mymanagement of hypertension.pptx
TRANSCRIPT

UPDATED IN MANAGEMENT OF HYPERTENSION
Leonardo Paskah S, MDA&E Department of SHKJ
References The 7th Joint National Committee (JNC 7th) on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
Guidelines for management of hypertension: report of the fourth Working Party of the British Hypertension Society IV (BHS) 2004. B Williams et al: J Hum Hyp (2004); 18: 139-185.
NICE Hypertension Guideline, 2006. www.nice.org.uk/CG034NICEguideline
Guideline of Hypertension-European Society of Cardiology (ESC) 2008
Canadian Hypertension Education Program (CHEP) Recommendation 2009

Partners in Healthcare Education, LLC 2009
Hypertension and Dyslipidemia Contribute
to Atherogenesis
EndothelialDysfunction
CVD
Hypertension Dyslipidemia
Atherosclerosis
Smooth MuscleCell Contraction
Impaired Bioavailability of Nitric Oxide
Impaired Vasodilation

Impact of Hypertension 50 million
individuals in the United States have hypertension1
277,000 deaths annually in US due to hypertension2
1American Association of Clinical Endocrinologists Medical Guidelines For Clinical Practice for the Diagnosis and Treatment of Hypertension. Endocrine Practice, Vol 12 No. 2 March/April 20062National Center for Health Statistics. Health, United States, 2005, with Chartbook on the Health of Americans. Hyattsville, Maryland: 2004. Available at: http://www.cdc.gov/nchs/hus.htm

Hypertension Remains One of the Most Important
Multipliers of CV RiskBP >140/90 mm Hg is associated with:
· 277,000 deaths in 2003
BP, blood pressure; CHF, congestive heart failure; MI, myocardial infarction.
Rosamond W et al. Circulation. 2007;115:1-103.
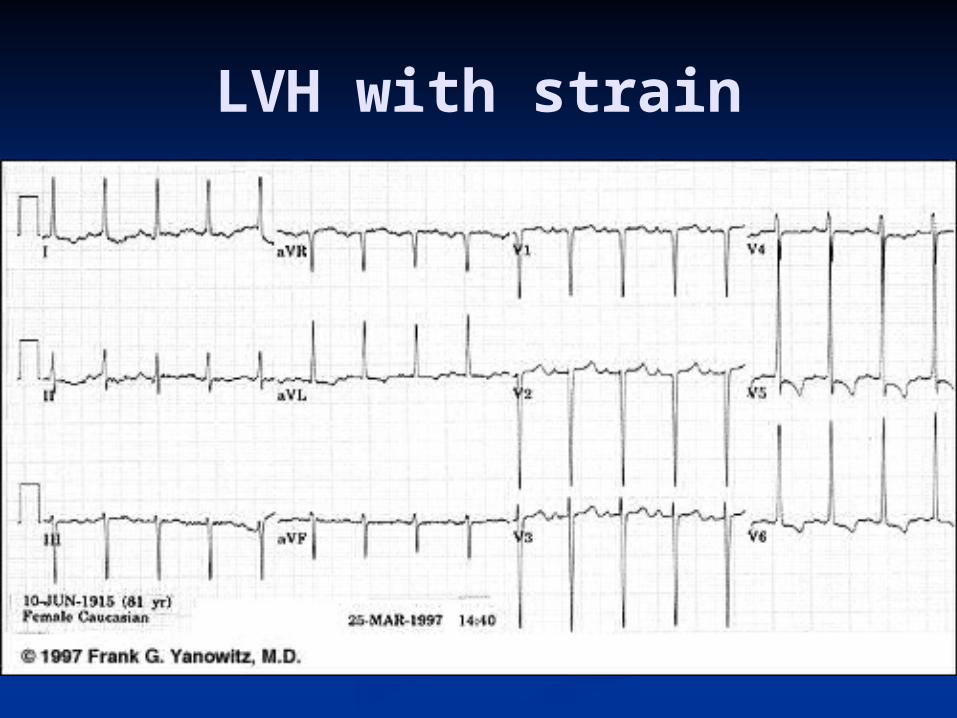
LVH with strain
Partners in Healthcare Education, LLC 2009
It is currently estimated that…
90% of normotensive 55 year olds will develop hypertension at some point in his/her lifetime
• Above 115/75 mmHg, CVD risk doubles with each BP increase of 20/10 mmHg
Partners in Healthcare Education, LLC 2009
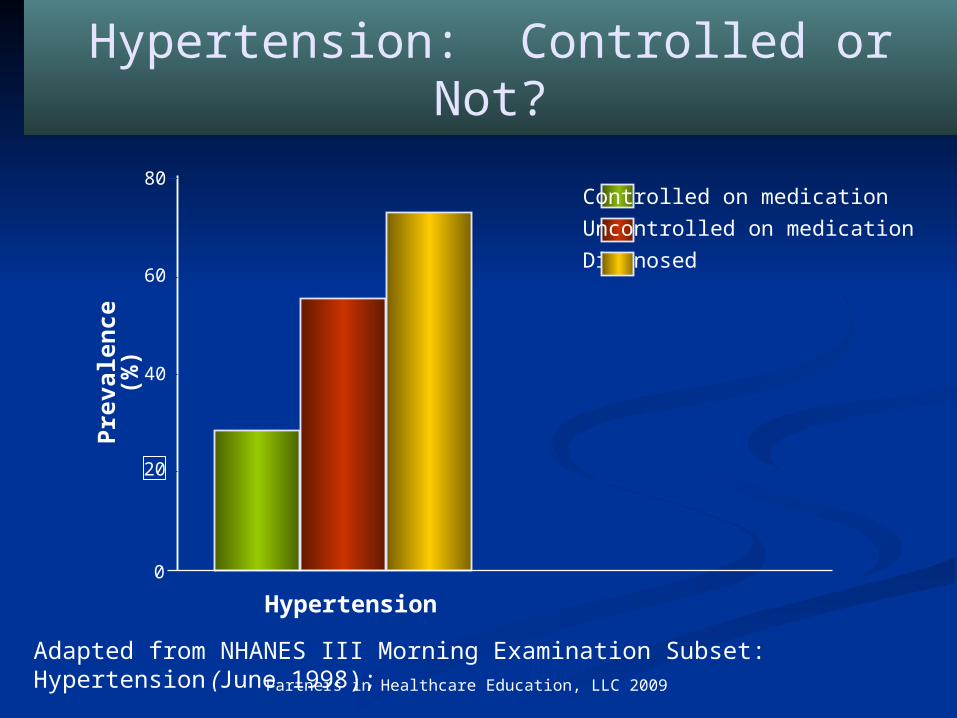
Hypertension: Controlled or Not?Pr
eval
ence
(%)
Hypertension
0
20
40
60
80Controlled on medicationUncontrolled on medicationDiagnosed
Adapted from NHANES III Morning Examination Subset: Hypertension (June 1998);
Partners in Healthcare Education, LLC 2009
Statistics of Interest
53% of patients with hypertension are being treated with medications
Of those treated, 29% have their blood pressure < 140/90
Lookinland, S. and Beckstrand, R. Evidence-Based Treatment of Hypertension: JNC7 Guidelines Provide an Updated Framework; Advance for Nurse Practitioners, Sept 2003.
So....
It is important to control blood pressure together with other CV risk factors
Strategy controlling HTN :Lifestyle modification +
pharmacotherapy
Current Guideline : the 7th JNC, BHS-NICE 2006, ESC 2007, CHEP 2009

