motivating behavior change what really works? practice of medicine i christine m. peterson, m.d....
TRANSCRIPT

Motivating Behavior ChangeWhat Really Works?
Motivating Behavior ChangeWhat Really Works?
Practice of Medicine I
Christine M. Peterson, M.D.
David Waters, Ph.D.

Pre-TestPre-Test

Mokdad et al., JAMA 2004;291(10)1238-1245.
Do You Know?Do You Know? Half of all deaths in the US are attributable to
personal behavior, including: Tobacco = 435,000 deaths (one of every 5) Poor diet and physical inactivity
= 365,000 deaths Alcohol = 85,000 deaths Drugs = 17,000 deaths Other: Homicide, suicide, some accidents,
etc.
Do You Know?Do You Know? Half of all patient visits require a
behavior change on the part of the patient as part of treatment Meds Diet Exercise Safer sex practices Substance avoidance Etc., etc., etc.




How to help?How to help?
How can we help our patients to change their behavior in health-promoting ways?

“Motivational Interviewing”“Motivational Interviewing”
“A directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”- Rollnick and Miller, 1995
Goals of this segment of PoM Goals of this segment of PoM
To gain a better understanding of the difficulty and complexity of behavior change
To practice approaching a patient in an open and non-judgmental manner
Behavioral objectives for studentsBehavioral objectives for students
To maintain an open and curious approach
To learn about techniques useful in motivating behavior change, esp. exploring ambivalence and limiting resistance
To learn about own attitudes and beliefs about changing behavior

Job descriptionsJob descriptions
Providing facts: physician’s job Interpreting personal
implications (i.e. “importance”) of those facts: patient’s job

Lessons We Have LearnedLessons We Have Learned
Information alone doesn’t work.
Attempts to persuade create resistance
Why is that?

Why do people develop negative habits?Why do people develop negative habits?
In an effort to feel better!
External factors: life stresses Internal factors:
inadequate coping skills emotional issues physiological reinforcement congruence of behavior and identity
Contrary to our instincts….Contrary to our instincts….
Attempts at persuasion just increase the stress!

Research findings:Behavior change = Adult learningResearch findings:Behavior change = Adult learning
Self-initiated and self-directed Practical, useful, applicable to real life
(problem-solving) Incorporates feedback about efforts
In clinical setting, physician should be: partner, not expert; coach, not parent; mirror, not (magic) bullet.
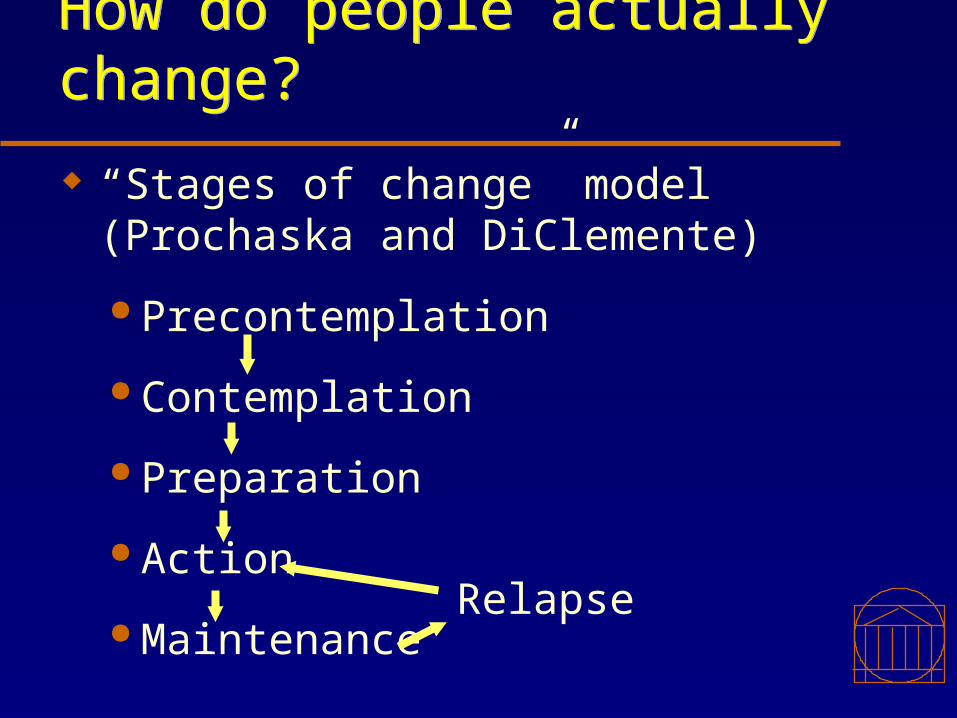
How do people actually change?How do people actually change?
“Stages of change” model(Prochaska and DiClemente)
Precontemplation
Contemplation
Preparation
Action
MaintenanceRelapse

