musculoskeletal imaging
TRANSCRIPT

IMAGINGMUSCULOSKELETAL
30 D I E U R O P E JULY/AUGUST 2013
By Dr Christopher Vercollone, Dr Scott Martin, Dr Bin Liu, & Dr Mark E Brezinski
New approaches to the management of musculoskeletal disease using Optical Coherence Tomography (OCT)
Imaging modalities such as MRI, CT, and ultra-sound are critical to managing the patient with musculoskeletal disease. However, a need still exists for assessing many pathologic states at
higher resolutions, near that of histology. This is par-ticularly critical for early pathology of bone, cartilage, and tendon, as they are generally not readily amenable to biopsy. Specific pathophysiologies where this level of resolution is needed includes early osteoarthritis (OA), tendon disorders (particularly rotator cuff repairs, RCR), and rheumatoid arthritis (RA). Optical coher-ence tomography (OCT) is a micron scale imaging technology which is now in widespread use in ophthal-mology and cardiology [1,2]. This papers looks at the role of OCT in musculoskeletal disorders.
This paper is organized in the following manner: first, we briefly review the technology, which is discussed in depth in other places. In the next section, we focus on the use of OCT in early OA, which is perhaps its most important application in orthopedics. In the third sec-tion, we discuss its role in rotator cuff repair, where we feel at this stage its ability to monitor the study of fibro-cartilage regeneration will have the biggest impact. Once therapeutics have been established to augment rotator cuff repair, then we foresee its transition to direct patient care. The fourth section deals with its role in RA man-agement. Here, a need exists for identifying the subset of early destructive disease for aggressive therapy, an objec-tive not achievable with current imaging modalities. In addition to patient management, it has demonstrated feasibility for rheumatoid animal research work in both understanding pathophysiology and therapeutics.
OPTICAL COHERENCE TOMOGRAPHY
OCT is analogous to ultrasound, measuring the back-reflection of infrared light (as a function of depth) rather than sound. However due to the high speed associated with light propagation, the backreflec-tion time cannot be measured directly so a technique known as low-coherence interferometry (LCI) is used. This is discussed elsewhere [1]. By plotting backreflec-tion intensity as a function of depth, two and three dimensional data sets can be generated which pro-vide information on tissue microstructure. This tech-nique leads to resolutions of 2-20μm (depending on the source) and recording speeds up to 120 frames/sec. More importantly, OCT can be incorporated into endocatheters (arthroscopes) as small as 0.017 inches ( 0.43 mm), with the engine itself smaller than a por-table ultrasound machine [3,4]. These features have allowed real time micron scale, real-time clinical imag-ing during arthrosocopy and the potential of office based imaging [0,17].
Although various adjunct OCT technologies exist above pure structural imaging, the polarization sensi-tive embodiment (PS-OCT) is particularly useful for musculoskeletal analysis [5,8]. PS-OCT is capable of assessing collagen organization and angle in tissues such as tendon and cartilage. Collagen changes are a hallmark of early musculoskeletal disease in particu-lar. Briefly, as the polarization state of incident light is rotated, a large change in the degree of backreflec-tion intensity signifies the presence of a highly orga-nized, dense collagen. In contrast, breakdown of this organized birefringence is indicative of early micro-structural degradation, allowing the relative health of tissue to be assessed before gross image changes [5,8]. This capability has been demonstrated to lead to ear-lier detection of clinical pathophysiologies than other imaging modalities [10,17].
The Authors:
Christopher Vercollone 1, 2, Scott Martin1, 2, Bin Liu1, 2 and Mark
E. Brezinski 1, 2, 3
1. Center for Optical Coherence Tomography and Optical Physics, Department of Orthopedic Surgery, Brigham and Women’s Hospital,75 Francis Street, Boston, MA 02115, USA
2. Harvard Medical School, Boston, MA 02115, USA
3. Massachusetts Institute of Technology, Cambridge, MA 02139
Correspondence should be addressed to:
Mark E. Brezinski; email: [email protected]
“...Polarisation-sensitive OCT is particularly useful for musculoskeletal analysis...”