Changes in BP Classification
Hypertension 2003;289:2560-2572.

Why Prehypertension?
Patients normotensive at age 55 have a 90% lifetime risk to develop HTN
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
Prehypertensive: 120–139 / 80–89 mmHg Require health-promoting lifestyle
modifications to prevent CVD Public health goal: Prevent
hypertension and cardiovascular disease before it happens

Blood Pressure Classification
BP Classification SBP mmHg* DBP mmHg Lifestyle Modification
Drug Therapy**
Normal <120 and <80 Encourage No
Prehypertension 120-139 or 80-89 Yes No
Stage 1 Hypertension 140-159 or 90-99 Yes Single
Agent
Stage 2 Hypertension ≥ 160 or ≥ 100 Yes Combo
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
*Treatment determined by highest BP category; **Consider treatment for compelling indications regardless of BP

BP Measurement Techniques
Method Brief Description
In-officeTwo readings, 5 minutes apart. Sitting in chair, not on exam table. Confirm elevated reading in contralateral arm.
Self-measurementProvides information on response to therapy. May help improve adherence to therapy and evaluate “white-coat” HTN.
Ambulatory BP monitoring
Indicated for evaluation of “white-coat” HTN. Can be used to confirm self-measurement when inconsistent with in-office measurement.
http://hin.nhlbi.nih.gov/nhbpep_slds/menu.htm; Accessed October 20, 2003; 8:15AM

Key Messages JNC 7 (Joint National Committee)
• Thiazide-type diuretics should be included in initial drug therapy for most
• Compelling indications for other drug classes remain in the guideline
• Most patients require two or more drugs to achieve goal BP
• If BP is >20/10 mmHg above goal, initiate therapy with two agents
http://hin.nhlbi.nih.gov/nhbpep_slds/menu.htm; Accessed October 20, 2003; 8:15AM
Key messages CHEP 2009
(Canadian Hypertension Education Program) Ensure blood pressure in diabetic patients is
below 130/80 mmHg All Canadian adults need to have blood pressure
assessed at all appropriate clinical visits Optimum management of BP requires
assessment of overall cardiovascular risk Lifestyle modifications are effective in preventing
hypertension, treating hypertension and reducing cardiovascular risk
Treat to target Combinations of therapies (both lifestyle and
drug) are generally necessary to achieve target blood pressures
Monitor patients whose blood pressure is above target regularly and increase the intensity of treatment until the targets are achieved
Focus on adherence

