national program on prevention and control of infection and antimicrobial resistance, jose artur...
TRANSCRIPT
National Program on Prevention and Control of Infection and Antimicrobial Resistance – PPCIRA / PORTUGAL
José Artur Paiva, Elaine Pina, Maria Goreti Silva, Paulo André Fernandes, Anabela Coelho, José Alexandre Diniz, Francisco George Manuela Caniça, Jorge Machado, Ana Silva
Where were we in 2011-2012 ?
Before PPCIRA……

Prevalence of HAI AM use
Portugal EU Portugal EU
Men 12,4% 7,2% 48,3% 39,2%
Women 8,8% 5,4% 42,3% 33,2%
Global population
10,5%
6,1%
45,3%
35,8%
PPS DGH 2012
High prevalence of hospital acquired infection and high antimicrobial consumption

High hospital consumption of carbapenems
“ In 2012, consumption of carbapenems varied by a factor of 14, from 0.01 (Bulgaria) to 0.14 DDD per 1 000 inhabitants and per day (Portugal)“ “The proportion of consumption of carbapenems out of antibacterials for systemic use ranged from 0.8% (Latvia) to 9.8% (Portugal) with an EU/EEA population-weighted mean of 2.9%.”
2010
Carbapenems
ECDC; ESAC Net 2012
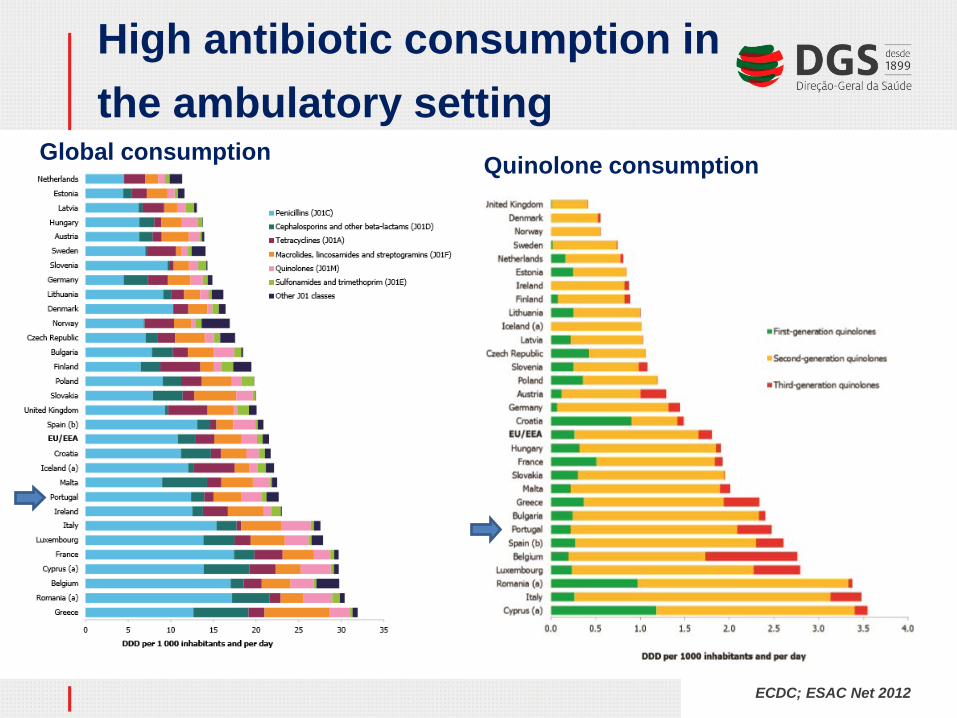
High antibiotic consumption in the ambulatory setting
Insira o seu texto
ECDC; ESAC Net 2012
Global consumption Quinolone consumption
6
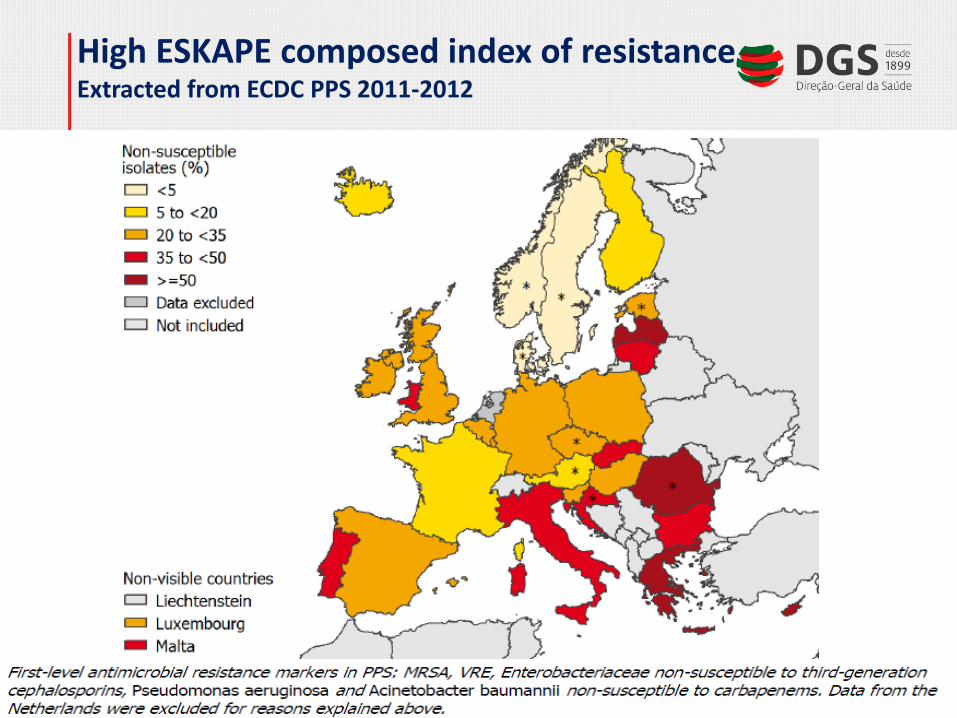
High ESKAPE composed index of resistance Extracted from ECDC PPS 2011-2012
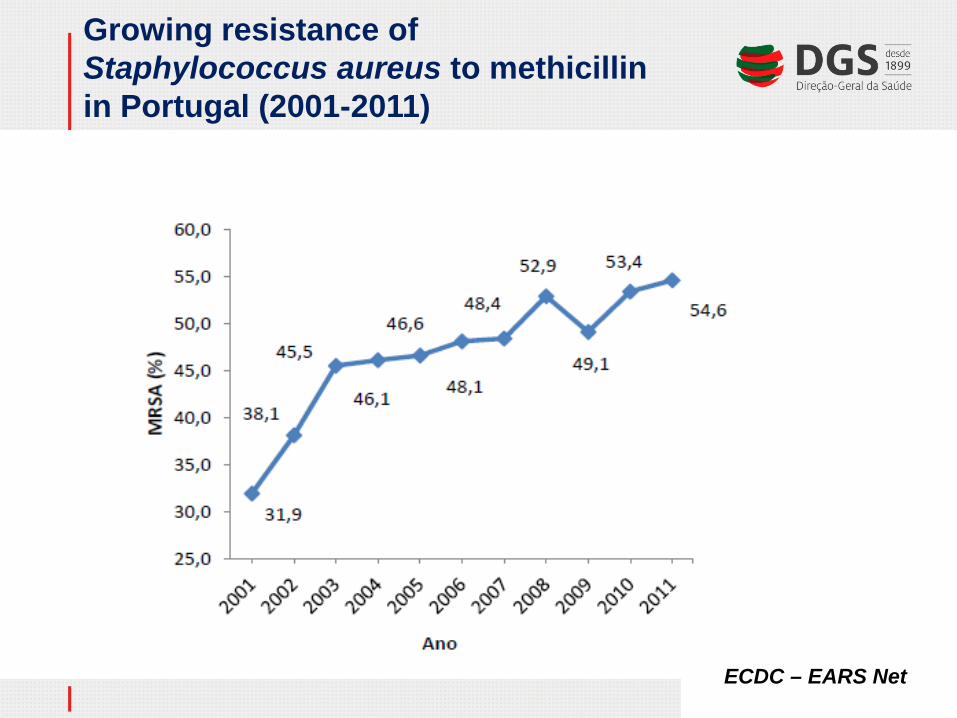
Growing resistance of Staphylococcus aureus to methicillin in Portugal (2001-2011)
ECDC – EARS Net

