multiplex genetic test in liver detoxification function for predicting liver disease progression ran...
TRANSCRIPT
Multiplex Genetic Test in Liver Multiplex Genetic Test in Liver Detoxification Function for Detoxification Function for Predicting Liver Disease Predicting Liver Disease
ProgressionProgression
Ran Oren, Hava Peretz, Sigal Fishman, Guy Rosner, Zamir Halpern




Liver Biopsy
• Is the gold standard for the diagnosis
• Who should we biopsy?
• When should we biopsy?
• Can we biopsy everybody?




L'appareil
Probe3.5 MHz
Specific electronic equipmentUltrasound acquisition chipDigital signal processing
Integrated computerPatient data base

The examination
• The examination can be made following the ultrasound scan, with, the patient lying down in the same position
• The time needed for examination is less than 5 minutes.
• The examination can be carried out by qualified hospital staff other than doctors : nurses, technicians


ObjectiveObjective• Up to 33% of Hepatitis C Patients Up to 33% of Hepatitis C Patients
progress to cirrhosis in less than 20yprogress to cirrhosis in less than 20y
• It is of great importance to find It is of great importance to find reliable predicting markers of reliable predicting markers of cirrhosis progressioncirrhosis progression
• Previous studies have shown an Previous studies have shown an association between CYP2D6 association between CYP2D6 polymorphism and liver cirrhosispolymorphism and liver cirrhosis

BackgroundBackground• The human cytochrome P450 (CYP) superfamily The human cytochrome P450 (CYP) superfamily
comprises 57 genescomprises 57 genes
• These code for enzymes having role in drug These code for enzymes having role in drug metabolism, foreign chemicals, arachidonic acid, metabolism, foreign chemicals, arachidonic acid, cholesterol metabolism, generation of ROS in the cholesterol metabolism, generation of ROS in the liver, etc.liver, etc.
• Studies have shown that a number of gene Studies have shown that a number of gene polymorphisms influence the progression of polymorphisms influence the progression of fibrosis in patients with various liver diseasesfibrosis in patients with various liver diseases– Alcoholic liver disease : CYP2E1Alcoholic liver disease : CYP2E1– NASH : HFENASH : HFE
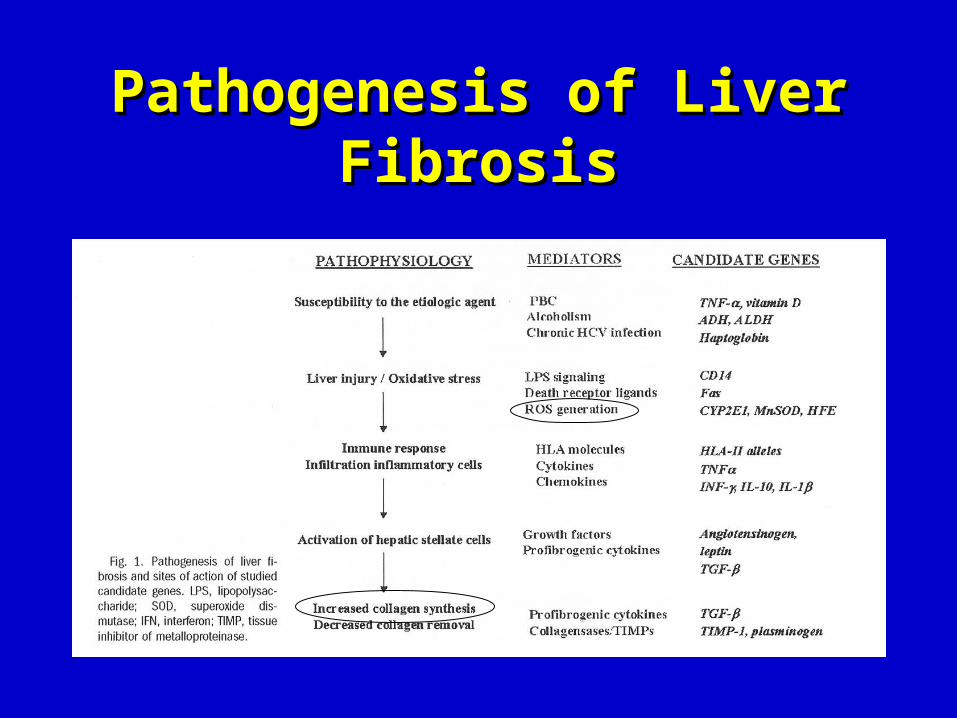
Pathogenesis of Liver Pathogenesis of Liver FibrosisFibrosis
Role of CYP in liver fibrosis - Role of CYP in liver fibrosis - HypothesisHypothesis
• Hepatic cyctochrome P450 generates ROS -> Hepatic cyctochrome P450 generates ROS -> activation of HSCs-> -> Fibrosisactivation of HSCs-> -> Fibrosis
• Arachidonic AcidArachidonic Acid
Collagen type 1Collagen type 1
CYP2 familyCYP2 family
degradation

