mtm module
DESCRIPTION
MTM trainingTRANSCRIPT
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
© 2014, American Pharmacists Association. All rights reserved.
14-289
A National Certificate Training Program
Module 1. The Current Landscape for MTM Services
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
Module 1. The Current Landscape for MTM Services 2
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
IntroductionThe U.S. health care system incurs annual costs of more than $200 billion due to inappropriate use of medications. These costs include approximately 10 million avoidable hospital admissions, 78 million outpatient treatments, 246 million prescriptions, and 4 million emergency department visits and constitute 8% of total annual health care expenditures.1 Improving medication use in this country is an important public health goal that is recognized in the national public health initiative Healthy People 2020 (healthypeople.gov). Several goals in this initiative focus on improving medication use. Examples (and final objective numbers) include2:
■■ Increase the proportion of adults with hypertension who are taking the prescribed medications to lower their blood pressure (HDS-11).
■■ Reduce emergency department visits for common, preventable adverse events from medications (MPS-5).
■■ Reduce the proportion of older adults with disabil-ities who use inappropriate medications (DH-7).
Medication therapy management (MTM) is designed to allow health care providers to identify and resolve medication-related problems, and has been shown to both reduce health care costs and improve clinical outcomes.3,4 Many pharmacists are eager to expand their patient care activities and assist patients with medication-related problems. However, they may need to fine-tune various patient care skills, increase their expertise in therapeutics, or develop the infrastructure required to support these services.
This certificate program presents a systematic approach for developing, implementing, delivering, and sustaining MTM services. It includes an overview of the marketplace for delivering MTM services, guidance for implementing MTM services in pharmacy practice, a review of the essential skills and knowledge needed for performing MTM successfully, and an organized process for identifying medication-related problems.
The History of MTMPharmacists have provided individualized patient care services in numerous settings for decades; these services were often described as pharmaceutical care, a term that was coined in 1990.5 The term medication therapy management has been in wide use since the early 2000s, when the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) put MTM on the health care map as part of the Medicare Part D benefit.
The inclusion of MTM in the Part D benefit stimulated devel-opment of national standardization of such services by expanding access to services for patients and compensation opportunities for pharmacists. MMA includes a provision for pharmacists and other health care professionals to deliver MTM services to Medicare beneficiaries at high risk for medication-related problems and allows prescription drug plans to pay pharmacists for providing these services. (Of note, the legislation did not grant Medicare Part B provider status to pharmacists, and lack of this status continues to impede payments to pharmacists in some settings.) Today, pharmacists provide MTM to a wide variety of patient popula-tions in addition to Part D beneficiaries.
Learning ObjectivesAfter completing this module of the self-study activity, pharmacists will be able to:
1. Explain the key components of medication therapy management (MTM).
2. Define the five core elements of the MTM service model.
3. Discuss the MTM provisions of the Medicare Part D benefit, including requirements established by the Centers for Medicare and Medicaid Services and the Affordable Care Act.
4. List opportunities for providing MTM services including those that were created by the Affordable Care Act, such as patient-centered medical homes, accountable care organizations, and transition of care activities.
5. Cite data that describe the current status of MTM provision in the United States.
6. Discuss quality measures that can be impacted by MTM services or used to evaluate MTM services.
7. Describe economic and clinical outcomes that are affected by pharmacist-provided patient care services.
When the term “patient” is used in this program, it refers to the patient or the patient’s caregiver who may be present during delivery of MTM services or other health care visits.
Module 1. The Current Landscape for MTM Services 3
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
What Is MTM?MTM encompasses a broad range of health care services provided by pharmacists. As defined in a consensus definition adopted by the pharmacy profession in 2004, MTM is a distinct service or group of services that optimizes therapeutic outcomes for individual patients (Appendix A).6 The definition supports services that optimize therapeutic outcomes for individual patients, promote collaboration with other health care providers, and facilitate continuity of care. This definition includes a range of professional activities and services within the scope of pharmacy practice, applicable within the broad range of pharmacy practice settings, and appropriate for any patient in need of MTM services. (However, some limitations may exist based on scope of practice regulations in individual states.)
MTM services are distinct from medication dispensing and the routine patient counseling provided by a pharmacist when a patient picks up a prescription medication. These brief counseling sessions usually involve instructions for the particular medication being dispensed, and address the patient’s questions specifically relating to that medication. In contrast, MTM is a patient-centered process of care that includes assessment and evaluation of the patient and his or her complete medication therapy regimen rather than focusing on an individual medication product.
Disease management programs and MTM services also are distinct. MTM services comprehensively address a patient’s full range of potential or actual medication-related problems; disease management programs focus on patient education and management of a specific disease. More advanced MTM services may include aspects of disease management programs, such as blood pressure monitoring and lipid management. Likewise, MTM services, such as a compre-hensive and targeted medication therapy reviews, may be a component of a comprehensive disease management program.
MTM services can be delivered face-to-face or telephoni-cally. Face-to-face interaction helps establish the pharmacist-patient relationship while also allowing the pharmacist to visually assess the patient for signs and symptoms of possible medication-related problems (e.g., lethargy, confusion, bruising, extrapyramidal symptoms). In-person encounters give the pharmacist an opportunity to observe visual clues that might provide insight to the patient’s comprehension and acceptance of the pharmacist’s comments. The pharmacist also may conduct physical assessments, vital sign measurement, and point-of-care testing as needed during the face-to-face visit.
Face-to-face services can occur in a variety of settings, such as a community pharmacy, a hospital, a clinic, the patient’s home, a community center, or other settings. Telephonic MTM services enable pharmacists to provide services to patients when in-person consultations may be challenging to arrange, such as patients who are home bound or who live in remote rural areas. Additionally, telephonic MTM services reach the patient in a comfortable, private setting where they have access to their medications and any medical records they keep at home. Both telephonic and face-to-face services require good communication skills and the ability to assess the patient.
Finally, although the terms MTM services and MTM programs are often used synonymously, there is a distinction. As currently used, MTM programs are developed by health plans or other health care entities focused on optimizing patients’ therapeutic outcomes. MTM services are components of MTM programs and are delivered by health care professionals, such as pharmacists.
Core Elements of an MTM ServiceNot all MTM services will look exactly alike. The specific services provided will vary based on the patient’s individual needs and, to some extent, the pharmacist’s areas of expertise.
The Medicare Prescription Drug Benefit: Part DPrior to January 2006, the Medicare program consisted of Part A (inpatient hospital services, skilled nursing facility benefits, and hospice care), Part B (physician and outpatient hospital services, annual mammography and other cancer screenings, and services such as laboratory procedures and medical equipment acquisition), and Part C (Medicare managed care plans). MMA added Part D, an optional prescription drug benefit available to any Medicare beneficiary, which included payment for MTM services for selected beneficiaries.
Medicare Parts A, B, and C are administered by the Centers for Medicare and Medicaid Services (CMS). However, Medicare Part D is administered by private insurers—Prescription Drug Plans and Medicare Advantage Prescription Drug (MA-PD) plans—that are reimbursed by CMS. Plans offering Part D prescription coverage follow regulations and guidelines that are developed by CMS.
Module 1. The Current Landscape for MTM Services 4
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
Third-party payers also may influence services that are offered. However, to establish a set of standardized compo-nents for MTM services, the American Pharmacists Association (APhA) and the National Association of Chain Drug Stores (NACDS) Foundation built on the consensus definition and developed an MTM model framework (Appendix B).7
The MTM model framework is designed to improve collabo-ration among pharmacists, physicians, and other health care professionals; enhance communication between patients and their health care team; empower patients to be self-advocates; and optimize medication use for improved patient outcomes. This framework establishes core elements for all MTM services provided by pharmacists.
The model framework consists of five core elements that can be provided by pharmacists across the spectrum of pharmacy. Its structure improves efficiency and creates consistency of MTM services while meeting the expectations that CMS has for MTM: enhancing patients’ understanding of appropriate drug use, increasing adherence to medication therapy, and improving detection of adverse drug events. The framework does not represent a specific minimum or maximum level of services that could be delivered by pharmacists. Instead, it delineates a structured approach for medication review that
promotes ongoing evaluation of the patient’s medication therapy, recommendations to prescribers, and documentation of interventions and results. It creates a solid foundation for pharmacists to build and expand MTM services.
The core elements of MTM service delivery were designed to help patients take an active role in managing their medica-tions. The five core components of an MTM service include7:
■■ Medication therapy review (MTR).■■ Personal medication record (PMR). ■■ Medication-related action plan (MAP).■■ Intervention and/or referral. ■■ Documentation and follow-up.
The following descriptions summarize each of these elements. Specific details and examples of forms can be found in Appendix B.
Learning ActivityMatch the word or phrase on the left with the statement on the right that best describes it.1. Counseling
2. Disease management
3. MTM programs
4. MTM services
a. A brief, medication-centered discussion about a specific medication that the patient picks up from the pharmacy.
b. A patient-centered process that includes an assessment of the patient’s complete medication regimen and identification of the individual’s medication-related problems.
c. Focuses on patient education and the management of a specific disease.
d. Developed by health plans to optimize therapeutic outcomes.
5. The consensus definition of MTM services adopted by the pharmacy profession supports the following three objectives:
Answers are located at the bottom of the page.
Learning Activity Answer Key1. a; 2. c; 3. d; 4. b; 5. Optimization of therapeutic outcomes for individual patients, collaboration with other health care providers, continuity of care.

Module 1. The Current Landscape for MTM Services 5
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
Medication Therapy ReviewThe MTR is a systematic process in which the pharmacist collects patient-specific information, assesses medication therapies, identifies medication-related problems, develops a prioritized list of medication-related problems, and creates a plan to resolve them. It is designed as a collaborative process to improve patients’ knowledge of their medications, address problems or concerns they may have, and enable patients to self-manage their medications and health conditions.
MTRs are either comprehensive or targeted for a specific medication-related problem. During a comprehensive MTR, the pharmacist reviews all current medications for clinical appropriateness, including prescription and nonprescription medications, herbal products, and other dietary supplements. The pharmacist assesses the patient’s medications for the presence of any medication-related problems, and works with the patient, the prescriber, and other health care professionals as needed to determine appropriate options for resolving identified problems. In addition, the pharmacist supplies the patient with education and information to enhance the patient’s medication self-management and assist with promoting appropriate lifestyle changes.
The targeted MTR addresses a specific medication problem or ongoing medication monitoring. It usually is performed for patients who previously have received a comprehensive MTR. The targeted MTR also can be a component of the prospective medication review that pharmacists may perform during the dispensing process. Whether for a new problem or subse-quent monitoring, the pharmacist assesses the specific therapy problem in the context of the patient’s complete medical and medication history. Following assessment, the pharmacist inter-venes and provides education and information to the patient, the prescriber, community advocates, or other health care professionals, as appropriate.
The MTR is tailored to the individual needs of the patient at each encounter. Ideally, a patient receives an annual compre-hensive MTR with additional targeted MTRs to address new or ongoing medication-related problems. A comprehensive MTR may be needed sooner if a significant event occurs, such as changes in the patient’s health status, an emergency department visit, or an admission to or discharge from a hospital or long-term care facility. Patients are more vulnerable to medication-related problems during transitions of care, therefore systems that support MTM during transitions are crucial.
Personal Medication RecordThe pharmacist develops a PMR for the patient after the MTR has been completed. A PMR is a comprehensive document listing the patient’s medications, including prescription, nonprescription, herbal, and dietary supplement products. The PMR is completed and updated either by the pharmacist or the patient with the pharmacist’s assistance. Engaging the patient in completing the PMR may help reinforce education concepts and enhance the patient’s understanding of his or her medication therapy. The PMR is a portable record of all the patient’s medications with a summary of important details written so the patient understands its contents.
Patients use the PMR as a tool to self-manage medications and to improve continuity of care among multiple prescribers. Maintenance of the PMR is a collaborative effort among the patient, pharmacist, prescriber, and other health care profes-sionals. Pharmacists should encourage patients to maintain and update the PMR and carry it with them at all times. Patients should be advised to share their PMRs at all health care visits, including routine appointments and admission to or discharge from an institutional setting. To ensure a complete and accurate record, patients should be instructed to bring the PMR to all visits for the pharmacist to update as needed. Ultimately, patients (who are able) have a responsibility to ensure that their PMR is updated in collaboration with their care team, share this information with all of their health care providers, and be knowledgeable about their medications.
Medication-Related Action PlanThe document known as the MAP is typically provided to the patient at the end of the MTR, or shortly thereafter. It contains specific information for the patient to use for optimizing medication self-management and making positive lifestyle changes. The MAP may include a list of medication-related issues identified, proposed actions to resolve the medication-
Core Elements of an MTM Service ModelMedication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 is a collaboration between APhA and the NACDS Foundation. It focuses on the provision of MTM services in settings where patients (or their caregivers) can be actively involved in managing their medications. This service model was developed with the input of an advisory panel of pharmacy leaders representing diverse pharmacy practice settings.
Module 1. The Current Landscape for MTM Services 6
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
related issues, the person responsible for action, and other pertinent information. The pharmacist creates this document in collaboration with the patient, physician, and other health care providers, as appropriate. The MAP is primarily intended for patient use, therefore it should be written in language the patient easily understands and at a literacy level appropriate for the patient. The MAP should include only items that the patient can act on and are within the pharmacist’s scope of practice or agreed to by relevant members of the health care team. It should not contain outstanding items that require review or approval from other health professionals; these outstanding items should be included in separate internal documentation that facilitates follow-up.
Pharmacists should encourage patients to voluntarily share both the MAP and the PMR with other health care providers. Patients should be instructed to bring the MAP with them to all future visits thereby allowing the pharmacist who provides MTM to record the date and the results of interventions and/or resolutions of medication-related problems. The pharmacist can use the MAP as a resource when communicating action plan information to the patient’s physician and other health care providers. Additionally, the patient can bring the MAP to visits with other health care providers to aid continuity of care. Widespread use of the MAP will support uniformity and consistency in information sharing among members of the health care team.
MTM Documentation for Medicare Part DThe Affordable Care Act of 2010 directed CMS to develop a standardized format for the comprehensive medication review action plan and summary of MTM services provided to Medicare Part D beneficiaries.8 CMS developed a standardized format containing three components: a beneficiary cover letter, a medication action plan, and a personal medication list (PML). The PML is similar to the PMR. CMS noted that the format of the documents is consistent with MTM forms that were currently in use (i.e., those included in the core elements). Part D plans were required to begin using the CMS format in January 2013.9 The final forms and instructions for their use are available at: www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/MTM-Program-Standardized-Format-English-and-Spanish-Instructions-Samples-.pdf
Intervention and/or ReferralThe intent of providing intervention and/or referral is to optimize medication use, enhance continuity of care, and encourage patients to use appropriate health care services to prevent adverse outcomes. The pharmacist intervenes to resolve, minimize, or avoid medication-related problems identified during the MTR. When a patient’s needs are complex and extend beyond the basic MTM services, pharmacists may provide additional care based on their level of expertise, while staying within the scope of pharmacy practice. The value of MTM is determined by the quality of the pharmacists’ interventions. These interventions may include activities such as making recommendations to prescribers to change a patient’s therapy, implementing strategies to improve adherence, administering vaccines, and other activities. Pharmacists need to have updated clinical knowledge, be able to effectively and efficiently identify drug therapy problems, and provide clinically relevant recommendations to prescribers to ensure optimal outcomes.
However, in some cases, the pharmacist will need to refer the patient to another pharmacist with additional qualifications, a physician, or another health care provider. Examples of circumstances that may require referral include:
■■ Evaluation of a new problem discovered during the MTR.
■■ Advanced education to help the patient manage a chronic disease (e.g., diabetes, hypertension).
■■ Monitoring of high-risk medications (e.g., warfarin, digoxin).
■■ Laboratory monitoring (e.g., cholesterol panel, blood glucose levels, liver function tests).
■■ Medication therapy dose adjustments or changes.
Communication of timely and appropriate information to the prescriber or other health care professional—including complete yet succinct information regarding the selection of medications, suggestions to address medication problems, a complete reconciled medication list, and recommended follow-up care—is integral to the intervention component of the MTM service model.10
Documentation and Follow-UpDocumentation and follow-up are essential elements of the MTM process. Services performed should be documented in a consistent manner that is appropriate for evaluating patient progress and meeting billing requirements. Follow-up visits
Module 1. The Current Landscape for MTM Services 7
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
with the patient should be scheduled according to the patient’s medication-related needs or circumstances, such as follow-up monitoring when dose adjustments are made and following a patient’s transition from hospital to home.
Documentation Recording the information obtained during the MTR, such as the patient’s medication history and the actions needed to prevent adverse outcomes, helps create consistent documen-tation. A chronological record of the pharmacist’s care, provided in a standard format, such as a SOAP note (i.e., notes on Subjective observations, Objective observations, Assessment, and Plan of action), also should be included in the documentation.7,11
Documents resulting from the patient’s MTR are distributed to the patient, prescribers, other health care professionals, and payers, as applicable. Copies of these documents should
Learning ActivityMatch the phrase on the left with the correct definition on the right. 1. Medication therapy review
2. Personal medication record
3. Medication-related action plan
a. Patient-centric document containing specific information for the patient to use for optimizing medication self-management, including the medication-related issues identified, proposed actions, and the person responsible for action.
b. Systematic process that requires collecting patient-specific information, assessing medication therapies, and identifying medication-related problems.
c. Patient-centric portable record of all the patient’s medications with a summary of important details.
4. Under what circumstances should a pharmacist refer a patient to another provider?
5. List three stakeholders that are the intended audience for SOAP notes.
Answers are located at the bottom of the page.
Learning Activity Answer Key1. b; 2. c; 3. a; 4. Referral is indicated when the patient’s needs exceed the pharmacist’s knowledge or scope of practice; 5. Other pharmacists, prescribers, third-party payers.
be kept on file at the pharmacist’s practice site. Optimally, documentation should be electronic (with appropriate patient privacy security parameters in place) and should be shared with other health care professionals through secure electronic portals or health information exchanges. At the end of a visit, patients should receive their PMR, MAP, and other suitable educational materials. Patient materials should be written in easily understood language, free from medical jargon. Patient materials should be developed at an appropriate health literacy level, taking into account the patient’s ability to read, understand health care topics, and perform simple calculations

