myofibroblasts in health and disease
TRANSCRIPT

MYOFIBROBLASTS IN HEALTH AND DISEASEPALLAVI D. SHIROL, DAYANAND D. SHIROL
International Journal of Oral & Maxillofacial Pathology. 2012;3(1):23-27
Dr. RUCHI SHARMA

Myofibroblasts are a unique group of smooth
muscle like fibroblasts which play a significant role
in oncogenesis, inflammation, repair,
organogenesis and fibrosis in various organs and
tissues by the secretion of inflammatory and anti-
inflammatory cytokines, both lipid and gaseous
inflammatory mediators, chemokines, growth
factors as well as extracellular matrix proteins and
proteases.
2
INTRODUCTION
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

Because of their location next to epithelial or
parenchymal cells, myofibroblasts might also be
termed ‘‘JUXTAPARENCHYMAL CELLS’’.
They are present in organs with a high remodelling
capacity such as kidneys, lungs and the periodontal
ligament or during increased remodelling, such as
in growth, development, inflammatory responses
and the contraction of healing wounds.
3
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

DEFINITION
Myofibroblasts (MFs) are specialized fibroblasts
with smooth muscle-like features characterized by
the presence of contractile apparatus.
4
Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA. Myofibroblasts and mechano-regulation of
connective tissue remodelling. Nat Rev Mol Cell Biol 2002;3:349-63.
For years it was believed that collagen is the main
element responsible for wound contraction.
This concept changed in 1950 and it was found that
fibroblasts, under certain conditions, were capable of
contraction in vitro suggesting that cells were central
to wound contraction.
5
THE PREVIOUS CONCEPT
Gabbiani G, Ryan GB, Majno G. Presence of modified fibroblasts in granulation tissue and their possible
role in wound contraction. Experientia 1971;27:549-50.
Myofibroblasts were first discovered by electron
microscopy in granulation tissue by Guilio Gabbiani
et al.
6
Gabbiani G, Ryan GB, Majno G. Presence of modified fibroblasts in granulation tissue and their possible
role in wound contraction. Experientia 1971;27:549-50.
The granulation tissue
revealed numerous
bundles and aggregates of
microfilaments similar to
smooth muscle cells and
the term MF was
proposed.
DISCOVERY

large, spindle-shaped /stellate cells
long cytoplasmic extensions
amphophilic cytoplasm
indented nucleus
conspicuous nucleoli.
7
STRUCTURE
Schurch W, Seemayer TA, Hinz B, Gabbiani G. Myofibroblast. In: Mills SE, editor. Histology for Pathologists.
Philadelphia: Lippincott-Williams and Wilkins Publishers; 2007. p. 123-164.

ULTRASTRUCTURE
irregular, stellate cellular outlines with long cytoplasmic
extensions
8
Valentich J. D., Popov V., Saada J. I., Powell D. W.(1997) Phenotypic characterization of an intestinal
subepithelial myofibroblast cell line. Am. J. Physiol. 272(Cell Physiol. 41):C1513–C1524

9
numerous and often dilated cisternae of RER
cytoplasmic actin microfilaments(Stress Fibers),
sometimes arranged in discrete
bundles beneath the plasma membrane
Valentich J. D., Popov V., Saada J. I., Powell D. W.(1997) Phenotypic characterization of an intestinal
subepithelial myofibroblast cell line. Am. J. Physiol. 272(Cell Physiol. 41):C1513–C1524

slender fusiform and smooth, contoured nucleus
nucleus of activated myofibroblasts shows multiple
indentations
10
Mills, S E. Histology for Pathologists. Lippincott Williams & Wilkins, 3rd Edition
11
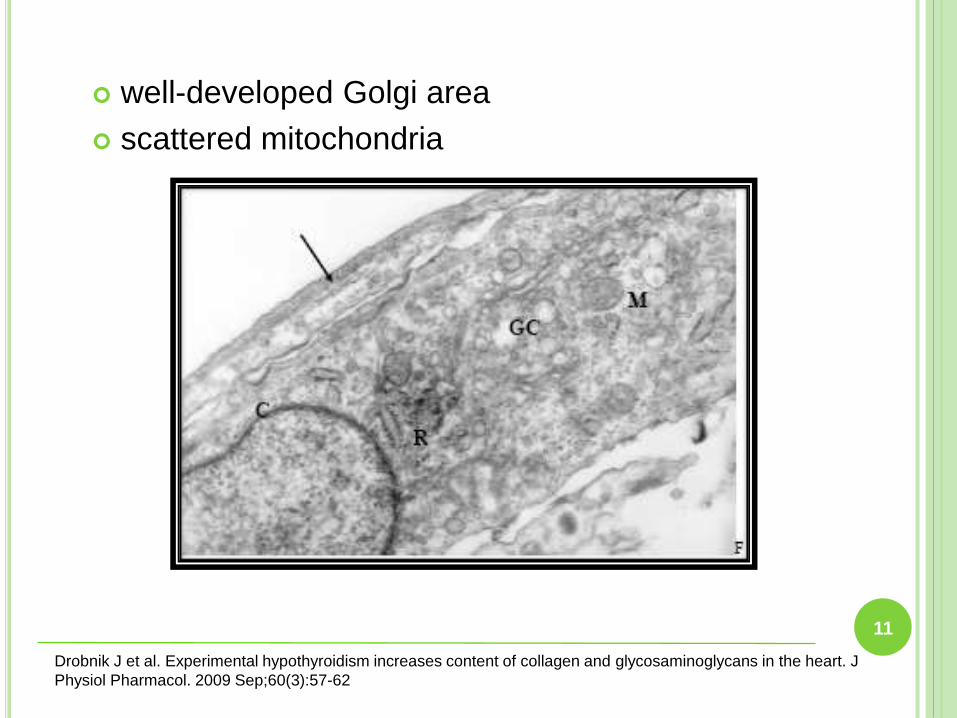
well-developed Golgi area
scattered mitochondria
Drobnik J et al. Experimental hypothyroidism increases content of collagen and glycosaminoglycans in the heart. J
Physiol Pharmacol. 2009 Sep;60(3):57-62