ObjectiveObjective
• CYP2D6*4 is the most common CYP2D6*4 is the most common ‘poor metabolizer’ variant‘poor metabolizer’ variant
• Prevalence in the Caucasian Prevalence in the Caucasian population - 23%population - 23%

AimAim
The aim of the study was to The aim of the study was to
elucidate the impact of CYP2D4*6 on elucidate the impact of CYP2D4*6 on
fibrosis progression ratefibrosis progression rate
Patients and methodsPatients and methods
• 75 Caucasians patients with chronic 75 Caucasians patients with chronic hepatitis Chepatitis C
• Other liver diseases were excludedOther liver diseases were excluded
• Blood of twenty healthy Caucasian Blood of twenty healthy Caucasian neonates served as controlneonates served as control
Patients and methodsPatients and methods
Histopathology:Histopathology:
Stage and grade were assessed Stage and grade were assessed according to the Batts and according to the Batts and
Ludwing systemLudwing system

Patients and methodsPatients and methods
Definition of “fast”Definition of “fast” and “slow” fibrosers and “slow” fibrosers
Poynard’s fibrosis progression model basedPoynard’s fibrosis progression model based
on age of exposure and duration of on age of exposure and duration of
InfectionInfection
J Hepatol. 2001 May;34(5):730-9J Hepatol. 2001 May;34(5):730-9

Adapted from Poynard T et al. J Hepatol. 2001;34:730-739.
Probability of Fibrosis Progression to F4 According to Age at Infection
0 10 20 30 400.00
0.25
0.50
0.75
1.00 >50
41–5031–40
21–30
<21
Duration of Infection (y)
Pro
bab
ilit
y
Patients and methodsPatients and methods
• Infection in age of less than 20 y- cirrhosis after 40yInfection in age of less than 20 y- cirrhosis after 40y
• Infection in 3Infection in 3rdrd and 4 and 4th th decades – cirrhosis after 30y decades – cirrhosis after 30y
• Infection in 5Infection in 5th th decade – cirrhosis after 20y decade – cirrhosis after 20y
• Infection after the age of 50y- cirrhosis after 15 yearsInfection after the age of 50y- cirrhosis after 15 years
Patients and methodsPatients and methodsNon biopsied patients:Non biopsied patients:• Clinical diagnosis of cirrhosis (signs Clinical diagnosis of cirrhosis (signs
&imaging)&imaging)
Patients with no date of exposure :Patients with no date of exposure :• Cirrhotic young patients - not expected to Cirrhotic young patients - not expected to
reach cirrhosis by the modelreach cirrhosis by the model

Patients and methodsPatients and methods
CYP2D6 assay:CYP2D6 assay:• Genomic DNA was extracted from peripheral Genomic DNA was extracted from peripheral
blood by a salting-out procedure.blood by a salting-out procedure.
• Cytochrome P450-2D6*4 mutation was detected Cytochrome P450-2D6*4 mutation was detected by real time PCR method, using Fluorecent by real time PCR method, using Fluorecent hybridization probes in the lightCycler instrument hybridization probes in the lightCycler instrument