Die_Juin-juillet_2013_p26-40.indd 30Die_Juin-juillet_2013_p26-40.indd 30 26/07/13 13:2026/07/13 13:20
JULY/AUGUST 2013 D I E U R O P E 31
OCT IN OSTEOARTHRITIS (OA)
One of the areas of greatest poten-tial impact for OCT and PS-OCT is in the early detection of OA, identify-ing the need for intervention prior to cartilage destruction. OA is a leading cause of disability, so identification at early stages and tailored interven-tion would not only impact patient morbidity, but could have a dramatic impact on the overall health care eco-nomic burden. OA is generally identi-fied at the stage of full/partial thick-ness cartilage defects with substantial distortion of the subchondral bone.
By this stage OA is essentially irrevers-ible. Thus, it is imperative to diagnose OA at early stages. Early OA changes in an arthritic joint consist of the loss of an organized collagen, subchondral bone integrity, and glycosaminoglycan matrix [6,7]. All three of these can be identified by OCT and its adjuvant approaches.
Initially, extensive analysis was performed to compare and match OCT imaging with histopathology to confidently make distinctions between normal and diseased tissue states (structural imaging). General microstructural features have since become easily distinguished, such as the thickness of cartilage and sub-chondral bone, and the presence of pathological fibrocartilage. Now, stud-ies have progressed to the imaging and assessment of human cartilage in vivo, open surgery and arthroscopic, including utilizing PS-OCT [10,17].
Normal tissue exhibited properties of highly organized collagen, as well as intact subchondral bone. In contrast, initial disease progression was dem-onstrated by the initial loss of orga-nized collagen and subchondral bone integrity. These results were verified with histopathology, including special staining, particularly in the open joint study [8-10].
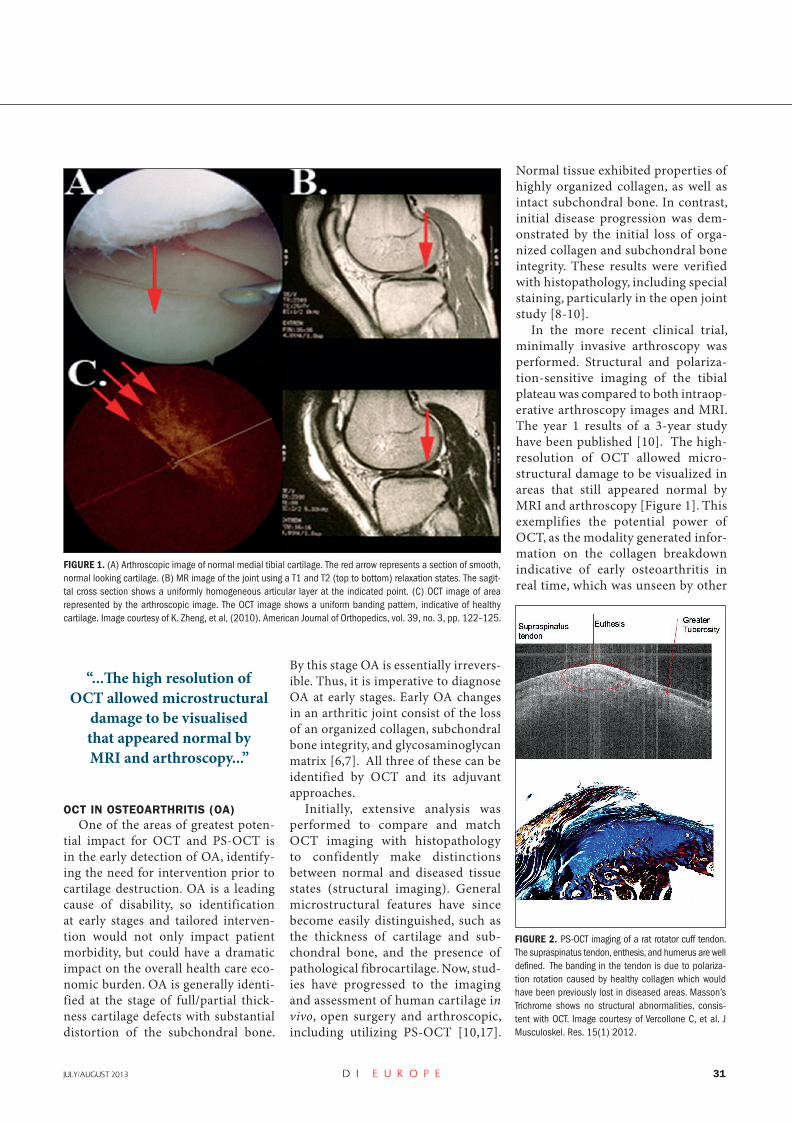