Weaknesses and threats
• Low level of integration and synergy of the several processes; no holistic vision; too many process leaders
• Understaffing underpowerment of the central and peripheral structures
• Absence of focus in the most relevant issues: MRSA, CRE, carbapenems, quinolones, Standard precautions campaign
• Problems of data sharing among state institutions and of data feedback to the providers
• Difficulties in implementing a collaborative model, increasing capacity building and maximizing participation.
• Reimbursement system not reflecting the indicators and targets and not boosting motivation
What has been done in 2013-2014?
PPCIRA initiatives
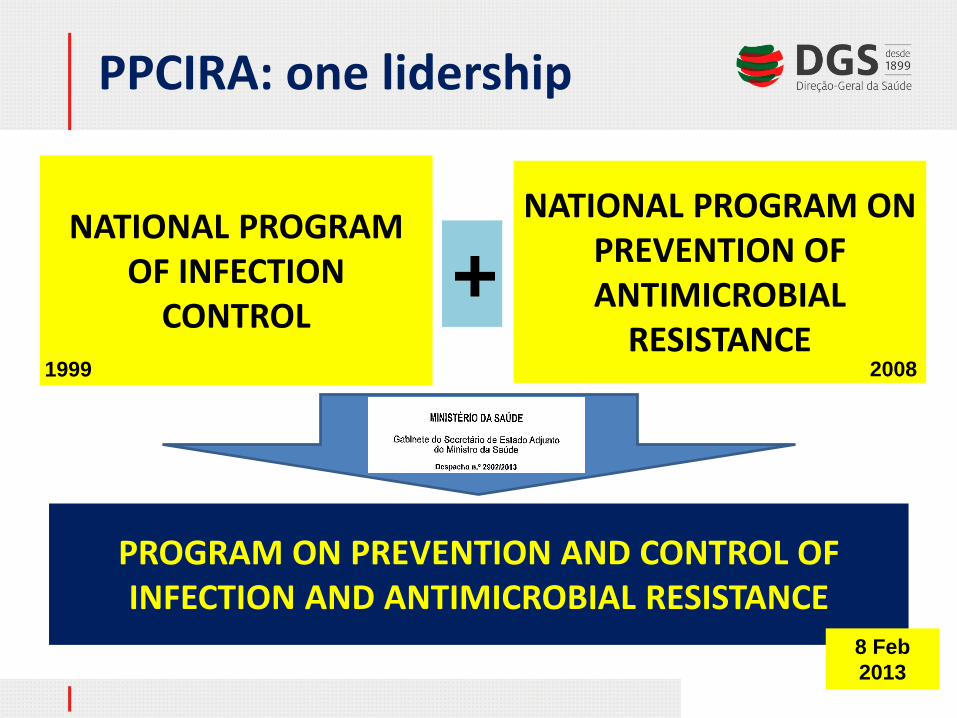
PROGRAM ON PREVENTION AND CONTROL OF INFECTION AND ANTIMICROBIAL RESISTANCE
NATIONAL PROGRAM
OF INFECTION CONTROL
NATIONAL PROGRAM ON PREVENTION OF ANTIMICROBIAL
RESISTANCE +
8 Feb 2013
1999 2008
PPCIRA: one lidership

PPCIRA management structure: law 15423/2013 Directorate
General of Health (DQS)
Regional Health Authority (RHA)
Health Units
94% H; 25% PC
PPCIRA central direction
PPCIRA Regional
Coordination Group
PPCIRA Local
Coordination Group
Pharmacy and Therapy Regional Committee
RHA Administrator on Quality
Local Comission on Quality and Safety
Pharmacy and Therapy Hospital Comission
Depart. Of Quality in Health - DNH
PPCIRA Scientific Council
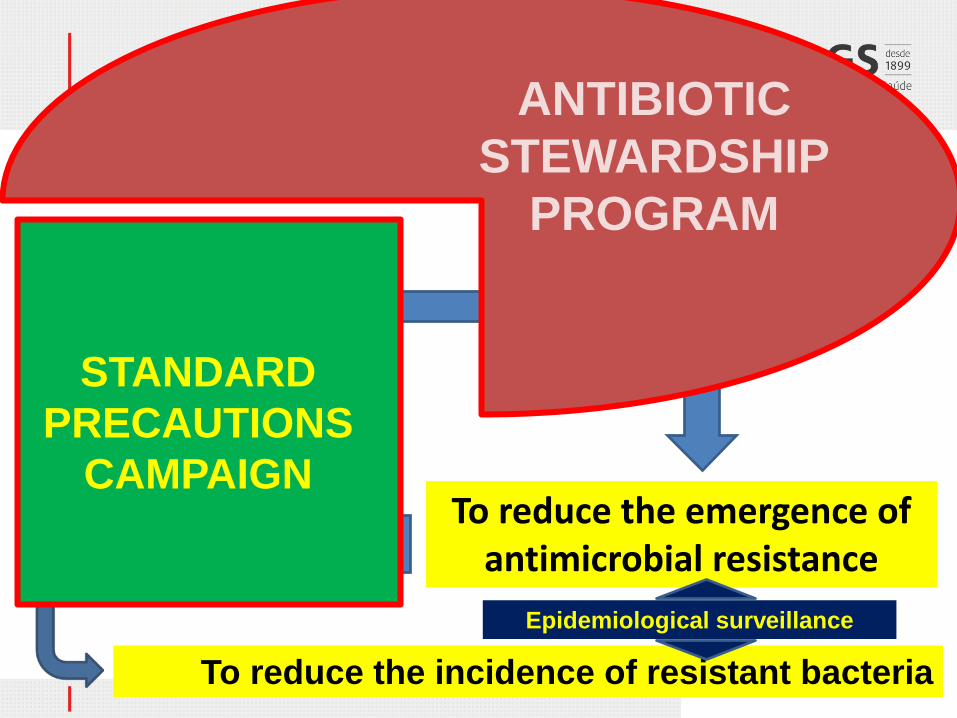
Reduce HCAI Reduce antimicrobial consumption
To reduce the emergence of antimicrobial resistance
Evict antibiotics when there is no
infection
Reduce transmission of antimicrobial
resistance
Shorten antibiotic treatment duration
To reduce the incidence of resistant bacteria
STANDARD PRECAUTIONS
CAMPAIGN
ANTIBIOTIC STEWARDSHIP
PROGRAM
Epidemiological surveillance