Module 1. The Current Landscape for MTM Services 8
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
if needed. Documentation to prescribers and other health care professionals may include a cover letter, the patient’s PMR and MAP, and the pharmacist’s chronological record of care and plan of action.
Payers usually will require documentation of the services performed, the amount of time spent on those services, and other billing information, such as billing codes and pharmacy or pharmacist identifiers (e.g., National Provider Identifier). More information about billing is included in Module 2.
Follow-Up The level of follow-up with the patient should correspond with individual patient requirements. Follow-up may take the form of a targeted MTM visit. However, follow-up does not neces-sarily have to be a face-to-face encounter. Instead, it may include a phone call to the patient and/or other providers on the patient’s health care team. When the patient transi-tions from one care setting to another (e.g., from home to a long-term care facility), follow-up with providers at the new setting promotes continuity of care. Patients should be instructed to bring their PMR and MAP to all follow-up visits so the pharmacist can document the results of the interventions and any new items.
The Value of MTM Services The value associated with MTM services can be measured in many ways, including the impact on patient care, the value to other members of the health care team in assisting with medication issues, and value to third-party payers through reduced overall health care costs and improvements on quality measure performance. Many pharmacists also derive professional and personal satisfaction in addition to financial compensation for providing the service to patients. A variety of metrics can be used to demonstrate value associated with pharmacists’ patient care services. (More information about quality measures appears in the next section, opportunities for phArMAcists to provide MtM services).
Examples of the Impact of MTM on Patient Outcomes and Health Care CostsA review of the literature reveals numerous studies showing that pharmacist-provided clinical services such as MTM signifi-cantly improve patient outcomes and reduce overall health care costs.4
One example of the benefits of MTM services comes from the Iowa Medicaid Pharmaceutical Case Management Program, which pays pharmacist-physician teams to manage the medication regimens of qualified Medicaid beneficiaries. In this program, the pharmacist performs an initial assessment for beneficiaries who are receiving four or more medications and have at least one of twelve specified diseases (i.e., congestive heart failure, ischemic heart disease, diabetes mellitus, hyper-tension, hyperlipidemia, asthma, depression, atrial fibrillation, osteoarthritis, gastroesophageal reflux disease, peptic ulcer disease, and chronic obstructive pulmonary disease). When problems are identified, the pharmacist makes written recom-mendations to the physician. Over the 2-year evaluation period for the program, the appropriateness of the patient’s medications improved and the use of high-risk medications decreased by nearly 25%.12
Another example comes from a CMS demonstration project in Connecticut that evaluated the impact of MTM services provided by nine pharmacists to 88 Medicaid patients over a 10-month period. Pharmacists identified 917 medication-related problems and resolved nearly 80% of them, resulting in an estimated annual savings of $1,595 per patient ($1,123 on medication costs and $472 on medical, hospital, and emergency department costs) compared with patients’ costs the previous year.13 Total savings achieved were 2.5 times the cost associated with pharmacists’ professional fees and network administration.13
In yet another analysis, researchers reported data from a 1-year study of MTM services provided to patients enrolled in a state-wide private insurance program in Minnesota.14 Patients who received MTM services at six ambulatory care clinics in Minnesota had improved outcomes, compared with similar patients who did not receive MTM services. A total of 637 drug therapy problems were resolved among 285 intervention patients, and the patients’ achievement of goals of therapy increased from 76% to 90% during 1 year of MTM services. Healthcare Effectiveness Data and Information Set (HEDIS) measures were improved for hypertension and choles-terol management for patients receiving MTM services. Total health expenditures for patients enrolled in the MTM service decreased from $11,965 to $8,197 (P <.0001), resulting in a return on investment (ROI) of 12:1.14 (Further information on ROI is discussed in Module 2.)
The Patient Safety and Clinical Pharmacy Services Collaborative (PSPC) provides further evidence of the value of MTM services. The PSPC is working to bring pharmacy services, such as MTM, to more than 450 organizations of community-based health care providers including community
Module 1. The Current Landscape for MTM Services 9
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
health centers, primary care associations, and rural health clinics. The PSPC has demonstrated that pharmacists’ services result in improved health outcomes and patient safety in high-risk, high-cost, complex patients. The incidence of adverse drug events has fallen by 49% in this patient population and the majority of patients whose medical condi-tions were once identified as “out of control” are now “under control.”15
Value of MTM for PharmacistsAnnual surveys of MTM providers have repeatedly shown that pharmacists report the greatest value of providing MTM services comes from increased professional satisfaction, followed by increased patient satisfaction, and increased quality of care/outcomes based on performance measures.3 Pharmacists report that MTM has helped them to3:
■■ Build connections with patients.■■ Enhance professionalism.■■ Establish collaboration.■■ Enhance the pharmacist’s image with the public and
colleagues.■■ Increase respect from patients.■■ Improve patient-provider-pharmacist interaction.■■ Establish trust with patients.■■ Create more personal interaction with patients.■■ Feel more connected with the health care team.■■ Increase patient loyalty.■■ Target patients who can benefit the most from
pharmacists’ services.■■ Build confidence and retention.■■ Identify and resolve medication-related problems for
patients before they occur.■■ Differentiate their practice from competition.■■ Create new partnerships with other organizations
and opening new opportunities.
Value of MTM Services for PayersAnnual surveys of MTM payers have found that improved quality of care and patient outcomes related to performance measures were the primary source of value for payers.3 Payers also reported overall health care cost savings and improved patient satisfaction were key aspects of the value of MTM
services. Payers have reported that several outcomes have been shown to be improved by MTM services, including:
■■ Completion rates of comprehensive medication reviews.
■■ Avoidance/discontinuation of inappropriate medications in elderly patients (i.e., Beers criteria).
■■ CMS star ratings. ■■ Patient quality of life.■■ HEDIS.■■ Pharmacy Quality Alliance (PQA) measures.■■ Hospital readmission rates.■■ Medication reconciliation measures.■■ Accountable care organization (ACO) quality
measures.Some of these measures will be described in more detail in the next section.
Opportunities for Pharmacists to Provide MTM ServicesGiven the extent of their education and medication-related expertise, pharmacists are ideally suited to provide MTM services and are the leaders for providing these services.3 In 2007, APhA began conducting environmental scans of MTM services, with resulting data providing a snapshot of the provision of services throughout the country. Data indicate that the majority of payers use pharmacists to provide services, with the percentage of payers using nurses to provide MTM services dropping from 29% in 2008 to 6% in 2013; some payers used more than one type of provider.3 Data from CMS indicate that 99.9% of Medicare Part D plans use pharmacists to deliver MTM services.16
Quality Measures and MTM OpportunitiesMany opportunities for pharmacists to provide MTM have arisen from financial incentives that are linked to perfor-mance quality measures. Several initiatives are ongoing to define, assess, and improve the quality of pharmacy services, including MTM. PQA, a pharmacy quality alliance, has led several of these initiatives to develop and test pharmacy measures as well as to create “report card” systems for communicating performance on quality measures. PQA
Module 1. The Current Landscape for MTM Services 10
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
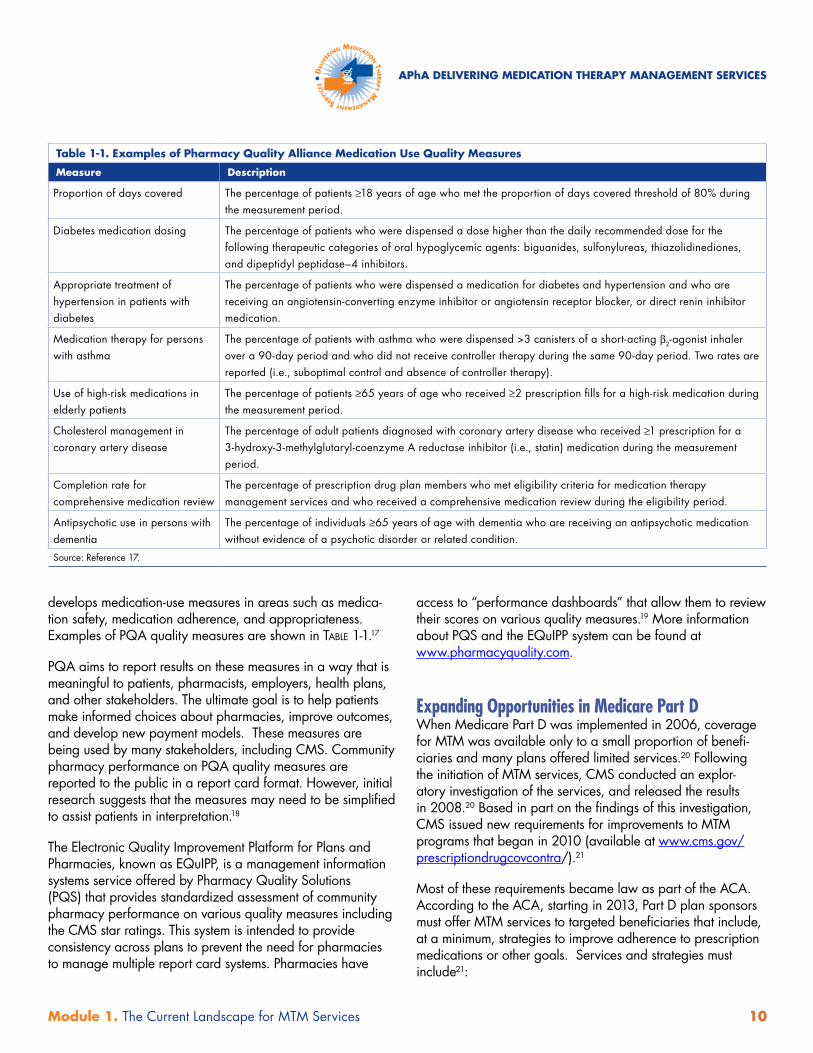
develops medication-use measures in areas such as medica- tion safety, medication adherence, and appropriateness. Examples of PQA quality measures are shown in tABle 1-1.17
PQA aims to report results on these measures in a way that is meaningful to patients, pharmacists, employers, health plans, and other stakeholders. The ultimate goal is to help patients make informed choices about pharmacies, improve outcomes, and develop new payment models. These measures are being used by many stakeholders, including CMS. Community pharmacy performance on PQA quality measures are reported to the public in a report card format. However, initial research suggests that the measures may need to be simplified to assist patients in interpretation.18
The Electronic Quality Improvement Platform for Plans and Pharmacies, known as EQuIPP, is a management information systems service offered by Pharmacy Quality Solutions (PQS) that provides standardized assessment of community pharmacy performance on various quality measures including the CMS star ratings. This system is intended to provide consistency across plans to prevent the need for pharmacies to manage multiple report card systems. Pharmacies have
access to “performance dashboards” that allow them to review their scores on various quality measures.19 More information about PQS and the EQuIPP system can be found at www.pharmacyquality.com.
Expanding Opportunities in Medicare Part DWhen Medicare Part D was implemented in 2006, coverage for MTM was available only to a small proportion of benefi-ciaries and many plans offered limited services.20 Following the initiation of MTM services, CMS conducted an explor-atory investigation of the services, and released the results in 2008.20 Based in part on the findings of this investigation, CMS issued new requirements for improvements to MTM programs that began in 2010 (available at www.cms.gov/prescriptiondrugcovcontra/).21
Most of these requirements became law as part of the ACA. According to the ACA, starting in 2013, Part D plan sponsors must offer MTM services to targeted beneficiaries that include, at a minimum, strategies to improve adherence to prescription medications or other goals. Services and strategies must include21:
Table 1-1. Examples of Pharmacy Quality Alliance Medication Use Quality Measures
Measure Description
Proportion of days covered The percentage of patients ≥18 years of age who met the proportion of days covered threshold of 80% during the measurement period.
Diabetes medication dosing The percentage of patients who were dispensed a dose higher than the daily recommended dose for the following therapeutic categories of oral hypoglycemic agents: biguanides, sulfonylureas, thiazolidinediones, and dipeptidyl peptidase–4 inhibitors.
Appropriate treatment of hypertension in patients with diabetes
The percentage of patients who were dispensed a medication for diabetes and hypertension and who are receiving an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, or direct renin inhibitor medication.
Medication therapy for persons with asthma
The percentage of patients with asthma who were dispensed >3 canisters of a short-acting β2-agonist inhaler over a 90-day period and who did not receive controller therapy during the same 90-day period. Two rates are reported (i.e., suboptimal control and absence of controller therapy).
Use of high-risk medications in elderly patients
The percentage of patients ≥65 years of age who received ≥2 prescription fills for a high-risk medication during the measurement period.
Cholesterol management in coronary artery disease
The percentage of adult patients diagnosed with coronary artery disease who received ≥1 prescription for a 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitor (i.e., statin) medication during the measurement period.
Completion rate for comprehensive medication review
The percentage of prescription drug plan members who met eligibility criteria for medication therapy management services and who received a comprehensive medication review during the eligibility period.
Antipsychotic use in persons with dementia
The percentage of individuals ≥65 years of age with dementia who are receiving an antipsychotic medication without evidence of a psychotic disorder or related condition.
Source: Reference 17.
Module 1. The Current Landscape for MTM Services 11
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
■■ An annual comprehensive medication review furnished person-to-person or using telehealth technologies (e.g., telephones, videoconferences) by a licensed pharmacist or other qualified provider. The comprehensive medication review must include: —■ A review of the individual’s medications.
■■ This review may result in the creation of a recommended medication action plan or other actions in consultation with the individual and with input from the prescriber to the extent necessary and practicable.
—■ A written or printed summary of the results of the review.
■■ CMS, in consultation with relevant stakeholders, has developed a standardized format for the action plan and the summary that must be used.
■■ Follow-up interventions as warranted based on the findings of the annual medication review or the targeted medication enrollment and which may be provided person-to-person or using telehealth technologies.
Medicare Part D plan sponsors must have a process to21:
■■ Assess, at least on a quarterly basis, the medication use of individuals who are at risk but not enrolled in the MTM program, including individuals who have experienced a transition in care (e.g., a hospital-ization or stay in a skilled nursing facility), if the prescription drug plan sponsor has access to that information.
■■ Automatically enroll targeted beneficiaries, including beneficiaries identified in the quarterly assessment.
■■ Permit beneficiaries to opt out of enrollment in the MTM program.
In 2010, an estimated 25% of Medicare Part D beneficiaries were eligible for MTM services, compared with 10% to 12% in previous years.16 Although eligibility does not necessarily equate with receipt of services, many MTM providers reported an increase in the number of patients receiving MTM services in 2010.22 Pharmacists play a key role in marketing MTM services to patients to help eligible patients take advantage of the benefit provided by their plan.
Part D opportunities have continued to evolve since the imple-mentation of the ACA. Each year in the spring, CMS publishes
a “call letter” for Medicare Part D plans that contains annual adjustments and requirements that Part D plans must implement for the following year. CMS efforts to improve and expand the Part D MTM program and expand the number of patients receiving these services were major themes in the 2014 call letter. CMS encouraged plans to23:
■■ Optimize their MTM programs for beneficiaries who may achieve the greatest benefit.
■■ Offer MTM services to an expanded population of beneficiaries who do not meet eligibility criteria.
■■ Use MTM to promote coordination of care. ■■ Adopt standardized health information technology
for documentation of MTM services. ■■ Promote beneficiary awareness about MTM.
In January 2014, CMS released a proposed rule that includes a number of major changes to the Part D program that had potential to create major shifts for participants in the Part D program. However, the final rule did not include the provi-sions related to the expansion of the MTM program, noting that “the timeline for implementing the proposed changes may be too aggressive and could negatively affect existing MTM programs. While our goal was to increase eligibility and access to MTM, we do not want to do it at the expense of sacrificing any quality with existing programs.” CMS noted that they would continue to monitor Part D plans’ MTM programs, “with the goal of proposing other revisions to criteria in future rulemaking that will help expand the program.”24
CMS Star RatingsCMS rates Medicare Part D plans using a star rating system, from one star to five stars based on their performance and quality. CMS rewards plans having higher ratings with higher payments. In addition, Medicare Advantage and MA-PD plans with a rating of four or more stars receive quality bonus payments. In 2015, quality bonus payments will be based on 2014 ratings, which were based on data from 2012 and 2013.
Star rating information serves an important role for marketing to and enrolling patients. The information is available to beneficiaries in the Medicare Prescription Drug Plan Finder. Plans with five stars have a special icon to encourage enrollment while poorly performing plans have a warning symbol. Plans that receive five stars may market to and enroll beneficiaries throughout the year (i.e., they are not limited to the open enrollment period). Furthermore, after 2014, plans with fewer than three stars for 3 consecutive years will not
Module 1. The Current Landscape for MTM Services 12
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
be permitted to enroll beneficiaries through the Medicare website and they run the risk of being dropped from Medicare altogether.25
Several factors are taken into account when determining the star rating, including customer service measures, beneficiary complaints, member experience with the plan, drug pricing, and patient safety. Within the patient safety section of the ratings, CMS considers PQA measures that can be influenced by pharmacist provision of MTM services. Pharmacists can make the strongest contributions to performance measures that are weighted most heavily for medication use, adherence, and chronic disease outcomes. The use of these measures encourages Part D plans to provide robust MTM services to enrolled beneficiaries. These factors include: (1) the percentage of beneficiaries aged 65 years or older who receive medications with a high risk of adverse effects in elderly patients, and (2) the percentage of beneficiaries who were dispensed a medication for diabetes and a medication for hypertension who were receiving an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker.25
In addition to star ratings, CMS uses “display measures” to provide further information about plans’ quality. In 2013, the display measures included three PQA-supported measures:
■■ Drug-drug interactions.■■ Excessive doses of oral diabetes medications.■■ Completion rate of comprehensive medication
reviews; (this measure may become part of the star ratings calculations in future years).
MTM Beyond MedicareAccording to the core elements model of MTM, “Any patient who uses prescription and nonprescription medications, herbal products, or other dietary supplements could potentially benefit from the MTM core elements outlined in this model. As part of the effort to effectively address the urgent public health issue of medication-related morbidity and mortality, MTM services should be considered for any patient with actual or potential medication-related problems.”7
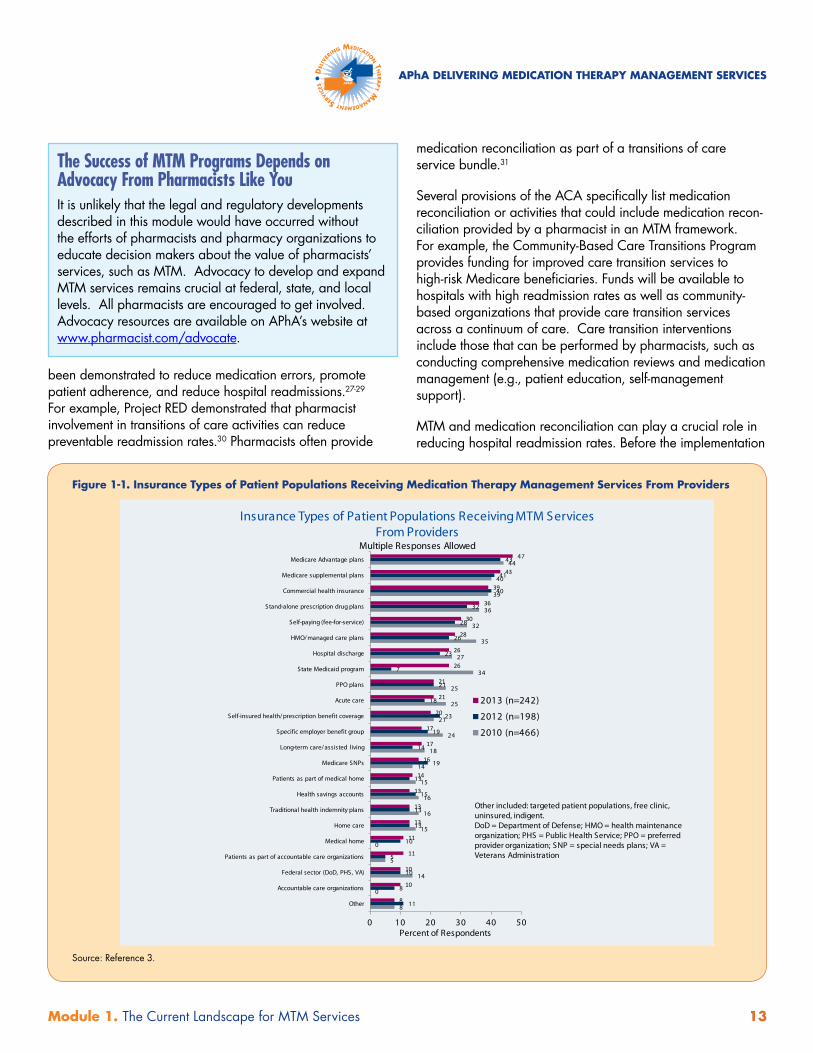
Accordingly, the pool of patients who could benefit from MTM is vast. While Medicare Part D acted as a catalyst for imple-menting MTM services, pharmacists have many opportunities beyond the population of qualified Medicare beneficiaries. A diverse set of third-party payers compensate pharmacists for the provision of MTM services. In a 2013 environmental scan of MTM service providers, more than a dozen types of third-
party payers were represented.3 As figure 1-1 shows, payment opportunities are numerous.
Health Care Reform and MTM: Beyond Part DThe ACA included many provisions that support MTM beyond expanding requirements for Medicare Part D beneficiaries. Among these provisions are the development of ACOs, emphasis on patient-centered medical homes (PCMHs), estab-lishment of the Center for Medicare and Medicaid Innovation within CMS (also known as the CMS Innovation Center, which will be testing MTM among other models), an “Independence at Home” demonstration program, and a hospital preventable readmissions reduction program that includes transition of care activities (e.g., medication reconciliation, post-discharge counseling, home visits).
MTM is an important element of many of these new initiatives. For example, medication reconciliation is the comprehensive evaluation of a patient’s medication regimen any time there is a change of therapy or level of care and is intended to avoid medication-related problems such as omissions, duplications, dosing errors, or drug interactions. Pharmacists can consis-tently and effectively provide medication reconciliation by using the framework of MTM services described in the core elements document.
Additionally, one of the centerpieces of the ACA is an emphasis on integrated care models to improve the quality of care while managing costs. ACOs, medical homes, community health teams, and home-based primary care teams (as well as the use of bundled payments for acute and post-acute care) are among these models. All of these models are structured to compensate providers through Medicare Part B. However, Medicare Part B does not currently cover pharmacists’ clinical services.
The new care models created by the ACA provide financial incentives to the health care organization providing care to share cost savings and receive positive financial incentives for achieving high results on quality metrics. Pharmacists generally must negotiate compensation for their services directly from medical homes and ACOs. Pharmacists who wish to contract with these types of models can justify the cost of their services.
Transitions of Care Activities and Reducing ReadmissionsMedication problems stemming from a lack of coordinated care are a known reason for emergency hospitalizations, especially in older adults.26 Medication reconciliation has
Module 1. The Current Landscape for MTM Services 13
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
been demonstrated to reduce medication errors, promote patient adherence, and reduce hospital readmissions.27-29
For example, Project RED demonstrated that pharmacist involvement in transitions of care activities can reduce preventable readmission rates.30 Pharmacists often provide
medication reconciliation as part of a transitions of care service bundle.31
Several provisions of the ACA specifically list medication reconciliation or activities that could include medication recon-ciliation provided by a pharmacist in an MTM framework. For example, the Community-Based Care Transitions Program provides funding for improved care transition services to high-risk Medicare beneficiaries. Funds will be available to hospitals with high readmission rates as well as community-based organizations that provide care transition services across a continuum of care. Care transition interventions include those that can be performed by pharmacists, such as conducting comprehensive medication reviews and medication management (e.g., patient education, self-management support).
MTM and medication reconciliation can play a crucial role in reducing hospital readmission rates. Before the implementation
The Success of MTM Programs Depends on Advocacy From Pharmacists Like YouIt is unlikely that the legal and regulatory developments described in this module would have occurred without the efforts of pharmacists and pharmacy organizations to educate decision makers about the value of pharmacists’ services, such as MTM. Advocacy to develop and expand MTM services remains crucial at federal, state, and local levels. All pharmacists are encouraged to get involved. Advocacy resources are available on APhA’s website at www.pharmacist.com/advocate.
Figure 1-1. Insurance Types of Patient Populations Receiving Medication Therapy Management Services From Providers
Insurance Types of Patient Populations Receiving MTM Services From Providers
Multiple Responses Allowed
8
0
14
5
0
15
16
16
15
14
18
24
21
25
25
34
27
35
32
36
39
40
44
11
8
10
5
10
13
13
15
13
19
14
19
23
18
21
7
23
26
28
32
40
41
43
8
10
10
11
11
13
13
13
14
16
17
17
20
21
21
26
26
28
30
36
39
43
47
0 10 20 30 40 50
Other
Accountable care organizations
Federal sector (DoD, PHS, VA)
Patients as part of accountable care organizations
Medical home
Home care
Traditional health indemnity plans
Health savings accounts
Patients as part of medical home
Medicare SNPs
Long-term care/ assisted living
Specific employer benefit group
Self-insured health/ prescription benefit coverage
Acute care
PPO plans
State Medicaid program
Hospital discharge
HMO/ managed care plans
Self-paying (fee-for-service)
Stand-alone prescription drug plans
Commercial health insurance
Medicare supplemental plans
Medicare Advantage plans
2013 (n=242)
2012 (n=198)
2010 (n=466)
Percent of Respondents
Other included: targeted patient populations, free clinic, uninsured, indigent.DoD = Department of Defense; HMO = health maintenance organization; PHS = Public Health Service; PPO = preferred provider organization; SNP = special needs plans; VA = Veterans Administration
Source: Reference 3.
Module 1. The Current Landscape for MTM Services 14
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
of the ACA, approximately 19% of hospitalized Medicare patients were readmitted to the hospital within 30 days of discharge.32 Readmission rates following a nonsurgical hospi-talization were higher for chronic conditions than for acute conditions, suggesting that poor chronic care contributes to readmission rates. Furthermore, post-discharge adverse events attributed to medications are one of the most common reasons for readmissions.33
The ACA creates a quality improvement program to help hospitals improve their readmission rates. These provisions have increased focus on robust discharge planning, including post-discharge medication reconciliation and medication management (e.g., patient assessment, providing patient education) by pharmacists. The ACA also created penalties for hospitals with excess readmissions. When then penalties began in October 2012, they were calculated based on all-cause 30-day readmission rates for patients with heart failure, pneumonia, and acute myocardial infarction. In 2015, the penalties will expand to include patients with chronic obstructive pulmonary disease, coronary artery bypass graft, percutaneous transluminal coronary angioplasty, and other vascular procedures. Moving forward, the penalties will be expanded to include more disease states.
Initial data indicate that the national readmission reduction program is having a beneficial effect. The all-cause 30-day hospital readmission rate among Medicare fee-for-service beneficiaries held constant at 19% from 2007 to 2011. In 2012, when the penalties were first implemented, this rate began to fall to 18.5%. Preliminary claims data show the Medicare readmission rate averaged less than 18% over the first 8 months of 2013.34 Pharmacists are involved in many of the models focused on reducing readmissions and improving transitions of care.
Patient-Centered Medical HomesIn 2007, the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association released a joint statement describing the concept of the PCMH. In the PCMH model, care is coordinated by primary care providers across all elements of the health care system (e.g., specialty care, hospitals, home health agencies, nursing homes) and the patient’s community (e.g., family, public and private community-based services). Care coordination among physi-cally dispersed providers is facilitated by registries, information technology, health information exchanges, and other means to ensure that patients get the indicated care when and
where they need and want it in a culturally and linguistically appropriate manner.35 In this model, providers are eligible to receive additional compensation for care coordination.
The ACA included provisions designed to promote the adoption of PCMH as a model for delivering primary care, with additional payment for improved quality of care. The law defined PCMH as a model of care that includes8:
■■ A primary care provider.■■ Whole person orientation.■■ Coordinated and integrated care.■■ Safe and high-quality care (including evidence-
based medicine, appropriate use of health information technology, continuous quality improvement).
■■ Expanded access to care. ■■ Payment that recognizes the added value of patient-
centered care.
These programs are intended to help coordinate disease prevention, health promotion, chronic disease management, and transitions between health care providers and settings, with priority given to preventive services.
Pharmacists can play integral roles in optimizing therapeutic outcomes and promoting safe, cost-effective medication use in PCMHs.36-39 For example, pharmacists can manage medication therapies for selected patients with chronic condi-tions in a more cost-effective manner than physicians, and pharmacists can discuss and help implement therapy recom-mendations with other care providers through the use of health information systems. This type of model allows the primary care practice to care for an increased number of patients by using pharmacists as extenders of the primary care model through collaborative relationships.
Prior to enactment of the ACA, pharmacists were already working in roles in medical home settings, often focusing on collaborative drug therapy.40,41 According to an article in Health Affairs, “Pharmacists should play key roles as team members in medical homes....”36 The ACA expands the roles for pharmacists in the PCMH model. According to the ACA, local primary care providers should be able to provide access to pharmacist-delivered MTM services. Transitional care programs must provide medication reconciliation upon admission/discharge and ensure that post-discharge plans include medication management. These programs include higher reimbursement rates for services if requirements such as medication reconciliation are completed, providing a
Module 1. The Current Landscape for MTM Services 15
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
financial incentive for primary care practices to collaborate with pharmacists as well. There are a number of collaborative opportunities for pharmacy services to be integrated into a successful PCMH.
Services provided by pharmacists in medical homes have included shared medical appointments with the physician and pharmacist, providing MTM services, assisting with transitions of care and medication reconciliation, diabetes services, running anticoagulation and osteoporosis clinics, providing interprofessional education, leading group patient education classes, and participating in continuous quality improvement initiatives.13,39,42
Providers in medical homes have reported experiencing enhanced value from integrating pharmacists’ services. In one survey of participants in a medical home model, respondents reported that inclusion of a pharmacist in their practice improved the quality of patient care, provided a valuable drug information resource for all providers and staff, and empowered patients. Furthermore, initial concerns
Figure 1-2. Example of a Standard for Patient-Centered Medical Homes From the National Committee for Quality Assurance
The practice has a process for managing medications, and systematically implements the process in the following ways:
1. Reviews and reconciles medications for more than 50% of patients received from care transitions. (CRITICAL FACTOR)
2. Reviews and reconciles medications with patients/families for more than 80% of care transitions.
3. Provides information about new prescriptions to more than 80% of patients/families/caregivers.
4. Assesses understanding of medications for more than 50% of patients/families/caregivers, and dates the assessment.
5. Assesses response to medications and barriers to adherence for more than 50% of patients, and dates the assessment.
6. Documents over-the-counter medications, herbal therapies, and supplements for more than 50% of patients, and dates the updates.
Source: Reference 43.
of the clinical and nonclinical staff regarding the utility of a pharmacist in the practice disappeared within the first months of pharmacist integration.13
Medical Home Quality MeasuresThe National Committee for Quality Assurance (NCQA) accredits and certifies a wide range of health care organiza-tions, including PCMHs. The NCQA 2014 standards and guidelines for PCMHs include factors that can be impacted by MTM. For example, within the “care management and support” category, several factors affect the “medication management” element (figure 1-2).43
Accountable Care OrganizationsAn ACO is a health care model that provides greater reimbursement or shared savings to coordinated groups of health care providers who meet certain quality measures while reducing the total cost of care for a specific population of patients. (While ACOs and medical homes have similar goals, an ACO is a financing model whereas a medical home is a care delivery model. An ACO may include practices that have organized themselves as PCMHs.)
ACOs are accountable for the quality and cost of patient care. They share financial risk as well as year-end savings if quality and cost thresholds are met. ACO structures vary widely, often reflecting the leading entity of the ACO (i.e., single or multiple insurers, independent physician practices, health systems, or pharmacy networks and/or providers). The ACA authorized two Medicare ACO initiatives within CMS—the Pioneer ACO demonstration and the Medicare Shared Savings Program. The development of these ACOs has spurred the development of many non-Medicare ACOs in the private sector in numerous markets. In addition, a few state Medicaid programs have developed ACOs and more are expected to follow suit.44
ACOs are instituting programs that increasingly engage pharmacists in both population heath management and direct patient care services. From a population health management perspective, pharmacists review an ACO’s entire patient panel to identify those at risk for medication-related problems due to gaps in care; assist in the development and management of best practices to improve gaps in care; and help assess, measure, and improve medication-related quality metrics.44
For direct patient care, ACOs are engaging pharmacists to provide a variety of services focused on improving care transitions, medication adherence, medication management,
Module 1. The Current Landscape for MTM Services 16
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
and chronic disease management. For example, after patients are identified (either through physician referral or population health management targeting), ACOs utilize pharmacists to deliver comprehensive medication reviews to identify and resolve medication problems and then monitor patients over multiple visits until medication-related goals are achieved. Because chronic diseases are primarily managed through appropriate medication use, pharmacists often concurrently manage the patient’s chronic conditions in collaboration with the health care team to achieve clinical care goals. Collaborative practice agreements between pharmacists and prescribers may be in place to facilitate efficient delivery of these services.45
Increasingly, ACOs are involving pharmacists as part of care transition teams that engage with patients from hospital admission, throughout the stay, and continue to monitor them at home after discharge. Pharmacists are also assisting ACOs in identifying patients who are nonadherent or at risk of being nonadherent to their medication regimen and implementing services to improve patient medication adherence.44
ACO Quality MeasuresMedicare ACOs (i.e., the Pioneer ACO and the Medicare Shared Savings Program) share a common set of 33 quality metrics, 12 of which are directly related to medications or
Learning ActivityIndicate whether each of the following statements about the ACA is true or false:
1. The law requires prescription drug plans to automatically enroll targeted beneficiaries in MTM services.
2. The law requires annual comprehensive medication reviews but does not address targeted reviews.
3. The law requires the development of a standardized format for the patient medication record and action plan that was implemented in 2013.
Match each of the following models included in the ACA with the correct description:
4. Patient-centered medical home
5. Accountable care organizations
6. Transition of care activities
a. A financing model in which entities (e.g., provider groups) are accountable for the quality and cost of patient care.
b. A patient care model in which patient care is coordinated by primary care providers across all elements of the health care system.
c. Provisions intended to reduce hospital readmission rates through strategies including medication reconciliation, patient education, and medication adherence interventions.
Answers are located at the bottom of the page.
Learning Activity Answer Key1. True; 2. False; 3. True; 4. b; 5. a; 6. c.
pharmacist-provided services, as well as other measures that can be influenced by pharmacists, such as health promotion and education.
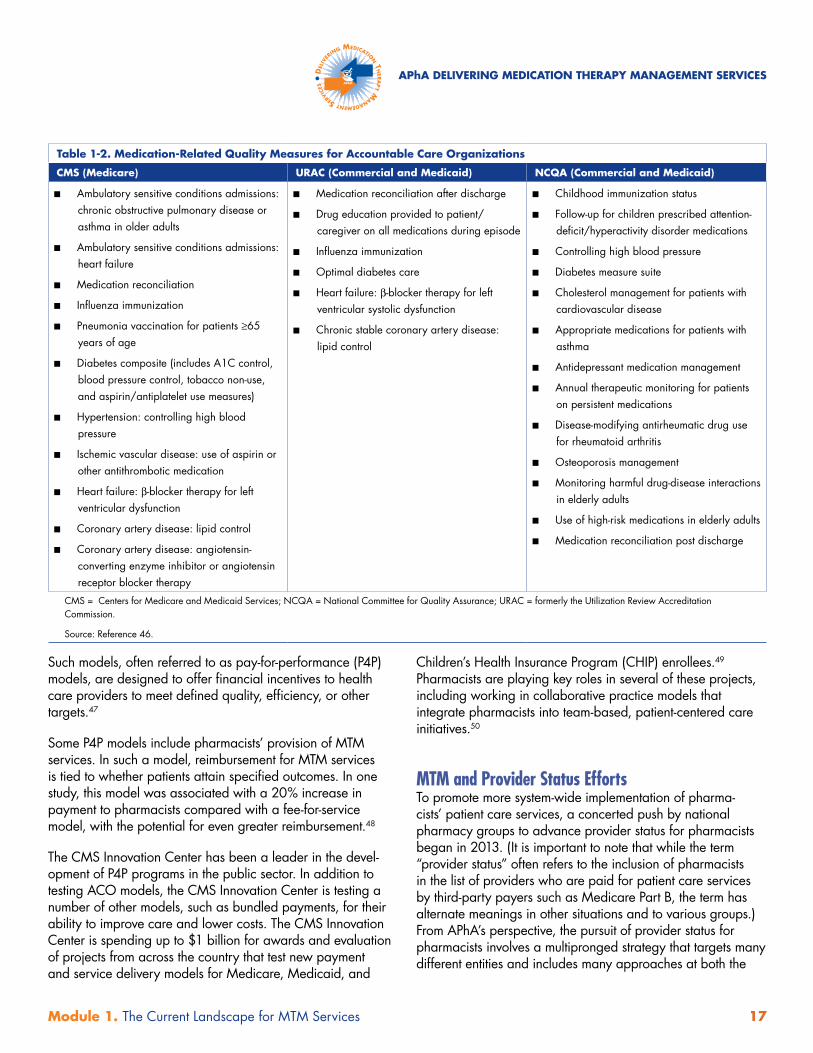
Commercial and Medicaid ACOs use a variety of quality metrics with little standardization among them. Some commercial payers require the ACOs with whom they contract to be accredited. Currently, there are at least two accred-iting agencies that offer ACO accreditation: URAC (formerly known as the Utilization Review Accreditation Commission) and NCQA. Both agencies include medication-related quality metrics in their accreditation requirements. tABle 1-2 summa-rizes medication-related quality measures evaluated by CMS and the accrediting agencies. While these measures will have the most direct influence on an ACO’s approach to medication use, nearly all quality measures contain, in one way or another, a medication component.46
Other Pay-for-Performance InitiativesIn addition to ACOs and PCMHs, several other types of models reward providers for delivering high-quality care.
Module 1. The Current Landscape for MTM Services 17
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
Such models, often referred to as pay-for-performance (P4P) models, are designed to offer financial incentives to health care providers to meet defined quality, efficiency, or other targets.47
Some P4P models include pharmacists’ provision of MTM services. In such a model, reimbursement for MTM services is tied to whether patients attain specified outcomes. In one study, this model was associated with a 20% increase in payment to pharmacists compared with a fee-for-service model, with the potential for even greater reimbursement.48
The CMS Innovation Center has been a leader in the devel-opment of P4P programs in the public sector. In addition to testing ACO models, the CMS Innovation Center is testing a number of other models, such as bundled payments, for their ability to improve care and lower costs. The CMS Innovation Center is spending up to $1 billion for awards and evaluation of projects from across the country that test new payment and service delivery models for Medicare, Medicaid, and
Children’s Health Insurance Program (CHIP) enrollees.49 Pharmacists are playing key roles in several of these projects, including working in collaborative practice models that integrate pharmacists into team-based, patient-centered care initiatives.50
MTM and Provider Status EffortsTo promote more system-wide implementation of pharma-cists’ patient care services, a concerted push by national pharmacy groups to advance provider status for pharmacists began in 2013. (It is important to note that while the term “provider status” often refers to the inclusion of pharmacists in the list of providers who are paid for patient care services by third-party payers such as Medicare Part B, the term has alternate meanings in other situations and to various groups.) From APhA’s perspective, the pursuit of provider status for pharmacists involves a multipronged strategy that targets many different entities and includes many approaches at both the
Table 1-2. Medication-Related Quality Measures for Accountable Care Organizations
CMS (Medicare) URAC (Commercial and Medicaid) NCQA (Commercial and Medicaid)
■■ Ambulatory sensitive conditions admissions: chronic obstructive pulmonary disease or asthma in older adults
■■ Ambulatory sensitive conditions admissions: heart failure
■■ Medication reconciliation
■■ Influenza immunization
■■ Pneumonia vaccination for patients ≥65 years of age
■■ Diabetes composite (includes A1C control, blood pressure control, tobacco non-use, and aspirin/antiplatelet use measures)
■■ Hypertension: controlling high blood pressure
■■ Ischemic vascular disease: use of aspirin or other antithrombotic medication
■■ Heart failure: β-blocker therapy for left ventricular dysfunction
■■ Coronary artery disease: lipid control
■■ Coronary artery disease: angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapy
■■ Medication reconciliation after discharge
■■ Drug education provided to patient/caregiver on all medications during episode
■■ Influenza immunization
■■ Optimal diabetes care
■■ Heart failure: β-blocker therapy for left ventricular systolic dysfunction
■■ Chronic stable coronary artery disease: lipid control
■■ Childhood immunization status
■■ Follow-up for children prescribed attention-deficit/hyperactivity disorder medications
■■ Controlling high blood pressure
■■ Diabetes measure suite
■■ Cholesterol management for patients with cardiovascular disease
■■ Appropriate medications for patients with asthma
■■ Antidepressant medication management
■■ Annual therapeutic monitoring for patients on persistent medications
■■ Disease-modifying antirheumatic drug use for rheumatoid arthritis
■■ Osteoporosis management
■■ Monitoring harmful drug-disease interactions in elderly adults
■■ Use of high-risk medications in elderly adults
■■ Medication reconciliation post discharge
CMS = Centers for Medicare and Medicaid Services; NCQA = National Committee for Quality Assurance; URAC = formerly the Utilization Review Accreditation Commission.
Source: Reference 46.