What’s New for 2009The Hypertensive
Diabetic Up to 80% of diabetic patients die of cardiovascular disease
Most patients with diabetes have hypertension Between 35 and 75% of diabetic complications
have been attributed to hypertension. Treatment of hypertension in patients with
diabetes reduces total mortality, myocardial infarction, stroke, retinopathy and progressive renal failure rates.
More intensive reduction in blood pressure reduces major cardiovascular events and total mortality by 25%Treating hypertension in the diabetic patient reduces death and disability
and reduces health care system costsTARGET <130 systolic and <80 mmHg diastolic
What’s New for 2009The Hypertensive
Diabetic 2/3rds of hypertensive diabetic patients have
uncontrolled hypertension (> 130/80 mmHg)
A combination of lifestyle changes and 3 or more medications are often required.
More intensive reduction in blood pressure in the hypertensive diabetic is one a few medical interventions where the cost of treatment is less than the cost of the complications prevented
Treating hypertension in the diabetic patient reduces death and disability and reduces health care system costs
TARGET <130 systolic and <80 mmHg diastolic

What’s New for 2009
Increased age on its own should not be a consideration in determining the need for antihypertensive drug therapy. Drug therapy for the elderly should be based on the same criteria as in younger adults however caution should be exercised in elderly patients who are frail or have postural hypotension.
N Engl J Med 2008;358:1887-98
What’s New for 2009
The use of combination of ACE inhibitor with an ARB should only be considered in selected and closely monitored people with advanced heart failure or proteinuric nephropathy.

Goals of Therapy To optimally reduce cardiovascular risk
reduce the blood pressure to specified targets. This usually requires two or more
drugs and lifestyle changes The systolic target is more difficult to
achieve however controlling systolic blood pressure is as important if not more important than controlling diastolic blood pressure

Blood pressure target values for treatment of hypertension
Condition Target
SBP and DBP mmHg
Isolated systolic hypertension <140
Systolic/Diastolic Hypertension• Systolic BP • Diastolic BP
<140<90
Diabetes or Chronic Kidney Disease• Systolic • Diastolic
<130<80
“The Goal is to get to Goal”

Treatment Overview
• Lifestyle modification
• Pharmacologic treatment• Initial therapy• Combination therapy
• Follow-up and monitoring

LIFE STYLE MODIFICATION

- Reduce sodium intake to less than 2300 mg / day (=5.8 g NaCl) - Healthy diet: high in fresh fruits, vegetables, low fat dairy products, dietary
and soluble fiber, whole grains and protein from plant sources, low in saturated fat, cholesterol and sodium
- Regular physical activity: accumulation of 30-60 minutes of moderate intensity cardiorespiratory activity (e.g. a brisk walk) 4-7 days/week in addition to routine activities of daily living
- Low risk alcohol consumption (≤2 standard drinks/day and less than 14/week for men and less than 9/week for women)
- Maintenance of ideal body weight (BMI 18.5-24.9 kg/m2)
- Waist Circumference Men Women- Europid, Sub-Saharan African, Middle Eastern <94 cm <80 cm- South Asian, Chinese <90 cm <80 cm
- Smoke free environment- Stress management
Lifestyle Recommendations for Prevention and Treatment of
Hypertension
Dietary Approaches to Stop Hypertension
Lowers systolic BP in normotensive
patients by an average of 3.5 mm Hg
In hypertensive patients by 11.4 mm Hg
Copies available from NHLBI websitehttp://www.nhlbi.nih.gov/health/public/heart/hbp/dash/

DASH Eating Plan
Low in saturated fat, cholesterol, and total fat
Emphasizes fruits, vegetables, and low fat diary products
Reduced red meat, sweets, and sugar containing beverages
Rich in magnesium, potassium, calcium, protein, and fiber
3 -1.5 g sodium per day Can reduce BP in 2 weeks
Sacks FM. NEJM. 2001; 344:3-10.

