaries) in the core of the villi.
iv. Focal trophoblast hyperplasia with only mild atypia.
v. All above in addition to likely history of passage of fleshy materials together with
the vesicles par vaginam.

20
Invasive Mole
Lesions or cases will be diagnosed as invasive mole if they meet or satisfy the following
criteria:
i. A background of surrounding myometrial tissue (composed of bundles and fascicles
of smooth muscle cells).
ii. Molar tissue including hydropic villi with the covering hyperplastic trophoblast,
extending directly into the background myometrium.
iii. With added history of persistently elevated serum β-hCG following molar
evacuation.
Choriocarcinoma
Lesions or cases will be diagnosed as choriocarcinoma if they meet or satisfy the following
criteria:
i. Absence of chorionic villi predominantly
ii. Abnormal trophoblast hyperplasia and anaplasia with other cytologic and nuclear
features of malignancy.
iii. Neoplastic cytotrophoblast and syncytiotrophoblatic cells alternating in areas.
iv. Non-viable tissues with necrosis and haemorrhage alternating in the background
with intervening neoplastic cells.
Placental Site Trophoblastic Tumour
Lesions will be diagnosed as placental-site trophoblastic tumour if they satisfy the following
criteria:
i. Absence of chorionic villi
ii. Presence of intermediate or extravillous trophoblast in the form of sheets, nests and
21
cords.
iii. Background of myometrial tissue with minimal foci of necrosis and haemorrhage.
The data was analyzed using the EPI info statistical software version 7 and were presented in
histogram, pie chart and tables.
3.3ETHICAL CONSIDERATION
Ethical consideration was given to this research; ethical clearance was obtained and its terms
were strictly adhered to in the conduct of this research.