Demographic and clinical Demographic and clinical characteristics of the two groupscharacteristics of the two groups
Fast Fast fibrosers fibrosers (42)(42)
Slow Slow fibrosers fibrosers (33)(33)
PP-value-value
MaleMale(%) (%) 2626) ) 61.961.9((1919) ) 57.657.6((0.710.71Mean Age(SD)Mean Age(SD)4343) ) 9.49.4((5757) ) 16.816.8((<<0.00010.0001Mean age of Mean age of exposure(SD)exposure(SD)
24.624.6) ) 11.311.3((23.923.9) ) 11.311.3((0.790.79
Mean duration of Mean duration of infection:years infection:years (SD)(SD)
1818) ) 7.97.9((36.436.4) ) 12.412.4((<<0.00010.0001
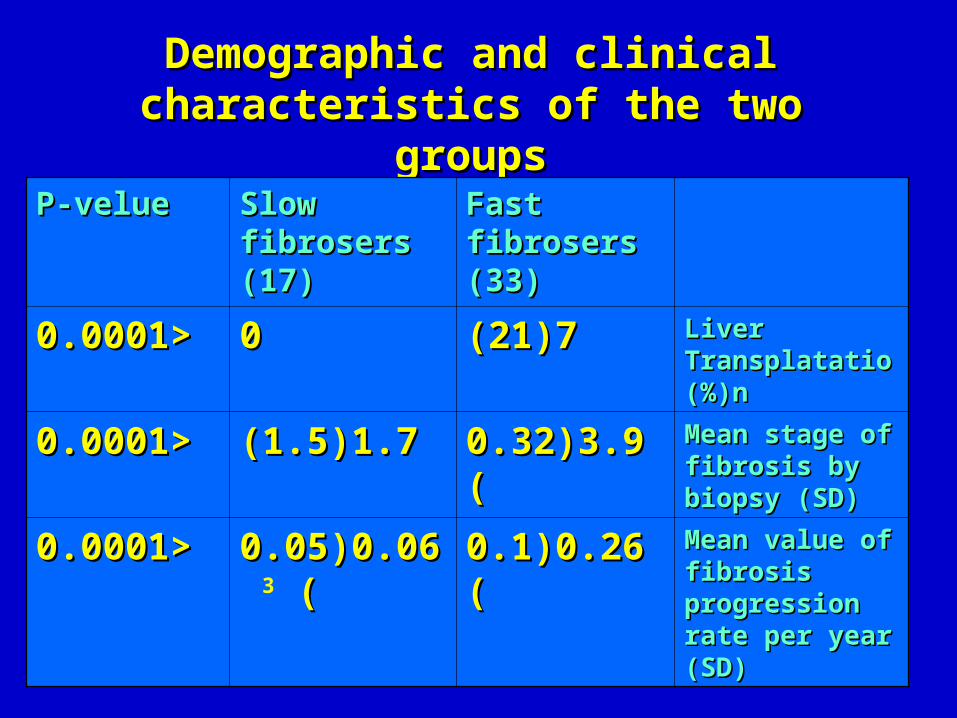
Demographic and clinical Demographic and clinical characteristics of the two groupscharacteristics of the two groups
Fast fibrosers Fast fibrosers (33)(33)
Slow fibrosers Slow fibrosers (17)(17)
P-velueP-velue
Liver Liver TransplatationTransplatation%)%)
((