Lifestyle Modification: The Target
Intervention Target
Reduce foods with added sodium
< 2300 mg /day
Weight loss BMI <25 kg/m2
Alcohol restriction < 2 drinks/day
Physical activity 30-60 minutes 4-7 days/week
Dietary patterns DASH diet
Smoking cessation Smoke free environment
Waist Circumference- Europid- South Asian, Chinese
Men Women <94 cm <80 cm <90 cm <80 cm

Impact of Lifestyle Therapies on Blood Pressure in Hypertensive
Adults
Intervention Intervention SBP/DBP
Reduce foods with added sodium
-1800 mg/day sodium
Hypertensive-5.1 / -2.7
Weight loss -1 kg -1.1 / -0.9
Alcohol intake -3.6 drinks/day -3.9 / -2.4
Aerobic exercise 120-150 min/week -4.9 / -3.7
Dietary patternsDASH diet
HypertensiveNormotensive
-11.4 / -5.5-3.6 / -1.8
Applying the 2005 Canadian Hypertension Education Program recommendations: 3. Lifestyle modifications to prevent and treat hypertension Padwal R. et al. CMAJ ・ SEPT. 27, 2005; 173 (7) 749-751

PHARMACOTHERAPY INTERVENTION
Indications for Pharmacotherapy• In low risk patients with stage 1 hypertension
(140-159/90-99 mmHg) lifestyle modification can be the sole therapy.
• Over 90% of Canadians with hypertension have other risk factors and pharmacotherapy should be considered in these patients if blood pressure remains equal to or above 140/90 mmHg with lifestyle modification.
• Patients with target organ damage (e.g. left ventricular hypertrophy) are recommended to be treated with pharmacotherapy if blood pressure is equal to or above 140/90 mmHg
• Patients with diabetes or chronic kidney disease should be considered for pharmacotherapy if the blood pressure is equal or over 130/80 mmHg

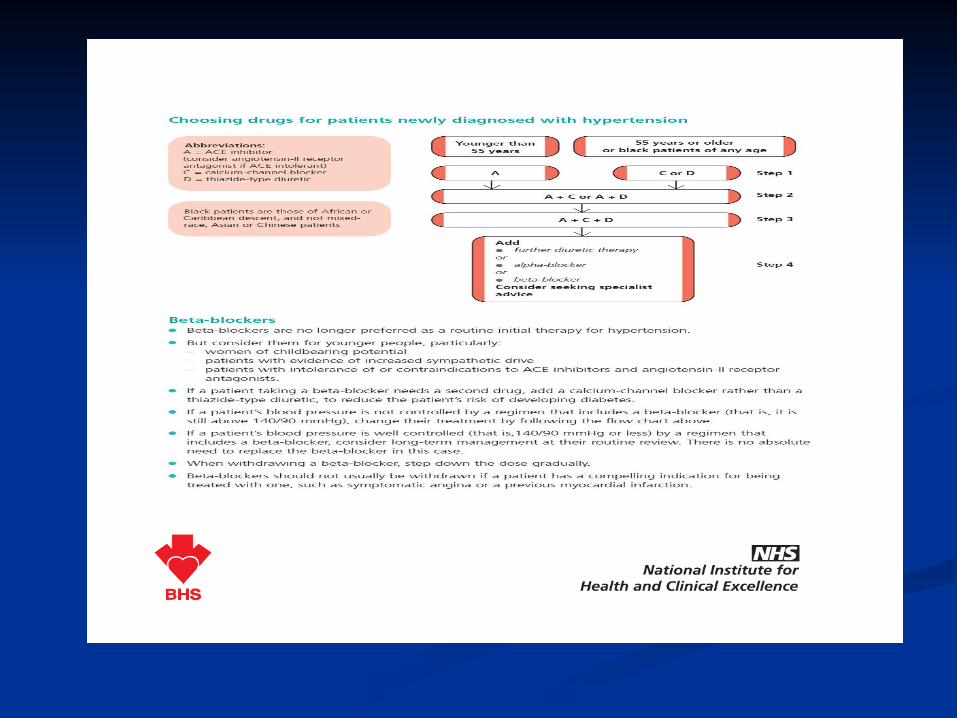
What to choose first?
Initial antihypertensive therapy without compelling indications• JNC 6: Diuretic or a beta-blocker
• JNC 7: Thiazide-type diuretics • Most outcome trials base
antihypertensive therapy on thiazides
Antihypertensive and Lipid-Lowering to Prevent Heart Attack Trail (ALLHAT)
ALLHAT. JAMA. 2002 288(23):2981-97
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314

Considerations Regarding the Choice of First-Line Therapy
Use caution in initiating therapy with 2 drugs in whom adverse events are more likely (e.g. frail elderly, those with postural hypotension or who are dehydrated).
ACE inhibitors, renin inhibitors and ARBs are contraindicated in pregnancy and caution is required in prescribing to women of child bearing potential.
Beta adrenergic blockers are not recommended for patients age 60 and over without another compelling indication.
The use of combination of ACE inhibitor with a ARB should only be considered in selected and closely monitored people with advanced heart failure or proteinuric nephropathy.
ACE-I are not recommended (as monotherapy) for black patients without another compelling indication.