22
CHAPTER FOUR
4.1 RESULTS
A total of one hundred and fifty five (155) cases were diagnosed histologically as gestational
trophoblastic diseases (GTD), during the study period. These accounted for 0.8% of all the
surgical pathology specimens received, which were a total of 20,131 specimens within the
study period.
The total number of pregnancies and deliveries registered at the Obstetrics and Gynaecology
Department were 26,319 and 25,395 respectively.
One hundred and fifty one (97.4%) of the histologically diagnosed cases of gestational
trophoblastic diseases were included in the study. Four cases however, were excluded from the
study for not meeting the inclusion criterion, of having complete biodata.
The 151 cases of GTD translate to a frequency of 5.7 cases per 1,000 pregnancies.
Alternatively expressed against the total deliveries, the frequency of GTD was 5.9 cases in
1,000 deliveries.
Of the 151 histologically diagnosed cases, the following histological subtypes were seen: sixty
three cases (41.7%) were diagnosed as partial hydatidiform mole, forty-two cases (27.8%) were
choriocarcinoma, thirty-five cases (25.8%) were diagnosed as complete hydatidiform mole
(Table 1). Furthermore, four cases diagnosed as invasive mole accounted for 2.7%, which is
closely followed by 3 cases of placental site trophoblastic tumour (PSTT), accounting for
approximately 2% of GTDs. However, no case of epithelioid trophoblastic tumour (ETT) was
seen.
23
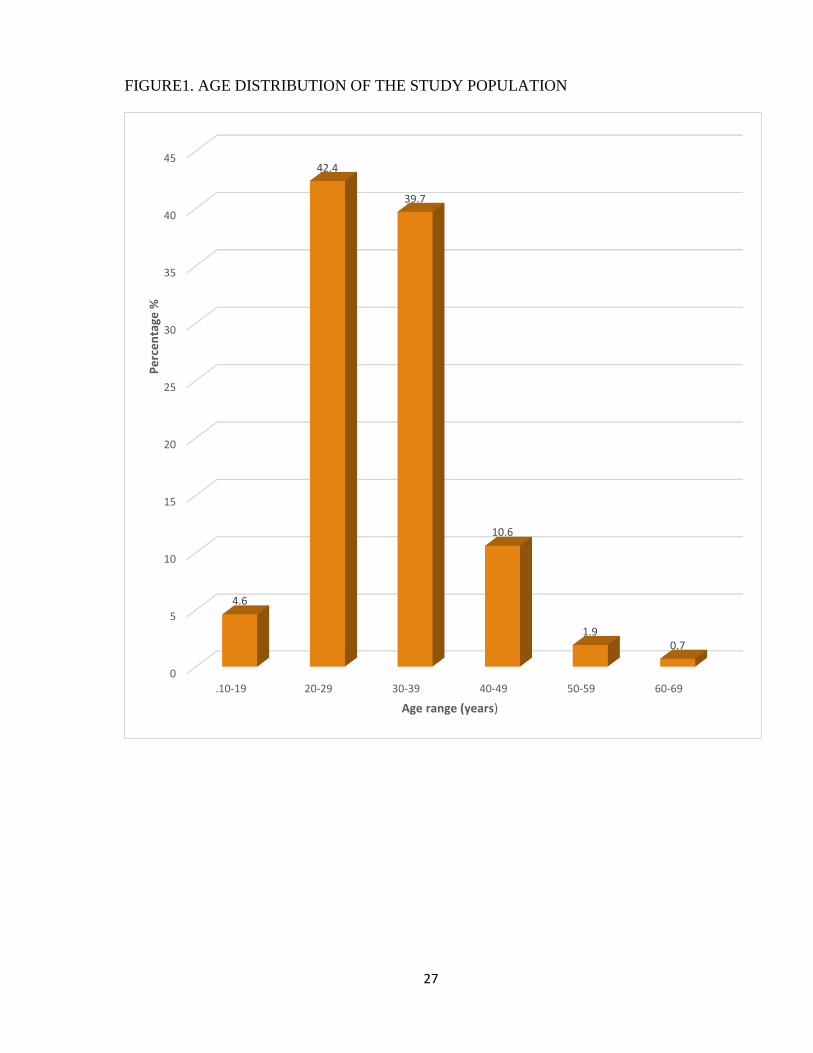
The ages of the patients ranged from 17 to 65 years, with a mean age of 30.7 years. The peak
age for all GTD was in the third decade.
The most common histologic sub-type seen was partial hydatidiform mole (41.7%), with a
mean age at 31 years and peak age within the age range 30 to 39 years. This is followed by
choriocarcinoma (27.8%) with a mean age at 30 years and peak age within the age range 20 to
29 years.
Complete hydatidiform mole (CHM) represented 25.8% of cases with a mean age at 30.4
years, and peak age within the age range of 20 to 29 years.
The four cases of invasive mole had a mean age at diagnosis of 40.5 years, and a median age
of 39.0 years (Table 2).
The cases diagnosed as placental site trophoblastic tumour (PSTT) had a mean age of 24 years
and a median age of 23 years. The peak age was within the age range of 20 to 29 years
(Table 3).
24
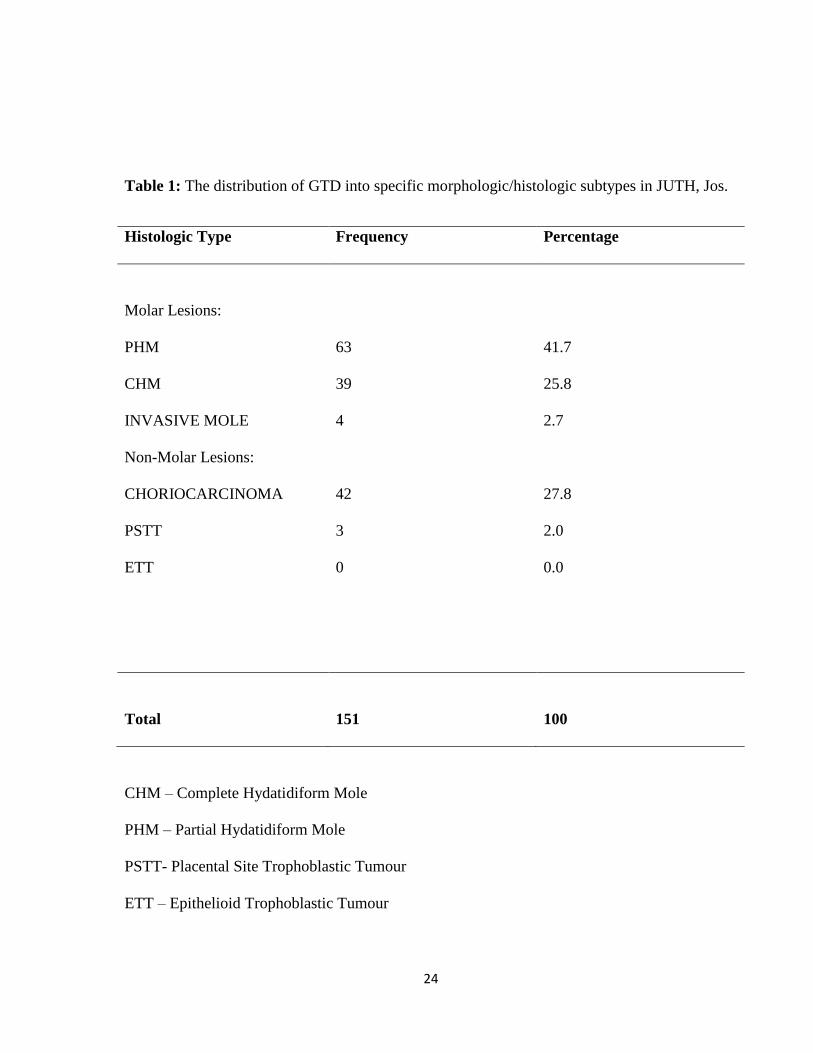
Table 1: The distribution of GTD into specific morphologic/histologic subtypes in JUTH, Jos.
Histologic Type Frequency Percentage
Molar Lesions:
PHM
CHM
INVASIVE MOLE
Non-Molar Lesions:
CHORIOCARCINOMA
PSTT
ETT
63
39
4
42
3
0
41.7
25.8
2.7
27.8
2.0
0.0
Total 151 100
CHM – Complete Hydatidiform Mole
PHM – Partial Hydatidiform Mole
PSTT- Placental Site Trophoblastic Tumour
ETT – Epithelioid Trophoblastic Tumour