12
intercellular gap junctions and adherens junctions
Valentich J. D., Popov V., Saada J. I., Powell D. W.(1997) Phenotypic characterization of an intestinal
subepithelial myofibroblast cell line. Am. J. Physiol. 272(Cell Physiol. 41):C1513–C1524
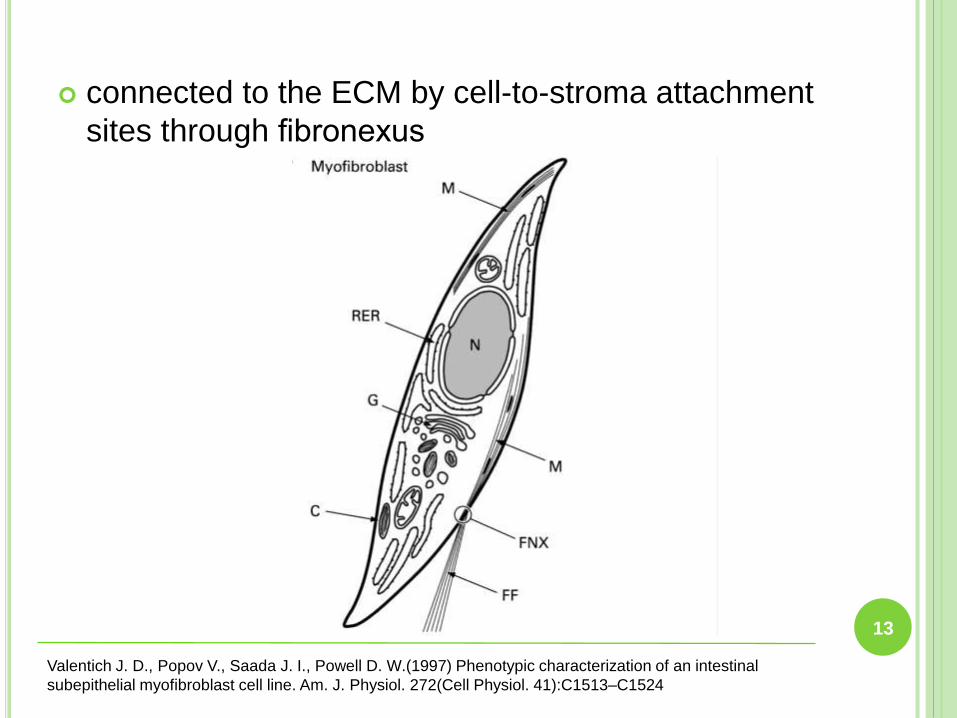
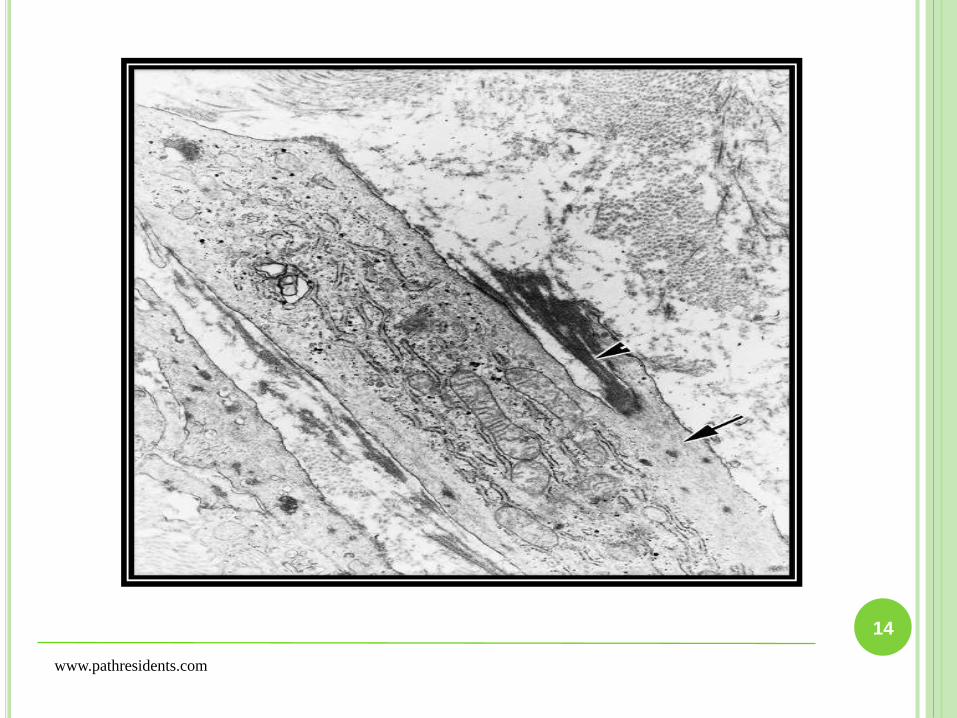
connected to the ECM by cell-to-stroma attachment
sites through fibronexus
13
Valentich J. D., Popov V., Saada J. I., Powell D. W.(1997) Phenotypic characterization of an intestinal
subepithelial myofibroblast cell line. Am. J. Physiol. 272(Cell Physiol. 41):C1513–C1524
14
www.pathresidents.com