Algorithm for Treatment of Hypertension
Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease)
Initial Drug Choices
Drug(s) for the compelling indications
Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB)
as needed.
With Compelling Indications
Lifestyle Modifications
Stage 2 HTN (SBP >160 or DBP >100 mmHg)
2-drug combination for most (usually thiazide-type diuretic and
ACEI, or ARB, or BB, or CCB)
Stage 1 HTN (SBP 140–159 or DBP 90–99 mmHg)
Thiazide-type diuretics for most. May consider ACEI, ARB, BB,
CCB, or combination.
Without Compelling Indications
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
Not at Goal Blood Pressure
Optimize dosages or add additional drugs until goal blood pressure is achieved.
Consider consultation with hypertension specialist.

Treatment of Systolic-Diastolic Hypertension without Other
Compelling Indications(CHEP 2009)
CONSIDER
• Nonadherence• Secondary HTN• Interfering drugs or
lifestyle• White coat effect
Dual Combination
Triple or Quadruple Therapy
Lifestyle modification
Thiazidediuretic ACEI Long-acting
CCBBeta-
blocker*
TARGET <140/90 mmHg
ARB
*Not indicated as first line therapy over 60 y
Initial therapy
A combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmHg systolic or >10 mmHg diastolic above target

Compelling Indications for Individual Drug Classes
Compelling Indication
Initial Therapy Options
Clinical Trial Basis
Heart failure THIAZ, BB, ACEI, ARB, ARA
ACC/AHA Heart Failure Guideline, MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, ValHEFT, RALES
Postmyocardialinfarction
BB, ACEI ACC/AHA Post-MI Guideline, BHAT, SAVE, Capricorn, EPHESUS
Angina BB, long acting CCB
ESC, CHAP 2009

Compelling Indications for Individual Drug Classes
Compelling Indication
Initial Therapy Options
Clinical Trial Basis
Diabetes ACEI, ARB, CCB, THIAZ, BB,
NKF-ADA Guideline, UKPDS, ALLHAT
Chronic kidney disease (non-diabetogenic)
ACEI, ARB;THIAZ/FURO
NKF Guideline, Captopril Trial, RENAAL, IDNT, REIN, AASK
Recurrent stroke prevention, CVD, TIA
THIAZ, ACEI PROGRESS, CHEP
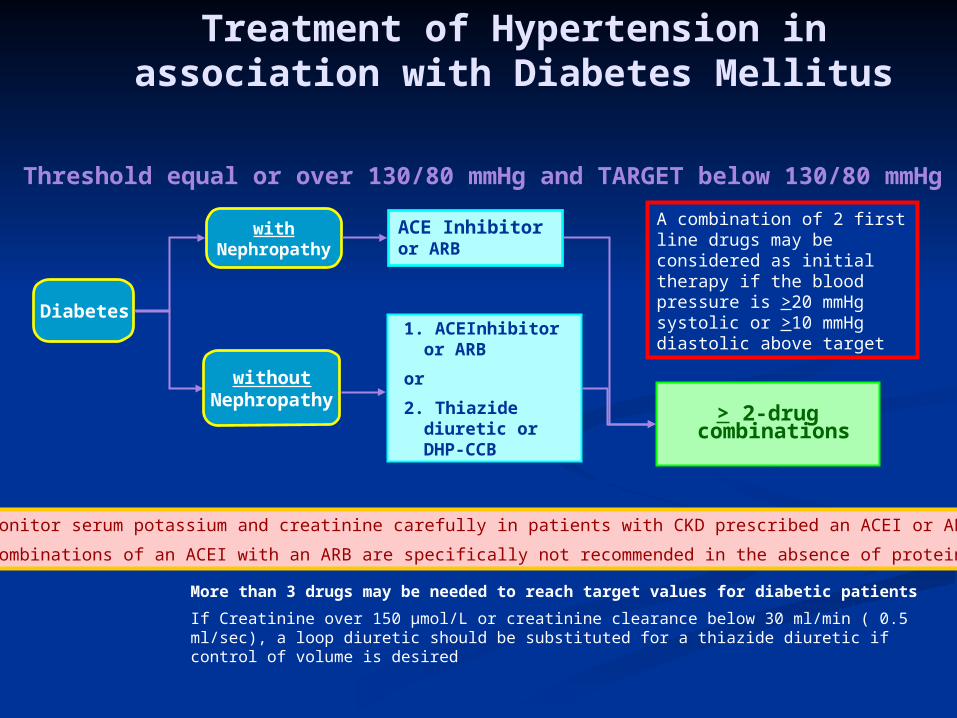
Treatment of Hypertension in association with Diabetes Mellitus
More than 3 drugs may be needed to reach target values for diabetic patients
If Creatinine over 150 µmol/L or creatinine clearance below 30 ml/min ( 0.5 ml/sec), a loop diuretic should be substituted for a thiazide diuretic if control of volume is desired
Threshold equal or over 130/80 mmHg and TARGET below 130/80 mmHg
Diabetes
withNephropathy
> 2-drug combinations
ACE Inhibitoror ARB
withoutNephropathy
1. ACEInhibitor or ARB
or
2. Thiazide diuretic or DHP-CCB
Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB
Combinations of an ACEI with an ARB are specifically not recommended in the absence of proteinuria
A combination of 2 first line drugs may be considered as initial therapy if the blood pressure is >20 mmHg systolic or >10 mmHg diastolic above target

