musculoskeletal audit
TRANSCRIPT

NationalServicesScotland
Hip fracture care pathway report 2016
Musculoskeletal audit.

© NHS National Services Scotland/Crown Copyright 2016
First published October 2009
Brief extracts from this publication may be reproduced provided the source is fully acknowledged. Proposals for reproduction of large extracts should be addressed to:
PHI Graphics Team NHS National Services Scotland Gyle Square 1 South Gyle Crescent Edinburgh EH12 9EB
Tel: +44 (0)131 275 6233 Email: [email protected]
Designed and typeset by: Chris Dunn, PHI Graphics Team
Translation Service If you would like this leaflet in a different language, large print or Braille (English only), or would like information on how it can be translated into your community language, please phone 0845 310 9900 quoting reference 287407.

MSk Audit — Hip Fracture Care Pathway — Report 2016
1
Contents
Foreword from Chief Medical Officer for Scotland .......................................................................................................................................2
1.0 Background ..........................................................................................................................................................................................................................................................3
2.0 Key Results and Recommendations – Quick Reference ........................................................................................................5
3.0 Audit Results ..................................................................................................................................................................................................................................................11
Appendices ....................................................................................................................................................................................................................................................................31
A - Demographics ................................................................................................................ 31
B - Scottish Hip Fracture Audit and Advisory Group Membership & Contacts .................... 31
C - References .....................................................................................................................33
D - Access to the Trauma and Orthopaedic Dashboard ...................................................... 34

MSk Audit — Hip Fracture Care Pathway — Report 2016
2
Foreword from Chief Medical Officer for Scotland
February 2016 saw the publication of ‘A National Clinical Strategy for Scotland’1, which provided clarity on the priorities for NHS Scotland in pursuing health and social care reform.
As the elderly population of Scotland increases, the demands placed on primary care and hospital services will increase. Understanding the effects of such changes in population demographics is vital in achieving sustainable reform and service development. This is particularly pertinent for Trauma and Orthopaedic services where a significant increase in the number of elderly patients who are at risk of sustaining fragility fractures is expected. A quality pathway of care, that optimises patient recovery without delay to surgery and to discharge, increases the likelihood of their return to their pre-fracture level of mobility and independence. Each extra day that a patient with a hip fracture spends in an acute orthopaedic bed before discharge home or to a rehab setting is also an inefficient use of a valuable hospital bed.
For the patient, delay increases future dependency levels. The detailed process measures outlined in this report are measures of quality. We should remember that ultimately the patient wishes to return home at the earliest opportunity: that should be our goal.
Patients with hip fracture experience all aspects of care, from arrival in the Emergency Department to rehabilitation in the community, including preventing the risk of further falls and improving bone health. Given the complex input required from many professionals in the care of patients who have sustained a hip fracture, there is a unique opportunity to further develop this multi-disciplinary care pathway and extend it into the community with the integration of health and social care underway. By improving the quality of care hip fracture patients receive at every stage we can facilitate a return to previous levels of function and residence prior to this potentially life changing injury.
Working together in this way will help to develop a more resilient workforce which can continue to support continuous improvement in the quality of care and the service that patients receive.
The data in this report provides evidence to support change and should be used to contribute to the local planning of services and identification of potential regional or national strategies which could be explored to improve patient outcomes.
Catherine Calderwood
Chief Medical Officer for Scotland
MSk Audit — Hip Fracture Care Pathway — Report 2016
3
1.0 Background
Hip fracture is the most common, serious orthopaedic injury to affect the elderly, with more than 6,000 patients admitted to hospital in Scotland each year. The burden of hip fracture in Scotland is likely to increase significantly over the coming decade as a consequence of population demographic changes. It is therefore essential that we manage this injury as effectively and efficiently as possible, primarily for the benefit of patients, but also for the optimum use of NHS resources. Hip fracture represents an effective ‘tracer’ condition as the management of this injury often requires a complex journey of clinical and social care involving many different disciplinary teams and community based services. As such, if we improve the quality of care for hip fracture patients, then we can expect to improve the care provided to other fragility fracture patients.
The original Scottish Hip Fracture Audit2 ran from 1993 to 2008. The development of SIGN 563 in 2002, superseded by SIGN 111 in 20094, made Scotland the first country to have both evidence based treatment guidelines and a prospective national audit of hip fracture care. During this time there were significant changes and improvements to the way hip fracture patients were managed across Scotland. From 2009, Boards were tasked with internal monitoring and the audit resource was diverted to other aspects of orthopaedic care.
In 2012/13, a four month ‘snapshot’ audit of hip fracture patients was undertaken5. This looked at key interventions along the patient journey from the Emergency Department admission to discharge from the acute orthopaedic unit. This report highlighted a number of important areas for further improvement in clinical care.
In 2014, The Scottish Standards of Care for Hip Fracture Patients6 were developed. This document outlines the key elements which constitute a standard of care for all hip fracture patients in Scotland. The Hip Fracture Care Pathway7 was also launched as one of five priority work strands of the MSK and Orthopaedic Quality Drive7. This included, for one week in four, a ‘Rolling Audit’, collected from all acute orthopaedic hospitals and reported back to monitor progress against the Standard, providing rapid feedback to facilitate ‘closing the loop on action’. The measures are now included in the Trauma and Orthopaedic Dashboard (See Appendix D for access details). In addition, funds have been provided by the Scottish Government to ‘pump-prime’ quality development projects such as Advanced Nurse Practitioners (ANP) specialising in hip fracture care. National hip fracture workshops have taken place to facilitate the spread of knowledge and quality improvement practices between units across the country.
This second audit undertaken from October 2015 to January 2016 and reported here, demonstrates that, with the hard work and dedication of all members of the hip fracture multi-disciplinary team at each hospital in Scotland, improvements in the quality of care and more rapid recovery for hip fracture patients has occurred.
The audit specifically focuses on providing measures to enable the following principles of continuous quality improvement as stated in 2020 Vision for quality efficiency and value.8
● Reduce unwarranted variation in service provision, remove waste and eliminate harm.
● Improve healthcare quality by increasing the safety, effectiveness, experience and responsiveness of services.
● Use good quality benchmarking and performance data, together with insight into service provision, to identify where productive opportunities lie.

MSk Audit — Hip Fracture Care Pathway — Report 2016
4
Moving forward, the Scottish Hip Fracture Audit and Advisory Group plans to collect data for every hip fracture patient admitted to hospital in Scotland aged over 50 on an on-going basis. This will give further insight into the elements of care that have an overall impact on patient outcomes.
Updates to The Scottish Standards of Care for Hip Fracture Patients have been made to take account of strengthening clinical evidence in a number of areas and to align more closely to the National Hip Fracture Database (NHFD) for England, Wales and Northern Ireland.
The Scottish Hip Fracture Audit and Advisory Group will continue to drive forward the aim of improving the quality of care every hip fracture patient in Scotland receives when they sustain this potentially life changing injury. We hope that by improving the quality of the complex and multi-disciplinary care this will be equally applicable to all fragility fracture patients and the wider patient population.
Graeme Holt
Chairman, Scottish Hip Fracture Audit and Advisory Group

MSk Audit — Hip Fracture Care Pathway — Report 2016
5
2.0 Key Results and Recommendations – Quick Reference
This section summarises the considerable improvements in care for patients with a hip fracture achieved between the 2012/13 (December to March) audit and the most recently audited period in 2015/16 (October to January).
Standard 1: Patients with a hip fracture should be transferred from the Emergency Department to the Orthopaedic ward within four hours.Summary: More patients are moved quickly to the ward of definitive care, which is particularly important for these, often frail and elderly patients. Time in the Emergency Department (ED) has improved, with fewer patients breaching the four-hour target (see Figure 1.1). ED stays of greater than three hours have reduced from 58% of sampled patients to 40% and the previous peak transfer time from ED to the Orthopaedic ward in the 15 minute period prior to the four-hour target has been reduced. Figure 1.2 demonstrates a change in the pattern of transfer time to a more even spread across the two to four hour time period.
Recommendation: All clinically appropriate patients should be transferred from the ED to the Orthopaedic/receiving ward within four hours unless indicated for essential medical interventions. Process mapping of the patient journey, to identify and remove points of delay, should be undertaken at all hospitals where prolonged stays and four-hour breaches are common.
Standard 2: Patients who have a clinical suspicion or confirmation of a hip fracture should have the ‘Big Six’ interventions/treatments before leaving the Emergency Department.Summary: Care in the ED has improved. In 2012/13 this bundle was completed for only 2% of patients but has risen to 20% of patients receiving all six interventions/treatments (Provision of Pain Relief, Delirium Screening, Early Warning Score, Bloods Investigations, Fluid Therapy and Pressure Area Inspection) and 83% receiving at least four (See Figure 2.1). Delirium Screening and the recording of Pressure Area Inspection are the interventions that are the least likely to be undertaken and therefore prevent units achieving the Standard. It should be noted, however, that the percentage of patients assessed for delirium in ED has doubled since 2012/13 (from 22% to 44%), allowing early management of this distressing condition. See Figures 2.2 and 2.3.