15
Mills, S E. Histology for Pathologists. Lippincott Williams & Wilkins, 3rd Edition

CLASSIFICATION
16
Schmitt-Graff, A., A. Desmouliere, and G. Gabbiani. Heterogeneity of myofibroblast phenotypic features:
an example of fibroblastic cell plasticity. Virchows Arch. 425: 3–24, 1994.
Vimentin (V)
Vimentin and Desmin (VD)
Vimentin, α-SM actin and Desmin (VAD)
Vimentin and Myosin (VM)
Vimentin and α-SM actin (VA)

ORIGIN AND DIFFERENTIATION OF
MYOFIBROBLASTS
It is uncertain that the origin of myofibroblasts is
from progenitor stem cells (possibly
neuroepithelial stem cells), from the neural crest
or simply transdifferentiate from resident tissue
fibroblasts or from tissue smooth muscle cells.
17
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

18
Scotton C J, Chambers R C. Molecular targets in pulmonary fibrosis -The myofibroblast in focus. CHEST
132- 4 (Oct 2007).
19
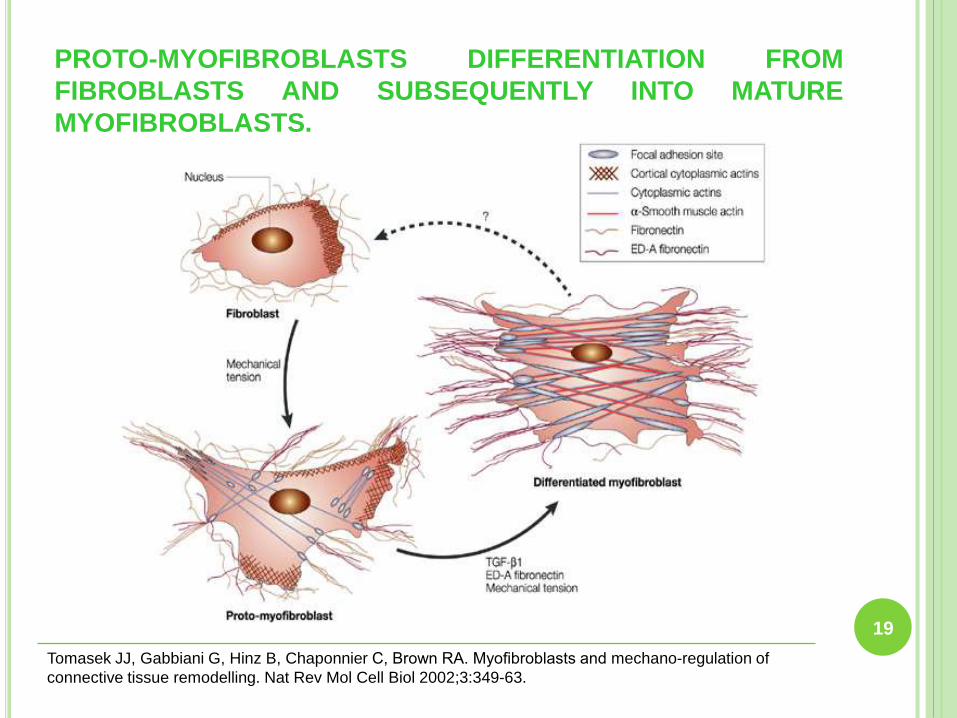
PROTO-MYOFIBROBLASTS DIFFERENTIATION FROM
FIBROBLASTS AND SUBSEQUENTLY INTO MATURE
MYOFIBROBLASTS.
Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA. Myofibroblasts and mechano-regulation of
connective tissue remodelling. Nat Rev Mol Cell Biol 2002;3:349-63.

FUNCTIONS OF MYOFIBROBLASTS
Tissue or Organ Function
EPITHELIUM
Granulation tissue Epithelial growth and
differentiation; wound repair
Pericyte Angiogenesis; regulation of local
blood flow
ORAL CAVITY
Periodontal ligament Attachment of teeth
Gingival myofibroblasts Structure of gingiva
Palatal mucosa Structure of palate
20
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

