!muscular dystrophy association - …old.mda.org.au/infomd2008/andrew kornberg.pdfcohen hj, molnar...
TRANSCRIPT

The Management of Childhood Neuromuscular Disease in 2008
A/Prof. Andrew J. KornbergRoyal Children’s HospitalMelbourne, Australia

Neuromuscular Disorders
Muscular dystrophies– Dystrophinopathies– Congenital muscular dystrophy– Limb-Girdle muscular dystrophy– Fascioscapulohumeral muscular dystrophy– Emery-Dreifuss muscular dystrophy– Other
Myotonic dystrophyCongenital myopathiesMyasthenia gravisChannelopathiesSpinal muscular atrophiesHereditary motor and sensory neuropathiesMitochondrial disorders
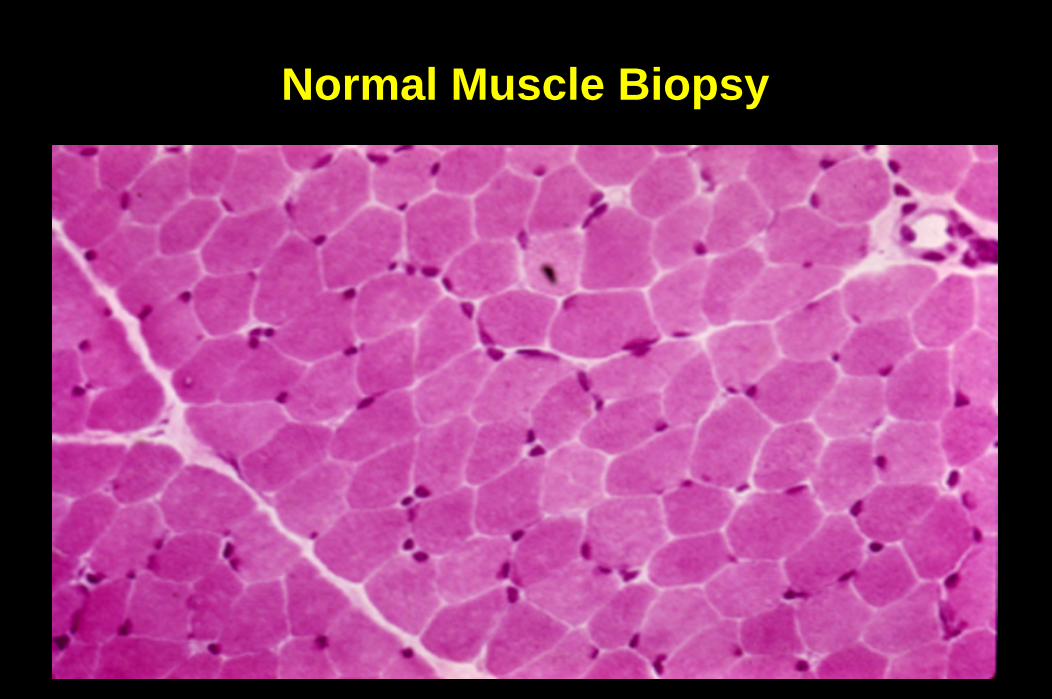
Normal Muscle Biopsy

Dystrophic Muscle Biopsy

Muscular DystrophyImmunostaining
Normal AbsentReduced

Zatz M et al. Neuromuscul Disord 2003;13:532-544.

1423 5
678
910
PyridoxineNicotinic Acid
CoQ10Creatine
GlutamineOxatomide
IL-1 RAEDTA
TaurinePentoxyfilline
Drugs with Potential to Interrupt Theorized DMD Pathophysiologic Cascades

Muscle Disease TherapyFuture Therapies
1
4
2
3
5
6
7
8
9
10
Pyridoxine + 55%Nicotinic Acid + 50%
CoQ10 + 50%Creatine + 50%
Glutamine + 42%Oxatomide + 50%
IL-1 RA + 37%EDTA + 43%
Taurine + 39%Pentoxyfilline + 50%
Mice are given target drugs or sham treatment daily for 3 months and subjected to involuntary treadmill running for 30 minutes twice per week, then tested for whole-body strength
Granchelli JA et al. Pre-clinical screening of drugs using the mdx mouse. Neuromuscul Disord 2000;10:235-239.

