musculoskeletal chest pain in patients with stable angina ... · thoracic angina identified by case...
TRANSCRIPT

Musculoskeletal chest pain in patientswith stable angina pectoris –
diagnosis and treatment
Ph.D. Thesis
Henrik Wulff Christensen
Faculty of Health Sciences
University of Southern Denmark
Department of Clinical Physiology and Nuclear Medicine, Odense University Hospital
2004
Musculoskeletal chest pain in patientswith stable angina pectoris –
diagnosis and treatment
Ph.D. Thesis
Henrik Wulff Christensen
Faculty of Health SciencesUniversity of Southern Denmark
Department of Clinical Physiology and Nuclear Medicine, Odense University Hospital2004

2
The thesis is based on the following 4 part projects:
Part project IChristensen HW, Vach W, Vach K, Manniche C, Haghfelt T, Hartvigsen L, Høilund-Carlsen PF.Palpation of the upper thoracic spine: an observer reliability study. J Manipulative Physiol Ther2002;25(5):285-292.
Part project IIChristensen HW, Vach W, Manniche C, Haghfelt T, Hartvigsen L, Høilund-Carlsen PF. Palpationfor muscular tenderness in the anterior chest wall: an observer reliability study. J ManipulativePhysiol Ther 2003;26(8):469-475.
Part project IIIChristensen HW, Vach W, Gichangi A, Manniche C, Haghfelt T, Høilund-Carlsen PF. Cervico-thoracic angina identified by case history and palpation findings in patients with stable anginapectoris (submitted).
Part project IVChristensen HW, Vach W, Gichangi A, Manniche C, Haghfelt T, Høilund-Carlsen PF. Manualtherapy for patients with stable angina pectoris (submitted).
The articles and manuscripts are reprinted in the appendix. The roman numerals are used for referralin the body of the text.
Supervisors: Professor, consultant, DMSc Poul Flemming Høilund-Carlsen, Department ofClincal Physiology and Nuclear Medicine, Odense University Hospital, Denmark.Professor, consultant, DMSc Torben Haghfelt, Department of Cardiology, OdenseUniversity Hospital, Denmark.Professor, consultant, DMSc Claus Manniche, The Back Research Center, Fynen,Denmark.
Examiners: Chiropractor, Professor, Ph.D. Gert Brønfort, Northwestern Health SciencesUniversity, Minnesota, USA.Consultant, DMSc, Ph.D. Hans Erik Bøtker, Department of Cardiology, SkejbyHospital, Denmark.Professor, DMSc Peter Junker, Internal Medicine: Rheumatology, ClinicalInstitute, University of Southern Denmark, Denmark.

3
PREFACE
This thesis is based on studies performed while I was enrolled as a PhD student at the Faculty ofClinical Science, Department of Clinical Physiology and Nuclear Medicine, University of SouthernDenmark. I wish to thank my co-workers and everyone who helped me making this thesis possible.In particular I wish to express my gratitude to:Poul Flemming Høilund-Carlsen, my principal supervisor, for the numerous hours, patient attitude,inspiring discussions, enthusiasm, intellect and his passion for the writing. He has been my truementor. Torben Haghfelt, newer failing support and the unbiased approach toward my interest forchest pain from the musculoskeletal system. Claus Manniche, for support and constructiveguidance. Werner Vach for his open-minded, constructive and systematic approach to making thenumbers talks. I am grateful for his supervision in the statistical analysis. Anthony Gichangi for hisassistance with data management and data analysis. Mette Møldrup for her ability to organizepatient logistic and patient records. Her constant support and never fading help with the presentstudy. Annette Albæk for her patient attitude and never failing help. Jan Hartvigsen for his support,inspiration and tolerance. Kristian Græsborg and the staff at the Nordic Institute of Chiropracticand Clinical Biomechanics for their permanent support of my work.Lisbet Hartvigsen for participating and helping with the planning of part projects I and II. RoniEvans for help with proofreading the manuscripts. My chiropractic partners Per Mortensen andPeter Højgaard, for their continuous support and tolerance in my reduced hours as practicingchiropractor.Secretaries Anne-Marie Møller and Bente Wichmann, Department of Cardiology, and laboratorytechnicians of the “Heart Group”, phycicians, laboratory technicians Karina Madsen and TinaGodskesen, Department of Clinical Physiology and Nuclear Medicine.Financial assistance was provided by: The Foundation for Chiropractic Research and PostgraduateEducation, Nordic Institute of Chiropractic and Clinical Biomechanics and University of SouthernDenmark, Odense.To all the patients, who willingly participated in the studyLast but not least, I thank my family and my fiancée Susanne for their kind-hearted support andencouragement.
4
TABLE OF CONTENTS
1. Abbreviations 5
2. Definitions 6
3. Introduction 8
3.1 Objective/aim
3.2 Background
3.2.1 Angina pectoris
3.2.2 Aetiology of chest pain
3.2.3 The musculoskeletal system – palpation and manual therapy
4. Material and methods 12
4.1 Study population
4.2 Pain assessment
4.3 Quality of life questionnaire
4.4 Clinical examination including palpation methods
4.5 Manual therapy
4.6 Myocardial perfusion imaging
4.7 Coronary angiography
4.8 Statistics
5. Results 17
6. Discussion 21
7. Conclusions 26
8. Perspectives 27
9. Summary in English 28
10. Summary in Danish 29
11. References 30
12. Appendix 38
Part project I - Reprint from J Manipulative Physiol Ther 2002;25(5):285-292.
Part project II - Reprint from J Manipulative Physiol Ther 2003;26(8):469-475.
Part project III - Submitted
Part project IV - Submitted

5
1. ABBREVIATIONS
AP = Angina pectoris
CAG = Coronary angiography
CCS = Canadian Cardiovascular Society
CTA = Cervico-thoracic angina
HVLA = High velocity low amplitude
MILES = Myocardial Ischemic Logistics Evaluation Study
MPI = Myocardial perfusion imaging
MP = Motion palpation
NCA = Normal coronary anatomy
ROM = Range of motion

6
2. DEFINITIONS
Angina pectorisEugene Braunwald: clinical syndrome characterized by discomfort in the chest, jaw, shoulder, backor arm. It is typically aggravated by exertion or emotional stress and relieved by rest ornitroglycerin.(1)
Danish Society of Cardiology and Danish Society of Thoracic Surgery:(2)
a) Pain/discomfort in the chest wall, eventually radiating to the neck, jaw, upper extremity or the back, lasting a few minutes up to 10-15 minutes.b) The pain/discomfort is provoked by cold, physical or psychological stress.c) The pain/discomfort is normally relieved by rest or nitroglycerin.
Typical angina pectoris: a+b+c.Atypical angina pectoris: a+b or b+c or a+c.Noncardiac chest pain: a or b or c.
Joint range of motion
Figure 1. This diagram represents joint motion in one plane starting from neutral position. Joint- play occursin the neutral position, followed by active and passive ranges of motion (ROM). The passive ROM goesbeyond the active ROM entering the joint´s elastic barrier. End-play is evaluated at the end of passive ROM.Beyond the anatomical limit, trauma results.
PalpationMotion palpation: Variable manual pressure performed during active or passive joint
movements and additionally involves evaluation of accessory jointmovements.(3)
Prone motion palpation: Manual pressure and joint evaluation performed in the neutral jointposition to evaluate joint play.(3)
Sitting motion palpation: Manual pressure and joint evaluation performed at the end of passiverange of motion of the joint to evaluated end play.(3)
Tenderness evaluation: A flat digital index contact with a standardized pressure used formanualpalpation. Patient should indicate the presence of tendernessverbally.

7
Manual therapyManual procedures in which the hands of the treating person are used with the purpose ofinfluencing the soft tissue directly or the tissues around a joint. They aim at restoring pain-free jointmovement.
High velocity low amplitude spinal manipulation: Manual procedure using a short lever with amanual thrust of low amplitude and high velocity, directed toward a specific vertebral segment.

8
3. INTRODUCTION
The musculoskeletal system is recognized as a possible source of pain in patients with chestdiscomfort.(1;4-7) However, a confident diagnosis of musculoskeletal chest pain can be difficult toestablish since no gold standard exists to verify this diagnosis. Normally, patients suspected ofhaving angina pectoris (AP) are admitted to a cardiology ward because the heart, i.e., myocardialischemia, is under suspicion as the pain source, but the aetiology of pain may be non-cardiac in upto 50 % of cases.(8) The differential diagnoses are of primarily pulmonary, gastrointestinal,psychosocial, or musculoskeletal origin.(1;7;9-15) Furthermore, up to 30% of all patients catheterizedfor the investigation of chest pain have normal coronary anatomy (NCA).(7) These patients have aexcellent prognosis for survival and a future risk of cardiac morbidity similar to that reported in thebackground population.(16;17) As a consequence, it may sometimes seem expedient to reassure andthen discharge these patients.(7) However, about three quarters of the patients continue to sufferfrom residual chest pain with large socio-economic consequences.(7;18-21) Therefore, a search shouldbe made for an alternative cause with related possibilities of treatment.
Given these perspectives the general objective of the present work was to study the diagnosisand treatment of chest pain originating from the musculoskeletal system of the spine and thorax inpatients with chest pain due to known or suspected AP. The project comprised of four part projects:two methodological (I and II) and two clinical ones (III and IV).
3.1 Objectives
The specific aims were:1) To assess the interobserver reliability and the intraobserver reliability with three palpation
procedures for the detection of spinal biomechanical dysfunction and paraspinal tendernessin the upper eight segments of the thoracic spine (part project I).
2) To assess the interobserver reliability and the intraobserver reliability of palpation formuscular tenderness in the anterior chest wall (part project II).
3) To use preferred palpation procedures to obtain a diagnostic tool for early identification ofcervico-thoracic angina (CTA) in the clinical setting (part project III).
4) To investigate and describe the decision making process of an experienced chiropractor indiagnosing non-cardiac musculoskeletal chest pain in the shape CTA, based on patienthistory and clinical examination (part project III).
5) To validate the CTA diagnosis (part project III).6) To elucidate in an open clinical trial if patients with a diagnosis of CTA would benefit from
manual therapy as compared to CTA negative patients (part project IV).
It was not the purpose to describe the mechanism of chest pain and AP in detail, as it was not theobjective to describe in particular the theoretical and biomechanical rationale for the manualtherapy applied. Nor was it an aim to describe the diagnosis and treatment of other non-cardiacchest pain aetiologies (e.g., the gastrointestinal system or psychosocial). This study was pragmaticin its clinical approach to the diagnosis and treatment of chest pain from the musculoskeletal systemin terms of biomechanical dysfunction of the spine and/or muscular tenderness in muscles of thethorax.
3.2 Background
3.2.1 Angina pectorisFrom the historical review by P. Procacci on cardiac pain(22) the first term that was found for cardiacpain was passio cardiaca propria used by Caelius Aurelianus, a fifth-century Roman Physician.During the Middle Ages several scientists mentioned pain in the chest referred to the heart.Heberden introduced the term AP in 1768 in a lecture to the Royal College of Physicians of London

9
to designate a very distinctive “disorder of the breast” with “a sense of strangling and anxiety”. Theword has probably been adopted from the similarity of the symptoms to those of the inflammatorydiseases of the throat, accompanied by a feeling of choking and strangling, for which ancient Greekand Latin writers used the term angina. Heberden differentiated between AP and other forms ofchest pain, which were assembled under the heading of “dolor pectoris”. (22)
Today, AP is defined as “a clinical syndrome characterized by discomfort in the chest, jaw,shoulder, back, or arm. It is typically aggravated by exertion or emotional stress and relieved bynitroglycerin”.(23) In the present thesis, the word typical AP is reserved for chest pain presumablycaused by myocardial ischemia.
3.2.2 Aetiology of chest painElucidation of the cause of chest pain is a challenge to a variety of clinicians. Although chest pain isone of the cardinal manifestations of heart disease end especially ischemic disease, it is important torecognize that such pain may originate not only from the heart, but also in:
a) a variety of intrathoracic structures, such as the aorta, pleura, oesophagus, and diaphragm,b) tissues of the neck or thoracic wall, including the skin, thoracic muscles, cervicothoracic
spine, costochondral junctions, breasts, sensory nerves,c) subdiaphragmatic organs such as stomach, duodenum and gallbladder.(1)
Pain of psychosocial origin may also exist.(9)
Because of this variety of areas of reference, different kinds of pain may exist in the samearea. Pain from the heart, oesophagus, stomach, etc. is visceral in type, whereas somatic pain refersto pain from the musculoskeletal structures, dermal tissues, and the coverings of major organs. Thedepth of the tissue in somatic pain tends to determine if it is superficial somatic (skin, tendonsheaths, periosteum, superficial fasciae) or deep somatic (muscle, fasciae, tendons, joint capsules,ligaments, periosteum).(24)
Mechanism of cardiac chest painCardiac pain is transmitted by afferent sympathetic nerve fibers and vagal nerve fibers.(24) Thisvisceral type of pain is mediated by free nerve endings that have receptors located in the mucosa,muscle, and serosa of the heart and can be stimulated chemically or mechanically.(32-34) Thesympathetic nerves have cell bodies in the dorsal root ganglia and synapse on the interneurons inthe dorsal horn of the spinal cord. Interneurons that receive visceral pain are called viscerosomaticneurons. They also receive somatic afferent input from skin, tendons, and muscles. The visceralpain from the heart is transmitted via the 4-5 upper thoracic spinal segments as well as somecervical segments. The sensory impulses from the viscera of the thorax and from the body wall(muscles, skin, joints), however, share the same spinal segments, making the differentiation ofcauses and diagnosis of chest pain difficult in many cases.(35;36) The convergence of visceral andsomatic pain fibers on the same interneurons in the spinal cord might explain why visceral pain isoften referred, i.e., why it is often perceived in somatic areas remote from the involved organ.
Therefore, pain arising from different organs, such as the chest wall, esophagus, or the heartmay be indistinguishable as may pain arising from the spine.(36) The ascending pathways to thebrain project through the anterolateral system of the spinal cord to the medulla, midbrain, andthalamus. In the medulla, visceral pain pathways interact with the reticular formation, mediatingarousal and autonomic responses to pain. In the midbrain, projections to the periaqueductal graymatter are important for descending modulation. From the thalamus, visceral pain input is relayed toareas of the cortex, as demonstrated in man using positron emission tomography, where it isdecoded as a painful sensation.(37)
Mechanism of chest pain from the musculoskeletal systemSensory receptors in musculoskeletal structures are characterized by an ability to respond to aparticular stimulus with a relative insensitivity to certain other stimuli. Nociceptors are sensitive tostimuli that are potential noxious. Mechanical, chemical and thermal stimuli may cause nociception.

10
The nociceptors can be sensitized by a wide variety of mechanisms, which can lower the thresholdfrom nociceptive stimuli and make it possible for non-nociceptive stimuli to be registered as painproducing stimuli. The pain impulses are mediated by afferent nerve fibers linking the peripheralnociceptor with the spinal cord. The primary afferent enters the dorsal horn of the spinal cord andsynapses with second order neurons.(38) The ascending ways have been described previously.
Different musculoskeletal structures of the spinal region are recognized as pain producing inhumans. Kellgren outlined the distribution of pain from ligaments, which was different from thewell-known dermatomes. He found that fascia, periosteum and tendons give rise to pain ofsegmental distribution.(39) Inman and Saunders introduced the concept of “sclerotomes” for this typeof pain distribution.(40) Feinstein outlined the distribution for pain and tenderness when theinterspinous ligament is irritated. Several spinal segments referred pain to the anterior chest wall.(41)
Further, the thoracic zygapophyseal joints at segments T3-T9 can cause intense areas of provokedpain one segment inferiorly and slightly lateral to the joint injected and similar pain referred towardthe anterior chest wall.(42) Large and more recent studies of the mechanisms do not exist.
Chest pain and normal angiographyCoronary angiography (CAG) is used to evaluate patients with chest pain suspected of having AP,because the heart, i.e., arteriosclerotic lesions in the epicardial arteries, is under suspicion as thereason for their chest pain. A large proportion of these patients receiving CAG are shown to havenormal anatomy. These negative clinical investigations and authoritative reassurance by acardiologist is not always effective for these patients. Those patients who continue to experiencesymptoms want an explanation which can assure them that they do not have a serious medicalproblem, and a piece of useful advice about how to return to a full life.(25) This could probably beprovided by addressing patients’ fear of being heart diseased and more reassuring about the heartdespite negative CAG,(26;27) and, finally, more consideration of the non-cardiac disorders and thepossible treatment regimes of the persistent pain.(5;6;26;28;29) Further, among patients with angina andNCA other specific heart diseases may exist, e.g., spasm of the epicardial vessels, valvular diseases,pericardial diseases or cardiomyopathy. Still others are believed to have compromisedmicrocirculation in the cardiac muscle in the form of microvascular disease (angina) or SyndromeX. This term is reserved for a group of patients who have NCA and, exercise-inducedelectrocardiographic changes indicative of cardiac ischemia.(30;31)
Cervical anginaCervical angina, mimicking chest pain of cardiac ischemia, has been described by different authorsin the past 70 years(43-48) as being caused by various skeletal conditions, e.g., cervical discopathyand thoracic outlet syndrome (pain thought to be caused by compression of nerves and vessels tothe upper extremity). Cervical angina has lately been defined as chest pain that resembles truecardiac angina but originates from cervical discopathy with nerve root compression.(49) Thepathogenesis of cervical angina can be explained by the fact that cervical neural roots from C4 toC8 contribute to the sensory and motor innervations of the anterior chest wall.(50)
Other non-cardiac chest pain conditionsGastro-oesophageal reflux disease, oesophageal motility disorders, and oesophageal spasm have allbeen coupled with chest pain as differential diagnoses.(1;51) Despite a high incidence ofosesophageal abnormalities in patients with chest pain and NCA, a causative link is only found in asmall proportion.(52-54)
Some investigators have reported that patients with chest pain and NCA score higher onpsychological measures such as neuroticism and anxiety, than do patients with chest pain andischemic heart disease.(55) Others have been unable to find such differences,(56) although abnormalcardiac perception in patients with NCA(57) and differences between patients with NCA andischemic heart disease in sensitivity to experimental pain stimuli have been reported.(57;58) A morerecent study found higher scores on various psychosocial measures in both chest pain groups and

11
that they were related to their pain, rather than being the cause of pain, and did not support apsychogenic explanation for chest pain in the presence of NCA.(59) The results of the mentionedstudies are inconsistent.
3.2.3 The musculoskeletal system – palpation and manual therapyMotion palpation of human joints is recognized as an essential skill by manual medicine disciplinesand is used extensively by chiropractors,(3) physical therapists,(60) osteopaths,(61) and some medicaldoctors(62) in clinical practice to diagnose mechanical dysfunctions suitable for spinal manipulation.
However, in a recent study it has been shown that motion palpation in terms of end-playassessment does not in and of itself contribute to relief of neck pain and neck stiffness after spinalmanipulation in neck pain patients.(63) Uptil now, palpation research has focused on the assessmentof the reliability of different palpation procedures. Five systematic reviews have been published andare consistent in their conclusions regarding agreement on the detection of segmental motionrestriction in the spine. Poor interexaminer reliability for motion palpation was found throughoutthe spine (κ<0.2), whereas intraexaminer reliability appeared to be moderate (κ: 0.4-0.6).(64-67) 68)
Only two studies on the thoracic spine has been identified. The validity of motion palpation hasbeen examined indirectly by the use of mechanical models: Moderate sensitivity was demonstrated(0.48-0.54) for identifying segmental motion restriction(69) and further that therapists can gradespinal stiffness to identify spinal endplay restriction in clinical practice.(70) Additionally, there isindirect evidence of motion palpation validity from a study which showed that examiners candistinguish endplay improvement following manipulation(71) and another study in whichzygapophysial joint injections were used to verify the identification of segmental spinal dysfunctionin the neck.(72)
Manual therapy as a treatment option for mechanical pain conditions of low back and neckpain conditions is well recognized within different manual medicine disciplines.(3;60-62) Theevidence of the effectiveness of spinal manipulation for neck pain has been suggested in threesystematic reviews.(73-75) A recent meta-analysis of 26 randomized clinical trials evaluating spinalmanipulation for acute and chronic back pain concluded also that manual therapy was effective.(76)
The evidence for the effectiveness of spinal manipulation for thoracic spine pain is, however,limited. In a small controlled clinical trial on the use of spinal manipulation for the treatment ofthoracic spinal pain, to subjects without chest pain there was significant reduction in pain on anumerical pain rating scale, but no reduction on a disability index.(77) No previous study hasevaluated the effect of manual therapy in patients with chest pain of musculoskeletal origin.

12
4. MATERIALS AND METHODS
4.1 Study population
I and IIIn total, 107 subjects were scheduled to take part in the study. Of these, 51 were patients referredconsecutively to the Department of Cardiology because of known or suspected stable AP. Theremaining 56 were control subjects recruited from the Department of Nuclear Medicine andfulfilling the following criteria: a history without heart disease, a normal resting electrocardiogram,and no chest pain.
III and IVThis study was conducted as a substudy of the Myocardial Ischemic Logistic Evaluation Study(MILES), (8) the objective of which was to compare the results of MPI and CAG in a prospectiveseries of patients referred from General Practitioners or local hospitals to Odense UniversityHospital for CAG because of known or suspected stable AP. A total of 516 out of 972 consecutivepatients were included in the MILES study. Of the 516 patients, 275 were included in the present.The rest, 241 fulfilling ≥1 of a series of predefined exclusion criteria, were not included (Table 1).The local ethic committee approved the study. Informed consent was obtained from all personsparticipating.
Table 1. Exclusion criteria in the study and their frequencies in 241 patients. Note that some patients fulfilled several criteria.
No. of pts.
Lack of compliance (withdrawal prior to program) 89
No written consent 49
Previous surgery to the thorax 32
No selfreported chest pain, neck pain or thoracic spinal pain 26
Inflammatory joint disease 18
Malignant disease 18
Apoplexia 14
Others 13
4.2 Pain assessment
Within the field of cardiology is has been common to classify the type of chest pain into threecategories in line with Danish guidelines(2) adopted from Diamond(78): typical angina, atypicalangina, or non-cardiac chest pain, and the severity into four classes given by the CanadianCardiovascular Society (CCS, grade 1-4).(79) However, there has been no tradition for recording ofthe patient´s subjective feeling of pain intensity by the use of uni-dimensional scales (verbal ratingscales, numerical rating scale, visual analogue scale or 11-point box scale).(80)
No single method can objectively record the pain intensity the individual experiences,nevertheless, in an attempt to systematically register the intensity of chest pain we choose to use abox scale.
This 11- point box scale has been used extensively, among others for measurement of backpain(81) and neck pain.(82) The intensity of pain was graded from 0 to 10, indicating minimal andmaximal intensity, respectively. We used this approach to grade the patient´s chest pain “now” (i.e.,on the day of examination), together with the following types of pain experienced during the lastfortnight: maximal and average chest pain, average thoracic spine pain, average cervical spine pain,

13
and average shoulder arm pain. All pain measures were repeated at 4 week follow-up. Pain wastreated as a binary variable (pain=0 and pain>0) and ordered (pain intensity).
4.3 Quality of life questionnaire
Patients assessed their quality of life using the SF-36 health survey(83) at baseline and at 4 weeks.The SF-36 comprises 36 items that can be combined into the following eight multi-item summaryscores: physical functioning (ten items), vitality (four items), bodily pain (two items), mental health(five items), social functioning (two items), role limitation due to physical health (four items) anddue to emotional problems (three items) and general health perceptions (five items), plus one itemassessing a change in health over the past year. Each summary score is obtained by simple un-weighted summation of item scores and is then scaled from 0 to 100, with 0 and 100 indicating“worst” and “best” possible health, respectively. Higher scores indicated better perceived health.The SF-36 has been recommended and used for AP patients(84-87) and been validated in a Danishsetting(88) and will have the same interpretation across countries.(89)
4.4 Clinical examination
The same examiner, who used standardized questions on prefabricated sheets, interviewed patientsthroughout the study. This was done to ensure consistency and exactly the same amount ofinformation about all patients. There were questions on factors and events related to ischemic heartdisease. The chest pain was described, with regard to duration, location, and provoking andrelieving factors. Specific questions were asked about symptomatology of the lungs andgastrointestinal system, the past medical history and consumption of medicine. All questions had tobe answered by ‘yes’ or ‘no’ or via predefined categories. Patients were classified according to typeof angina and CCS. Next, patients had their height and weight measured, blood pressure and pulserecorded, heart and lung stethoscophy performed, abdominal palpation and auscultation, neckauscultation, clinical signs of left ventricular failure were noted. Neurological examination of upperand lower extremities in terms of reflexes, sensibility to touch and vibration, muscle strength aswell as orthopaedic examination of the neck and shoulder joints was performed to rule out nerveroot compression syndromes.
Finally, a standardized manual examination of the neck and thoracic spine and chest wall wascarried out. See I, II and III for details. This examination program together with the detailed casehistory was applied by the experienced chiropractor to the population of AP patients to make adiagnose of CTA.
Four types of palpation was carried out:
1. Sitting manual palpation for muscular tenderness on 14 points of the anterior chest wall (figure 2) (study II – IV).
2. Prone manual palpation for paraspinal muscular tenderness segmentally (Th1-8) (figure 3) (study I, III and IV).3. Prone motion palpation (MP) for joint-play restriction segmentally (Th1-8) (figure 1+4) (study I, III and IV).4. Sitting MP for end-play restriction in lateral flexion and rotation segmentally of the cervical (C4-7) and thoracic spine (Th1-8) (figure 1+5) (study I, III and IV).

14
Figure 2. Illustration of the 14 points of the ant- Figure 3. Illustration of the points used forerior chest wall evaluated for muscular tenderness. paraspinal evaluation of muscular tenderness.
Figure 4. Motion palpation for joint-play. Figure 5. Motion palpation for end-play.
4.5 Manual therapy
All CTA positive patients received eight treatment sessions during four weeks by the samechiropractor. Each participant got at least one spinal manipulation at each session according tomotion palpation findings. Trigger point therapy intervention followed clinical practice, in whichthe choice of initial and subsequent therapy is decided by the treating chiropractor. Not all patientsgot trigger point therapy. Participants in the CTA negative group were interviewed and informedabout the CTA diagnosis by the chiropractor and underwent the same examination program of themusculoskeletal system, but received no therapy.

15
Spinal manipulationSpinal manipulation was delivered to the restricted or hypomobile joints of the spine. High-velocityand low-amplitude (HVLA) spinal manipulation directed at one or more restricted cervical and/orthoracic joint segments (figure 6), as described by Bergmann et al.(90) When this study was planned,there was some evidence that HVLA spinal manipulation was efficacy in the treatment of patientswith low back pain and neck pain.(91)
Figure 6. High velocity low amplitude spinal manipulation of the thoracic spine.
Trigger point therapyTrigger point therapy intervention followed clinical practice, in which the choice of initial andsubsequent trigger point therapy is decided by the treating chiropractor. The pectoralis major andminor muscles and the intercostal muscles were examined and trigger points were located. Manualpressure as trigger point pressure release and deep stroking massage on the different trigger points,were used ad modum Travell & Simons.(92)
4.6 Myocardial perfusion imaging
This non-invasive test is designed to evaluate regional myocardial perfusion under rest and stressconditions. It involves the injection of a radiolabelled substance, which is extracted by themyocardium and accumulates in proportion to myocardial blood flow. Such substances are injectedunder stress as well as resting conditions, and images are obtained to define the regional distributionof radioactivity within the myocardium. Based on this information stress images were comparedwith the rest images. Defects that were present at rest and remained unchanged during stress wereconsidered as fixed defects. The appearance of new or worsening defects following stress wasconsidered to be defect reversibility.
Gated single photon emission computed tomographic imaging was performed using asequential same-day rest thallium-201/stress technetium-99m sestamibi dual-isotope protocol aspreviously described by Berman and coworkers.(93) Standard procedures for image interpretationincluded review of all scans by two experienced observers who were blinded to clinical history,physical examination data, and the result of coronary angiography. Final and overall imageinterpretation was achieved by consensus.

