mostly medicaid summer 2009 issue
DESCRIPTION
The Great Healthcare Reform Debate - Page 8 CHIP Update - Page 15 Enrollment Keeps Going Up - Page 3 Job Listings - Page 12 Hospitals Fighting to Survive - Page 4 Medicaid Crossword - Page 17TRANSCRIPT

Jeyaram & Associates offers extensive healthcare legal expertise found at larger, more expensive firms at more reasonable costs with a higher degree of service. Our areas of expertise include:
Jeyaram & Associates is an AV rated firm. "The AV Peer Review rating . . is a reflection of the firm's expertise, experience, integrity and overall professional excellence." – LexisNexis letter of 1/3/08
For more information call 404-995-6792
or visit our web-site at
www.jeylaw.com
• Integrity audits • Administrative
hearings • Contracts • HIPAA • Fraud and abuse
• Medicaid and Medicare provider issues
• Stark, Anti-Kickback and False Claims
• Physician licensure • CON/LNR • Recovery Audit Contractor
and Program
And the Medicaid Rolls Just Keep Growing and
Growing…..
We have been watching the rolls increase for several months now, waiting for the recession to take full
effect. From what we’re seeing in Arizona and Colorado, it looks like the impact of job losses is starting
to show up in Medicaid.
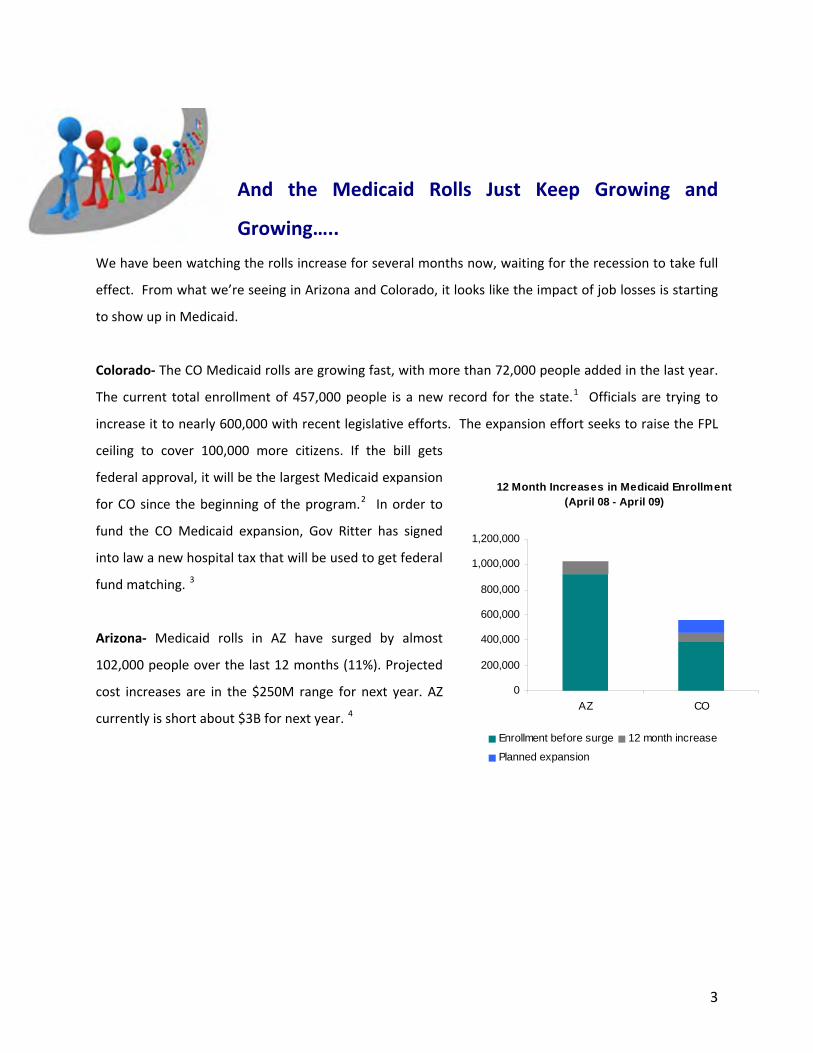
Colorado‐ The CO Medicaid rolls are growing fast, with more than 72,000 people added in the last year.
The current total enrollment of 457,000 people is a new record for the state.1 Officials are trying to
increase it to nearly 600,000 with recent legislative efforts. The expansion effort seeks to raise the FPL
ceiling to cover 100,000 more citizens. If the bill gets
federal approval, it will be the largest Medicaid expansion
for CO since the beginning of the program.2 In order to
fund the CO Medicaid expansion, Gov Ritter has signed
into law a new hospital tax that will be used to get federal
fund matching. 3
12 Month Increases in Medicaid Enrollment (April 08 - April 09)
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
AZ CO
Enrollment before surge 12 month increase
Planned expansion
Arizona‐ Medicaid rolls in AZ have surged by almost
