m.rogha m.d isfahan university of medical sciences
TRANSCRIPT

M.Rogha M.DIsfahan university of medical sciences

Anatomy and PhysiologyConsists of the auricle and EAMSkin-lined apparatusApproximately 2.5 cm in lengthEnds at tympanic membrane

Anatomy and PhysiologyAuricle is mostly
skin-lined cartilageExternal auditory
meatusCartilage: ~40%Bony: ~60%S-shapedNarrowest portion
at bony-cartilage junction

Anatomy and PhysiologyEAC is related to
various contiguous structuresTympanic membraneMastoidGlenoid fossaCranial fossaInfratemporal fossa

Anatomy and PhysiologyInnervation: cranial nerves V, VII, IX, X, and
greater auricular nerveArterial supply: superficial temporal,
posterior and deep auricular branchesVenous drainage: superficial temporal and
posterior auricular veinsLymphatics

Anatomy and PhysiologySquamous
epitheliumBony skin –
0.2mmCartilage skin
0.5 to 1.0 mmApopilosebaceous
unit

Perichondritis/ChondritisInfection of perichondrium/cartilageResult of trauma to auricleMay be spontaneous (overt diabetes)

Perichondritis: SymptomsPain over auricle and deep in canalPruritus

Perichondritis: SignsTender auricleIndurationEdemaAdvanced cases
Crusting & weeping
Involvement of soft tissues

Perichondritis: TreatmentMild: debridement, topical & oral antibioticAdvanced: hospitalization, IV antibioticsChronic: surgical intervention with excision
of necrotic tissue and skin coverage

Relapsing PolychondritisEpisodic and progressive inflammation of
cartilagesAutoimmune etiologyExternal ear, larynx, trachea, bronchi, and
nose may be involvedInvolvement of larynx and trachea causes
increasing respiratory obstruction

Relapsing PolychondritisFever, painSwelling,
erythemaAnemia, elevated
ESRTreat with oral
corticosteroids

Herpes Zoster OticusJ. Ramsay Hunt described in 1907Viral infection caused by varicella zosterInfection along one or more cranial nerve
dermatomes (shingles)Ramsey Hunt syndrome: herpes zoster of the
pinna with otalgia and facial paralysis
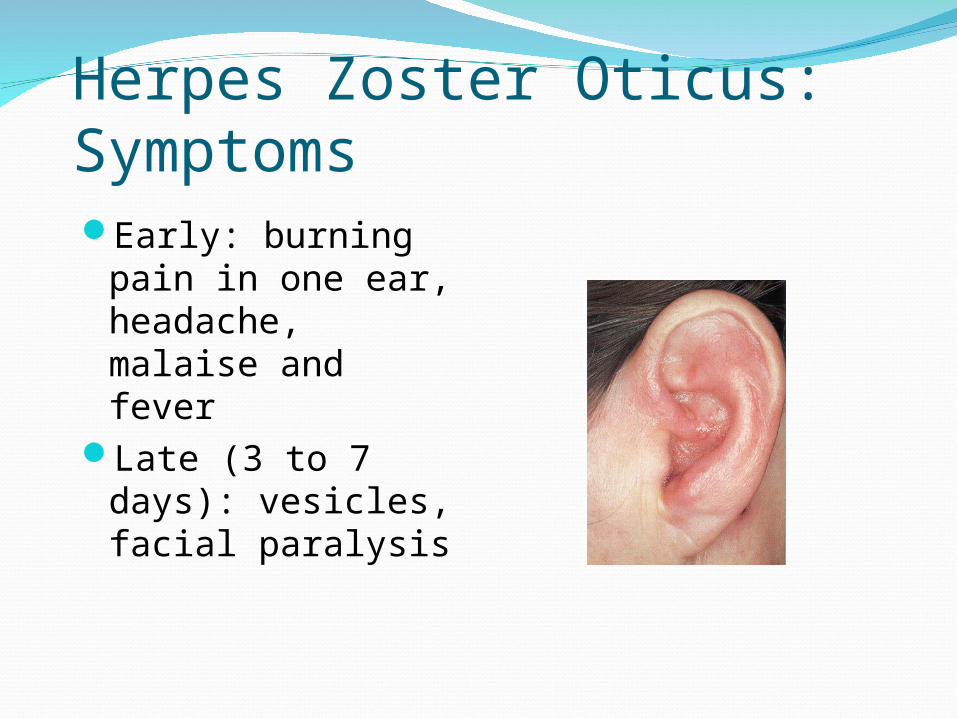
Herpes Zoster Oticus: SymptomsEarly: burning
pain in one ear, headache, malaise and fever
Late (3 to 7 days): vesicles, facial paralysis

Herpes Zoster Oticus: TreatmentCorneal protectionOral steroid taper (10 to 14 days)Antivirals

ErysipelsAcute superficial
cellulitisGroup A, beta
hemolytic streptococciSkin: bright red; well-
demarcated, advancing margin
Rapid treatment with oral or IV antibiotics if insufficient response