A paediatric Quantitative muscle strength testing (QMT) system is employed as a primary endpoint at each CINRG site where clinical trials are conducted.
Bloorview MacMillan Center, OntarioChildren’s Hospital of VirginiaChildren’s Hospital of PittsburghChildren’s National Medical CenterRoyal Children’s Hospital, Melbourne,
AustraliaTexas Scottish Rite HospitalTulane UniversityUniversity of Leuven, BelgiumUniversity of MississippiUniversity of Puerto RicoUniversity of Tel AvivUniversity of Tennessee, MemphisWashington University at St. Louis
CINRG in Clinical TrialsCooperative International Neuromuscular
Research Group

Duchenne Muscular DystrophyManagement
Multifaceted and best using a multidisciplinary approach
Genetic counselling begins at diagnosis
Management issues include:– Physical
– Emotional
– Social
– Educational
– Vocational
One major problem in bridging the physical and educational issues is intelligence capacity

Duchenne Muscular DystrophyManagement
Maintain Ambulation
Prevent or Treat Contractures
Anticipatory Monitoring
Medical Therapy

Maintain AmbulationAs long as the child with DMD is ambulant, he can usually live a reasonably independent existence and cope with most daily activitiesWhen ambulant, there is also less tendency to develop contractures and scoliosisOnce the child loses ambulation he loses much of his independence and is prone to various complications such as contractures and deformities
Duchenne Muscular DystrophyManagement

Duchenne Muscular DystrophyManagement
Maintain Ambulation
Prevent or Treat Contractures
Anticipatory Monitoring
Medical Therapy

Prevent or Treat ContracturesMaintain ambulation
Passive stretching
Night time splints
Surgical release of contractures
Duchenne Muscular DystrophyManagement

Duchenne Muscular DystrophyManagement
Maintain Ambulation
Prevent or Treat Contractures
Anticipatory Monitoring
Medical Therapy

Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone HealthScoliosisRespiratoryCardiac

Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone healthScoliosisRespiratoryCardiac

3
810
11
32
20
12
9
3
0
3
6
9
12
15
18
21
24
27
30
33
36
<50 50-59 60-69 70-79 80-89 90-99 100-109 110-119 120+
TO
TA
L N
o. O
F C
ASE
S
IQ RANGE
Normal IQ distributionPMD CasesTOTAL -106
MEAN IQ = 86.1
Distribution Of IQ Scores In DMD Cases
Cohen HJ, Molnar GE, Taft LT. The genetic relationship of progressive muscular dystrophy (Duchenne type) and mental retardation. Dev Med.Child Neurol 1968; 10:754-765.

Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone healthScoliosisRespiratoryCardiac

Duchenne Muscular DystrophyBone Health
Duchenne muscular dystrophy associated with:– Reduced bone mineral density– Increased risk of fractures
Steroids may exacerbate the reduced bone mineral densityIssues:
– How to follow bone mineral density?Z-scores do not predict fracture riskZ-scores lower than aged matched controls throughout life
– Vitamin D and calcium supplementation?No data to show that risk is reducedWho should be supplemented?
– Are there other interventions that are useful?Quinlivan R et al. Neuromuscul Disord 2005;15:72-79.Biggar WD et al. Neuromuscul Disord 2005;15:80-85.

Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone healthScoliosisRespiratoryCardiac

Duchenne Muscular DystrophyScoliosis Surgery
Average age at surgery is about 14 years
To undergo surgery– Spinal curve > 25 degrees
– Vital capacity > 30% of predicted
– No active infection
– Cardiovascular system not compromised
Rate of scoliosis surgery varies from centre to centre

Duchenne Muscular DystrophyScoliosis

Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone healthScoliosisRespiratoryCardiac
Predictable stages of decline
Nocturnal hypoventilation and hypoxia is typical– Nocturnal assisted ventilation may be helpful for symptomatic relief
Respiratory failure typically occurs in the late teens or early 20’s with an insidious onset
– Respiratory status ultimately worsens and is typically associated with demise
Steroids seem to preserve respiratory function
Duchenne Muscular DystrophyRespiratory Management
Duchenne Muscular DystrophyManagement
Anticipatory MonitoringSchool functioningContracturesBone healthScoliosisRespiratoryCardiac

Exons 48-53 deletions possibly associated with a higher incidenceDilated cardiomyopathy > hypertrophic > conduction defectsSymptomatic in 57% by age 18
– insidious onset– Cardiac death in 10% of cases
Steroids may have long term benefit on cardiac function1
Presymptomatic afterload reduction may be of long term benefit
Markham LW et al. Pediatr Cardiol 2005;26:768-771.
Duchenne Muscular DystrophyCardiac Management

Duchenne Muscular DystrophyCardiac Deficit

Duchenne Muscular DystrophyManagement
Maintain Ambulation
Prevent or Treat Contractures
Anticipatory Monitoring
Medical Therapy

Muscular DystrophyManagement
Medical Therapy
Nutritional / Chemical therapy
Drug therapy
Gene therapy– Cell replacement: myoblast transfer therapy
– Gene replacement
– Gene repair
– Gene up-regulation
– Nonsense mutation suppression
– Targeted exon skipping