102,000 people over the last 12 months (11%). Projected
cost increases are in the $250M range for next year. AZ
currently is short about $3B for next year. 4
3
Hospitals Fighting to Survive in the Economy: Medicaid and the
Summer Squeeze of 2009
According to a survey conducted by the American Hospital Association (AHA), hospitals across the country are taking drastic measures to survive in the recession, including reducing services like patient education and clinics. Key financial metrics like days cash on hand are "slipping" and may signal a time in the near future when creditors call in chips. http://www.aha.org/aha/content/2009/p
df/090427econcrisisreport.pdf
We take a look at some on the ground examples in 7 states:
Washington‐ Hospitals in WA say the state owes them money for
patients whom Medicaid should have covered and who received
services from 1994 to 2009. 18 hospitals are suing the state for $31M
in back payments. This case is one of many across the country that
seeks similar payments, but it is considered to be the strongest one
out there currently. If the hospitals win this one in WA, expect many
more to follow across the nation. In 1995, Medicaid accounted for
about 90% of WA hospital revenues ‐ now its about 83%.5
Nevada‐ Hospitals are phasing out services to deal with the economic recession. University Medical
Center of Southern Nevada has closed its mammography center and plans to start shutting down its
outpatient cancer program in 4Q09. The $30M in overall state Medicaid cuts are seen as a contributing
factor.6
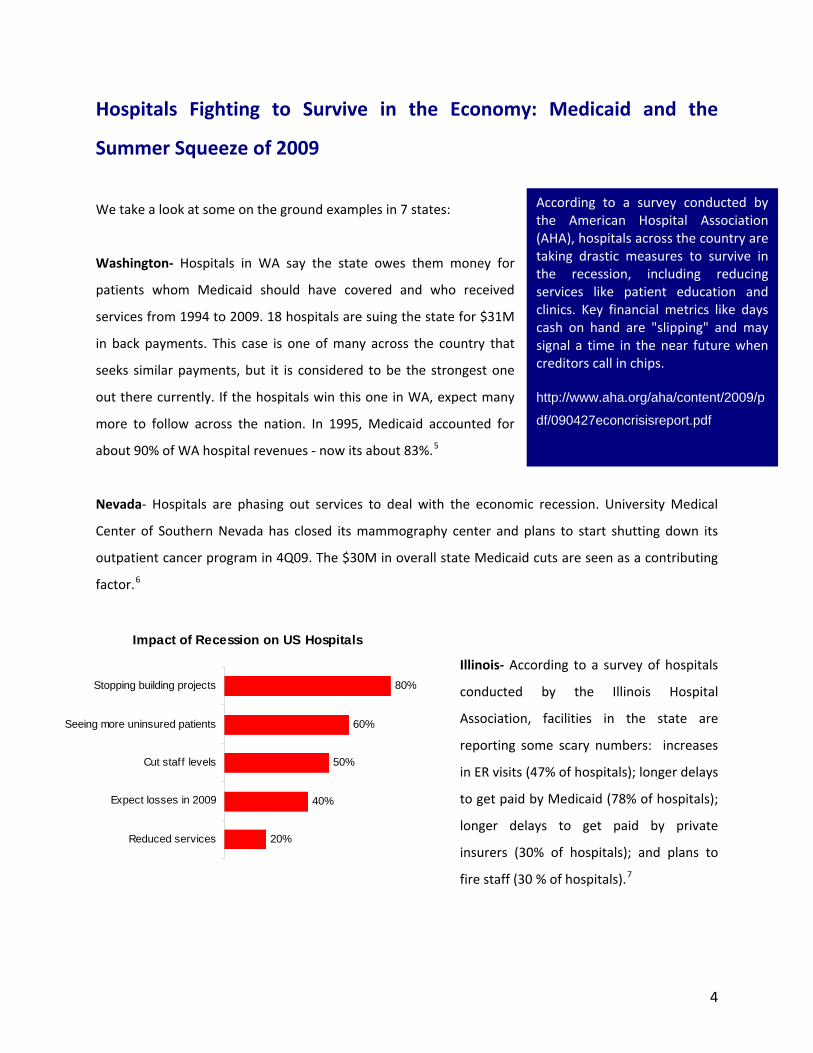
Impact of Recession on US Hospitals
20%
40%
50%
60%
80%
Reduced services
Expect losses in 2009
Cut staff levels
Seeing more uninsured patients
Stopping building projects
Illinois‐ According to a survey of hospitals
conducted by the Illinois Hospital
Association, facilities in the state are
reporting some scary numbers: increases
in ER visits (47% of hospitals); longer delays
to get paid by Medicaid (78% of hospitals);
longer delays to get paid by private
insurers (30% of hospitals); and plans to
fire staff (30 % of hospitals).7
4