16
4.7 Coronary angiography
Selective CAG is invasive and was performed ad modum Judgkin according to the routine of thecardiology department.(94) The results were interpreted by the physicians on duty in thecatheterization laboratory and, if necessary, reviewed and corrected at the Heart Conference of theDepartment of Cardiology. For the purpose of this study, significant coronary stenoses were thosewith ≥50% luminal diameter narrowing of an epicardial coronary artery.
4.8 Statistics
Agreement within and between observers was expressed as absolute agreement and by means of theKappa statistic. Two rates of agreement were computed: one for ”strict agreement” (I and II) andanother for ”expanded agreement” (I).
Descriptive statistics were applied using percentages for discrete variables and means andstandard deviations for continuous variables. The statistical analysis included also usage of standardnon-parametric statistical methods. Comparisons were performed by tests such as Mann-Whitney,McNemar, Wilcoxon and Fisher’s exact test. Odds ratios (OR) were used to quantify associations.Quality of life scores were standardized for each patient by subtracting the corresponding age andsex specific mean in the Danish population.
In the analysis of the clinical decision of CTA classification (III), initial comparisons ofcandidate variables were done. Many of the variables were correlated and it was therefore difficultto judge the role of each single variable in the decision process. To obtain further insight we tried toreconstruct the clinical decision process by selecting serially variables with nearly uniquediscriminating power in the sense that they allowed us to define a subgroup with almost exclusivelyCTA positive or CTA negative diagnoses. In the absence of such variables we selected thosevariables with maximal discriminative power in the sense of a minimal p-value, and combined theminto risk scores to define according subgroups.
Changes in the continuous variables were described by the mean and SD of the individualincrease or decrease, and the differences between CTA positive and CTA negative patients wereassessed by the difference of the mean values. These same differences were then adjusted forimbalances in the baseline values using an ANCOVA with an interaction between baseline andgroup and evaluating the group’s difference from the population mean. Logistic regression analyseswere done to modelling the outcome at follow-up as a linear function of the baseline status andgroup membership. P-values less than 5% were regarded as significant.

17
5. RESULTS
IThe intraobserver and interobserver reliability of sitting MP, prone MP, and paraspinal palpation fortenderness in the upper eight segments of the thoracic spine were established in this investigation.Using an ”expanded” definition of agreement which accepts small inaccuracies (+/- one segment) inthe numbering of spinal segments we found – based on pooled data - kappa values of 0.59 to 0.77for the hour-to-hour and the day-to-day intraobserver reliability with all three palpation procedures.Kappa coefficients were 0.24 and 0.22 for the interobserver reliability with prone and sitting MPand 0.67 and 0.70, respectively, with paraspinal palpation for tenderness.
The prevalence of positive MP findings in the cervical spine was < 2% for each segment,making a statistical evaluation of the reliability of palpation in the cervical spine inappropriate.Nonetheless, we used cervical palpation in III.IIThe intraobserver reliability and interobserver reliability of palpation for muscular tenderness in theanterior chest wall were assessed in this study. Based on a pooled analysis of data from palpation ofthe anterior chest wall we found kappa values of 0.21 to 0.28 for the day-to-day intraobserverreliability and of 0.44 to 0.49 for the hour-to-hour intraobserver reliability. For the interobserverreliability, kappa values ranged between 0.22 and 0.31.IIIThe decision making process of the CTA diagnosis was investigated along with a possible tool forthe identification of CTA. Finally, the diagnosis of CTA was validated. Eighteen percent of thepatients were classified as CTA positive, of which 80% had a normal MPI compared to 50% ofCTA negative patients (p< 0.001). Patient characteristics and MPI and CAG result are outlined intable 2.
Table 2. Patient characteristics and results. Results of myocardial perfusion imaging and coronaryangiography.
CTA total(N=275)
CTA positive(N=50)
CTA negative(N=225)
p
Patient characteristicsAge 56.31 (9.26) 50.36 (9.14) 57.63 (8.78) <0.001Weight 81.24 (15.58) 82.02 (20.18) 81.08 (14.43) 0.899Height 171.43 (12.50) 170.84 (18.68) 171.56 (10.74) 0.765BMI 27.08 (3.81) 26.39 (3.46) 27.22 (3.87) 0.262Systolic BP 141.17 (16.64) 136.76 (17.81) 142.15 (6.25) 0.009Diastolic BP 85.57 (9.12) 83.24 (7.90) 86.08 (9.32) 0.025Gender % female n=104 (38%) n=22 (44%) n=82 (36%) 0.337Referred from GP n=135 (49%) n=38 (76%) n=97 (43%) <0.001Perfusion imagingNormal n=151 (56%) n=40 (80%) n=111 (50%)Partly reversible defects n=33 (12%) n=1 (2%) n=32 (14%)Reversible defects n=63 (23%) n=4 (8%) n=59 (27%)
<0.001
Fixed defects n=25 (9%) n=5 (10%) n=20 (9%)Missing 3 0 3Coronary angiographyNormal n=152 (59%) n=40 (91%) n=112 (52%)1-vessel disease n=42 (16%) n=2 (5%) n=40 (19%)2-vessel disease n=34 (13%) n=1 (2%) n=33 (15%)
<0.001
3-vessel disease n=31 (12%) n=1 (2%) n=30 (14%)Missing 16 6 10
BMI = Body mass index. BP = Blood pressure. GP = General Practice.Data are expressed as means (SD) or absolute numbers (relative frequencies).

18
Noncardiac chest pain and atypical AP was significantly more frequent in the CTA positive group.There was a significant trend for a generally higher CCS class in the CTA negative group(p<0.001). Conversely, CTA positive patients suffered more often from neck pain (p < 0.001),thoracic spine pain (p<0.001), and shoulder arm pain (p=0.041). No differences were found withrespect to the pain intensities (table 3).
Palpation findings in form of paraspinal muscular tenderness, end-play, and joint-play MPrestrictions were significantly more frequent among CTA positive patients (table 3).
Table 3. Discrimination between the CTA groups at baseline in palpation findings, chest, neck andthoracic pain, and cardiovascular classification. Shown are absolute numbers and relative frequencies (inparentheses).
CTA total(N=275)
CTA positive(N=50)
CTA negative(N=225)
P
Palpation Chest wall tenderness 214 (78) 49 (98) 165 (73) 0.053 Paraspinal tenderness 133 (48) 48 (96) 85 (38) <0.001 End-play motion palpation 160 (58) 50 (100) 110 (49) <0.001 Joint-play motion palpation 90 (33) 50 (100) 40 (18) <0.001Type of chest pain Non-cardiac chest pain 39 (14) 17 (34) 22 (10) Atypical angina 80 (29) 22 (44) 58 (26) <0.001 Typical angina 156 (57) 11 (22) 145 (64)CCS I 133 (48) 43 (86) 90 (40) II 128 (47) 7 (14) 121 (54) III 14 (5) 0 (0) 14 (6)
<0.001
IV 0 (0) 0 (0) 0 (0)Presence of chest pain Today 159 (58) 31 (62) 128 (57) 0.531 Pain past 14 days 249 (91) 44 (88) 205 (91) 0.592Chest pain intensity * Intensity today 2.63 (1.61) 2.74 (1.29) 2.60 (1.69) 0.283 Max. intensity past 14 days 4.29 (2.21) 4.14 (1.97) 4.32 (2.27) 0.697 Average intensity past 14 days 3.36 (1.87) 2.91 (1.63) 3.46 (1.91) 0.090Presence of neck pain 106 (38) 37 (74) 69 (31) <0.001Neck pain intensity * Average intensity past 14 days 3.55 (1.99) 3.57 (1.89) 3.54 (2.06) 0.713Presence of thoracic pain 109 (40) 32 (64) 77 (34) <0.001Thoracic pain intensity * Average intensity past 14 days 3.45(1.99) 3.19 (1.94) 3.56 (2.02) 0.194Presence of shoulder arm pain 144 (52) 33 (66) 111 (49) 0.041Shoulder arm pain intensity * Average intensity past 14 days 3.80 (2.18) 3.61 (2.25) 3.86 (2.17) 0.459
*Pain intensity data are expressed in means (SD) within patients reporting pain, i.e., a value between 1 and10.
Finally, the main determinants in the decision process of the chiropractor could be identified givingrise to a classification tree, which was an approximate reconstruction of the decision process asoutlined in III.

19
IVIn this part we investigated if patients with a diagnosis of CTA would benefit from manual therapyas compared to CTA negative patients. Approximately 75% of CTA positive patients reportedimprovement of pain and of general health after treatment compared to 20%-22% of CTA negativepatients (p<0.0001) (figure 7)(IV, table 4).
Figure 7. Patients’ self perceived assessments of chest pain and general health at follow up.
Pain intensity decreased in both groups with consistently larger decreases for all types of painamong CTA positive patients (table 4) with two of the decreases being significant. SF-36 scoresincreased in the CTA positive group in 5 out of 8 scales and remained unchanged in CTA negativegroup (table 5).
Table 4. Change in pain intensity at follow-up among subjects with pain at baseline.
Decrease Unadjustet Diff Adjusted Diff
VariableCTA Mean (SD) Diff 95% CI Diff 95% CI p
+ 0.79 (1.8)Chest pain now
- 0.28 (2.1)0.50 -0.4, 1.4 0.46 -0.4, 1.3 0.274
+ 1.15 (2.0)Maximum chestpain* - 0.12 (2.2)
1.03 0.3, 1.8 1.15 0.4, 1.8 0.001
+ 0.56 (1.7)Average chestpain* - 0.23 (2.0)
0.33 -0.3, 1.0 0.63 0.0, 1.2 0.048
+ 1.03 (2.5)Average thoracicspine pain* - 0.69 (2.0)
0.35 -0.6, 1.3 0.54 -0.3, 1.4 0.228
+ 1.00 (2.4)Average neckpain* - 0.59 (2.0)
0.41 -0.5, 1.3 0.45 -0.3, 1.2 0.256
+ 1.31 (2.1)Average shoulderarm pain* - 0.89 (2.2)
0.42 -0.5, 1.3 0.44 -0.4, 1.4 0.294
* During the preceding 14 days.

20
Table 5. Increases in quality of life profile (SF-36) scores at follow-up compared to baseline.
Increase Unadjusted Diff Adjusted DiffVariable
CTA Mean (SD) Diff 95% CI Diff 95% CIp-value
+ 0 (12.9)Physicalfunctioning - -1.39 (13.0) 1.4 -2.8, 5.6 2.5 -1.8, 6.8 0.253
+ 8.15 (21.1)Rolephysical - -0.44 (30.6) 8.6 -0.8, 18.0 12.3 2.8, 21.9 0.011
+ 4.22 (14.7)BodilyPain
-0.39 (17.3) 3.8 -1.6, 9.2 4.9 -0.3, 10.1 0.066
+ 0.53 (12.5)Generalhealth - -0.27 (12.9) 0.8 -3.3, 5.0 2.6 -1.7, 6.8 0.232
+ 10.44 (17.7)Vitality- 0.72 (15.8) 9.7 4.5, 14.9 0.6 4.6, 14.5 <0.001
+ 4.62 (17.2)Socialfunctioning - -1.51 (15.9) 6.1 0.9, 11.3 5.4 0.6, 10.3 0.029
+ 16.30 (34.5)Roleemotional - 2.59 (37.6) 13.7 1.7, 25.7 16.2 5.6, 26.8 0.003
+ 4.43 (15.1)MentalHealth - -0.74 (14.4) 5.2 0.5, 9.8 4.8 0.4, 9.2 0.033
CTA+: N=46 and CTA-: N=208.
After manual treatment, there was an increase from 37 (74%) to 42 (91%) (p=0.02) in CTA positivepatients who believed they had chest pain originating from muscles and joints of the thorax and theneck and a decline from 26 (52%) to 18 (39%) (p=0.27) in patients who believed they had chestpain of cardiac origin. Similarly, there was a decline from 37 (74%) to 22 (48%) (p=0.002) in CTApositive patients who were afraid of their chest pain. In comparison, no statistically significantchanges were observed in the CTA negative group from baseline to follow-up for any of these threequestions.

21
6. DISCUSSION
It is generally accepted that the musculoskeletal system can produce chest pain, (1;4-7) but the term“musculoskeletal chest pain” does not imply a well-defined disease entity. On the contrary, chestpains from the musculoskeletal system covers a heterogeneous group with various designations likeTietze’s syndrome(95) costochondritis,(96) fibromyalgia,(96) chest wall tenderness,(12) degenerativepathology of the spine,(45;48;97) myositis,(11) segmental thoracic dysfunction,(11;15;98) costovertebraldysfunctions,(99-102) etc. Previous studies have suggested that 13%-18% of patients with chronicchest discomfort(11;12) and 23%-28% with more acute chest pain(103;104) may suffer frommusculoskeletal chest pain. However, none of these applied validated palpatory examinationprocedures, which limit their clinical value.
In the present work, we focused on a subgroup of stable AP population, namely patients witha musculoskeletal cause of chest pain in the shape of CTA. This diagnosis was given to 18% of thepopulation with known or suspected AP referred for CAG at a University Hospital.
Palpation
The perception remains that palpation is a reliable procedure(105;106) despite the lack in evidence.(64-
67;107) The reason for this paradox may be the “face validity” of palpation:(64;65;106) the proceduremakes sense intuitively and it seems to be a reasonable approach to identify spinal dysfunction.Furthermore, palpation appears to be a useful clinical tool in that it is non-invasive, easy to employ,inexpensive and risk-free.
Reliability studies on palpation procedures have primarily focused on the ability to identifycorrectly the presence of the same segmental dysfunction in a controlled research environment. Inthe clinical situation, however, it is less important to identify the exact segmental level of adysfunction than to identify the presence of abnormality.(69;108) In line with this, it has beendemonstrated that the mechanical effects of spinal manipulation lack spatial specificity.(109)
Obviously, reliability is crucial when palpation procedures from clinical trials with groupcomparisons are translated into the daily clinical practices with its focus on the individual patient.Nevertheless, the number of studies investigating the reliability of motion palpation procedures ofthe upper thoracic spine is very limited,(110;111) and none of these have focused on chest painpatients. In fact, the literature is totally devoid of reports on the reliability of manual palpation fortenderness of the thoracic muscles. As a consequence, we choose to establish and investigate ourown examination program based on motion palpation procedures (I & II) combined with patienthistory (III). In part project I we used strict and “expanded” agreement. Strict agreement meantexact spatial concordance between the observers’ findings of a certain dysfunction, whereasexpanded agreement allowed minor spatial disagreement of ± 1 vertebral segment. Our results (I)suggested that an experienced observer using sitting and prone MP could achieve acceptably lowhour-to-hour and day-to-day variability. Additionally, we obtained an acceptably low intra- andinterobserver variability when paraspinal tenderness was diagnosed in the thoracic spine (I), afinding which was in keeping with results from palpation of other spinal regions.(66;112;113) We didnot use the expanded agreement in II because topographic uncertainty locating the 14 anatomicpoints was not to be expected among observers (figure 2). The results in II suggested anunacceptably high intra- and interobserver variability with palpation for tenderness in the anteriorchest wall. No comparable study exists.
Despite the high observer variability in II and the consequent methodological limitations, wechoose to combine the palpation procedures from I & II into one protocol. We did so becauseseveral previous investigations had used palpation for tenderness of the thorax to classify orcategorize patients with AP,(12;114;115) and further because there exists no generally acceptedalternative procedures for examination for chest wall tenderness. The concept of diagnosing joint dysfunctions and muscular tenderness with manual palpationis well known within different medical disciplines like cardiology and rheumatology as it is within

22
physical therapy, chiropractic, and manual medicine.(116-118) However, within the medical fieldsthere has been no tradition for evaluating the reliability of these procedures although moderntextbooks describe the use of manual palpation.(62;116)
The diagnosis of musculoskeletal chest pain
There exist no golden standard to assess the existence of CTA. We used proxy measures such asmanual palpation procedures and the case history to establish the diagnosis. In III, we combined theprotocol of I and II with a detailed case history to investigate the decision making process of thechiropractor and to identify the most important determinants from both patient history and clinicalexamination to create a classification tree (III, figure 1).(119) First, we compared the frequency of thecandidate variables in the CTA positive and CTA negative patients (III). The role of each singlevariable in the decision process can be difficult to judge since many of the variables are correlated.Even if a variable has an influence in certain subgroups it does not necessarily have a highdiscriminative power in the whole population. If it was not possible to select serial variables with adistinctive discriminating power we selected the variables with minimal p-values and combinedthem into a risk score (III).
Highest significance for association with the CTA positive diagnosis was found for a) CCSgrade of angina, b) presence of neck pain, c) type of angina, d) four palpation findings, and e) spinaltenderness. Further, we found 27 variables that were less closely associated with the CTAdiagnosis. By these means we were able to give an example of the reconstructed decision processfor the CTA positive patients (III, figure 1).
Additionally, by comparison with an independent and totally different modality like MPI, wefound support for the validity of the chiropractic CTA diagnosis.
Manual treatment of musculoskeletal chest pain
It is of great interest to explain if, and to what extent, manual therapy to patients withmusculoskeletal chest pain are capable of reducing the symptoms of the disorder in a favourabledirection. Our non-randomised clinical treatment study is the first prospective trial in the literature.The overall impression from our study is that manual therapy may have an effect.
The major criticism of our positive outcome in IV may be our study design. With itslimitations, the non-randomised trial may be used to detect associations between intervention andoutcome although one cannot rule out that some associations were caused by a third factor linked toboth intervention and outcome. It is not always feasible to conduct a randomised controlled trialespecially not if a certain treatment is considered mandatory or preferable to others. Further,exposing patients to an intervention believed to be inferior to current treatment may be superfluousor even unethical. Strong patient preferences or certain belief (“the heart is the pain source”) maylimit recruitment and cause bias. It appeared that our study design was the most feasible solutionwithin the time window available (2 years). There was no need to start a randomised trial unless wehad found a diagnostic means and a treatment option which we believed would work at an earlystage of the disease. Except for a few case reports(11;15;120-125) suggesting a beneficial effect ofmanual therapy we had no indication of which kind of manual therapy, which intensity, and whichduration of treatment was needed for it to be effective. Given these constraints, we had to make ourown choice with regard to palpation and treatment procedures, recognizing that one or both mightturn out not to be ideal. In doing this we hoped at least to see patterns and pointers that could makethe basis for future randomised trials.
Quality of lifeWe found that five out of eight quality of life scores increased significantly in the CTA positivegroup and remained unchanged in the CTA negative. The SF-36 is a generic quality-of-lifeinstrument not created especially for chest pain patients. Nevertheless, it did ably document patient

23
self-perceived benefits of manual therapy in role physical, vitality, social functioning, roleemotional and mental health scores (table 5). The bodily pain scale was borderline significant. Thephysical functioning and the general health scores were not able to quantify significant treatmenteffect. The lack of improvement in the SF-36 general health score was contradicted by the patients’self perceived general health (figure 7).
Pain measurementsThe quality of pain was fairly uniform in the CTA positive and CTA negative group, except forsharp pain, being more frequent among the CTA positive patients (III). Distinction could not bemade from symptoms often regarded as characteristic for musculoskeletal chest pain (III). Wefound the expected differences concerning type and severity of AP in the two groups namely morenon-cardiac chest pain and lower CCS class among the CTA positive patients, compared to moretypical AP and higher CCS class among the CTA negative patients (III). More neck, thoracic, and,shoulder arm pain was found in the CTA positive group (III). The intensity of these different painshad no discriminative power for neck, thoracic, chest, and, shoulder arm pain (table 3).
Since there has been no tradition for systematic observer unrelated assessment of painintensity in patients with AP, we choose to use rating scales and patient perception of pain. Weapplied a questionnaire with intensity grading on a 11-point box scale(80) of chest pain, thoracicspine pain, cervical spine pain, and shoulder arm pain. A major advantage of this serial measure ofsensory pain intensity is its ratio scale properties, making it appropriate to speak about differencesbetween measurements obtained at different point in time.(126) At the same time it is easy toadminister and score.(80) Its major limitation is the assumption that pain is an uni-dimensionalexperience which can be measured with a single item scale.(127)
As we can see in figure 8, the results of the rating scale score usually show a distribution witha distinct peak at 0, i.e., a substantial fraction of subjects indicated no pain. The remaining valueswere often spread over a wide range with a peak in the region of 1-3. Therefore, we decided toanalyse the scores in the following way: First, we considered the relative frequency to observe ascore of 0, and, secondly, we considered the distribution of the scores among patients with a ratingscale score >0, reporting mean and standard deviation (table 3).
On the binary scales we found no effect of the manual therapy in any of the six pain scales(IV). However, maximum chest pain intensity and average chest pain intensity during the lastfortnight did improve significantly in the CTA positive compared to the CTA negative group andwith the remaining four scales there was an insignificant tendency for reduction in pain intensityamong the CTA positive patients (table 4).
Patient perception of pain and general healthIn addition to the rating scale we used the patient’s own perception of pain and general health. Thisapproach has been criticized and avoided in many clinical studies in the past because of concern ofrecall bias.(128)
About 74% of the CTA positive patients reported improvement of pain after treatment (IV)compared to 22% among the CTA negative ones. Thirteen percent of the CTA negative groupreported worse chest pain after treatment compared to none in the CTA positive group (figure 7)(IV, table 4).
These conflicting results with pain measurements, suggest that rating scales are not anappropriate tool to assess improvement in such a low level pain population, neither as a binary noras a continuous variable. This might be explained by the fact that in studies on the effect of manualtherapy using rating scales scores as an outcome measure baseline values have typically a meanabout 5-6 allowing a mean reduction by 3 to 4 points to be observed.(129;130) In our population ofpatients we had a mean of 3.5 at baseline, and - in contrast to most other studies – a substantialfraction of patients with no pain (figure 8). Similarly, the high standard deviations of about 2 for thechange in the pain scores among the CTA negative patients made assessment of improvementdifficult (table 4).

24
Figure 8. Distribution of pain ratings for the 6 different types of pain.

25
Other investigators have found poor agreement and low correlation between a serial measureof pain intensity and the patients’ retrospective perception of pain.(131;132) Similar tendencies mightexplain our findings.
Participants in the clinical studies III and IVOur patients did not come to us for manual examination and treatment. They were recruited fromthe MILES study, the aim of which was to investigate the prevalence of various myocardialperfusion patterns in patients referred to cardiac catheterisation for known or suspected stable AP.In fact, many of the patients who were included in the present study were surprised to know that themusculoskeletal system could potentially cause chest pain. They had been told beforehand that theirpain was probably of cardiac origin, and that it might become dangerous if it was not examined andtreated accordingly.
Of our 972 prospective patients roughly one half were not included in the MILES study due tochosen exclusion criteria (III). Of the 516 eligible patients approximately 25% did not comply orgave no written consent to participate, and about 22% were not included for medical reasons (III,table 2). The 25% was a disappointing high number. The most frequent reasons the patient gaveduring the interview were lack of time, fear for the manual treatment and a firm belief that the heartand not other organs was the cause of symptoms and, consequently, additional examinationappeared redundant to them.

26
7. CONCLUSIONS
We found good intraobserver reliabilty with prone and sitting motion palpation for biomechanicaldysfunction and paraspinal palpation for tenderness (I) and good interobserver reliabilty with regardto paraspinal tenderness (I), but poor interobserver reliability with prone and sitting motionpalpation and palpation of the chest wall and poor intraobserver reliability with palpation of thechest wall (I and II).
A standardized clinical examination program was established to prepare a diagnosis ofnoncardiac chest pain originating from the musculoskeletal system (I and II). Further, it wasdemonstrated that it is possible to identify a subset of patients with suspected AP who match thediagnosis of CTA, in the present material approximately 1/5 of patients. Among the CTA positivepatients, 80% had normal myocardial perfusion compared to 50% of CTA negative patients (III)indicating more angina due to myocardial ischemia among the CTA negative ones.
Finally, our treatment series suggested that patients with suspected AP and a chiropracticbased diagnosis of CTA might benefit from manual therapy (IV).

27
8. PERSPECTIVES
A two-year follow-up of the MILES population will finish in November 2003. Of the 507 patientsinvited for follow-up, 404 have accepted participation.These results, including data from the CTA positive and CTA negative patients, are presently beingevaluated. We hope to answer some of the following questions: 1) Did the positive treatment effectlast for two years? 2) Did the musculoskeletal findings change during the follow-up period? 3) Didthe quality of life scores change? 4) Did the pain symptoms vanish in the CTA negative group whenthey had the CAG examination performed and the appropriate treatment or advice? 5) Did thepatients with normal MPI have their antianginal medicine reduced?
This is the first in a series of projects on how to identify spinal dysfunction by manualexamination and the relation between patient self-reported pain and manual examination. Presently,the investigator is involved in a systematic review of the peer-reviewed literature about thereliability and reproducibility of manual examination procedures of the spine, taking into accountthe quality of the studies. This information shall be used in future study designs for reliability andvalidity studies on manual palpation.
Further, we would like to improve the manual diagnosis as part of the improved differentialdiagnosis in the non-cardiac chest pain disorders as a contribution to obtaining meaningful,manageable and clinical relevant definitions of the different non-cardiac chest pain disorders.
As a consequence of the possibility to identify a subgroup of patients with suspected AP whohave in fact noncardiac chest pain originating from the musculoskeletal system – the use of casehistory and a standardized examination program should be advocated in general practice and atcardiological wards by means of postgraduate courses. The perspective could be that a number ofpatients could be without extensive investigations (MPI/CAG).
Retrospectively, we have come to realize that patients’ reporting of chest pain reflect both asensory experience and the patient’s affective and cognitive responses, accordingly, it might havebeen more useful to apply a multidimensional scale, like the McGill pain questionnaire, whichconsists of 3 major classes of word descriptors – sensory, affective and evaluative – and has beendeveloped to provide more comprehensive information about the subjective pain experience.(127) Infuture studies we will consider adopting this scale.
Alternative outcome variables should be considered. A functional measure like the SeattleAngina Questionnaires which is an 19-item self-administered questionnaire measuring fivedimensions of coronary artery disease: physical limitation, anginal stability, anginal frequency,treatment satisfaction and disease perception, could be used. It has been found valid and reliable(133), and superior to the Specific Activity Scale and the Duke Activity Status Index which onlypredict physical limitation and have been tested in patients with heart disease and not non-cardiacangina.(134;135)
The development of a “chest pain disability index” should be pursued in which a combinationof different outcome measures could differentiate non-cardiac from cardiac aetiologies. The chestpain disability index could combine physical and psychological capacity and include the aspects ofhow distressing patients find their chest pain. Obviously, such an index should be developed in acollaboration between different medical specialities and manual therapy disciplines.
Concomitantly, it probably would be necessary to study further the basic mechanism of chestpain in corporation with physiologists. This might help refining the various diagnostic means and,hopefully, provide a better basis for more individualized and further optimized therapy in thiscategory of patients.

