musculoskeletal examination of the runner part 1 …-+h2+-+ch...shear. evaluate the mobility and...
TRANSCRIPT

Musculoskeletal Examination of the Runner – Part 1 Clinical Examination of the Runner: Assessment, Testing, Gait Correlations, and Corrections Jay Dicharry – MPT, SCS
Exercise Slides (Ch. 2)
Image(s) Check Off
Bilateral Squat 6 - 8
Dynamic valgus or symmetry correlates to poor vs. effective movement strategy. Early heel rise can suggest tight chords. Knee forward suggests quad dominance and potential over-stride. Hips
back suggest good glut recruitment.
Single Leg Stance
8
Correlates to general balance. Pay special attention to foot contact of 1st ray. Wobble is ok, as long as the wobble “strategy” is to maintain 1st metatarsal head support. Ask the patient to keep
eyes up to increase the challenge
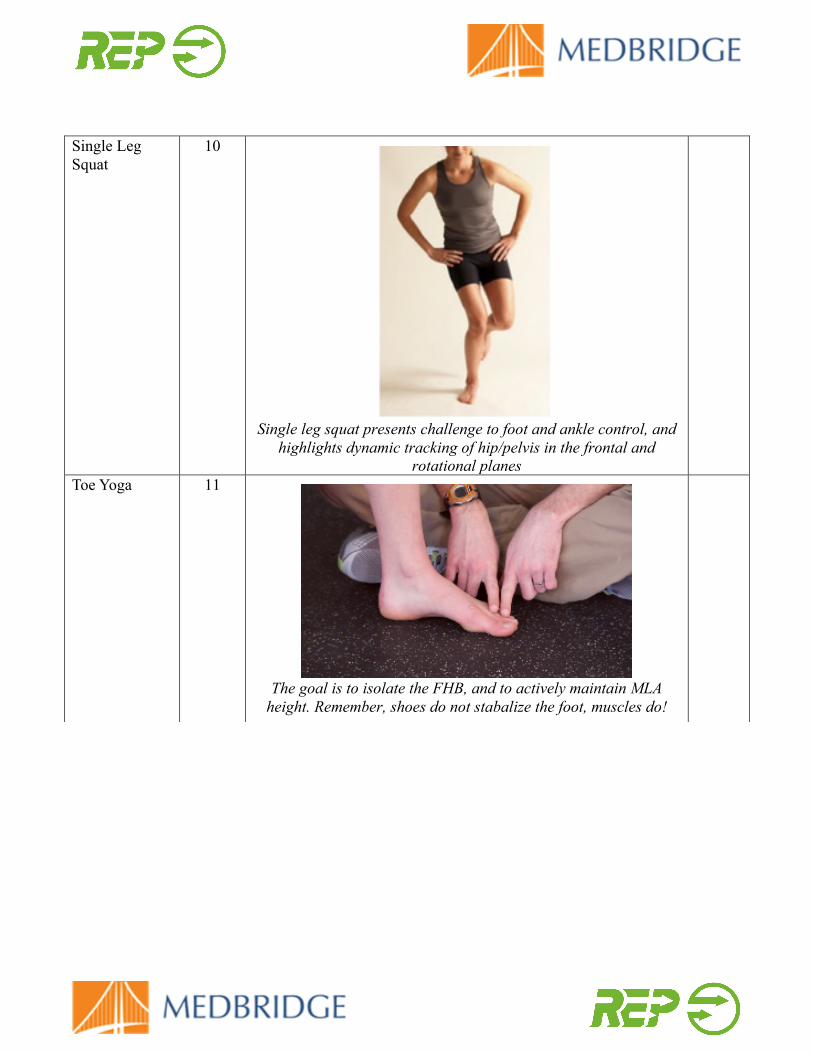
Single Leg Squat
10
Single leg squat presents challenge to foot and ankle control, and
highlights dynamic tracking of hip/pelvis in the frontal and rotational planes
Toe Yoga 11
The goal is to isolate the FHB, and to actively maintain MLA
height. Remember, shoes do not stabalize the foot, muscles do!