In the more recent clinical trial, minimally invasive arthroscopy was performed. Structural and polariza-tion-sensitive imaging of the tibial plateau was compared to both intraop-erative arthroscopy images and MRI. The year 1 results of a 3-year study have been published [10]. The high-resolution of OCT allowed micro-structural damage to be visualized in areas that still appeared normal by MRI and arthroscopy [Figure 1]. This exemplifies the potential power of OCT, as the modality generated infor-mation on the collagen breakdown indicative of early osteoarthritis in real time, which was unseen by other
FIGURE 1. (A) Arthroscopic image of normal medial tibial cartilage. The red arrow represents a section of smooth, normal looking cartilage. (B) MR image of the joint using a T1 and T2 (top to bottom) relaxation states. The sagit-tal cross section shows a uniformly homogeneous articular layer at the indicated point. (C) OCT image of area represented by the arthroscopic image. The OCT image shows a uniform banding pattern, indicative of healthy cartilage. Image courtesy of K. Zheng, et al, (2010). American Journal of Orthopedics, vol. 39, no. 3, pp. 122–125.
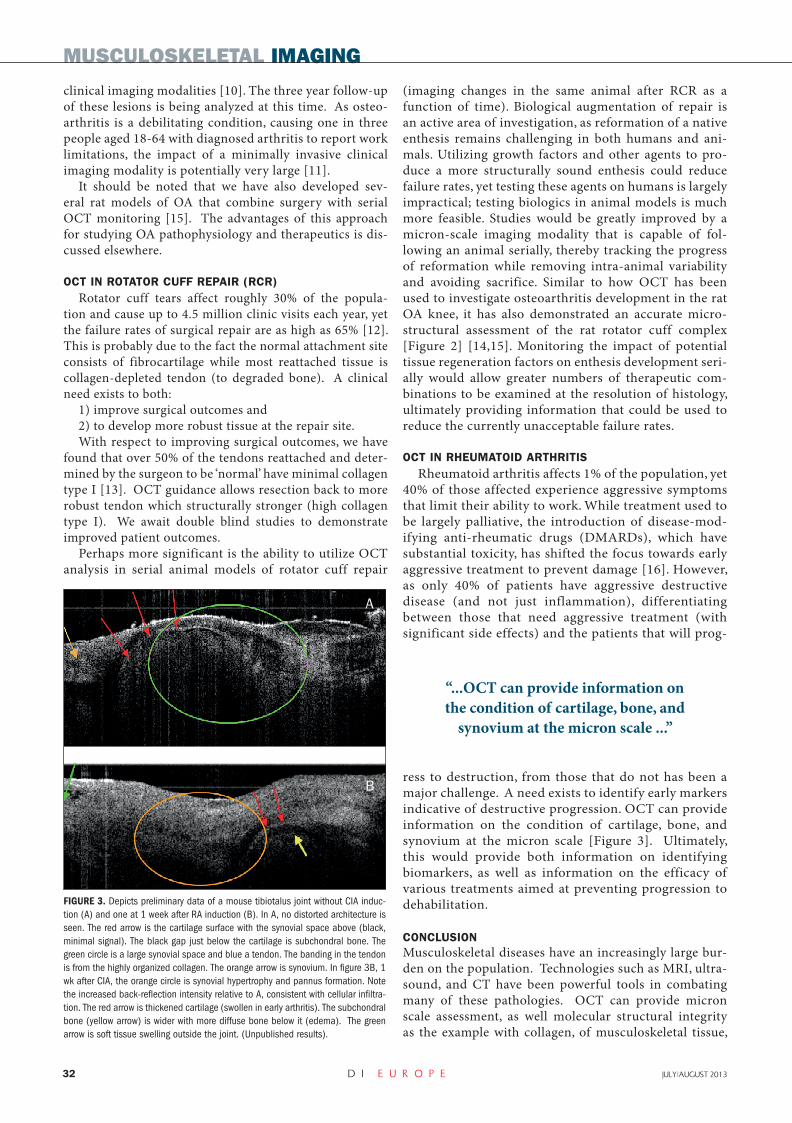
FIGURE 2. PS-OCT imaging of a rat rotator cuff tendon. The supraspinatus tendon, enthesis, and humerus are well defined. The banding in the tendon is due to polariza-tion rotation caused by healthy collagen which would have been previously lost in diseased areas. Masson’s Trichrome shows no structural abnormalities, consis-tent with OCT. Image courtesy of Vercollone C, et al. J Musculoskel. Res. 15(1) 2012.
“...Th e high resolution of OCT allowed microstructural
damage to be visualised that appeared normal by MRI and arthroscopy...”
Die_Juin-juillet_2013_p26-40.indd 31Die_Juin-juillet_2013_p26-40.indd 31 26/07/13 13:2026/07/13 13:20
32 D I E U R O P E JULY/AUGUST 2013
MUSCULOSKELETAL IMAGING
clinical imaging modalities [10]. The three year follow-up of these lesions is being analyzed at this time. As osteo-arthritis is a debilitating condition, causing one in three people aged 18-64 with diagnosed arthritis to report work limitations, the impact of a minimally invasive clinical imaging modality is potentially very large [11].
It should be noted that we have also developed sev-eral rat models of OA that combine surgery with serial OCT monitoring [15]. The advantages of this approach for studying OA pathophysiology and therapeutics is dis-cussed elsewhere.