Physician’s role in behavior changePhysician’s role in behavior change
Goal = Help patient move ahead to the next stage First, accurately assess patient’s
current stage Then, facilitate movement to next
stage (”double DARES”)

Adult behavior change:Adult behavior change: What to do? Why to do it? (= “Importance”) How to do it? ( = “Confidence”)

What is readiness?What is readiness?
Confidence (How?)
Low High
Importance (Why?)
High
LowHuh?
I should, but I can’t.
I could, but why should I bother?
I’m ready!
Starting point
Ending point
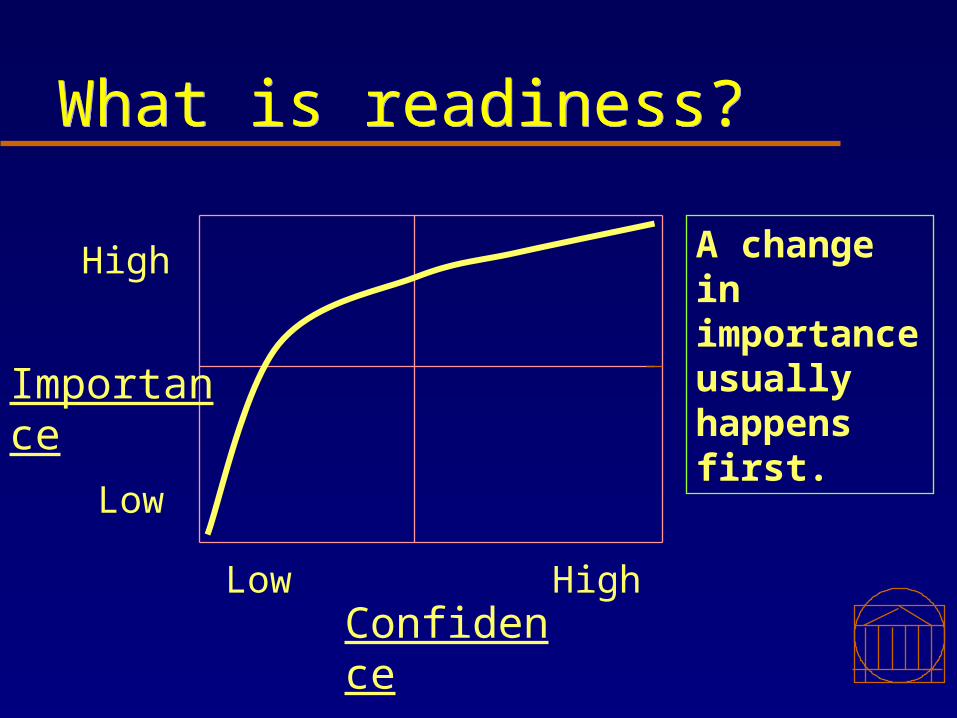