MSk Audit — Hip Fracture Care Pathway — Report 2016
6
Recommendation: Units should use standardised admission forms to make sure that all six interventions/treatments have been completed prior to the patient leaving the ED, thus supporting rapid optimisation of the patient.
Standard 3: Every patient with a hip fracture should receive the ‘Inpatient Bundle of Care’ within 24 hours of admission.Summary: Care in the pre-operative period has improved. The full bundle of four assessments (Cognitive, Nutritional, Pressure Area and Falls Assessments) had been completed in 37% of patients in 2012/13 but is now completed for more than 60% of patients. An increase in Cognitive Assessment from 53% to 90% accounts for the largest change, with the majority of patients continuing to undergo Falls, Nutritional and Pressure Area assessments. There is, however, a notable range from hospitals completing all four assessments from 100% to 30% of patients. See Figures 3.1 and 3.2.
Recommendation: Hospitals should use standardised admission forms to ensure that all four assessments and the required care they identify, have been completed within 24 hours of admission to support optimised recovery for each patient.
Standard 4: Patients must undergo surgical repair of their hip fracture within 36 hours of admissionSummary: Two changes to this standard have been made. Firstly, it now applies to all patients, thus removing the exclusion of those considered initially unfit for surgery, and secondly, patients must undergo surgery within 36 hours rather than 48 hours of admission.
The original standard was 95% of patients considered medically fit for theatre to have their operation within 24 ‘safe operating hours’ (i.e. within 48 hours) from admission to the Orthopaedic ward. This has been consistently achieved at the majority of hospitals in Scotland. In this audit period (November 2015 to February 2016) 92% was achieved nationally. See Figure 4.1.

MSk Audit — Hip Fracture Care Pathway — Report 2016
7
Based on the new standard, there has been an improvement since 2012/13 from 63% to 70% of patients (See Figure 4.2). This compares to a figure of 72% for the NHFD9.
Recommendation: Every hospital must strengthen their review of trauma practices to ensure efficient use of trauma theatre resource. Patients should not be delayed for surgery for non-correctable medical pathology. Early, pro-active management plans should be put in place to ensure rapid optimisation of patients for theatre within 36 hours of admission. There must be adequate provision of senior staff, theatres and facilities (e.g. image intensifiers) to allow 7-day access to surgery.
Standard 5: No patients should be repeatedly fasted in preparation for surgery. In addition, oral fluids should be encouraged up to two hours prior to surgery.Summary: The prolonged and repeated fasting of hip fracture patients represents an ongoing problem. The original standard has been modified to put the emphasis on avoiding repeated fasting (this data was not collected in 2012/13). This audit shows that approximately 20% of hip fracture patients are fasted on more than one occasion. See Figure 5.1.
Patients should be allowed and encouraged to drink clear fluids until two hours prior to surgery, yet approximately one in five of all patients have no oral fluids for periods of 10 hours or longer prior to surgery. This does however represent a notable improvement from 2012/13 when more than 50% of patients received no oral fluids for more than 10 hours prior to surgery. See Figure 5.2.
Recommendation: There is considerable variation across the country for the number of patients who are repeatedly fasted (from 5% to 40%). Each hospital must examine local trauma practices to avoid unnecessary fasting of patients who are unlikely to go to theatre that day and good communication is essential between the ward and trauma theatre.
Standard 6: Pre-operative catheterisation should only be carried out for identified medical reasons and not be used as ‘routine’ practice.Summary: Pre-operative catheterisation has reduced from 36% of patients to 22%, but considerable variation in practice exists between hospitals. See Figure 6.1.
Recommendation: Routine bladder catheterisation should be avoided, and should only be carried out for medical indications.

MSk Audit — Hip Fracture Care Pathway — Report 2016
8
Standard 7: Cemented hemi-arthroplasty implants should be standard, unless clinically indicated otherwise.Summary: There has been an increase in the use of cemented implants from 70% to 83% of patients undergoing hemi-arthroplasty surgery. The range at hospital level however varies from 30% to 100% (See Figure 7.1).
Recommendation: Hospitals should refer to both SIGN 1114 and NICE Guideline (CG124)10 for the surgical management of intra-capsular hip fractures in elderly patients.
Standard 8: Every patient who is identified locally as being frail should receive geriatric assessment within three days of admission.Summary: Geriatric assessment has improved, with more patients undergoing a ‘Comprehensive Geriatric Assessment’ and appropriate ortho-geriatric intervention within three days of admission. In the 2012/13 audit only 22% of patients had undergone assessment within this time period but this has more than doubled to 59%. Considerable variation still exists across Scotland, with anywhere between 0% and 98% of patients at individual hospitals receiving the required assessment within three days.
Recommendation: Comprehensive Geriatric Assessment and specialist input are essential to ensuring a positive patient outcome. The use of specialist Advanced Nurse Practitioners to prioritise care and undertake many of the tasks, and ward sessions for GPs with a special interest, should be considered in areas where the geriatric medicine resource is insufficient to meet the required need.

MSk Audit — Hip Fracture Care Pathway — Report 2016
9
Standard 9: Mobilisation should have begun by the end of the first day after surgery and every patient should have Physiotherapy assessment by end of day two.
AndStandard 10: Patients with a hip fracture should have an Occupational Therapy (OT) assessment by the end of day three post-operatively.Summary: Early mobilisation of patients following surgery is key to a more rapid recovery and has increased slightly, but 35% of patients experienced a delay to initial mobilisation (See Figure 9.1). Access to allied health professionals to support patient recovery and discharge is improving but one in ten patients have not received their first Physiotherapy assessment by the end of Day Two (See Figure 9.2) and four out of ten have not received an Occupational Therapy assessment by the end of Day Three, although this has improved significantly since 2012/13 (See Figure 10.1).
Recommendation: All hospitals should prioritise early mobilisation of patients and provide sufficient Physiotherapy and Occupational Therapy resource early in the patient’s recovery. Services should be designed to provide input on a 7-day basis. This has the potential to optimise the patient’s recovery and shorten length of stay.
Standard 11: Every patient who has a hip fracture should have an assessment of their bone health prior to leaving the acute orthopaedic ward.Summary: Since the 2012/13 audit there has been improvement in the number of patients who have an assessment of their bone health prior to leaving the acute orthopaedic ward. There is, however, significant variation across Scotland (see Figure 11.1). It is noted that some patients have an assessment carried out following discharge.
Recommendation: Every hospital should have systems in place to ensure that each patient with a hip fracture has a bone assessment carried out and relevant treatment started during their acute admission, or soon after discharge, aimed at reducing future fracture risk.

MSk Audit — Hip Fracture Care Pathway — Report 2016
10
Standard 12: Every patient’s recovery should be optimised by a multi-disciplinary team approach so that they are discharged back to their original place of residence within 30 days from the date of admission.The main aim of the audit and improvement work is to get patients back to their original place of residence as rapidly as possible, with a level of mobility, function and independence which is acceptable to them, by optimising the pathway of care during their acute hospital stay.
The Scottish Hip Fracture Audit and Advisory Group plan to expand this aim to include the whole patient journey by developing standards to include: fracture prevention through services providing falls prevention programmes; management of osteoporosis and discharge management to rehabilitation units as well as to the community setting.
Summary: Median Length of Stay (LOS) in an acute hospital varies considerably. Nationally, if a patient is discharged home, median LOS is 11 days; to a care-home is 9 days and to a rehabilitation unit is 11 days (See Figure 12.1).
Improvements in the interventions along the pathway have resulted in a reduced total LOS (acute and rehab settings) since the previous audit. The large variation between hospitals, with some having a median total LOS double those with the lowest LOS, is largely driven by the percentage of patients discharged straight back home/to a care home rather than on to a rehab setting (See Figure 12.2). More patients are discharged directly home or back to a care home now than in the previous audit, with a variation from 25% to 80% between hospitals (See Figure 12.3).
Since 2012/3 there has been an increase in the percentage of patients admitted from their own home who return there by 30 days from 42% to 58%. This represents the group of patients who may potentially lose their previous independence following a hip fracture (See Figures 12.4 to 12.6).
There has been an increase in the percentage of previously mobile patients who have returned to their pre-fracture level of mobility within four months of their hip fracture.
The Readmission Rate is an important measure of the quality of the hip fracture care pathway and the discharge process. There has been no change in the national rate but there is a considerable variation between hospitals (See Figure 12.9).
Overall Recommendation: Hospitals are encouraged to use all of the measures in this audit to focus improvement on the patient journey to meet the Scottish Standards of Care for Patients with a Hip Fracture and therefore impact positively on patient length of stay and successful and rapid return to their previous residence. Further analysis to understand variation in discharge delay reason is being undertaken.
All hospitals should begin discharge planning as soon as the patient is admitted, with early communication with primary care agencies such as social work to facilitate the early and safe discharge of patients following surgery for hip fracture.

