national health programmes
TRANSCRIPT

Dr. Vineetha.kDepartment of Public Health Dentistry
UNIVERSAL IMMUNISATION PROGRAMME
NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS

GOOD MORNING
“Those who would benefit most from a service are least likely to obtain it”

NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS

CONTENTS• INTRODUCTION• BURDEN OF DISEASE• THE PROGRAM• GOALS AND OBJECTIVES• BUDGET• ELEVENTH FIVE YEAR PLAN• STRATEGIES• ACTIVITES• ORGANIZATIONAL STRUCTURE• EXTERNALLY AIDED PROJECTS• RIGHT TO SIGHT• ACHEIVEMENTS

INTRODUCTIONOne of the basic human right is the right to see. We have to ensure that no citizen goes blind needlessly , or being blind , does not remain so, if by reasonable deployment of skill and resources, his eyesight can be prevented from deterioration or if already lost can be restored. npcb.nic.in

• BLINDNESS – Visual acquity of less than 3/60 snellan
• Avoidable blindness has been defined as blindness that could reasonably be prevented or cured within the limits of resources
BLINDNESS
Approximately 80% of all blindness is considered to be avoidable

WORLD314 million - Visually impaired 45 million - Of them are blind
• 1990- ranged from 0.08% of children to 4.4% of persons aged over 60 years, with an overall global prevalence of 0.7%.
• 7 million people become blind each year and that the number of blind people worldwide was increasing by 1–2 million per year.
BURDEN OF DISEASE

INDIA• 2003-1.1% in the major States and 1.38% in the
north-eastern States• 2006-07 -1%.• 12 million blind persons• 26% children

MAJOR CAUSES OF CHILDHOOD BLINDNESS
VISUAL IMPAIRMENT DUE TO UNCORRECTED REFRACTIVE
ERRORS
VITAMIN A DEFICIENCY
DEVELOPMENTAL CATARACT
RETINAL CONDITIONS
OPTIC ATROPHY
CONGENITAL ANOMALIES

MAJOR CAUSES OF BLINDNESS IN INDIA
Disease %Cataract 62.60Refractive error 19.70Corneal blindness 0.9Glaucoma 5.80Surgical complication
1.20
Post. Capsular opacification
0.9
Posterior segment disorder
4.7
Others 4.19

HEALTH POLICY
• 2002• 1.1% to <0.5%, 2010.

1976 - Ministry of Health and family welfare
India- First country to launch
Incorporates earlier Trachoma programme 1963
100% centrally sponsored
Decentralized in 1994-96 DBCs formed
PROGRAM

GOALSTo reduce prevalence of blindness from
1.4% <0.3% by 2020
To establish an infrastructure and efficiency levels to cater new cases of blindness every year.

To reduce the backlog of blindness through identification and treatment of blind.
To improve quality of service delivery
To develop comprehensive eye care facilities in every district
To develop human resources for eye care services
To enhance community awareness on eye care
To secure participation of civil society, NGOs, and the private sector in eye care
OBJECTIVES

NPCB BUDGET
9th Five Year Plan 2500 Million INR
1.2% of GDP on Health
0.9% of health expenditure on NPCB

TARGETS FOR ELEVENTH FIVE YEAR PLAN
• Prevention, control, management- diabetes retinopathy.
• Hospital based screening of glaucoma and prevention of childhood
blindness.
• Improve visual outcome of cataract surgery by IOL implantation.
• Paediatric opthalmology units.
• Vision centres in rural areas.
• Fully functional eye bank networks.
• Human resource and institutional capacity.

STRATEGY OF THE PROGRAMME
Strengthening service delivery
Developing human
resources for eye care
Promoting out-reach
activities and public
awareness
Developing institutional
capacity
To establish eye care
facilities for every 5 lac persons.

REVISED STRATEGIES
To make NPCB more comprehensive-corneal blindness, refractive error, post op cataract, glaucoma.
To shift eye camp approach to a fixed facility surgical approach.
To expand world bank project activities like construction of dedicated eye operation theatres
To strengthen participation of voluntary organization in programme.
To enhance eye care services in tribal and other under served areas.

ACTIVITIES


OTHER MAJOR ACTIVITIES
CHEMOTHERAPY

ORGANISATIONAL STRUCTURENational Program Management Cell
State Program Cell
District Blindness Control Society
District
District hospital District Health OfficerOphthalmic Surgeon District mobile unit CHCs
PHC s
Medical officers
Paramedical Ophthalmic assistants

EXTERNALLY AIDED PROJECTS
• WORLD BANK assisted cataract blindness control project
• DANISH assistance to NPCB
• WHO assistance for prevention of blindness
VISION 2020- THE RIGHT TO SIGHT

Vision 2020 : The right to sight

THE RIGHT TO SIGHTGlobal Initiative To Reduce Avoidable Blindness By 2020
Human resource development as well as infrastructure and technology development at various levels of health system.
TARGET DISEASES
1. CATARACT2. REFRACTIVE ERRORS3. CHILDHOOD BLINDNESS4. CORNEAL BLINDNESS5. GLAUCOMA6. DIABETIC RETINOPATHY.