What is readiness?What is readiness?
ConfidenceLow High
Importance
High
Low
A change in importance usually happens first.
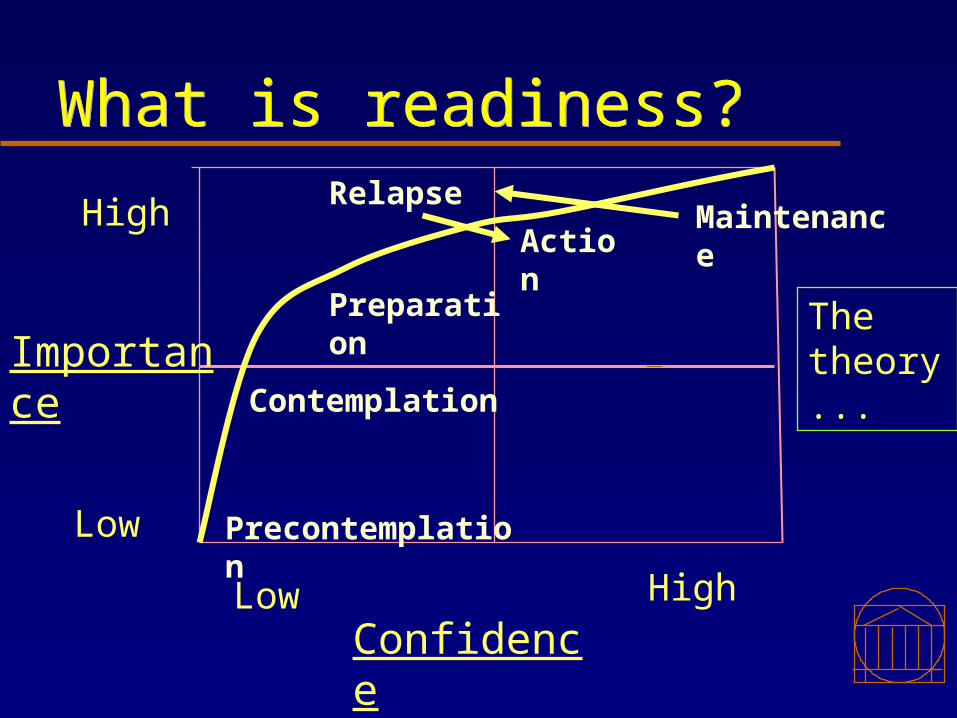
What is readiness?What is readiness?
ConfidenceLow High
Importance
High
Low Precontemplation
Contemplation
Preparation
ActionMaintenance
The theory...
Relapse
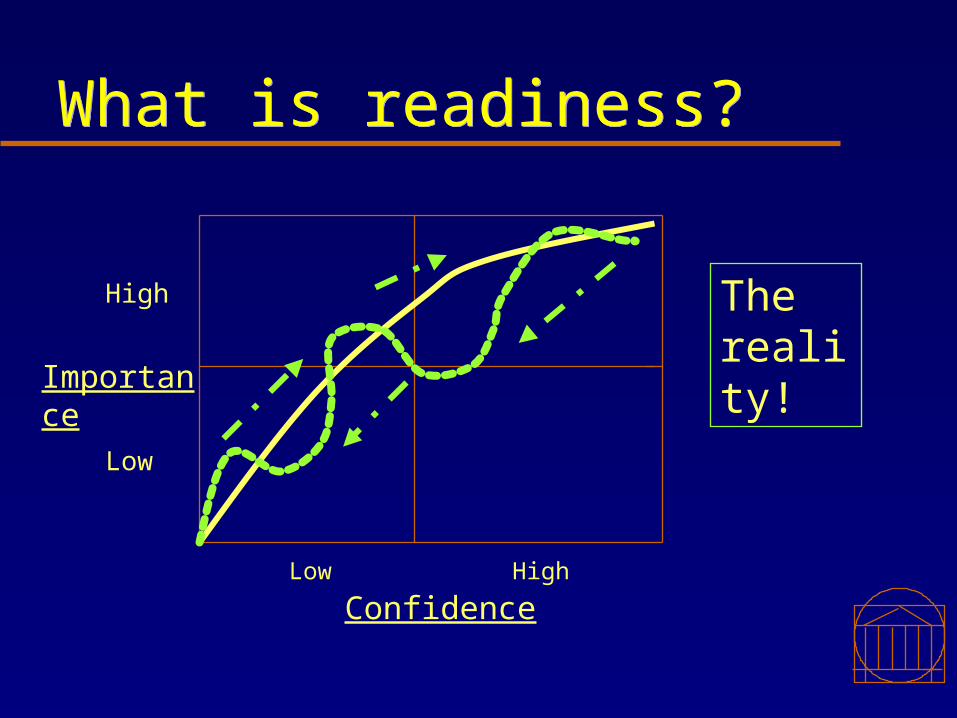
What is readiness?What is readiness?
ConfidenceLow High
Importance
High
Low
The reality!

What is readiness?What is readiness?
Confidence
Low High
Importance
High
Low
The real reality…!

O'Connell D., Ch. 16 Behavior Change in Feldman, Christensen "Behavioral Medicine in Primary Care"
Assessment: PrecontemplationAssessment: Precontemplation
Denial Reluctance Other-defined Reactance Argument
Patient

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Assessment: ContemplationAssessment: Contemplation
Openness Weighs pros and cons Dabbles in action Can be obsessive
Patient
O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Assessment: PreparationAssessment: Preparation
Understands need for change Begins to commit Can picture overcoming
obstacles May procrastinate
Patient

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Assessment: ActionAssessment: Action
Describes plan Follows a plan Shows commitment Resists slips Remains vulnerable
Patient

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Assessment: MaintenanceAssessment: Maintenance
Has accomplished Notes improvement Aware of need for vigilance May lose ground New lifestyle may help make
relapse less likely
Patient

O'Connell D., Ch. 16 Bahavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Assessment: RelapseAssessment: Relapse
Returns to problem behavior Begins as slips Cycles back to earlier stage Needs help to shorten relapse
Patient

Assessing readinessAssessing readiness
ConfidenceLow High
Importance
High
Low Precontemplation
Contemplation
Preparation
ActionMaintenance
Relapse

After assessment, how to help?After assessment, how to help?
How can behavior change be facilitated by physicians?
The answer is in the patient!

Link Behavior with Outcome; Establish Agenda Link Behavior with Outcome; Establish Agenda
The patient’s agenda! Ask directly about patient’s goals. Link patient’s desired health outcome to a
specific patient behavior: “You have [condition] …...And that
is causing your [symptom or problem]. I think it might help to consider [behavior change] ...……”
Establish patient’s agenda: “What do you think?” Avoid assigning physician’s agenda.

“Motivational Interviewing”“Motivational Interviewing”
“A directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”- Rollnick and Miller, 1995
O'Connell D., Ch. 16 Behavior Change in Feldman, Christensen "Behavioral Medicine in Primary Care"
PrecontemplationPrecontemplation
Denial Reluctance Other-defined Reactance Argument
Strategy: When the patient is ready, I’ll be here.
“I have some concern, but if you don’t, I’ll accept that for now.”
Physician’s Basic ResponsePatient

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
ContemplationContemplation
Openness Weighs pros and
cons Dabbles in action Can be
obsessive
Strategy: Go slow, reflect, don’t rush, nurture the idea.
“Would you like to work on this with my help?”
Patient Physician’s Basic Response

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
PreparationPreparation
Understands need for change
Begins to commit Can picture
overcoming obstacles
May procrastinate
Strategy: Don’t jump too fast, don’t assume too much; don’t take over.
“How can I help as you get ready?”
Patient Physician’s Basic Response

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
ActionAction
Describes plan Follows a plan Shows
commitment Resists slips Remains
vulnerable
Strategy: Stay positive and supportive, help with weak spots.
“What do you need from me to keep this going?”
Patient Physician’s Basic Response

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
MaintenanceMaintenance
Has accomplished Notes
improvement Aware of need for
vigilance May lose ground New lifestyle may
make relapse unlikely.
Strategy: Look for lessons from past for future use.
“I’m rooting for you.”
Patient Physician’s Basic Response
O'Connell D., Ch. 16 Bahavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
RelapseRelapse
Returns to problem behavior
Begins as slips Cycles back to
earlier stage Needs help to
shorten relapse
Strategy: Do you want to stay on it and start again?
“I’m not discouraged; let’s talk about when (not ‘if’) to try again.
Patient Physician’s Basic Response

Yet another mnemonic:Yet another mnemonic:
Double DARESDouble DARES Develop Discrepancy Avoid Argument Roll with Resistance Express Empathy Support Self-efficacy

Develop Discrepancy;;Establish Ambivalence
Develop Discrepancy;;Establish Ambivalence
Have patient describe the discrepancy between their current behavior and what they have told you is important to them ambivalence.
Have them present the reasons for change in terms of their desired outcome

Establish Ambivalence; Pros and Cons Establish Ambivalence; Pros and Cons
Examine pros and cons - help patient identify problem area or area of concern
• Good things less good things about current behavior
• Re-state their reasoning for andagainst change

Avoid ArguingAvoid Arguing• Be aware of threat of loss of
freedom• “It should never be you against the
patient; it should be the part of the patient that wants to change against the part that doesn’t….”

Roll with Resistance (description)Roll with Resistance (description)
Arises whenever there is tension or disagreement
Results from traps: Taking control awayMisjudging importance, confidence or readinessMeeting force with force
Manifests in: ignoring, inattention, discounting, excusing, blaming, hostility, splitting, etc.
It is a sign that rapport needs attention.

Roll with Resistance (management)Roll with Resistance (management)
It is your cue to change strategies. Strategies:
Emphasize personal choice and controlReassess stage and/or readiness (importance, confidence)
Back off and come alongside the patient Stay committed but curious. “It’s like dancing - you have to stay relaxed.”