MSk Audit — Hip Fracture Care Pathway — Report 2016
11
3.0 Audit Results
This section compares the audit data for each hospital against the Scottish Hip Fracture Care Standard and highlights considerable national improvement since the 2012/13 audit. It also identifies areas where the standards have been updated.
Standard 1: Patients with a hip fracture should be transferred from the Emergency Department to the Orthopaedic ward within four hours.More patients are moved quickly to the ward of definitive care, which is particularly important for these often frail and elderly patients. Time in the Emergency Department (ED) has improved, with fewer patients breaching the four hour target.
Fig. 1.1 Time in ED
Inverc
lyde (
27)
Monkla
nds (
41)
DGRI (33)
Ninewell
s (55
)
Wes
tern I
sles (
14)
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
<=2 hours 2-3 hours 3-4 hours >4 hours Data unavailable
Raigmore
(42)
Elgin (
27)
BGH (36)
Fife (9
7)
Perth (
36)
Wish
aw (4
5)
Crossh
ouse
(34)
RIE (1
08)
Forth V
alley
(62)
Aberde
en (4
1)
Hairmyre
s (43
)
QEUHG (43)
Ayr (33
)
GRI (60)
RAH (62)
All Site
s 12/1
3 (12
37)
All Site
s 15/1
6 (93
9)
ED stays of greater than three hours have reduced from 58% of sampled patients to 40% and the previous peak transfer time from ED to the Orthopaedic ward in the 15 minute period prior to the four-hour target has been reduced. Figure 1.2 demonstrates a change in the pattern of transfer time to a more even spread across a two to four hour post-admission time period.

MSk Audit — Hip Fracture Care Pathway — Report 2016
12
Fig. 1.2 Transfer Time from ED to Ward
0
5
10
15
0 1 2 3 4 5
Per
cent
age
of P
atie
nts
Time in ED (hours)
2012/13 2015/16
Higher percentageof patients in ED for<3 hours in 2015/16
Fewer patients in ED formore than 4 hours in2015/16, and fewerdischarged just beforethe 4-hour target
Recommendation: All clinically appropriate patients should be transferred from the ED to the Orthopaedic ward within 4 hours, unless indicated for essential medical interventions. Process mapping of the patient journey, to identify and remove points of delay should be undertaken at all hospitals where prolonged stays and four-hour breaches are common (including access to interventions and treatments within ED as well as delays to a bed within the ward).
Standard 2: Patients who have a clinical suspicion or confirmation of a hip fracture should have the ‘Big Six’ interventions/treatments before leaving the Emergency Department.Care in the ED has improved. In 2012/13 this bundle was completed for only 2% of patients but has risen to 20% of patients receiving all six interventions/treatments (Provision of Pain Relief, Delirium Screening, Early Warning Score, Bloods Investigations, Fluid Therapy and Pressure Area Inspection) and 83% receiving at least four. Delirium Screening and the recording of Pressure Area Inspection are the interventions that are the least likely to be undertaken and therefore prevent units achieving the Standard.
These interventions/treatments are not specific to Hip Fracture patients and therefore are likely to reflect the percentage of all frail elderly patients for whom these interventions/treatments are undertaken.
Fig 2.1 ‘Big Six’ ED Interventions/Treatments
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
All 6 4-5 1-3 None Missing data
Raigmore
(42)
BGH (36)
DGRI (33)
RAH (62)
Crossh
ouse
(34)
RIE (1
08)
QEUHG (43)
Fife (9
7)
Ninewell
s (55
)
Perth (
36)
Inverc
lyde (
27)
Monkla
nds (
41)
Hairmyre
s (43
)
Wes
tern I
sles (
14)
Aberde
en (4
1)
GRI (60)
Ayr (33
)
Elgin (
27)
Forth V
alley
(62)
Wish
aw (4
5)
All Site
s 12/1
3 (12
37)
All Site
s 15/1
6 (93
9)

MSk Audit — Hip Fracture Care Pathway — Report 2016
13
Pain Relief - An improvement has been seen nationally in this standard from 93% to 96% but some units continue to fall below 90% of patients. Further education in these units on the importance of effective early analgesia for improving patient comfort as well as preventing long term chronic pain complications should be a priority.
Delirium Screening - Improvements have been made in patients receiving delirium screening. The percentage of patients assessed for delirium in ED has doubled since 2012/13 (from 22% to 44%) allowing early management of this distressing condition. Marked variation exists, with some units undertaking no screening. Failure to recognise and manage delirium early has the potential to lead to a slower recovery for the patient and therefore greater length of stay with associated cost to the service.
Early Warning System Score - Nationally the recording of EWS scores in the ED is at a high level (an increase from 86% to 90% of patients between the two audits, with some units at, or very nearly at, 100%). It is notable that there remain some units not achieving this high level.
Fig. 2.2 Big Six Interventions/Treatments – Pain Relief, Delirium Screening, Early Warning Score
0
20
40
60
80
100
Per
cent
age
of P
atie
nts
Analgesia given Delirium screened EWS recorded
Ayr (33
)
Crossh
ouse
(34)
BGH (36)
DGRI (33)
Fife (9
7)
Forth V
alley
(62)
Aberde
en (4
1)
Elgin (
27)
GRI (60)
QEUHG (43)
RAH (62)
Inverc
lyde (
27)
Raigmore
(42)
Hairmyre
s (43
)
Monkla
nds (
41)
Wish
aw (4
5)
RIE (1
08)
Ninewell
s (55
)
Perth (
36)
Wes
tern I
sles (
14)
All Site
s 12/1
3 (12
37)
All Site
s 15/1
6 (93
9)
*An increase in delirium screening in ED was noted despite the audit criteria having changed to only record use of recognised delirium screening tools
Bloods Investigations - An overall improvement has been seen since the last audit with almost all units approaching 100% of patients having this workup completed. (N.B. The two Tayside hospitals have a different front-door policy for surgical patients who are transferred directly to ward level care on arrival at the ED unless requiring resuscitation).
Fluid Therapy - An increase in IV fluid usage has occurred nationally, although it is still only used in 75% of patients. Considerable variation across units exists and this may be in part due to patients still drinking normally as they are not designated ‘nil by mouth’ as they will not go to theatre on the same day.
Pressure Area Inspection - Documentation of pressure area inspection and management has improved nationally but remains one of the most variably completed assessments, with some units achieving almost 100% and others rarely completing this assessment.

MSk Audit — Hip Fracture Care Pathway — Report 2016
14
Fig. 2.3 Big Six Interventions/Treatments – Bloods, Fluids, Pressure Area Assessment
20
40
60
80
100
Per
cent
age
of P
atie
nts
0
Ayr (33
)
Crossh
ouse
(34)
BGH (36)
DGRI (33)
Fife (9
7)
Forth V
alley
(62)
Aberde
en (4
1)
Elgin (
27)
GRI (60)
QEUHG (43)
RAH (62)
Inverc
lyde (
27)
Raigmore
(42)
Hairmyre
s (43
)
Monkla
nds (
41)
Wish
aw (4
5)
RIE (1
08)
Ninewell
s (55
)
Perth (
36)
Wes
tern I
sles (
14)
All Site
s 12/1
3 (12
37)
All Site
s 15/1
6 (93
9)
Bloods taken IV fluids commenced Pressure areas recorded
Recommendation: Units should use standardised admission forms to make sure that all six interventions/treatments have been completed prior to the patient leaving the ED, thus supporting rapid optimisation of the patient.
Where an Early Warning System (EWS) Score had been documented in both ED and on arrival in the ward, the vast majority of patients had either a decrease in the EWS score or experienced no change. It is recognised that small increases in the EWS score may occur for reasons other than a genuine deterioration in the patient’s condition (e.g. moving a patient from a trolley onto a hospital bed may cause a transient rise in heart rate which could be falsely interpreted as a worsening in their state). An increase in score of two or more is likely to reflect a significant deterioration and a review of interventions to reduce this occurrence should be undertaken at each hospital.
Fig 2.4 Changes in Early Warning System (EWS*) score from ED to Ward
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
EWS increased >=2 by admission EWS increased by 1 by admission EWS same in ED and orthoEWS decreased by admission Not recorded
Perth (
36)
Forth V
alley
(62)
Wish
aw (4
5)
Wes
tern I
sles (
14)
Monkla
nds (
41)
BGH (36)
Hairmyre
s (43
)
Aberde
en (4
1)
DGRI (33)
Ninewell
s (55
)
RIE (1
08)
Inverc
lyde (
27)
GRI (60)
Crossh
ouse
(34)
Ayr (33
)
QEUHG (43)
Raigmore
(42)
RAH (62)
Fife (9
7)
Elgin (
27)
All Site
s 12/1
3 (12
37)
All Site
s 15/1
6 (93
9)
*This includes SEWS, MEWS and NEWS dependent on local protocol