28
9. SUMMARY IN ENGLISH
This is a ph.d.-dissertation on diagnosis and treatment of chest pain from the musculoskeletalsystem in patients with known or suspected stable angina pectoris (AP), more definite namedcervico-thoracic angina (CTA). The dissertation comprises 4 part projects (I-IV). The aim was toassess the reliability of different manual palpation methods for the detection of muscular tendernessin the thorax and biomechanical dysfunction in the spine (I-II). Additional, illustrate the occurrenceof CTA in AP patients and describe the possible diagnostic decision process based on case historyand clinical examination including manual palpation (III). Finally, it was examined if patients witha CTA positive diagnosis would benefit from manual treatment (IV).
In I and II we investigated the intra- and interobserver reliability of 4 palpation methods in 85patients. I part project III, 507 patients referred for coronary angiography (CAG) were examined.Out of these 275 gave consent to participate. Myocardial perfusion imaging (MPI) was done toevaluate the perfusion of the myocardium and later CAG were done. The result was notcommunicated. The treatment part (IV) was done as a non-randomised trial where 50 patients withthe diagnosis CTA were offered manual therapy. The studies showed, that it was possible toestablish an examination program with low intraobserver variation, but with high interobservervariation except for paraspinal tenderness. Further, it was shown, that an experienced chiropractor,by systematic manual palpation of the spine and thorax in combination with a number of variablesfrom the case history and the clinical examination, could identify a subgroup of AP patients withCTA, in the present material 18%. In this group we found normal myocardial perfusion in 80%compared with 50% in the CTA negative group. Finally, the non-randomised treatment seriessuggested that patients with suspected AP and a chiropractic-based diagnosis of CTA might benefitfrom manual therapy (IV). To sum up, the study gave the impression that musculoskeletaldysfunction can be a (contributory) cause of the chest pain in patients referred for furtherinvestigation of AP, and that manual therapy is a possible treatment offer to these patients.
The clinical consequences of the treatment trial cannot be concluded before we have long-term results and more controlled treatment trials.

29
10. SUMMARY IN DANISH
Denne ph.d.-afhandling omhandler diagnostik og behandling af brystsmerter afledt fra detmuskuloskeletale apparat hos patienter med kendt eller formodet stabil angina pectoris (AP),såkaldt cerviko-thorakal angina (CTA). Afhandlingen består af 4 delprojekter (I-IV). Formålet varat vurdere reproducerbarheden af forskellige manuelle palpationsmetoder til påvisning af muskulærømhed i thorax samt biomekaniske dysfunktioner i rygsøjlen (I-II). Desuden at belyse forekomstenaf CTA hos AP patienter og i den forbindelse beskrive den mulige diagnostiske beslutningsprocesbaseret på sygehistorie og klinisk undersøgelse inklusive palpation (III). Endelig blev det søgtvurderet, om patienter med diagnosen CTA havde gavn af manuel behandling (IV).
I I og II undersøgtes intra- og interobservatør variationen af 4 palpationsmetoder hos 85patienter. I delarbejde III undersøgtes 507 patienter henvist til koronararteriografi (KAG). Af disseindvilligede 275 i deltagelse. Der blev udført myokardiescintigrafi (MPI) til vurdering afmyokardieperfusionen og senere KAG. Resultatet af disse undersøgelser blev ikke oplyst.Behandlingsdelen (IV) blev gennemført som et ikke-randomiseret forsøg, hvori 50 patienter meddiagnosen CTA blev tilbudt manuel behandling. Studierne viste, at det var muligt at etablere etundersøgelsesprogram med lav intraobservatør variation, men med høj interobservatør variationmed undtagelse af palpation for paraspinal ømhed. Det blev yderligere vist, at en erfarenkiropraktor, ved systematisk manuel palpation af rygsøjlen og thorax i kombination med en rækkevariabler fra sygehistorien og den kliniske undersøgelse, kan identificere en undergruppe af APpatienter med CTA, i det aktuelle materiale 18%. Hos 80% af denne gruppe blev der fundet normalperfusion i myokardiet mod 50% i gruppen af CTA negative patienter. Endelig antydede denurandomiserede behandlingsdel, at AP patienter med den kiropraktiske diagnose CTA muligvis kanhave gavn af manuel behandling. Sammenfattende gav projektet indtryk af, at muskuloskeletaldysfunktion kan være en (medvirkende) årsag til brystsmerter hos patienter henvist til nærmereundersøgelse for AP, samt at manuel terapi muligvis er en behandlingsmulighed hos disse.
De kliniske konsekvenser af det gennemførte behandlingsforsøg kan ikke drages, før derforeligger langtidsresultater og mere kontrollerede behandlingsserier, end der har kunnet rummes idet nærværende ph.d.-projekt.

30
11. REFERENCES
(1) Braunwald E. Part I: Examination of the patient: The history. In: Braunwald E, editor. Heartdisease. 6th ed. W.B. Saunders Company, 2001:27-45.
(2) Haghfelt T, Alstrup P, Grande P, Madsen JK, Rasmussen K, Thiis J. [Guidelines for diagnosis andtreatment of patients with stable angina pectoris]. Copenhagen: Danish Society of Cardiology andDanish society of Thoracic Surgery, 1996.
(3) Peterson DH, Bergmann TF. Joint assessment principles and procedures. In: Burgess L, editor.Chiropractic technique. New York: Churchill Livingstone, 1993:51-122.
(4) Kryger P. Medicinsk Kompendium. 15 ed. Copenhagen: Nyt Nordisk Forlag Arnold Busch, 1999.
(5) Best RA. Non-cardiac chest pain: a useful physical sign? Heart 1999; 81(4):450.
(6) Chambers J, Bass C, Mayou R. Non-cardiac chest pain: assessment and management. Heart 1999;82(6):656-657.
(7) Chambers J, Bass C. Chest pain with normal coronary anatomy: a review of natural history andpossible etiologic factors. Prog Cardiovasc Dis 1990; 33(3):161-184.
(8) Hoilund-Carlsen PF, Johansen A, Christensen HW, Vach W, Bartram P, Veje A et al. Myocardialperfusion as guidance for diagnostic catheterization and management decision in stable anginapectoris, (submitted) 2003.
(9) Hemingway H, Marmot M. Evidence based cardiology: psychosocial factors in the aetiology andprognosis of coronary heart disease. Systematic review of prospective cohort studies. BMJ 1999;318(7196):1460-1467.
(10) Fleet RP, Dupuis G, Marchand A, Burelle D, Beitman BD. Panic disorder, chest pain and coronaryartery disease: literature review. Can J Cardiol 1994; 10(8):827-834.
(11) Bechgaard P. Segmental thoracic pain in patients admitted to a medical department and a coronarycare unit. Acta Med Scand 1982; (supple 644): 87-89.
(12) Wise CM, Semble EL, Dalton CB. Musculoskeletal chest wall syndromes in patients withnoncardiac chest pain: A study of 100 patients. Arch Phys Med Rehabil 1992;73:147-149.
(13) Epstein SE, Gerber LH, Borer JS. Chest wall syndrome:A common cause of unexplained cardiacpain. Journal of the American Medical Association 1979;241[26]:2793-2797.
(14) Levine PR, Mascette AM. Musculoskeletal chest pain in patients with "angina": A prospectivestudy. South.Med.J 1989;82[5]:580-585.
(15) Hamberg J, Lindahl O. Angina pectoris symptoms caused by thoracic spine disorders. Clinicalexamination and treatment. Acta Med Scand Suppl 1981;644:84-86.
(16) Berman DS, Germano G, Shaw LJ. The role of nuclear cardiology in clinical decision making.Semin Nucl Med 1999;29(4):280-297.
(17) Klocke FJ, Baird MG, Lorell BH, Bateman TM, Messer JV, Berman DS et al. ACC/AHA/ASNCguidelines for the clinical use of cardiac radionuclide imaging--executive summary: a report of theAmerican College of Cardiology/American Heart Association Task Force on Practice Guidelines(ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of CardiacRadionuclide Imaging). Circulation 2003;108(11):1404-1418.

31
(18) Lavey EB, Winkle RA. Continuing disability of patients with chest pain and normal coronaryarteriograms. J Chronic Dis 1979;32(3):191-196.
(19) Ockene IS, Shay MJ, Alpert JS, Weiner BH, Dalen JE. Unexplained chest pain in patients withnormal coronary arteriograms: a follow-up study of functional status. N Engl J Med 1980;303(22):1249-1252.
(20) Sullivan AK, Holdright DR, Wright CA, Sparrow JL, Cunningham D, Fox KM. Chest pain inwomen: clinical, investigative, and prognostic features. BMJ 1994;308(6933):883-886.
(21) Lantinga LJ, Sprafkin RP, McCroskery JH, Baker MT, Warner RA, Hill NE. One-yearpsychosocial follow-up of patients with chest pain and angiographically normal coronary arteries.Am J Cardiol 1988;62(4):209-213.
(22) Procacci P, Maresca M. Historical considerations of cardiac pain. Pain 1985;22(4):325-335.
(23) Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS et al. ACC/AHA 2002guideline update for the management of patients with chronic stable angina: a report of theAmerican College of Cardiology/American Heart Association Task Force on practice guidelines(Committee to Update the 1999 Guidelines for the Management of Patients With Chronic StableAngina) . American Col lege of Cardiology Web Si te Avai label a t :http://www.acc.org/clinical/guidelines/stable/stable.pdf 2002.
(24) Procacci P, Zoppi M, Maresca M. Textbook of pain. 4 ed. Churchill Livingstone, 1999.
(25) Mayou R, Bryant B, Forfar C, Clark D. Non-cardiac chest pain and benign palpitations in thecardiac clinic. Br Heart J 1994;72(6):548-553.
(26) Mayou RA, Bass CM, Bryant BM. Management of non-cardiac chest pain: from research toclinical practice. Heart 1999;81(4):387-392.
(27) Nijher G, Weinman J, Bass C, Chambers J. Chest pain in people with normal coronary anatomy.BMJ 2001;323(7325):1319-1320.
(28) Coulshed DS, Eslick GD, Talley NJ. Non-cardiac chest pain. Patients need diagnoses. BMJ 2002;324(7342):915.
(29) Eslick GD, Coulshed DS. Rapid assessment of chest pain. Chest pain clinics may be one stepforward, two steps back. BMJ 2002; 324(7334):422.
(30) Maseri A. Syndrome X: still an appropriate name. J Am Coll Cardiol 1991;17(7):1471-1472.
(31) Bøtker HE, Sonne HS, Frøbert O, Thomassen AR. Syndrom X: Angina pectoris hos patienter medangiografisk normale koronararterier. Ugeskr Læger 1997;159[25]:3925-3928.
(32) Sylven C. Angina pectoris. Clinical characteristics, neurophysiological and molecularmechanisms. Pain 1989;36(2):145-167.
(33) Crea F, Pupita G, Galassi AR, el Tamimi H, Kaski JC, Davies G et al. Role of adenosine inpathogenesis of anginal pain. Circulation 1990;81(1):164-172.
(34) Tomai F, Crea F, Gaspardone A, Versaci F, Esposito C, Chiariello L et al. Mechanisms of cardiacpain during coronary angioplasty. J Am Coll Cardiol 1993;22(7):1892-1896.
(35) Souza TA. Differentiating mechanical pain from visceral pain. Top Clin Chiro 1994;1[1], 1-12.
(36) Ness TJ, Gebhart GF. Visceral pain: a review of experimental studies. Pain 1990;41(2):167-234.

32
(37) Rosen SD, Paulesu E, Frith CD, Frackowiak RS, Davies GJ, Jones T et al. Central nervouspathways mediating angina pectoris [see comments]. Lancet 1994;344(8916):147-150.
(38) Harford WV. Southwestern Internal Medicine Conference: the syndrome of angina pectoris: roleof visceral pain perception. Am J Med Sci 1994;307(4):305-315.
(39) Kellgren JH. On the distribution of pain arising from deep somatic structures with charts ofsegmental pain areas. Clinical Science 1939;4:35-46.
(40) Inman VT, Saunders JB. Referred pain from skeletal structures. J Nerv and Ment Dis1944;(99):660-667.
(41) Feinstein B, Langton JNK, Jameson RM, Schiller F. Experiments on pain referred from deepsomatic tissues. Journal of bone and joint surgery 1954;36[5]:981-997.
(42) Dreyfuss P, Tibiletti C, Dreyer SJ. Thoracic zygapophyseal joint pain patterns. A study in normalvolunteers. Spine 1994;19(7):807-811.
(43) Nachlas IW. Pseudo-angina pectoris originating in the cervical spine. Journal of the AmericanMedical Association 1934;[103]:323-325.
(44) LeBan MM, Meerschaert JR, Taylor RS. Breast pain: A symptom of cervical radiculopathy. ArchPhys Med Rehabil 1979;60:315-317.
(45) Davis D, Ritvo M. Osteoarthritis of the cervicodorsal spine (radiculitis) simulating coronary-arterydisease. Clinical and roentgenologic findings. N.Engl.J Med. 1948;238[25]:857-866.
(46) Davis D. Spinal nerve root pain (radiculitis) simulating coronary occlusion: a common syndrome.Am Heart J 1948;35:70-80.
(47) Booth RE, Rothstein RD. Cervical angina. Spine 1976;1[1]:28-32.
(48) Brodsky AE. Cervical angina. A correlative study with emphasis on the use of coronaryarteriography. Spine 1985;10[8],699-709.
(49) Wells P. Cervical angina. Am Fam Physician 1997;55(6):2262-2264.
(50) Dwyer A, Aprill C, Bogduk N. Cervical zygapophyseal joint pain patterns. I: A study in normalvolunteers. Spine 1990;15(6):453-457.
(51) Davies HA, Jones DB, Newcombe RG. Angina-like esophageal pain: differentiation from cardiacpain by history. J Clin Gastroenterol 1985;7:477-481.
(52) Wu EB, Cooke R, Anggiansah A, Owen W, Chambers JB. Are oesophageal disorders a commoncause of chest pain despite normal coronary anatomy? QJM 2000;93(8):543-550.
(53) Cohen S. Noncardiac chest pain. The crumbling of the sphinx. Dig Dis Sci 1989;34(11):1649-1650.
(54) Frobert O, Funch JP, Bagger JP. Diagnostic value of esophageal studies in patients with angina-like chest pain and normal coronary angiograms. Ann Intern Med 1996;124(11):959-969.
(55) McCroskery JH, Schell RE, Sprafkin RP, Lantinga LJ, Warner RA, Hill N. Differentiating anginalpatients with coronary artery disease from those with normal coronary arteries using psychologicalmeasures. Am J Cardiol 1991;67(7):645-646.

33
(56) Tennant C, Mihailidou A, Scott A, Smith R, Kellow J, Jones M et al. Psychological symptomprofiles in patients with chest pain. J Psychosom Res 1994;38(4):365-371.
(57) Cannon RO, III, Quyyumi AA, Schenke WH, Fananapazir L, Tucker EE, Gaughan AM et al.Abnormal cardiac sensitivity in patients with chest pain and normal coronary arteries. J Am CollCardiol 1990;16(6):1359-1366.
(58) Turiel M, Galassi AR, Glazier JJ, Kaski JC, Maseri A. Pain threshold and tolerance in women withsyndrome X and women with stable angina pectoris. Am J Cardiol 1987; 60(7):503-507.
(59) Zachariae R, Melchiorsen H, Frobert O, Bjerring P, Bagger JP. Experimental pain and psychologicstatus of patients with chest pain with normal coronary arteries or ischemic heart disease. AmHeart J 2001;142(1):63-71.
(60) Keating J, Matyas TA, Bach TM. The effect of traning on the physical therapists´ ability to applyspecified forces of palpation. Phys Ther 73[1], 38-46. 1993.
(61) Beal MC. Louisa Burns Memorial Lecture: Perception through palpation. J Am Ostopath Assoc1989;89[10]:1334-1352.
(62) Friss J, Junker P, Manniche C, Petersen J, Steengaard-Pedersen K. Reumatologi. 1 ed.Copenhagen: FADL's Forlag, 2001.
(63) Haas M, Groupp E, Panzer D, Partna L, Lumsden S, Aickin M. Efficacy of cervical endplayassessment as an indicator for spinal manipulation. Spine 2003;28(11):1091-1096.
(64) Keating-JC J. Inter-examiner reliability of motion palpation of the lumbar spine: A review ofquantitative literature. Am J Chiropr Med 1989;2:107-110.
(65) Panzer DM. The reliability of lumbar motion palpation [published erratum appears in JManipulative Physiol Ther 1992 Nov-Dec;15(9):following table of contents]. J ManipulativePhysiol Ther 1992;15(8):518-524.
(66) Hestbæk L, Leboeuf-Yde C. Are chiropractic tests for the lumbo-pelvic spine reliable and valid? Asystematic critical literature review. J Manipul Physiol Ther 2000;23[4]:258-275.
(67) van der Wurff P, Hagmeijer RH, Meyne W. Clinical tests of the sacroiliac joint. A systemicmethodological review. Part 1: reliability. Man Ther 2000;(1):30-36.
(68) Huijbregts PA. Spinal Motion Palpation: A Review of Reliability Studies. J Manual andManipulative Ther 2002;10(1):24-39.
(69) Harvey D, Byfield D. Preliminary studies with a mechanical model for the evaluation of spinalmotion palpation. Clin Biomech 1991;6,79-82.
(70) Macfadyen N, Maher CG, Adams R. Number of sampling movements and manual stiffnessjudgments. J Manipulative Physiol Ther 1998;21(9):604-610.
(71) Haas M, Panzer D, Peterson D, Raphael R. Short-Term Responsiveness of Manual Thoracic End-Play Assesment to Spinal Manipulation: A Randomized Trial of Construct Validity. J ManipulPhysiol Ther 1995;18[9]:582-589.
(72) Jull G, Bogduk N, Marsland A. The accuracy of manual diagnosis for cervical zygapophysial jointpain syndromes. Med J Aust 1988;148(5):233-236.
(73) Aker PD, Gross AR, Goldsmith CH, Peleso P. Conservative management of mechanical neck pain:systematic overview and meta-analysis. BMJ 1996;313:1291-1296.

34
(74) Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. Manipulation and mobilization ofthe cervical spine. A systematic review of the literature. Spine 1996;21(15):1746-1759.
(75) Gross AR, Kay T, Hondras M, Goldsmith C, Haines T, Peloso P et al. Manual therapy formechanical neck disorders: a systematic review. Man Ther 2002;7(3):131-149.
(76) Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG. Spinal manipulative therapy for lowback pain. A meta-analysis of effectiveness relative to other therapies. Ann Intern Med 2003;138(11):871-881.
(77) Schiller L. Effectiveness of spinal manipulative therapy in the treatment of mechanical thoracicspine pain: a pilot randomized clinical trial. J Manipulative Physiol Ther 2001;24(6):394-401.
(78) Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med 1979;300(24):1350-1358.
(79) Campeau L. Letter: Grading of angina pectoris. Circulation 1976;54(3):522-523.
(80) Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of sixmethods. Pain 1986; 27(1):117-126.
(81) Manniche C. Assesment and exercise in low back pain. University of Copenhagen, 1995.
(82) Jordan A, Bendix T, Nielsen H, Hansen FR, Host D, Winkel A. Intensive training, physiotherapy,or manipulation for patients with chronic neck pain. A prospective, single-blinded, randomizedclinical trial. Spine 1998; 23(3):311-318.
(83) Bjørner JB, Damsgaard MT, Watt T, Bech P, Rasmussen NK, Kristensen TS et al. Dansk manualtil SF-36 - et spørgeskema om helbredsstatus. Lif Lægemiddelindustriforeningen, 1997.
(84) Pocock SJ, Henderson RA, Clayton T, Lyman GH, Chamberlain DA. Quality of life after coronaryangioplasty or continued medical treatment for angina: three-year follow-up in the RITA-2 trial.Randomized Intervention Treatment of Angina. J Am Coll Cardiol 2000; 35(4):907-914.
(85) Marquis P, Fayol C, Joire JE. Clinical validation of a quality of life questionnaire in anginapectoris patients. Eur Heart J 1995; 16(11):1554-1560.
(86) Bowling A. Cardiovascular diseases. Measuring disease. A review of disease-specific quality oflife measurement scales. Open University Press, 1995: 234-258.
(87) Smith HJ, Taylor R, Mitchell A. A comparison of four quality of life instruments in cardiacpatients: SF-36, QLI, QLMI, and SEIQoL. Heart 2000; 84(4):390-394.
(88) Bjorner JB, Thunedborg K, Kristensen TS, Modvig J, Bech P. The Danish SF-36 Health Survey:translation and preliminary validity studies. J Clin Epidemiol 1998; 51(11):991-999.
(89) Keller SD, Ware JE, Jr., Bentler PM, Aaronson NK, Alonso J, Apolone G et al. Use of structuralequation modeling to test the construct validity of the SF-36 Health Survey in ten countries: resultsfrom the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol 1998;51(11):1179-1188.
(90) Peterson DH. Principles of Adjustive Technique. In: Bergmann TF, Peterson DH, Lawrence DJ,editors. Chiropractic Technique. New York: Churchill Livingstone Inc, 1993: 123-196.
(91) Brønfort G. Efficacy of manual therapes of the spine. Vrije University, Amsterdam, 1997.
(92) Simons DS, Travell JG, Simons LS. Myofascial Pain and Dysfunction. The trigger point manual.2[1], 1-1029. 1999. Baltimore, Williams & Wilkins.

35
(93) Berman DS, Kiat H, Friedman JD, Wang FP, van Train K, Matzer L et al. Separate acquisition restthallium-201/stress technetium-99m sestamibi dual-isotope myocardial perfusion single-photonemission computed tomography: a clinical validation study. J Am Coll Cardiol 1993;22(5):1455-1464.
(94) Davidson CD, Bonow RO. Cardiac catheterization. In: Braunwald E, Zipes DP, Libby P, editors.Heart Disease. Philadelphia: W.B. Saunders Company, 2001:359-386.
(95) Wise CM. Chest wall syndromes. Curr Opin Rheumatol 1994;6(2):197-202.
(96) Mukerji B, Mukerji V, Alpert MA, Selukar R. The prevalence of rheumatologic disorders inpatients with chest pain and angiographically normal coronary arteries. Angiology 1995;46(5):425-430.
(97) Bruckner FE, Greco A, Leung AW. 'Benign thoracic pain' syndrome: role of magnetic resonanceimaging in the detection and localization of thoracic disc disease. J R Soc Med 1989;82(2):81-83.
(98) Bruckner FE, Allard SA, Moussa NA. Benign thoracic pain. J R Soc Med 1987;80(5):286-289.
(99) Wolf E, Stern S. Costosternal syndrome - its freguency and importance in differential diagnosis ofcoronary heart disease. Arch Intern Med 136, 189-191. 1976.
(100) Arroyo JF, Jolliet Ph, Junod AF. Costovertebral joint dysfunction: another misdiagnosed cause ofatypical chest pain. Postgrad Med J 1992;68:655-659.
(101) Fam AG, Smythe HA. Musculoskeletal chest wall pain. CMAJ 1985;133(5):379-389.
(102) Johnsen HH. Thoracocostal subluxation syndrome: an often overlooked cause of chest and armpain. Chiropr Tech 7[4], 134-138. 1995.
(103) Rouan GW, Hedges JR, Toltzis R, Goldstein-Wayne B, Brand D, Goldman L. A chest pain clinicto improve the follow-up of patients released from an urban university teaching hospitalemergency department. Ann Emerg Med 1987;16(10):1145-1150.
(104) Fruergaard P, Launbjerg J, Hesse B, Jorgensen F, Petri A, Eiken P et al. The diagnoses of patientsadmitted with acute chest pain but without myocardial infarction. Eur Heart J 1996;17(7):1028-1034.
(105) Walker BF, Buchbinder R. Most commonly used methods of detecting spinal subluxation and thepreferred term for its description: a survey of chiropractors in Victoria, Australia. J ManipulativePhysiol Ther 1997;20(9):583-589.
(106) Troyanovich SJ, Harrison DD, Harrison DE. Motion palpation: it's time to accept the evidence. JManipulative Physiol Ther 1998;21(8):568-571.
(107) Russell R. Diagnostic palpation of the spine: a review of procedures and assessment of theirreliability. J Manipulative Physiol Ther 1983;6(4):181-183.
(108) Breen A. The reliability of palpation and other diagnostic methods. J Manipulative Physiol Ther1992;15(1):54-56.
(109) Herzog W, Kats M, Symons B. The effective forces transmitted by high-speed, low-amplitudethoracic manipulation. Spine 2001;26(19):2105-2110.
(110) Haas M, Raphael R, Panzer D, Peterson D. Reliability of manual end-play palpation of the thoracicspine. Chiropractic Technique 1995;7[4]:120-124.

36
(111) Love RM, Brodeur RR. Inter- and intra-examiner reliability of motion palpation for thethoracolumbar spine. J Manipulative Physiol Ther 1987;10(1):1-4.
(112) Boline PD, Haas M, Meyer JJ, Kassak K, Nelson C, Keating-JC J. Interexaminer reliability ofeight evaluative dimensions of lumbar segmental abnormality: Part II [see comments]. JManipulative Physiol Ther 1993;16(6):363-374.
(113) Levoska S, Keinänen-Kiukaanniemi S, Bloigu R. Repeatability of measurement of tenderness inthe neck-shoulder region by dolorimeter and manual palpation. The Clinical Journal of Pain1993;9[4]:229-235.
(114) Ho M, Walker S, McGarry F, Pringle S, Pullar T. Chest wall tenderness is unhelpful in thediagnosis of recurrent chest pain. QJM 2001;94(5):267-270.
(115) Frobert O, Fossgreen J, Sondergaard-Petersen J, Hede J, Bagger JP. Musculo-skeletal pathology inpatients with angina pectoris and normal coronary angiograms. J Intern Med 1999;245(3):237-246.
(116) Braunwald E, Perloff JK. Physical examination of the heart and circulation. In: Braunwald E,Zipes DP, Libby P, editors. Heart Disease. Philadelphia: W.B. Saunders Company, 2001: 45-81.
(117) Friis J, Junker P, Manniche C, Petersen J, Steengaard-Pedersen K. Reumatologi. 1ed ed.Copenhagen: FADL's forlag, 2001.
(118) Peterson DH, Bergmann TF. Joint Assesment Principles and Procedures. In: Bergmann TF,Peterson DH, Lawrence DJ, editors. Chiropractic Technique. New York: Churchill LivingstoneInc, 1993: 51-122.
(119) Vach W. Classification trees. Computational Statistics 1995;(10):9-14.
(120) Mortensen PS. Angina pectoris - pseudoangina pectoris. Nordisk Medicin 1963;69[23].
(121) Hansen PH, Duel P. Angina Pectoris. Ugeskr Læger 1982;144, 50-51.
(122) Wax CM, Abend DS, Pearson PH. Chest pain and the role of somatic dysfunction. J Am OsteopathAssoc 1997; 97(6):347-52,355.
(123) Polkinghorn BS, Colloca CJ. Chiropractic management of chronic chest pain using mechanicalforce, manually assisted short-lever adjusting procedures. J Manipulative Physiol Ther 2003;26(2):108-115.
(124) Barker ME. Manipulation in general medical practice for thoracic pain syndromes. Br OsteopathicJ 1983;15:95-97.
(125) Rogers JT, Rogers JC. The role of osteopathic manipulative therapy in the treatment of coronaryheart disease. J Am Osteopathic Ass 1976;76:71-81.
(126) Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratioscale measures for chronic and experimental pain. Pain 1983; 17(1):45-56.
(127) Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain 1975;1(3):277-299.
(128) Wulff HR, Gøtzsche PC. Rational diagnosis and treatment: evidence-based clinical decisionmaking. 3rd ed. London: Blackwell Science Ltd, 2000.
(129) Bronfort G, Evans R, Nelson B, Aker PD, Goldsmith CH, Vernon H. A randomized clinical trial ofexercise and spinal manipulation for patients with chronic neck pain. Spine 2001; 26(7):788-797.

37
(130) Hoving JL, Koes BW, de Vet HC, van der Windt DA, Assendelft WJ, van Mameren H et al.Manual therapy, physical therapy, or continued care by a general practitioner for patients withneck pain. A randomized, controlled trial. Ann Intern Med 2002; 136(10):713-722.
(131) Elliott AM, Smith BH, Hannaford PC, Smith WC, Chambers WA. Assessing change in chronicpain severity: the chronic pain grade compared with retrospective perceptions. Br J Gen Pract2002; 52(477):269-274.
(132) Fischer D, Stewart AL, Bloch DA, Lorig K, Laurent D, Holman H. Capturing the patient's view ofchange as a clinical outcome measure. JAMA 1999; 282(12):1157-1162.
(133) Spertus JA, Winder JA, Dewhurst TA, Deyo RA, Prodzinski J, McDonell M et al. Developmentand evaluation of the Seattle Angina Questionnaire: a new functional status measure for coronaryartery disease. J Am Coll Cardiol 1995; 25(2):333-341.
(134) Goldman L, Hashimoto B, Cook EF, Loscalzo A. Comparative reproducibility and validity ofsystems for assessing cardiovascular functional class: advantages of a new specific activity scale.Circulation 1981; 64(6):1227-1234.
(135) Hlatky MA, Boineau RE, Higginbotham MB, Lee KL, Mark DB, Califf RM et al. A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). AmJ Cardiol 1989; 64(10):651-654.