Module 1. The Current Landscape for MTM Services 18
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
state and federal levels. APhA also believes provider status advancement is critical to expanding the number of patients who can benefit from pharmacists’ patient care services.
As part of its provider status efforts, APhA is a founding member of the Patient Access to Pharmacists’ Care Coalition (PAPCC). The PAPCC mission is to develop and help enact a federal policy proposal that would enable patient access to, and payment for, Medicare Part B services by state-licensed pharmacists in medically underserved communities. Inclusion of pharmacists as providers under Medicare Part B also would position them for inclusion as critical members of team-based care models.
In March 2014, H.R. 4190 was introduced in the House by Representatives Brett Guthrie (R-KY), G.K. Butterfield (D-NC), and Todd Young (R-IN). H.R. 4190 amends Title XVIII of the Social Security Act to enable patient access to, and coverage for, Medicare Part B services by state-licensed pharmacists in medically underserved communities. Pharmacists should stay apprised of legislative activity that can impact opportunities to provide MTM and other patient care services. While it remains to be seen whether this bill will progress through the legislative process, it is one example of the many ongoing developments in the push to obtain pharmacists’ provider status. All pharma-cists are encouraged to stay apprised of ongoing develop-ments and explore opportunities to advocate on behalf of their profession.
Each state provides its own legislative and regulatory oppor-tunities for advancing the pharmacy profession. Potential strategies include seeking changes in Medicaid programs to include coverage for pharmacist-provided services as well as seeking the expansion of states’ scope of practice and the services pharmacists can legally perform in each state. For example, in 2013, California passed legislation (SB 493) that provides new practice authorities for pharmacists in the state. (While the new law specifically designates pharmacists as health care providers, it does not address payment issues.) Examples of the expanded authorities include: ordering and interpreting tests to monitor and manage the efficacy and toxicity of drug therapies, and initiating and administering routine vaccinations. The law also creates a new practitioner title for pharmacists—Advanced Practice Pharmacist (APP)—and provides additional authorities to pharmacists who receive the APP credential.51 The California Pharmacists Association website provides a detailed summary of authorities granted to pharmacists under the new the law.52 North Carolina and New Mexico have similar practitioner titles with expanded scope of practice for pharmacists.
ConclusionMMA was a powerful catalyst for MTM services, triggering the development of a profession-wide consensus definition and model of care. The success of many of these programs at both reducing costs and improving the quality of care has led to a steady expansion of services, with continued growth in opportunities expected over the next several years. Moreover, the provision of MTM services on a larger scale is expected to result in safer medication use for patients, greater professional fulfillment for pharmacists, and national recognition of the value of MTM services provided by pharmacists.
References1. IMS Health. IMS health study identifies $200+ billion annual
opportunity from using medicines more responsibly [press release]. June 19, 2013. Available at: http://www.imshealth.com/portal/site/imshealth/menuitem.c76283e8bf81e98f53c753c71ad8c22a/?vgnextoid=12531cf4cc75f310VgnVCM10000076192ca2RCRD&vgnextfmt=default. Accessed April 16, 2014.
2. U.S. Department of Health and Human Services. Healthy People 2020: Topics and objectives index. Available at: http://healthypeople.gov/ 2020/topicsobjectives2020/default.aspx. Accessed May 13, 2014.
3. American Pharmacists Association. Medication Therapy Management Digest. The Pursuit of Provider Status to Support the Growth and Expansion of Pharmacists’ Patient Care Services. March 2014. Available at: http://www.pharmacist.com/sites/default/files/MTM %20Digest_2014%20FINAL.pdf. Accessed May 13, 2014.
4. Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes Through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service. December 2011.
5. Rovers JP, Currie JE, Hagel HP, eds. A Practical Guide to Pharmaceutical Care. 2nd ed. Washington, DC: American Pharmacists Association; 2003.
6. Bluml BM. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc. 2005;45:566–72.
7. American Pharmacists Association; National Association of Chain Drug Stores Foundation. Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model. Version 2.0. March 2008. Available at: http://www.pharmacist.com/MTM. Accessed September 20, 2011.
8. Patient Protection and Affordable Care Act. H.R. 3590. Available at: http://www.gpo.gov/fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf. Accessed May 13, 2014.
9. Centers for Medicare and Medicaid Services. Medicare Part D Medication Therapy Management Program Standardized Format. Available at: http://www.cms.gov/medicare/prescription-drug-coverage/prescriptiondrugcovcontra/downloads/mtm-program-standardized-format-english-and-spanish-instructions-samples-v032712.pdf. Accessed May 13, 2014.

Module 1. The Current Landscape for MTM Services 19
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
10. Berger BA. Interacting with physicians. In: Berger BA, ed. Communication Skills for Pharmacists: Building Relationships, Improving Patient Care. 2nd ed. Washington, DC: American Pharmacists Association; 2005:131–9.
11. Zierler-Brown S, Brown TR, Chen D, Blackburn RW. Clinical documentation for patient care: models, concepts, and liability considerations for pharmacists. Am J Health Syst Pharm. 2007;64:1851–8.
12. Chrischilles EA, Carter BL, Lund BC, et al. Evaluation of the Iowa Medicaid pharmaceutical case management program. J Am Pharm Assoc. 2004;44:337–49.
13. Smith M, Giuliano MR, Starkowski MP. In Connecticut: improving patient medication management in primary care. Health Aff. 2011;30:646–54.
14. Isetts BJ, Schondelmeyer SW, Artz MB, et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J Am Pharm Assoc. 2008;48:203–11.
15. Health Resources and Services Administration. HRSA’s Patient Safety and Clinical Pharmacy Services Collaborative. Available at: http://www.hrsa.gov/ruralhealth/media/508ehrincentive052609.pdf. Accessed May 13, 2014.
16. Centers for Medicare and Medicaid Services. 2010 Medicare Part D Medication Therapy Management (MTM) Programs. Fact Sheet. June 8, 2010. Available at: https://www.cms.gov/prescriptiondrugcovcontra/082_mtm.asp. Accessed October 12, 2011.
17. PQA Pharmacy Quality Alliance. PQA measures. Available at: http://pqaalliance.org/measures/default.asp. Accessed May 13, 2014.
18. Shiyanbola OO, Mort JR, Lyons K. Advancing the use of community pharmacy quality measures: a qualitative study. J Am Pharm Assoc. 2013;53:400–7.
19. Pharmacy Quality Solutions. Available at: http://www.pharmacy quality.com. Accessed May 13, 2014.
20. Abt Associates Inc. Final Report: Exploratory Research on Medication Therapy Management. Cambridge, MA: Abt Associates Inc.; July 8, 2008.
21. Centers for Medicare and Medicaid Services. 2010 Combined Call Letter. March 30, 2009. Available at: https://www.cms.gov/prescriptiondrugcovcontra. Accessed July 13, 2011.
22. American Pharmacists Association. Medication Therapy Management Digest. Tracking the Expansion of MTM in 2010: Exploring the Consumer Perspective. March 2011. Available at: http://www.pharmacist.com/AM/Template.cfm?Section=MTM&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=25712. Accessed May 27, 2014.
23. Centers for Medicare and Medicaid Services. Announcement of Calendar Year (CY) 2014 Medicare Advantage Capitation Rates and Medicare Advantage and Part D Payment Policies and Final Call Letter. April 1, 2013. Available at: http://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Downloads/Announcement2014.pdf. Accessed May 13, 2014.
24. Centers for Medicare and Medicaid Services. Medicare Program; Contract year 2015 policy and technical changes to the Medicare Advantage and the Medicare Prescription Drug Benefit programs. May 23, 2014. Federal Register. 2014;79:29844–968. Available at: http://www.gpo.gov/fdsys/pkg/FR-2014-05-23/pdf/2014-11734.pdf. Accessed June 19, 2014.
25. American Pharmacists Association; Academy of Managed Care Pharmacy. Medicare star ratings: stakeholder proceedings on community pharmacy and managed care partnerships in quality. J Am Pharm Assoc. 2014;54:228–40.
26. Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med. 2011;365:21;2002–12.
27. Kripalani S, Jackson AT, Schnipper JL, Coleman EA. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2:314–23.
28. Cua YM, Kripalani S. Medication use in the transition from hospital to home. Ann Acad Med Singapore. 2008;37:136–6.
29. American Pharmacists Association. Improving Care Transitions: Optimizing Medication Reconciliation. March 2012. Available at: http://www.pharmacist.com/sites/default/files/files/2012_improving_care_transitions.pdf. Accessed June 11, 2014.
30. Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization. Ann Intern Med. 2009;150:178–87.
31. Kwan JL, Lo L, Sampson M, Shjania K. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Inter Med. 2012;158(5 pt 2):397–403.
32. Ventura T, Brown D, Archibald T, et al. Improving care transitions and reducing hospital readmissions. Remington Report. January/February 2010. Available at: http://www.amedisys.com/images/news/care_ transition_article_remington_report_jan_2010. Accessed May 13, 2014.
33. Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare. June 2007. Available at: http://www.medpac.gov/documents/jun07_entirereport.pdf. Accessed May 13, 2014.
34. Centers for Medicare and Medicaid Services. The CMS Blog. New data shows Affordable Care Act reforms are leading to lower hospital readmission rates for Medicare beneficiaries. December 6, 2013. Available at: http://blog.cms.gov/2013/12/06/new-data-shows-affordable-care-act-reforms-are-leading-to-lower-hospital-readmission-rates-for-medicare-beneficiaries. Accessed May 13, 2014.
35. American Academy of Family Physicians; American Academy of Pediatrics; American College of Physicians; American Osteopathic Association. Joint Principles of the Patient-Centered Medical Home. February 2007. Available at: http://www.pcpcc.net/content/joint-principles-patient-centered-medical-home. Accessed October 13, 2011.
36. Smith M, Bates DW, Bodenheimer T, Cleary PD. Why pharmacists belong in the medical home. Health Aff. 2010;29:906–13.
37. American College of Clinical Pharmacy. Integration of Pharmacists’ Clinical Services in the Patient-Centered Primary Care Medical Home. March 2009. Available at: http://www.accp.com/docs/misc/pcmh_services.pdf. Accessed October 13, 2011.
38. Scott MA, Hitch B, Ray L, Colvin G. Integration of pharmacists into a patient-centered medical home. J Am Pharm Assoc. 2011;51:161–6.
39. Moczygemba LR, Goode JV, Gatewood SB, et al. Integration of collaborative medication therapy management in a safety net patient-centered medical home. J Am Pharm Assoc. 2011;51:167–72.
40. Worth T. Tick tock, tick tock: clock running out on Capitol Hill. Pharmacy Today. December 2009:13–4.
Module 1. The Current Landscape for MTM Services 20
DEL
IVER
ING MEDICATIO
N TH
ERA
PY M
ANAGEMENT SERVI
CES
APhA DELIVERING MEDICATION THERAPY MANAGEMENT SERVICES
41. Erickson S, Hambleton J. A pharmacy’s journey toward the patient-centered medical home. J Am Pharm Assoc. 2011;51:156–60.
42. Kozminski M, Busby R, McGivney MS, et al. Pharmacist integration into the medical home: qualitative analysis. J Am Pharm Assoc. 2011;51:173–83.
43. National Committee for Quality Assurance. NCQA standards and guidelines 2014. Available at: http://store.ncqa.org/index.php/recognition/patient-centered-medical-home-pcmh/2014-pcmh-standards-and-guidelines-epub-single-user.html. Accessed June 19, 2014.
44. American Pharmacists Association. Issue Brief #8—ACOs: Highlights and Considerations for Pharmacists. March 2014. Available at: http://www.pharmacist.com/apha-accountable-care-organization-aco-briefs. Accessed April 21, 2014.
45. American Pharmacists Association. Issue Brief #6—ACO Engagement of Pharmacists. March 2014. Available at: http://www.pharmacist.com/apha-accountable-care-organization-aco-briefs. Accessed April 21, 2014.
46. American Pharmacists Association. Issue Brief #5—ACO Approaches to Medication Use. February 2014. Available at: http://www.pharmacist.com/apha-accountable-care-organization-aco-briefs. Accessed April 21, 2014.
47. Agency for Healthcare Research and Quality. Pay for Performance (P4P): AHRQ Resources. Available at: http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/pay4per/index.html. Accessed May 13, 2014.
48. Lenz T, Monaghan MS. Pay-for-performance model of medication therapy management in pharmacy practice. J Am Pharm Assoc. 2011;51:425–31.
49. Centers for Medicare and Medicaid Services. Health Care Innovation Awards Round Two. Available at: http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Round-2.html. Accessed September 11, 2013.
50. Centers for Medicare and Medicaid Services. Health Care Innovation Awards: Virginia. Available at: http://innovation.cms.gov/initiatives/Health-Care-Innovation-Awards/Virginia.html. Accessed October 3, 2013.
51. Pharmacy practice. California Senate Bill 493, 469 (2013). Available at: http://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201320140SB493. Accessed May 27, 2014.
52. California Pharmacists Association. What does SB 493 mean for me? Available at: http://www.cpha.com/Portals/45/Docs/CEO%20Message%20Misc/SB493FactGuide.pdf. Accessed May 27, 2014.
Appendix A
Medication Therapy Management Services Definition and Program Criteria
Medication Therapy Management is a distinct service or group of services that optimize therapeutic outcomes for individual patients. Medication Therapy Management Services are independent of, but can occur in conjunction with, the provision of a medication product.
Medication Therapy Management encompasses a broad range of professional activities and responsibilities within the licensed pharmacist’s, or other qualified health care provider's, scope of practice. These services include but are not limited to the following, according to the individual needs of the patient:
a. Performing or obtaining necessary assessments of the patient’s health status; b. Formulating a medication treatment plan; c. Selecting, initiating, modifying, or administering medication therapy; d. Monitoring and evaluating the patient’s response to therapy, including safety and
effectiveness; e. Performing a comprehensive medication review to identify, resolve, and prevent medication-
related problems, including adverse drug events; f. Documenting the care delivered and communicating essential information to the patient’s
other primary care providers; g. Providing verbal education and training designed to enhance patient understanding and
appropriate use of his/her medications; h. Providing information, support services and resources designed to enhance patient adherence
with his/her therapeutic regimens; i. Coordinating and integrating medication therapy management services within the broader
health care-management services being provided to the patient.
A program that provides coverage for Medication Therapy Management Services shall include: a. Patient-specific and individualized services or sets of services provided directly by a
pharmacist to the patient*. These services are distinct from formulary development and use, generalized patient education and information activities, and other population-focused quality assurance measures for medication use.
b. Face-to-face interaction between the patient* and the pharmacist as the preferred method of delivery. When patient-specific barriers to face-to-face communication exist, patients shall have equal access to appropriate alternative delivery methods. Medication Therapy Management programs shall include structures supporting the establishment and maintenance of the patient*-pharmacist relationship.
c. Opportunities for pharmacists and other qualified health care providers to identify patients who should receive medication therapy management services.
d. Payment for Medication Therapy Management Services consistent with contemporary provider payment rates that are based on the time, clinical intensity, and resources required to provide services (e.g., Medicare Part A and/or Part B for CPT & RBRVS).
e. Processes to improve continuity of care, outcomes, and outcome measures.
* In some situations, Medication Therapy Management Services may be provided to the caregiver or other persons involved in the care of the patient.
Approved July 27, 2004 by the Academy of Managed Care Pharmacy, the American Association of Colleges of Pharmacy, the American College of Apothecaries, the American College of Clinical Pharmacy, the American Society of Consultant Pharmacists, the American Pharmacists Association, the American Society of Health-System Pharmacists, the National Association of Boards of Pharmacy**, the National Association of Chain Drug Stores, the National Community Pharmacists Association and the National Council of State Pharmacy Association Executives. ** Organization policy does not allow NABP to take a position on payment issues.