MSk Audit — Hip Fracture Care Pathway — Report 2016
15
Standard 3: Every patient with a hip fracture should receive the ‘Inpatient Bundle of Care’ within 24 hours of admission.Care in the pre-operative period has improved. The full bundle of four assessments (Cognitive, Nutritional, Pressure Area and Falls Assessments) had been completed in 37% of patients in 2012/13 but is now completed for more than 60% of patients. An increase in Cognitive Assessment from 53% to 90% accounts for the largest change, with the majority of patients continuing to undergo Falls, Nutritional and Pressure Area assessments. There is, however, a notable range from hospitals completing all four assessments from 100% to 30% of patients.
Fig 3.1 Inpatient Assessment Bundle
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
All 4 3 1-2 None Data not available
QEUHG (46)
RAH (72)
Crossh
ouse
(35)
Raigmore
(56)
Wes
tern I
sles (
17)
Inverc
lyde (
32)
Wish
aw (4
7)
Fife (1
05)
Elgin (
29)
Forth V
alley
(63)
Monkla
nds (
44)
GRI (61)
Aberde
en (4
3)
Ayr (34
)
BGH (36)
Ninewell
s (63
)
RIE (1
39)
Hairmyre
s (43
)
DGRI (38)
Perth (
38)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)
Cognition assessment - Improvement is demonstrated in cognition assessment, from 53% in the 2012/13 audit, to above 90% in this audit. This may have been supported by Healthcare Improvement Scotland’s Delirium Toolkit (2014)11, and associated educational programmes, which incorporates baseline cognitive status assessment.
Falls assessment - Some improvement is demonstrated in rates of falls assessment, with 83% completion in 2012/13 and greater than 88% in this audit.
Nutritional assessment - Completion of nutritional assessment has risen from 70% in 2012/13 to 72% in this audit but this assessment is now the most frequent missing bundle element.
Pressure area assessment - Pressure area assessment has been consistently completed for greater than 89% of patients since 2012/13.

MSk Audit — Hip Fracture Care Pathway — Report 2016
16
Fig. 3.2 Inpatients assessments by type
0
20
40
60
80
100
Per
cent
age
of P
atie
nts
Cognition Assessment Falls Assessment Nutritional Assessment Pressure Areas Assessment
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
05)
Forth V
alley
(63)
Aberde
en (4
3)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (72)
Inverc
lyde (
32)
Raigmore
(56)
Hairmyre
s (43
)
Monkla
nds (
44)
Wish
aw (4
7)
RIE (1
39)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)
Recommendation: Hospitals should use standardised admission forms to ensure that all four assessments and the required care they identify, have been completed within 24 hours of admission to support optimised recovery for each patient.
Standard 4: Patients must undergo surgical repair of their hip fracture within 36 hours of admission.Two changes to this standard have been made. Firstly, it now applies to all patients, thus removing the exclusion of those considered initially unfit for surgery, and secondly, patients must undergo surgery within 36 hours rather than 48 hours of admission. The original standard was 95% of patients considered medically fit for theatre to have their operation within 24 ‘safe operating hours’ (i.e. within 48 hours) from admission to the Orthopaedic ward. This has been consistently achieved at the majority of hospitals in Scotland. In this audit period (October 2015 to January 2016) 92% was achieved nationally.
Fig. 4.1 Time to theatre for all patients deemed medically fit
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Within 48h 48-72 hours 72-96 hours More than 96 hours Delayed - other *
GRI (57)
Inverc
lyde (
31)
Perth (
32)
Ninewell
s (62
)
Raigmore
(54)
QEUHG (44)
Monkla
nds (
39)
DGRI (38)
Crossh
ouse
(31)
Hairmyre
s (31
)
Ayr (30
)
Elgin (
26)
BGH (35)
Wes
tern I
sles (
17)
RAH (62)
Fife (9
3)
Wish
aw (4
3)
Forth V
alley
(56)
Aberde
en (3
9)
RIE (1
23)
All Site
s 12/1
3 (12
30)
All Site
s 15/1
6 (94
3)
* ‘Delayed - Other’ refers to patients who were medically fit for theatre during the first 48 hours of admission but then became unfit for theatre.
Based on the new standard, there has been an improvement since 2012/13 from 63% to 70% of patients. This compares to a figure of 72% for the NHFD9.

MSk Audit — Hip Fracture Care Pathway — Report 2016
17
Fig 4.2 Time to theatre for all patients
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
<24 hours 24-36 hours 36-48 hours >48 hours Conservative treatment Not known
Inverc
lyde (
32)
DGRI (38)
QEUHG (46)
Raigmore
(56)
Ayr (34
)
Ninewell
s (63
)
GRI (61)
BGH (36)
Wish
aw (4
7)
Monkla
nds (
44)
RAH (72)
Elgin (
29)
Perth (
38)
Fife (1
05)
Forth V
alley
(63)
Wes
tern I
sles (
17)
Hairmyre
s (43
)
Aberde
en (4
3)
Crossh
ouse
(35)
RIE (1
39)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)
In this audit a similar percentage of patients were considered unfit for surgery within 48 hours of admission to orthopaedic care as in the 2012/13 audit.
Fig. 4.3 Percentage of patients treated surgically but initially documented as unfit for theatre within 48 hours of ward admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Fit for theatre Documented as Unfit Not known
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
00)
Forth V
alley
(58)
Aberde
en (4
1)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (71)
Inverc
lyde (
32)
Raigmore
(55)
Hairmye
rs (41
)
Monkla
nds (
44)
Wish
aw (4
4)
RIE (1
37)
Ninewell
ls (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)

MSk Audit — Hip Fracture Care Pathway — Report 2016
18
Fig 4.4 Reasons for theatre delay if more than 48 hours
0%
10%
20%
30%
40%
50%
Per
cent
age
of P
atie
nts
Lack of theatre time Initially treated conservatively Delayed diagnosisDelayed consent Delay for THR OtherReason for delay unknown No delay
GRI (57)
Inverc
lyde (
31)
Perth (
32)
Ninewell
s (62
)
Raigmore
(54)
QEUHG (44)
Monkla
nds (
39)
DGRI (38)
Crossh
ouse
(31)
Hairmyre
s (31
)
Ayr (30
)
Elgin (
26)
BGH (35)
Wes
tern I
sles (
17)
RAH (62)
Fife (9
3)
Wish
aw (4
3)
Forth V
alley
(56)
Aberde
en (3
9)
RIE (1
23)
All Site
s 12/1
3 (12
27)
All Site
s 15/1
6 (94
3)
Delays at RIE were mainly in one month when 23/30 patients were delayed
Recommendation: Every hospital must strengthen their review of trauma practices to ensure efficient use of trauma theatre resource. Patients should not be delayed for surgery for non-correctable medical pathology. Early, pro-active management plans should be put in place to ensure rapid optimisation of patients for theatre within 36 hours of admission. There must be adequate provision of senior staff, theatres and facilities (e.g. image intensifiers) to allow 7-day access to surgery.

MSk Audit — Hip Fracture Care Pathway — Report 2016
19
Standard 5: No patients should be repeatedly fasted in preparation for surgery. In addition, oral fluids should be encouraged up to two hours prior to surgery.The prolonged and repeated fasting of hip fracture patients represents an ongoing problem. The original standard has been modified to put the emphasis on avoiding repeated fasting (this data was not collected in 2012/13). This audit shows that approximately one in five patients with a hip fracture are fasted on more than one occasion.
Fig 5.1 Was fasting cycle repeated?
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Yes No Not knownW
ester
n Isle
s (17
)
Inverc
lyde (
32)
QEUHG (46)
DGRI (38)
GRI (61)
BGH (36)
Ninewell
s (63
)
Raigmore
(55)
Ayr (34
)
Fife (1
00)
Forth V
alley
(58)
RAH (71)
Wish
aw (4
4)
Perth (
38)
Monkla
nds (
44)
Hairmyre
s (41
)
Elgin (
29)
RIE (1
37)
Crossh
ouse
(35)
Aberde
en (4
1)
All Site
s 12/1
3 (0)
All Site
s 15/1
6 (10
20)
Patients should be allowed and encouraged to drink clear fluids until two hours prior to surgery, yet approximately one in five of all patients have no oral fluids for periods of ten hours or longer prior to surgery. This does however represent a notable improvement from 2012/13 when more than 50% of patients received no oral fluids for more than 10 hours prior to surgery.
Fig. 5.2 When were clear oral fluids stopped prior to induction of anaesthetic?
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
<= 2 hours 2-6 hours 6-10 hours >10 hours Not recorded
Elgin (
29)
Perth (
38)
Fife (1
00)
RAH (71)
Raigmore
(55)
Forth V
alley
(58)
GRI (61)
Hairmye
rs (41
)
Wish
aw (4
4)
Monkla
nds (
44)
Crossh
ouse
(35)
Ninewell
s (63
)
Wes
tern I
sles (
17)
QEUHG (46)
DGRI (38)
BGH (36)
Inverc
lyde (
32)
Ayr (34
)
Aberde
en (4
1)
RIE (1
37)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)
Recommendation: There is considerable variation across the country for the number of patients who are repeatedly fasted (from 5% to 40%). Each hospital must examine local trauma practices to avoid unnecessary fasting of patients who are unlikely to go to theatre that day and good communication is essential between the ward and trauma theatre.