Idaho‐ Medicaid hospital rehab providers
got a stay of execution in late April when a
judge blocked reimbursement cuts (some as
high as 55%). The judge gave a 3 week
reprieve, and arguments were scheduled to
resume in late May.8
Utah‐ Medicaid is slashing hospital
reimbursement this July 1, with most
facilities staring down the barrel of a 25%
cut. Making it worse is the fact that most
hospitals are not really prepared ‐ a
temporary plug was found to avoid the cut
last year so it did not hit the radar. Hope
still persists, with some lawmakers
suggesting the use of tobacco tax increases
or perhaps raiding a special fund for about
$9M.9
Massachusetts‐ Nearly 2/3 of MA hospitals
are reporting drops in profit margins,
largely due to reductions in elective
surgeries and other delayed care. The
average facility has lost more than 50% of
its margin‐ plummeting from 0.7% in 4Q08
down to 0.3% in 1Q09. Jobs are
disappearing and new clinics and other
expansions are on hold. Caritas Christ is
laying off 160 people. Lahey Clinic has
tabled plans to build a new $100M facility.
Some MA hospitals report no decline in
volume, but have seen less waiting time for
patients. 10
Pennsylvania‐ PA hospitals are getting
crushed as the state reckons with a $3B
deficit. Profit has dropped 13% for the
average PA hospital since December 2007,
and the proposed $75M in cuts for FY 2010
are expected to turn a crisis into a
catastrophe for hospitals. Most of the cuts
are to supplemental payments above and
beyond standard PA Medicaid rates. Stories
of decline at individual hospitals give a
sense of the state as a whole:
Univ of Pittsburgh Medical Center has seen
revenue decrease 3% and fired 500
employees.
West Penn Allegheny Health System had a
$9M loss in 2Q09. 11
Your Ad Here
FREE The fine print: all you have to do is write an article for an upcoming issue, or join our blog team. Paid ads
also available at low rates.
Email us for more info [email protected]
5

More news over at the Mostly Medicaid Blogs
blog.mostlymedicaid.com where the best Medicaid minds mingle.
recent entries New use of the old healthcare fraud statute
It’s getting ugly‐ cuts across the states Provider taxes everywhere! CMS should reconsider Colonoscopy decision Stimulus strings attached EHR updates Medicaid fraud news
Now we’re on Facebook and Twitter, too! Look us up searching “medicaid” or “mostly medicaid”
6