77))2121((00<<0.00010.0001
Mean stage of Mean stage of fibrosis by biopsy fibrosis by biopsy (SD)(SD)
3.93.9))0.320.32((1.71.7))1.51.5((<<0.00010.0001
Mean value of Mean value of fibrosis fibrosis progression rate progression rate per year (SD)per year (SD)
0.260.26))0.10.1((0.060.06))0.050.05 ( (3 <<0.00010.0001
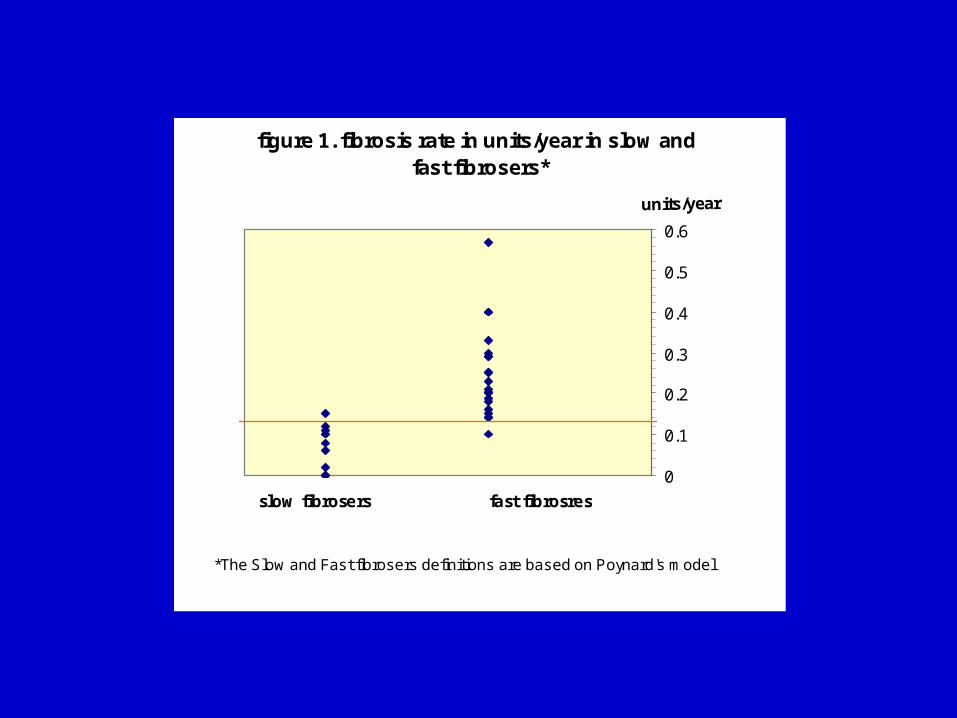
figure 1. fibrosis rate in units/year in slow and fast fibrosers*
0
0.1
0.2
0.3
0.4
0.5
0.6
slow fibrosers fast fibrosres
units/year
*The Slow and Fast fibrosers definitions are based on Poynard's model
0.13
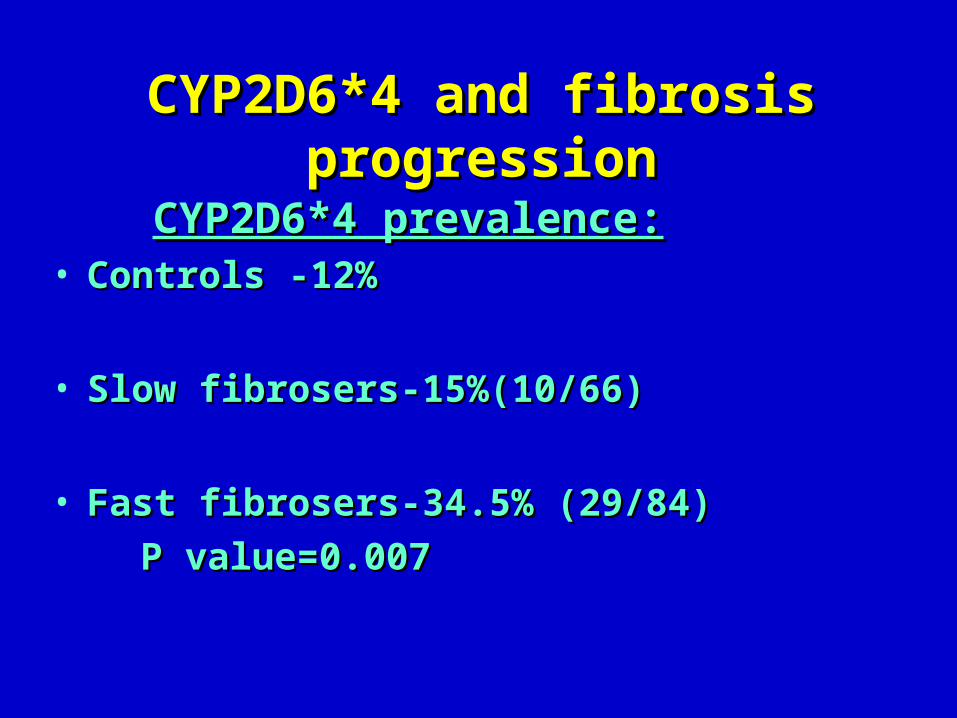
CYP2D6*4 and fibrosis progressionCYP2D6*4 and fibrosis progression
CYP2D6*4 prevalence:CYP2D6*4 prevalence:• Controls -12%Controls -12%
• Slow fibrosers-15%(10/66)Slow fibrosers-15%(10/66)
• Fast fibrosers-34.5% (29/84) Fast fibrosers-34.5% (29/84)
P value=0.007P value=0.007