MSk Audit — Hip Fracture Care Pathway — Report 2016
20
Standard 6: Pre-operative catheterisation should only be carried out for identified medical reasons and not be used as ‘routine’ practice.Pre-operative catheterisation has reduced from 36% of patients to 25%, but considerable variation in practice exists between hospitals.
Fig. 6.1 Catheterisation
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Pre-op Intra-op Post-op Catheterised, but timing unknown Not known Not catheterised
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
00)
Forth V
alley
(58)
Aberde
en (4
1)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (71)
Inverc
lyde (
32)
Raigmore
(55)
Hairmyre
s (41
)
Monkla
nds (
44)
Wish
aw (4
4)
RIE (1
37)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
49)
All Site
s 15/1
6 (10
20)
Pre-transfer catheterisation included as ‘Pre-op’.
Recommendation: Routine bladder catheterisation should be avoided, and should only be carried out for medical indications.
Standard 7: Cemented hemi-arthroplasty implants should be used as standard, unless clinically indicated otherwise.In 2012/13, 70% of patients underwent hemi-arthroplasty with cemented implant designs which has risen to over 80% in this audit. Significant variation in practice remains across the country with the percentage of cemented implants used ranging from 30% to 100%. Such variation exists contrary to the recommendations and evidence base presented in both SIGN 1114 and the NICE Guideline (CG124)10 for the management of hip fractures.
Fig. 7.1 Hemi-arthroplasty – use of cement
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Cemented Uncemented Unknown
Ayr (16
)
DGRI (19)
Forth V
alley
(27)
RAH (28)
Wes
tern I
sles (
6)
RIE (6
7)
QEUHG (24)
GRI (22)
Aberde
en (1
9)
Inverc
lyde (
15)
Wish
aw (1
4)
Monkla
nds (
22)
BGH (19)
Hairmyre
s (19
)
Ninewell
s (34
)
Crossh
ouse
(19)
Perth (
22)
Elgin (
15)
Fife (5
0)
Raigmore
(37)
All Site
s 12/1
3 (64
6)
All Site
s 15/1
6 (48
9)

MSk Audit — Hip Fracture Care Pathway — Report 2016
21
There has been an increase in the number of total hip replacements performed from 5% in 2012/13 to 9% in this audit. This number remains much lower than would be expected based on current published recommendations. The use of ‘pin and plate’ fixation has remained relatively constant, although the use of intra-medullar devices varies significantly across the country from 0% to 40%.
Fig. 7.2 Type of operation
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Cannulated screws Intramedullary fixation Pin & Plate (includes DHS) HemiarthroplastyTHR Other Not known
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
00)
Forth V
alley
(58)
Aberde
en (4
1)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (71)
Inverc
lyde (
32)
Raigmore
(55)
Hairmyre
s (41
)
Monkla
nds (
44)
Wish
aw (4
4)
RIE (1
37)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)
Recommendation: Hospitals should refer to both SIGN 1114 and NICE Guideline (CG124)10 for the surgical management of intra-capsular hip fractures in elderly patients.
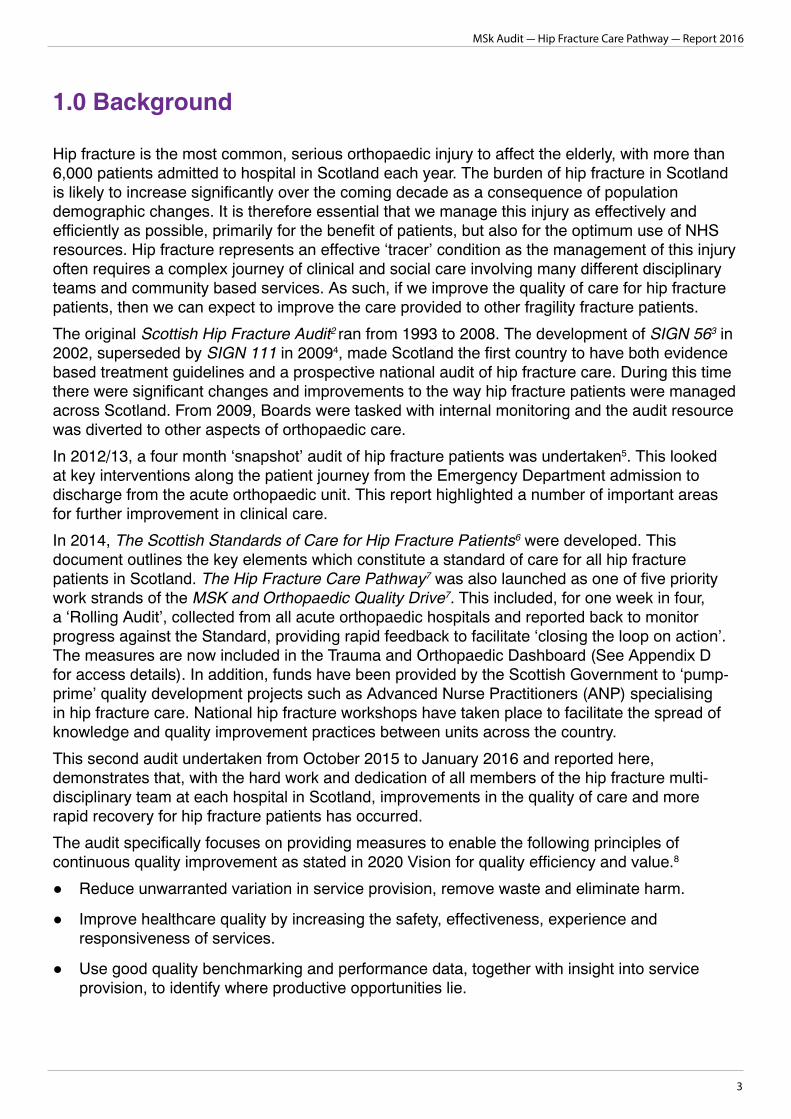
The ideal anaesthetic for hip fracture surgery has yet to be identified. With the current evidence, neuraxial (e.g. spinal, epidural) anaesthesia does not appear to be superior to general anaesthesia. Many hip fracture guidelines, however, indicate that spinal anaesthesia may be the preferred approach. Nerve blocks reduce pain and reduce opioid requirement, which may reduce the incidence of delirium. Nerve blocks should therefore be considered in all patients.
Fig. 7.3 Type of anaesthetic - Spinal or GA
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
General Spinal Regional/Nerve Block or Other only Not known
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
00)
Forth V
alley
(58)
Aberde
en (4
1)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (71)
Inverc
lyde (
32)
Raigmore
(55)
Hairmyre
s (41
)
Monkla
nds (
44)
Wish
aw (4
4)
RIE (1
37)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)
One patient given epidural, included in ‘Spinal’ group
MSk Audit — Hip Fracture Care Pathway — Report 2016
22
Fig. 7.4 Type of anaesthetic – use of nerve blocks and local infiltrated anaesthesia (LIA)
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Regional/Nerve block Regional/Nerve block + LIA LIA Neither Not known
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
00)
Forth V
alley
(58)
Aberde
en (4
1)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (71)
Inverc
lyde (
32)
Raigmore
(55)
Hairmyre
s (41
)
Monkla
nds (
44)
Wish
aw (4
4)
RIE (1
37)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)
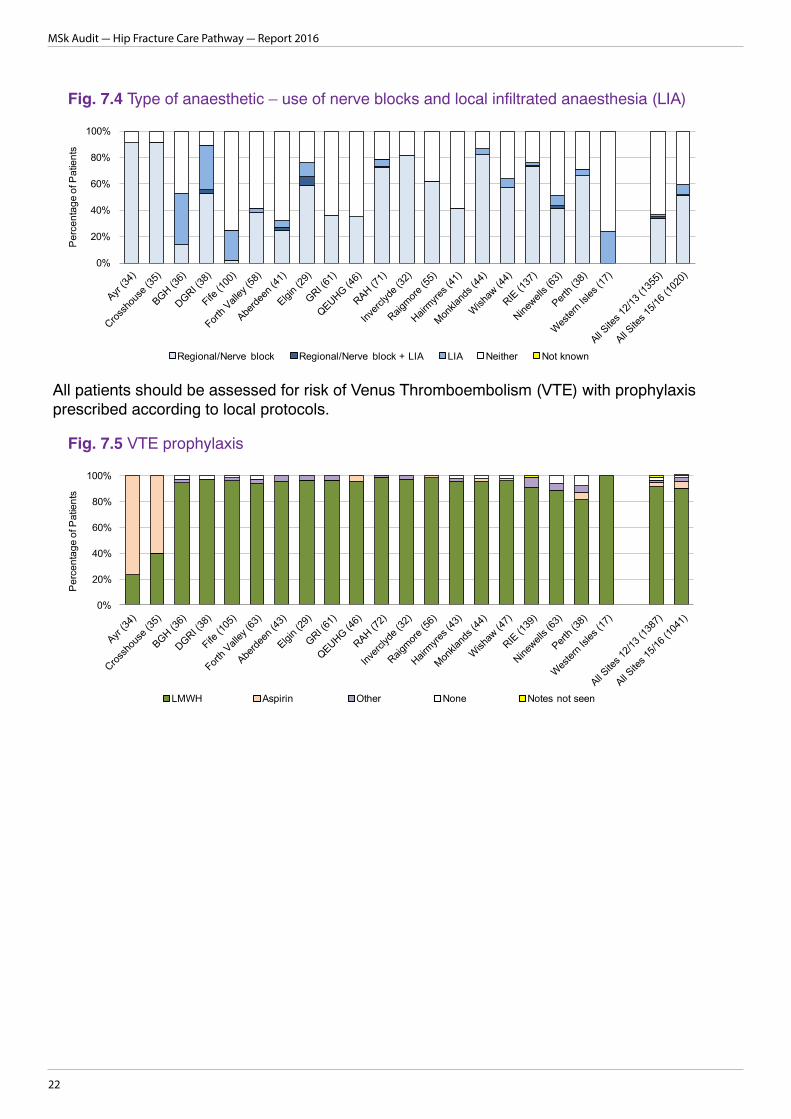
All patients should be assessed for risk of Venus Thromboembolism (VTE) with prophylaxis prescribed according to local protocols.
Fig. 7.5 VTE prophylaxis
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
LMWH Aspirin Other None Notes not seen
Ayr (34
)
Crossh
ouse
(35)
BGH (36)
DGRI (38)
Fife (1
05)
Forth V
alley
(63)
Aberde
en (4
3)
Elgin (
29)
GRI (61)
QEUHG (46)
RAH (72)
Inverc
lyde (
32)
Raigmore
(56)
Hairmyre
s (43
)
Monkla
nds (
44)
Wish
aw (4
7)
RIE (1
39)
Ninewell
s (63
)
Perth (
38)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)