The Great Healthcare Reform Debate: The 4 Critical Obstacles to Reform that No One is Taking Seriously Enough
Everyone is all abuzz with the possibility that the full‐scale, national health
reform dream will happen give convergence of key current events. A
President has been elected that will push for it. We learned from Hillary’s
mistakes 15 years ago, and she is on today’s team to make sure we don’t
forget. The global economic crisis has brought the middle class to the brink
of actually facing the costs of their own coverage and maybe even losing it.
And – in an astounding move – major stakeholders who profit from US
healthcare spending have gone on record volunteering to take a $2T hit to
make the reform plans work.
It all seems to add up to a slam‐dunk.
But there are key problems and obstacles that we are not engaging in the
debate. And by “we”, we mean the vast majority of us who make our living
from being connected to the U.S. healthcare industry – and happen to also
be predominantly Democrats. There’s no denying it (and no need to). But
sometimes the political ideology keeps our heads in the sand when
confronted with real barriers to our goals.
The 4 Critical Obstacles We Need to Take More Seriously
#4 – No one really believes the industry will sacrifice trillions in profit.
Trust is key to getting the nation to provide the faith needed to embark
on a reform journey that will take at least decades. The surprising
announcement that key US health industry players would forego $2T in
revenues (via spending cuts) to make Obama's health care proposal work
was, well, surprising. Voices on both sides of the aisle are skeptical. Besides
the fact that these same groups have historically fought the very same
8
This is a 20 page report that covers the role Medicaid may (or may not) play in any reform plans. The report points out the impact Medicaid costs play in the overall trends, but also that a whole separate set of issues emerge when reformers realize that Medicaid may need to be "folded into new insurance arrangements." The report also makes the key point that the line between public and private coverage has often become blurred in America. Finally ‐ the report covers lots of ground, including an overview of the reform bills (and related committees) already in play. This report is a great way to get up to speed quickly on the reform talk today. Other Sources The Washington Post also started a new section on the healthcare reform debate‐ http://voices.washingtonpost.com/health‐care‐reform/ Marilyn Werber at the National Journal threw out 2 key topics to several heavy hitters in health economics today. In addition to asking if the estimated $2.7B in savings from increased fraud prevention efforts are realistic, she also asked commenters to weigh in on the plausibility of the now famous health industry‐volunteered $2T in savings to make health reform work. The comments come from the likes of John Goodman, Uwe Reinhardt, Denis Cortese, and Chuck Grassley. For anyone interested in various perspectives on the industry's claims to put some skin in the game ‐ this read is a gold mine. http://healthcare.nationaljournal.com/2009/05/policing‐medicare‐fraud‐worth.php
An Overview of Where the Debate is Today – Read this Report Whitepapers and primers on healthcare reform are popping up everywhere. The folks at Healthjournalism.org have done a good job of boiling the debate down to 3 main issues ‐ 1. Coverage‐ Roughly 1 in 7 people were without it in 2007 and Americans in general are starting to care. 2. Cost and Spending ‐ It's eating up GDP (16% in 2008) and its scaring retirees. 3. Quality ‐ American medicine is in the middle of the global pack on this one, despite the high price tag.
Its (one of) the elephant(s) in the
healthcare room. Innovative
fixes whose effectiveness is
unknown and won't be for
decades aside ‐ Medicare is
broke and we all know it. We
have for a while now, and we
just have to simply face it.
proposed savings measures, analysts just don't believe that insurers, providers
and others will sacrifice their own economic self‐interest to make this all work.
Others feel that the announcement itself was the accomplishment (or tactic
depending on who you listen to). In other words, they believe the press
conference showing the American Medical Association, American Hospital
Association, the Pharmaceutical Research and Manufacturer's Association all
reaching consensus on a voluntary $2T pay cut sent a strong message of progress ‐
whether or not its impossible to actually achieve.12
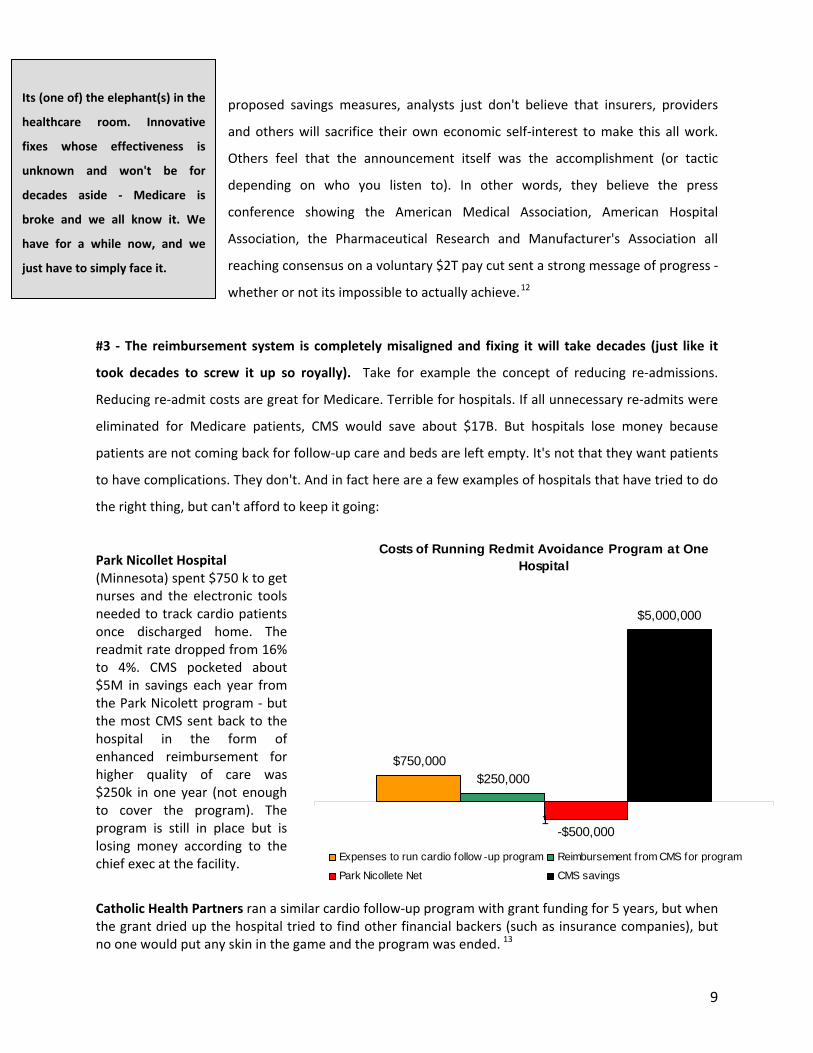
#3 ‐ The reimbursement system is completely misaligned and fixing it will take decades (just like it
took decades to screw it up so royally). Take for example the concept of reducing re‐admissions.
Reducing re‐admit costs are great for Medicare. Terrible for hospitals. If all unnecessary re‐admits were
eliminated for Medicare patients, CMS would save about $17B. But hospitals lose money because
patients are not coming back for follow‐up care and beds are left empty. It's not that they want patients
to have complications. They don't. And in fact here are a few examples of hospitals that have tried to do
the right thing, but can't afford to keep it going:
Costs of Running Redmit Avoidance Program at One
Hospital
$750,000$250,000
-$500,000
$5,000,000
1
Expenses to run cardio follow -up program Reimbursement from CMS for program
Park Nicollete Net CMS savings
Park Nicollet Hospital (Minnesota) spent $750 k to get nurses and the electronic tools needed to track cardio patients once discharged home. The readmit rate dropped from 16% to 4%. CMS ocketed about $5M in savings each year from the Park Nicolett program ‐ but the most CMS sent back to the hospital in the form of enhanced reimbursement for higher quality of care was $250k in one year (not enough to cover the program). The program is still in place but is losing money according to the chief exec at the facility.
p
Catholic Health Partners ran a similar cardio follow‐up program with grant funding for 5 years, but when the grant dried up the hospital tried to find other financial backers (such as insurance companies), but no one would put any skin in the game and the program was ended. 13
9