25
Table 2 Age distribution of GTD and the histologic subtypes in JUTH, Jos
Age
range
(years)
CHM PHM Invasive
Mole
Choriocarcinoma PSTT Frequency Percentage
(%)
10-19 1 3 0 3 0 7 4.6
20-29 21 21 1 18 3 64 42.4
30-39 13 30 1 16 0 60 39.7
40-49 3 8 1 4 0 16 10.6
50-59 1 1 1 0 0 3 1.9
60-69 0 0 0 1 0 1 0.7
Total 39 63 4 42 3 151 100
The overall peak age for all GTDs, in JUTH = 30.0+8.1years; Mean age (all GTD) = 30.7+8.1
years; Median age = 30.0+8.1years.
Age range (all GTD) = 17-65 years in JUTH

26
Table 3: Frequencies of histologic types of GTD expressed in relation to total pregnancies
and deliveries in JUTH.
Histologic type Frequency Percentage (%) Freq. per
1,000
pregnancies
Freq. per 1,000
deliveries
(births)
CHM 39 25.83 1.48 1.54
PHM 63 41.72 2.39 2.48
CHORIOCARCINOMA 42 27.81 1.60 1.65
INVASIVE MOLE 4 2.65 0.15 0.16
PSTT 3 1.99 0.11 0.12
ETT 0 0.00 0.00 0.00
Total 151 100 5.73 5.95
27
FIGURE1. AGE DISTRIBUTION OF THE STUDY POPULATION
0
5
10
15
20
25
30
35
40
45
.10-19 20-29 30-39 40-49 50-59 60-69
4.6
42.4
39.7
10.6
1.90.7
Pe
rce
nta
ge %
Age range (years)
28
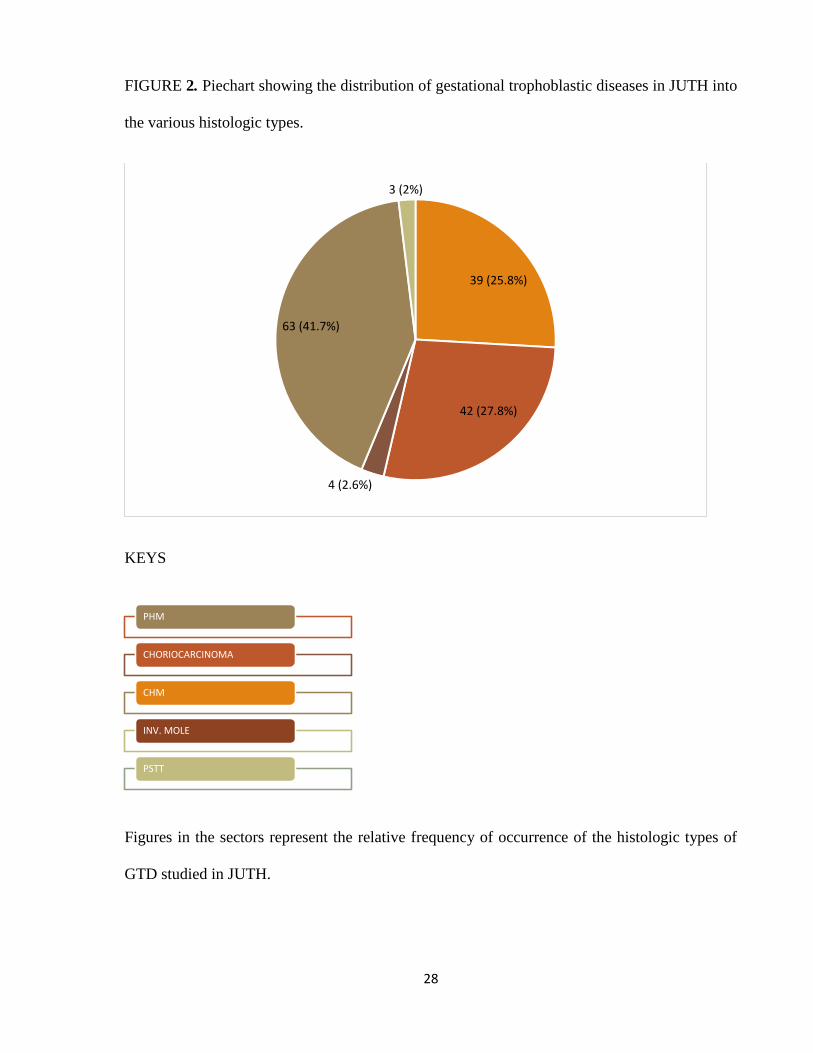
FIGURE 2. Piechart showing the distribution of gestational trophoblastic diseases in JUTH into
the various histologic types.
KEYS
Figures in the sectors represent the relative frequency of occurrence of the histologic types of
GTD studied in JUTH.
39 (25.8%)
42 (27.8%)
4 (2.6%)
63 (41.7%)
3 (2%)
PHM
CHORIOCARCINOMA
CHM
INV. MOLE
PSTT

29
Figure 3: Photomicrograph depicting partial hydatidiform mole with oedematous,
vascular villous core. H &E X 40

30
Figure 4: Histological photomicrograph of complete hydatidiform mole showing stromal
oedema imparted by cisternae, and a rim of surrounding roughly uniform basophilic
trophoblast. H and E X 20.
31
Figure 5: Histological photomicrograph of choriocarcinoma showing foci of neoplastic
syncytiotrophoblast (black arrow) alternating with neoplastic cytotrophoblast.
H and E X 10.