MSk Audit — Hip Fracture Care Pathway — Report 2016
23
Standard 8: Every patient who is identified locally as being frail should receive geriatric assessment within three days of admission.Geriatric assessment has improved, with more patients undergoing a ‘Comprehensive Geriatric Assessment’ and appropriate ortho-geriatric intervention within three days of admission. In the 2012/13 audit only 22% of patients had undergone assessment within this time period but this has more than doubled to 59%. Considerable variation still exists across Scotland, with between 0% and 98% of patients at individual hospitals receiving geriatric assessment within three days.
Fig. 8.1 Time until geriatric input
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
By first day post-admission On Day 2 post-admission On Day 3 post-admission Not seen by Day 3 Not known
RIE (1
33)
Raigmore
(53)
Fife (1
03)
Ninewell
s (59
)
QEUHG (43)
BGH (34)
DGRI (37)
Crossh
ouse
(34)
GRI (57)
Monkla
nds (
43)
Forth V
alley
(56)
Elgin (
28)
Hairmyre
s (39
)
Aberde
en (4
1)
RAH (55)
Ayr (32
)
Perth (
38)
Inverc
lyde (
32)
Wish
aw (4
6)
Wes
tern I
sles (
16)
All Site
s 12/1
3 (13
40)
All Site
s 15/1
6 (97
9)
In the 2012/13 audit, only ‘Time seen by geriatrician’ was recorded. Following clarification of roles and responsibilities, the input of selected specialist nurses was classed as the commencement of geriatric input. Excludes patients under 60 years old, those that did not fulfil individual hospitals’ geriatric referral criteria, and those who died on day of admission.
Recommendation: Comprehensive Geriatric Assessment and specialist input are essential to ensuring a positive patient outcome. The use of specialist Advanced Nurse Practitioners to prioritise care and undertake many of the tasks, and ward sessions for GPs with a special interest, should be considered in areas where the geriatric medicine resource is insufficient to meet the required need.

MSk Audit — Hip Fracture Care Pathway — Report 2016
24
Standard 9: Mobilisation should have begun by the end of the first day after surgery and every patient should have Physiotherapy assessment by end of day two.Early mobilisation of patients following surgery is key to a more rapid recovery and has increased slightly, but one in five patients experienced a delay to initial mobilisation.
Fig. 9.1 Mobilisation
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Crossh
ouse
(35)
Wes
tern I
sles (
17)
QEUHG (46)
Forth V
alley
(58)
Ayr (34
)
Monkla
nds (
44)
Raigmore
(55)
Ninewell
s (63
)
GRI (61)
Fife (1
00)
DGRI (38)
RAH (71)
Wish
aw (4
4)
Perth (
38)
RIE (1
37)
Hairmyre
s (41
)
Elgin (
29)
Inverc
lyde (
32)
BGH (36)
Aberde
en (4
1)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
20)
By first day post-op Second day post-op 3rd day post-op or later/Not mobilised Not known
Excludes patients treated conservatively.
Access to allied health professionals to support patient recovery and discharge is improving but one in ten patients still have not received their first Physiotherapy assessment by the end of Day Two.
Fig. 9.2 Time from surgery until seen by physio
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
On day of operation Day 1 post-op Day 2 post-op Not seen by Day 2 post-op Not known
Crossh
ouse
(35)
Ayr (34
)
Fife (9
9)
Raigmore
(55)
DGRI (38)
Forth V
alley
(58)
QEUHG (46)
Aberde
en (4
1)
RAH (71)
RIE (1
35)
BGH (36)
Wish
aw (4
3)
Perth (
38)
Ninewell
s (63
)
Monkla
nds (
44)
GRI (61)
Inverc
lyde (
32)
Wes
tern I
sles (
17)
Elgin (
29)
Hairmyre
s (41
)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
16)
Excludes patients who died within two days of surgery

MSk Audit — Hip Fracture Care Pathway — Report 2016
25
Standard 10: Patients with a hip fracture should have an Occupational Therapy (OT) assessment by the end of day three post-operatively.Four out of every ten patients still experience a delay in receiving an Occupational Therapy assessment, although this has improved significantly since 2012/13.
Fig. 10.1 Time from surgery until seen by OT
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Within 3 days of operation Not seen within 3 days Not known
Fife (9
9)
Raigmore
(55)
RAH (71)
Forth V
alley
(58)
Monkla
nds (
44)
Ayr (34
)
Aberde
en (4
1)
DGRI (38)
Crossh
ouse
(35)
Hairmyre
s (41
)
QEUHG (46)
Wish
aw (4
3)
Wes
tern I
sles (
17)
Inverc
lyde (
32)
Elgin (
29)
BGH (36)
Ninewell
s (63
)
GRI (60)
Perth (
37)
RIE (1
34)
All Site
s 12/1
3 (13
55)
All Site
s 15/1
6 (10
13)
Recommendation: All hospitals should prioritise early mobilisation of patients and provide sufficient Physiotherapy and Occupational Therapy resource early in the patient’s recovery. Services should be designed to provide input on a 7 day basis. This has the potential to optimise patients’ recovery and shorten length of stay.
Standard 11: Every patient who has a hip fracture should have an assessment of their bone health prior to leaving the acute orthopaedic ward.Since the 2012/13 audit there has been improvement in the number of patients who have an assessment of their bone health prior to leaving the acute orthopaedic ward. There is, however, significant variation across Scotland. It is noted that some patients have an assessment carried out following discharge.
Fig. 11.1 Bone protection medication assessment
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Assessed Awaits DXA or referred to FLS or OS service Not assessed Not known
QEUHG (46)
RAH (72)
Raigmore
(56)
BGH (36)
Fife (1
05)
Ninewell
s (63
)
DGRI (38)
Wes
tern I
sles (
17)
GRI (61)
Inverc
lyde (
32)
Forth V
alley
(63)
Aberde
en (4
3)
Perth (
38)
Monkla
nds (
44)
RIE (1
39)
Ayr (34
)
Wish
aw (4
7)
Hairmyre
s (43
)
Crossh
ouse
(35)
Elgin (
29)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)
* Dual energy X-ray absorptiometry (DXA), Fracture Liaison Service (FLS), Osteoporosis Service (OS) Note that ‘awaits DXA or referred’ category may also include patients who had a bone protection assessment before leaving acute care.