Treatment of hypertension in renovascular disease
Close follow-up and intervention (angioplasty and stenting or surgery) should be considered for patients with: uncontrolled hypertension despite therapy with three or more drugs, or deteriorating renal function, or bilateral atherosclerotic renal artery lesions (or tight atherosclerotic stenosis in a single kidney), or recurrent episodes of flash pulmonary edema.
Does not imply specific treatment choice
Renovascular disease
Caution in the use of ACEI or ARB in bilateral renal artery stenosis or unilateral disease with solitary kidney
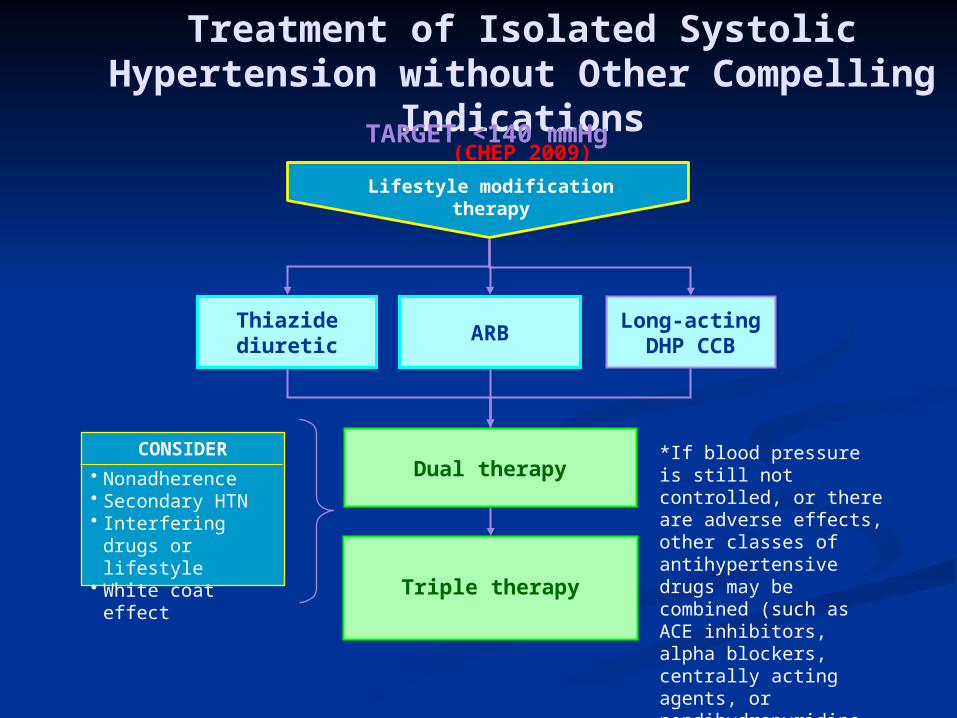
Treatment of Isolated Systolic Hypertension without Other Compelling
Indications(CHEP 2009)
CONSIDER
• Nonadherence• Secondary HTN• Interfering drugs or
lifestyle• White coat effect
Thiazide diuretic
Long-actingDHP CCB
Dual therapy
Triple therapy
Lifestyle modificationtherapy
ARB
TARGET <140 mmHg
*If blood pressure is still not controlled, or there are adverse effects, other classes of antihypertensive drugs may be combined (such as ACE inhibitors, alpha blockers, centrally acting agents, or nondihydropyridine calcium channel blocker).