June 8-10, 2009 Hyatt Regency, Baltimore, MD
www.MMCCongress.com
Special Thanks to Featured Media Partner
CONFIRMED: Senator Tom Daschle to Speak at MCC
Senator Tom Daschle, Former Senate Majority and Minority Leader, has confirmed his keynote session on Solving the Healthcare Crisis for Tuesday, June 9, 2009.
Keynote and Featured Speakers
Philip M. Bonaparte, MD Vice President of Clinical Affairs, Horizon Blue Cross Blue Shield of New Jersey, Chief Medical Officer HORIZON NJ HEALTH
Carolyn Ingram Director, Medical Assistance Division NEW MEXICO DEPARTMENT OF HUMAN SERVICES
Anthony Rodgers Director ARIZONA HEALTH CARE COST CONTAINMENT
Bruce Johnson Technical Director, Division of Benefits, Eligibility and Managed Care CMS
Medicaid Managed Care Congress
17th Annual
Next Gen Medicaid Managed Care – Optimizing Quality, Access and Efficiency
What is Changing for 2009• Medicaid Reform Roundtable with representation
from the Obama Administration
• Medicaid 101 Workshop for Healthcare Executives New to Medicaid, Managed Care or in Need of a Refresher
• Strategies to Improve Health Literacy to Affect True Behavioral Change
• Tools to Implement a Comprehensive Program to Track, Report and Reduce Never Events
• Opportunities to Leverage the Medical Home Model in Medicaid
• Expanded State Medicaid Director and Health Plan CEO Panels
PTi international is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
This event is jointly sponsored by CME LLC and the Institute for International Research.
Accreditations
20+ States Represented!
‘09www.MostlyMedicaid.com