OCT IN ROTATOR CUFF REPAIR (RCR)
Rotator cuff tears affect roughly 30% of the popula-tion and cause up to 4.5 million clinic visits each year, yet the failure rates of surgical repair are as high as 65% [12]. This is probably due to the fact the normal attachment site consists of fibrocartilage while most reattached tissue is collagen-depleted tendon (to degraded bone). A clinical need exists to both:
1) improve surgical outcomes and2) to develop more robust tissue at the repair site. With respect to improving surgical outcomes, we have
found that over 50% of the tendons reattached and deter-mined by the surgeon to be ‘normal’ have minimal collagen type I [13]. OCT guidance allows resection back to more robust tendon which structurally stronger (high collagen type I). We await double blind studies to demonstrate improved patient outcomes.
Perhaps more significant is the ability to utilize OCT analysis in serial animal models of rotator cuff repair
(imaging changes in the same animal after RCR as a function of time). Biological augmentation of repair is an active area of investigation, as reformation of a native enthesis remains challenging in both humans and ani-mals. Utilizing growth factors and other agents to pro-duce a more structurally sound enthesis could reduce failure rates, yet testing these agents on humans is largely impractical; testing biologics in animal models is much more feasible. Studies would be greatly improved by a micron-scale imaging modality that is capable of fol-lowing an animal serially, thereby tracking the progress of reformation while removing intra-animal variability and avoiding sacrifice. Similar to how OCT has been used to investigate osteoarthritis development in the rat OA knee, it has also demonstrated an accurate micro-structural assessment of the rat rotator cuff complex [Figure 2] [14,15]. Monitoring the impact of potential tissue regeneration factors on enthesis development seri-ally would allow greater numbers of therapeutic com-binations to be examined at the resolution of histology, ultimately providing information that could be used to reduce the currently unacceptable failure rates.
