ncl joint commissioning committee thursday, 7 …...ncl joint commissioning committee thursday, 7...
TRANSCRIPT

NCL Joint Commissioning Committee Thursday, 7 February 2019 2.30pm – 4.30pm Committee Room 1 Hendon Town Hall The Burroughs London NW4 4BG
Voting Members
Ms Karen Trew (Chair) Governing Body Vice Chair and Lay Member, Enfield CCG
Dr Mo Abedi Governing Body Chair, Enfield CCG Dr Charlotte Benjamin Governing Body Chair, Barnet CCG Ms Sorrel Brookes Governing Body Lay Member, Islington CCG Dr Peter Christian Governing Body Chair, Haringey CCG Ms Kathy Elliott Governing Body Lay Member, Camden CCG Mr Simon Goodwin NCL Chief Finance Officer, Barnet, Camden, Enfield,
Haringey and Islington CCGs Dr Neel Gupta Governing Body Chair, Camden CCG Ms Catherine Herman Governing Body Lay Member, Haringey CCG Dr Fawad Hussain Governing Body Secondary Care Clinician, Enfield CCG Ms Helen Pettersen NCL Accountable Officer, Barnet, Camden, Enfield,
Haringey and Islington CCGs Dr Jo Sauvage Governing Body Chair, Islington CCG Ms Sharon Seber Nurse Representative, Haringey CCG Mr Dominic Tkaczyk Governing Body Lay Member, Barnet CCG
Non-Voting Members Ms Sarah James Councillor, Haringey London Borough Council Ms Parin Bahl Healthwatch Enfield Ms Janet Burgess Councillor, Islington London Borough Council Ms Alev Cazimoglu Councillor, Enfield London Borough Council Mr Richard Cornelius Councillor, Barnet London Borough Council Dr Tamara Djuretic Director of Public Health, Public Health Barnet Ms Sharon Grant Healthwatch Haringey Attendees Ms Aimee Fairbairns Director of Quality and Clinical Services, Enfield CCG Ms Eileen Fiori NCL Director of Acute Commissioning Mr Will Huxter NCL Director of Strategy Mr Ed Nkrumah NCL Director of Performance Mr Ian Porter Director of Corporate Services, NCL CCGs Ms Sarah Rothenberg NCL PoD Director, North East London Commissioning
Support Unit Mr Paul Sinden NCL Director of Performance, Planning and Primary