32
Figure 6: Histological photomicrograph of choriocarcinoma showing foci of neoplastic
syncytiotrophoblast (black arrows) alternating with neoplastic cytotrophoblast with a
focus of necrosis and haemorrhage at the left lower half.
H and E X 40.

33
Figure 7: Histological photomicrograph showing the large polygonal intermediate
trophoblastic cells of PSTT. They have abundant eosinophilic cytoplasm.
H and E X 40.
34
CHAPTER FIVE
DISCUSSION
Gestational trophoblastic diseases are a heterogeneous group of neoplastic conditions. These
diseases vary from partial hydatidiform mole (PHM) which rarely metastasizes, to the highly
malignant choriocarcinoma. The total burden of gestational trophoblastic diseases (GTD) in our
series (151 cases) translates to a frequency of 5.7 cases in 1000 pregnancies. In relation to the
total deliveries it is 5.9 cases in 1000 deliveries. A study carried out by Mayun51in Gombe,
North-eastern Nigeria reported a frequency of 6 in 1000 deliveries. This places the Jos study
very close to the Gombe study. This similarity may be due to the fact that the studies were both
carried out in the same geographical location, the northern part of the country. The age range of
our study population, 17 to 65 years varies from that of the Gombe study population, which has
an age range of 15 to 44 years. The occurrence patterns of GTD within an early age range in
Gombe may be the result of early marriages and multiparity in the early years of the women’s
reproductive life. The peak age of occurrence of GTD in Gombe was noted in the second
decade which is similar to ours in the Jos series. The GTD frequency observed in Jos is much
higher than the 3.58 per 1000 deliveries reported in Ebonyi by Anuma and Coworkers8, who
also reported an age range of 19 to 55 years and a mean age of 33.4±7.4 years. The Jos
frequency was however, much lower than the 46 cases per 1000 deliveries reported in Nnewi
(South-east Nigeria)9. This may be due to regional variations with respect to different
speculative factors.
The age range in our study is higher than that observed at Nnewi, which is put at 15 to 46 years.
The mean age of patients reviewed in the index study reported to be 30.7±8.1 years is slightly
lower than 33.4 years in Ebonyi, but is comparable to 31.0±8.6 years reported in Nnewi9. The

35
slight variations noted may be due to the different sample sizes used in the different studies.
However the mean ages were all observed within the third decade of life which is compatible
with reproductive life. The frequency of GTD reported in Benin City (4 in 1000 deliveries) by
Aligbe et al32, was comparatively lower than the observation in our study. The frequency of
GTD in Ile-Ife put at 1.7 in 1000 deliveries38 is below the frequency observed in Jos. However,
the frequency in Ibadan of 5.8 cases in 1000 deliveries and that in Lagos of 5.4 in 1000
deliveries39 are seen to compare well with the observation in our own study.
Several studies appear to show variations in the incidence of GTD worldwide. This could be
associated with some peculiar geographical factors, pregnancy risks, unknown environmental
agents and genetic factors. The peak age in the present study of 30 years is higher than the peak
ages reported in the Benin series by Aligbe et al32 and the multicenter study by Nggada et
al37(in Maiduguri, Ilorin and Nnewi), which are respectively in the third, and second and third
decades of life. The mean age of patients in the index study population of thirty (30) years is
comparably higher than that observed by Nggada et al37 put at 27.7 years, and is also higher
than that reported by Ocheke et al28 in a previous gynaecological review in Jos over a 5 years
period (2001-2005), which was 28 years.
A prevalence study in Nigeria reported a frequency of 0.99 to 3.35 cases of molar gestation per
1000 pregnancies44 which is higher than the frequency reported in Ethiopia as 2.8 per 1000
deliveries by Negussie et al33. In the Ethiopian series, the mean age was 30.9±6.5 years, and the
median age was 34.5 years while the ages of the patients were in the range 14 to 53years. These
are approximately comparable to the observations made in the Jos study.
The frequency of GTD reported in Tunisia by Chechia et al27 which was 1.3 in 1000
pregnancies is markedly lower than the frequency in our study. However, the mean age of the
36
Tunisian study population of 31.7 years is slightly above the mean age of our patients of 30.7
years. The mean age of the study population in Jos is also slightly higher than that recorded in
a South African review of 112 patients that was put at 28.5 years45.
Compared to the incidences in the United Kingdom (UK) and Japan which respectively had
frequencies of 1.5 and 2.0 in 1000 pregnancies20, the frequency of GTDs in Jos of 5.7 in 1000
pregnancies is considerably higher.
The mean age of a study population reviewed in America, over a 10 years period by Robert et
al10 was 25.2 years, the median age was 25 years while the age range was 14 to 45 years which
are all comparably lower than the corresponding data assessed in our study. These differences
in frequency and age characteristics between our local studies and those done in Western
countries might be explained by the availability of and access to healthcare facilities and
service delivery in the Western world, which however are conspicuously lacking or deficient in
our environment.
Partial hydatidiform mole (PHM) turned out to be the most common histologic type of all the
histopathological patterns of GTD, characterized in this study. With a frequency of 63 out of
151 cases, it accounted for 41.7% of the total study population of women diagnosed with one
pattern or the other of GTD, which is quite a deviation from what is known and published in
standard texts of histopathology and gynecologic pathology from the Western world14. The
converse, which however is obtained in published literature, is that complete hydatidiform mole
constitutes the most frequent pattern of GTD seen globally14.
Nevertheless the outcome of PHM seen in Jos, doesn’t stand alone as a few other studies
previously conducted and indigenous to our clime have shown a similar pattern, or
outcome32,37. For instance the pattern or outcomes observed in the multicenter study by Nggada