#2 Thinking that US taxpayers might pay more than they do now to cover other people may ignore a
growing lower‐my‐taxes movement. It certainly ignores that the recession is hitting taxpayers just as
hard as everyone else. One health reform proposal in the US Senate would have taxpayers paying even
more to fund Medicaid, albeit indirectly. The Senate Finance Committee is considering whether to
remove the current tax‐exempt status of employer‐sponsored health coverage. Obama opposes this
(largely due to labor unions ties) as way to achieve reform, but advocates like the Kaiser Commission on
Medicaid and the Uninsured say 21M more Americans could have health insurance if another $19B can
be found somewhere in the budget. Other advocacy groups like the Center on Budget and Policy
Priorities (CBPP) further elaborate the fiscal justice position. The director of CBPP believes the current
tax‐exempt status of employer‐sponsored health coverage "gives the greatest benefit to . . . the group
that needs the least help paying for health insurance." Max Baucus brings the debate back to reality
when he reminds us that mechanisms that increase the burden on taxpayers (like raising the price of
their own healthcare by 30% by taxing it) are of little use for forging healthcare reform that works.14
Don’t count on taxpayers taking this one sitting down.
#1 – It just may be that the numbers really don’t add up and maybe
never will. As much as advocates, academics, Democrats and those
who profit from the US healthcare industry believe that reform (and
ultimately universal coverage) should happen, it may not be actually
possible from a fiscal viewpoint. Until this harsh possibility is at least
considered possible, efforts making the should match the is will
continue to waste time and resources that could be geared toward a
different movement with similar objectives.
Think its really just a simple exercise in finding the money or moving it around? Take a look at Medicare
and SSI. Fundamental deficiencies in the basic financing model of these two programs have made one
thing clear to the average American – you can not keep spending money you do not have forever. The
economic meltdown has reinforced this. Asking Americans to believe anything different will eliminate
credibility. Reform’s best hope –maybe it’s only hope – is if we can be transparent and simple enough in
our reform efforts to win back the faith of an American populace who will be paying for this thing for
11

generations. The Americans who signed off on SSI and Medicare and Medicaid 70 and 40 years ago
were much less jaded than Americans today.
Not only is Medicare going broke (and broker), Social Security is set to be bust in 2016. The insolvency
dooms‐day for each of these programs is now projected 2 years closer than was projected last year. The
WSJ makes a mind‐blowingly simple observation. If $13T (the current Medicare hospital deficit) were
put in an interest bearing account today, Medicare would be funded until almost the next century
(2084).
That was just the Medicare hospital fund. When you look at all parts of Medicare (doctors services,
drugs, etc) the amount of money Medicare owes but does not have is almost $38T. According to one
analyst, that is more than twice the size of the entire U.S. economy. Spread to each household, each US
family owes about $325k to cover Medicare. Social Security is bad off, but not as bad as Medicare. (SSI
owes about $5.3T over the next 75 years). According to Geithner, once healthcare reform is completed,
SSI reform is next.15
The recently released Medicare
Trustees report just could not go
unanswered. HHS Secretary Sibelius
issued an official commentary on the
underlying message of the report. She
calls it a wake‐up call" for people
concerned about healthcare in
America, and vows (on behalf of
Obama) that "whatever it takes to
protect it" will be done. You have to
wonder if that is actually possible.
Current Unfunded Obligations of Medicare and SSI Compared to Size of US Economy (all in $ trillion)
$38
$19
$5
-$24
Medicare UnfundedObligations
US Economy SSI UnfundedObligations
Net
"
Sibelius covers the more ominous data from the report. Medicare is in the hole today. Not ten years
from now. It is spending more than it takes in and government officials are using fund balances to fill the
gap. In 2017 they will run out of band‐aids and Medicare retirees will face premiums that more
12

realistically reflect the cost of their care. No one has admitted yet that they may just lose coverage
alltogether.
If we sound skeptical, its because we are. We agree that this is a crisis (it's easy to agree with the
obvious). We just don't believe rhetoric and vague new funding mechanisms will generate the cold, hard
cash needed to get us out of the mess. 16 Now get out there and come up with some better ideas.
FREE The fine print: all you have to do is write an article for an upcoming issue, or join our blog team. Paid ads
also available at low rates.
Email us for more info [email protected]
Your Ad Here
13

What if you could identify your frail members?
The Power of Information • A web-based tool, the HRAPlus screens and identifies in-home, high-risk members
• The tool generates a reliable and objective measure of function and risk to establish someone’s specific
needs on a daily basis
• Such information helps care managers allocate appropriate member management resources which al-
lows for early intervention in maintaining a safe living environment
The Clout of Evidence • Based on 400,000+ clinical cases in this web-based tool, HomeSafe is a comprehensive in-home assess-
ment of identifying members for risk factors
• With 350 different data elements, the HomeSafe assessment produces a detailed summary for care plan-ning
• The HomeSafe application includes automated reporting for identifying individual risk factors and care needs
To see how others have benefited from this one-of-a-kind technology, email [email protected] or call 866.755.3374 www.seniormetrix.com
For the first time in health care, an objective and evidence-based resource is available to accurately determine high-risk members and manage their risks associated with frailty. SeniorMetrix, pioneers in predictive modeling, introduces its newest technical solutions – HRAPlus and HomeSafe – de-signed with caregivers and health plans in mind.