Is it appropriate to start 2 agents?
In ALLHAT, 60% of patients achieved SBP control
Inadequate titration of drug regimens is a primary reason patients do not reach BP goal
The Rule of 10 (for Systolic) & Rule of 5 (for diastolic).
Patients and providers should be educated that more than one antihypertensive is the norm not the exception
Indication depend on:- stage of hypertension- target point- total cardiovascular risks
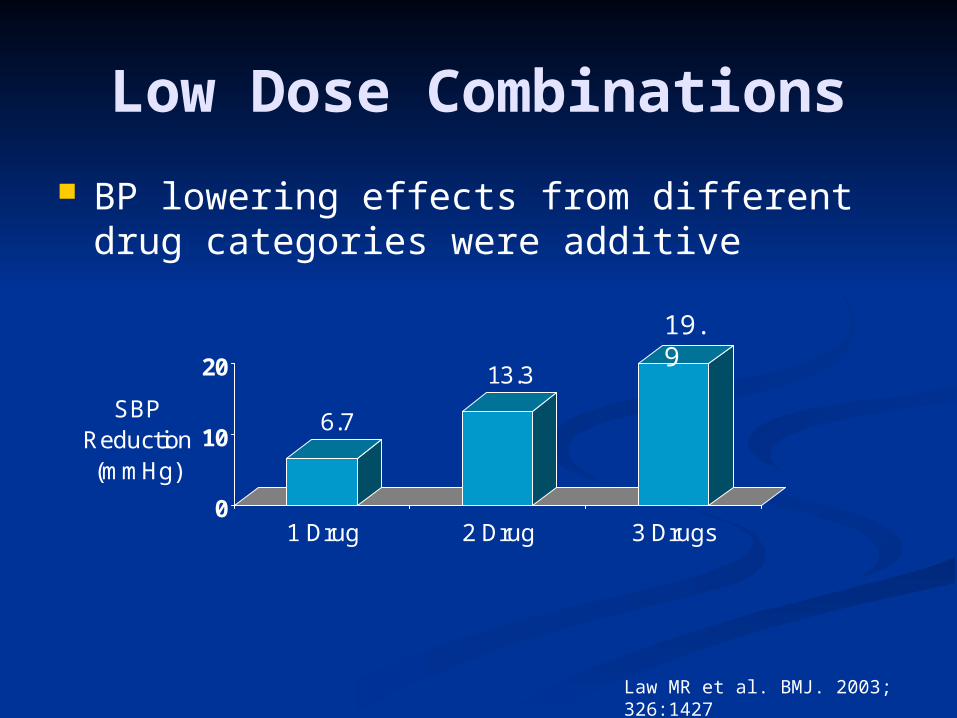
Low Dose Combinations
BP lowering effects from different drug categories were additive
6.7
13.3
0
10
20
SBP Reduction (mmHg)
1 Drug 2 Drug 3 Drugs
Law MR et al. BMJ. 2003; 326:1427
19.9

Low Dose Combinations
Adverse effects in all drug categories, except ACEI, were dose related
Prevalence of adverse effects in combination was less than additive
Conclusion:Utilization of low dose combination therapy can effectively reduce blood pressure while limiting the incidence of side effects
Law MR et al. BMJ. 2003; 326:1427

Rational Combination Therapy:
Chinese Menu Approach

Algebra of Blood Pressure
BP = Cardiac Output x SVR
CO = HR x Stroke Volume
↓
BP = HR x Stroke Volume x SVR

Heart
HR
Arteries
SVR
Veins
Stroke Volume
Physiologic Components of BP


Pharmacologic Sites of Action
ThiazidesLoopsAldosterone Ant.Nitrates
ACEIARB
Beta BlockersDiltiazemVerapamil
Via Central Mechanism:Clonidine
Dihydropyridine CCBsHydralazineMinoxidilAlpha1 Blockers
ACEIARB
HeartArteries
Veins
Short-actingnifedipine
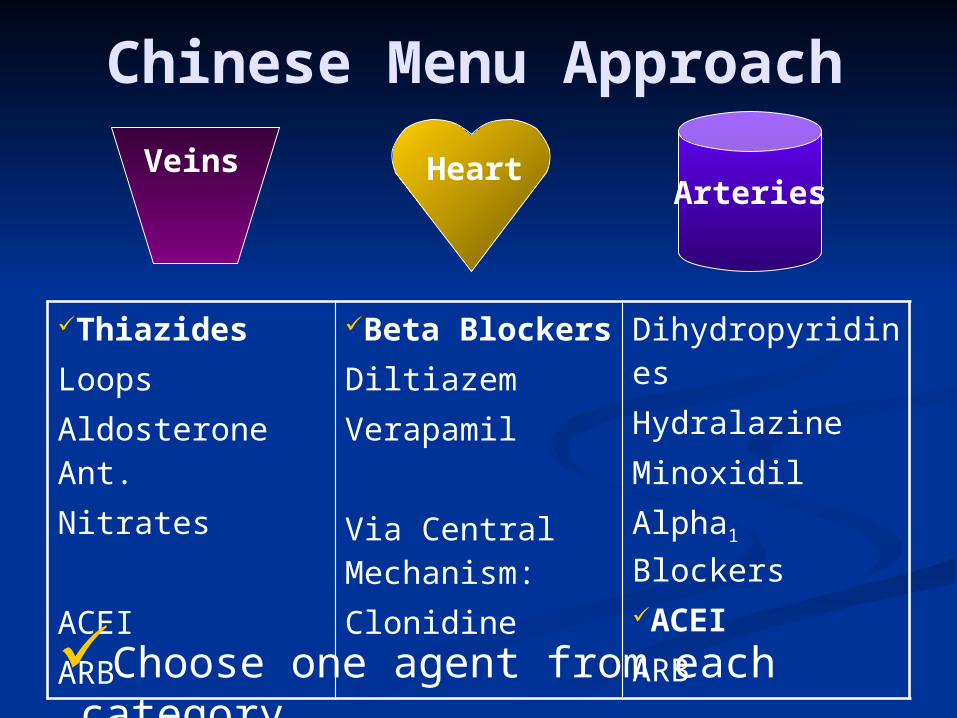
Chinese Menu Approach
ThiazidesLoopsAldosterone Ant.Nitrates
ACEIARB
Beta BlockersDiltiazemVerapamil
Via Central Mechanism:Clonidine
DihydropyridinesHydralazineMinoxidilAlpha1 BlockersACEIARB
HeartArteries
Veins
Choose one agent from each category

Caution for Drug Combinations
Two drug combinations of beta blockers, ACE inhibitors and angiotensin receptor blockers have not been proven to have additive hypotensive effects. Therefore these potential two drug combinations should not be used unless there is a compelling indication
Combinations of an ACEI with an ARB do not reduce cardiovascular events more than the ACEI alone and have more adverse effects therefore are not generally recommended
Monitor serum creatinine and potassium when combining K sparing diuretics, ACE inhibitors and/or angiotensin receptor blockers.

Caution for Drug Combinations
Caution should be exercised in combining a non dihydropyridine CCB (diltiazem, verapamil) and a beta blocker to reduce the risk of bradycardia or heart block.
If a diuretic is not used as first or second line therapy, triple dose therapy should include a diuretic, when not contraindicated.
• Global Vascular Protection for Hypertensive Patients• Statins if 3 or more additional cardiovascular
risks• Aspirin once blood pressure is controlled

Causes of Resistant Hypertension
Improper BP measurement (technical) Fail to maintain healthy lifestyle (obesity, lack of exercise,
excess sodium/alcohol intake) Medication
• Inadequate doses; loose compliance• Drug actions and interactions:
Nonsteroidal antiinflammatory drugs (NSAIDs), steroid, illicit drugs (cocaine), sympathomimetics, oral contraceptives (estrogen)
• Over-the-counter (OTC) drugs and herbal supplements Identifiable causes of HTN (secondary HTN)
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314
Identifiable Causes of Hypertension
Obstructive Sleep apnea Drug-induced or related causes Chronic kidney disease Primary aldosteronism Renovascular disease Chronic steroid therapy and Cushing’s syndrome Pheochromocytoma Coarctation of the aorta Thyroid or parathyroid disease
JNC 7 Express. JAMA. 2003 Sep 10; 290(10):1314

Drug-Induced Hypertension:
Steroids Estrogens NSAIDS Phenylpropanolam
ines (PPA) Cyclosporine/
tacrolimus Erythropoietin Sibutramine Methylphenidate Ergotamine
Ketamine Desflurane Carbamazepin
e Bromocryptine Metoclopramid
e Antidepressant
s Venlafaxine
Buspirone Herbal : Ma
Huang. Licorice

Other medications for hypertensive patients
Primary prevention
(1) Aspirin: use 75mg daily if patient is aged 50 years with blood pressure controlled to <150/90 mm Hg and either; target organ damage, diabetes mellitus, or 10 year risk of cardiovascular disease of 20% (measured by using the new Joint British Societies’ cardiovascular disease risk chart)
(2) Statin: use sufficient doses to reach targets if patient is aged up to at least 80 years, with a 10 year risk of cardiovascular disease of 20% (measured by using the new Joint British Societies’ cardiovascular disease risk chart) and with total cholesterol concentration 3.5mmol/l
(3) Vitamins—no benefit shown, do not prescribe

Vascular Protection for Hypertensive
Patients: STATINS
In addition to current Canadian recommendations on management of dyslipidemia, statins are recommended in high-risk hypertensive patients with established atherosclerotic disease or with at least 3 of the following criteria:• Male
• Age 55 or older• Smoking• Total-C/HDL-C ratio of 6
mmol/L or higher
• Family History of Premature CV disease
• LVH• ECG abnormalities• Microalbuminuria or
Proteinuria
ASCOT-LLA Lancet 2003;361:1149-58

Summary Lifestyle modifications are important for
the prevention and treatment of hypertension
The goal is to get to goal: Initial therapy after lifestyle modification has
failed Consider compelling indications Initiate low dose combination therapy if BP
>20/10 mmHg above goal Consider the physiologic site of action of
agents when choosing combination therapy Patient education and motivation are
important for adherence

References The 7th Joint National Committee (JNC 7th) on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
Guidelines for management of hypertension: report of the fourth Working Party of the British Hypertension Society IV (BHS) 2004. B Williams et al: J Hum Hyp (2004); 18: 139-185.
NICE Hypertension Guideline, 2006. www.nice.org.uk/CG034NICEguideline
Guideline of Hypertension-European Society of Cardiology (ESC) 2008
Canadian Hypertension Education Program (CHEP) Recommendation 2009