38
12. APPENDIX

Part project I

ORIGINAL ARTICLES
PALPATION OF THE UPPER THORACIC SPINE:AN OBSERVER RELIABILITY STUDY
Henrik Wulff Christensen, DC, MD,a Werner Vach, PhD,c Kirstin Vach, MSc,c Claus Manniche, MD, DMSc,d
Torben Haghfelt, MD, DMSc,b Lisbet Hartvigsen, DC, DMSc,b and Poul Flemming Høilund-Carlsen, MD, DMSca
ABSTRACT
Objective: To assess the intraobserver reliability (in terms of hour-to-hour and day-to-day reliability)and the interobserver reliability with 3 palpation procedures for the detection of spinal biomechanicdysfunction in the upper 8 segments of the thoracic spine.
Design: A repeated-measures design was used in all substudies.
Setting: Department of Nuclear Medicine, Odense University Hospital, Denmark.
Participants: Two chiropractors examined 29 patients and 27 subjects in the interobserver part and 1chiropractor examined 14 patients and 15 subjects in the intraobserver studies.
Intervention: Three types of palpation were performed: Sitting motion palpation and prone motionpalpation for biomechanic dysfunction and paraspinal palpation for tenderness. Each dimension was ratedas “absent” or “present” for each segment. All examinations were performed according to a standardwritten procedure.
Results: Using an “expanded” definition of agreement that accepts small inaccuracies (�1 segment) inthe numbering of spinal segments, we found—based on the pooled data from the thoracic spine—kappavalues of 0.59 to 0.77 for the hour-to-hour and the day-to-day intraobserver reliability with all 3 palpationprocedures. Kappa coefficients were 0.24 and 0.22 for the interobserver reliability with prone and sittingmotion palpation and 0.67 and 0.70, respectively, with paraspinal palpation for tenderness.
Conclusion: With expanded agreement we found good hour-to-hour and day-to-day intraobserverreliability with all 3 palpation procedures and good interobserver reliability for paraspinal tenderness. Theinterobserver reliability was unacceptably poor with prone and sitting motion palpation. (J ManipulativePhysiol Ther 2002;25:285-92)
Key Indexing Terms: Observer Variation; Reliability; Chest Pain; Thoracic Spine; Chiropractic
aDepartment of Nuclear Medicine, Odense University Hospital,Denmark,
bDepartment of Cardiology, Odense University Hospital, Denmark,cDepartment of Statistics and Demography, University of
Southern Denmark, Denmark,dBack Clinic, Ringe Hospital, Denmark.ePrivate practice of chiropractic.This study was supported by the Nordic Institute of Chiropractic
and Clinical Biomechanics, Odense, Denmark, and the Foundationfor the Advancement of Chiropractic Research and PostgraduateEducation, Denmark.
Submit reprint requests to: Henrik Wulff Christensen, DC, MD,Department of Nuclear Medicine, Odense University Hospital,Sdr. Bouldvard 29, DK-5000 Odense C, Denmark (e-mail: [email protected]).
Paper submitted February 13, 2001; in revised form March 15,2001.
Copyright © 2002 by JMPT.0161-4754/2002/$35.00 � 0 76/1/124424doi:10.1067/mmt.2002.124424
285

INTRODUCTION
The diagnosis of biomechanic dysfunction is funda-mental to disease classification within the muscu-loskeletal system.1 Palpation is the method of
choice for diagnosis of biomechanical dysfunction. Text-books on chiropractic describe comprehensively palpatorytechniques2,3 to identify a biomechanical dysfunction in thespinal column suitable for manipulation. Similarly, otherdisciplines that practice manual therapy use palpation as anassessment tool for mechanical musculoskeletal dysfunc-tion.4,5 Consequently, in clinical trials comparing groups ofpatients and in the routine focusing on individual patients,knowledge of the reliability of palpation as a diagnosticmeans is crucial.
We wanted to examine the role of symptomatology of themusculoskeletal component in a clinical trial on patientswith stable angina pectoris. Before doing this we had tochoose and test the relevant palpation procedures becausereports in peer-reviewed literature on the reliability of pal-pation procedures in the thoracic region are sparse.
Because no gold standard for the finding and grading ofspinal segmental dysfunction exists, we examined differentaspects of observer reliability. The aim was to test theintraobserver reliability (in terms of hour-to-hour and day-to-day reliability) and the interobserver reliability with 3palpation procedures in the detection of spinal dysfunctionin the upper thoracic spine. Only those procedures with“acceptably high” reliability would be feasible in our laterclinical trial on patients with stable angina pectoris. The 3procedures were (1) prone motion palpation, (2) sittingmotion palpation, and (3) palpation for paraspinal tender-ness.
METHODS
Study PopulationA total of 107 subjects without suspicion of rheumatic
inflammatory disease or fibromyalgia were scheduled totake part in the study. Of these, 51 were patients (18females, 33 males), median age 61 years (range 31-74), whowere referred consecutively to the Department of Cardiol-ogy because of known or suspected stable angina pectorislasting more than 3 months. The remaining 56 were controlsubjects (21 females, 35 males), median age 56 years (range39-68), from the Department of Nuclear Medicine whofulfilled the following criteria: a history without heart dis-ease, a normal resting electrocardiogram, and no chest pain.Twenty-two subjects dropped out for various reasons: with-drawal of consent (8), did not show up (7), coronary an-giography performed between time of consent and biome-chanical examination (5), and other causes (2). Of theremaining 43 patients and 42 controls, 29 and 27, respec-tively, were enrolled in the interobserver reliability protocol(of these, 12 and 15, respectively, took part in the hour-to-hour intraobserver protocol), and 14 and 15, respectively,
participated in the day-to-day intraobserver protocol. Theproject was approved by the local ethics committee and allsubjects gave oral and written informed consent.
DesignTwo experienced chiropractors (observers A and B) con-
ducted the interobserver part of the study, and observer Aundertook the intraobserver parts. The examination proce-dures were thoroughly practiced between the examiners in a4-hour training session followed by a small pilot seriesincluding 8 patients. A third person without knowledge ofthe clinical findings instructed the subjects on the day of theexamination about the protocol and recorded their demo-graphics. Each observer was blind to subjects’ characteris-tics and to the findings of the other observer. Similarly, thesubjects were blind to the findings of the 2 observers.
In the hour-to-hour intraobserver part, all subjects werereexamined in random order within an interval of 1 1/2-2hours. The intra- and interobserver studies were done within10 days. Observer A saw 14 to 22 subjects on a single dayand observer B examined 5 to 8 subjects in addition toseveral private patients in her clinic (15-20 on a single day).In the day-to-day part, all subjects were examined at thesame hour on 2 consecutive days. In both intraobserverparts, the heads of the subjects were covered by a balaclavahelmet at the repeat examination. In the interobserver part,one half of the patients were examined first by observer A,whereas the other half was examined first by observer B. Itwas determined by random numbers which observer was thefirst to palpate.
Examination ProtocolThree types of palpation3 were carried out in the follow-
ing order:1. Sitting motion palpation for end-play restriction in
lateral flexion and rotation segmentally (sitting).2. Prone motion palpation for joint-play evaluation seg-
mentally (prone).3. Paraspinal palpation for tenderness segmentally
(prone).Each dimension was rated as 0 � absence of abnormality,
or 1 � presence of abnormality. All examinations werecarried out according to a standard written procedure. First,the subjects were seated on a chair with arms next to theirsides. The spinous process of vertebra T1 was marked bythe first examiner. In the sitting position, sitting motionpalpation of the upper thoracic spine (vertebrae T1-T8) wasperformed. Next, the patients were asked to lie prone on theexamination table for prone motion palpation of the spinalcolumn and palpation for paraspinal tenderness over thezygapophyseal joints at the thoracic spine (vertebrae T1-T8).
286 Christensen et al Journal of Manipulative and Physiological TherapeuticsThoracic Spine Palpation June 2002

Agreement DefinitionTraditionally, agreement between 2 observers is defined
as “strict agreement”, (ie, an exact concordance between theobservers’ findings). The straight-forward application ofthis idea in the present context would be to consider 2observers as agreeing with respect to a single vertebralsegment if they made the same positive finding in exactlythe same segment (eg, vertebra T4).
However, this definition is too narrow for the followingreasons. In case of a mechanical pain condition in thethoracic spine, treatment decisions do not depend on thepalpation of a specific segment. Usually an “area” of symp-toms is treated with spinal manipulative therapy rather thana specific vertebral segment. Therefore, the exact location ofa finding among the vertebral segments is not relevant in theclinical setting when the location determined by 2 observersdiffers by a single segment. However, the traditional “strictagreement” requires that examiners locate exactly the samesegment. From a clinical point of view and in the decisionon specific manipulative therapy, the numbering of a certainsegmental level is not essential as long as the area to betreated is correctly identified manually, or as long as thesame segment is being treated by the different observersalthough they may number it differently. (eg, �1 segment).6
We decided that agreement with regard to the localization ofan abnormal finding was present if it was reproduced on thesecond occasion in exactly the same vertebral segment or ina neighboring segment, this we termed “expanded agree-ment.” Hence, we regarded 2 decisions as disagreeing if andonly if one observer recorded a positive finding in a certainsegment and the other observer recorded a negative findingin the same segment and in the 2 neighboring segments (Fig1). In the cranial and caudal parts of the thoracic region
examined, we only used the available 2 segments to deter-mine the expanded agreement.
Statistical AnalysisThe frequencies of a positive finding were computed for
sitting motion palpation, prone motion palpation, andparaspinal tenderness. Intra- and interobserver reliabilitywas assessed by agreement rates and corresponding kappavalues. The intra- and interobserver reliability were ana-lyzed separately with respect to sitting motion palpation,prone motion palpation, and spinal tenderness on both theleft and right sides of the spine. For all segments wecomputed the 2 rates of agreement, one for “strict agree-ment” and another for “expanded agreement.”
Kappa coefficients were computed for both types ofagreement; details are given in Appendix. For the interpre-tation of kappa values, we refer to the 5 categories asdescribed by Landis and Koch7: poor � 0.20, fair 0.21-0.40,moderate 0.41-0.60, good 0.61-0.80, and very good agree-ment 0.81-1.00. Acceptable reproducibility, ie, clinicallyimportant agreement, was defined a priori as a kappa value�0.50.
For the statistical analyses we applied the program pack-age STATA (Statistical Software 6.0, College Station,Tex.).8
RESULTS
Table 1 shows the results on the basis of pooled data fromall 8 segments in the upper thoracic spine. Thus, it displaysthe prevalences of a positive finding by observers A and B,the data for strict agreement, and the data for expandedagreement with regard to the hour-to-hour intraobserver
Fig 1. Definition of expanded agreement and strict agreement at vertebral segment K. A, Observer A; B, observer B; O, absence;1, presence; x, O or 1.
287Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 25, Number 5 Thoracic Spine Palpation

reliability, the day-to-day intraobserver reliability and theinterobserver reliability. The complete data set of segment-specific results for all 8 segements of the upper thoracicspine are shown in Table 2 with respect to the hour-to-hourintraobserver reliability. The corresponding segment-spe-cific results for the day-to-day intraobserver and interob-server reliability are not given.
DISCUSSION
In a clinical setting we would like to regard certainpalpation procedures as accurate measurements of underly-ing biomechanic dysfunction of the spinal column. How-ever, we are unable to assess such agreement by comparisonwith the truth because we are short of infallible referenceprocedures. Hence, we can only estimate the reliability orreproducibility of a procedure (ie, the ability of an observerto agree with himself or with another observer).
We used an appropriate statistical approach for evalua-tion of the reproducibility of spinal palpation,9 acknowledg-ing the clinical experience that the location of a positivefinding may easily vary by one spinal segment. We areaware that the introduction of the “expanded agreement”concept and the consequent better agreement rates andhigher kappa values is debatable. On the other hand, be-cause of the uncertainty in precise anatomic localization,one may also argue that the rates of “strict agreement” andcorresponding kappa values do not do the method justice,because from a clinical point of view, it may be morerelevant to validate the different palpation tools in making apositive diagnosis instead of testing their topographic capa-bilities.
As we deal with comparable biologic changes in differentvertebral segments of the thoracic spine, we can, in addition,expect that the reliability of palpation does not vary muchamong the vertebral segments of this region even if theprevalences of the positive findings vary. Hence, it seemsalso justified to pool the data from adjacent segments and toconsider the overall rate of agreement, counting all subjectsand all segments of that region. This overall rate of “ex-panded agreement” on the basis of the pooled data gives us,of course, nothing else than the arithmetic mean of thesegment-specific agreement rates. However, as these aver-ages pool the information from the different segments, theyand their corresponding kappa values are a more reliabledescription of the diagnostic capability than their segment-specific counterparts. We used symptomatic patients andasymptomatic subjects because restriction to asymptomaticsubjects is not recommended.10
Our FindingsIt appears that comparable papers on the examination of
the thoracic spine do not exist. In our study, the secondobserver reported consistently higher prevalence of positivefindings (Table 2). This alone made perfect agreement im-possible. Still, with our concept of “expanded agreement”using pooled data, we found sitting and prone motion pal-pation kappa values of about 0.6 for the hour-to-hour andfor the day-to-day intraobserver reliability but values ofonly 0.22 and 0.24 for the interobserver reliability (Table 1).This suggests that it is possible to use each single subject ashis or her own control in treatment studies, provided “be-fore” and “after” examinations are performed by the same
Table 1. Prevalences, agreement rates, and kappa values based on pooled analysis of hour-to-hour intraobserver, day-to-dayintraobserver, and interobserver data from examination of the spine, vertebral segments T1 to T8 (95% CI in parentheses)
Strict agreement
CI
Expanded agreement
CIPrevalence
1APrevalence2A or 1B
Relativefrequency Kappa
Relativefrequency Kappa
Hour-to-hour intraobserver data (1A/2A, N � 216)SMP 27 19 0.86 0.13 (–0.66-0.94) 0.94 0.60 (0.00-1.00)PMP 42 40 0.82 0.33 (–0.21-0.87) 0.93 0.68 (0.24-1.00)STL 35 38 0.88 0.57 (0.13-1.00) 0.94 0.77 (0.43-1.00)STR 45 53 0.83 0.50 (0.21-0.92) 0.92 0.73 (0.38-1.00)Day-to-day intraobserver data (1A/2A, N � 232)SMP 25 25 0.88 0.33 (–0.33-0.99) 0.93 0.59 (0.05-1.00)PMP 42 54 0.84 0.45 (–0.01-0.91) 0.91 0.64 (0.22-1.00)STL 40 51 0.81 0.34 (–0.16-0.84) 0.90 0.63 (0.23-1.00)STR 52 61 0.82 0.45 (0.02-0.88) 0.92 0.73 (0.40-1.00)Interobserver data (1A/1B, N � 448)SMP 47 68 0.80 0.00 (–0.52-0.52) 0.86 0.22 (–0.29-0.73)PMP 89 122 0.68 –0.03 (–0.42-0.36) 0.81 0.24 (–0.17-0.65)STL 94 126 0.79 0.38 (0.07-0.69) 0.90 0.67 (0.49-0.93)STR 121 143 0.77 0.38 (0.08-0.68) 0.90 0.70 (0.46-0.94)
SMP, Sitting motion palpation; PMP, prone motion palpation; ST, spinal tenderness at the zygaphophysial joints; L, left; R, right; N, total number ofspinal segments examined; Prevalence 1A, number of positive findings on the first examination by observer A; Prevalence 2A, number of positive findingson the second examination by observer A; Prevalence 1B, number of positive findings on the first examination by observer B.
288 Christensen et al Journal of Manipulative and Physiological TherapeuticsThoracic Spine Palpation June 2002

observers. In contrast, the kappa values representing “strictagreement” indicated a very poor reproducibility close tochance agreement for the segment specific decisions (Table1).
For spinal tenderness we obtained kappa values between0.63 and 0.77 for all 3 kinds of reliability in the pooledanalysis, indicating relatively good reproducibility (Table1). Because we obtained similar kappa values for the intra-and interobserver reliability, we can conclude that thesource of disagreement is related less to the subjectivity ofdifferent observers than to the uncertainty of each singleobserver. Kappa values for the strict agreement were ac-ceptable (0.57 and 0.50) for the hour-to-hour intraobserverreliability, but were equally low for the day-to-day intraob-server reliability (0.34 and 0.45) and the interobserver reli-ability (0.38 and 0.38). This suggests a biologic variation insubjects in the hour-to-hour intraobserver part of the study,
or that relocalization of a specific vertebral segment is moreeasily done on the same instead of different days.
Considering expanded agreement we found no great dif-ferences between hour-to-hour and day-to-day intraobserverreliability for the 3 signs we looked for. Hence, increasingthe interval between 2 examinations from 2 to 24 hours didnot decrease the reliability as a result of a single observer.Apparently, this is the first time this has been demonstratedfor a chiropractic issue.
Other InvestigationsHarvey and Byefield11 also recognized the problem with
inaccurate anatomic localization when using a mechanicmodel for evaluation of spinal motion palpation, and theyalso suggest allowing for localization differing by 1 seg-ment. However, the details of their statistical approachremain unknown. There are only 2 previous reports dealing
Table 2. Prevalences and agreement rates of hour-to-hour intraobserver data for specific vertebral segmental findings of sittingmotion palpation, prone motion palpation, and spinal tenderness in the spine, vertebral segments T1 to T8
Prevalence1A (N � 27)
Prevalence2A (N � 27)
Strict agreement Expanded agreement
Relativefrequency Kappa
Relativefrequency Kappa
SMP T1 3 1 0.93 0.46 0.93 0.46SMP T2 5 1 0.85 �0.15 0.93 0.42SMP T3 5 5 0.85 0.42 0.93 0.67SMP T4 5 6 0.74 0.04 0.85 0.35SMP T5 5 3 0.70 �0.58 0.89 0.35SMP T6 2 2 0.85 �0.50 0.96 0.56SMP T7 1 1 1.00 1.00 1.00 1.00SMP T8 1 0 0.96 �1.00 1.00 1.00PMP T1 2 1 0.96 0.64 0.96 0.64PMP T2 4 2 0.93 0.53 1.00 1.00PMP T3 8 10 0.63 �0.06 0.93 0.68PMP T4 10 13 0.67 0.06 0.93 0.71PMP T5 9 9 0.70 0.14 0.81 0.17PMP T6 5 3 0.78 �0.10 0.89 0.31PMP T7 4 2 0.93 0.59 0.93 0.56PMP T8 0 0 1.00 1.00 1.00 1.00STL T1 0 0 1.00 1.00 1.00 1.00STL T2 7 3 0.85 0.35 0.93 0.70STL T3 4 7 0.81 0.44 0.93 0.76STL T4 5 8 0.89 0.71 0.93 0.78STL T5 6 8 0.93 0.82 0.96 0.88STL T6 5 6 0.81 0.41 0.89 0.63STL T7 5 6 0.89 0.67 0.93 0.77STL T8 3 0 0.89 �0.10 0.96 0.60STR T1 1 0 0.96 0.43 0.96 0.43STR T2 9 7 0.70 0.14 0.85 0.55STR T3 8 7 0.81 0.46 0.93 0.77STR T4 7 9 0.93 0.83 1.00 1.00STR T5 7 10 0.81 0.56 0.89 0.72STR T6 5 9 0.78 0.45 0.85 0.58STR T7 6 10 0.78 0.49 0.85 0.59STR T8 2 1 0.89 0.15 1.00 1.00
SMP, sitting motion palpation; PMP, prone motion palpation; ST, spinal tenderness; T, thoracic spine; L, left; R, right; N, number of subjects.Prevalence 1A, number of positive findings on the first examination by observer A. Prevalence 2A, number of positive findings on the second examinationby observer A.
289Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 25, Number 5 Thoracic Spine Palpation

with the reliability of clinical motion palpation of the tho-racic spine. Hass et al12 found moderate intraobserver reli-ability and poor interobserver reliability with manual end-play palpation of the thoracic spine, which correspondspartially with our figures for strict aggrement, whereas Loveand Brodeur13 found statistically significant agreement forintraobserver reliability but not for interobserver reliabilitywhen the most hypomobile segment was found. Since theyused a semi-quantitative outcome, namely the position, theywere able to use effect measures other than kappa. Hence, itis difficult to compare the magnitude of their results withour binary findings. With regard to tenderness in the tho-racic region, no studies are available. Focus has been moreon evaluation of palpation in the cervical spine and lumbarspine, although the thoracic spine is being treated in 40% to45% of patients entering chiropractic clinics.14
Because observer variation exists with almost every di-agnostic procedure, the crucial question is not whether itoccurs. The important thing is whether it is sufficientlysmall to identify or exclude disease in the individual patientwith reasonable certainty.15 The degree of interobservervariation with palpation of biomechanic dysfunction is notlarger than that associated with the recording of manysymptoms and clinical signs in medical practice. Interob-server variation was evaluated in the clinical examination ofpregnant women with pelvic pain. Eight tests with positivesigns in terms of pain had kappa between 0.41 and 0.62.16
Jarlov et al.17 examined the clinical assesment in terms ofobservation and palpation of the thyroid gland and foundinterobserver variation in terms of kappa between – 0.04and 0.54. In another clinical field, Gadsbøll et al18 foundkappa 0.53 to 0.73 for the detection of a displaced apexheart beat compared with kappa 0.00 to 0.16 for palpation ofhepatomegaly in patients with signs of heart failure. Incomparison, Boline et al10 reported kappa coefficients forstrict agreement of interobserver repeatability in the rangeof 0.40 to 0.79 for soft tissue pain in the lumbar spine, andKeating et al.19 found kappa coefficients between 0.10 and0.59 in the same region. In the neck-shoulder region Le-voska et al.20 obtained kappa coefficients of 0.15 to 0.62 forinterobserver repeatability.
Clinical ImplicationsBy changing from strict to expanded agreement, we in-
creased the overall rate of agreement. As kappa values com-pare the observed rate of agreement with the expected rateunder random conditions, and as this expected rate increases,kappa values do not need to increase when changing fromstrict to expanded agreement. However, we always observedhigher kappa values for expanded agreement than for strictagreement. This might indicate that it is essential for a clini-cally relevant evaluation of the reproducibility of palpationtechniques to use the wider definition, because we underesti-mate the reproducibility otherwise. This may explain partiallythe unfavorable results of previous studies on reproducibility.
With respect to sitting and prone motion palpation ourresults suggest that an experienced observer can achieveacceptably low hour-to-hour and day-to-day variability aftera training session as long as exact anatomic localization isless important than the presence or absence of a positivefinding in a certain region (ie, the thoracic spine). In con-trast, a recent review21 concluded that these examinationprocedures appear to have consistently poor agreement inthe lumbar spine.
In addition, our results suggest that after some training, itis possible to obtain an acceptably low intra- and interob-server variability with regard to diagnosing spinal tender-ness in the thoracic spine and to achieve results comparableto those reported from palpation of other spinal re-gions.10,20,21 Thus we can conclude that a good reproduc-ibility among 2 observers with respect to diagnosing spinaltenderness can be achieved after some training, but that suchtraining is not sufficient to achieve an acceptable reproduc-ibility with respect to sitting or prone palpation.
Limitations of the StudyFirst, the blinding in the hour-to-hour intraobserver part was
not ideal, since the clothing of the subjects was not altered andbecause we obviously could not change their voices and otherpersonal characteristics. This may, in part, explain the higherkappa values for strict agreement with regard to the hour-to-hour compared with the day-to-day interobserver agreement(Table 1). Second, because of the small size of the studygroups, the prevalences of some of the positive findings werelimited, causing less than ideal conditions for the statisticalevaluation, especially for segment specific analyses. Third,palpation itself has a number of inherent sources of error, someof which deserve further mention.
It is conceivable that areas that were not painful at thefirst examination could become so after a second examina-tion. This source of error was intended to be the same foreach observer by reversing the order of observers half waythrough the examination series. A narrow instead of a widecontact area of palpation and a higher pressure could, intheory, produce a positive finding which was negative onpalpation with a wide contact area at a lower finger pressure.In fact, it has been demonstrated by computerized pressurealgometry on small joints that the pressure rate and thepressure area are crucial for the patient’s experience ofpain.22 Moreover, exact identification of anatomical land-marks is difficult and made us use the extended definition ofagreement and correponding kappa values. This phenome-non may have a greater role in the thoracic spine wherelandmarks are limited to the spinous process of the firstthoracic vertebrae than in the lumbar spine with its morefixed points de repere (iliac crest, posterior superior iliacspine, sacrum) or in the cervical spine (occiput). Further,interpretation of a positive finding is a subjective matter.Two clinicians may have different thresholds for the detec-tion of a certain mechanical dysfunction, and even the same
290 Christensen et al Journal of Manipulative and Physiological TherapeuticsThoracic Spine Palpation June 2002

observer may exhibit different levels from time to time. Inaddition, the patient’s own experience of tenderness and ofbeing examined may vary with the observer (tall or small,handsome or ugly, male or female) and from time to time.
CONCLUSION
All kappa values for strict agreement were low (�0.50),whereas when using the more appropriate alternative ofexpanded agreement, kappa values indicated good agree-ment with regard to the hour-to-hour intraobserver reliabil-ity (with reservation for a less than perfect masking of thestudy subjects) and moderate to good agreement for theday-to-day intraobserver reliability. However, the interob-server variation was still unacceptably high for prone mo-tion palpation and sitting motion palpation. With this res-ervation, we have established a protocol for examinationand reexamination with an acceptably low intraobservervariation (in terms of hour-to-hour and day-to-day varia-tion) for prone motion palpation, sitting motion palpation,and the presence of spinal tenderness.
REFERENCES
1. World Health Organization. International statistical classi-fication of diseases and related health problems, 10th ed.Geneva: Office of Publication, World Health Classification,Geneva, Switzerland; 1992. p. 676.
2. Schafer RC, Faye LJ. Motion palpation and chiropractictechnic, 1st ed. Huntington Beach, CA: The Motion Palpa-tion Institute; 1989. 143-92.
3. Peterson DH, Bergmann TF, Lawrence DJ. Chiropractictechnique, 1st ed. New York, NY: Churchill Livingstone;1993. p. 51-122.
4. Hamberg J, Lindahl O. Angina pectoris symptoms causedby thoracic spine disorders. Clinical examination and treat-ment. Acta Med Scand Suppl 1981;644(suppl):84-6.
5. Bechgaard P. Segmental thoracic pain in patients admittedto a medical department and a coronary care unit. Acta MedScand 1981;644:(suppl) 87-9.
6. Breen A. The reliability of palpation and other diagnosticmethods. J Manipulative Physiol Ther 1992;15:54-6.
7. Landis JR, Koch GG. The measurement of observer agree-ment for categorical data. Biometrics 1977;33(1):159-74.
8. Fleiss JL. Statistical methods for rates and proportions, 2nded. New York, NY: John Wiley and Sons; 1981. p. 222.
9. Haas M. Statistical methodology for reliability studies. JManipulative Physiol Ther 1991;14:119-32.
10. Boline PD, Haas M, Meyer JJ, Kassak K, Nelson C, Keat-ing JC. Interexaminer reliability of eight evaluative dimen-sions of lumbar segmental abnormality: Part II. J Manipu-lative Physiol Ther 1993;16:363-74.
11. Harvey D, Byfield D. Preliminary studies with a mechan-ical model for the evaluation of spinal motion palpation.Clin Biomech 1991;6:679-82.
12. Haas M, Raphael R, Panzer D, Peterson D. Reliability ofmanual end-play palpation of the thoracic spine. ChiroprTechnique 1995;7:120-4.
13. Love RM, Brodeur RR. Inter- and intra-examiner reliabilityof motion palpation for the thoracolumbar spine. J Manip-ulative Physiol Ther 1987;10:1-4.
14. Leboeuf YC, Andren JA, Gernandt M, Malmqvist S. Qual-
ity assurance in chiropractic practice: a comparison of twostudy methods. J Manipulative Physiol Ther 1996;19:513-7.
15. Gjorup T, Hendriksen C, Bugge PM, Jensen AM. Globalassessment of patients—a bedside study. II. Inter-observervariation and frequency of clinical findings. J Intern Med1990;228:147-50.
16. Wormslev M, Juul AM, Marques B, Minck H, Bentzen L,Hansen TM. Clinical examination of pelvic insufficiencyduring pregnancy. An evaluation of the interobserver vari-ation, the relation between clinical signs and pain and therelation between clinical signs and physical disability.Scand J Rheumatol 1994;23:96-102.
17. Jarlov AE, Hegedus L, Gjorup T, Hansen JM. Observervariation in the clinical assessment of the thyroid gland.J Intern Med 1991;229:159-61.
18. Gadsbøll N, Hoilund-Carlsen PF, Nielsen GG, Berning J,Bruun NE, Stage P, et al. Symptoms and signs of heartfailure in patients with myocardial infarction: Reproduc-ibility and relationship to chest X-ray, radionuclide ven-triculography and right heart catheterization. Eur Heart J1989;10:1017-28.
19. Keating JC, Bergmann TF, Jacobs GE, Finer BA, Larson K.Interexaminer reliability of eight evaluative dimensions oflumbar segmental abnormality. J Manipulative PhysiolTher 1990;13:463-70.
20. Levoska S, Keinanen-Kiukaanniemi S, Bloigu R. Repeat-ability of measurement of tenderness in the neck-shoulderregion by dolorimeter and manual palpation. Clin J Pain1993;9:229-35.
21. Hestbæk L, Leboeuf-Yde C. Are chiropractic tests for thelumbo-pelvic spine reliable and valid? A systematic criticalliterature review. J Manipulative Physiol Ther 2000;23:258-75.
22. Jensen, M.P. Computer controlled pressure algometry inhuman joints, Ph.D. thesis, University of Aarhus; 1999.
23. Altman DG. Practical statistics for medical research, 1st ed.London: Chapman & Hall; 1995.
APPENDIX
The kappa coefficient tries to adjust raw rates of a agree-ment for random agreement. The general formula is:
� �A � EA
1 � EA
where A denotes the rate of agreement and EA the corre-sponding expected value under the assumption of indepen-dence. Considering strict agreement at a specific vertebralsegment, formulas for EAk (ie, the expected rate of agree-ment at segment k is well-known).23 For the expandedagreement the expected value at segment k is equal to
EAk � p01k � p0
2k � p11k � p1
2k � p12k � p1
1k � p11k � p1
2k with
p0ik � P� xk � 0 for observer i�
p1ik � P� xk � 1 for observer i�
p1ik � P� xk�1 � 1 or xk � 1 or xk�1 � 1 for observer i�
with xk denoting the finding at segment k. In the segment
291Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 25, Number 5 Thoracic Spine Palpation

specific analysis, we have computed a specific EAk whichwe obtain by replacing propabilities with the correspondingrelative frequencies. In this case, the kappa coefficient forexpanded agreement is a special case of Cohen’s weightedkappa.23 For the pooled analysis one computes EA as the
averages of the EAk.Standard errors are based on Cohen’s formula, using
the number of patients as the sample size. This is a conser-vative approach taking the dependence among the segmentswithin a patient into account.
292 Christensen et al Journal of Manipulative and Physiological TherapeuticsThoracic Spine Palpation June 2002

Part project II

ORIGINAL ARTICLES
PALPATION FOR MUSCULAR TENDERNESS IN THE
ANTERIOR CHEST WALL: AN OBSERVER RELIABILITY
STUDY
Henrik Wulff Christensen, DC, MD,a Werner Vach, PhD,b Claus Manniche, MD, DMSc,c
Torben Haghfelt, MD, DMSc,d Lisbet Hartvigsen, DC,e and Poul Flemming Høilund-Carlsen, MD, DMScf
ABSTRACT
Objective: To asses the interobserver and intraobserver reliability (in terms of day-to-day and hour-to-hourreliability) of palpation for muscular tenderness in the anterior chest wall.
Design: A repeated measures designs was used.
Setting: Department of Nuclear Medicine, Odense University Hospital, Denmark.
Participants: Two experienced chiropractors examined 29 patients and 27 subjects in the interobserver part, and 1of the 2 chiropractors examined 14 patients and 15 subjects in the intraobserver studies.
Intervention: Palpation for muscular tenderness was done in 14 predetermined areas of the anterior chest wallwith all subjects sitting. Each dimension was rated as absent or present for tenderness or pain for each location. Allexaminations were carried out according to a standard written procedure.
Results: Based on a pooled analysis of data from palpation of the anterior chest wall, we found � values of 0.22 to0.31 for the interobserver reliability. For the intraobserver reliability, we found � values of 0.21 to 0.28 for the day-to-day reliability and 0.44 to 0.49 for the hour-to-hour reliability.
Conclusion: Our results indicated great variations between experienced chiropractors palpating for intercostaltenderness or tenderness in the minor and major pectoral muscles in a population of patients with and without chestpain. This may hamper the ability of clinicians to diagnose and classify the musculoskeletal component of chest painif based exclusively on palpation of the anterior chest wall. (J Manipulative Physiol Ther 2003;26:469-75)
Key Indexing Terms: Observer Variation; Reliability; Tenderness; Chest Pain
INTRODUCTION
The concept of diagnosing muscular tendernesswith manual palpation is well known within dif-ferent clinical disciplines such as cardiology,
rheumatology, chiropractic, physical therapy, and manualmedicine.
Several authors have described palpation for musculartenderness in the chest wall as a tool to diagnose andclassify patients with different clinical presentations of painalbeit without a prior evaluation of the method used.1-3
There are no generally accepted biochemical, electro-myographic, or diagnostic imaging criteria for the diagnosisof tenderness in muscles. This leaves manual palpationskills, in conjunction with feedback from the patient, for
aPhD student, Nuclear Medicine, Odense University Hospital,Odense, Denmark.
bProfessor, Department of Statistics and Demography, Univer-sity of Southern Denmark, Odense, Denmark.
cProfessor, Back Clinic, Ringe Hospital, Ringe, Denmark.dProfessor, Cardiology, Odense University Hospital, Odense,
Denmark.ePrivate practice of chiropractic, Odense, Denmark.fProfessor, Nuclear Medicine, Odense University Hospital,
Odense, Denmark.Submit requests for reprints to: Henrik Wulff Christensen, De-
partment of Nuclear Medicine, Odense University Hospital, Sdr.Boulevard 29, DK-5000 Odense C, Denmark (e-mail:[email protected]).
Paper submitted June 06, 2002.Copyright © 2003 by National University of Health Sciences.0161-4754/2003/$30.00 � 0doi:10.1067/S0161-4754(03)00103-9
469

diagnosis and treatment. However, this approach can bequestioned due to lack of validation studies demonstratingthat palpation can reliably identify tenderness, triggerpoints, and tender points in soft tissues.
This is a problem not only in clinical trials comparinggroups of patients but also in the routine evaluation ofindividual patients in clinical practice. In both settings,knowledge of the reliability of manual palpation as a diag-nostic tool is crucial.
An upcoming clinical trial examining the role of muscu-loskeletal components in patients with stable angina pecto-ris required the selection and testing of the relevant manualpalpation procedures. In a previous work,4 we tested 3 typesof manual palpation of the posterior chest wall: seated andprone motion palpation for biomechanical dysfunction andparaspinal palpation for tenderness. We found good inter-observer reliability for left and right paraspinal tenderness(� � 0.67 and 0.70) but not for prone and sitting motionpalpation (� � 0.22 and 0.24). Further, there was goodday-to-day and hour-to-hour intraobserver reliability withall 3 procedures (� � 0.59-0.77). The current article ad-dresses the continuation of this work, namely the testing ofmanual palpation of the anterior chest wall.
Since no gold standard exists for the finding and gradingof chest wall tenderness, we were unable to examine theaccuracy (agreement with truth)5 of the chosen palpationapproach. We could, however, study different aspects ofobserver reliability. The aim was to test the interobserverreliability and the intraobserver reliability (in terms of day-to-day and hour-to-hour reliability) with palpation of 14predetermined points used to diagnose pectoralis and inter-costal myosis of the anterior chest wall in patients with andwithout angina pectoris.
METHODS
Study PopulationThe study population has been thoroughly described in a
previous publication.4 In short, 85 subjects took part in thepresent study. Of these, 43 were patients referred consecu-tively for coronary angiography because of known or sus-pected stable angina pectoris. The remaining 42 were con-trol subjects without symptoms and signs of heart disease,all of whom had a normal resting electrocardiogram and nochest pain. Twenty-nine patients and 27 controls, respec-tively, were enrolled in the interobserver reliability protocol(of these, 12 patients and 15 controls took part in thehour-to-hour intraobserver protocol), and 14 patients and 15controls participated in the day-to-day intraobserver proto-col.
The local ethics committee approved the project and allsubjects gave oral and written informed consent.
DesignTwo experienced chiropractors (observers A and B) car-
ried out the interobserver part of the study and observer A
undertook the intraobserver parts. The examination proce-dures were thoroughly practiced between the examiners in a4-hour training session, followed by a small pilot seriesincluding 8 patients. A third person without knowledge ofthe clinical findings instructed the subjects on the day of theexamination about the protocol and recorded their demo-graphics. Each observer was blind to the subjects’ charac-teristics and to the findings of the other observer. Similarly,the subjects were blind to the findings of the 2 observers.
The complete interobserver and intraobserver studieswere done within 10 days. So, observer A saw 14 to 22subjects on a single day, and observer B examined 5 to 8subjects plus 15 to 20 private patients in her clinic on asingle day. In the interobserver part, one half of the patientswere examined first by observer A, while the other half wereexamined first by observer B. It was determined by randomnumbers which observer was the first to palpate.
In the day-to-day part, all subjects were examined at thesame hour on 2 consecutive days. In the hour-to-hour in-traobserver part, all subjects were reexamined in randomorder within an interval of 1.5 to 2 hours. In both intraob-server parts, a balaclava helmet covered the heads of thesubjects at the repeat examination in an attempt to keep theobserver blinded to the subjects’ identities.
Examination ProtocolManual palpation was performed on 14 points of the
anterior chest wall (Fig 1). The pectoralis major points(PeMa) were located at the anterior axillary line 3 cm caudalto the clavicles (Fig 1, points 1 and 8). The pectoralis minorpoints (PeMi) were located at the medioclavicular lines justcaudal to the clavicles (Fig 1, points 2 and 9). Points 3through 7 and 10 through 14 were located lateral to thesternum at the intercostal space between II/III to VI/VII, oneach side of the anterior chest wall.
The palpation findings were rated as 0 � absence ofabnormality, 1 � presence of tenderness, and 2 � presenceof severe tenderness (pain). In our analysis; we do notdistinguish between ratings 1 and 2 (ie, we regard bothvalues just as a positive finding). All examinations werecarried out according to a standard written procedure. Thesubjects were seated on a chair with arms down along theirsides. The anterior chest wall was examined prior to thethoracic spine and the paraspinal region.4 A flat digitalindex contact with a standardized pressure was used formanual palpation.
Agreement DefinitionWe decided that agreement with regard to the localization
of tenderness was present if it was reproduced on the secondoccasion in exactly the same location. Hence, we regarded2 decisions as disagreeing, if 1 observer recorded a positivefinding in a certain segment and the other observer recordeda negative finding at the same location.
470 Christensen et al Journal of Manipulative and Physiological TherapeuticsChest Wall Tenderness October 2003

In the previous study, focusing on the thoracic spine andthe paraspinal region, we introduced the concept of “ex-panded agreement,” acknowledging that in the clinical ex-perience the location of a positive finding may easily varyby 1 spinal segment.4 However, when it comes to palpationof the anterior chest wall, we did not expect the sametopographic uncertainty among observers in locating a pre-cise anatomic point. Hence, in the present study, we did notuse the concept of expanded agreement.
Statistical AnalysisThe prevalence of a positive finding was computed for
anterior chest wall tenderness. Interobserver and intraob-server reliabilities were assessed by agreement rates andcorresponding � values. The interobserver and intraobserverreliabilities were analyzed separately with respect to each ofthe 14 predetermined points of the anterior chest wall. Forall locations, we calculated the relative frequency of agree-ment (ie, sum of positive and negative findings), which the2 observers agreed on, expressed as a fraction of the totalpossible number of findings. Additionally, data were pooledfrom comparable points4 to consider the overall rate ofagreement, and analysis was performed in a similar fashion.In doing this, we considered points 1, 2, 8, and 9 as com-parable, as well as locations 3 through 7 and 10 through 14.
Kappa coefficients were computed and standard errorswere based on Cohen’s formula, using the number of pa-tients as the sample size.4 This is a conservative approach,taking the dependence among the points within a patientinto account. For the interpretation, we referred to the 5arbitrary categories proposed by Landis and Koch6: poor �0.20, fair 0.21 to 0.40, moderate 0.41 to 0.60, good 0.61 to0.80, and very good agreement 0.81 to 1.00. Acceptablereproducibility (ie, clinically important agreement) was de-fined arbitrarily a priori as a � value � 0.50.
For the statistical analyses, we used STATA (Stata Corp,College Station, Tex) version 6.0 program package.7 Abinary response was used in the analysis: 0 � absence oftenderness, 1 � presence of tenderness.
RESULTS
Table 1 shows data for the interobserver reliability withpalpation of the 14 points on the anterior chest wall fortenderness. Thus, it displays the prevalences of the positivefindings made by observers A and B, the relative frequen-cies of agreement, and the corresponding � values. Theday-to-day intraobserver reliability and the hour-to-hourintraobserver reliability data are listed in Tables 2 and 3,respectively. In Table 4, a pooled analysis is shown forcomparable points of the 3 kinds of observer reliability.
DISCUSSION
Procedures for manual palpation of the anterior chest wallare used in the daily clinical routine of many specialties asa diagnostic tool to classify a possible muscular component
Fig 1. Location of the 14 palpation points of the anterior chestwall.
Table 1. Interobserver reliability
Location
Prevalences of positivefindings Agreement
ObserverA1
ObserverB1
Relativefrequency Kappa
1 Right 20 39 0.61 0.192 24 37 0.66 0.243 21 26 0.70 0.194 17 20 0.73 0.295 15 18 0.77 0.386 14 17 0.73 0.237 15 20 0.73 0.368 Left 19 38 0.55 0.139 22 40 0.64 0.29
10 16 27 0.70 0.2711 18 18 0.64 0.0312 16 15 0.80 0.4413 11 18 0.80 0.4614 11 21 0.68 0.24
Results obtained in 56 study subjects (29 patients � 27 controls).Prevalences are given as absolute numbers, agreement rates, and kappavalues based on interobserver data from examination of the anterior chestwall (14 predetermined points).
471Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 26, Number 8 Chest Wall Tenderness

of chest pain. Although it would be optimal to ascertain theaccuracy of these procedures, we were unable to do sobecause of the lack of an infallible reference procedure.Hence, we could estimate only the reliability or reproduc-ibility of such a procedure (ie, the ability of an observer toagree with himself or with another observer).8
As we deal with comparable biological changes in dif-ferent locations of the anterior chest wall, we can, in addi-
tion, expect that the reliability of palpation does not varymuch among the predetermined points of this region, evenif the prevalences of the positive findings may vary. Hence,it seems justified to pool4 the data from comparable pointsand to consider the overall rate of agreement, countingoverall subjects and all points.
In the interobserver part of the present study, observer Bconstantly reported higher prevalences of positive findingsthan observer A (Table 1). This systematic difference be-tween observers indicated a different clinical threshold be-tween these examiners, which may not be surprising butmay be difficult to explain. One reason may be that observerB (a female) was more susceptible to the subjects’ reactionsthan observer A (a male). Observer B may have created ahigher palpation pressure per square millimeter than ob-server A due to a smaller index contact area. Observer Bmay have been more aware of other (palpation unrelated)information indicating muscular tenderness. These factorsalone would make perfect agreement impossible. Similarly,in the intraobserver part, observer A, in general, reportedhigher prevalences on the second occasion with both thehour-to-hour and the day-to-day reexaminations (Tables 2and 3). This may have been a result of a “carryover effect,”in that increased local irritation as a result of the initialpalpation was still present at reexamination. Alternatively, itis possible that higher finger pressure on the second occa-sion was exerted because the examiner was more consider-ate on the first contact with the subjects to not produce painon palpation.
The relative frequencies of agreement had somewhatlower values for the interobserver part (0.62 and 0.73) thanfor the intraobserver parts (0.72 and 0.81 and 0.76 and 0.82)(Table 4), indicating, as expected, that an observer canbetter reproduce his own findings than those of anotherobserver. The change in time interval from hour-to-hour to1 day did not affect the relative frequencies for the sameobserver. These figures apparently indicated a relativelygood agreement even between and within observers. How-ever, the relative frequencies include the unavoidableamount of agreement between the examiners caused bychance, even if they were guessing. Kappa statistics correctfor this and yielded much lower values (Table 4), indicatingconsiderable disagreement between and within observers.The � values for the hour-to-hour intraobserver reliabilitywere higher than the day-to-day values and more close tothe proposed lower limit of acceptable agreement(� � 0.50). Unfortunately, this points to a larger degree ofbias in the shape of insufficient blinding when palpation isrepeated within a short (hours) compared to a larger timeinterval (days) or to considerable biological variation withtime, or both.
Whatever the reason, all the � values were below 0.50(Table 4), which, in practice, indicate poor agreement, al-though, of course, interpretation must depend on circum-stances. Differences between examiners in terms of inter-
Table 2. Day-to-day intraobserver reliability
Location
Prevalences of positivefindings Agreement
PrevalenceA1
PrevalenceA2
Relativefrequency Kappa
1 Right 6 14 0.66 0.262 9 13 0.72 0.353 6 11 0.55 �0.104 7 7 0.86 0.535 5 4 0.83 0.266 5 3 0.79 0.057 4 3 0.90 0.508 Left 7 8 0.83 0.509 7 8 0.69 0.09
10 4 10 0.79 0.4511 2 5 0.76 �0.2012 2 2 0.93 0.4213 4 2 0.79 �0.1714 1 1 0.93 0.00
Analysis was based on 29 subjects (14 patients � 15 controls). Preva-lences are given as absolute numbers, agreement rates, and kappa valuesbased on day-to-day intraobserver data from examination of the anteriorchest wall (14 predetermined points).
Table 3. Hour-to-hour intraobserver reliability
Location
Prevalences of positivefindings Agreement
ObserverA1
ObserverA2
Relativefrequency Kappa
1 Right 7 12 0.74 0.412 11 14 0.74 0.433 11 12 0.74 0.384 9 10 0.74 0.385 7 6 0.81 0.416 4 4 0.93 0.767 5 4 0.96 0.888 Left 8 10 0.85 0.619 11 13 0.70 0.32
10 9 11 0.70 0.2511 10 9 0.67 0.1312 7 5 0.78 0.2913 4 5 0.96 0.8614 5 5 0.93 0.77
Results from 27 subjects (12 patients � 15 controls). Prevalences aregiven as absolute numbers, agreement rates, and kappa values based onhour-to-hour intraobserver data from examination of the anterior chest wall(14 predetermined points).
472 Christensen et al Journal of Manipulative and Physiological TherapeuticsChest Wall Tenderness October 2003

pretation and fingers size and pressure applied may play aconsiderable role. To compensate for this, different palpa-tion instrumentations, including algometry9 and palpom-etry,10 have been proposed in attempts to make palpationmore objective and repeatable. The former method detectsthe individual mechanical pain threshold, whereas the latterexamines whether or not a given region is tender to palpa-tion with fixed pressure intensity. However, none of theseprocedures have been used for anterior chest wall palpation.
Together, our previous study4 examining the thoracicspine and the paraspinal region and the present study on theanterior chest wall demonstrate that despite exactly thesame amount of training period of manual palpation proce-dures and the same number of trial patients, there aredifferences between the 2 regions in terms of manual pal-pation reliability. Our 2 studies give no obvious explanationfor this finding.
Several authors have introduced palpation for tendernessin the anterior chest wall to categorize and classify patientswith stable angina pectoris or nonanginal chest pain,1-3
despite the fact that the literature lacks reports on thereliability of manual palpation for tenderness in this regionof the body.
Table 5 summarizes a number of studies which havelooked at manual palpation of soft tissue. Hubka andPhelan11 reported good interexaminer reliability (� � 0.68)for locating the most tender of 7 points on each of theparaspinal areas of the cervical region. However, theirmethod was not comparable to our approach, because weexamined the tenderness of all our predetermined points andnot only the most tender ones. Levoska et al,12 on the otherhand, studied manual palpation of tender points in the neckand shoulder region and graded the response as tender/nottender. They found poor to moderate intraexaminer reliabil-ity (� � 0.13-0.47) and poor to good interexaminer reliabil-
ity (� � 0.15-0.62). Keating et al13 studied soft tissuetenderness in the paraspinal lumbar region and found mar-ginal interexaminer reliability (� � 0.30) and good reliabil-ity for osseous tenderness (� � 0.48). In the same region,McCombe et al14 obtained only poor to fair interexaminerreliability for paraspinal tenderness (� � 0.11-0.38). How-ever, since they did not describe their palpation procedure,comparison with their study is impossible. Similar � valueshave been found by others,15,16 but more than half of allstudies do not report prevalences of abnormality, whichrenders interpretation difficult, since the � value dependsheavily on prevalence.
The reliability of manual palpation of muscles for triggerpoints has been examined in several studies. Travel andSimons17 describe the clinical features of trigger points toinclude: (1) a cord-like taut muscle band containing discretenodules; (2) a history of focal tenderness; (3) a local twitchresponse and/or a spontaneous exclamation of pain by thepatient; and, finally, (4) a referred pain pattern.
In a study by Wolfe et al,18 8 different muscles of theupper body were studied for all 5 clinical features of triggerpoints in 8 patients. From data in this study, a � value of0.61 can be calculated for interrater reliability with respectto focal tenderness. Njoo and Van der Does19 had 12 ex-aminers examine 3 sites in the thoracolumbar paraspinalmuscles of 50 patients, resulting in a � value of 0.66 forinterrater reliability of focal tenderness. Finally, Gerwin etal20 found interrater reliability with a � of 0.71 for focaltenderness in 3 muscles of the upper body. All 3 studiesused more than 2 observers and the � value for manyobservers compared to our 2 observers.
The reliability of palpation for tender points in fibromy-algia has been studied to some extent, yielding � values forintraexaminer reliability on 18 different locations of the
Table 4. Prevalences, agreement rates, kappa values, and standard errors (SE) obtained by pooled analysis of interobserver, day-to-day intraobserver, and hour-to-hour intraobserver data
Point
Prevalences of positive findings Agreement
SEObserver
A1ObserverA2 or B1
Relativefrequency Kappa
Interobserver data (A1/B1)PeMa � PeMi (N � 224) 85 154 0.62 0.22 0.13 (�0.04-0.48)Intercostal (N � 560) 154 200 0.73 0.31 0.15 (0.01-0.61)
Day-to-day intraobserver data (A1/A2)PeMa � PeMi (N � 108) 29 43 0.72 0.28 0.21 (�0.14-0.70)Intercostal (N � 270) 40 48 0.81 0.21 0.30 (�0.38-0.80)
Hour-to-hour intraobserver data (A1/A2)PeMa � PeMi (N � 116) 37 49 0.76 0.44 0.19 (0.06-0.82)Intercostal (N � 290) 71 71 0.82 0.49 0.21 (0.08-0.90)
PeMa � PeMi muscles (points 1, 2, 8, and 9), intercostal muscles (point, 3 through 7 and 10 through 14).N � total amount of possible positive and negative findings.95% CI given in parentheses.SE, Standard error.
473Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 26, Number 8 Chest Wall Tenderness

skeleton, ranging from 0.31 to 0.71.21 Interexaminer reli-ability has not been evaluated.
LimitationsAs already pointed out, there are several limitations in
a reproducibility study, such as the present one. Many ofthese have been addressed previously and above.4,22,23
Our results may have been influenced by several otherfactors: the inability to completely blind the observers,the limited numbers of observers, and the relatively fewstudy subjects (but data was pooled to reduce this limi-tation). Both examiners were equally experienced with �10 years of chiropractic practice; therefore, the study tellsnothing about the palpation skills of inexperienced chi-ropractors.
Clinical ImplicationsThe actual presence of tenderness of muscles in the chest
wall is unknown, and its role as a source of nociception inpatients with chest pain is poorly understood. The preva-lence of tenderness in patients with chest pain remainsuncertain, until objective and more repeatable manual pal-pation methods become available. At present, a physician’sfinding of tenderness in the chest wall of a patient withsuspected angina pectoris but without a definite cardiacdiagnosis is often regarded as a sign of intercostal myosis ormyosis of the pectoralis muscles, indicating a musculoskel-etal reason for the chest pain (T. Haghfelt, oral communi-
cation, February 2002). Our results question this line ofdeduction and call for more precise and reliable ways ofestablishing the diagnosis of pectoralis and intercostal my-osis. However, we studied palpation only and, therefore,cannot exclude the possibility that a stepwise workup, in-cluding several relevant items like case history and addi-tional clinical examination and palpation prior to palpationof the anterior chest wall, might lead to a clinically moreuseful result.
CONCLUSION
We undertook this study to examine if palpation fortenderness in the anterior chest wall can be used as a reliablemethod to categorize and classify patients’ chest pain in acoming clinical trial.
All � values were below the arbitrarily chosen limit of0.50 for acceptable agreement, indicating great variationsbetween experienced chiropractors palpating for intercostaltenderness or tenderness in the minor and major pectoralmuscles in subjects with and without chest pain. Thesefindings question the ability of clinicians to reliably diag-nose chest pain from pectoralis and intercostal myosis ifbased solely on manual palpation.
ACKNOWLEDGMENTS
The study was supported by the Nordic Institute of Chi-ropractic and Clinical Biomechanics, Odense, Denmark,
Table 5. Reliability studies of soft-tissue palpation in different areas of the human body
StudyPalpation
for Area/locationType ofvariation
Prevalence ofpositive findings
Agreement(%) Kappa Comments
McCombeet al14
Tenderness Lumbar/paraspinal Interexaminer Not given Not given 0.11 and0.38
Palpation method notdescribed
McCombeet al14
Tenderness Pelvic/gluteal region Interexaminer Not given Not given 0.31 and0.34
Palpation method notdescribed
Keatinget al13
Tenderness Lumbar/paraspinal Interexaminer Given Not given 0.30
Cott et al21 Tenderpoint
Truncus/neck/pelvis,fibromyalgiapoints
Interexaminer Given 78 0.51 Fibromyalgia points (24)
Wolfe et al18 Triggerpoint
Upper truncus Interexaminer Given Not given 0.61 No. calculated fromoriginal data (19)
Levoska et al12 Tenderpoints
Neck-Shoulder/2pair of muscles
Interexaminer Not given 57-85 0.15-0.62Intraexaminer 57-85 0.13-0.47
Boline et al15 Tenderness Lumbar/paraspinal Interexaminer Given 48-90 0.42-0.78Hubka et al11 Tenderness Cervical/paraspinal Interexaminer Not given Not given 0.68 Most tender of 7 pointsNjoo et al19 Trigger
pointLumbar/2 pair of
musclesInterexaminer Not given Not given 0.66
Strender et al16 Tenderness Lumbar/paraspinal Interexaminer Given 72 0.27Gerwin et al20 Trigger
pointTruncus/5 muscle
pairsInterexaminer Not given � 83 0.48-1.00 After training of
examinersChristensen
et al4Tenderness Thoracic/paraspinal Interexaminer Given 68-80 0.38 Strict agreement
Intraexaminer Given 81-88 0.34-0.57Christensen
et al4Tenderness Thoracic/paraspinal Interexaminer Given 81-90 0.67-0.70 Expanded agreement
Intraexaminer Given 90-94 0.63-0.77
474 Christensen et al Journal of Manipulative and Physiological TherapeuticsChest Wall Tenderness October 2003