Posterior Tibialis Insufficiency
12
Rear foot on forefoot control. Implicated in plantar fascia issues, post tibialis, soleus, and gastrocnemius strains. Performance is
dependant on forefoot stability
Foot Alignment
13
Look for structural reasons why the patient may be staying excessively lateral or medial on the foot in stance. Examine need
for orthotic to provide full foot contact. Evaluate whethere the patient can paintain STJN with full contact of 1st ray.
ROT Trunk on Pelvis & Pelvis on Trunk
14
Evaluates lumbar coordination and stabilization, and separates
rotation vs. default to pelvic shift or extension.

Lumbar Range of Motion
15
Look for symmetry, do you see reveral of lordosis in flexion?
Correlation to psoas? Extension? Symmetric rotation and SB? Stiffness or pain may indicated a shift in pelvis and ML
stabilization.
VCT for Postural Stability
16
Athletes should know of to find neutral posture while walking, training, lifting, and under fatigue.
Overhead Reach Lunge Test
17
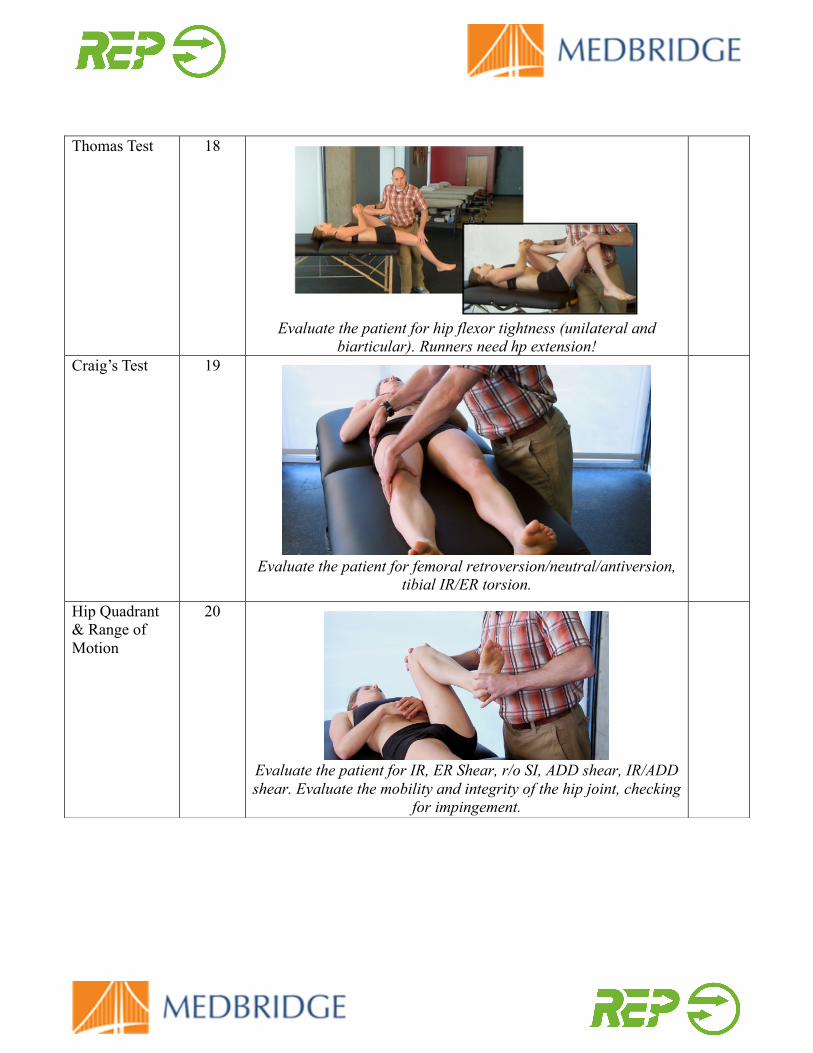
Thomas Test 18
Evaluate the patient for hip flexor tightness (unilateral and
biarticular). Runners need hp extension!
Craig’s Test 19
Evaluate the patient for femoral retroversion/neutral/antiversion,
tibial IR/ER torsion.
Hip Quadrant & Range of Motion
20
Evaluate the patient for IR, ER Shear, r/o SI, ADD shear, IR/ADD shear. Evaluate the mobility and integrity of the hip joint, checking
for impingement.
Notes: