musings from a child psychiatrist
TRANSCRIPT
Everything you wanted to know about
child psychiatry (maybe) but were afraid
to ask
Betty Tang, MD, FRCPC
2016
OUTLINE
• What is psychiatry?
• Developmental factors
• Temperament
• Environment
• Genetics
• Diagnostic Assessment
• Psychiatric disorders
• Treatment options

WHAT IS PSYCHIATRY?
• The branch of medicine that deals with the
diagnosis, treatment, and prevention of
mental and emotional disorders
• Any psychiatric disorder is a clinical
diagnosis, looking at phenomenology
• Specific causality is not usually part of any
diagnosis
CASE HISTORY 1
• “Bev” is a client with moderate DD in her
mid-40s. She had lived with her caregiver
for about 5 years; during this time, this
caregiver found Bev’s behaviour very
difficult, with irritability, trouble sleeping,
and verbal aggression. 3 medications for
depression and anxiety were trialed
without success (and added side effects).

CASE HISTORY 2
• “Elaine” is 14 years old. There is a family
history of mood disorders. Elaine is
described by her mother as severely
oppositional with running away behaviour,
swearing, and school refusal. She had
previously been diagnosed as having
conduct disorder. On further history,
significant episodes of depression were
identified.

CASE HISTORY 3
• “John” had a poor relationship with his
mother and an excellent relationship with
his father. He was diagnosed with ADHD,
which his father felt was inaccurate.

CASE HISTORY 4
• “Angie” was 14 years old when we first
met her. She had already seen 2
psychiatrists at BCCH and had been
diagnosed with substance abuse,
depression, and anxiety. She was
prescribed an SSRI antidepressant.

Brain Development
• Neuroanatomical regions and neurotransmitter systems develop at different rates and mature at different times
• Neurogenesis, cell migration, formation of connectivity, and myelination
• Overproduction and pruning during childhood and adolescence
• Plasticity and sensitive periods
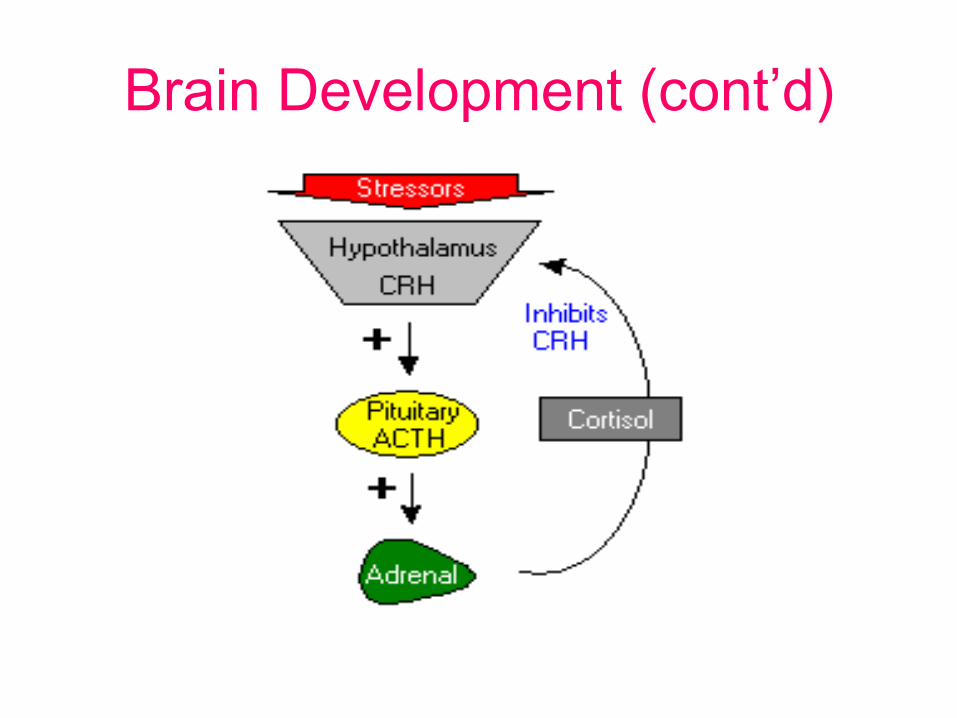
Brain Development (cont’d)
• Relationship between stress, activation of limbic-hypothalamic-pituitary-adrenal axis, and cortisol
• Blunted ACTH responses to CRF challenge
• Early stress may hinder hippocampal neurogenesis, and alter structure and functioning (particularly learning and memory)
Brain Development (cont’d)
Attachment, Cognition, and all that • Plasticity and sensitive periods
• John Bowlby, Mary Ainsworth – Attachment – preferences for particular familiar people
– tendency to seek proximity to those people, especially in times of distress
– the ability to use the familiar adults as a secure base from which to explore the environment.
• Jean Piaget – Theory of Cognitive Development – Sensorimotor – 0 to 2 years
– Preoperational (egocentric, symbolic play) – 2 – 7 years
– Concrete Operations (logic, classification) - 7 – 11 years
– Formal operations (abstract reasoning) – 11 – 16 years
• Erik Erikson – Life Stages – Trust vs Mistrust
– Autonomy vs Shame and Doubt
– Initiative vs Guilt
– Industry vs Inferiority
– Identity vs Role Confusion

TEMPERAMENT
• Dimensions: – Activity level, rhythmicity, approach-withdrawal, adaptability,
persistence-attention span, intensity of reaction, distractibility, threshold of responsiveness, quality of mood
• Easy (40%): regular routines, cheerful, adaptable
• Difficult (10%): irregular, slow to accept change, tending to respond negatively
• Slow to warm up (15%): inactive, mild, low-key responsiveness, negative or neutral mood and slow adjustment
• Mix of characteristics (35%)
• “goodness of fit” predicts adaptability and resilience

PARENTING STYLE (Berk, Child Development, 2005)
PARENTING
STYLE
NURTURANCE CONTROL AUTONOMY
AUTHORITATIVE Warm, attentive and
sensitive to child’s
needs
Reasonable demands
for maturity, explains
and reinforces rules
Permits child to make
decisions when
developmentally ready
AUTHORITARIAN Cold and rejecting,
degrades child
Makes demands
coercively by yelling
and criticising
Makes decisions for
the child and rarely
listens to the child’s
viewpoint
PERMISSIVE Warm and
overindulgent or
inattentive
Makes few or no
demands
Permits child to make
many decisions before
developmentally ready
UNINVOLVED Emotionally detached
and withdrawn
Makes few or no
demands
Is indifferent to child’s
decision making and
viewpoint

ENVIRONMENT • Attachment - Ainsworth
– Secure
– Insecure (avoidant, ambivalent / resistant)
– disorganized
• Family and caregiver influences – poor child-parent relations
– Parental alcoholism
– Physical abuse
– Degree of parental impairment (i.e. severe depression)
– Severe parental discord (actually more pathogenic than loss of a
parent by death)
• Peer relationships, school, social media
• Cultural context
GENETICS
• Depression (MDE): – First-degree relatives of individuals with MDE are 1.5-3 X more
likely to develop MDE
• Bipolar Affective Disorder (BAD): – concordance rate for monozygotes: 43% dizygotes: 6%.
– About 50% with BAD have one parent with mood disorder
– one parent with BAD: 25% chance of developing a mood disorder
• Schizophrenia: – concordance rate for monozygotes: 50%
– If both parents have schizophrenia: 47%
• ADHD: – High heritability (65% - 80%)

Diagnostic Assessment
• Identification
• History of Presenting Illness
• Review of Systems
• Past Psychiatric History
• Developmental History
• Medical History and substance use
• Family History
• Social History – education, family and peer relationships
• Mental status examination
• Rating scales

Confidentiality
• BC Infants Act
• “capable”
• Limits to confidentiality
SOME PSYCHIATRIC
SYNDROMES

ADHD
• Inattentive type - 6 of: fails to give / sustain / avoid attention / sustained mental effort; makes careless mistakes; does not seem to listen / distracted by extraneous stimuli; does not follow through on instructions; difficulty organizing task and activities; loses things necessary for tasks or activities; forgetful in daily activities
• Hyperactivity/impulsivity type - 6 of: Fidgets, squirms in seat; Leaves seat; Runs / climbs about excessively; Difficulty playing quietly; “on the go” or “driven by a motor”; Talks excessively; Blurts out answers; Difficulty awaiting turn; Interrupts or intrudes
• Other criteria
– Symptoms for at least 6 months, causing impairment before age 12 years
– Clinically significant impairment from symptoms present in two or more setting
– Does not occur exclusively during the course of another mental disorder
• 50-80% co-morbid for another disorder
• 10-50% co-morbid for learning disorder
• Over 50% co-morbid for a disruptive behaviour disorder
• 10-30% co-morbid for major depression or dysthymic disorder
• 10-35% co-morbid for anxiety disorder
Turgay 2005
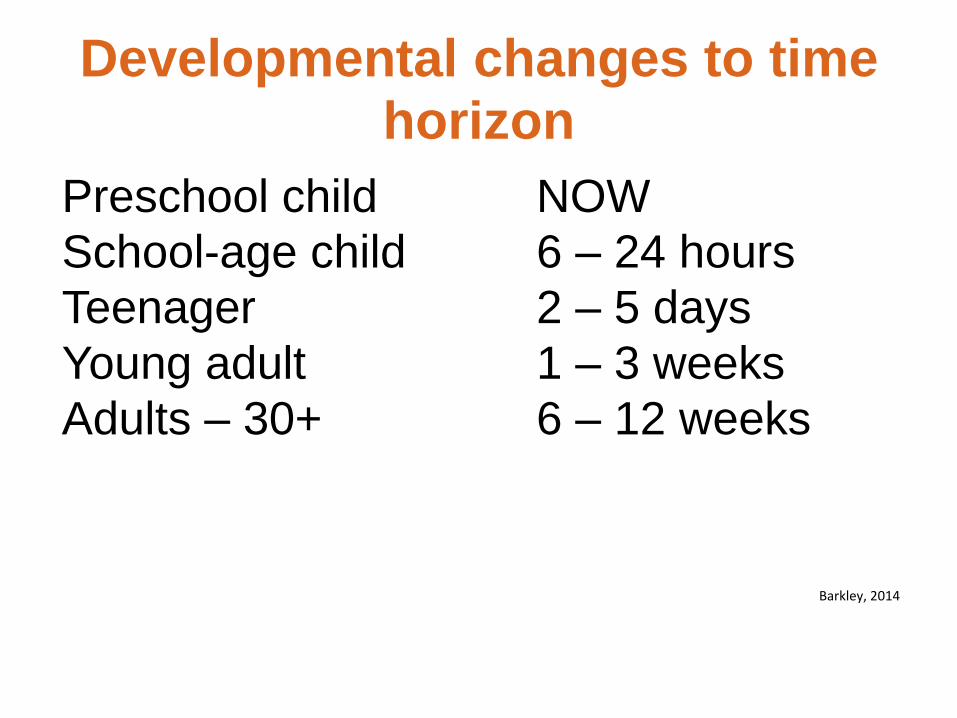
Developmental changes to time
horizon
Preschool child NOW
School-age child 6 – 24 hours
Teenager 2 – 5 days
Young adult 1 – 3 weeks
Adults – 30+ 6 – 12 weeks
With ADHD, development of executive functioning approximately 30% delayed
Barkley, 2014

Not likely ADHD if…
Symptoms in only one setting
Not functionally impairing
ADHD type symptoms may secondary to:
Post Traumatic Stress Disorder (PTSD) - consider PTSD as a diagnostic possibility in youth who exhibit ADHD symptoms for whom a significant traumatic event has recently occurred
Depression
Anxiety
Learning disorders

OPPOSITIONAL DEFIANT DISORDER
• negativistic and defiant behavior lasting at least 6 months, with at least four of:
• Often loses temper / argues with adults
• often actively defies / refuses to comply with adults' requests or rules; often deliberately annoys people
• blames others for his or her mistakes or misbehavior
• often touchy or easily annoyed by others
• often angry and resentful; spiteful or vindictive
• Consider a criterion met only if the behavior occurs more frequently than is typically observed in individuals of comparable age and developmental level.
• The disturbance in behavior causes clinically significant impairment in social, academic, or occupational functioning.
OPPOSITIONAL DEFIANT DISORDER
• Developmental theory: ODD is a result of incomplete development. For some reason, ODD children never complete the developmental tasks that normal children master during the toddler years. They get stuck in the 2-3 year old defiant stage and never really grow out of it.
• Medically, the most important consideration is to treat other disorders that come along with ODD.
• Parent training is still the most effective treatment for ODD.

AUTISM SPECTRUM DISORDER
• Social communication and social interaction deficits, such as social-emotional reciprocity
• Restricted, repetitive patterns of behaviour, interests, or activities, such as stereotypies

LEARNING DISORDERS
• the result of neurodevelopmental factors which may affect the acquisition, organization, retention, understanding or use of verbal and nonverbal information
• result from impairments in one or more processes related to perceiving, thinking, remembering or learning including: – language processing
– phonological processing
– visual spatial processing
– processing speed, memory, attention and executive functions such as planning and decision making that create a discontinuity between one’s ability & performance.
ATTACHMENT DISORDER - SYMPTOMS
• Intense control battles, defiance and anger
• Resists affection on parental terms
• May show no outward remorse
• Manipulative - superficially charming and engaging
• Indiscriminately affectionate with strangers, poor peer relationships
• Steals, lies about the obvious, destructive to property, self and/or others
• Lack of impulse control, hypervigilant/hyperactive
• Learning lags/delays, speech and language problems
• Inappropriately demanding and/or clingy
• Very concerned about tiny hurts but brushes off big hurts
• The child was neglected and/or abused
ANXIETY
• Subtypes: generalized anxiety, separation anxiety, specific phobia, obsessive-compulsive disorder, social phobia
• Excessive worrying that interferes with functioning
• Associated physical symptoms: irritability, poor sleep, impaired concentration, muscle tension, headaches, stomachaches

POST TRAUMATIC STRESS DISORDER
• a condition characterized by intense fear, helplessness, or horror (or disorganized or agitated behavior in children) resulting from the exposure to extreme trauma
• characteristic symptoms include persistent re-experiencing of the traumatic event, persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness, and persistent symptoms of increased autonomic arousal
• The full symptom picture must be present for more than 1 month, and the disturbance must cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
DEPRESSION
• 5 / 9 symptoms:
• At least one of: depressed mood or anhedonia
• Change in: – Appetite
– Sleep
– Energy
– Concentration
• Feelings of guilt
• Psychomotor agitation or retardation
• Suicidal ideation
• At least 2 weeks duration
• In children, may have irritable (as opposed to depressed) mood
BIPOLAR DISORDER
• What are “mood swings”?
• Classic manic symptoms:
– Euphoria / Grandiosity
– Reduced NEED for sleep
– Flight of ideas / pressured speech
– Sexualized behaviour
• Other (non-specific) symptoms:
– Distractibility, impulsivity, excessive activity

SCHIZOPHRENIA
• a serious disturbance in an individual’s reality testing as reflected by specific pathological signs such as thought disturbance, hallucinations, or delusions
• psychosis is not pathognomonic for schizophrenia
• developmentally or culturally appropriate beliefs by themselves do not suggest psychosis
• Transient hallucinations particularly at times of stress and anxiety; often visual and tactile and often at night; prognostically relatively benign
• May be associated with prodrome of worsened hygiene, poor sleep, negative symptoms, withdrawal, odd behaviours, irritability

Personality Disorder
• “Personality” - the enduring behavioral and mental traits that distinguish human beings
• Personality disorders - experiences and behaviors that differ from societal norms and expectations, with difficulties in cognition, emotiveness, interpersonal functioning or control of impulses
• personality disorders are inflexible and pervasive across many situations
• Functional impairment: personal and social disruption; maladaptive coping skills
• Behaviors are ongoing since early adolescence and the beginning of adulthood and, in some instances, childhood

ADHD vs Bipolar Disorder
• Family history of ADHD
• Unlikely elevated mood and grandiosity
• Stimulant response
• Earlier onset
• Rage episode ends to baseline
• Accident prone
• No psychosis
• Family history of bipolar disorder
• Elevated mood, grandiosity, psychosis
• High dose stimulants; side effects
• Later onset
• Rage episode ends with depression
Jain 2005

ADHD (inattentive) vs GAD
• Loss of attention –
scattered
• Motor restlessness
• Family history of
ADHD
• Forgetfulness
• Stimulants have some
benefit at low doses
• Intense sense of
surroundings
• Nervous tension
• Family history of
anxiety-depression
• Hypervigilant
• Stimulants may
aggravate symptoms
Jain 2005

Mood vs personality disorder
• Change from baseline
• episodic
• Neurovegetative symptoms
• Not necessarily related to any environmental stressors
• Family history of mood disorder
• pervasive pattern of instability of interpersonal relationship, self-image, and affects
• Longstanding
• May not have any neurovegetative symptoms
• Frequently, history of trauma
• Reactive to environmental stressors
Treatment options
• Medication
• Non-medication – Counselling options (for parents / child / family)
– Parent / staff training
– Environmental stability
• Both medication and non-medication treatments have been found to impact on brain functioning

Treatment questions to consider
– Is there a psychiatric diagnosis? What are the target symptoms?
– How severe are the symptoms?
– What is the impact of these symptoms on functioning?
– What is the goal of treatment, either medication or psychotherapy?
– What are the potential benefits versus risks of treatment?
– What would be the risks of non-treatment?

Developmental
psychopharmacology • The nervous system shows different responses
depending on age and level of plasticity
• Medications which work in typical adults may not work in children or those with developmental disability, and vice versa
• Some medications are potentially more toxic and may have more side effects in those with vulnerable brains compared to adults
• Global developmental disturbances may alter response to pharmacotherapy
• Balance between treating current functional impairment versus medication side effects
Medication classes
– Medications for ADHD (stimulants, non-
stimulants)
– Serotonin specific reuptake inhibitors for
depression and anxiety
– Antipsychotic medications for psychosis,
mania, adjunctive treatment for depression
and anxiety, behavioural disturbances
– Mood stabilizers for bipolar disorder,
aggression

What medication to choose?
– Psychiatric diagnosis and comorbidity
– Target symptoms
– Potential quickness of response; some
medications can work more immediately,
others take at least 4 – 6 weeks to start to
work
– Side effect profile of the medications
– Personal or family history of response / side
effects to medication

Dosing considerations
– Weight
– Potential for fast / slow metabolism
– Hepatic impairment
– Renal impairment
– DRUG INTERACTIONS INCLUDING HERBAL OR OVER THE COUNTER MEDICATIONS
– There are dosing guidelines for children for many medications; generally “start low go slow”

Is the medication working?
– Very important to keep on evaluating whether
medication is helpful or not
– Medication needs to be at a high enough
dose for a long enough time for a proper
evaluation
– Mood / behaviour / side effect charting in
multiple settings (home, school)
– Also need to chart environmental / other
stressors
PSYCHOTHERAPY
– An important part of any treatment regime
– Psychotherapy can act as a “medication”
– Psychotherapy can reduce the amount of
medication required
– Psychotherapy takes more time than
medication to see results, but tends to have
longer-lasting effects

CASE HISTORY 1 - CONCLUSION
• It was not until she finally moved into a new pri-care home that Bev was able to verbalize that her previous caregiver and she had not gotten along. Bev did not require any medication at her new home, and follow-up visits with Bev proved that she got along well with her new pri-care giver. Of note, there were no complaints of irritability, difficulty sleeping, or aggression in the home.
CASE HISTORY 2 - CONCLUSION
Elaine had no behavioural or psychiatric difficulties until age 12. There had been no traumatic childhood events.
After the depressive symptoms were identified, the “conduct disorder” symptoms were found to occur during significant and unusual elevations of mood.
Elaine was subsequently diagnosed with bipolar disorder.
CASE HISTORY 3 - CONCLUSION
Information from John’s parents was inconsistent, understandably because of how differently they interacted with him. His father had learned to provide him with a lot of support, without noticing it as such. At school, staff indicated that there were no behavioural difficulties as occurred with his mother. He needed reminders, continual redirection, and learning difficulties were related to inattention.

CASE HISTORY 4 - CONCLUSION
• With counselling support and Sertraline /
Seroquel combination, Angie’s anxiety and
depression improved. Underlying ADHD
symptoms were then identified. She was
prescribed Vyvanse and was weaned off
all other medications (at her request).
Anxiety symptoms subsequently recurred,
despite ongoing improvement in academic
achievement.

RESOURCES FOR FAMILIES
• American Academy of Child and Adolescent psychiatry (www.aacap.org)
• National Institute of Mental Health (http://www.nimh.nih.gov/health)
• Canadian Attention Deficit Hyperactivity Disorder Resource Alliance (www.caddra.ca) and Children and adults with Attention Deficit / Hyperactivity Disorder (www.chadd.org)
• Children and adolescent bipolar foundation (www.bpkids.org)
• Children’s Disabilities Information (www.childrensdisabilities.info)

50
Anxiety BC
www.anxietybc.com
Teen Mental Health
www.teenmentalhealth.org
Mind Check
www.mindcheck.ca
Kelty
www.keltymentalhealth.ca
Suggested Websites
51
www.mindcheck.ca
51
mindcheck.ca
Mood
& Anxiety
Stress
Alcohol &
Other Drugs
Reality
Check
Body
Image
& Eating
Speak
Up
Why do I need to get
HIGH so often????
Why did I get so
WASTED again????
Why am I so
STRESSED
OUT???
Why can’t I look
like that ???
Why do I FEEL
so SAD?? Things don’t
seem right
Why do I WORRY
so much??? Why do I feel
ANXIOUS around people???
Distress phone Service 24-hour, 7/days (Crisis centre) /week 1-800-SUICIDE: 1-800-784-2433
ONLINE CHATS: www.youthinbc.com : noon-1am daily www.crisiscentrachat.ca : noon to 1am daily
Kids help phone line (age 20 and under): 24-hour toll free 1-800-668-6868
Mental Health Support: 310-6789 (no area code needed)
IN CRISIS?
References
• Becoming Attached (Karen, 1994)
• Child Development (Berk, 2005)
• Clinical Child Psychiatry (Klykylo, Kay, and Rube, 1998)
• Clinical handbook of psychotropic drugs for children and adolescents (Bezchlibnyk-Buter and Virani, 2004)
• American Academy of Child and Adolescent Psychiatry (www.aacap.org)
• DSM - V
• Encounters with Children (Dixon and Stein, 2006)
• Practical Child and Adolescent Psychopharmacology (Kutcher, 2002)