ROLE OF MYOFIBROBLASTS IN HEALTH AND
DISEASE
Through epithelial-mesenchymal interactions,
myofibroblasts are main components of
morphogenesis or organogenesis i.e. the growth
and development of the tissue or organ.
They do so by the discharge of soluble mediators of
inflammation and growth factors and expression of
their receptors and by the production of interstitial
matrix and or molecules of basement membrane.
21
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.
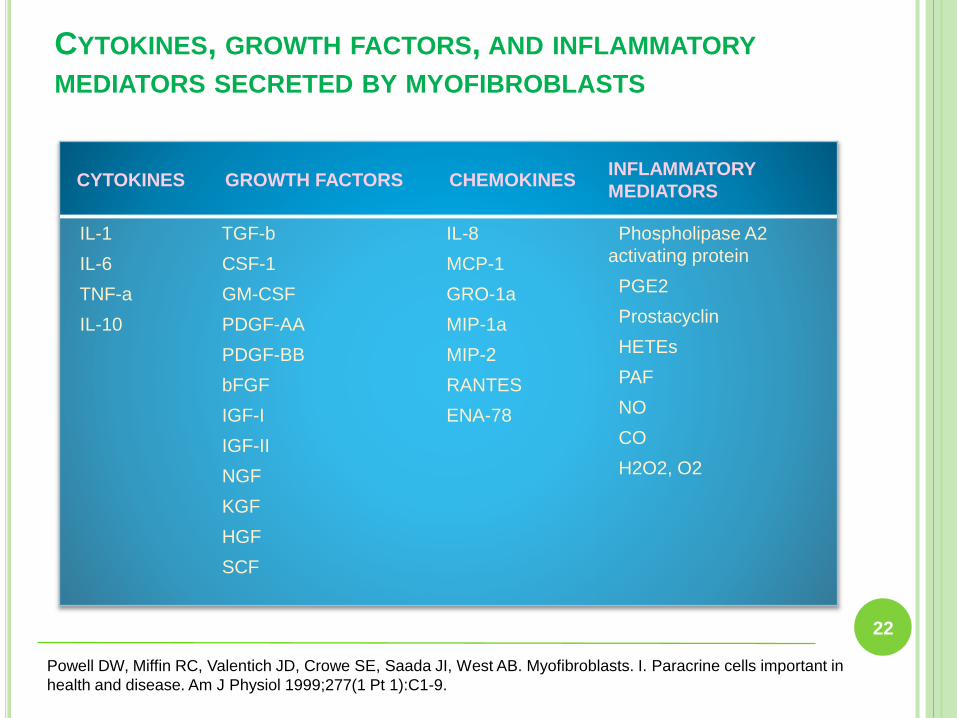
CYTOKINES, GROWTH FACTORS, AND INFLAMMATORY
MEDIATORS SECRETED BY MYOFIBROBLASTS
CYTOKINES GROWTH FACTORS CHEMOKINESINFLAMMATORY
MEDIATORS
IL-1
IL-6
TNF-a
IL-10
TGF-b
CSF-1
GM-CSF
PDGF-AA
PDGF-BB
bFGF
IGF-I
IGF-II
NGF
KGF
HGF
SCF
IL-8
MCP-1
GRO-1a
MIP-1a
MIP-2
RANTES
ENA-78
Phospholipase A2
activating protein
PGE2
Prostacyclin
HETEs
PAF
NO
CO
H2O2, O2
22
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

RECEPTORS EXPRESSED BY MYOFIBROBLASTS
CYTOKINES GROWTH
FACTORS
INFLAMMATORY
MEDIATORS
NEUROTRANSMITTERS
AND PARACRINE
MEDIATORS
ADHESION
PROTEINS
IL-1 TGF-a/EGFR Prostaglandins Acetylcholine ICAM-1
IL-1Ra TGF-b RI and RII HETEs Histamine VCAM-1
TNF-a PDGF-a Serotonin NCAM
IL-6 R PDGF-b Bradykinin MCP-1
IL-8 R c-kit Endothelin a1b1 integrin
IL-4 R aFGF and bFGF R Atrial natriuretic factor CD18
IL-11 R IGF-IR Aldosterone or ANG II
Thrombin receptor
FGFR-II
23
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.
They play a key role in the wound healing,
seemingly as an addition to their function in normal
growth and differentiation.
They are also involved in the formation and repair
of the extracellular matrix (ECM) and proliferation
and differentiation of epithelial (or parenchymal),
vascular and neurogenic elements.
24
ROLE OF MYOFIBROBLASTS IN WOUND HEALING
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

Myofibroblasts also express α and β integrins that
are part of the adhesion mechanism of
myofibroblast to matrix protein. They produce
matrix molecules such as collagen, glycosamino-
glycans, tenascin and fibronectin in the interstitial
space or basement membrane and play important
role in growth, differentiation and wound healing
which if deranged or separated can result in tissue
fibrosis.
25
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

MATRIX MOLECULES IMPORTANT IN GROWTH
DIFFERENTIATION AND WOUND REPAIR
26
•Types I–VI, XVIIICOLLAGENS
• Laminins
• Entactin/nidogen
• Fibronectin
• Tenascin
• Sparc/BM40
• Thrombospondin
GLYCOPROTEINS
• Glycosaminoglycans (GAGS)
• Hyaluronic acid (HA-type)
• Heparan sulfate (HS-type)
• Chondroitin sulfate (CS-type)
• Perlecan
PROTEOGLYCANS
• Matrix metalloproteinases (MAPs)
• Tissue inhibitor of metalloproteinases (TIMPs)
MATRIX MODIFYING PROTEINS
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, West AB. Myofibroblasts. I. Paracrine cells important in
health and disease. Am J Physiol 1999;277(1 Pt 1):C1-9.