ACHIEVEMENTSCATARACT SURGERIES• Success rates• Proportion <9 1994 to 93% 2007• 2009-10 92.5% cataract surgeries
against 95% target• 2011-12 63,49,205 surgeries with
95% IOL implantation
307 DEDICATED EYE OPERATION THEATRES AND EYE WARDS IN DISTRICT LEVEL HOSPITALS

Free Spectacles to school children 708861
Collection of donated eyes
53543
2000 Eye Surgeons trained in IOL surgery
and other super specialties.

UNIVERSAL IMMUNISATION PROGRAMME

CONTENTS
• INTRODUCTION• EVOLUTION• OBJECTIVES• VACCINES UNDER UIP• IMMUNIZATION SCHEDULE• VACCINATION PROGRAMMES• PROGRAMME ACHEIVEMENTS

INTRODUCTION
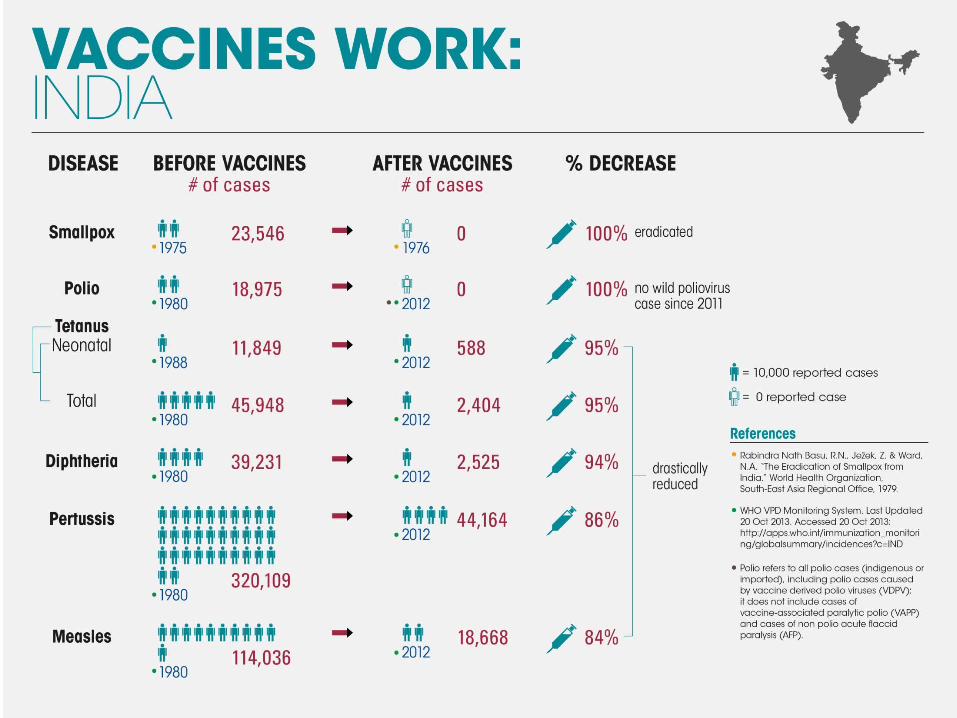
• Vaccine preventable diseases were widespread and were a major cause of childhood morbidity, mortality and lifelong physical and mental disabilities prior to immunization programmes.

UNIVERSAL IMMUNIZATION PROGRAM
• Largest UIP program in the world.• Targets include 27 MILLION INFANTS and
30.2 MILLION PREGNANT WOMEN every year• Protection against six Vaccine Preventable Diseases
(VPDs) – Tuberculosis, Diphtheria, Tetanus, Pertussis, Polio and Measles
• Two new vaccines (JE and Hepatitis B) introduced in select areas

MILESTONES1962 •BCG was the first immunization which started against TB
1978•Expanded program on immunization•BCG OPV DPT TYPHOID
1979•Renamed as Universal Immunization Program•Measles was added
1992 •Merged with Child survival and safe motherhood program
1997 •Merged with Reproductive and Child Health Program I
2005 •RCH II and National Rural Health Mission

AIMS100%
coverage of pregnant women
Two doses of tetanus
toxoid
Atleast 85% coverage of infants
3 doses of DPT, OPV
One dose of BCG and measles vaccine.