The prevalence of homozygotes , heterozygotes The prevalence of homozygotes , heterozygotes and carriers in the ‘fast’ and ‘slow’ fibrosersand carriers in the ‘fast’ and ‘slow’ fibrosers
CYP2D6*4 CYP2D6*4 carrier statuscarrier status
Fast fibrosersFast fibrosersSlow fibrosersSlow fibrosers
Homozygote (%)Homozygote (%)117(16.7)7(16.7)1(3.0)1(3.0)
Heterozygote (%)Heterozygote (%)15(35.7)15(35.7)8(24.2)8(24.2)
Homozygote or Homozygote or heterozygote (%)heterozygote (%)
22(52.4)22(52.4)9(27.3)9(27.3)11
None (%)None (%)20(47.6)20(47.6)24(72.7)24(72.7)
11P-valueP-value = 0.06= 0.06
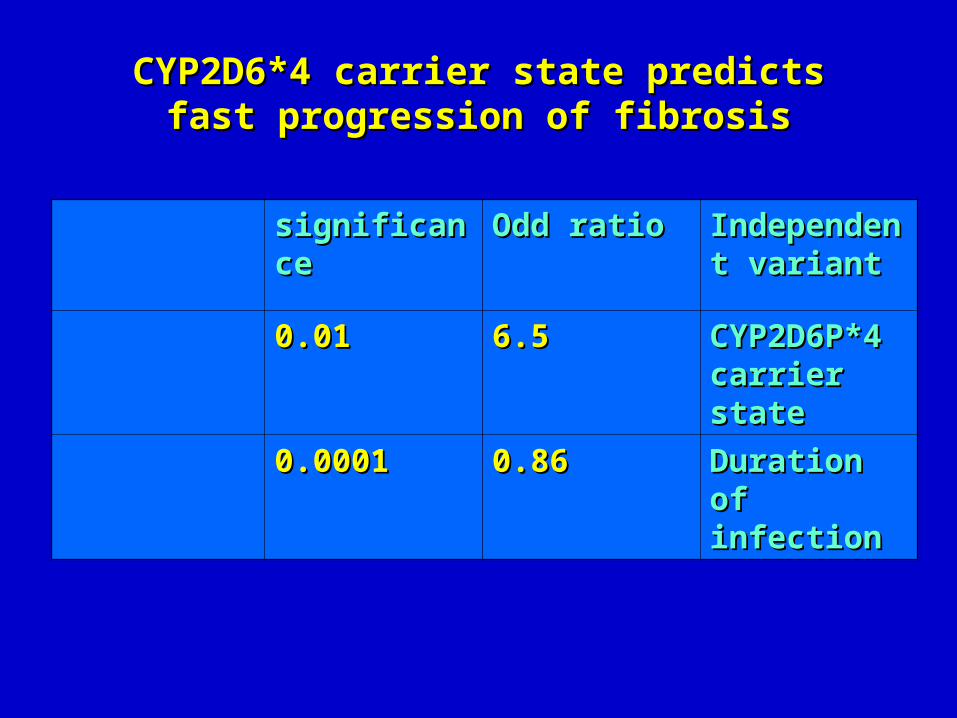
CYP2D6*4 carrier state predicts fast CYP2D6*4 carrier state predicts fast progression of fibrosisprogression of fibrosis
Independent Independent variantvariant
Odd ratioOdd ratiosignificancesignificance
CYP2D6P*4 CYP2D6P*4 carrier statecarrier state
6.56.50.010.01
Duration of Duration of infectioninfection
0.860.860.00010.0001

SummarySummary
• CYP2D6*4 allele is associated with CYP2D6*4 allele is associated with fast progression to cirrhosisfast progression to cirrhosis
• CYP2D6*4 allele frequency is CYP2D6*4 allele frequency is significantly higher in the ‘fast significantly higher in the ‘fast fibrosers’ than in the ‘slow fibrosers’ fibrosers’ than in the ‘slow fibrosers’

Conclusions
• Genetic variations influencing hepatic fibrogenesis is a topic of scientific interest
• Liver fibrosis progression rate may be predicted
• CYP2D6*4 might serve as a genetic non CYP2D6*4 might serve as a genetic non invasive marker for ‘fast fibrosers’invasive marker for ‘fast fibrosers’
Subject of the Discussion
• To develop a commercial kit for predicting the progression of liver disease in chronic liver disease patients
• The kit will be composed of:– Various CYP2D6 alleles (*1, *4, *3, *5, *6)– Other genetic variants can be studied (TNF alpha, IL10, etc)
• Target population:– Chronic liver disease patients (hepatitis C, hepatitis B, fatty
liver, …)

Biological kit for predicting liver disease progression
• The project has to include:– Founder– Consultant– Laboratory– Technicians