27
PHASES OF WOUND HEALING

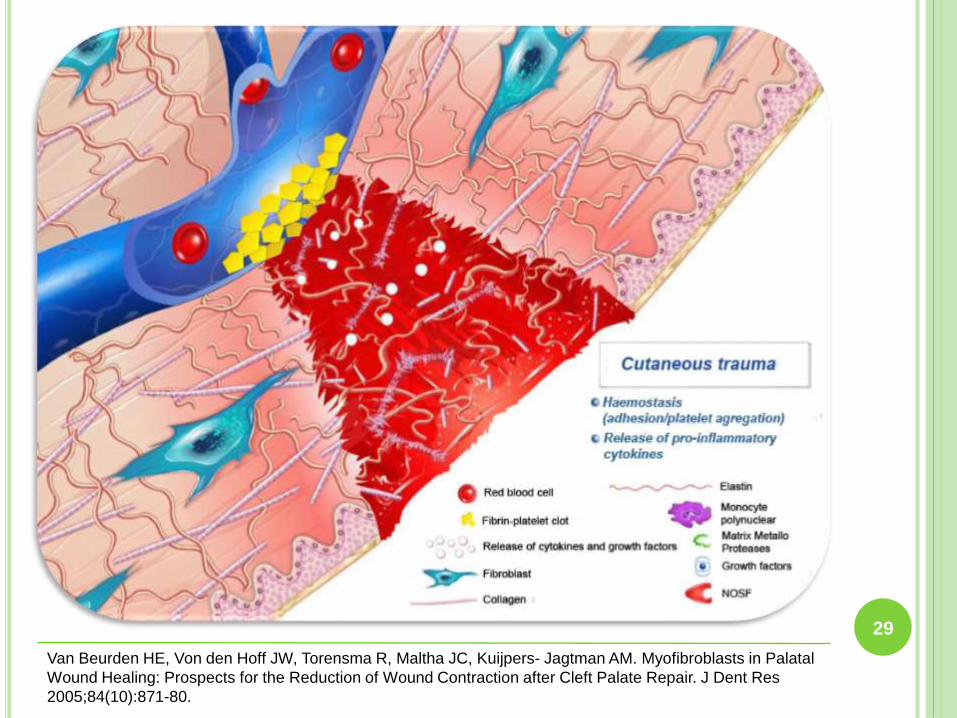
INFLAMMATORY PHASE
Following injury, vasoconstriction reduces
haemorrhage and favours platelet aggregation.
Almost simultaneously, vasodilatation enables
inflammatory cells to enter the site of injury and
clean the wound.
Neutrophils and macrophages migrate into the
wound to prevent the invasion and proliferation of
micro-organisms.
Platelet aggregation and coagulation result in the
formation of a provisional fibrin clot that covers the
wound.
28
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.
29
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

Myofibroblasts have an important position in theinflammatory response.
They produce both cytokines and chemokines and arecapable of augmenting or down regulating theinflammatory response by the secretion of these solublemediators of inflammation.
They also synthesise prostaglandins, expressing bothCOX-1 and the inducible COX-2 protein.
On activation, myofibroblasts also express molecules foradhesion like intracellular adhesion molecule-1, vascularadhesion molecule and neural cell adhesion molecule.
Thus lymphocytes, mast cells and neutrophils may dockon the myofibroblasts and participate in organisedimmunological and inflammatory reactions.
30
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.
ROLE OF MYOFIBROBLASTS IN THE INFLAMMATORY
PHASE

PROLIFERATORY PHASE
This phase starts with the migration of fibroblasts intothe wound area and their propagation.
These fibroblasts start to produce granulation tissuecomponents such as fibronectin, collagen andhyaluronic acid.
Some fibroblasts differentiate into myofibroblasts, whichare principally responsible for tissue contraction, butalso produce extracellular matrix components.
Simultaneously, re- epithelisation occurs by proliferationand migration of epithelial cells from the wound edges.
Soon after re-epithelialisation,wound contraction stopsand myofibroblasts start to disappear, probably throughapoptosis.
31
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

32
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

PHASE OF REMODELLING
The number of blood vessels decline and apoptosis
of myofibroblasts results in scar tissue with a low
cell density.
Eventually the scar contains only some fibroblasts
having well developed rough endoplasmic
reticulum.
Myofibroblasts may exist in pathological conditions,
such as hypertrophic scars.
33
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

34
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.
ROLE OF MYOFIBROBLASTS IN WOUND
CONTRACTION
Initially tractional forces are exerted by migrating
fibroblasts on the adjacent collagen matrix.
This mechanical tension stimulates fibroblasts to
differentiate into proto-myofibroblasts by the
development of stress fibres.
Fibroblasts under tension via the extracellular
matrix also express TGFβ1.
35
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.
The last maturation phase will last for several
months and will result in the final scar.
This phase begins early, during the formation of the
granulation tissue, with progressive reorganisation
of the matrix under the influence of myofibroblasts.
These cells contract their microfilament bundles
which are bonded to the extracellular matrix,
causing compaction of the collagen network and
contraction of the wound.
36
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

Proto- myofibroblasts generate contractile fibreswithout the expression of α-SM actin.Proto- myofibroblasts can also synthesise andorganise fibronectin and form small fibronexi. Proto-myofibroblasts can differentiate into maturemyofibroblasts in response to specific factors likeTGβ1, ED-A fibronectin (ED-A FN) and mechanicaltension.
Mature myofibroblasts express α- SM actin in stressfibers and form large fibronexi.
Once the wound is repaired, mature myofibroblastsdisappear through apoptosis or by dedifferentiation.
37
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC, Kuijpers- Jagtman AM. Myofibroblasts in Palatal
Wound Healing: Prospects for the Reduction of Wound Contraction after Cleft Palate Repair. J Dent Res
2005;84(10):871-80.