37
and coworkers37 makes it appear to be an almost similar or reproducible pattern in comparison
with our index study. PHM was the commonest histological type of GTD seen by Nggada et
al37, accounting for 64.5%, followed by choriocarcinoma which accounted for 21.5% of cases.
The complete hydatidiform mole (CHM) made 12.9% of cases, while invasive mole accounted
for 1.1% of all GTDs reviewed, but there was no case of placental site trophoblastic tumour
(PSTT) seen in their series.
Comparably, in our study choriocarcinoma was the second most frequent pattern of GTD
accounting for 27.8%, followed by CHM accounting for 25.8%, while the invasive mole and
PSTT accounted for 2.65% and 1.99% respectively. This pattern almost or approximately
shows a similarity that mirrors the outcome of the Nggada et al37 series, except that they had no
case of PSTT just as no case of epithelioid trophoblastic tumor was seen in the Jos study.
In Benin City, PHM was the most frequent histologic type encountered accounting for 47.9%
of the GTD cases found, followed by choriocarcinoma at 12.5%, and then invasive mole
accounting for 2.1%. No CHM or PSTT cases were recorded32.
The pattern of gestational trophoblastic diseases observed in our study exhibited a contrast to
that reported by Mayun51 at the Federal Medical Centre, Gombe in which series CHM
constituted 52.9% of the total cases studied, PHM was reported in 47.15% of cases, and no case
of invasive mole was seen51. The pattern of GTDs in Jos, again shows a contrast to that
reported by Mayun et al35 in a separate study in Zaria, where complete hydatidiform mole was
the commonest type with a proportion of 60.7%, followed by choriocarcinoma making a
proportion of 37%, while PHM and invasive mole, each accounted for 35.7% and 3.6%
respectively of all the GTD cases seen. Moreover, the mean age reported by Mayun et al35 of
25.7 years is below the mean age in Jos, but vaginal bleeding appears to be the commonest

38
clinical presentation, across board in almost all the studies. In addition, honeycomb uterine
appearance on pelvic ultrasound and passage of vesicles per vagina were reported as other
modes of clinical presentation by Ocheke et al28. It is instructive to observe that, in an earlier
study in Jos, only 28% of the cases reviewed were actually confirmed by histopathological
examination according to Ocheke et al28. Thus, this emphasizes a real need for more clinicians
to engage and patronize the services of pathologists to procure accurate histologic diagnoses for
their clients, especially as it concerns gestational trophoblastic diseases.
Expectedly, the pattern of the histologic types seen in Tunisia is consistent with that reported in
published western literature with CHM accounting for 55% and PHM 45% of the cases of GTD
analyzed.
The frequency reported in Uganda (East Africa) was 3.42 cases in 1000 deliveries (particular
reference to CHM) by Kaye26 which again is quite on the lower side compared to the local
frequency in Jos. However, the mean age of 29.6 years among the Ugandan patients with CHM
compares relatively well to the mean age of patients in Jos, Nigeria.
The frequency of GTD observed in Morocco by Boufettal and coworkers46 was 0.4 per 1000
pregnancies (reference to PHM) which is way below the local frequency in Jos. The mean age
of patients in this series was 26 years, while the age range was 16 to 55 years. A similar study
also by the same authors in Morocco (reference to CHM), showed up with a frequency of 4.3
per 1000 pregnancies (or 0.43%) and a mean age of 25 years47 which are again lower than the
frequency and mean age in our study. However, all the cases analyzed in the Moroccan series
were subjected to confirmation by histopathological examination47. Complete hydatidiform
mole was more common than PHM in Morocco, reflecting a reversal to the pattern seen in the
Jos GTD series.