MSk Audit — Hip Fracture Care Pathway — Report 2016
26
Recommendation: Every hospital should have systems in place to ensure that each patient with a hip fracture has a bone assessment carried out and relevant treatment started during their acute admission, or soon after discharge, aimed at reducing future fracture risk.
Standard 12: Every patient’s recovery should be optimised by a multi-disciplinary team approach so that they are discharged back to their original place of residence within 30 days from the date of admission.The main aim of the audit and improvement work is to get patients back to their original place of residence as rapidly as possible, with a level of mobility, function and independence which is acceptable to them, by optimising the pathway of care during their acute hospital stay.
The Scottish Hip Fracture Audit and Advisory Group plan to expand this aim to include the whole patient journey by developing standards to include: fracture prevention through services providing falls prevention programmes; management of osteoporosis and discharge management to rehabilitation units as well as to the community setting.
Median Length of Stay (LOS) in an acute hospital varies considerably. Nationally, if a patient is discharged home, median LOS is 11 days; to a care-home is 9 days and to a rehabilitation unit is 11 days. The median LOS for patients returning to care homes is shorter than for other patients at a number of hospitals. Although a shorter LOS can be a positive finding, it is important that these patients have the opportunity to receive the advice, care and support needed post-discharge to maximise recovery.
Fig 12.1 Median length of acute orthopaedic stay by discharge destination
0
5
10
15
20
25
Med
ian
LOS
To Home To Care Home To Rehab
Ayr (20
/5/7)
Crossh
ouse
(22/6
/6)
BGH (13/5
/17)
DGRI (12/8
/17)
Fife (3
2/20/4
4)
Forth V
alley
(9/9/
43)
Aberde
en (6
/5/28
)
Elgin (
9/4/15
)
GRI (28/1
3/12)
QEUHG (16/3
/24)
RAH (21/8
/31)
Inverc
lyde (
6/5/16
)
Raigmore
(17/9
/26)
Hairmyre
s (20
/7/12
)
Monkla
nds (
21/7/
16)
Wish
aw (1
4/8/18
)
RIE (3
4/24/6
8)
Ninewell
s (33
/11/18
)
Perth (
19/5/
13)
Wes
tern I
sles (
7//7)
All Site
s 12/1
3 (37
9/201
/638)
All Site
s 15/1
6 (35
9/162
/438)
Large symbols are based on samples of more than 5 patients, small symbols 3-5 patients; samples of 1-2 patients are not plotted. Actual sample sizes in brackets (Own home/Care home/Rehab). Medians reflect normal practise and compared to mean values are less likely to be influenced by a small number of patients with lengthy admissions as a result of specific medical problems.
Improvements in the interventions along the pathway have resulted in a reduced total LOS (acute and rehab settings) since the previous audit. The large variation between hospitals, with some having a median total LOS double those with the lowest LOS, is largely driven by the percentage of patients discharged straight back home/to a care home rather than on to a rehab setting.

MSk Audit — Hip Fracture Care Pathway — Report 2016
27
Figure 12.2 Median length of total hospital stay
0
10
20
30
40
50
60
Leng
th o
f sta
y (d
ays)
Median +/- 25 and 75 percentiles
Perth (
38)
Crossh
ouse
(35)
GRI (61)
Ninewell
s (62
)
Ayr (34
)
Monkla
nds (
44)
Fife (1
05)
Elgin (
29)
RAH (71)
Hairmyre
s (43
)
QEUHG (46)
Forth V
alley
(63)
Raigmore
(56)
BGH (34)
DGRI (38)
Inverc
lyde (
32)
Aberde
en (4
3)
Wish
aw (4
7)
RIE (1
39)
Wes
tern I
sles (
17)
All Site
s 12/1
3 (12
56)
All Site
s 15/1
6 (10
37)
Points represent the median length of total hospital stay (acute orthopaedic care, plus any subsequent rehabilitation or continuing NHS care). Lines extend to show the interquartile range (lower and upper values indicate the number of days within which a quarter and three-quarters of patients were discharged). Data includes patients who died during their acute orthopaedic stay.
More patients are discharged directly home or back to a care home now than in the previous audit, with a variation from 25% to 80% between hospitals.
Fig 12.3 Discharge destination
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Home/sheltered Care home Rehab Other * Died (in acute care)
Crossh
ouse
(35)
Ayr (34
)
Ninewell
s (63
)
Perth (
38)
Monkla
nds (
44)
Hairmyre
s (43
)
GRI (61)
Wes
tern I
sles (
17)
BGH (36)
QEUHG (46)
DGRI (38)
Elgin (
29)
Fife (1
05)
Raigmore
(56)
Wish
aw (4
7)
RAH (72)
RIE (1
39)
Inverc
lyde (
32)
Forth V
alley
(63)
Aberde
en (4
3)
All Site
s 12/1
3 (13
87)
All Site
s 15/1
6 (10
41)
* ‘Other’ includes those transferred to other acute medical wards, NHS Continuing Care or respite care, and those still in acute orthopaedic care at 120 days post-admission
Figures 12.4 to 12.6 show the percentage of patients back at their previous place of residence at 30 days. Since 2012/3 there has been an increase in the percentage of patients admitted from their own home who return there by 30 days from 42% to 58%. This represents the group of patients who may potentially lose their previous independence following a hip fracture.

MSk Audit — Hip Fracture Care Pathway — Report 2016
28
Fig 12.4 Percentage of patients admitted from home or a care home who were again resident there at 30 days post-admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Back in place of origin Not back
Monkla
nds (
41)
Forth V
alley
(61)
Ninewell
s (55
)
Perth (
38)
Ayr (33
)
Crossh
ouse
(34)
GRI (58)
BGH (33)
Hairmyre
s (43
)
QEUHG (45)
Raigmore
(56)
RAH (65)
Fife (9
8)
DGRI (37)
Inverc
lyde (
30)
Elgin (
27)
RIE (1
12)
Wish
aw (4
5)
Aberde
en (4
2)
Wes
tern I
sles (
16)
All Site
s 12/1
3 (11
01)
All Site
s 15/1
6 (78
2)
Includes patients who died within 30 days of admission.
Fig 12.5 Percentage of patients admitted from home who were again resident there at 30 days post-admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Home Not home
Ayr (27
)
Ninewell
s (44
)
Forth V
alley
(50)
Monkla
nds (
34)
Perth (
33)
BGH (26)
Crossh
ouse
(29)
GRI (42)
RAH (56)
QEUHG (37)
Hairmyre
s (35
)
Fife (7
2)
Raigmore
(45)
Inverc
lyde (
25)
DGRI (28)
Elgin (
23)
RIE (8
8)
Wish
aw (3
8)
Wes
tern I
sles (
16)
Aberde
en (3
4)
All Site
s 12/1
3 (86
8)
All Site
s 15/1
6 (78
2)
Home includes sheltered housing. Includes patients who died within 30 days of admission.
Fig 12.6 Percentage of patients admitted from a care home who were again resident there at 30 days post-admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Back in Care Home Not back in care home
Inverc
lyde (
5)
Monkla
nds (
7)
Raigmore
(11)
DGRI (9)
Hairmyre
s (8)
Forth V
alley
(11)
Perth (
5)
Elgin (
4)
QEUHG (8)
Ninewell
s (11
)
RIE (2
4)
Fife (2
6)
RAH (9)
Aberde
en (8
)
GRI (16)
Crossh
ouse
(5)
Wish
aw (7
)
Ayr (6)
BGH (7)
Wes
tern I
sles (
0)
All Site
s 12/1
3 (23
3)
All Site
s 15/1
6 (18
7)
Includes patients who died within 30 days of admission.