OBJECTIVESRapidly increase immunization coverage
Improve the quality of services
Establish a reliable cold chain system to the health facility level Introduce a district-wise system for monitoring of performance
Achieve self-sufficiency in vaccine production

VACCINES UNDER UIP1. BCG (Bacillus Calmette Guerin)
2. DPT (Diphtheria, Pertussis and Tetanus Toxoid)
3. OPV (Oral Polio Vaccine)
4. Measles
5. Hepatitis B
6. TT (Tetanus Toxoid)
7. JE vaccination (in selected high disease burden districts)
8. Hib containing Pentavalent vaccine (DPT+HepB+Hib) (In selected States)


BCG
• At birth or as early as possible till one year of age
• 0.1 ml (0.05ml until one month of age)• Intra-dermal • Left upper arm

HEPATITIS-B-VACCINE
• Birth dose – within 24 hours of birth • 0.5 ml • Intramuscular• Antero-lateral side of mid-thigh• Rest three doses at 6 weeks, 10 weeks and 14
weeks

DPT
• Three primary doses at 6, 10 and 14 weeks with OPV-1, 2 and 3
• 0.5 ml• Intra-muscular• Antero-lateral side of mid-thigh• One booster at 16-24 m with OPV booster
(antero-lateral side of mid-thigh) and second booster at 5-6 years (upper arm)

MEASLES • At 9 completed months to 12 months• Give upto 5 years if not received at 9-12 months age• Second dose at 16-24 months (select states after
catch-up campaign) – Measles Containing Vaccine• 0.5 ml• Sub-cutaneous• Right upper arm• Along with Vitamin A (1st dose) – 1ml (1 lakh IU) - oral

OPV
• Zero dose – within first 15 days of birth• 2 drops • Oral• First, second and third doses at 6, 10 and 14
weeks with DPT-1, 2 and 3• OPV booster with DPT booster at 16-24
months

PULSE POLIO


• ACHIEVEMENTS - India was declared as a POLIO FREE NATION by WHO on 27th March 2014

TETANUS TOXOID• Intramuscular – upper arm – 0.5 ml• Pregnancy – 2 doses - 1st dose as early as possible
and second dose after 4 weeks of first dose and before 36 weeks of pregnancy
• Pregnancy – booster dose (before 36 weeks of pregnancy) – If received 2 TT doses in a pregnancy within last three years. Give TT to woman in labour, if she has not received TT previously
• TT booster for both boys and girls at 10 years and 16 years
• No TT required between two doses in case of injury

VITAMIN A
• 1st dose – 1 ml (1 IU) - along-with Measles first dose - Oral
• Subsequent 8 doses (2 ml or 2 lakh IU) every six months till 5 years of age starting with DPT first booster at 16-24 months
• Use only plastic spoon provided with Vitamin A solution

JAPANESE ENCEPHALITIS• SA 14-14-2 vaccine in select endemic districts
after campaign in UP, Bihar, Assam, Haryana, Andhra Pradesh, Goa, Karnataka, Manipur, West Bengal, Tamil Nadu
• 16-24 months with DPT and OPV booster• 0.5 ml• Subcutaneous• Left upper arm

PENTAVALENT VACCINE• DPT + Hep B + Haemophilus influenzae b• Intramuscular• Antero-lateral side of mid-thigh• 0.5 ml dose• At 6, 10 and 14 weeks with booster at 16-24
months • Proposed to be piloted in Kerala and Tamil Nadu – pending ICMR study
completion





The coverage has increased by 4% in the last 4 years i.e. at the rate of 1% per year.
MISSION INDRADHANUSH
75.5 lakh children were vaccinated
19.7 lakh children were fully vaccinated. 20.8 lakh pregnant women were vaccinated for Tetanus toxoid. Infant mortality rate and under-five mortality rate due to vaccine preventable diseases
has decreased considerably.
ACHIEVEMENTS
India’s infant mortality rate has declined from 80 per 1,000 live births in 1990 to 40 per 1,000 live births in 2013 and under-five mortality rate from 126 per 1,000 live births in 1990 to 49 per 1,000 live births in 2013.
This has been possible due to child health interventions including immunization.

REFERENCES1)Park K. Park’s Textbook of Preventive and Social Medicine. 23rd ed. Jabalpur: Bhanot; 2016: 439 – 444
2)Kishore J. National Programs of India. 9th ed. New Delhi: Century Publications; 2011.
3)Ministry of Health and Family Welfare, Government of India.Universal immunization programme. www.mohfw.nic.in/WriteReadData/l892s/Immunization_UIP.pdf Accessed on July 23rd, 2016.
4)Ministry of Health and Family Welfare, Government of India. National programme for control of blindness. http://npcb.nic.in/index1.asp?linkid=29&langid=1Accessed on July 23rd, 2016.
5) Verma R, Khanna P, Prinja S, Rajput M, Arora V. The National Programme for Control of Blindness in India. The Australasian Medical Journal. 2011;4(1):1-3. doi:10.4066/AMJ.2011.505.

THANK YOU