39
Additionally, the profile of gestational trophoblastic disease studied in South Africa revealed
that choriocarcinoma accounted for 30% in a particular series44, which is almost comparable to
the 27.8% observed in JUTH, Jos.
In Ethiopia, choriocarcinoma was reported to have accounted for 15.1% of the cases analyzed,
invasive mole accounted for 13.9% and CHM was diagnosed in 72% of cases, making it the
most common histologic subtype reported by Negussie et al33. However no cases were recorded
of partial hydatidiform mole or placental site trophoblastic tumor.
It is curious that PHM turned out to be the most common histopathologic subtype of GTD seen
in this study. In a case-control study by Berkowitz et al52, the observation made was that there
is a difference in the epidemiologic patterns of complete and partial hydatidiform moles. The
risk for PHM is associated with reproductive history, but not with dietary history as
observed for CHM, which might serve to explain the pattern observed, of the GTD cases
reviewed in Jos. Risk factors according to these authors that may predict the development of
partial hydatidiform mole include:
i. Irregular menstrual cycles,
ii. Oral contraceptive use for more than four years,
iii. Previous pregnancy history including only male infants among prior live births.
Albeit, dietary factors previously postulated for CHM such as protein, fat, vitamin-A or
carotene were found not to be related to the risk for PHM. It is therefore probable that some of
the above given risk factors could have been present in the majority of the population studied,
to have made PHM the most prevalent or most common histological pattern of GTD observed
in this study. Nevertheless, this observation can provide an area of interest for further

40
collaborative clinicopathological studies on this subject matter, between Gynaecologists and
Pathologists, both in our centre and elsewhere.
Choriocarcinoma turned out to be the second most common pattern seen, of the GTD series
analyzed in our centre, with peak incidence reported in the third decade of life. The single case
of choriocarcinoma seen in a 65 year old woman stood in isolation as none gestational
choriocacinoma. Some risk factors that have been established to predict its development
include the following:
i.History of spontaneous miscarriages or ectopic pregnancies17,27.
ii.Advanced/ advancing maternal age49.
iii.Prior complete hydatidiform mole; an observation made was that, choriocarcinoma was a
thousand times more likely after a CHM, than it was following another normal pregnancy
event49.
iv.Ethnicity; the risk for choriocarcinoma is also increased in Asian women, those of
American-Indian descent, and African Americans49.
v.There seems to be increased risk in women on long term oral contraceptive pills, as well as
those of blood type-A.
Our study population was primarily of Black women, although we couldn’t define other risk
factors for choriocarcinoma. Hence, another basis for future collaborative studies is suggested
between Pathologists and Clinicians in this area of interest, moreso that a high cure rate is
associated with this lesion in particular.
41
Conclusion
In conclusion our study has found gestational trophoblastic diseases to be a common condition
in Jos in general, and PHM in particular was found to be the commonest histologic subtype,
closely followed by choriocarcinoma. While the molar lesions peaked in the third and fourth
decades, choriocarcinoma peaked in the third decade of life.

42
Recommendations
From the observation made in this study and few others carried out previously, the following
recommendations are suggested.
1. Awareness programmes should be extended to all women of the reproductive age group
to report and register all pregnancy-like and pregnancy events at the nearest facility for
proper follow-up.
2. The study recommends the use of p57 immunohistochemistry or marker, and some
aspects of cytogenetics to specifically delineate tissue sampled from hydropic abortion
and complete and partial hydatidiform moles.

43
REFERENCES
1. Rosai J. Pregnancy, Trophoblastic Disease and Placenta. Rosai and Ackerman’s Surgical
Pathology. Tenth Edition, St.Louis Washington, Elsevier. 2011; 1636-1645.
2. Shih I. Gestational Trophoblastic Neoplasia; Pathogenesis and potential therapeutic targets.
Lancet Oncol 2007; 8:642 – 650.
3. Hertig AT. Hydatidiform mole and chorionepithelioma In: Meigs JV, Sturgis SH, editors.
Progress in Gynaecology, Vol. Two, New York City, Grune and Stratton. 1950; 372-394.
4. Hsu CT, Chen TY, Chiu WH, Yang CC, Lai CH, Chancheng CH, et al. Some aspects of
trophoblastic diseases peculiar to Taiwan. Am J Obstet Gynaecol 1964; 90: 308-316.
5. Berkowitz RS, Goldstein DP. Chorionic tumours. N Engl J Med 1996;335: 1740-1748.
6. Li HW, Tsao SW, Cheung AN. Current Understanding of the Molecular Genetics of
Gestational Trophoblastic Disease. Placenta 2002; 23: 20 – 31.
7. Shih IM, Kurman RJ. Molecular Basis of Gestational Trophoblastic Disease. Curr Mol Med
2002; 2:1–12.
8. Anuma ON, Umeora OUJ, Obuna JA, Agwu UM. Profiling Gestational Trophoblastic
Diseases in a Tertiary Hospital in South East Nigeria. Trop J Obstet Gynaecol 2009; 26:
157-164.
9. Mbamara SU, Obiechina NJ, Eleje GU, Akabuike CJ, Umeononihu OS. Gestational
Trophoblastic Diseases in a Tertiary Hospital in Nnewi, South-East Nigeria. Niger Med J
2009; 50(4):87–89.
10. Robert M, Krista J, Debra H. Characteristics of patients who present to the Emergency
Department with Molar pregnancy. Southern Med J 2008; 101(8): 797-799.
11. Dim CC, Ezegwui HU. Choriocarcinoma in Enugu, South-East Nigeria; A need for a shift
from mortality to survival. Niger J Med 2013; 22(2): 123-127.

44
12. Yakasai IA, Adamu N, Galadanchi HS. Ruptured tubal molar pregnancy. Niger J Clin
Pract 2012; 15:491-493.
13. Seleye-Fubara D, Uzoigwe SA. Pattern of primary female genital cancers in Port-Harcourt,
Nigeria: A twelve year Review. Sahel Med J 2003; 6(2):34-39.
14. Bitterman P. Female Reproductive System In: Gattuso P, Reddy V, David O, Spitz DJ,
Haber MH, editors. Differential Diagnosis in Surgical Pathology. Second Edition,
Philadelphia, Elsevier. 2010; 694-699.
15. Aziz N, Yousfani S, Soomro I, Mumtaz F. Gestational Trophoblastic Diseases. J Ayub Med
College Abbottabad 2012; 24(1): 7-9.
16. Nwana EJC. Chorionic tumours or Gestational Trophoblastic Tumors In: Lectures
Delivered at the update/revision course. National Postgraduate Medical College of Nigeria,
Faculty of Pathology. National Hospital Abuja: March 2012.
17. Yang JJ, Xiang Y, Wan XR, Yang XY. Prognosis of Malignant Gestational Trophoblastic
Neoplasia: 20 years of experience. J Reprod Med 2008; 53: 600-607.
18. Schorge JO. Gestational trophoblastic diseases In: Schorge JO, Halvorson LM, Schaffer JI,
Hoffman BL, Bradshaw KD, Cunningham FG, editors. Williams Gynaecology. Second
Edition, New York city, McGraw Hill. 2008; 755–768.
19. Lurain JR. Gestational Trophoblastic Diseases; Epidemiology, Pathology, Clinical
presentation and Diagnosis of GTD, and Management of Hydatidiform moles. Am J Obstet
Gynaecol 2010; 203: 531-537
20. DiSaia PJ, Creasman WT. Gestational Trophoblastic Neoplasia. Clinical Gynaecologic
Oncology. Third Edition, St Louis, The C.V. Mosby Company. 1989; 214–238.
21. Lewis JL. Treatment of Metastatic Gestational Trophoblastic Neoplasms; A brief review of
development in the years 1968 to 1978. Am J Obstet Gynaecol 1980; 136:163–172.
45
22. Philip R, Jackson BB, Frederick H. Tumours of the Female Reproductive Organs.
Clinical Oncology for Medical Students and Physicians; A multidisciplinary Approach.
Sixth Edition, New York city, The American Cancer Society. 1983; 454 – 457.
23. Hertig A, Mansell H. Tumors of the female sex organs, part I; Hydatidiform mole and
choriocarcinoma. Ann Intern Med 1958; 48(2): 442-442.
24. Moore LE, Hernandez E. Hydatidiform mole. eMedicine Obstetrics and Gynaecology.
Pritzker JG, editor. Medscape. 2 Nov 2009. Cited on 20 Sept 2014. Available at:
http://emedicine.medscape.com/article/405778-overview.
25. Graham HI, Fajardo AM, Richards RL. Epidemiological study of Complete and Partial
Hydatidiform Moles in Abu Dhabi; Influence of age and ethnic group. J Clin Pathol 1990;
43: 661-664.
26. Kaye DK. Gestational Trophoblastic Diseases following Complete Hydatidiform Mole in
Mulago Hospital Kampala, Uganda. Afr Health Sci 2002; 2: 47–51.
27. Chechia A, Koubaa A, Makhlouf T, Anis B, Terras K, Hamouda B. Molar pregnancy; A
Retrospective study of 60 cases in Tunisia. La Tunisie mèdicale 1979; 8: 441–446. Cited on
21 Sept 2014. Available at: www.unboundmedicine.com/medline/citation
28. Ocheke AN, Musa J, Uamai AO. Hydatidiform mole in Jos, Nigeria. Niger Med J 2011;
52: 223–226.
29. Lifshitz S, Outhouse C, Buchsbaum HJ. Malignant Gestational Trophoblastic Disease. J
Iowa Med Society1977; 67: 391–395.
30. Lai CY, Chan K, Khoo US, Ngan HY, Xue W, Chui MP. Analysis of gestational
trophoblastic diseases by genotyping and chromosome in situ hybridization. Mod Pathol
2003; 17: 40-48.

46
31. Mayun AA, Rafinadadi AH, Shehu MS. Choriocarcinoma in Northwestern Nigeria; A
Histopathological Review. Niger Postgrad Med J 2012; 19:215-218.
32. Aligbe JU, Ekanem VJ, Akhiwu WO, Banjo AA. Gestational Trophoblastic Diseases
(GTD); a 10-year review of clinicopathological features of cases seen at University of
Benin Teaching Hospital, Benin city. Annals Biomed Sci 2002;1:94–99.
33. Negussie D, Belachew T. Profile of Gestational Trophoblastic Diseases in Two Teaching
Hospitals in Addis-Ababa, Ethiopia. Ethiopia J Health Sci 2008; 17: 195-201.
34. Cortes-Charry R, Figueira LM, Garcia-Barriola V, de Gomez M, Vivas Z, Salazar A.
Gestational Trophoblastic Neoplasia; Clinical trends in eight (8) years at the Hospital
Universitario de Caracas. J Reprod Med 2006; 51: 888-891.
35. Mayun AA, Rafindadi AH, Shehu MS. Pathomorphology of Molar Gestation in Zaria.
Niger Med J 2010; 51: 1–4.
36. Mohammed A, Ahmed SA, Oluwole OP, Avidime S. Malignant tumours of the female
genital tract in Zaria, Nigeria: Analysis of 513 cases. Annals Afr Med 2006; 5: 93–96.
37. Nggada HA, Odike M, Ojo BA. Gestational Trophoblastic Diseases in Nigeria: A
multicentered histopathological study. Highland Medical Research Journal 2005; 3:81–86.
38. Eniola OA, Mabayoje P, Ogunniyi SO. Hydatidiform mole in Ile-Ife, Nigeria; A ten year
review. J Obstet Gynaec 2001;21: 405–407.
39. Osmor JO, Oluwasola AO, Adewole IF. A clinicopathological study of complete and partial
hydatidiform moles in a Nigerian population. J Obstet Gynaec 2002;22:423-425.
40. Equatu VE, Ozumba BC. Observation on molar pregnancy in Enugu, Nigeria. Intl J
Gynaecol Obstet 1989; 29: 219–225.

47
41. Garrett LA, Garner EI, Felmate CM, Goldstein DP, Berkowitz RS. Subsequent Pregnancy
outcomes and persistent Gestational Trophoblastic Neoplasia. J Reprod Med 2008; 53:
481–486.
42. Rees HC, Paradinas FJ. The Diagnosis of Hydatidiform mole in early tubal ectopic
pregnancy. Histopathology 2001;39: 320–321.
43. Curry SL, Hammond CB, Tyrey L, Creasman WT, Parker RT. Hydatidiform mole. Obstet
and Gynaecol1975; 45: 1–8.
44. Snyman LC. Gestational Trophoblastic Disease; An Overview. South Afr J Gynaecol Oncol
2009; 1(1): 32-36.
45. Moodley M, Tunkyi K, Moodley J. Gestational Trophoblastic Syndrome; An audit of 112
patients, A South African experience. Intl J Gynaecol Cancers 2003; 13: 234–239.
46. Boufettal H, Coullin P, Mahdaoui S, Noun M, Hermas S, Samouh N. Partial Hydatidiform
mole in Morocco; An epidemiological and clinical study. Eastern Mediterranean Health J
2012; 18(7): 755-761. Cited on 22/9/2014.
Available at: www.unboundmedicine.com/medline/citation
47. Boufettal H, Coullin P, Mahdaoui S, Noun M, Hermas S, Samouh N. Complete
hydatidiform mole in Morocco; Epidemiological and clinical study. Journal de
Gynaecologie, obstetrique et biologie de la reproduction (J Gynaecol, Obstet Biol
Reprod)2011; 40(5):419–429. Cited on 22/9/2014.
Available at: www.unboundmedicine.com/medline/citation.
48. Othieno-Abinya NA, Ndirangu G, Mueke S, Nyongesa C. Gestational Trophoblastic
Disease. National Guidelines for Cancer Management, Kenya Nairobi. Ministry of Health.
2013: 105–107.
48
49. Lok CA, Ansink AC, Grootfaam D, van der Velden J, Verheijen RH, ten Kate-Booij MJ.
Treatment and prognosis of post term choriocarcinoma in the Netherlands. Gynaecol Oncol
2006;103:698–702.
50. Izhar R, Un-Nisa A.Prognosis of Gestational Choriocarcinoma at Khyber Teaching
Hospital Peshawar. J Ayub Med College Abbottabad 2003; 15:45-48.
51. Mayun AA. Hydatidiform mole in Gombe; a five year histopathological review. Niger J
Clin Pract 2008; 11: 134-138.
52. Berkowitz RS, Bernstein MR, Harlow BL, Rice LW, Lage JM, Goldstein DP et al. Case
Control Study of risk factors for partial molar pregnancy. Am J Obstet Gynaecol 1995; 173:
788-792.

49
APPENDIX A
Modified World Health Organization (WHO) Classification of Gestational Trophoblastic
Diseases (2002)18
MOLAR LESIONS
Hydatidiform mole
- Complete hydatidiform mole (CHM)
- Partial hydatidiform mole (PHM)
Invasive mole
NON MOLAR LESIONS
Choriocarcinoma
Placental-site trophoblastic tumour (PSTT)
Epithelioid trophoblastic tumour (ETT)
NB Gestational trophoblastic neoplasia (GTN) is a term used for a subset of gestational
trophoblastic diseases that develop malignant sequelae18.

50
APPENDIX B