MSk Audit — Hip Fracture Care Pathway — Report 2016
29
Fig 12.7 Place of residence at 30 days post-admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
Perth (
38)
Ayr (34
)
Forth V
alley
(63)
Monkla
nds(4
4)
Crossh
ouse
(35)
Ninewell
s (63
)
BGH (36)
QEUHG (46)
RAH (72)
GRI (61)
Hairmyre
s (43
)
Raigmore
(56)
Inverc
lyde (
32)
Fife (1
05)
Wes
tern I
sles (
17)
Elgin (
29)
DGRI (38)
Wish
aw (4
7)
Aberde
en (4
3)
RIE (1
39)
All Site
s 12/1
3 (12
15)
All Site
s 15/1
6 (10
41)
Care home NHS Continuing Care/Other RehabilitationAcute hospital Still in acute orthopaedic care Died UnknownHome/sheltered
There has been an increase in the percentage of previously mobile patients who have returned to their pre-fracture level of mobility within four months of their hip fracture.
Fig 12.8 Mobility indoors at 120 days post-admission of patients admitted from home who walked unaccompanied with no aids or one aid prior to admission
0%
20%
40%
60%
80%
100%
Per
cent
age
of P
atie
nts
No aids, unaccompanied One aid, unaccompanied Two aids/frame,unaccompaniedRequires accompaniment Unable to walk
Monkla
nds (
25)
Ninewell
s (14
)
BGH (15)
Forth V
alley
(27)
QEUHG (17)
GRI (13)
Elgin (
8)
RAH (32)
Wes
tern I
sles (
9)
Perth (
11)
Inverc
lyde (
15)
Aberde
en (1
1)
Ayr (9)
RIE (5
7)
Crossh
ouse
(12)
Raigmore
(30)
Fife (1
8)
DGRI (22)
Wish
aw (1
8)
Hairmyre
s (23
)
All Site
s 12/1
3 (52
4)
All Site
s 15/1
6 (38
6)
Excludes patients who died within 120 days (10%) or could not be contacted (17%). The percentage who could not be contacted is higher in 2015/16 than in 2012/13 (8%).

MSk Audit — Hip Fracture Care Pathway — Report 2016
30
The readmission rate is an important measure of the quality of the hip fracture care pathway and the discharge process. There has been no change in the national rate but there is a considerable variation between hospitals.
Fig 12.9 Percentage of patients who were readmitted within 14 days of hospital discharge
0%
5%
10%
15%
20%
25%
30%
Per
cent
age
of P
atie
nts
Re-admitted within 14 days of hospital discharge Not re-admitted within 14 days
Raigmore
(48)
Elgin (
22)
BGH (27)
DGRI (31)
Fife (8
6)
Perth (
35)
Wish
aw (4
2)
Ninewell
s (56
)
RAH (60)
Inverc
lyde (
24)
Crossh
ouse
(33)
RIE (1
07)
Forth V
alley
(55)
Aberde
en (3
5)
Hairmyre
s (38
)
Wes
tern I
sles (
13)
Monkla
nds (
41)
QEUHG (39)
Ayr (31
)
GRI (49)
All Site
s 12/1
3 (90
3)
All Site
s 15/1
6 (87
2)
Overall Recommendation: Hospitals are encouraged to use all of the measures in this audit to focus improvement on the patient journey to meet the Scottish Standards of Care for Patients with a Hip Fracture and therefore impact positively on patient length of stay and successful and rapid return to their previous residence. Further analysis to understand variation in discharge delay reason is being undertaken.
All hospitals should begin discharge planning as soon as the patient is admitted, early communication with primary care agencies such as social work would facilitate the early and safe discharge of patients following surgery for hip fracture.

MSk Audit — Hip Fracture Care Pathway — Report 2016
31
Appendices
A - DemographicsThe median age of hip fracture patients audited was 82 years (80.3 in 2012/13 audit). 26% of patients were under 75 years old, 15% were over 90. 73% of patients were female.
75% of patients who suffered a hip fracture lived at home immediately prior to the fracture. 18% lived in a care home. A further 6% fell whilst in hospital (acute, rehab or continuing care). Of those who lived at home prior to fracture, 65% lived independently whilst 13% lived with carers. 5% had a carer but not every day, 4% had a carer once a day and 13% more than once per day.
Prior to hip fracture 50% of patients walked unaccompanied and without aids whilst walking indoors. 17% used single sticks or other aids, and 22% walked with two or more aids or a frame but were otherwise unaccompanied indoors. 10% of patients required accompaniment whilst walking indoors, and 1.4% were chair- or bed-bound.
63% of this sample of hip fracture patients had documented significant co-morbidities. 19% had two co-morbidities and 5% three or more co-morbidities. Dementia was not included as a co-morbidity as such, but affected 26% of all patients.
For patients with a documented and clear history, 30% had fallen at least once in the previous six months. 18% had fallen more than once. 7% of all patients had a documented previous hip fracture, and 7% a previous wrist fracture.
Six (0.6%) fractures were pathological fractures.
B - Scottish Hip Fracture Audit and Advisory Group Membership & Contacts
Name Role Organisation EmailGraeme Holt
Chairman, Consultant orthopaedic surgeon
NHS, Ayrshire and Arran
Kirsty Ward
National Clinical Coordinator, MSk Audit
National Services Scotland, ISD
Karen Adam
National Clinical Improvement Advisor
Scottish Government [email protected]
Kate James
National Programme Lead T&O
Scottish Government [email protected]
Rik Smith Senior analyst, MSk audit
National Services Scotland, ISD
Jon Antrobus
Consultant Anaesthetist NHS Borders [email protected]
Lucy McCracken
Consultant, Medicine for the Elderly
NHS Glasgow and Clyde
Kathleen Ferguson
Consultant anaesthetist NHS Grampian [email protected]
Mayrine Fraser
National Development Manager/Specialist
Nurse
National Osteoporosis Society

MSk Audit — Hip Fracture Care Pathway — Report 2016
32
Name Role Organisation EmailStephen Gallacher
Consultant Physician NHS Glasgow & Clyde
Rashid Abu-Rajab
Consultant orthopaedic surgeon
NHS Glasgow and Clyde
Krishna Murthy
Consultant Emergency Medicine
NHS Lothian [email protected]
Ruth Houson
Advanced nurse practitioner
NHS Ayrshire and Arran
Ann Murray
Falls programme manager
NHS Ayrshire and Arran
Ann-Marie Owens
Trauma Liason Nurse
NHS Glasgow and Clyde
Angela Stuart
Advanced nurse practitioner
NHS Ayrshire and Arran
Hazel Dodds
Senior Nurse, Scottish Healthcare Audits
National Services Scotland, ISD
Ann Murdoch
Senior Social Worker NHS Lothian [email protected]
Catherine Nivison
Chief Allied Health Professional
NHS Glasgow and Clyde
Fiona Graham
GP in orthopaedic rehabilitation
NHS Dumfries and Galloway
Seng Wong
Foundation Doctor NHS Tayside [email protected]
Lesley Holdsworth
eHealth Clinical Lead Hip Fracture Best
Practice Guidance Lead
Scottish Government Chartered Society of
Physiotherapy
Leanne Knox
Care of the Elderly Nurse Practitioner
NHS Glasgow and Clyde
Karen Goudie
National Clinic Lead, Older People’s Care
Healthcare Improvement Scotland
AcknowledgementsThis report could not have been prepared without the dedicated work of the Local Audit Coordinators who tirelessly collected and validated this information as well as providing an
essential link role between audit and clinical staff.

MSk Audit — Hip Fracture Care Pathway — Report 2016
33
C - References1. The Scottish Government (2016) A National Clinical Strategy for Scotland. Available here
http://www.gov.scot/Resource/0049/00494144.pdf
2. The MSk Audit
3. Scottish Intercollegiate Network (SIGN). (June 2002) Prevention and Management of Hip Fracture in Older People, SIGN 56
4. Scottish Intercollegiate Network (SIGN). (June 2009) Management of Hip Fracture in Older People, SIGN 111
5. Musculoskeletal Audit (ISD) on behalf of the Scottish Government (2013) ‘Audit of care pathways for hip fracture patients in Scotland (December 2012 to March 2013)’. Available at http://www.msk.scot.nhs.uk/reports/main.html
6. Scottish Government (2014) Scottish Standards for Care of Hip Fracture Patients. Available here Hip Fracture Care Pathway
7. MSK & orthopaedics quality drive
8. Scottish Government (2011) 2020 Vision
9. National Hip Fracture Database http://www.nhfd.co.uk/
10. National Institute for Clinical Excellence (NICE) Clinical guideline 124 (2011) ‘Hip fractures. The Management of Hip Fracture in Adults.’ Available at http://guidance.nice.org.uk/CG124/NICEGuidance/pdf/English
11. Healthcare Improvement Scotland (2014) Improving Care for Older People: Delirium Toolkit.

MSk Audit — Hip Fracture Care Pathway — Report 2016
34
D - Access to the Trauma and Orthopaedic DashboardAudit data is routinely updated on this web based platform each month and is provided for multi-disciplinary teams to measure and monitor the sustainability of their improvement actions. To become an approved user of the Trauma & Orthopaedic Portal please go to NSS User Access System.
For help with registration please go to http://www.isdscotland.org/Products-and-Services/Datamarts/User-Support/
If you have any issues or questions please contact the team at: [email protected]

MSk Audit — Hip Fracture Care Pathway — Report 2016
35

shfa.scot.nhs.uk