MYOFIBROBLASTS IN PATHOLOGIC TISSUES
• GIANT CELL GRANULOMA
• GIANT CELL FIBROMA
• PHENYTOIN-INDUCED GINGIVAL HYPERPLASIA
INFLAMMATORY AND REACTIVE LESIONS
• NODULAR FASCIITIS
• BENIGN MYOFIBROBLASTOMA
• FIBROMATOSIS
• SARCOMAS
PROLIFERATIVE MYOFIBROBLASTIC LESIONS
• AMELOBLASTOMA
• ODONTOGENIC KERATOCYST
• ODONTOGENIC MYXOMAODONTOGENIC LESIONS
• ORAL SUBMUCOUS FIBROSIS
• SQUAMOUS CELL CARCINOMA
PRECANCEROUS AND CANCEROUS LESIONS
38
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofibroblasts in oral lesions: A review. J
Oral Maxillofac Pathol 2014;18:52-7.

ODONTOGENIC KERATOCYST
39
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofi broblasts in oral lesions: A review. J
Oral Maxillofac Pathol 2014;18:52-7.

FOLLICULAR AMELOBLASTOMA
40
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofi broblasts in oral lesions: A review. J
Oral Maxillofac Pathol 2014;18:52-7.

UNICYSTIC AMELOBLASTOMA
41
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofi broblasts in oral lesions: A review. J
Oral Maxillofac Pathol 2014;18:52-7.

SQUAMOUS CELL CARCINOMA
42
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofi broblasts in oral lesions: A review. J
Oral Maxillofac Pathol 2014;18:52-7.

ROLE OF MYOFIBROBLASTS IN FIBROSIS
After tissue injury, fibroblasts differentiate intocontractile and secretary myofibroblasts which helpin tissue repair during wound healing, but this canseverely disturb the organ function whencontraction and extracellular matrix proteinsecretion become excessive, such as inscleroderma, hypertrophic scars, kidney, lung andheart fibrosis.
Myofibroblasts play significant roles in promotingECM deposition, release of inflammatory mediatorsand epithelial injury, which are believed to beimportant factors in perpetuating the cycle of injuryof fibrosis.
43
Hinz boris, Phan Sem H, Thannickal Victor J, Galli Andrea, Bochaton-Piallat Marie-Luce, Gabbiani Giulio.
The myofibroblast – One Function, Multiple Origins. Am J Pathol 2007;170(6):180716.

44
de Haan and Arslan: Highlights of Keystone symposium ‘Fibrosis : from bench to bedside’ Fibrogenesis
& Tissue Repair 2014, 7:11

The fate of activated myofibroblasts in injured
tissues may eventually decide whether there will be
normal healing or progression to the end-stage
fibrosis.
Resolution with myofibroblast apoptosis would
terminate progression; however, this would be
countered by persistence of TGFβ1 expression and
ECM deposition, which promote the pro-survival or
antiapoptotic phenotype.
45
Hinz boris, Phan Sem H, Thannickal Victor J, Galli Andrea, Bochaton-Piallat Marie-Luce, Gabbiani Giulio.
The myofibroblast – One Function, Multiple Origins. Am J Pathol 2007;170(6):180716.
It is shown in recent studies that during fibrotic
situations, myofibroblasts develop the ability of
creating a long-lasting tension essentially regulated
at the level of RhO/RhO kinase-mediated inhibition
of myosin light chain phosphatase, compared with
the usual contraction-relaxation activity depending
on Ca2+ induced phosphorylation of myosin light
chain kinase taking place in smooth muscle cells-
SMCs.
46
Hinz boris, Phan Sem H, Thannickal Victor J, Galli Andrea, Bochaton-Piallat Marie-Luce, Gabbiani Giulio.
The myofibroblast – One Function, Multiple Origins. Am J Pathol 2007;170(6):180716.
In one study it was shown that Oral Sub Mucous
Fibrosis (OSMF) may possibly represent an
abnormal healing process in response to chronic
mechanical and chemical irritation due to areca nut
chewing as exhibited by the increased incidence of
myofibroblasts in this disease.
Also it was seen that there was progressive
increase in myofibroblasts from early to advanced
stages.
Hence to control fibrosis it is essential to stop
myofibroblast activities.
47
Angadi PV, Kale AD, Hallikerimath S. Evaluation of myofibroblasts in oral submucous fibrosis: correlation
with disease severity. J Oral Pathol Med 2011;40(3):208-13.

ROLE OF MYOFIBROBLASTS IN ORAL CANCER
It is well known fact that many epithelial tumours
are characterised by the local accumulation of
connective tissue cells and extracellular material;
this phenomenon has been called the stroma
reaction.
In stroma reaction, the myofibroblast is one of the
cellular components.
Myofibroblasts interact with epithelial cells and
other connective tissue cells and may thus control
such phenomena as tumour invasion and
angiogenesis.48
Gabbiani G. The Evolution of the Myofibroblast Concept: a Key Cell for Wound Healing and fibrotic diseases. G
Gerontol 2004;52:280-2.