CHIP UPDATE SUMMER 2009
We look at what 4 states are doing with their
CHIP programs:
North Dakota‐ North Dakota shut down
attempts to expand its CHIP using an increased
Federal Poverty Level ceiling of 200%. Right
now 150% of FPL is the cut‐off.17
Iowa‐ With one piece of legislation, Iowa just
moved to the front of the line in terms of states
with the highest percent of kids covered. In fact
its just about 100% now that the 53,000
remaining uninsured kids are covered under a
bill passed with widespread and bi‐partisan
support. The initial price tag was about $10M,
but with CHIPRA (see the sidebar below) putting
more cash on the table, its more like $7.5M.18
Hawaii‐ Usually CHIP programs face challenges
like caps in enrollment or funding shortfalls.
Hawaii's Keiki Care is fighting just to exist. It got
started in mid‐2008 but was shut down by the
Governor who felt it covered families who could
afford insurance anyway. Dems in the Hawaii
legislature are looking for ways around a veto
this time around, inserting about $600k in the
state budget for Keiki Care in FY 2010.19
Texas‐ Dems are trying to double the current TX
CHIP coverage period (from 6 to 12 months) to
try and ensure 250,000 kids would be covered.
Right now their parents have to re‐apply every
six months to prove they are still eligible, and
advocates claim this "beaurocratic hurdle"
reduces the rolls unnecessarily. Opponents say
that without the required reapplication, you
can't be sure that only the neediest kids get
care. Doubling the time that beneficiaries can
go without re‐applying is estimated to cost TX
another $300M in state funds (but would
leverage the match to get another $500M in
federal funds). 20
15
Under the CHIP Reauthorization Act (CHIPRA), states can get a higher federal match if they exceed their enrollment targets AND implement 5 of 8
policies near and dear to the feds. The enhanced FMAPs can be as high as 92%. The strings attached include continuous enrollment targets, not
having asset tests and other items. The days of exceeding your CHIP enrollment goals and then being punished with an enrollment cap or funding
shortfall may just be over. Check out the full report for more details‐ www.kff.org/medicaid/upload/7884.pdf

Mostly Medicaid LinkedIn Group Has Passed 450 Members! In less than 10 months the Mostly Medicaid group on LinkedIn has skyrocketed to 450+ members. This makes the Mostly Medicaid group the largest group on LinkedIn that connects Medicaid industry professionals for sales opportunities, job openings and knowledge sharing. Our members include Medicaid directors, hospital executives, industry analysts, government officials, consultants, and many other leading professionals in the Medicaid industry. Mostly Medicaid is a group of hundreds of Medicaid industry professionals who network and share information. If you are involved in the Medicaid industry, we have a spot for you at our ever‐growing table! Go to linkedin.com and search groups using “Medicaid” to find us and join.
16
Medicaid Crossword Summer 2009
Across 3. One of the 4 obstacles to reform, according to Mostly Medicaid 4. Medicare _______ Report. Report that recently predicts Medicare will be insolvent in 8 years 8. State that does not have a CHIP program 9. Big word in Medicaid policy today, and focus of this issue of the MM newsletter 13. State where hospitals just received a 25% cut in Medicaid reimbursement 14. State where one hospital is closing a mammography center 15. The word for when the enrollment increase is planned
Down 1. North ________. State that just pulled out of efforts to increase the CHIP FPL floor to 200%. 2. State where hospitals are suing Medicaid agency for back payment for services to the indigent 3. % of US hospitals who have reduced services during the recession 5. One word for what has occurred in Medicaid enrollment in the past 12 months 6. The act that brought CHIP back 7. _______-sponsored coverage. the senate finance committee is considering taxing this for the first time 10. % of US hospitals who expect to post a loss in 2009 11. One of the 3 keys to the reform debate, according to healthjournalism.org 12. State with the highest % of kids covered
17