Radiation-Induced Otitis ExternaOE occurring
after radiotherapyOften difficult to
treatLimited infection
treated like COEInvolvement of
bone requires surgical debridement and skin coverage

Otitis ExternaBacterial infection of external auditory canalCategorized by time course
AcuteSubacuteChronic

Acute Otitis Externa (AOE)“swimmer’s ear”Preinflammatory stageAcute inflammatory stage
MildModerateSevere
AOE: Preinflammatory StageEdema of stratum corneum and plugging of
apopilosebaceous unitSymptoms: pruritus and sense of fullnessSigns: mild edemaStarts the itch/scratch cycle

AOE: Mild to Moderate StageProgressive
infectionSymptoms
PainIncreased pruritus
SignsErythemaIncreasing edemaCanal debris,
discharge

AOE: Severe StageSevere pain,
worse with ear movement
SignsLumen obliterationPurulent otorrheaInvolvement of
periauricular soft tissue

AOE: TreatmentMost common pathogens: P. aeruginosa and
S. aureusFour principles
Frequent canal cleaningTopical antibioticsPain controlInstructions for prevention

Chronic Otitis Externa (COE)Chronic inflammatory processPersistent symptoms (> 2 months)Bacterial, fungal, dermatological etiologies

COE: SymptomsUnrelenting pruritusMild discomfortDryness of canal skin

COE: SignsAsteatosisDry, flaky skinHypertrophied
skinMucopurulent
otorrhea (occasional)

COE: TreatmentSimilar to that of AOETopical antibiotics, frequent cleaningsTopical SteroidsSurgical intervention
Failure of medical treatmentGoal is to enlarge and resurface the EAC

FurunculosisAcute localized infectionLateral 1/3 of posterosuperior canalObstructed apopilosebaceous unitPathogen: S. aureus

Furunculosis: SymptomsLocalized painPruritusHearing loss (if lesion occludes canal)

Furunculosis: SignsEdemaErythemaTendernessOccasional
fluctuance

Furunculosis: TreatmentLocal heatAnalgesicsOral anti-staphylococcal antibioticsIncision and drainage reserved for localized
abscessIV antibiotics for soft tissue extension

OtomycosisFungal infection of EAC skinPrimary or secondaryMost common organisms: Aspergillus and
Candida

Otomycosis: SymptomsOften indistinguishable from bacterial OEPruritus deep within the earDull painHearing loss (obstructive)

Otomycosis: SignsCanal erythemaMild edemaWhite, gray or
black fungal debris


Otomycosis: TreatmentThorough cleaning and drying of canalTopical antifungals

Granular Myringitis (GM)Localized chronic inflammation of pars tensa
with granulation tissueToynbee described in 1860Sequela of primary acute myringitis, previous
OE, perforation of TMCommon organisms: Pseudomonas, Proteus

GM: SymptomsFoul smelling discharge from one earOften asymptomaticSlight irritation or fullnessNo hearing loss or significant pain

GM: SignsTM obscured by
pus “peeping”
granulationsNo TM
perforations

GM: TreatmentCareful and frequent debridementTopical anti-pseudomonal antibioticsOccasionally combined with steroidsAt least 2 weeks of therapyMay warrant careful destruction of
granulation tissue if no response

Bullous MyringitisViral / mycoplasma infection Confined to tympanic membranePrimarily involves younger children

Bullous Myringitis: SymptomsSudden onset of severe painNo feverNo hearing impairmentBloody otorrhea (significant) if rupture

Bullous Myringitis: SignsInflammation
limited to TM & nearby canal
Multiple reddened, inflamed blebs
Hemorrhagic vesicles

Bullous Myringitis: TreatmentSelf-limitingAnalgesicsTopical antibiotics to prevent secondary
infectionIncision of blebs is unnecessary

Necrotizing External Otitis(NEO)Potentially lethal infection of EAC and
surrounding structuresTypically seen in diabetics and
immunocompromised patientsPseudomonas aeruginosa is the usual culprit

NEO: SymptomsPoorly controlled diabetic with h/o OEDeep-seated aural painChronic otorrheaAural fullness

NEO: SignsInflammation and
granulation Purulent
secretionsOccluded canal
and obscured TMCranial nerve
involvement

NEO: ImagingPlain filmsComputerized tomography – most usedTechnetium-99 – reveals osteomyelitis Gallium scan – useful for evaluating RxMagnetic Resonance Imaging

NEO: DiagnosisClinical findingsLaboratory evidenceImagingPhysician’s suspicion

NEO: TreatmentIntravenous antibiotics for at least 4 weeks –
with serial gallium scans monthlyLocal canal debridement until healedPain controlUse of topical agents controversialHyperbaric oxygen experimentalSurgical debridement for refractory cases

NEO: MortalityDeath rate essentially unchanged despite
newer antibiotics (37% to 23%)Higher with multiple cranial neuropathies
(60%)Recurrence not uncommon (9% to 27%)May recur up to 12 months after treatment