Express EmpathyExpress Empathy
Express empathy without accepting the status quo.
“I can understand that you might feel that way.”
“Yes, it sounds pretty difficult, doesn’t it?”
Support Self-efficacySupport Self-efficacy
Fearful Information: No one wants it! ONLY WHEN PATIENT REQUESTS,
provide information Patient’s interest :
“What have you heard about….?” “I wonder, would you be interested in
knowing more about…. Avoid having the patient put you in the
“Yes, but…” trap.

Roadblocks to Behavior ChangeRoadblocks to Behavior Change
Disagreeing, judging, blaming; Warning, threatening; Shaming, labeling.

More Roadblocks to Behavior ChangeMore Roadblocks to Behavior Change
Moralizing (“shoulds”); Persuading; Challenging with questions; Directing, ordering, commanding.
More Roadblocks to Behavior ChangeMore Roadblocks to Behavior Change
Giving advice, suggestions, solutions;
Agreeing, approving, praising based on physician’s agenda.

More Roadblocks to Behavior ChangeMore Roadblocks to Behavior Change
Reassuring, consoling; Interpreting, analyzing; Withdrawing, humoring.
Maintaining Behavior Change: The 3 F’s Maintaining Behavior Change: The 3 F’s
Timely follow-up by physician (or team member)
Feedback Non-judgmental “When you …… , then ……
occurred.” Focused on patient’s agenda

Post-TestPost-TestPost-TestPost-Test
Motivating Behavior ChangeMotivating Behavior ChangePart 2Part 2
Motivating Behavior ChangeMotivating Behavior ChangePart 2Part 2
Practice of Medicine I
Christine Peterson, M.D.David Waters, Ph.D.
““Motivational Interviewing”Motivational Interviewing”““Motivational Interviewing”Motivational Interviewing”
“A directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence.”- Rollnick and Miller, 1995

Keep in mind:Keep in mind:
Double DARESDouble DARES Develop Discrepancy Avoid Argument Roll with Resistance Express Empathy Support Self-efficacy

O'Connell D., Ch. 16 Behavior Change in Feldman, Christensen "Behavioral Medicine in Primary Care"
Moving Beyond PrecontemplationMoving Beyond Precontemplation
Denial Reluctance Other-defined Reactance Argument
Permission Inquiry Discrepancies Concern Asks pt. to
think between visits
Physician’s TacticsPatient

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Moving Beyond ContemplationMoving Beyond Contemplation
Openness Weighs pros
and cons Dabbles in
action Can be
obsessive
Elicits pt’s perspective
Helps with pros and cons
Asks about promoters
Suggests trials
Patient Physician’s Tactics
O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Moving Beyond PreparationMoving Beyond Preparation
Understands need for change
Begins to commit Can picture
overcoming obstacles
May procrastinate
Summarizes pt’s reasons
Negotiates a start date
Encourages public statement
Arranges follow-up
Patient Physician’s Tactics

O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Moving Beyond ActionMoving Beyond Action
Describes plan Follows a plan Shows
commitment Resists slips Remains
vulnerable
Shows interest Supports pros Slip vs relapse Anticipates
handling slip Helps to modify Arranges follow-up
Patient Physician’s Tactics
O'Connell D., Ch. 16 Behavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Staying with MaintenanceStaying with Maintenance
Has accomplished Notes
improvement Aware of need for vigilance
May lose ground Lifestyle may
preclude relapse
Shows support Inquires re feelings Asks about slips Helps plan for
intensifying effort Supports lifestyle Reflects on
permanence of change
Physician’s TacticsPatient

O'Connell D., Ch. 16 Bahavior Change in Feldman and Christensen "Behavioral Medicine in Primary Care"
Recovering from RelapseRecovering from Relapse
Returns to problem behavior
Begins as slips Cycles back to
earlier stage Needs help to
shorten relapse
Frames as learning opportunity
Asks for specifics Reminds reasons are
valid “When” not ‘if” pt.
changes again Normalizes
Patient Physician’s Tactics

Maintaining Behavior Change: The 3 F’s Maintaining Behavior Change: The 3 F’s
Timely follow-up by physician (or team member)
Feedback Non-judgmental “When you …… , then ……
occurred.” Focused on patient’s agenda

Role Play Time……Role Play Time……