Adhesion to the main interventions
Launching 2012 2014 Epidemiological surveillance of antimcrobial resistance (Microbiology Lab)
Guideline NRL/DGH
21 February 2013
22
70
Epidemiological surveillance of at least one of the HAI
Law 15423/2013
18 November 2013
85%
Antimicrobial Stewardship Program
Law 15423/2013
18 November 2013
0
40% hospitals
Standard Precautions Campaign
5 May 2014
-
70% hospitals
24% PCC
September 2014 PPCIRA /DGH

PPCIRA “bundles”
Hand hygiene Adequate use of gloves • Patient/clinical environmental hygiene “Anti-MRSA” policy Surgical antibiotic prophylaxis for no more than 24 h Duration of antibiotic duration limited to 7 days (with exceptions) • Reduction of quinolone and carbapenem prescription Antimicrobial stewardship program in the first 96 h
Hand hygiene Adequate use of gloves • Patient/Clinical environmental hygiene Compliance with the vaccination program • Adquate tretment of wounds • Reduction in the prescription of quinolones • Guideline for the treatment of RTI Guideline for the treatment of UTI Antimicrobial stewardship program
Hospital Bundle
Comunity Bundle

Education and Pedagogy
• “Train the trainers” course • In all RHA (7 health regions) • Topics: strategy, implementation and science • Two modules, hospital and ambulatory, in two
consecutive days • 4 trainers per course; a total of 8 trainers • In October 2014, more than 600 doctors and
nurses were trained as trainers

Citizen’s awareness Winter 2013

What has been achieved ?
PPCIRA results

Reduction of large spectrum antibiotic consumption in the ambulatory setting
Quinolones: Higher consumption among ECDC
countries in 2010 Improvement to 7th place in 2013 European median= 1,81
GUIDELINES: - Duration of antibiotic
therapy - Treatment of UTI
INFARMED, 2014
Quinolone consumption
Large spectrum over small spectrum antbiotic consumption

Reduction of antibiotic consumption in the hospital setting
GUIDELINES: - Duration of antibiotic treatment - Treatment of UTI - Surgical antibiotic prophylaxis
INFARMED, 2014
Feedbacking data to
hospitals
Hospital antibiotic consumption in the 1st semester of the year