Job Listings Hey‐ We know it’s tough out there. Here’s a few Medicaid‐specific opportunities.
If you are interested in more specific details about any of the positions below, please contact Eve Crane &
Associates Inc via email: [email protected]
Clinical Product Designer
Location: South
Licensed RN with a minimum of a bachelor's degree
(masters' preferred) OR a Masters' level professional
with public health background and extensive
experience in behavior change and health education.
Project Management
Product Development
Knowledge of Technical healthcare systems
Medical Director
Location: East Coast
JOB SUMMARY: Oversees all medical care for
Company products and services. Oversees the health
care needs of the membership and serves as the
principal medical manager and policy advisor to the
company and health plan CEO or COO. Is
accountable for and provides professional leadership
and direction to the utilization/cost management
and clinical quality management functions. Works
collaboratively with other plan functions that
interface with medical management such as provider
relations, member services, benefits and claims
management, etc. Assists in short and long range
program planning, total quality management (quality
improvement) and external relationships. Works
with Corporate Health and Medical Affairs for
support, assistance and direction in overall medical
management effectiveness. Reports all issues of
clinical quality management to the health plan CEO,
COO, the Board and the Chief Medical Officer (CMO)
of Corporation. Collaborates with the CMO and
other health plan medical directors on national
medical policies and carries out national medical
policies at the health plan in collaboration with the
health plan CEO or COO
VP of Proposal Development
JOB SUMMARY: Under the direction of the SVP
Business Development, the VP is accountable for the
production of a high quality proposal response that
incorporates COMPANY marketing messages and
win themes with the required elements of the
18

technical requirements. The VP plans, organizes, and
manages the work of the Business Development unit
to support business acquisition in new and existing
markets for COMPANY with a primary focus on the
proposal development process, tools and the
integration of COMPANY marketing messages within
the technical response.
VP of Health Plan Services
Location: East Coast
JOB SUMMARY: The Vice President of HPS serves as
a significant contributor to the senior leadership
team of Health Plan Services and reports directly to
the Senior Vice President of Health Plan Services.
This position collaborates with leaders at the highest
level of the company and with internal customers
and business partners.
This position requires a strong proven ability to lead,
with strong functional skills in technology, business
process engineering and business planning and
execution. Experience includes a blend of strategic
and operational experience with effective
communications and a strong background in the
healthcare IT industry. Essential responsibilities
include overall leadership and management of a
regional market.
19

Crossword Answers
20

1 “Number on Medicaid sets record for state.” Allison Sherry. The Denver Post. May 16, 2009 2 “Federal funds will help enroll more people in Medicaid.” Tim Hoover and Jennifer Brown. The Denver Post. April 22, 2009 3 Colorado Governor Signs Bill To Expand State Medicaid Program. Medical News Today. April 27, 2009 4 “Economic slump leads to 11% jump in Az Medicaid.” Tucson Citizen. May 7, 2009 5 Tim Klass. AP. 4/24/09 6 “Hospitals cutting services, staff amid recession” Las Vegas Sun. Apr 26, 2009 7 “Illinois Hospitals Hit Hard By Recession.” Medical News Today. April 10, 2009 8 “State Medicaid Developments.” Idaho Statesman, 4/28 9 "Medicaid Cuts Leave Hospitals Strapped.” Salt Lake Tribune. May 1, 2009 10 “Hospitals, patients suffer from decline in elective surgeries.” Megan Woolhouse. Boston Globe
May 4 2009 11 “Hospitals fear Pennsylvania spending cuts in Medicaid.” Mike Wereschagin. Tribune Review
April 28, 2009 12 “Kaiser Daily Health Policy Report Feature Highlights Recent Blog Entries.”Kaisernetwork.org 5/12/09 13 “Hospitals Pay for Reducing Costly Readmissions.” NYT. May 8, 2009 14 Reuters May 12, 2009 15 “Social Security, Medicare bleeding faster ‐ Washington Times. 5/29/09; WSJ. David Dickson
May 13, 2009 16 “Sebelius Statement On New Medicare Trustees' Report.” CMS and Medical News Today. 5/15/09 17 Wetzel. AP/ Rockford Register Star. 4/25/09 18 “Iowa Legislature approves health expansion.” USA Today. Mike Glover. 4/24/09 19 “Hawaii Democrats Look To Put Funding for Children's Insurance Program in Several Appropriations Bills To Sidestep Veto.”
Kaiser Daily Health Policy Report. Apr 30, 2009 20 “Advocates push for children's Medicaid expansion in Texas Legislature.” Dallas News. May 12, 2009
21