Cancer invasion progresses by ECM degradation at
the cancer-stroma interface, loss of epithelial
morphology and acquisition of mesenchymal
characteristics, referred to as the epithelial-
mesenchymal transition (EMT), are typical for
invasive carcinoma cells and predispose tumours to
a more advanced state of progression.
49
Kawashiri S, Tanaka A, Noguchi N, Hase T, Nakaya H, Ohara T, et al. Significance of Stromal Desmoplasia
and Myofibroblast appearance at the invasive front in Squamous Cell Carcinoma of the Oral Cavity. Head
Neck 2009;31(10):1346-53.

In normal mucosa, physiological turnover of the epithelium is the only stimulus for a stromalreaction.
In contrast, cancer cells invade the stroma by altering the stromal microenvironment via the destruction of normal tissue.
Although both the synthesis and degradation of the ECM occur during wound healing, cancer invasion may progress when ECM degradation exceeds its synthesis, preventing complete healing.
The mesenchymal cells that mediate proteolyticactivity in the stroma could be myofibroblasts. The fibrous stroma in oral SCC is a desmoplasticresponse.
50
Kawashiri S, Tanaka A, Noguchi N, Hase T, Nakaya H, Ohara T, et al. Significance of Stromal Desmoplasia
and Myofibroblast appearance at the invasive front in Squamous Cell Carcinoma of the Oral Cavity. Head
Neck 2009;31(10):1346-53.

In many types of solid tumour SMA-positive
myofibroblasts (Peritumour fibroblasts, carcinoma-
associated fibroblasts) are found within the stromal
compartment.
Most commonly, myofibroblasts have been
described as differentiating locally from fibroblasts.
However, it is now evident that a number of other
cell types may undergo myofibroblastic
transdifferentiation.
51
Kawashiri S, Tanaka A, Noguchi N, Hase T, Nakaya H, Ohara T, et al. Significance of Stromal Desmoplasia
and Myofibroblast appearance at the invasive front in Squamous Cell Carcinoma of the Oral Cavity. Head
Neck 2009;31(10):1346-53.

These include other locally-derived mesenchymal
cells such as adipocytes, stellate cells and
pericytes, as well as circulating mesenchymal stem
cells, monocytes in bone marrow and epithelial
cells, but it is not possible to identify which cells in
cancer tissue transit myofibroblasts.
Cancer cell derived transforming growth factor
(TGF) stimulation may activate fibroblasts, leading
to their transdifferentiation into myofibroblasts.
52
Kawashiri S, Tanaka A, Noguchi N, Hase T, Nakaya H, Ohara T, et al. Significance of Stromal Desmoplasia
and Myofibroblast appearance at the invasive front in Squamous Cell Carcinoma of the Oral Cavity. Head
Neck 2009;31(10):1346-53.
Transition of myofibroblast appearance in invasive
cancer and particularly tumour desmoplasia, is an
important reflection of the tumour-host interaction
especially in aggressive cancers.
Several cytokines including TGF-β, PDGF, IL-4 &
IGF-II have been reported to induce myofibroblastic
differentiation. TGF-β1 is a pleiotropic cytokine
which is over expressed in many carcinomas and
may be pro-oncogenic.
53
Kawashiri S, Tanaka A, Noguchi N, Hase T, Nakaya H, Ohara T, et al. Significance of Stromal Desmoplasia
and Myofibroblast appearance at the invasive front in Squamous Cell Carcinoma of the Oral Cavity. Head
Neck 2009;31(10):1346-53.

In one study it was demonstrated that tumour cells
induced transdifferentiation of oral normal
fibroblasts to myofibroblasts via secretion of
transforming growth factor beta- 1 (TGF-β1).
In turn, myofibroblasts secreted factors that
stimulated OSCC cell proliferation as revealed by
Ki67 expression.
54
Kellermann MG, Sobral LM, da Silva SD, Zecchin KG, Graner E, Lopes MA, et al. Mutual paracrine effects of
oral squamous cell carcinoma cells and normal oral fibroblasts: Induction of fibroblast to myofibroblast
transdifferentiation and modulation of tumor cell proliferation. Oral Oncol 2008;44(5):509-17.
Myofibroblasts also promote invasion by
remodelling the extracellular matrix and
metalloproteinases (MMPs) and their inhibitors
produced by both cancer and stromal cells are
known to play a role in altering the composition of
the tumour micro environment and are prognostic.
55
Kellermann MG, Sobral LM, da Silva SD, Zecchin KG, Graner E, Lopes MA, et al. Mutual paracrine effects of
oral squamous cell carcinoma cells and normal oral fibroblasts: Induction of fibroblast to myofibroblast
transdifferentiation and modulation of tumor cell proliferation. Oral Oncol 2008;44(5):509-17.

In another study, data demonstrated activin A
(growth factor) is required for the proliferative
effects of myofibroblasts on OSCC cells.
Myofibroblasts in the stroma of OSCC may
influence proliferation and invasion, resulting in
more aggressive tumour.
56
Sobral LM, Bufalino A, Lopes MA, Graner E, Salo T, Coletta RD. Myofibroblasts in the stroma of oral
cancer promote tumorigenesis via secretion of activin A. Oral Oncol 2011;47(9):840-6.