Reduction of the rate of Staphylococcus aureus resistance to methicillin (MRSA)
ECDC / EARS Net
% of the invasive Staph aureus isolates resistant to methicillin
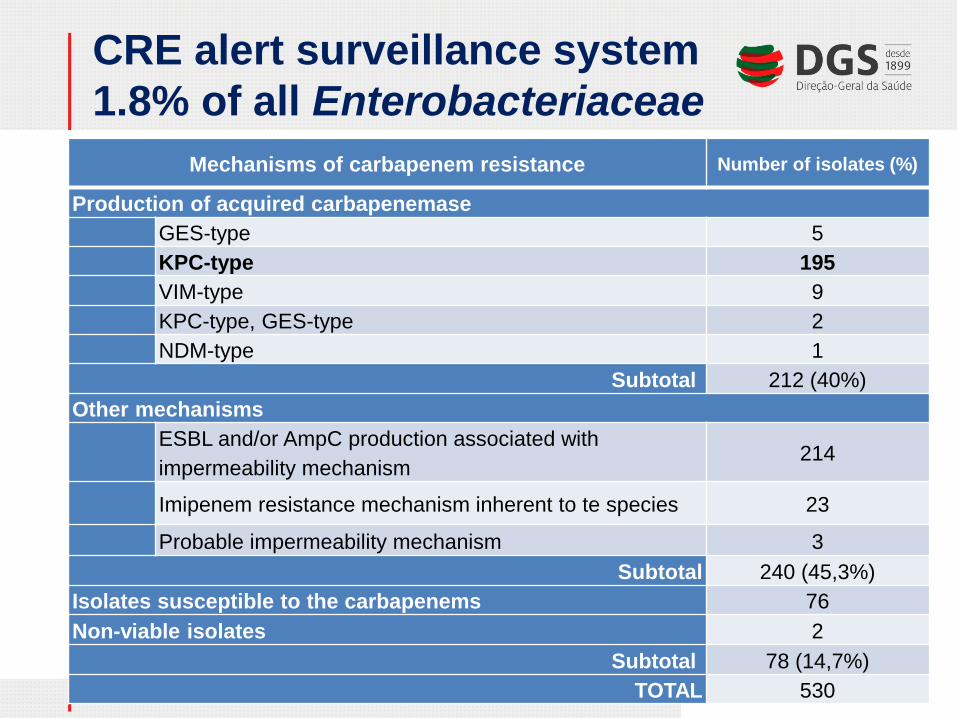
CRE alert surveillance system 1.8% of all Enterobacteriaceae
Mechanisms of carbapenem resistance Number of isolates (%)
Production of acquired carbapenemase GES-type 5 KPC-type 195 VIM-type 9 KPC-type, GES-type 2
NDM-type 1 Subtotal 212 (40%)
Other mechanisms ESBL and/or AmpC production associated with impermeability mechanism
214
Imipenem resistance mechanism inherent to te species 23
Probable impermeability mechanism 3 Subtotal 240 (45,3%)
Isolates susceptible to the carbapenems 76 Non-viable isolates 2
Subtotal 78 (14,7%) TOTAL 530

CR-BSI (per 1000 CVC days): 2003-2013
3.1 3.0
2.5
2.1 1.9 1.9
0.9
1.4
1.9
2.4
2.9
3.4
2002-2004 2005-2007 2010 2011 2012 2013
Variação da taxa de INCS associada a CVCLinear (Variação da taxa de INCS associada a CVC)

Reduction of some of the HAI
Density of nosocomial BSI due to Staphylococcus aureus and by MRSA
Infections in Adult ICUs
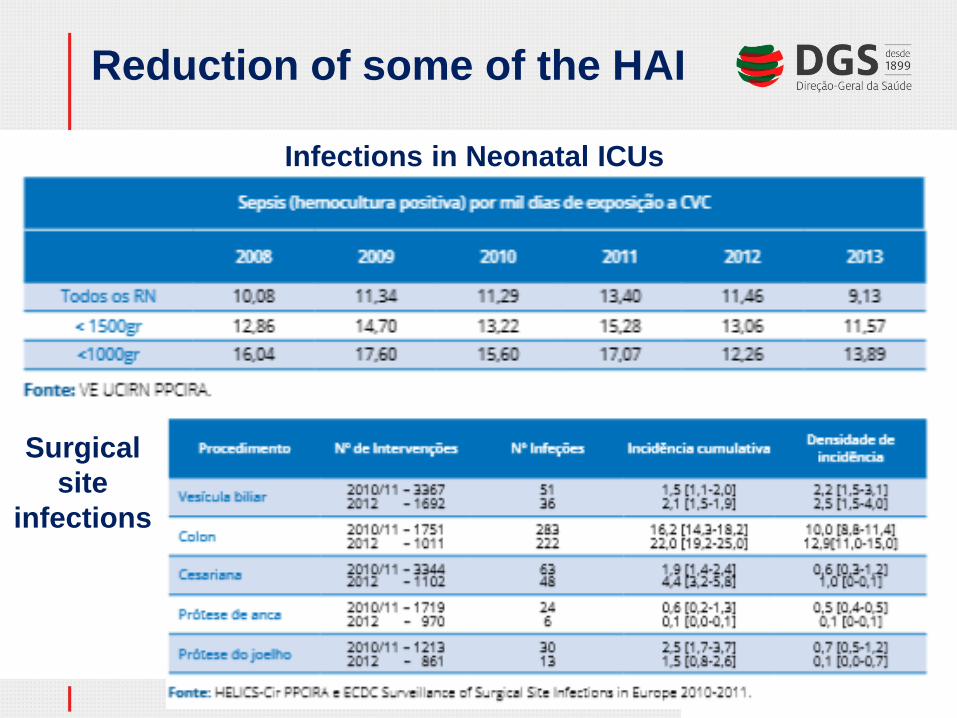
Reduction of some of the HAI
Infections in Neonatal ICUs
Surgical site
infections