Medication Therapy Management inPharmacy Practice Core Elements of an MTM Service Model
Version 2.0 March 2008
Appendix B

1
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
AcknowledgmentThe American Pharmacists Association and the National Association of Chain Drug Stores Foundation respectfully acknowledge the contributions of all individuals and organizations that participated in the development of Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 document for application across the pharmacy profession.
This service model is supported by the following organizations:
Academy of Managed Care Pharmacy
American Association of Colleges of Pharmacy
American College of Apothecaries
American College of Clinical Pharmacy
American Society of Consultant Pharmacists
American Society of Health-System Pharmacists
National Alliance of State Pharmacy Associations
National Community Pharmacists Association
© 2008 American Pharmacists Association and National Association of Chain Drug Stores Foundation. All rights reserved.
Core Elements of an MTM Service Model
Medication Therapy Management in Pharmacy Practice:
Version 2.0A joint initiative ofthe American Pharmacists Association andthe National Association of Chain Drug Stores Foundation
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form, or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior permission of the American Pharmacists Association and the National Association of Chain Drug Stores Foundation, with the sole exception that Appendices C and D may be reproduced, stored, or transmitted without permission.

2
PrefaceEleven national pharmacy organizations achieved consensus on a defi nition of medication therapy management (MTM) in July 2004 (Appendix A). Building on the consensus defi nition, the American Pharmacists Association and the National Association of Chain Drug Stores Foundation developed a model framework for implementing effective MTM services in a community pharmacy setting by publishing Medication Therapy Management in Community Pharmacy Practice: Core Ele-ments of an MTM Service Version 1.0. The original version 1.0 document described the foundational or core elements of MTM services that could be provided by pharmacists across the spectrum of community pharmacy.1
Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 is an evolutionary document that focuses on the provision of MTM services in settings where patients* or their caregivers can be actively involved in managing their medications. This service model was developed with the input of an advisory panel of pharmacy leaders representing diverse pharmacy practice settings (listed in Addendum). While adoption of this model is voluntary, it is important to note that this model is crafted to maximize both effectiveness and effi ciency of MTM service delivery across pharmacy practice settings in an effort to improve continuity of care and patient outcomes.
*In this document, the term patient refers to the patient, the caregiver, or other persons involved in the care of the patient.
Notice: The materials in this service model are provided only for general informational purposes and do not constitute business or legal advice. The National Association of Chain Drug Stores Foundation and the American Pharmacists Association assume no responsibility for the accuracy or timeliness of any information provided herein. The reader should not under any circumstances solely rely on, or act on the basis of, the materials in this service model. These materials and information are not a substitute for obtaining business or legal advice in the appropriate jurisdiction or state.
The materials in this service model do not represent a standard of care or standard business practices. This service model may not be appropriate for all pharmacists or pharmacies. Service programs should be designed based on unique needs and circumstances and model examples should be modifi ed as appropriate.
Nothing contained in this service model shall be construed as an express or implicit invitation to engage in any illegal or anticompetitive activity. Nothing contained in this service model shall, or should be, construed as an endorsement of any particular method of treatment or pharmacy practice in general.

3
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
IntroductionMedication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 is designed to improve collaboration among pharmacists, physicians, and other healthcare professionals; enhance communication between patients and their healthcare team; and optimize medication use for improved patient outcomes. The medication therapy management (MTM) services described in this model empower patients to take an active role in managing their medications. The services are dependent upon pharmacists working collaboratively with physicians and other healthcare professionals to optimize medication use in accordance with evidence-based guidelines.2,3
MTM services,* as described in this model, are distinct from medication dispensing and focus on a patient-centered, rather than an individual product-centered, process of care.4 MTM services encompass the assessment and evalu-ation of the patient’s complete medication therapy regimen, rather than focusing on an individual medication product. This model framework describes core elements of MTM service delivery in pharmacy practice and does not represent a specifi c minimum or maximum level of all services that could be delivered by pharmacists.5
Medication-related problems are a signifi cant public health issue within the healthcare system. Incidence estimates suggest that more than 1.5 million preventable medication-related adverse events occur each year in the United States, accounting for an excess of $177 billion in terms of medication-related morbidity and mortality.6,7 The Institute of Medicine advocates that healthcare should be safe, effective, patient-centered, timely, effi cient, and effective to meet patients’ needs and that patients should be active participants in the healthcare process to prevent medica-tion-related problems.3,7
MTM services, as described in this service model, may help address the urgent public health need for the prevention of medication-related morbidity and mortality.3 MTM services may contribute to medication error prevention, result in improved reliability of healthcare delivery, and enable patients to take an active role in medication and healthcare self-management.7 The MTM services outlined in this model are aligned with the Centers for Medicare & Medicaid
Services’ expectations, as stated in the Medicare Prescrip-tion Drug, Improvement, and Modernization Act of 2003, that MTM services will enhance patients’ understanding of appropriate drug use, increase adherence to medication therapy, and improve detection of adverse drug events.8
MTM programs are demonstrating positive clinical, economic, and humanistic outcomes across diverse patient populations in various patient care settings.9–15 MTM services are currently being delivered in both the public and private sectors. In the public sector, some state Medicaid and Medicare Part D plans have focused on a comprehen-sive medication therapy review as the foundation of their MTM programs. Pharmacists participating in these programs often provide patients with an initial compre-hensive assessment and ongoing follow-up assessments to identify and resolve medication-related problems.11, 16–20
In the private sector, MTM programs are beginning to emerge nationwide, offering MTM services to traditional insured groups, managed-care populations, self-insured employers, and self-paying individual patients.9,10,12
Any patient who uses prescription and nonprescription medications, herbal products, or other dietary supple-ments could potentially benefi t from the MTM core elements outlined in this model. As part of the effort to effectively address the urgent public health issue of medication-related morbidity and mortality, MTM services should be considered for any patient with actual or potential medication-related problems, regardless of the number of medications they use, their specifi c disease states, or their health plan cover-age. Although MTM program structure and the needs of individual patients may vary, the use of a consistent and recognizable framework for core MTM services, as described in this model, will enhance their effi cient delivery and effective quality measurement. As new opportunities arise, pharmacists in all practice settings must share a common vision for patient-centered MTM services that improve medication therapy outcomes and provide value within our nation’s healthcare system.
* MTM services are built upon the philosophy and process of pharmaceutical care that was fi rst implemented in pharmacy practice in the early 1990s. As pharmacy education, training, and practice continue to evolve to a primarily clinical “patient-centered” focus, pharmacists are gaining recognition from other healthcare professionals and the public as “medication therapy experts.” Recognizing the pharmacist’s role as the medication therapy expert, the pharmacy profession has developed a consensus defi nition for medication therapy management and is increasingly using this term to describe the services provided by pharmacists to patients.