Muscle DiseaseNutritional / Chemical Therapy
SeleniumVitamin EL-tyrosineL-arginineJuvenTM
Coenzyme Q10GlutamineCreatine monohydrate

Muscle DiseaseNutritional / Chemical Therapy
Selenium1
– Antioxidant– No benefit shown in clinical studies
Vitamin E1,2
– “Panacea” for many disorders– Antioxidant effect and “energy promoter”– Data in open-label pilot study of vitamin E in DMD2
No significant benefit on strength or progression of disease 1Backman E et al. Acta Neurol Scand 1988;78:429-435.
2Fenichel GM et al. Muscle Nerve 1988;11:1164-1168. 3Hankard RG et al. Pediatr Res 1998;43:222-226.

Muscle DiseaseNutritional / Chemical Therapy
L-arginineSome studies have shown benefit of L-arginine in mdxmouse
– Increased levels of utrophin and improved resistance to contraction-related muscle fiber injury
L-arginine may activate muscle fibre repair mechanisms, as well as stabilizing their membranes and perhaps improving their handling of calciumMechanism may be via nitric oxideNo evidence of benefit in humans
– Could be some detrimental effects as well– Biologically active

Muscle DiseaseNutritional / Chemical Therapy
L-tyrosine–Improved endurance and strength in a child with
nemaline myopathy1
–Improvement in secretions and bulbar function2
–No major side effects2
–Dosage used is about 250–500 mg/day2
1Kalita D. J Orthomolec Med 1989;4:70-74.2Wallgren-Pettersson C, et al. Neuromuscul Disord 2003;13:501-507.

Muscle DiseaseNutritional / Chemical Therapy
Juven– Three key ingredients
HMB (beta-hydroxy-beta-methylbutyrate), arginine and glutamine
– May promote muscle protein synthesis and increase muscle mass
– Studies show benefit in patients with cancer and HIV/AIDS in building lean muscle mass
Benefit has led to many families using this compound– Open label with limited objective measures possible benefit– $150/mo– Trial needed

Neurology, January 11, 2005
Prednisolone
O
HO
CH3
CH3CO
CH2OH
O
HO
CH3
CH3CO
CH2OOCCH3
O
NCH3
Deflazacort

CorticosteroidsMechanism of Action
The mechanism of action of steroids in Duchenne muscular dystrophy is not known, but there are a number of theories:– positive effect of steroids on myogenesis– anabolic effect on muscle, resulting in increased muscle
mass– stabilization of muscle fibre membranes– attenuation of muscle necrosis (this is controversial)– effect on intracellular calcium concentrations– immunosuppressive effect with reduction of
mononucleated cells, in particular cytotoxic CD8 cells
CorticosteroidsSide Effects
Cushingoid featuresGrowth failure (childhood)Weight gainBone
– Avascular necrosis– Osteoporosis
Myopathy– Myosin-loss– Type II atrophy
DiabetesSkin: Acne; StriaeHypertensionPsychosis and mood disturbancePseudotumor cerebriEye: Cataracts; GlaucomaInfection

Duchenne Muscular DystrophyTreatment with Steroids (1)
Usually offered at time of decline and frequent falls– Steroids would be offered earlier if:
Long term side effects were not an issueEarly therapy is shown to be important in longer term
– Some preliminary data to suggest this is the case
Rapidly improved strength– Measurable in 10 days– Maximum benefit in 3 months
Slows loss of function for up to 3 years– Prolongs ambulation by up to 2 years– Effect on natural history of disease is not known but may confer benefit
into teens

Duchenne Muscular DystrophyTreatment with Steroids (2)
Optimum studied dose of prednisone 0.75 mg/kg/d– At least 16 studies on nearly 1000 affected children have been published in the last three
decades– Daily superior to alternate days in original studies– Major problems are side effects
Early low dose alternate day steroids1
– Beneficial but weight and growth affected– As steroids are effective in prolonging function, but not in recovering lost function, the
authors propose that treatment be started with low-dose prednisone in DMD
Low-dose, intermittent schedule of steroid2,3
– First 10 days of the month or 10 days on, 10 days off– Beneficial with no effects on growth, weight or bone in early patients
1. Merlini L et al. Muscle Nerve 2003;27:222-227.2. Dubowitz V. Neuromuscul Disord 1997;7:261-267.3. Kinali M et al. Neuromuscul Disord 2002;12 (Suppl 1):S169-S174.
Duchenne Muscular DystrophyTreatment with Steroids (3)
Weekly steroids1– 5-10mg/kg/week over 1-2 days– Efficacy might be as good as daily steroids in pilot studies
CINRG trial– Side effects are minimal with growth and weight not affected
1. Connolly AM et al. Neuromuscul Disord 2002;12:917-925.

Duchenne Muscular DystrophyTreatment with Deflazacort
Deflazacort is an oxazolone derivative of prednisolone, which has anti-inflammatory and immunosuppressive effects
– The therapeutic equivalence is approximately 1.2 mg deflazacort to 1 mg prednisone
– Usual deflazacort dosage studied is 0.9 mg/kg/d
Short-term studies in Germany, Italy, and Argentina suggest that deflazacort can delay the loss of muscle function in DMD
– In those studies the ability to walk continued significantly longer in boys treated with deflazacort in comparison to no treatment
Side effects less frequent overall (in comparison to prednisone)
– Weight, growth less affected in short term studies– Asymptomatic cataracts were documented in a higher percentage of boys

What is a clinical trial?• Research study in human volunteers to answer specific
health questions• The fastest and safest way to find treatments that work
in people and ways to improve health • Interventional trials determine whether experimental
treatments or new ways of using known therapies are safe and effective under controlled environments
• Observational trials address health issues in large groups of people or populations in natural settings
Source: www.clinicaltrials.gov

Why participate in a clinical trial?
• Participants in clinical trials can play a more active role in their own health care
• Gain access to new research treatments before they are widely available
• Help others by contributing to medical research
Source: www.clinicaltrials.gov
Who can participate in a clinical trial?
• All trials have guidelines about who can participate• Inclusion/exclusion criteria is an important principle of
medical research that helps to produce reliable results • The criteria are used to identify appropriate participants
and keep them safe and help ensure that researchers will be able to answer the questions they plan to study
Source: www.clinicaltrials.gov

What happens during a clinical trial?
• The clinical team includes: doctors and nurses as well as other health care professionals
• The team: – Checks the health of the participant at the beginning of the
trial– Gives instructions for participating in the trial– Monitor the participants carefully during the trial– Stay in touch after the trial is completed
• Clinical trial participation is most successful when the protocol is carefully followed
Source: www.clinicaltrials.gov

What are the different types of clinical trials?
• Treatment trials: test experimental treatments, new combinations of drugs, or new approaches to treatments
• Prevention trials: look for better ways to prevent disease
• Diagnostic trials: find better tests or procedures for diagnosing particular disease
• Screening trials: detect certain disease or conditions• Quality of Life trials: explore ways to improve comfort
and quality of life
Source: www.clinicaltrials.gov

Clinical Trials - History• 1747 – Lind: Experiment with untreated control group (disease:
scurvy)• 1800 – Waterhouse: US based smallpox trial• 1863 – Gull: First use of placebo treatment• 1858 – Duchenne de Boulogne: First described the disease and
tested different treatments • 1931 – Amberson: First randomized trial• 1937 – NIH started grant support • 1944 – Introduction of multicenter studies• 1980s – Clinical Investigators in Duchenne Dystrophy (CIDD group)
was formed and started first trials with Duchenne

CINRG Clinical Trials
• CINRG was formed in 1999 • Academic multi-center network to facilitate clinical
trials for DMD• Central site is located at Children’s National
Medical Center in Washington, DC• Largest clinical trial network for DMD with 22
centers worldwide


Quantitative Muscle Testing
• Quantitative muscle testing (QMT) is a sensitive and precise method to test muscle strength
• CINRG developed a pediatric version, which includes video game-like features

Muscle Testing output
Breathing Testing output

Duchenne Muscular DystrophyTreatment Strategies
Type of Mutations
Gene replacement
Cell transferExon skipping
Nonsense mutation read-
through
Improve dystrophic
muscle health
Gene deletions X X X
Gene duplications X X X
Nonsense mutations X X X X
Other mutations X X
Stage of Development
Pre-clinicalEarly clinical trial
Pre-clinicalEarly clinical trial
Pre-clinicalEarly clinical trial
ClinicalClinical trial

PTC124• A small molecule that reads through a premature stop signal
in the gene that would prevent production of full-length dystrophin protein
• PTC Therapeutics granted orphan drug status from the FDA to investigate the potential of PTC124 in the treatment of cystic fibrosis and DMD
• Phase 2 human clinical trial in DMD: preliminary human trial data released Oct 2006
STOP

Neuromuscular Disease TherapySummary
These are exciting times as there is a greater understanding of the genetic, molecular, and physiological genesis of the neuromuscular disorders
– The better understanding will hopefully lead to new and hopefully effective therapies
Rapid pre-clinical screening in animal models of drugs and genetic treatments will lead to more efficient studies of their effectiveness in humansImprovement in the way we assess response to therapy in human studies, and the development of cooperative groups such as CINRG will allow the rapid study of new therapies