HCAI in long term care institutions
GUIDELINES: - Standard
precautions - Prevention of
surgical site infection
- Prevention of chronic wound infection
Next months……..
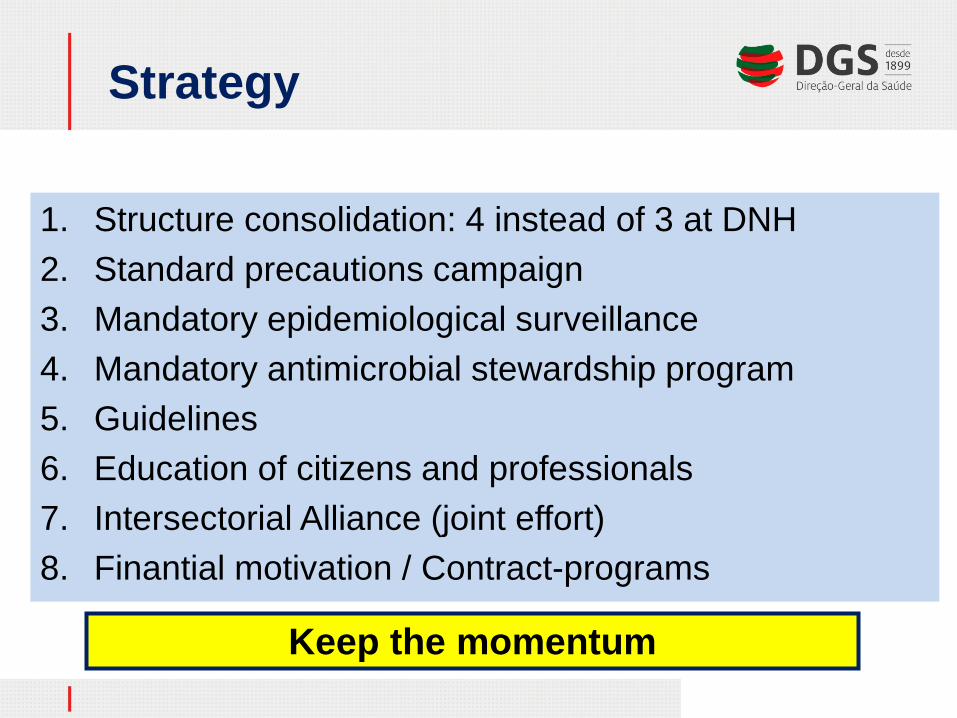
Strategy
1. Structure consolidation: 4 instead of 3 at DNH 2. Standard precautions campaign 3. Mandatory epidemiological surveillance 4. Mandatory antimicrobial stewardship program 5. Guidelines 6. Education of citizens and professionals 7. Intersectorial Alliance (joint effort) 8. Finantial motivation / Contract-programs
Keep the momentum

PPCIRA institutional assessment
1. To have PPCIRA-Local Coordinating Group in accordance with 15423/2013 law 2. To participate in the epidemiollogical surveillance of antimicrobial resisitance,
through LCG and Microbiology Labs. 3. To participate in the 4 epidemiological surveillance programs on HAI 4. To analyse institution’s data on antimicrobial consumption,
relating them to antimicrobial resistance patterns 5. To have a Antimicrobial Stewardship Program 6. To participate in the Standard Precautions Campaign 7. To reduce mean duration of antibiotic treatment course 8. To reduce to zero surgical antibiotic prophylaxis > 24h 9. To increase antibiotic free days 10. To reduce carbapenem consumption in hospitals 11. To reduce % patients that acquire colonization or infection by MDR in hospitals 12. To reduce hospital MRSA rate 13. To avoid increase in CRE rate 14. To reduce % of patients on antibiotic treatment for chronic wound 15. To reduce quinolone consumption in the ambulatory setting