and the Foundation for the Advancement of ChiropracticResearch and Postgraduate Education, Denmark.
REFERENCES
1. Wise CM, Semble EL, Dalton CB. Musculoskeletal chest wallsyndromes in patients with noncardiac chest pain: a study of100 patients. Arch Phys Med Rehabil 1992;73:147-9.
2. Cooke RA, Smeeton N, Chambers JB. Comparative study ofchest pain characteristics in patients with normal and abnor-mal coronary angiograms. Heart 1997;78:142-6.
3. Wu EB, Smeeton N, Chambers JB. A chest pain score forstratifying the risk of coronary artery disease in patients hav-ing day case coronary angiography. Int J Cardiol 2001;78:257-64.
4. Christensen HW, Vach W, Manniche C, Haghfelt T, Hartvig-sen L, Høilund-Carlsen PF. Palpation of the upper thoracicspine—an observer reliability study. J Manipulative PhysiolTher 2002;25:285-92.
5. Gjorup T. Reliability of diagnostic tests. Acta Obstet GynecolScand 1997;166(Suppl):9-14.
6. Landis JR, Koch GG. The measurement of observer agree-ment for categorical data. Biometrics 1977;33:159-74.
7. Stata statistical software. College Station (TX): Stata Corpo-ration; 2000.
8. Høilund-Carlsen PF. On measuring ventricular ejection frac-tion [doctoral thesis]. Denmark: Copenhagen University;1988.
9. Jensen MP. Computer controlled pressure algometry in humanjoints [PhD thesis]. Denmark: University of Aarhus; 1999.
10. Bendtsen L, Jensen R, Jensen NK, Olesen J. Pressure-con-trolled palpation: a new technique which increases the reli-ability of manual palpation. Cephalalgia 1995;15:205-10.
11. Hubka MJ, Phelan SP. Interexaminer reliability of palpationfor cervical spine tenderness. J Manipulative Physiol Ther1994;17:591-5.
12. Levoska S, Keinanen-Kiukaanniemi S, Bloigu R. Repeatabil-ity of measurement of tenderness in the neck-shoulder regionby dolorimeter and manual palpation. Clin J Pain 1993;9:229-35.
13. Keating JC, Bergmann TF, Jacobs GE, Finer BA, Larson K.Interexaminer reliability of eight evaluative dimensions oflumbar segmental abnormality. J Manipulative Physiol Ther1990;13:463-70.
14. McCombe PF, Fairbank JC, Cockersole BC, Pynsent PB.1989 Volvo Award in clinical sciences. Reproducibility ofphysical signs in low-back pain. Spine 1989;14:908-18.
15. Boline PD, Haas M, Meyer JJ, Kassak K, Nelson C, KeatingJC. Interexaminer reliability of eight evaluative dimensions oflumbar segmental abnormality: part II. J Manipulative PhysiolTher 1993;16:363-74.
16. Strender LE, Sjoblom A, Sundell K, Ludwig R, Taube A.Interexaminer reliability in physical examination of patientswith low back pain. Spine 1997;22:814-20.
17. Simons DS, Travell JG, Simons LS. Myofascial pain anddysfunction. The trigger point manual. Baltimore: Williams &Wilkins; 1999. p. 1-1029.
18. Wolfe F, Simons DG, Fricton J, Bennett RM, Goldenberg DL,Gerwin R, et al. The fibromyalgia and myofascial pain syn-dromes: a preliminary study of tender points and trigger pointsin persons with fibromyalgia, myofascial pain syndrome andno disease. J Rheumatol 1992;19:944-51.
19. Njoo KH, Van der Does E. The occurrence and inter-raterreliability of myofascial trigger points in the quadratus lum-borum and gluteus medius: a prospective study in non-specificlow back pain patients and controls in general practice. Pain1994;58:317-23.
20. Gerwin RD, Shannon S, Hong CZ, Hubbard D, Gevirtz R.Interrater reliability in myofascial trigger point examination.Pain 1997;69:65-73.
21. Cott A, Parkinson W, Bell MJ, Adachi J, Bedard M, CividinoA, et al. Interrater reliability of the tender point criterion forfibromyalgia. J Rheumatol 1992;19:1955-59.
22. Haas M. The reliability of reliability. J Manipulative PhysiolTher 1991;14:199-208.
23. Haas M. Statistical methodology for reliability studies. J Ma-nipulative Physiol Ther 1991;14:119-32.
24. Wolfe F, Smythe HA, Yuns MB, Bennett RM, Bombardier C,Goldenberg DL, et al. The American College of Rheumatol-ogy 1990 Criteria for the classification of fibromyalgia. Ar-thritis and Rheu 1990;33:160-72.
475Journal of Manipulative and Physiological Therapeutics Christensen et alVolume 26, Number 8 Chest Wall Tenderness

Part project III

Cervico-thoracic angina identified by case historyand palpation findings in patients with stable
angina pectoris
Henrik Wulff Christensen, D.C., M.D.1, Werner Vach, Ph.D.4, Anthony Gichangi, M.Sci.4 Claus Manniche,M.D., D.M.Sci.5, Torben Haghfelt, M.D., D.M.Sci.3, Poul Flemming Høilund-Carlsen, M.D., D.M.Sci.2
1)Nordic Institute of Chiropractic and Clinical BiomechanicsDepartments of 2)Nuclear Medicine and 3) Cardiology, Odense University Hospital,
4) Department of Statistics, University of Southern Denmark,5) The Back Research Center, Fynen, Denmark
Reprints and correspondence:
Henrik Wulff ChristensenDepartment of Nuclear Medicine
Odense University HospitalSdr. Boulevard 29, DK-5000 Odense C, Denmark
Phone: + 45 65 41 13 95Fax: + 45 65 90 61 92
E-Mail: [email protected]

Abstract
Objective To investigate the decision making process of an experienced chiropractor in diagnosingnon-cardiac musculoskeletal chest pain in the shape of cervico-thoracic angina (CTA) in patientswith stable angina pectoris (AP), based on patient history and clinical examination. Secondly, toexamine the possibility of obtaining an objective diagnostic rule tool for the identification of CTAand, finally, to validate the diagnosis of CTA.
Design Non-randomised prospective trial.
Setting Tertiary hospital.
Participants A total of 516 out of 972 consecutive patients referred for coronary angiographybecause of known or suspected AP were asked to participate in the study. Of these, 275 gaveinformed consent to a standardized manual examination of their spine and thorax.
Main outcome measure The main outcome was the diagnoses of an experienced chiropractor onCTA patients. Myocardial perfusion imaging and coronary angiography were used for validation. Aset of candidate variables from patient history and clinical examination was tested for their role inthe decision making.
Results Eighteen percent of the patients were diagnosed with CTA. Eighty percent of these had anormal myocardial perfusion compared to 50% of CTA negative patients. The main determinants ofthe decision process could be identified.
Conclusion This study demonstrated that an experienced chiropractor could identify a subset of APpatients as suffering from CTA. Systematic manual palpation of the spine and thorax could be usedas part of the clinical examination together with basic cardiological variables to screen patients withchest pain allowing for improvements in referral patterns for specialist opinion or angiography.
2

Introduction
According to current guidelines, angina pectoris (AP) is “a clinical syndrome characterized bydiscomfort in the chest, jaw, shoulder, back or arm. It is typically aggravated by exertion oremotional stress and relieved by rest or nitroglycerin”.1 The term ”angina pectoris” is usuallyconfined to cases in whom the syndrome can be attributed to myocardial ischaemia, althoughessentially similar symptoms can be caused of disorders by the esophagus, lungs or musculoskeletalsystem.2 Reports suggest that about 50% of patients with chest pain and a negative coronaryangiography (CAG) have esophageal reflux or motility disorder,3 and that 60% have evidence ofbreathing disorders and/or psychological abnormalities.4-6
Chest wall tenderness has been observed in 69% of patients undergoing CAG.7 However, dueto overlap of possible causes and lack of a generally accepted examination protocol, the diagnosisof musculoskeletal chest pain can be difficult to establish as can the concept of cause and effectwhen searching for an explanation of chest pain.8;9 Our group has previously reported on astandardized clinical examination protocol, including palpation of the cervical and thoracic spine,the chest wall and thoracic paraspinal area, to assist in reaching a diagnosis of noncardiac chest painoriginating from the musculoskeletal system.10;11 Up to 30% of all patients catheterized for theinvestigation of chest pain have normal coronary anatomy.3 about three quarters of the patientscontinue to suffer from residual chest pain with large socio-economic consequences.3;12-15
Therefore, a search should be made for an alternative cause with related possibilities of treatment.In the present investigation, this protocol together with a detailed case history was applied by anexperienced chiropractor in patients with stable AP to diagnose “cervico-thoracic angina” (CTA),i.e., chest discomfort originating from the cervical spine and the thorax. The aim was to investigatethe decision making process of the chiropractor and to identify the most important determinantsfrom the patient history and clinical examination. Additionally, we investigated the possibility ofobtaining an objective and diagnostic rule tool for early identification of CTA in the clinical setting.Finally, we tested the validity of the chiropractor’s diagnosis.
Methods
Study populationThis study was conducted as a substudy of the Myocardial Ischemic Logistic Evaluation Study(MILES) project16, the objective of which was to compare the results of myocardial perfusionimaging (MPI) and CAG in a prospective series of patients referred to a tertiary hospital for CAGbecause of known or suspected stable AP. A total of 516 out of 972 consecutive patientsparticipated in the MILES study. This initial selection was made from the referral letter based onpredetermined exclusion criteria ensuring a fairly well-defined population without too manyconcurrent diseases. Important exclusion criteria were age >75 years, diabetes mellitus, acceleratedcatheterisation, recent acute myocardial infarction, and ischemic heart disease already known to thecardiology department. All patients in the MILES study were interviewed and invited to participatein the present study, which was approved by the local ethics committee. Of the 516 patientsapproached, 275 patients were included upon written consent. Patients who gave no written consent,had lack of compliance, previous thoracic surgery, no selfreported chest pain, inflammatory jointdisease, malignant disease, apoplexia and others were excluded from participating. As a result, 241patients, met one or more exclusion criteria, and were not included in this study (table 1). Baselinecharacteristics of the CTA population are shown in table 2.
3

Patient evaluationEach patient underwent the following procedures on a single day: 1) completion of questionnaireson health history, quality of life, and chest discomfort and 2) interrogation and physical examinationby a single physician. Patients were classified by the physician into three types of chest pain: typicalangina, atypical angina, or non-cardiac chest pain in accordance with the Danish guidelines17 andDiamond et al.18 The physician also classified patients’ chest pain into four classes of severityaccording to the criteria given by the Canadian Cardiovascular Society (CCS).19 Consistent with theMILES study, MPI was carried out in all patients on the same day as the clinical examination, andCAG was undertaken in 262 patients within 6 months after MPI. The results of MPI were notcommunicated.
QuestionnairesAll patients were given two sets of questionnaires by a laboratory technician not participating in thestudy: 1) The SF-36 quality of life questionnaire20 and 2) a questionnaire with intensity grading on a11 point box scale21 of chest pain, thoracic spine pain, cervical spine pain and shoulder arm pain.The questionnaires were filled out prior to the interview and physical examination and returned tothe laboratory technician.
Physical examinationAn experienced chiropractor (HWC), interviewed all patients using structured questionnairesthroughout the study. The standardized examination protocol for the cervical spine and thorax wascarried out as previously described. 10;11 The following procedures were performed: 1) Sittingmotion palpation (MP) for endplay restriction at segments C4-T8 of the cervical and thoracic spine;2) Sitting palpation for tenderness of the anterior chest wall; 3) Prone MP for joint play restrictionat segments T1-T8 of the spine; 4) Prone paraspinal palpation for tenderness at segments T1-T8.
Myocardial perfusion imagingSingle photon emission computed tomographic imaging was performed using a same-day restthallium-201/stress technetium-99m sestamibi dual-isotope protocol initially introduced by Bermanet al.22 and adopted by our group as previously described for a two-day protocol23. Standardprocedures for image interpretation included review of all scans by two experienced observers whowere blinded to all other data including the result of CAG. Final segmental and overall imageinterpretation was achieved by consensus. Defects that were present at rest and remained unchangedduring stress were considered as fixed. The appearance of new or worsening defects followingstress were considered to be defect reversibility. The segmental scoring system used for thisanalysis included documentation of infarct (i.e. fixed defects) or ischemia (i.e. reversible or partiallyreversible defects) in the three main vascular territories.
Coronary angiographySelective coronary angiography was performed according to Judgkin using standard techniques inmultiple views. For the purpose of this study, significant coronary stenoses were those with ≥ 50%luminal diameter narrowing of an epicardial coronary artery.
Clinical decision makingThe chiropractor was blind to the results of MPI and CAG. The case history and clinicalexamination were the basis for a decision made on the examination day of whether the patients wereCTA positive or CTA negative.
4
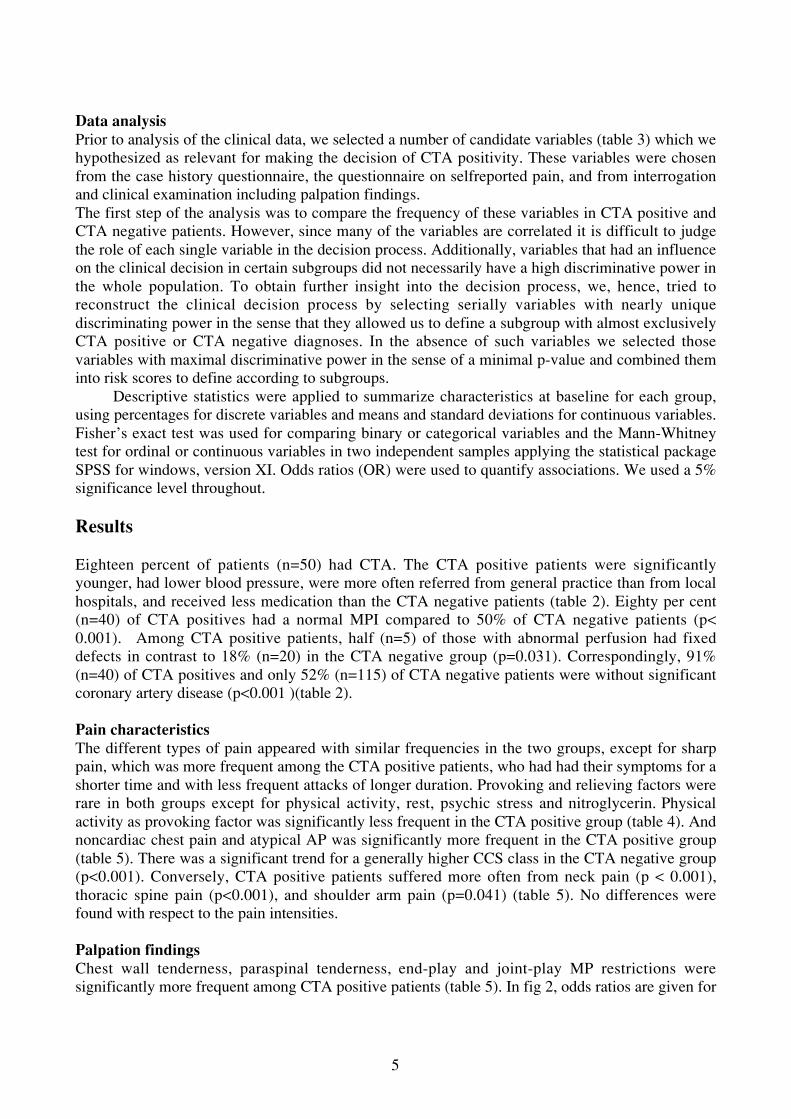
Data analysisPrior to analysis of the clinical data, we selected a number of candidate variables (table 3) which wehypothesized as relevant for making the decision of CTA positivity. These variables were chosenfrom the case history questionnaire, the questionnaire on selfreported pain, and from interrogationand clinical examination including palpation findings.The first step of the analysis was to compare the frequency of these variables in CTA positive andCTA negative patients. However, since many of the variables are correlated it is difficult to judgethe role of each single variable in the decision process. Additionally, variables that had an influenceon the clinical decision in certain subgroups did not necessarily have a high discriminative power inthe whole population. To obtain further insight into the decision process, we, hence, tried toreconstruct the clinical decision process by selecting serially variables with nearly uniquediscriminating power in the sense that they allowed us to define a subgroup with almost exclusivelyCTA positive or CTA negative diagnoses. In the absence of such variables we selected thosevariables with maximal discriminative power in the sense of a minimal p-value and combined theminto risk scores to define according to subgroups.
Descriptive statistics were applied to summarize characteristics at baseline for each group,using percentages for discrete variables and means and standard deviations for continuous variables.Fisher’s exact test was used for comparing binary or categorical variables and the Mann-Whitneytest for ordinal or continuous variables in two independent samples applying the statistical packageSPSS for windows, version XI. Odds ratios (OR) were used to quantify associations. We used a 5%significance level throughout.
Results
Eighteen percent of patients (n=50) had CTA. The CTA positive patients were significantlyyounger, had lower blood pressure, were more often referred from general practice than from localhospitals, and received less medication than the CTA negative patients (table 2). Eighty per cent(n=40) of CTA positives had a normal MPI compared to 50% of CTA negative patients (p<0.001). Among CTA positive patients, half (n=5) of those with abnormal perfusion had fixeddefects in contrast to 18% (n=20) in the CTA negative group (p=0.031). Correspondingly, 91%(n=40) of CTA positives and only 52% (n=115) of CTA negative patients were without significantcoronary artery disease (p<0.001 )(table 2).
Pain characteristicsThe different types of pain appeared with similar frequencies in the two groups, except for sharppain, which was more frequent among the CTA positive patients, who had had their symptoms for ashorter time and with less frequent attacks of longer duration. Provoking and relieving factors wererare in both groups except for physical activity, rest, psychic stress and nitroglycerin. Physicalactivity as provoking factor was significantly less frequent in the CTA positive group (table 4). Andnoncardiac chest pain and atypical AP was significantly more frequent in the CTA positive group(table 5). There was a significant trend for a generally higher CCS class in the CTA negative group(p<0.001). Conversely, CTA positive patients suffered more often from neck pain (p < 0.001),thoracic spine pain (p<0.001), and shoulder arm pain (p=0.041) (table 5). No differences werefound with respect to the pain intensities.
Palpation findingsChest wall tenderness, paraspinal tenderness, end-play and joint-play MP restrictions weresignificantly more frequent among CTA positive patients (table 5). In fig 2, odds ratios are given for
5

specific segmental restrictions of the spinal column examined by end-play and joint-play MP. Weobserved a tendency for higher ORs around segments T5 and T6 (3.60 – 6.94) compared with theother thoracic segments (0.79 – 3.09). Segments C5 to C7 also had higher ORs.
Reconstruction of the clinical decision processThe first variable identified was a restriction at joint-play MP because this is a prerequisite for amusculoskeletal cause. All 50 CTA positive patients were found among the 90 subjects who had apositive finding with joint-play MP (fig 1), all of whom had also a restriction at end-play MP (table5). Among these 90 patients, noncardiac chest pain defined a subgroup of 18 patients, 17 of whichwere CTA positive. In the remaining 72 patients, none of the candidate variables were able to definea subgroup with almost entirely CTA positive or CTA negative patients. Twenty-seven variableswere at least slightly associated with the diagnosis of CTA, 19 of these with a p-value <5%. Highestsignificance was found for a) grade of angina (CCS)(p=000018), b) presence of neck pain(p=0.000048), c) type of angina (p=0.00020), d) four palpation findings (p=0.00064), e) spinaltenderness (p=0.0013). Because type and grade of angina were highly associated as were spinaltenderness and the number of positive palpation findings, it was not possible to analyse their jointeffect. However, selecting any triple of variables from a or c, d and e or b, and analysing their jointeffect in a linear logistic model, we found that they all contributed significantly to the diagnosis. Ifwe used the combined presence of three such factors (i.e., presence of neck pain + lowest CCSgrade + four palpation findings, see score 1 in fig 1) to define a risk score, we found that none of theseven patients without any of these factors were CTA positive, that two out of 21 with only onefactor were CTA positive, 12 out of 23 with two, and 19 out of 21 with all three of these factorswere positive. Adding other factors to the aforementioned three factors in the logistic regressionmodel one by one, the following factors showed a significant additional effect: diffuse chest pain(p=0.04), number of chest pain attacks (p=0.036), end-play MP T5/6 (p=0.028), joint-play MP T5/6(p=0.010), joint-play MP T6/7 (p=0.014). However, a score based on all eight variables did notimprove the discrimination.
Looking at the subgroup of 23 subjects with two of the three factors being positive we foundfour variables with a significant association and one with borderline significance: 1) chest paindescribed as sharp (p=0.035), 2) chest pain relieved by rest (p=0.049), 3) end-play MP T4/5(p=0.062), 4) end-play MP T5/6 (p=0.016), and finally 5) joint-play MP T5/6 (p=0.035). Usingthese 5 factors to define a new score (score 2) we saw that absence of all defined the CTA negativedecision and presence of three of five factors were enough to diagnose CTA positivity. Remainingwere 12 patients with presence of one or two of these factors. However, in these 12 patients, wecould still find borderline significant or significant associations: thoracic spine pain (p=0.079), neckpain (p=0.079), shoulder arm pain (p=0.079), physical activity aggravates (p=0.038), maritalrelation (p=0.067), typical angina (p=0.023), CCS 1 (p=0.023), beta-adrenergic blocker medication(p=0.079) and, finally, joint-play MP T2/3 (p=0.004). The last one allowed a nearly definite split:Presence of this variable indicated CTA positivity in seven out of eight patients, absence indicatedCTA negativity in four of four (fig 1).
6

Discussion
This appears to be the first study to systematically examine the combination of case history andpalpation findings as a tool for identifying musculoskeletal causes of chest pain. In our sample ofstable AP patients, this approach resulted in a separation of nearly 1/5 patients with suspected non-cardiac musculoskeletal chest pain (CTA positives) and 4/5 (CTA negatives) more prone to haveeither AP, i.e., angina caused by myocardial ischemia, or chest discomfort due to other reasons(table 2). Separation could not be achieved by the use of single items from case history and clinicalexamination alone. By combining different items in a decision tree, we could nearly reconstruct thedecision process illustrating the complexity of this kind of daily clinical practice (fig 1).The presence of chest pain was the same in the two groups with expected differences concerningtype and severity of AP. More neck, thoracic, and, shoulder arm pain was found in the CTApositive group. Pain intensity seemed to have no discriminative power. Also, distinction could notbe made from symptoms (pain on movement, deep breath, coughing pain) often regarded ascharacteristic for musculoskeletal chest pain.24;25 Chest pain precipitated by physical activity,lasting less than 10 minutes and relieved by rest and nitroglycerin were found more common in theCTA negative group. Accordingly, this group received more heart medication. Reconstruction ofthe decision process suggested that joint-play and end-play MP findings together with traditionalclinical classification of chest discomfort played a major role in the decision making process.Among the candidate variables, the CCS class had a high discriminatory power for diagnosing CTApositivity (p=0.000018). When patients were classified according to type of AP variables likemedication or thoracic spine pain had little relevance. Significantly more patients in the CTApositive group were referred from general practice suggesting that a systematic manual palpationprogram might be useful for the GP as a screening tool in these patients. MPI categorized thepopulation into those with normal and those with abnormal myocardial perfusion (table 2). Eightypercent of the CTA positive population had normal perfusion compared to 50% in the CTAnegative group. The 20% of CTA positives with a perfusion abnormality were not necessarilymisclassified, but might have had two diagnoses at the same time. Two of these 10 patients hadindeed typical angina of CCS class 2 in spite of the CTA positive diagnosis. Five other patients hadirreversible ischemia possibly caused by previous undetected myocardial infarction. The fact that asmany as half of the CTA negative group had normal perfusion may indicate a conservativechiropractic diagnosis making or that reasons other than ischemic heart disease and musculoskeletaldisorders may account for a sizable fraction of patients suffering from chest pain.3;6;9;26 Similarrelationships were found when patients were stratified according to catheterisation results (table 2).Most previous studies were retrospective, often focusing on patients with a normal CAG.7;27 In anopen study in patients with suspected AP but normal CAG, Wise et al. applied limited palpationmanoeuvres on the spine and chest wall and found that 69 of 100 patients had chest wall tendernesscompared to 0 of 25 control patients with arthritis and no chest pain.7 Frobert et al. did a blindedconsecutive study on patients with AP and normal CAG and found that patients had significantlymore complaints of pain from the neck, chest, and thoracic spine, together with more pain radiatingto the arms than control individuals. Physical examination showed abnormal findings morefrequently in patients localized to the anterior and posterior chest wall, spinal levels T1-T6, and themuscles of the neck and shoulder girdle.27 One prospective study compared positive palpationfindings of chest wall tenderness in patients with normal CAG and abnormal CAG and found nodifference among the two groups.28 None of these observations are directly comparable to ourresults, but they support the view that musculoskeletal disorders are common in patients with chestpain.
7

Clinical decision makingToday there exists no operational definition of chest pain originating from the musculoskeletalsystem. It has been suggested that the clinician rely on case history and aberrant movement of thethoracic spine to make a diagnosis, sometimes referred to as “the thoracic facet syndrome”.25;29;30
Apart from this, recognized textbooks state that among several differential diagnosesmusculoskeletal disorders may also account for conditions like “dysfunction of the thoracic spine”,“intercostal myoses” and “myositis”, without providing a satisfactory explanation for their existenceand thumb rules for their detection.1;25
Tables 4 and 5 show the discriminative power of different variables in distinguishing CTApositive from CTA negative patients. Since many of these variables were correlated it was difficultto judge the role of each single variable. Additionally, variables that had an influence on the clinicaldecision in certain subgroups did not necessarily have a high discriminative power in all groups.Therefore, we reconstructed a decision tree, which, if simple and sufficiently accurate, mightbecome useful outside the field of chiropractic. For the 6 patients violating our decision model weidentified some potential reasons. One patient was classified CTA negative despite non-cardiacchest pain classification. The patient did not report cervical or thoracic spine pain within the last 14days, suggesting that our time window for CTA positivity might have been too narrow. Two CTApositive patients had only one of three factors in score 1. However, both had thoracic spine pain andrestriction at joint-play and end-play MP evaluation indicating two competing conditions, ischemicheart disease and a musculoskeletal disorder. Two CTA negative patients had a score 1 value of 3.One had a gastrointestinal disorder, and the other patient reported daily and constant pain – whichmakes a musculoskeletal diagnosis unlikely. Lastly, one CTA negative patient with T2/T3 specificjoint-play MP restriction had convincing cardiac symptoms (moderate dyspnoea, CCS 2, and typicalAP) which spoke against classifying the patient as CTA positive.
LimitationsOur data did not apply to patients with recent onset of pain, whose symptoms may be more atypical.The present population was selected for catheterisation at a university hospital and, consequently,the discriminative value of certain criteria could be different in a wider clinical setting includingthose types of patients we excluded. Also, we did not consider other potential causes of chest pain,and, therefore, could not allege CTA positivity to be the sole cause of chest discomfort in patientswithout perfusion abnormalities or coronary stenoses. However, we were able to identify a fewcandidate variables which, when added to certain palpation findings, identified almost all CTApositive patients. In order to test to what degree patients can benefit from a positive CTA diagnosisall positive patients were offered chiropractic treatment, the result of which shall be publishedelsewhere.
Conclusion
The results of this study suggest that an experienced chiropractor can fairly convincingly identify asubset of angina pectoris patients as suffering from CTA. Systematic manual palpation of the spineand thorax could be used as part of the clinical examination in combination with basic cardiologicalvariables to screen patients with chest pain to allow for improvements in referral patterns forspecialist opinion or angiography. The suggested decision tree may serve as an example of how tobase the diagnosis of noncardiac chest pain from the musculoskeletal system on a more objectiveand reproducible procedure, facilitating its use outside the field of chiropractic.
8

Acknowledgements
We greatly appreciate the assistance of the following persons: secretaries Anne-Marie Møller andBente Wichmann, Department of Cardiology, and laboratory technicians of the “Heart Group”,phycicians, head secretary Anette Albæk, laboratory technicians Karina Madsen and TinaGodskesen, and chief laboratory technician Mette Møldrup, Department of Nuclear Medicine. Thestudy was supported by the Nordic Institute of Chiropractic and Clinical Biomechanics, Odense,Denmark, and The Foundation for Chiropractic Research and Postgraduate Education, Denmark.
9

Table 1 Exclusion criteria and their frequencies in 241 patients. Note that some patients fulfilled>one criterion.
No. of pts
Lack of compliance (withdrawal prior to FUMU program) 89
No written consent 49
Previous surgery to the thorax 32
No selfreported chest pain, neck pain or thoracic spinal pain 26
Inflammatory joint disease 18
Malignant disease 18
Apoplexia 14
Others 13
10

Table 2. Patient characteristics, medication, and results of myocardial perfusion imaging andcoronary angiography.
CTA total(N=275)
CTA positive(N=50)
CTA negative(N=225)
p
Patient characteristicsAge 56.31 (9.26) 50.36 (9.14) 57.63 (8.78) <0.001Weight 81.24 (15.58) 82.02 (20.18) 81.08 (14.43) 0.899Height 171.43 (12.50) 170.84 (18.68) 171.56 (10.74) 0.765BMI 27.08 (3.81) 26.39 (3.46) 27.22 (3.87) 0.262Systolic BP 141.17 (16.64) 136.76 (17.81) 142.15 (6.25) 0.009Diastolic BP 85.57 (9.12) 83.24 (7.90) 86.08 (9.32) 0.025Gender % female n=104 (38%) n=22 (44%) n=82 (36%) 0.337Referred from GP n=135 (49%) n=38 (76%) n=97 (43%) <0.001MedicationBeta-blocker n=115 (42%) n=10 (20%) n=105 (47%) <0.001Ca++-antagonist n=64 (23%) n=7 (14%) n=57 (25%) 0.098ACE inhibitor n=40 (15%) n=2 (4%) n=38 (17%) 0.015Short acting nitrates n=68 (25%) n=4 (8%) n=64 (28%) 0.002Long lasting nitrates n=36 (13%) n=0 (0%) n=36 (16%) 0.001Magnyl n=157 (57%) n=15 (30%) n=142 (63%) <0.001Anticholesterol n=78 (28%) n=4 (8%) n=34 (33%) <0.001Perfusion imagingNormal n=151 (56%) n=40 (80%) n=111 (50%)Partly reversible defects n=33 (12%) n=1 (2%) n=32 (14%)Reversible defects n=63 (23%) n=4 (8%) n=59 (27%)Fixed defects n=25 (9%) n=5 (10%) n=20 (9%)
<0.001
Missing 3 0 3Coronary angiographyNormal n=152 (59%) n=40 (91%) n=112 (52%)1-vessel disease n=42 (16%) n=2 (5%) n=40 (19%)2-vessel disease n=34 (13%) n=1 (2%) n=33 (15%)3-vessel disease n=31 (12%) n=1 (2%) n=30 (14%)Missing 16 6 10
<0.001
BMI = Body mass index. BP = Blood pressure. GP = General Practice.Data are expressed as means (SD)
11

Table 3 Candidate variables.
Type Description Cause of selection Expected findingsSelf-reportedpain
Chest pain, neck pain,thoracic pain,shoulder-arm pain
Pain is the primarycomplaint and outcomeparameter
Chest and neck painpresence the same in bothgroups. More shoulder armpain in CTAneg. Morethoracic pain in CTApos
Case history Description ofsymptoms, duration ofattacks, aggravatingand relieving factors
Empirical tradition thatcertain aspects of the casehistory are characteristic interms of cardiac and non-cardiac chest pain
Typical AP chest painprecipitated by physicalactivity, < 10 minutesduration, relieved by restand nitroglycerin.CTApos chest painprecipitated by movement,deep breath and cough
Type of anginapectoris
Classification of chestpain from case history
There is evidence whichindicates that the prevalenceof coronary-artery disease isrelated to type of angina18
More non-cardiac AP inCTApos. More typical andatypical AP in CTAneg
Medication Antianginousmedication,painkillers
Patient using heartmedication might bias thedecision of the examiningchiropractor
Less cardiac medication inthe CTApos compared toCTAneg
Palpationfindings
Joint-play motionpalpation, end-playmotion palpation,paraspinal tenderness,chest wall tenderness
Palpation is used as indirectmethods to evaluatestructures of themusculoskeletal systemsuspected to producenon-cardiac angina
Expect more palpationrestrictions and tendernessin the CTApos group.
CTApos = CTA positive; CTAneg = CTA negative.
12

Table 4 Comparability on specific case history items for CTA patients.
CTA positive(N=50)
CTA negative(N=225)
p
How would you describe yoursymptoms? Squeezing/pressurelike n=41 (82%) n=203 (90%) 0.134 Tenderness n=1 (2%) n=16 (7%) 0.326 Sharp n=16 (32%) n=40 (18%) 0.023 Well demarcated n=2 (4%) n=9 (4%) 0.679 Diffuse n=6 (12%) n=18 (8%) 0.255 Burning n=3 (6%) n=10 (4%) 0.431 Prickly n=11 (22%) n=28 (12%) 0.068 Other n=4 (8%) n=23 (10%) 0.433Duration of each attack? <10 minutes n=26 (52%) n=173 (77%) 10 minutes – 1 hour n=12 (24%) n=35 (16%) 0.009 More than 1 hour n=12 (24%) n=17 (7%)Attacks Monthly n=24 (48%) n=61 (27%) Weekly n=18 (36%) n=107 (48%) 0.019 Daily n=8 (16%) n=57 (25%)Symptoms for how long time? < 6 month n=24 (48%) n=81 (36%) 6-24 month n=16 (32%) n=108 (48%) 0.034 > 24 month n=10 (20%) n=36 (16%)Provoking factors Physical activity precipitates n=25 (50%) n=190 (84%) <0.001 Movement of the thorax n=4 (8%) n=5 (2%) 0.060 Rest n=17 (34%) n=77 (34%) 1.000 Sexual activity n=2 (4%) n=26 (12%) 0.127 Sleep n=3 (6%) n=5 (2%) 0.162 Leaning foreward n=1 (2%) n=4 (2%) 1.000 Swallowing n=0 (0) n=2 (1%) 1.000 Deep breath n=0 (0) n=2 (1%) 1.000 Eating n=1 (2%) n=5 (2%) 1.000 Cold n=1 (2%) n=16 (7%) 0.149 Psychic stress n=19 (38%) n=57 (25%) 0.053 Other n=9 (18%) n=16 (7%) 0.230Relieving factors Rest n=23 (46%) n=146 (65%) 0.016 Movement of the affected part n=2 (4%) n=5 (2%) 0.614 Nitroglycerin n=9 (18%) n=84 (37%) 0.008 Other antiangina medication n=0 (0) n=10 (4%) 0.217 Pain killers n=2 (4%) n=2 (1%) 0.152 Tranquilizers n=2 (4%) n=0 (0) 0.033 Antiacid medicin n=0 (0) n=0 (0) 1.000
13

Table 5 Discrimination between the CTA groups at baseline in palpations findings, chest, neck andthoracic pain and cardiovascular classification. Shown are absolute numbers and relativefrequencies (in parentheses).
CTA total(N=275)
CTA positive(N=50)
CTA negative(N=225)
p
Palpation Chest wall tenderness 214 (78) 49 (98) 165 (73) 0.053 Paraspinal tenderness 133 (48) 48 (96) 85 (38) <0.001 End-play motion palpation 160 (58) 50 (100) 110 (49) <0.001 Joint-play motion palpation 90 (33) 50 (100) 40 (18) <0.001Type of chest pain Non-cardiac chest pain 39 (14) 17 (34) 22 (10) Atypical angina 80 (29) 22 (44) 58 (26) <0.001 Typical angina 156 (57) 11 (22) 145 (64)CCS I 133 (48) 43 (86) 90 (40) II 128 (47) 7 (14) 121 (54) III 14 (5) 0 (0) 14 (6) <0.001 IV 0 (0) 0 (0) 0 (0)Presence of chest pain Today 159 (58) 31 (62) 128 (57) 0.531 Pain past 14 days 249 (91) 44 (88) 205 (91) 0.592Chest pain intensity * Intensity today 2.63 (1.61) 2.74 (1.29) 2.60 (1.69) 0.283 Max. intensity past 14 days 4.29 (2.21) 4.14 (1.97) 4.32 (2.27) 0.697 Average intensity past 14 days 3.36 (1.87) 2.91 (1.63) 3.46 (1.91) 0.090Presence of neck pain 106 (38) 37 (74) 69 (31) <0.001Neck pain intensity * Average intensity past 14 days 3.55 (1.99) 3.57 (1.89) 3.54 (2.06) 0.713Presence of thoracic pain 109 (40) 32 (64) 77 (34) <0.001Thoracic pain intensity * Average intensity past 14 days 3.45(1.99) 3.19 (1.94) 3.56 (2.02) 0.194Presence of shoulder arm pain 144 (52) 33 (66) 111 (49) 0.041Shoulder arm pain intensity * Average intensity past 14 days 3.80 (2.18) 3.61 (2.25) 3.86 (2.17) 0.459*Pain intensity data are expressed in means (SD) within patients reporting pain, i.e., a rating scalevalue between 1 and 10.
14

Figure 1 The reconstructed decision tree. The rhombs are showing variables defining subgroups.The rectangles show the values defining subgroups and the numbers of the CTA positive patients(left number) and total number of patients (right number) in this subgroup.
15

Figure 2 Segmental motion palpation restriction findings. Endplay – left, Joint play – rightNumbers = Odds ratio (OR)[95% CI] comparing frequency of positive findings between CTApositive and CTA negative patients
16

Reference List
1. Braunwald E. Part I: Examination of the patient: The history. In Braunwald E, 16 ed. Heart disease, 27-45.W.B. Saunders Company, 2001.
2. Management of stable angina pectoris. Recommendations of the Task Force of the European Society ofCardiology. Eur Heart J 1997;18:394-413.
3. Chambers J, Bass C. Chest pain with normal coronary anatomy: a review of natural history and possibleetiologic factors. Prog.Cardiovasc.Dis. 1990;33:161-84.
4. Bass C, Wade C, Hand D, Jackson G. Patients with angina with normal and near normal coronary arteries:clinical and psychosocial state 12 months after angiography. Br.Med J (Clin.Res.Ed) 1983;287:1505-8.
5. Katon W, Hall ML, Russo J, Cormier L, Hollifield M, Vitaliano PP et al. Chest pain: relationship ofpsychiatric illness to coronary arteriographic results. Am.J Med 1988;84:1-9.
6. Nijher G, Weinman J, Bass C, Chambers J. Chest pain in people with normal coronary anatomy. BMJ2001;323:1319-20.
7. Wise CM, Semble E L, and Dalton CB. Musculoskeletal chest wall syndromes in patients with noncardiacchest pain: A study of 100 patients. Arch Phys Med Rehabil 1992;73:147-149.
8. Eslick GD, Coulshed DS. Rapid assessment of chest pain. Chest pain clinics may be one step forward, twosteps back. BMJ 2002;324:422.
9. Best RA. Non-cardiac chest pain: a useful physical sign? Heart 1999;81:450.
10. Christensen HW, Vach W, Manniche C, Haghfelt T, Hartvigsen L, Høilund-Carlsen PF. Palpation of the upperthoracic spine: an observer reliability study. J Manipulative Physiol Ther 2002; 25(5): 285-292.
11. Christensen HW, Vach W, Manniche C, Haghfelt T, Hartvigsen L, Høilund-Carlsen, PF. Palpation of theanterior chest wall - an observer reliability study (to appear). J Manipulative Physiol Ther . 2003.
12. Lavey EB, Winkle RA. Continuing disability of patients with chest pain and normal coronary arteriograms. JChronic.Dis. 1979;32:191-6.
13. Ockene IS, Shay MJ, Alpert JS, Weiner BH, Dalen JE. Unexplained chest pain in patients with normalcoronary arteriograms: a follow-up study of functional status. N.Engl.J Med 1980;303:1249-52.
14. Sullivan AK, Holdright DR, Wright CA, Sparrow JL, Cunningham D, Fox KM. Chest pain in women: clinical,investigative, and prognostic features. BMJ 1994;308:883-6.
15. Lantinga LJ, Sprafkin RP, McCroskery JH, Baker MT, Warner RA, Hill NE. One-year psychosocial follow-upof patients with chest pain and angiographically normal coronary arteries. Am.J Cardiol. 1988;62:209-13.
16. Hoilund-Carlsen PF, Johansen A, Christensen HW, Bartram P, Veje A, Lerbjerg G, Mickley H, Haghfelt T,and Vach, W. Myocardial perfusion as guidance for diagnostic catherization and management decision instable angina pectoris (submitted 2003).
17. Haghfelt T, Alstrup P, Grande P, Madsen J K, Rasmussen K, Thiis, J. Guidelines for diagnosis and treatmentof patients with stable angina pectoris. 1-40. 1996. Copenhagen, Own publisher, Danish Society of Cardiologyand Danish society of Thoracic Surgery, Consensus report.
18. Diamond GA,.Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-arterydisease. N.Engl.J.Med. 1979;300:1350-8.
19. Campeau L. Letter: Grading of angina pectoris. Circulation 1976;54:522-3.
17

20. Bjørner JB, Damsgaard MT, Watt T, Bech P, Rasmussen NK, Kristensen TS et al. Dansk manual til SF-36 - etspørgeskema om helbredsstatus. Lif Lægemiddelindustriforeningen, 1997.
21. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain1986;27:117-26.
22. Berman DS, Kiat H, Friedman JD, Wang FP, van Train K, Matzer L et al. Separate acquisition rest thallium-201/stress technetium-99m sestamibi dual-isotope myocardial perfusion single-photon emission computedtomography: a clinical validation study. J Am.Coll Cardiol. 1993;22:1455-64.
23. Johansen A, Gaster AL, Veje A, Thayssen P, Haghfelt T, Hoilund-Carlsen PF. Interpretive intra- andinterobserver reproducibility of rest/stress 99Tcm-sestamibi myocardial perfusion SPECT in a consecutivegroup of male patients with stable angina pectoris before and after percutaneous transluminal angioplasty.Nucl.Med Commun. 2001;22:531-7.
24. Allison, D. R. Pain in the chest wall simulating heart disease. BMJ 1950;1:332-336.
25. Kryger P. Medicinsk Kompendium. Copenhagen: Degenerative reumatiske sygdomme 543-553 Nyt NordiskForlag Arnold Busch, 1999.
26. Eslick GD, Coulshed DS, Talley NJ. Review article: the burden of illness of non-cardiac chest pain.Aliment.Pharmacol.Ther 2002;16:1217-23.
27. Frobert O, Fossgreen J, Sondergaard-Petersen J, Hede J, Bagger JP. Musculo-skeletal pathology in patientswith angina pectoris and normal coronary angiograms. J Intern.Med. 1999;245:237-46.
28. Ho M, Walker S, McGarry F, Pringle S, Pullar T. Chest wall tenderness is unhelpful in the diagnosis ofrecurrent chest pain. QJM. 2001;94:267-70.
29. Bechgaard, P. Det torakale segmentære smertesyndrom, facet syndrom. Ugeskr Laeger 1982;144(1):11-12.
30. Hamberg J,.Lindahl O. Angina pectoris symptoms caused by thoracic spine disorders. Clinical examinationand treatment. Acta Med.Scand.Suppl. 1981;644:84-6.
18

Part project IV

Manual therapy for patients withstable angina pectoris?
A non-randomized trial
Henrik Wulff Christensen, D.C., M.D.1, Werner Vach, Ph.D.4, Anthony Gichangi, M.Sci.4 Claus Manniche,M.D., D.M.Sci.5, Torben Haghfelt, M.D., D.M.Sci.3, Poul Flemming Høilund-Carlsen, M.D., D.M.Sci.2
1)Nordic Institute of Chiropractic and Clinical BiomechanicsDepartments of 2)Nuclear Medicine and 3) Cardiology, Odense University Hospital,
4) Department of Statistics, University of Southern Denmark,5) The Back Research Center, Fynen, Denmark
Reprints and correspondence:
Henrik Wulff ChristensenDepartment of Nuclear Medicine
Odense University HospitalSdr. Boulevard 29, DK-5000 Odense C, Denmark
Phone: + 45 65 41 13 95Fax: + 45 65 90 61 92
E-Mail: [email protected]
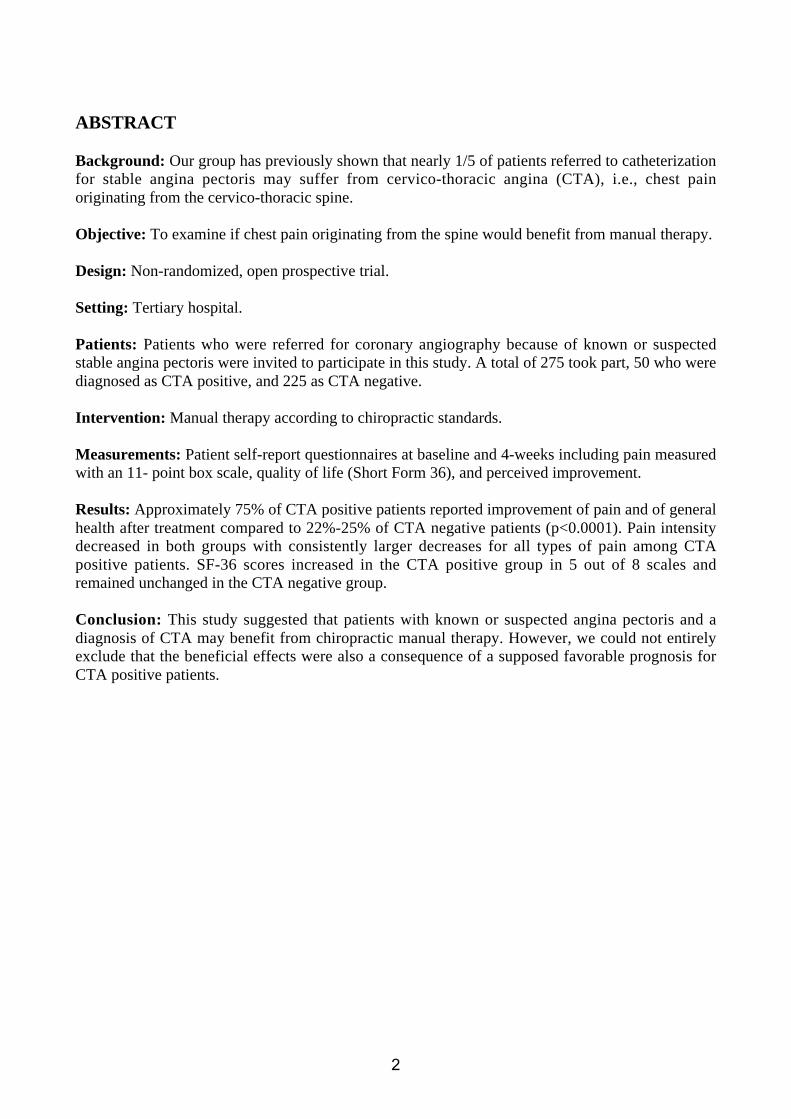
ABSTRACT
Background: Our group has previously shown that nearly 1/5 of patients referred to catheterizationfor stable angina pectoris may suffer from cervico-thoracic angina (CTA), i.e., chest painoriginating from the cervico-thoracic spine.
Objective: To examine if chest pain originating from the spine would benefit from manual therapy.
Design: Non-randomized, open prospective trial.
Setting: Tertiary hospital.
Patients: Patients who were referred for coronary angiography because of known or suspectedstable angina pectoris were invited to participate in this study. A total of 275 took part, 50 who werediagnosed as CTA positive, and 225 as CTA negative.
Intervention: Manual therapy according to chiropractic standards.
Measurements: Patient self-report questionnaires at baseline and 4-weeks including pain measuredwith an 11- point box scale, quality of life (Short Form 36), and perceived improvement.
Results: Approximately 75% of CTA positive patients reported improvement of pain and of generalhealth after treatment compared to 22%-25% of CTA negative patients (p<0.0001). Pain intensitydecreased in both groups with consistently larger decreases for all types of pain among CTApositive patients. SF-36 scores increased in the CTA positive group in 5 out of 8 scales andremained unchanged in the CTA negative group.
Conclusion: This study suggested that patients with known or suspected angina pectoris and adiagnosis of CTA may benefit from chiropractic manual therapy. However, we could not entirelyexclude that the beneficial effects were also a consequence of a supposed favorable prognosis forCTA positive patients.
2
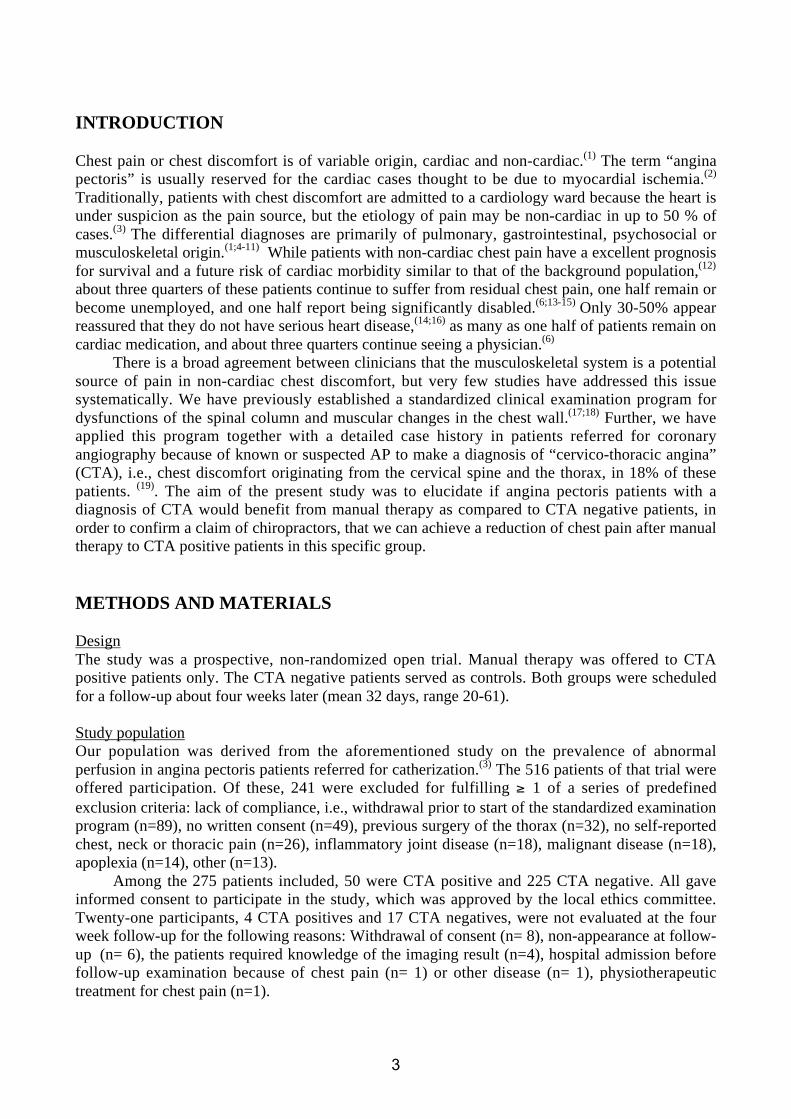
INTRODUCTION
Chest pain or chest discomfort is of variable origin, cardiac and non-cardiac.(1) The term “anginapectoris” is usually reserved for the cardiac cases thought to be due to myocardial ischemia.(2)
Traditionally, patients with chest discomfort are admitted to a cardiology ward because the heart isunder suspicion as the pain source, but the etiology of pain may be non-cardiac in up to 50 % ofcases.(3) The differential diagnoses are primarily of pulmonary, gastrointestinal, psychosocial ormusculoskeletal origin.(1;4-11) While patients with non-cardiac chest pain have a excellent prognosisfor survival and a future risk of cardiac morbidity similar to that of the background population,(12)
about three quarters of these patients continue to suffer from residual chest pain, one half remain orbecome unemployed, and one half report being significantly disabled.(6;13-15) Only 30-50% appearreassured that they do not have serious heart disease,(14;16) as many as one half of patients remain oncardiac medication, and about three quarters continue seeing a physician.(6)
There is a broad agreement between clinicians that the musculoskeletal system is a potentialsource of pain in non-cardiac chest discomfort, but very few studies have addressed this issuesystematically. We have previously established a standardized clinical examination program fordysfunctions of the spinal column and muscular changes in the chest wall.(17;18) Further, we haveapplied this program together with a detailed case history in patients referred for coronaryangiography because of known or suspected AP to make a diagnosis of “cervico-thoracic angina”(CTA), i.e., chest discomfort originating from the cervical spine and the thorax, in 18% of thesepatients. (19). The aim of the present study was to elucidate if angina pectoris patients with adiagnosis of CTA would benefit from manual therapy as compared to CTA negative patients, inorder to confirm a claim of chiropractors, that we can achieve a reduction of chest pain after manualtherapy to CTA positive patients in this specific group.
METHODS AND MATERIALS
DesignThe study was a prospective, non-randomized open trial. Manual therapy was offered to CTApositive patients only. The CTA negative patients served as controls. Both groups were scheduledfor a follow-up about four weeks later (mean 32 days, range 20-61).
Study populationOur population was derived from the aforementioned study on the prevalence of abnormalperfusion in angina pectoris patients referred for catherization.(3) The 516 patients of that trial wereoffered participation. Of these, 241 were excluded for fulfilling ≥ 1 of a series of predefinedexclusion criteria: lack of compliance, i.e., withdrawal prior to start of the standardized examinationprogram (n=89), no written consent (n=49), previous surgery of the thorax (n=32), no self-reportedchest, neck or thoracic pain (n=26), inflammatory joint disease (n=18), malignant disease (n=18),apoplexia (n=14), other (n=13).
Among the 275 patients included, 50 were CTA positive and 225 CTA negative. All gaveinformed consent to participate in the study, which was approved by the local ethics committee.Twenty-one participants, 4 CTA positives and 17 CTA negatives, were not evaluated at the fourweek follow-up for the following reasons: Withdrawal of consent (n= 8), non-appearance at follow-up (n= 6), the patients required knowledge of the imaging result (n=4), hospital admission beforefollow-up examination because of chest pain (n= 1) or other disease (n= 1), physiotherapeutictreatment for chest pain (n=1).
3

EvaluationOn the day of inclusion, all patients answered two sets of questionnaires given by a laboratorytechnician not participating in the study: One questionnaire recorded the intensity on an 11- pointbox scale with grading from 0 (= no pain) to 10 (= unbearable pain) of the patient’s chest pain“now” (i.e., on the day of examination), together with the following types of pain experiencedduring the last fortnight: maximal and average chest pain, average thoracic spine pain, averagecervical spine pain and average shoulder arm pain. Also, the patients should indicate if theybelieved that the musculoskeletal system and/or the heart was the source of their chest pain, and,finally, if they were afraid of their chest pain. The other was a quality of life questionnaire (ShortForm 36 (SF-36)), which measures physical and mental health. When completed, the laboratorytechnician collected the questionnaires.
Immediately after, all patients were interviewed and examined physically by a singleexperienced chiropractor (HWC) who was also a medical doctor. The standardized examinationprogram for the cervical spine and thorax was carried out as previously described,(17;18) includingthe following steps: 1. Sitting motion palpation for endplay restriction at segments C4-T8 of thecervical and thoracic spine. 2. Sitting palpation for tenderness of the anterior chest wall. 3. Pronemotion palpation for joint play restrictions at segments T1-T8 of the thoracic spine. 4. Proneparaspinal palpation for tenderness at T1-T8. Based on the history and the physical examination, thechiropractor classified each patient as CTA positive or CTA negative.(19)
Finally, patients had myocardial perfusion imaging performed to evaluate the presence of reducedmyocardial blood flow indicating ischemia.
Treatment protocolPatients received eight treatment sessions during four weeks by the same chiropractor. Eachparticipant got at least one manual thrust at each session, applied with high velocity and lowamplitude force directed at one or more restricted cervical and/or thoracic joint segments asdescribed by Bergmann et al.(20) Trigger point therapy intervention followed clinical practice, inwhich the choice of initial and subsequent trigger point therapy was decided by the treatingchiropractor. Manual pressure and deep stroking massage on the different trigger points was appliedto trigger points as described by Travell & Simons.(21) Participants in the CTA negative group wereinterviewed and informed about the CTA diagnosis by the chiropractor and underwent the sameexamination of the musculoskeletal system as the CTA positive, but received no therapy.
Follow-upAfter 4-weeks, the same questionnaires that were administered on entrance were repeated.Additional questions addressed whether patients thought their chest pain and general health hadturned worse or a little worse, or whether they were unchanged, a little better or better (Table 4),and, further, if they felt that the manual therapy had helped them or not. Then the standardizedexamination program was applied again. The examiner was blind to palpation findings at baselineand the result of perfusion imaging, but not to the original CTA status of the patients.
Statistical AnalysesFor the analysis at baseline, SF-36 scores were standardized for each patient by subtracting thecorresponding age and sex specific mean in the Danish population(22) and dividing by thecorresponding standard deviation (SD). Changes in the continuous variables between baseline andfollow-up were described by the mean and SD of the individual increase or decrease, and thedifferences between CTA positive and negative patients were assessed by the difference of themean values. These differences were then adjusted for imbalances in the baseline values using anANCOVA with an interaction between baseline and group and evaluating the group difference from
4
the population mean. Changes in binary variables were assessed by the relative frequencies atbaseline and follow-up and the absolute number of changes in both directions. Significance of thedifferences between baseline and follow-up was assessed using the McNemar test. Differencesbetween the two groups with respect to the change in a binary variable were assessed by theWilcoxon test applied to the difference (-1,0,1). Further, by a logistic regression analysis modellingthe outcome at follow-up as a linear function of the baseline status and group membership and,hence, taking differences at baseline into account. P-values less than 5% were regarded assignificant.
RESULTS
Baseline ResultsThe different types of pain were equally frequent among CTA positive and CTA negative patientsat baseline and at follow-up among patients suffering from pain (Table 1). At baseline, our totalpopulation had lower quality of life scores than normal for their ages and gender, i.e., median valuesbetween 0.5 and 1 SD below the population mean (Figure 1). The baseline distribution of the eightSF-36 quality of life scales is displayed in Table 2 according to which CTA positive patients hadsignificantly higher scores for physical functioning, role physical, and general health compared toCTA negative patients, while other scores were comparable. Table 3 shows that with all four typesof palpation nearly 100% of CTA positives had abnormal findings at baseline compared to muchlower frequencies (range 17% - 74%) among CTA negative patients, in whom chest wall tendernesswas the most common abnormality. At baseline, 74% (N=37) of CTA positive patients thought thatthey had musculoskeletal pain compared to only 41% (N=92) of CTA negative patient, 81%(N=183) of whom felt that they suffered from cardiac pain as opposed to only 52% (N=26) of theCTA positive patients. However, approximately 75% of patients in both groups were afraid of theirchest pain.
Follow-up ResultsApproximately 3/4 of the CTA positive patients reported improvement of pain and of general healthafter treatment, and the remaining 1/4 reported no change (Table 4). In comparison, 13% of theCTA negative group reported worse chest pain and a poorer general health at follow-up, 65%reported unchanged chest pain and 58% unchanged general health, while the rest indicated less pain(22%) and improvement in general health (26%), these differences between groups being highlysignificant (Table 4). Asked directly, fourty-four patients (96%) of the CTA positive patientsindicated that the chiropractic treatment had helped.
Despite the lack of significant changes in the presence of pain in the two groups from baselineto follow-up (Table 1), both groups showed at follow-up a mean decrease in pain intensity on all 6pain scales. The decrease was consistently larger in CTA positive patients and significantly so withregard to maximal and average chest pain experienced during the last two weeks (Table 5).
Changes in the SF-36 scores between baseline and follow-up are shown in Table 6 displayingvirtually no change in mean scores in the CTA negative group as opposed to improvements in theCTA positive group of all 8 scores, five of which were statistically significant. Table 3 shows ahighly significant decrease in abnormal palpation findings among the CTA positive patients incontrast to significant increases in three out of four types in the CTA negative group.
After manual treatment, there was an increase from 37 (74%) to 42 (91%) (p=0.02) in CTApositive patients who believed they had chest pain originating from muscles and joints of the thoraxand the neck and a decline from 26 (52%) to 18 (39%) (p=0.27) in patients who believed they hadchest pain of cardiac origin. Similarly, there was a decline from 37 (74%) to 22 (48%) (p=0.002) in
5

CTA positive patients who were afraid of their chest pain. In comparison, no statistically significantchanges were observed in the CTA negative group from baseline to follow-up for any of these threequestions.
DISCUSSION
It has been debated how often the diagnosis of non-cardiac chest pain is neglected by thecardiologists.(23-26) Less attention has been paid to the management of extra-cardiac causes,especially the musculoskeletal ones, perhaps because they are a heterogeneous group withconsiderable overlap of symptoms, which are difficult to interpret, but should be considered.(27-30)
The present study is the first trying to elucidate the possible benefit of a CTA positive diagnosesand subsequent manual therapy in a prospective trial on a sample of patients with known orsuspected stable angina pectoris.
PainWe have previously shown that significantly more CTA positive than CTA negative patients sufferfrom neck pain, thoracic pain, and shoulder arm pain, whereas there is little difference with regardto intensity of chest pain, neck pain, thoracic pain, and shoulder arm pain.(19) Further, 80% of CTApositive patients appeared to have normal myocardial perfusion compared to 50% of CTA negativepatients indicating more angina due to myocardial ischemia among the CTA negative ones. In thepresent trial, we observed some apparently conflicting results with the various measurement scalesfor pain. With binary scales we found no effect of the manual therapy in any of the six pain scales(Table 1). However, maximum chest pain intensity and average chest pain intensity during the lastfortnight did improve significantly in the CTA positive compared to the CTA negative group andwith the remaining four scales there was a tendency for a reduction in pain intensity among theCTA positive patients (Table 5). Also, this lack of effect on the binary scales was in contrast to the74% of CTA positive patients who on follow-up indicated improvement in the shape of less chestpain and better general health. No one in this group experienced worsening compared to 13% of theCTA negative group (Table 4). However, 8, 3 and 3 patients, respectively, deteriorated with regardto chest pain now and maximum and average chest pain during the last two weeks (Table 1),suggesting that these patients were not able to recall correctly their rating scale judgment of 0 atbaseline or that the actual deterioration was too small to affect their subjective evaluation of achange.We would like to point out, that in studies on the effect of manual therapy using VAS scores as anoutcome measure baseline values have typically a mean about 5-6 and a mean reduction by 3 to 4points can be observed.(31;32) In our population of patients we have a mean of 3.5 at baseline, and -in contrast to most other studies – a substantial fraction of patients with no pain. However the highstandard deviations of about 2 for the change in the pain scores among the CTA negative patientsmay indicate, that VAS are not an appropriate tool to assess improvement in such a low level painpopulation, neither as a binary nor as a continuous variable.Elliott et al. assessed different methods of measuring change in chronic pain severity and foundpoor agreement and low correlation between a serial measure and patient retrospectiveperception.(33) Similar tendencies might have influenced our findings.
Quality of lifeThe CTA negative group did not change in any of the SF-36 scales at follow-up in contrast to theCTA positive group, which improved significantly in five of the eight scales (Table 6). Thisimprovement was in the “soft scales” whereas no significant improvement was obtained in the
6

“hard scales” (physical functioning, bodily pain, and general health). However, the CTA positivepatients had at baseline, distinctly higher level of physical functioning and general health statusscores than the CTA negative patients. In fact, the CTA positive patients’ the physical functioningscore were close to what is seen in healthy subjects (median standardized score = –0.3).
Palpation findingsThe CTA positive patients improved dramatically whereas the CTA negative ones became worse(Table 3). The latter result was somewhat surprising, because one would rather expect a stablesituation in the latter group. One explanation might be that these patients became more anxious,causing more muscle tension, while waiting for catheterization, which was not performed prior tofollow-up. Another, recalling the central role of palpation for the diagnosis of CTA(19) and thelimited reproducibility of palpation findings,(17;18) that it was due to ‘regression to the mean’.(34)
Thus, some CTA positive patients may be overlooked on the day of diagnosis and falsely assignedto the CTA negative group and, hence, showing their real status only at follow-up. If so, one has toask if the improvement among the CTA positive patients could be explained in a similar manner.However, at follow-up, at least two of the four abnormal findings were less frequent among CTApositive patients than among CTA negative patients at baseline, and, consequently, theimprovement in CTA positive patients was bigger than could be explained by regression to themean. On the other hand, one cannot exclude that this improvement could be a result of observerbias, i.e., the therapist would expect his treatment to diminish the abnormal musculoskeletalfindings.
In summary, the most favorable results were found for the subjective assessment ofimprovement in chest pain and general health and the least favorable ones were on the rating scales.A statistical significant reduction in the patients’ anxiety for their chest pain was found among theCTA positives compared to no change in the CTA negative group. This might be explained by theobserved reduction in chest pain intensity and/or by more attention of the chiropractor during thetreatment period. Further, more CTA positive patients considered the musculoskeletal system to bethe pain source after treatment. This is in line with patient self-assessment of chest pain in that mostpatients responded positively to manual treatment. When asked, 96% of CTA positive patients (44of 46 treated) “believed that the chiropractic treatment had helped”.
Others’ findingsThere are several case reports on manual therapy of chest pain in patients with atypical or non-cardiac angina, (11;35-41) but there have been no randomized studies. A single randomized clinicaltrial on manual therapy for thoracic spine pain of mechanical origin and unknown duration hasbeen conducted in 30 subjects with a mean baseline value for thoracic spine pain of 4.8 on a ratingscale compared to 3.2 in our study. One group received spinal manipulative therapy and anothernonfunctional ultrasound treatment. The authors found a significant reduction in pain but not indisability. Their results, however, are difficult to interpret because of inconsistencies in significancelevels and the interpretation of p-values.(42)
The literature is more abundant when it comes to manual therapy for neck pain in patientswithout chest pain. In a systematic review from 1996 of 9 randomized trials it was found thatmanipulation or mobilization may be more effective than muscle relaxants or usual medical care inproducing short-term pain relief.(43) In the latest systematic review of 20 randomized trials(including 8 of the aforementioned 9) on manual therapy for mechanical neck disorders in chestpain free patients, Gross et al. concluded that evidence favoured multimodal care, i.e.,mobilization/massage or manipulation in combination with either exercise with thermal modalitiesover manipulation alone. No benefit was found for manual therapies given alone with a shorterduration (three weeks) and lower frequency (eight treatments). In the long term, manipulation alone
7

was less effective than high-technology exercise or manipulation and low-technology exercise. Thetreatment duration was 20 sessions over 11 weeks.(31;44)
Limitations and clinical implicationsThe present study should merely be regarded as a first pilot study raising the question if manualtherapy may benefit some patients with chest pain normally considered to be a type of anginapectoris. Further evidence would require prospective, randomized trials in a population of patientsreferred from general practitioners.The limitations in our study were several. First, we conducted a non-randomized study in whichallocation and in part the assessment of treatment effects were done by the chiropractor who had anobvious interest in a positive outcome. However, the CTA positive group was highly associatedwith a normal myocardial perfusion imaging, and, hence, validated by an objective, externalmeasure, the result of which was not known to the chiropractor. This agreement cannot be affectedby the chiropractor’s interest. Second, our study population did not represent an unselected stableangina pectoris population as many eligible patients refused to participate. Furthermore, patientswere “prejudiced” in that they had been told beforehand that their symptoms were most likelycaused by coronary artery disease. This circumstance made it difficult to recruit patients and was anobvious source of bias opposing a positive result of manual therapy because patients would be lesslikely to think they would benefit from manual therapy. Third, at follow-up the diagnostic test forwhich they had been referred (i.e. angiography) and which they had been told would provide a clueto their symptoms, had still not been performed. Fourth, recent systematic reviews suggest that amultimodal care approach is preferable with 20 treatment sessions for mechanical neck pain, albeitin patients without chest pain. Our treated patients received eight treatments only.
Conclusion
The result of this study suggest that patients with suspected angina pectoris might benefit from achiropractic based diagnosis of CTA and subsequent manual therapy. We cannot completelyexclude that our findings could potentially be explained by the fact that a positive CTA diagnosis isoften associated with a good prognosis by itself, which, however, does not eliminate the need foridentifying these patients, some of which may not necessarily benefit from invasive investigationand treatment.
Acknowledgements
We greatly appreciate the assistance of the following persons: secretaries Anne-Marie Møller andBente Wichmann, Department of Cardiology, and laboratory technicians of the “Heart Group”,phycicians, head secretary Anette Albæk, laboratory technicians Karina Madsen and TinaGodskesen, and chief laboratory technician Mette Møldrup, Department Clinical Physiology ofNuclear Medicine. The study was supported by the Nordic Institute of Chiropractic and ClinicalBiomechanics, Odense, Denmark, and The Foundation for Chiropractic Research and PostgraduateEducation, Denmark.
8

Table 1. Presence and change in pain intensity on binary scales.
% With Pain Absolute Numbers p-valueType of
painCTA Baseline
Follow-up
Improved Deteriorated McNemar WilcoxonLogisticRegression
+ 60.9 60.9 8 8 1.00Chest painnow - 59.6 54.8 34 24 0.24
0.60 0.45
+ 89.1 89.1 3 3 1.00Maximumchest pain* - 91.4 88.0 15 8 0.21
0.54 0.66
+ 89.1 87.0 4 3 1.00Averagechest pain* - 91.4 87.0 15 6 0.07
0.71 0.82
+ 65.2 63.0 7 6 1.00Averagethoracicspine pain* - 33.6 37.5 19 27 0.30
0.45 0.19
+ 73.9 73.9 3 3 1.00Averageneck pain* - 30.8 40.9 14 35 <0.01
0.16 0.20
+ 63.0 63.0 5 5 1.00Averageshoulderarm pain* - 49.0 51.4 35 28 0.61
0.77 0.45
* During the preceding 14 days.
Table 2. Quality of life profile (SF-36) according to CTA status at baseline.
CTA positive (N=50) CTA negative (N=225) p-value
Physical functioning 79.7 (21.7) 70.6 (20.9) 0.0007Role physical 60.5 (39.5) 41.2 (40.1) 0.0032Bodily pain 61.7 (19.7) 58.4 (20.2) 0.2374General health 62.6 (16.1) 55.7 (17.6) 0.0066Vitality 49.9 (20.3) 51.0 (21.9) 0.9285Social functioning 80.5 (20.7) 83.4 (21.7) 0.2420Role emotional 60.7 (38.5) 55.9 (40.3) 0.4929Mental health 69.4 (15.0) 71.5 (18.5) 0.2186Data are mean (SD).Scores range from 0 (poor quality of life) to 100 (good quality of life).
9

Table 3. Presence of palpation findings on the chest wall and the thoracic spine. Data are expressedas absolute numbers and percentages of patients having positive findings (N (%)).
CTA BaselineN (%)
Follow-upN (%)
p-value
+ 44 (98) 28 (62) 0.0001Chest wall tenderness- 153 (74) 186 (90) <0.0001+ 43 (96) 16 (36) <0.0001Paraspinal tenderness- 79 (38) 101 (49) 0.0071
+ 45 (100) 29 (64) <0.0001End-play motionpalpation restriction - 102 (49) 132 (64) 0.0006
+ 45 (100) 14 (31) <0.0001Joint-play motionpalpation restriction - 36 (17) 51 (25) 0.0627
Table 4. Patient subjective assessment of chest pain and general health at follow up.
CTA positive CTA negative p
How is your chestpain nowcompared to4 weeks ago?
WorseA little worseNo changeA little betterBetter
0012 (26.1%)15 (32.6%)19 (41.3%)
3 (1.5%)25 (12.0%)135 (64.9%)25 (12.0%)20 (9.6%)
< 0.0001
How is yourgeneral healthnow comparedto 4 weeks ago?
WorseA little worseNo changeA little betterBetter
0012 (26.1%)21 (45.6%)13 (28.3%)
4 (1.9%)28 (13.5%)134 (64.4%)32 (15.4%)10 (4.8%)
< 0.0001
10

Table 5. Change in pain intensity at follow-up among subjects with pain at baseline.
Decrease Unadjusted Diff Adjusted Diff
VariableCTA Mean (SD) Diff 95% CI Diff 95% CI p
+ 0.79 (1.8)Chest pain now- 0.28 (2.1)
0.50 -0.4, 1.4 0.46 -0.4, 1.3 0.274
+ 1.15 (2.0)Maximum chestpain* - 0.12 (2.2)
1.03 0.3, 1.8 1.15 0.4, 1.8 0.001
+ 0.56 (1.7)Average chest pain*
- 0.23 (2.0)0.33 -0.3, 1.0 0.63 0.0, 1.2 0.048
+ 1.03 (2.5)Average thoracicspine pain* - 0.69 (2.0)
0.35 -0.6, 1.3 0.54 -0.3, 1.4 0.228
+ 1.00 (2.4)Average neck pain*
- 0.59 (2.0)0.41 -0.5, 1.3 0.45 -0.3, 1.2 0.256
+ 1.31 (2.1)Average shoulderarm pain* - 0.89 (2.2)
0.42 -0.5, 1.3 0.44 -0.4, 1.4 0.294
* During the preceding 14 days.
Table 6. Increases in quality of life profile (SF-36) scores at follow-up compared to baseline.
Increase Unadjusted Diff Adjusted DiffVariableCTA Mean SD Diff 95% CI Diff 95% CI
p-value
+ 0 12.9Physicalfunctioning - -1.39 13.0
1.4 -2.8, 5.6 2.5 -1.8, 6.8 0.253
+ 8.15 21.1Role physical- -0.44 30.6
8.6 -0.8, 18.0 12.3 2.8, 21.9 0.011
+ 4.22 14.7Bodily pain
- 0.39 17.33.8 -1.6, 9.2 4.9 -0.3, 10.1 0.066
+ 0.53 12.5General health- -0.27 12.9
0.8 -3.3, 5.0 2.6 -1.7, 6.8 0.232
+ 10.44 17.7Vitality
- 0.72 15.89.7 4.5, 14.9 0.6 4.6, 14.5 <0.001
+ 4.62 17.2Socialfunctioning - -1.51 15.9
6.1 0.9, 11.3 5.4 0.6, 10.3 0.029
+ 16.30 34.5Role emotional- 2.59 37.6
13.7 1.7, 25.7 16.2 5.6, 26.8 0.003
+ 4.43 15.1Mental health- -0.74 14.4
5.2 0.5, 9.8 4.8 0.4, 9.2 0.033
CTA+: N=46 and CTA-: N=208
11

Figure 1: Standardized quality of life scores (SF-36) in the entire study population (n=275). Avalue of 0 indicates equal score as in the background population, a negative value indicates a lowerand positive value a higher quality of life. Values are given as median values compared topopulation mean.
12

Reference List
(1) Braunwald E. Part I: Examination of the patient: The history. In: Braunwald E, Heartdisease. 6 ed. W.B. Saunders Company; 2001: 27-45.
(2) Management of stable angina pectoris. Recommendations of the Task Force of theEuropean Society of Cardiology. Eur Heart J. 1997;18:394-413.
(3) Hoilund-Carlsen, P. F., Johansen, A, Christensen, H. W., Bartram, P, Veje, A, Lerbjerg, G,Haghfelt, T., and Vach, W. Prevalence of normal myocardial perfusion in danish patientsreferred to diagnostic coronary angiography for stable angina pectoris (submitted).
(4) Hemingway H, Marmot M. Evidence based cardiology: psychosocial factors in the aetiologyand prognosis of coronary heart disease. Systematic review of prospective cohort studies.BMJ. 1999;318:1460-1467.
(5) Fleet RP, Dupuis G, Marchand A, Burelle D, Beitman BD. Panic disorder, chest pain andcoronary artery disease: literature review. Can J Cardiol. 1994;10:827-34.
(6) Chambers J, Bass C. Chest pain with normal coronary anatomy: a review of natural historyand possible etiologic factors. Prog Cardiovasc Dis. 1990;33:161-84.
(7) Bechgaard, P. Segmental thoracic pain in patients admitted to a medical department and acoronary care unit. Acta Med Scand 1981;supple 644:87-89.
(8) Wise, C. M., Semble, E. L., and Dalton, C. B. Musculoskeletal chest wall syndromes inpatients with noncardiac chest pain: A study of 100 patients. Arch Phys Med Rehabil 1992;73,147-149.
(9) Epstein, S. E., Gerber, L. H., and Borer, J. S. Chest wall syndrome:A common cause ofunexplained cardiac pain. JAMA 1979;241(26):2793-2797.
(10) Levine, P. R. and Mascette, A. M. Musculoskeletal chest pain in patients with "angina": Aprospective study. South.Med.J 1989;82(5):580-585.
(11) Hamberg J, Lindahl O. Angina pectoris symptoms caused by thoracic spine disorders.Clinical examination and treatment. Acta Med Scand Suppl. 1981;644:84-86.
(12) Berman DS, Germano G, Shaw LJ. The role of nuclear cardiology in clinical decisionmaking. Semin Nucl Med. 1999;29:280-297.
(13) Lavey EB, Winkle RA. Continuing disability of patients with chest pain and normalcoronary arteriograms. J Chronic Dis. 1979;32:191-96.
(14) Ockene IS, Shay MJ, Alpert JS, Weiner BH, Dalen JE. Unexplained chest pain in patientswith normal coronary arteriograms: a follow-up study of functional status. N Engl J Med.1980;303:1249-52.
(15) Sullivan AK, Holdright DR, Wright CA, Sparrow JL, Cunningham D, Fox KM. Chest painin women: clinical, investigative, and prognostic features. BMJ. 1994;308:883-86.
13

(16) Lantinga LJ, Sprafkin RP, McCroskery JH, Baker MT, Warner RA, Hill NE. One-yearpsychosocial follow-up of patients with chest pain and angiographically normal coronaryarteries. Am J Cardiol. 1988;62:209-13.
(17) Christensen, H. W., Vach, W., Manniche, C., Haghfelt, T., Hartvigsen, L., and Hoilund-Carlsen, P. F. Palpation of the upper thoracic spine: an observer reliability study. JManipulative Physiol Ther 2002;25(5): 285-292.
(18) Christensen, H. W., Vach, W., Manniche, C., Haghfelt, T., Hartvigsen, L., and Hoilund-Carlsen, P. F. Palpation of the anterior chest wall - an observer reliability study. JManipulative Physiol Ther (to appear).
(19) Christensen, H. W., Vach, W., Gichangi, A., Manniche, C., Haghfelt, T., and Hoilund-Carlsen, P. F. Cervico-thoracic angina identified by case history and palpation findings inpatients with stable angina pectoris (submitted).
(20) Peterson DH. Principles of Adjustive Technique. In: Bergmann TF, Peterson DH, LawrenceDJ, eds. Chiropractic Technique. 1 ed. New York: Churchill Livingstone Inc; 1993: 123-96.
(21) Simons, D. S., Travell, J. G., and Simons, L. S. Myofascial Pain and Dysfunction. Thetrigger point manual. 2(1), 1-1029. 1999. Baltimore, Williams & Wilkins.
(22) Bjørner JB, Damsgaard MT, Watt T, Bech P, Rasmussen NK, Kristensen TS et al. Danskmanual til SF-36 - et spørgeskema om helbredsstatus. Lif Lægemiddelindustriforeningen;1997.
(23) Nijher G, Weinman J, Bass C, Chambers J. Chest pain in people with normal coronaryanatomy. BMJ. 2001;323:1319-20.
(24) Coulshed DS, Eslick GD, Talley NJ. Non-cardiac chest pain. Patients need diagnoses. BMJ.2002;324:915.
(25) Eslick GD, Coulshed DS. Rapid assessment of chest pain. Chest pain clinics may be onestep forward, two steps back. BMJ. 2002;324:422.
(26) Capewell S, McMurray J. "Chest pain-please admit": is there an alternative?. A rapidcardiological assessment service may prevent unnecessary admissions. BMJ. 2000;320:951-52.
(27) Best RA. Non-cardiac chest pain: a useful physical sign? Heart. 1999;81:450.
(28) Chambers J, Bass C, Mayou R. Non-cardiac chest pain: assessment and management. Heart.1999;82:656-57.
(29) Mayou R, Bryant B, Forfar C, Clark D. Non-cardiac chest pain and benign palpitations inthe cardiac clinic. Br Heart J. 1994;72:548-53.
(30) Cohn JK, Cohn PF. Cardiology patient pages. Chest pain. Circulation. 2002;106:530-531.
14

(31) Bronfort G, Evans R, Nelson B, Aker PD, Goldsmith CH, Vernon H. A randomized clinicaltrial of exercise and spinal manipulation for patients with chronic neck pain. Spine.2001;26:788-97.
(32) Hoving JL, Koes BW, de Vet HC, van der Windt DA, Assendelft WJ, van Mameren H et al.Manual therapy, physical therapy, or continued care by a general practitioner for patientswith neck pain. A randomized, controlled trial. Ann Intern Med. 2002;136:713-22.
(33) Elliott AM, Smith BH, Hannaford PC, Smith WC, Chambers WA. Assessing change inchronic pain severity: the chronic pain grade compared with retrospective perceptions. Br JGen Pract. 2002;52:269-74.
(34) Bland JM, Altman DG. Some examples of regression towards the mean. BMJ.1994;309:780.
(35) Hansen, P. H. and Duel, P. Angina Pectoris. Ugeskr Laeger 1982;144:50-51.
(36) Mortensen, P. S. Angina pectoris - pseudoangina pectoris. Nordisk Medicin 1963;69:23.
(37) Bechgaard, P. Det torakale segmentære smertesyndrom, facet syndrom. Ugeskr Laeger1982;144(1):11-12.
(38) Wax CM, Abend DS, Pearson PH. Chest pain and the role of somatic dysfunction. J AmOsteopath Assoc. 1997;97:347-52.
(39) Polkinghorn BS, Colloca CJ. Chiropractic management of chronic chest pain usingmechanical force, manually assisted short-lever adjusting procedures. J ManipulativePhysiol Ther. 2003;26:108-15.
(40) Barker, M. E. Manipulation in general medical practice for thoracic pain syndromes. BrOsteopathic J 15, 95-97. 1983.
(41) Rogers, J. T. and Rogers, J. C. The role of osteopathic manipulative therapy in the treatmentof coronary heart disease. J Am Osteopathic Ass 1976;76:71-81.
(42) Schiller L. Effectiveness of spinal manipulative therapy in the treatment of mechanicalthoracic spine pain: a pilot randomized clinical trial. J Manipulative Physiol Ther.2001;24:394-401.
(43) Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. Manipulation andmobilization of the cervical spine. A systematic review of the literature. Spine.1996;21:1746-59.
(44) Gross AR, Kay T, Hondras M, Goldsmith C, Haines T, Peloso P et al. Manual therapy formechanical neck disorders: a systematic review. Man Ther. 2002;7:131-49.
15