OCT IN RHEUMATOID ARTHRITIS
Rheumatoid arthritis affects 1% of the population, yet 40% of those affected experience aggressive symptoms that limit their ability to work. While treatment used to be largely palliative, the introduction of disease-mod-ifying anti-rheumatic drugs (DMARDs), which have substantial toxicity, has shifted the focus towards early aggressive treatment to prevent damage [16]. However, as only 40% of patients have aggressive destructive disease (and not just inflammation), differentiating between those that need aggressive treatment (with significant side effects) and the patients that will prog-
ress to destruction, from those that do not has been a major challenge. A need exists to identify early markers indicative of destructive progression. OCT can provide information on the condition of cartilage, bone, and synovium at the micron scale [Figure 3]. Ultimately, this would provide both information on identifying biomarkers, as well as information on the efficacy of various treatments aimed at preventing progression to dehabilitation.
CONCLUSION
Musculoskeletal diseases have an increasingly large bur-den on the population. Technologies such as MRI, ultra-sound, and CT have been powerful tools in combating many of these pathologies. OCT can provide micron scale assessment, as well molecular structural integrity as the example with collagen, of musculoskeletal tissue,
FIGURE 3. Depicts preliminary data of a mouse tibiotalus joint without CIA induc-tion (A) and one at 1 week after RA induction (B). In A, no distorted architecture is seen. The red arrow is the cartilage surface with the synovial space above (black, minimal signal). The black gap just below the cartilage is subchondral bone. The green circle is a large synovial space and blue a tendon. The banding in the tendon is from the highly organized collagen. The orange arrow is synovium. In figure 3B, 1 wk after CIA, the orange circle is synovial hypertrophy and pannus formation. Note the increased back-reflection intensity relative to A, consistent with cellular infiltra-tion. The red arrow is thickened cartilage (swollen in early arthritis). The subchondral bone (yellow arrow) is wider with more diffuse bone below it (edema). The green arrow is soft tissue swelling outside the joint. (Unpublished results).
“...OCT can provide information on the condition of cartilage, bone, and
synovium at the micron scale ...”
A
B
Die_Juin-juillet_2013_p26-40.indd 32Die_Juin-juillet_2013_p26-40.indd 32 26/07/13 13:2026/07/13 13:20

JULY/AUGUST 2013 D I E U R O P E 33
both in humans and animals. This strongly predicts its powerful impact on the field, allowing assessments at unprecedented resolutions.
ACKNOWLEDGEMENTS
This work was supported by Dr. Brezinski’s funding from the National Institute of Health Grants R01 AR44812, R01 HL55686, R01 EB02638/HL63953, R01 AR46996, R01 EB000419, and R21EB015851-01. The authors would like to thank the efforts of Bin Liu PhD and Chris Vecollone in preparing the paper. We would also like Joseph Loscalzo MD, PhD for his insights.
REFERENCES
1. M. E. Brezinski, Optical Coherence Tomography: Principles and Applications Academic Press, Burlington, MA; 2006.
2. M.E. Brezinski, G.J. Tearney, B.E. Bouma, J.A. Izatt, M.R. Hee, E.A. Swanson, J.F. Southern, J.G. Fujimoto. Optical Coherence Tomography for Optical Biopsy: Properties and Demonstration of Vascular Pathology. Circulation 93, 1206-1213, 1996 (PMID: 8653843).
3. Brezinski ME, Fujimoto JG. Optical coherence tomography: High-resolution imaging in nontransparent tissue. IEEE J. Sel. Top. Quant. Electron. 1999; 5(4):1185-1192.
4. Tearney GJ, Brezinski ME, Bouma BE, et al. In vivo endoscop-ic optical biopsy with optical coherence tomography. Science. 1997;276(5321):2037-9.
5. Liu B, et al. Characterizing of Tissue Microstructure with Single-Detector Polarization-Sensitive Optical Coherence Tomography. Appl. Opt. 2006; 45:4464-4479
6. Ryu J, Treadwell BV, Mankin HJ. Biochemical and metabolic abnor-malities in normal and osteoarthritic human articular cartilage. Arthritis Rheum. 1984; 27:49.