4
Framework for Pharmacist-Provided MTM ServicesThis framework for MTM service delivery in pharmacy practice is designed to facilitate collaboration among the pharmacist, patient, physician, and other healthcare profes-sionals to promote safe and effective medication use and achieve optimal patient outcomes. MTM services in all patient care settings should include structures supporting the estab-lishment and maintenance of the patient–pharmacist relationship.
Providing MTM Services in Various Patient Care Settings
Patients with a potential need for MTM services can be iden-tifi ed by the pharmacist, the physician or other healthcare professionals, the health plan, or the patients themselves when medication-related problems are suspected. Appendix B provides considerations for identifi cation of patients who may benefi t from MTM services. Patients may be especially vulnerable to medication-related problems during transitions of care* such as when their healthcare setting changes, when they change physicians, or when their payer status changes. These transitions of care often result in medication therapy changes that may be due to changes in the patient’s needs or resources, the patient’s health status or condition, or formulary requirements. It is important that systems be established so that pharmacist-provided MTM services can focus on reconciling the patient’s medications and ensuring the provision of appropriate medication management dur-ing transitions of care.
For ambulatory patients, MTM services typically are offered by appointment but may be provided on a walk-in basis. MTM services should be delivered in a private or semi-private area, as required by the Health Insurance Portability and Accountability Act, by a pharmacist whose time can be devoted to the patient during this service.21 In other patient care settings (e.g., acute care, long-term care, home care, managed care), the environment in which MTM services are delivered may differ because of variability in structure and facilities design. Even so, to the extent MTM core elements are implemented, a consistent approach to their delivery should be maintained.
The Delivery of MTM Services by the Pharmacist
Within the MTM core elements service model, the patient receives an annual comprehensive medication therapy review and additional medication therapy reviews accord-ing to the patient’s needs. The patient may require ongoing monitoring by the pharmacist to address new or recurring medication-related problems.
The total number of reviews required to successfully manage a patient’s therapy will vary from patient to patient and will be ultimately determined by the complexity of the individual patient’s medication-related problems. The extent of health plan benefi ts or other limitations imposed by the patient’s payer may affect coverage for MTM services; however, this would not preclude additional services provided by the phar-macist for which the patient pays on a fee-for-service basis.
To perform the most comprehensive assessment of a patient, personal interaction with direct contact between a healthcare professional and a patient is optimal. A face-to-face interaction optimizes the pharmacist’s ability to observe signs of and visual cues to the patient’s health problems (e.g., adverse reactions to medications, lethargy, alopecia, extrapyramidal symptoms, jaundice, disorientation) and can enhance the patient–pharmacist relationship.22 The pharmacist’s observations may result in early detection of medication-related problems and thus have the potential to reduce inappropriate medication use, emergency depart-ment visits, and hospitalizations. It is recognized, however, that alternative methods of patient contact and interaction such as telephonic may be necessary for those patients for whom a face-to-face interaction is not possible or not desired (e.g., homebound patients) or in pharmacy prac-tice settings in which the pharmacist serves in a consultative role on the healthcare team. Irrespective of whether the MTM service is provided by the pharmacist to the patient face-to-face or by alternative means, the service is intended to support the establishment and maintenance of the patient–pharmacist relationship.
* Examples of transitions of care may include but are not limited to changes in healthcare setting (e.g., hospital admission, hospital to home, hospital to long-term care facility, home to long-term care facility), changes in healthcare professionals and/or level of care (e.g., treatment by a specialist), or changes in payer status (e.g., change or loss of health plan benefi ts/insurance).

5
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Core Elements of an MTM Service Model in Pharmacy Practice The MTM service model in pharmacy practice includes the following fi ve core elements:
• Medication therapy review (MTR)• Personal medication record (PMR)• Medication-related action plan (MAP)• Intervention and/or referral • Documentation and follow-up
These fi ve core elements form a framework for the delivery of MTM services in pharmacy practice. Every core element is integral to the provision of MTM; however, the sequence and delivery of the core elements may be modifi ed to meet an individual patient’s needs.
An MTR is conducted between the patient and the pharmacist. Pharmacist-provided MTR and consultation in various settings has resulted in reductions in physician visits, emergency department visits, hospital days, and overall healthcare costs.9,10,12,14,20,23–25 In addition, pharmacists have been shown to obtain accurate and effi cient medication-related information from patients.10,26,27 The MTR is designed to improve patients’ knowledge of their medications, address problems or concerns that patients may have, and empower patients to self-manage their medications and their health condition(s).
The MTR can be comprehensive or targeted to an actual or potential medication-related problem. Regardless of wheth-er the MTR is comprehensive or targeted, patients may be identifi ed as requiring this service in a variety of ways. Commonly, patients may be referred to a pharmacist by their health plan, another pharmacist, physician, or other healthcare professionals. Patients may also request an MTR independent of any referral. Additional opportunities for providing an MTR include when a patient is experiencing
a transition of care, when actual or potential medication-related problems are identifi ed, or if the patient is suspected to be at higher risk for medication-related problems.
In a comprehensive MTR, ideally the patient presents all current medications to the pharmacist, including all prescription and nonprescription medications, herbal products, and other dietary supplements. The pharmacist then assesses the patient’s medications for the presence of any medication-related problems, including adherence, and works with the patient, the physician, or other healthcare professionals to determine appropriate options for resolving identifi ed problems. In addition, the pharmacist supplies the patient with education and information to improve the patient’s self-management of his or her medications.
Targeted MTRs are used to address an actual or potential medication-related problem. Ideally, targeted MTRs are performed for patients who have received a comprehensive MTR. Whether for a new problem or subsequent monitoring, the pharmacist assesses the specifi c therapy problem in the context of the patient’s complete medical and medication history. Following assessment, the pharmacist intervenes and provides education and information to the patient, the physician or other healthcare professionals, or both, as appropriate. The MTR is tailored to the individual needs of the patient at each encounter.
Depending on its scope, the MTR may include the following:
• Interviewing the patient to gather data including demographic information, general health and activity status, medical history, medication history, immunization history, and patients’ thoughts or feelings about their conditions and medication use28
• Assessing, on the basis of all relevant clinical information available to the pharmacist, the patient’s physical and overall health status, including current and previous diseases or conditions
• Assessing the patient’s values, preferences, quality of life, and goals of therapy
• Assessing cultural issues, education level, language barriers, literacy level, and other characteristics of the patient’s communication abilities that could affect outcomes
• Evaluating the patient to detect symptoms that could be attributed to adverse events caused by any of his or her current medications
• Interpreting, monitoring, and assessing patient’slaboratory results
Medication Therapy Review: The medication therapy review (MTR) is a systematic process of collecting patient-specifi c information, assessing medication therapies to identify medication-related problems, devel-oping a prioritized list of medication-related problems, and creating a plan to resolve them.

6
• Assessing, identifying, and prioritizing medication-related problems related to
» The clinical appropriateness of each medication being taken by the patient, including benefi t versus risk
» The appropriateness of the dose and dosing regimen of each medication, including consid-eration of indications, contraindications, potential adverse effects, and potential problems with concomitant medications
» Therapeutic duplication or other unnecessary medications
» Adherence to the therapy » Untreated diseases or conditions » Medication cost considerations » Healthcare/medication access considerations
• Developing a plan for resolving each medication-related problem identifi ed
• Providing education and training on the appropriate use of medications and monitoring devices and the importance of medication adherence and understanding treatment goals
• Coaching patients to be empowered to manage their medications
• Monitoring and evaluating the patient’s response to therapy, including safety and effectiveness
• Communicating appropriate information to the physician or other healthcare professionals, including consultation on the selection of medications, sug-gestions to address identifi ed medication problems, updates on the patient’s progress, and recommended follow-up care29
In this service model, a patient would receive an annual comprehensive MTR and additional targeted MTRs to address new or ongoing medication-related problem(s). Signifi cant events such as important changes in the patient’s medication therapy, changes in the patient’s needs or re-sources, changes in the patient’s health status or condition, a hospital admission or discharge, an emergency depart-ment visit, or an admission or discharge from a long-term care or assisted-living facility could necessitate additional comprehensive MTRs.

7
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Personal Medication Record: The personal medication record (PMR) is a comprehensive record of the patient’s medications (prescription and nonprescription medications, herbal products, and other dietary supplements).Within the MTM core elements service model, the patient receives a comprehensive record of his or her medica-tions (prescription and nonprescription medications, herbal products, and other dietary supplements) that has been completed either by the patient with the assistance of the pharmacist or by the pharmacist, or the patient’s existing PMR is updated. Ideally, the patient’s PMR would be gener-ated electronically, but it also may be produced manually. Whether the pharmacist provides the PMR manually or electronically, the information should be written at a literacy level that is appropriate for and easily understood by the patient. In institutional settings, the PMR may be created at discharge from the medication administration record or patient chart for use by the patient in the outpatient setting. The PMR contains information to assist the patient in his or her overall medication therapy self-management. A sample PMR is included in Appendix C.
The PMR, which is intended for use by the patient, may include the following information:30
• Patient name • Patient birth date • Patient phone number• Emergency contact information
(Name, relationship, phone number)• Primary care physician
(Name and phone number) • Pharmacy/pharmacist
(Name and phone number) • Allergies (e.g., What allergies do I have? What
happened when I had the allergy or reaction?)• Other medication-related problems (e.g., What
medication caused the problem? What was the problem I had?)
• Potential questions for patients to ask about their medications (e.g., When you are prescribed a new drug, ask your doctor or pharmacist...)
• Date last updated
• Date last reviewed by the pharmacist, physician, or other healthcare professional
• Patient’s signature • Healthcare provider’s signature• For each medication, inclusion of the following:
» Medication (e.g., drug name and dose) » Indication (e.g., Take for…) » Instructions for use (e.g., When do I take it?) » Start date » Stop date » Ordering prescriber/contact information
(e.g., doctor) » Special instructions
The PMR is intended for patients to use in medication self-management. The maintenance of the PMR is a col-laborative effort among the patient, pharmacist, physician, and other healthcare professionals. Patients should be encouraged to maintain and update this perpetual docu-ment. Patients should be educated to carry the PMR with them at all times and share it at all healthcare visits and at all admissions to or discharges from institutional settings to help ensure that all healthcare professionals are aware of their current medication regimen.
Each time the patient receives a new medication; has a current medication discontinued; has an instruction change; begins using a new prescription or nonprescription medi-cation, herbal product, or other dietary supplement; or has any other changes to the medication regimen, the patient should update the PMR to help ensure a current and accurate record. Ideally, the pharmacist, physician, and other healthcare professionals can actively assist the patient with the PMR revision process.
Pharmacists may use the PMR to communicate and collabo-rate with physicians and other healthcare professionals to achieve optimal patient outcomes. Widespread use of the PMR will support uniformity of information provided to all healthcare professionals and enhance the continuity of care provided to patients while facilitating fl exibility to account for pharmacy- or institution-specifi c variations.

8
Medication-Related Action Plan: The medication-related action plan (MAP) is a patient-centric document containing a list of actions for the patient to use in tracking progress for self-management. A care plan is the health professional’s course of action for helping a patient achieve specifi c health goals.31 The care plan is an important component of the documentation core element outlined in this service model. In addition to the care plan, which is developed by the pharmacist and used in the collaborative care of the patient, the patient receives an individualized MAP for use in medication self-management. Completion of the MAP is a collaborative effort between the patient and the pharmacist. The patient MAP includes only items that the patient can act on that are within the pharmacist’s scope of practice or that have been agreed to by relevant members of the healthcare team. The MAP should not include outstanding action items that still require physician or other healthcare professional review or approval. The patient can use the MAP as a simple guide to track his or her progress. The Institute of Medicine has advocated the need for a patient-centered model of healthcare.7 The patient MAP, coupled with education, is an essential element for incorporating the patient-centered ap-proach into the MTM service model. The MAP reinforces a sense of patient empowerment and encourages the patient’s
active participation in his or her medication-adherence behavior and overall MTM. A sample MAP is included in Appendix D.
The MAP, which is intended for use by the patient, may include the following information:
• Patient name• Primary care physician
(Doctor’s name and phone number)• Pharmacy/pharmacist
(Pharmacy name/pharmacist name and phone number)
• Date of MAP creation (Date prepared)• Action steps for the patient: “What I need to do...”• Notes for the patient: ”What I did and when I did it...”• Appointment information for follow-up with
pharmacist, if applicableSpecifi c items that require intervention and that have been approved by other members of the healthcare team and any new items within the pharmacist’s scope of practice should be included on a MAP distributed to the patient on a follow-up visit. In institutional settings the MAP could be established at the time the patient is discharged for use by the patient in medication self-management.

9
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Intervention and/or Referral: The pharma-cist provides consultative services and intervenes to address medication-related problems; when necessary, the pharmacist refers the patient to a physician or other healthcare professional. During the course of an MTM encounter, medication-related problems may be identifi ed that require the pharmacist to intervene on the patient’s behalf. Interventions may include collaborating with physicians or other healthcare profes-sionals to resolve existing or potential medication-related problems or working with the patient directly. The com-munication of appropriate information to the physician or other healthcare professional, including consultation on the selection of medications, suggestions to address medication problems, and recommended follow-up care, is integral to the intervention component of the MTM service model.29
The positive impact of pharmacist interventions on outcomes related to medication-related problems has been demon-strated in numerous studies.32–37 Appropriate resolution of medication-related problems involves collaboration and communication between the patient, the pharmacist, and the patient’s physician or other healthcare professionals.
Some patients’ medical conditions or medication therapy may be highly specialized or complex and the patient’s needs may extend beyond the core elements of MTM service delivery. In such cases, pharmacists may provide additional services according to their expertise or refer the patient to a physician, another pharmacist, or other healthcare professional.
Examples of circumstances that may require referral include the following:
• A patient may exhibit potential problems discovered during the MTR that may necessitate referral for evalu-ation and diagnosis
• A patient may require disease management education to help him or her manage chronic diseases such as diabetes
• A patient may require monitoring for high-risk medications (e.g., warfarin, phenytoin, methotrexate)
The intent of intervention and/or referral is to optimize medication use, enhance continuity of care, and encourage patients to avail themselves of healthcare services to prevent future adverse outcomes.
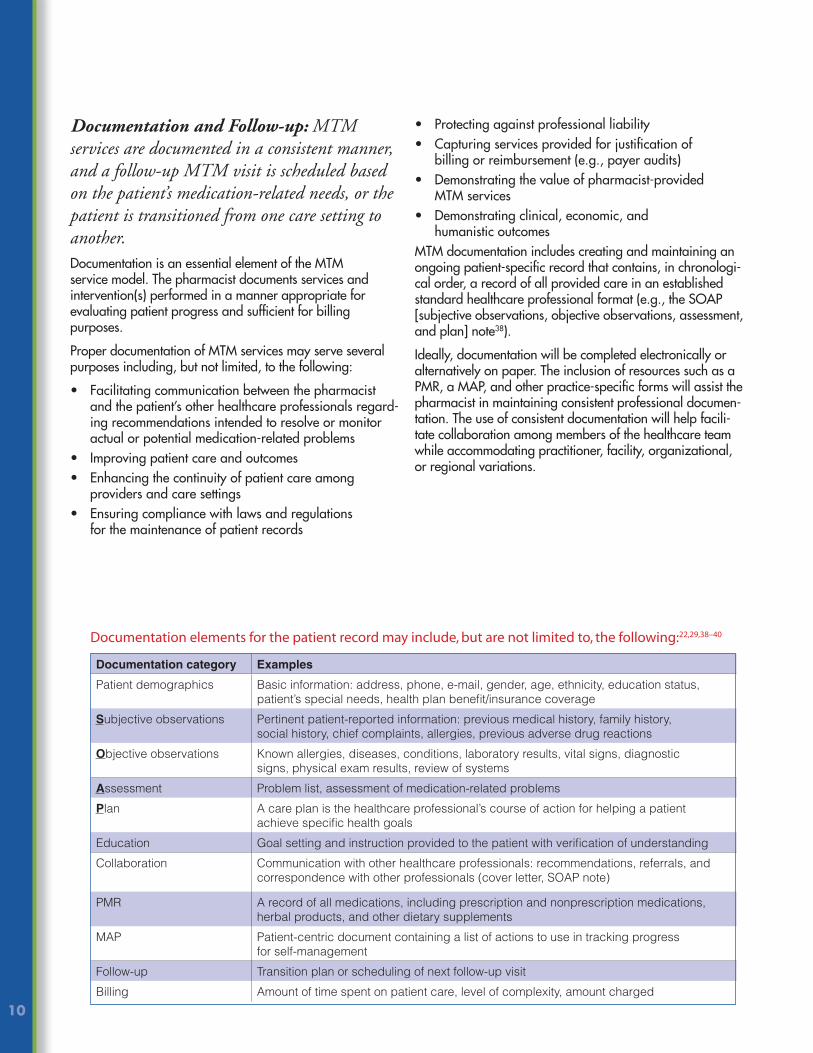
10
Documentation and Follow-up: MTM services are documented in a consistent manner, and a follow-up MTM visit is scheduled based on the patient’s medication-related needs, or the patient is transitioned from one care setting to another.Documentation is an essential element of the MTM service model. The pharmacist documents services and intervention(s) performed in a manner appropriate for evaluating patient progress and suffi cient for billing purposes.
Proper documentation of MTM services may serve several purposes including, but not limited, to the following:
• Facilitating communication between the pharmacist and the patient’s other healthcare professionals regard-ing recommendations intended to resolve or monitor actual or potential medication-related problems
• Improving patient care and outcomes• Enhancing the continuity of patient care among
providers and care settings• Ensuring compliance with laws and regulations
for the maintenance of patient records
• Protecting against professional liability • Capturing services provided for justifi cation of
billing or reimbursement (e.g., payer audits)• Demonstrating the value of pharmacist-provided
MTM services • Demonstrating clinical, economic, and
humanistic outcomesMTM documentation includes creating and maintaining an ongoing patient-specifi c record that contains, in chronologi-cal order, a record of all provided care in an established standard healthcare professional format (e.g., the SOAP [subjective observations, objective observations, assessment, and plan] note38).
Ideally, documentation will be completed electronically or alternatively on paper. The inclusion of resources such as a PMR, a MAP, and other practice-specifi c forms will assist the pharmacist in maintaining consistent professional documen-tation. The use of consistent documentation will help facili-tate collaboration among members of the healthcare team while accommodating practitioner, facility, organizational, or regional variations.
Documentation category Examples
Patient demographics Basic information: address, phone, e-mail, gender, age, ethnicity, education status, patient’s special needs, health plan benefi t/insurance coverage
Subjective observations Pertinent patient-reported information: previous medical history, family history, social history, chief complaints, allergies, previous adverse drug reactions
Objective observations Known allergies, diseases, conditions, laboratory results, vital signs, diagnostic signs, physical exam results, review of systems
Assessment Problem list, assessment of medication-related problems
Plan A care plan is the healthcare professional’s course of action for helping a patient achieve specifi c health goals
Education Goal setting and instruction provided to the patient with verifi cation of understanding
Collaboration Communication with other healthcare professionals: recommendations, referrals, and correspondence with other professionals (cover letter, SOAP note)
PMR A record of all medications, including prescription and nonprescription medications, herbal products, and other dietary supplements
MAP Patient-centric document containing a list of actions to use in tracking progress for self-management
Follow-up Transition plan or scheduling of next follow-up visit
Billing Amount of time spent on patient care, level of complexity, amount charged
Documentation elements for the patient record may include, but are not limited to, the following:22,29,38–40

11
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
External Communication of MTM Documentation
Following documentation of the MTM encounter, appropri-ate external communication should be provided or sent to key audiences, including patients, physicians, and payers. Providing the patient with applicable documentation that he or she can easily understand is vital to facilitating active involvement in the care process. Documentation provided to the patient at the MTM encounter may include the PMR, MAP, and additional education materials. Documentation to physicians and other healthcare professionals may include a cover letter, the patient’s PMR, the SOAP note, and care plan. Communicating with payers and providing appropri-ate billing information may also be necessary and could include the name of the pharmacist or pharmacy and appropriate identifi er, services provided, time spent on patient care, and appropriate billing codes.
Follow-up
When a patient’s care setting changes (e.g., hospital admis-sion, hospital to home, hospital to long-term care facility, home to long-term care facility), the pharmacist transi-tions the patient to another pharmacist in the patient’s new care setting to facilitate continued MTM services. In these situations, the initial pharmacist providing MTM services participates cooperatively with the patient’s new pharmacist provider to facilitate the coordinated transition of the patient, including the transfer of relevant medication and other health-related information.
If the patient will be remaining in the same care setting, the pharmacist should arrange for consistent follow-up MTM services in accordance with the patient’s unique medication-related needs. All follow-up evaluations and interactions with the patient and his or her other healthcare professional(s) should be included in MTM documentation.
ConclusionThe MTM core elements, as presented in this document, are intended to be applicable to patients in all care set-tings where the patients or their caregivers can be actively involved with managing their medication therapy, taking full advantage of the pharmacist’s role as the “medication ther-apy expert.”A fl ow chart of the core elements of an MTM service model contained in this document can be found in Appendix E. As the core elements service model continues to evolve to meet diverse patient needs, pharmacists are encouraged to make the most of the framework provided to improve patient outcomes and medication use.

12
References1. American Pharmacists Association, National Association of Chain Drug
Stores Foundation. Medication therapy management in community phar-macy practice: core elements of an MTM service (version 1.0). J Am Pharm Assoc. 2005;45:573-9.
2. Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice. 1998;1(1):2-4.
3. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: Institute of Medicine; 2001.
4. Cipolle RJ. Strand LM, Morley PC. Pharmaceutical Care Practice: The Clinician’s Guide. New York: McGraw Hill; 2004.
5. McGivney MS, Meyer SM, Duncan-Hewitt W, et al. Medication therapy management: its relationship to patient counseling, disease management, and pharmaceutical care. J Am Pharm Assoc. 2007;45:620-8.
6. Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: updating the cost-of-illness model. J Am Pharm Assoc. 2001;41:192-9.
7. Institute of Medicine. Report Brief: Preventing Medication Errors. Washington, DC: Institute of Medicine; July 2006. http://www.iom.edu/Object.File/Master/35/943/medication%20errors%20new.pdf. Accessed September 1, 2007.
8. Centers for Medicare & Medicaid Services. Medicare Prescription Drug Benefi t Final Rule: 42 CFR Parts 400, 403, 411, 417, and 423 Medicare Program. Federal Register, vol. 70, no. 18. January 28, 2005. http://a257.g.akamaitech.net/7/257/2422/01jan20051800/edocket.access.gpo.gov/2005/pdf/05-1321.pdf. Accessed September 1, 2007.
9. Garrett D, Bluml B. Patient self-management program for diabetes: fi rst-year clinical, humanistic, and economic outcomes. J Am Pharm Assoc. 2005;45:130-7.
10. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc. 2003;43:173-90.
11. Chrischilles EA, Carter BL, Lund BC, et al. Evaluation of the Iowa Medicaid pharmaceutical case management program. J Am Pharm Assoc. 2004;44:337-49.
12. Bunting BA, Cranor CW. The Asheville Project: long-term clinical, humanis-tic, and economic outcomes of a community-based medication therapy management program for asthma. J Am Pharm Assoc. 2003;46:133-47.
13. Jameson J, VanNoord G, Vanderwould K. The impact of a pharmacotherapy consultation on the cost and outcome of medical therapy. J Fam Pract. 1995;41(5):469-72.
14. Lipton HL, Bero LA, Bird JA, et al. The impact of clinical pharmacists’ consultations on physicians’ geriatric drug prescribing. Med Care. 1992;30:646-58.
15. Schumock GT, Butler MG, Meek PD, et al. Evidence of the economic benefi t of clinical pharmacy services: 1996–2000. Pharmacotherapy. 2003;23:113-132.
16. Minnesota Department of Human Services. MHCP enrolled professionals: medication therapy management services. http://www.dhs.state.mn.us/main/idcplg?IdcService=GET_DYNAMIC_CONVERSION&RevisionSelectionMethod=LatestReleased&dDocName=id_055325#P116_7762. Accessed February 5, 2007.
17. Traynor K. Wyoming program brings pharmacist consultations home. Am J Health Syst Pharm. 2004;61:760.
18. North Carolina Department of Health and Human Services. North Carolina Medicaid: Medication Therapy Management Program (MTMP). August 2006. http://www.dhhs.state.nc.us/dma/Forms/mtmpinstructions.pdf. Accessed September 1, 2007.
19. Touchette DR, Burns AL, Bough MA, et al. Survey of medication therapy management programs under Medicare part D. J Am Pharm Assoc. 2006;46:683-91.
20. Galt KA. Cost avoidance, acceptance, and outcomes associated with a pharmacotherapy consult clinic in a Veterans Affairs medical center. Phar-macotherapy. 1998;18:1103-11.
21. Rovers J, Currie J, Hagel H, et al. Re-engineering the pharmacy layout. In: A Practical Guide to Pharmaceutical Care. 2nd ed. Washington, DC: American Pharmacists Association; 2003:261-6.
22. Rovers J, Currie J, Hagel H, et al. Patient data collection. In: A Practical Guide to Pharmaceutical Care. 2nd ed. Washington, DC: American Phar-macists Association; 2003:26-51.
23. Borgsdorf LR, Miano JS, Knapp KK. Pharmacist-managed medication review in a managed care system. Am J Hosp Pharm. 1994;51:772-7.
24. Bond CA, Raehl CL, Franke T. Clinical pharmacy services, pharmacy staffi ng, and the total cost of care in the United States hospitals. Pharmacotherapy. 2000;20:609-21.
25. Christensen D, Trygstad T, Sullivan R, et al. A pharmacy management intervention for optimizing drug therapy for nursing home patients. Am J Geriatr Pharmacother. 2004;2:248-56.
26. Gurwich EL. Comparison of medication histories acquired by pharmacists and physicians. Am J Hosp Pharm. 1983;40:1541-2.
27. Nester TM, Hale LS. Effectiveness of a pharmacist-acquired medication his-tory in promoting patient safety. Am J Health Syst Pharm. 2003;3-14.
28. Rovers J, Currie J, Hagel H, et al. The case for pharmaceutical care. In: A Practical Guide to Pharmaceutical Care. 2nd ed. Washington, DC: Ameri-can Pharmacists Association, 2003:3-4.
29. Berger BA. Interacting with physicians. In: Communication Skills for Pharmacists. 2nd ed. Washington, DC: American Pharmacists Association; 2005:131-9.
30. Executive summary of the American Society of Health System Pharmacists (ASHP) and ASHP Research and Education Foundation Continuity of Care in Medication Use Summit. Am J Health Syst Pharm. In press.
31. Rovers J, Currie J, Hagel H, et al. Patient care plan development. In: A Prac-tical Guide to Pharmaceutical Care. 2nd ed. Washington, DC: American Pharmacists Association, 2003:69.
32. Rupp MT. Value of the community pharmacists’ interventions to correct prescribing errors. Ann Pharmacother. 1992;26:1580-4.
33. McMullin ST, Hennenfent JA, Ritchie D, et al. A prospective randomized trial to assess the cost impact of pharmacist-initiated interven-tions. Arch Intern Med. 1999;159:2306-9.
34. Knapp KK, Katzman H, Hambright JS, et al. Community pharmacist inter-vention in a capitated pharmacy benefi t contract. Am J Health Syst Pharm. 1998;55:1141-5.
35. Dobie RL, Rascati KL. Documenting the value of pharmacist interventions. Am Pharm. 1994;NS34(5):50-4.
36. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47:533-43.
37. Bootman JL, Harrison DL, Cox E. The healthcare cost of drug-related morbidity and mortality in nursing facilities. Arch Intern Med. 1997;157:2089-96.
38. Zierler-Brown S, Brown TR, Chen D, et al. Clinical documentation for patient care: models, concepts, and liability considerations for pharma-cists. Am J Health Syst Pharm. 2007;64:1851-8.
39. Currie JD, Doucette WR, Kuhle J, et al. Identifi cation of essential elements in documentation of pharmacist-provided care. J Am Pharm Assoc. 2003;43:41-9.
40. Culhane N, Brooks A, Cohen V, et al. Medication therapy management services: Application of the core elements in ambulatory settings. American College of Clinical Pharmacy. March 14, 2007.

13
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Medication Therapy Management is a distinct service or group of services that optimize therapeutic outcomes for in-dividual patients. Medication Therapy Management services are independent of, but can occur in conjunction with, the provision of a medication product.
Medication Therapy Management encompasses a broad range of professional activities and responsibilities within the licensed pharmacist’s, or other qualifi ed healthcare provider’s, scope of practice. These services include but are not limited to the following, according to the individual needs of the patient:
a. Performing or obtaining necessary assessments of the patient’s health status
b. Formulating a medication treatment planc. Selecting, initiating, modifying, or administering
medication therapyd. Monitoring and evaluating the patient’s response to
therapy, including safety and effectivenesse. Performing a comprehensive medication review to
identify, resolve, and prevent medication-related prob-lems, including adverse drug events
f. Documenting the care delivered and communicating essential information to the patient’s other primary care providers
g. Providing verbal education and training designed to enhance patient understanding and appropriate use of his/her medications
h. Providing information, support services, and resources designed to enhance patient adherence with his/her therapeutic regimens
i. Coordinating and integrating medication therapy management services within the broader healthcare management services being provided to the patient
A program that provides coverage for Medication Therapy Management services shall include:
a. Patient-specifi c and individualized services or sets of services provided directly by a pharmacist to the patient.* These services are distinct from formulary de-velopment and use, generalized patient education and information activities, and other population-focused quality-assurance measures for medication use
b. Face-to-face interaction between the patient* and the pharmacist as the preferred method of delivery. When patient-specifi c barriers to face-to-face communication exist, patients shall have equal access to appropri-ate alternative delivery methods. Medication Therapy Management programs shall include structures sup-porting the establishment and maintenance of the patient*–pharmacist relationship
c. Opportunities for pharmacists and other qualifi ed healthcare providers to identify patients who should receive medication therapy management services
d. Payment for medication therapy management ser-vices consistent with contemporary provider payment rates that are based on the time, clinical intensity, and resources required to provide services (e.g., Medicare Part A and/or Part B for CPT and RBRVS)
e. Processes to improve continuity of care, outcomes, and outcome measures
Approved July 27, 2004, by the Academy of Managed Care Pharmacy, the American Association of Colleges of Pharmacy, the American College of Apothecaries, the American College of Clinical Pharmacy, the American So-ciety of Consultant Pharmacists, the American Pharmacists Association, the American Society of Health-System Phar-macists, the National Association of Boards of Pharmacy,** the National Association of Chain Drug Stores, the National Community Pharmacists Association, and the National Council of State Pharmacy Association Executives.
Appendix A. Defi nition of Medication Therapy Management (MTM)�
* In some situations, medication therapy management services may be provided to the caregiver or other persons involved in the care of the patient.
** Organization policy does not allow NABP to take a position on payment issues.
� Bluml BM. Defi nition of medication therapy management: development of profession wide consensus.J Am Pharm Assoc. 2005;45:566–72.

14
Appendix B. Considerations for Identifi cation of Patients Who May Benefi t From MTM Services Any patients using prescription and nonprescription medications, herbal products, and other dietary supple-ments could potentially benefi t from the medication therapy management (MTM) services described in the core elements outlined in this service model, especially if medication-related problems or issues are discovered or suspected. Patients may be evaluated for MTM services regardless of the number of medications they use, their specifi c disease state(s), or their health plan coverage.
Opportunities for the identifi cation of patients targeted for MTM services may result from many sources including, but not limited to, pharmacist identifi cation, physician referral, patient self-referral, and health plan or other payer referral. Pharmacists may wish to notify physicians or other health-care professionals in their community or physicians within their facility, if applicable, of their MTM services, so that physicians may refer patients for MTM services.
To provide assistance in prioritizing who may benefi t most from MTM services, pharmacists, health plans, physicians, other healthcare professionals, and health systems may consider using one or more of the following factors to target patients who are likely to benefi t most from MTM services:
• Patient has experienced a transition of care, and his or her regimen has changed
• Patient is receiving care from more than one prescriber• Patient is taking fi ve or more chronic medications
(including prescription and nonprescription medica-tions, herbal products, and other dietary supplements)
• Patient has at least one chronic disease or chronic health condition (e.g., heart failure, diabetes, hypertension, hyperlipidemia, asthma, osteoporosis, depression, osteoarthritis, chronic obstructive pulmonary disease)
• Patient has laboratory values outside the normal range that could be caused by or may be improved with medication therapy
• Patient has demonstrated nonadherence (including underuse and overuse) to a medication regimen
• Patient has limited health literacy or cultural differences, requiring special communication strategies to optimize care
• Patient wants or needs to reduce out-of-pocket medication costs
• Patient has experienced a loss or signifi cant change in health plan benefi t or insurance coverage
• Patient has recently experienced an adverse event (medication or non-medication-related) while receiving care
• Patient is taking high-risk medication(s), including narrow therapeutic index drugs (e.g., warfarin, phenytoin, methotrexate)
• Patient self-identifi es and presents with perceived need for MTM services
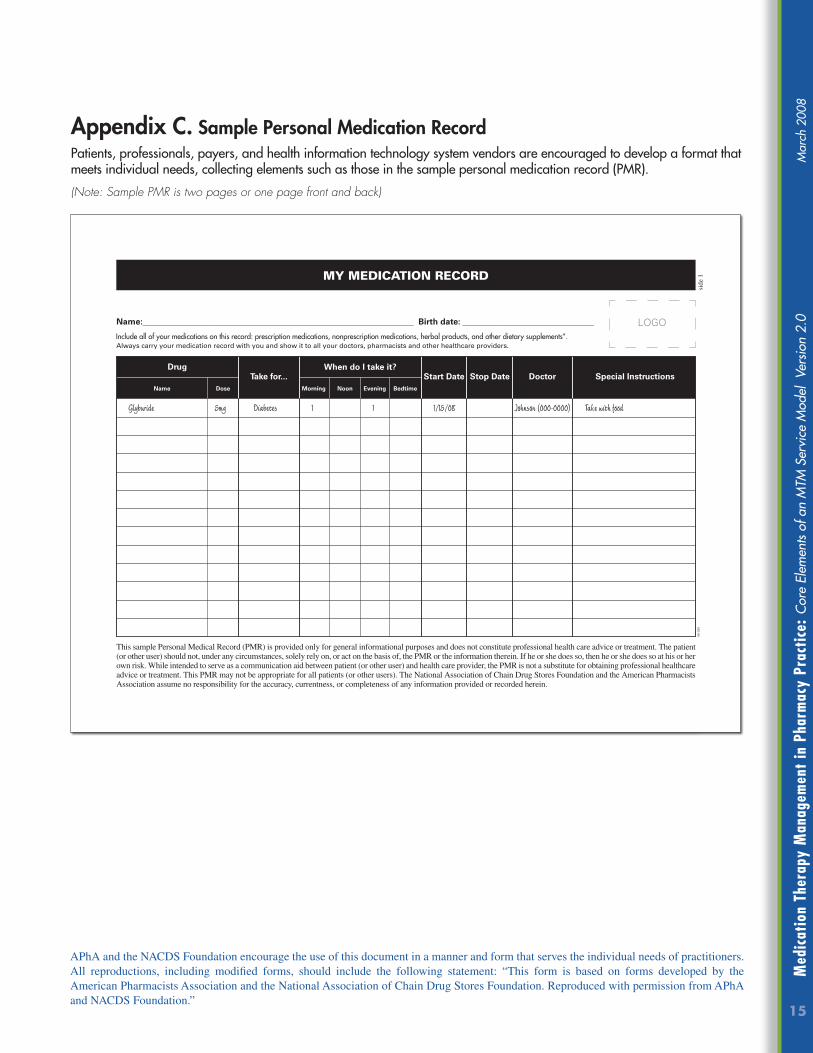
15
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Appendix C. Sample Personal Medication RecordPatients, professionals, payers, and health information technology system vendors are encouraged to develop a format that meets individual needs, collecting elements such as those in the sample personal medication record (PMR).
(Note: Sample PMR is two pages or one page front and back)
APhA and the NACDS Foundation encourage the use of this document in a manner and form that serves the individual needs of practitioners. All reproductions, including modifi ed forms, should include the following statement: “This form is based on forms developed by the American Pharmacists Association and the National Association of Chain Drug Stores Foundation. Reproduced with permission from APhA and NACDS Foundation.”
Glyburide 5mg Diabetes 1 1 1/15/08 Johnson (000-0000) Take with food
My Medication record
This sample Personal Medical Record (PMR) is provided only for general informational purposes and does not constitute professional health care advice or treatment. The patient (or other user) should not, under any circumstances, solely rely on, or act on the basis of, the PMR or the information therein. If he or she does so, then he or she does so at his or her own risk. While intended to serve as a communication aid between patient (or other user) and health care provider, the PMR is not a substitute for obtaining professional healthcare advice or treatment. This PMR may not be appropriate for all patients (or other users). The National Association of Chain Drug Stores Foundation and the American Pharmacists Association assume no responsibility for the accuracy, currentness, or completeness of any information provided or recorded herein.
DrugTake for... Start Date Stop Date Doctor Special Instructions
When do I take it?
Name Dose Morning Noon Evening Bedtime
Include all of your medications on this reord: prescription medications, nonprescription medications, herbal products, and other dietary supplements.Always carry your medication record with you and show it to all your doctors, pharmacists and other healthcare providers.
Name:________________________________________________________________ Birth date: _______________________________
08-0
29
LOGO
side
1
Include all of your medications on this record: prescription medications, nonprescription medications, herbal products, and other dietary supplements”.
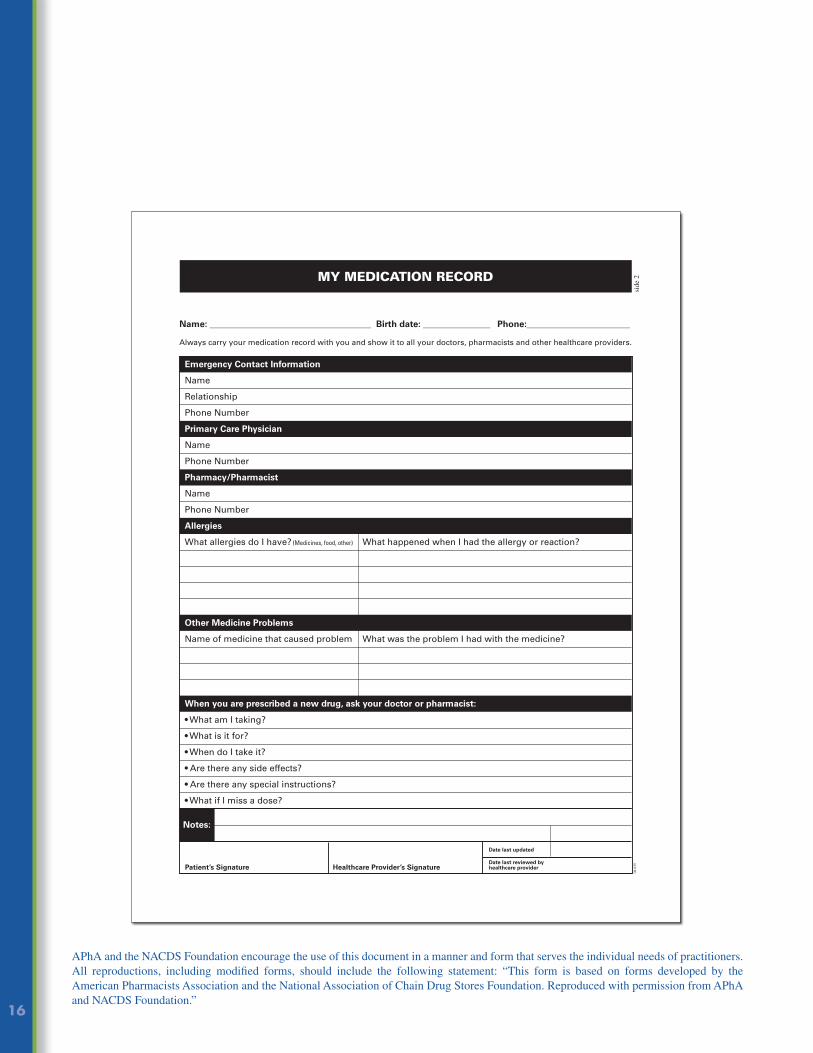
16
APhA and the NACDS Foundation encourage the use of this document in a manner and form that serves the individual needs of practitioners. All reproductions, including modifi ed forms, should include the following statement: “This form is based on forms developed by the American Pharmacists Association and the National Association of Chain Drug Stores Foundation. Reproduced with permission from APhA and NACDS Foundation.”
My Medication record
08-0
29
Emergency Contact Information
Name
Relationship
Phone Number
Primary Care Physician
Name
Phone Number
Pharmacy/Pharmacist
Name
Phone Number
Allergies
What allergies do I have? (Medicines, food, other) What happened when I had the allergy or reaction?
Other Medicine Problems
Name of medicine that caused problem What was the problem I had with the medicine?
When you are prescribed a new drug, ask your doctor or pharmacist:
• What am I taking?
• What is it for?
• When do I take it?
• Are there any side effects?
• Are there any special instructions?
• What if I miss a dose?
Notes:
Name: ____________________________________ Birth date: _______________ Phone:_______________________
Always carry your medication record with you and show it to all your doctors, pharmacists and other healthcare providers.
Patient’s Signature Healthcare Provider’s Signature
Date last updated
Date last reviewed by healthcare provider
side
2

17
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Appendix D. Sample Medication-Related Action Plan (for the Patient)Patients, healthcare professionals, payers, and health information technology system vendors are encouraged to develop a format that meets individual and customer needs, collecting elements such as those included on the sample medication-related action plan (MAP) below.
APhA and the NACDS Foundation encourage the use of this document in a manner and form that serves the individual needs of practitioners. All reproductions, including modifi ed forms, should include the following statement: “This form is based on forms developed by the American Pharmacists Association and the National Association of Chain Drug Stores Foundation. Reproduced with permission from APhA and NACDS Foundation.”
My Medication-related action Plan
Patient:
Doctor (Phone):
Pharmacy/Pharmacist (Phone):
Date Prepared:
The list below has important Action Steps to help you get the most from your medications. Follow the checklist to help you work with your pharmacist and doctor to manage your medications
AND make notes of your actions next to each item on your list.
Action Steps What I need to do… Notes What I did and when I did it…
My Next Appointment with My Pharmacist is on:__________________(date) at __________ AM PM
08-0
29
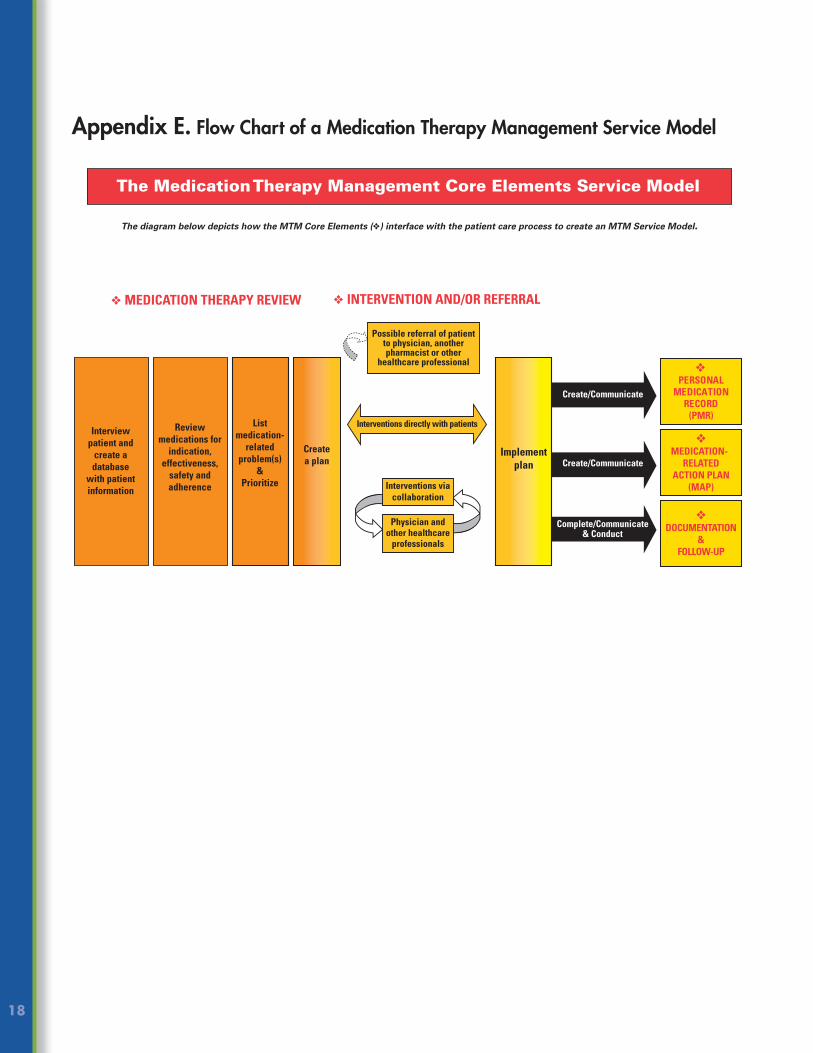
18
Appendix E. Flow Chart of a Medication Therapy Management Service Model

19
Med
icatio
n Th
erap
y M
anag
emen
t in
Pha
rmac
y Pr
actic
e: C
ore
Elem
ents
of a
n M
TM S
ervi
ce M
odel
Ver
sion
2.0
M
arch
200
8
Marialice S. Bennett, RPh, FAPhAThe Ohio State University
Rebecca W. Chater, RPh, MPH, FAPhAKerr Drug, Inc.
Kimberly Sasser Croley, PharmD, CGP, FASCPKnox County Hospital
Rachael Deck, PharmDWalgreen Co.
Jeffrey C. Delafuente, MS, FCCP, FASCP Virginia Commonwealth University School of Pharmacy
Susan L. Downard, RPh Kaiser Permanente of the Mid-Atlantic States, Inc
Margherita Giuliano, RPhConnecticut Pharmacists Association
Zandra Glenn, PharmDHRSA Pharmacy Services Support Center
Melinda C. Joyce, PharmD, FAPhA, FACHEThe Medical Center
Sandra Leal, PharmD, CDEEl Rio Community Health Center
Macary Weck Marciniak, PharmD, BCPSAlbany College of Pharmacy
Randy P. McDonough, PharmD, MS, CGP, BCPSTowncrest and Medical Plaza Pharmacies
Melissa Somma McGivney, PharmD, CDE University of Pittsburgh School of Pharmacy
Rick Mohall, PharmDRite Aid Corporation
Anthony Provenzano, PharmD, CDE SUPERVALU Pharmacies, Inc.
Michael Sherry, RPhCVS Caremark
Steven T. Simenson, RPh, FAPhAGoodrich Pharmacies
Donna S. Wall, RPh, PharmD, BCPS, FASHPClarian Healthcare Partners, Indiana University Hospital
Winston Wong, PharmD CareFirst BCBS
Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 advisory panel members provided expert advice. The content of this document does not necessarily represent all of their opinions or those of their affi liated organizations.
MTM Core Elements Service Model Version 2.0 Advisory Panel Members
AddendumMedication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model Version 2.0 was developed with the input of an advisory panel of pharmacy leaders representing diverse pharmacy practice settings. The pharmacy practice setting areas represented by members of the advisory panel included ambulatory care, community, government technical support services, hospital, long-term care, managed care health systems, managed care organization plan administration, and outpatient clinics.
Ben Bluml, RPhAmerican Pharmacists Association Foundation
Anne Burns, RPhAmerican Pharmacists Association
Ronna Hauser, PharmDNational Association of Chain Drug Stores
Crystal Lennartz, PharmD, MBA National Association of Chain Drug Stores
James Owen, PharmDAmerican Pharmacists Association
Afton Yurkon, PharmDNational Association of Chain Drug Stores
Staff
NOTES

Medication Therapy Management in Pharmacy Practice Core Elements of an MTM Service Model
Version 2.0
08-3
23
To request a single print copy of the publication, click on the following link:http://fs6.formsite.com/APhA-NACDS/print_request/index.html
To provide comments and/or feedback on this publication, click on the following link: http://fs6.formsite.com/APhA-NACDS/core_elements_feedback/index.html
To obtain a copy of a slide presentation explaining the MTM Core Elements Service Model or to submit a request for a presentation to your organization or group, click on the following link: http://fs6.formsite.com/APhA-NACDS/presentation_request/index.html