Studies conducted by Kellerman et al and
Moghadam et al revealed no statistically significant
difference in the mean number of myofibroblasts
between well, moderate and poorly differentiated
OSCC and suggested that transdifferentiation of
MFs occurs during the invasive stage of
carcinomatous epithelium and further loss of
tumoral differentiation does not affect the number
of cells.
57
Kellermann MG, Sobral LM, da Silva SD, Zecchin KG, Graner E, Lopes MA, et al. Mutual paracrine effects of
oral squamous cell carcinoma cells and normal oral fi broblasts: Induction of fi broblast to myofi broblast
transdifferentiation and modulation of tumor cell proliferation. Oral Oncol 2008;44:509-17.

58
Kellermann MG, Sobral LM, da Silva SD, Zecchin KG, Graner E, Lopes MA, et al. Myofibroblasts in the
stroma of oral squamous cell carcinoma is associated with poor prognosis. Histopathology 2007;51:849-53.

Morphologic characters of the invasive front may
better reflect the tumor prognosis than other parts
of the tumor. Few studies done in this regard,
reported high levels of collagen fibers and stromal
MFs at the invasive front and their number
increased with the increasing tumor invasiveness.
59
Vered M, Allon I, Buchner A, Dayan D. Stromal myofi broblasts accompany modifi cation in the epithelial
phenotype of tongue dysplastic and malignant lesions. Cancer Microenviron 2009;2:49-57.

The presence of MFs was also thought to be
associated with tumor prognosis.
Studies done in this regard showed that increased
MFs was associated with poor prognosis.
MFs in tongue cancer were associated with risk
score and prognosis.
60
Marsh D, Suchak K, Moutasim KA, Vallath S, Hopper C, Jerjes W, et al. Stromal features are predictive of
disease mortality in oral cancer patients. J Pathol 2011;223:470-81.

Patients whose specimens were weakly positive for
α-SMA had 5 year mean survival rate of 82%;
whereas, patients with samples that were strongly
positive with α-SMA had a mean survival rate of
38% indicating that the presence of more number of
MFs in the stroma is associated with poor
prognosis.
Thus, the presence of increased stromal MFs is an
effective predictor of oral squamous cell carcinoma
patient mortality.
61
Marsh D, Suchak K, Moutasim KA, Vallath S, Hopper C, Jerjes W, et al. Stromal features are predictive of
disease mortality in oral cancer patients. J Pathol 2011;223:470-81.

CONCLUSION
Myofibroblasts are ubiquituous cells with similar
properties and functions that play significant roles
in growth, development, wound repair as well as
disease.
As they are present in virtually every tissue, it is
possible that they may play a role in multisystem
diseases.
62

Understanding the role of the stromal cells and
extracellular matrix will allow us to identify more
precise prognostic markers and potentially device
new therapeutic options and prevent various
diseases caused by these miraculous multipotential
cells.
Studies can help us to use only beneficial effects of
myofibroblasts and control their activation wherever
they act hyperactive.
63
REFERENCES
64
Powell DW, Miffin RC, Valentich JD, Crowe SE, Saada JI, WestAB. Myofibroblasts. I. Paracrine cells important in health anddisease. Am J Physiol 1999;277(1 Pt 1):C1-9.
Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C, Brown RA.Myofibroblasts and mechano-regulation of connective tissueremodelling. Nat Rev Mol Cell Biol 2002;3:349-63.
Gabbiani G, Ryan GB, Majno G. Presence of modified fibroblastsin granulation tissue and their possible role in wound contraction.Experientia 1971;27:549-50.
Schurch W, Seemayer TA, Hinz B, Gabbiani G. Myofibroblast. In:Mills SE, editor. Histology for Pathologists. Philadelphia:Lippincott-Williams and Wilkins Publishers; 2007. p. 123-164.

Valentich J. D., Popov V., Saada J. I., Powell D. W.(1997) Phenotypiccharacterization of an intestinal subepithelial myofibroblast cellline. Am. J. Physiol. 272(Cell Physiol. 41):C1513–C1524
Mills, S E. Histology for Pathologists. Lippincott Williams &Wilkins, 3rd Edition
Drobnik J et al. Experimental hypothyroidism increases content ofcollagen and glycosaminoglycans in the heart. J PhysiolPharmacol. 2009 Sep;60(3):57-62
www.pathresidents.com
Schmitt-Graff, A., A. Desmouliere, and G. Gabbiani.Heterogeneity of myofibroblast phenotypic features: an exampleof fibroblastic cell plasticity. Virchows Arch. 425: 3–24, 1994.
65
Scotton C J, Chambers R C. Molecular targets in pulmonary fibrosis -The myofibroblast in focus. CHEST 132- 4 (Oct 2007).
Van Beurden HE, Von den Hoff JW, Torensma R, Maltha JC,Kuijpers- Jagtman AM. Myofibroblasts in Palatal Wound Healing:Prospects for the Reduction of Wound Contraction after Cleft PalateRepair. J Dent Res 2005;84(10):871-80.
Pinisetti S, Manyam R, Suresh B, Aparna V. Myofibroblasts in orallesions: A review. J Oral Maxillofac Pathol 2014;18:52-7.
Hinz boris, Phan Sem H, Thannickal Victor J, Galli Andrea, Bochaton-Piallat Marie-Luce, Gabbiani Giulio. The myofibroblast –One Function, Multiple Origins. Am J Pathol 2007;170(6):180716.
66