7. Hootman JM, Helmick CG. Projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum 2006; 54: 226–9.
8. Drexler W, et al., Correlation of Collagen Organization with Polarization Sensitive I aging in Cartilage: Implications for Osteoarthritis. J. of Rheum 2001 28:1311-1318
9. Herrmann J, et al. High Resolution Imaging Of Normal And Osteoarthritic Cartilage With Optical Coherence Tomography. J of Rheum. 1999;26:3:627-635.
10. Zheng K, Martin SD, Rashidifard CH, Liu B, Brezinski ME. In vivo micron-scale arthroscopic imaging of human knee osteoarthri-tis with optical coherence tomography: comparison with mag-netic resonance imaging and arthroscopy. Am. J. Ortho. 2010; 39(3):122–125.
11. Hootman J, Bolen J, Helmick C, Langmaid G. Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation. Morb. Mortal. Wkly. 2006; 55(40):1089-1092.
12. Oh LS, et al. Indications for rotator cuff repair: a systematic review. Clin Orthop Relat Res. 2007; 455:52.
13. Rashidifard C, et al. Single detector polarization-sensitive opti-cal coherence tomography for assessment of rotator cuff tendon integrity. Am. J. Ortho. 2012; 41(8):351-357
14. Vercollone C, et al. New technological approach to study rotator
cuff pathology. J Musculoskeletal Res. 2012; 15(1).
15. Adams SB, et al. High resolution imaging of progressive articular
cartilage degeneration. J Orthop Res. 2006; 24: 708-715.
16. Saag KG, et. al. Recommendations for the use of nonbiologic
and biologic disease mo fying anti-rheumatic drugs in RA. 2008;
Arth. Rheum. 59: 762-784.
17. X. Li, S. D. Martin, C. Pitris, et al., “High-resolution optical
coherence tomography imaging of osteoarthritic cartilage during
open knee surgery,” Arthritis Research & Therapy, vol. 7, pp.
R318–R323, 2005
AppendixThis appendix discusses some of the adjuvant OCT techniques beyond structural imaging.
Polarization-Sensitive OCT: PS-OCT measures the birefringence of samples by assessing the polarization state of back-reflected light. Highly organized tissue, such as collagen, modifies the polarization state of inci-dent light in a homogeneous fashion, producing a uniform banding pattern on OCT imaging. This not only provides microstructural infor-mation from conventional OCT, but allows the assessment of the sample’s organization (in terms of degree of birefringence), which is indicative of disease progression.
Doppler OCT: Doppler OCT combines traditional OCT with laser Doppler velocimetry. As the Doppler fre-quency shifts do not produce a large effect on the conventional OCT image, they can be used concurrently. And, as the wavelength of light is shorter than sound, the resolution is far greater than that generated by traditional ultrasound Doppler imaging. Adding this high resolution spatial imaging to the traditionally non-imaging technique of laser Doppler velocimetry allows for the assessment of clinical flow measurements, such as blood flow.
OCT Elastography: This technique measures the mechanical properties of tissue in a manner similar to ultrasound elas-tography. A mechanical force is applied to a tissue sample, and the resultant alteration in the tissue is recorded, producing information about the tissue’s composition. Applications include phantoms and skin, with recent advances in the use of Air-Inden-tation OCT Elastography to assess mechanical properties of in-vivo human skin in the extremities.
OCT Spectroscopy: In addition to OCT absorption spectroscopy, which functions by combining traditional OCT with spec-troscopic analyses, recent work has shown promise in the development of a second order correlation (SOC) measurement technique. This technique uti-lizes photon entanglement, a quantum phenom-
enon which gives insight into tissue composition.
Die_Juin-juillet_2013_p26-40.indd 33Die_Juin-juillet_2013_p26-40.indd 33 26/07/13 13:2026/07/13 13:20