Care Apologies Ms Pat Callaghan Councillor, Camden London Borough Council Mr Adam Sharples Governing Body Lay Member, Haringey CCG Minutes
Mr Steve Beeho Board Secretary, Haringey CCG
1
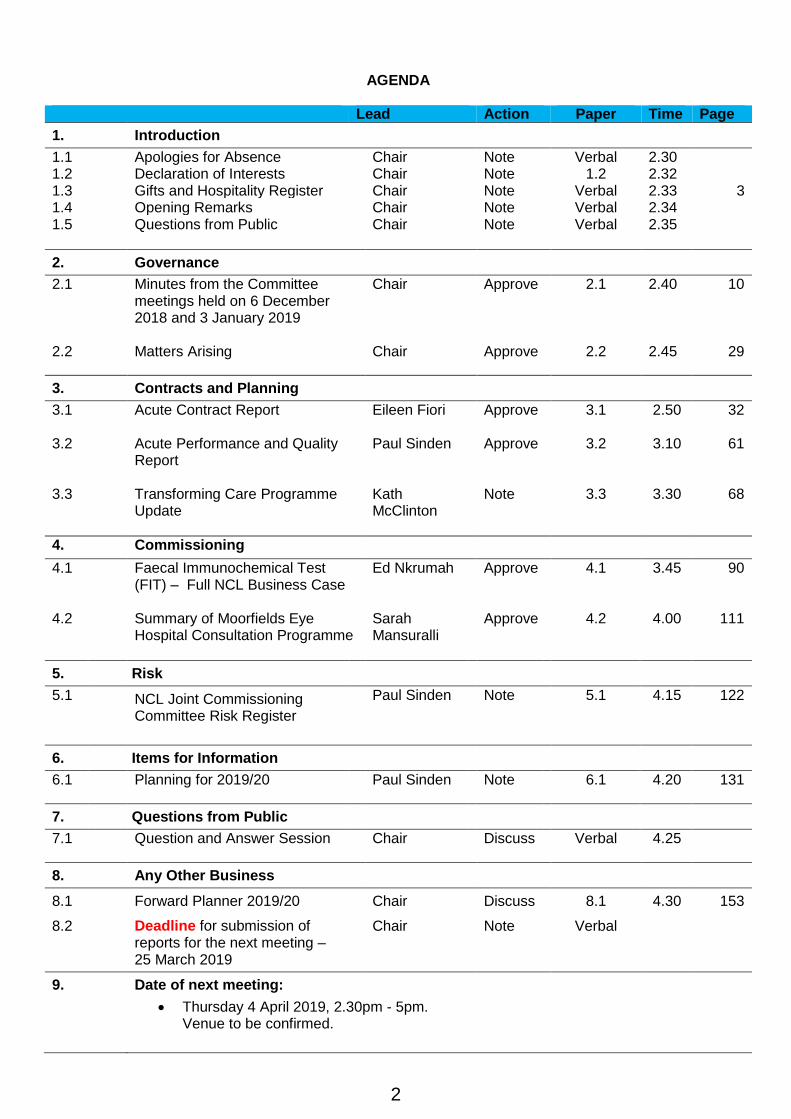
AGENDA
Lead Action Paper Time Page
1. Introduction
1.1 Apologies for Absence Chair Note Verbal 2.30 1.2 Declaration of Interests Chair Note 1.2 2.32 1.3 Gifts and Hospitality Register Chair Note Verbal 2.33 3 1.4 Opening Remarks Chair Note Verbal 2.34 1.5 Questions from Public
Chair Note Verbal 2.35
2. Governance
2.1
Minutes from the Committee meetings held on 6 December 2018 and 3 January 2019
Chair
Approve
2.1
2.40
10
2.2 Matters Arising Chair Approve 2.2 2.45 29
3. Contracts and Planning
3.1 Acute Contract Report Eileen Fiori Approve
3.1 2.50 32
3.2 Acute Performance and Quality Report
Paul Sinden Approve 3.2 3.10 61
3.3 Transforming Care Programme Update
Kath McClinton
Note 3.3 3.30 68
4. Commissioning
4.1 Faecal Immunochemical Test (FIT) – Full NCL Business Case
Ed Nkrumah Approve 4.1
3.45 90
4.2 Summary of Moorfields Eye Hospital Consultation Programme
Sarah Mansuralli
Approve 4.2 4.00 111
5. Risk
5.1 NCL Joint Commissioning Committee Risk Register
Paul Sinden Note 5.1 4.15 122
6. Items for Information
6.1 Planning for 2019/20 Paul Sinden Note 6.1 4.20 131
7. Questions from Public
7.1 Question and Answer Session Chair Discuss Verbal 4.25
8. Any Other Business
8.1 Forward Planner 2019/20 Chair Discuss 8.1 4.30 153
8.2 Deadline for submission of reports for the next meeting – 25 March 2019
Chair Note Verbal
9. Date of next meeting:
Thursday 4 April 2019, 2.30pm - 5pm. Venue to be confirmed.
2

From To
Fin
an
cia
l In
tere
sts
No
n-F
ina
nc
ial
Pro
fes
sio
na
l
Inte
res
ts
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
sts
East Enfield Medical
Practice - GP PracticeYes Yes Direct GP Principal Nov-02 current 30.8.18
Evergreen Surgery
Limited - GP PracticeYes Yes Direct Director/Shareholder 2004 current 30.8.18
Brick Lane Surgery Yes Yes Direct Partner 2013 current 30.8.18
Brick Lane Surgery Yes Indirect Wife is a GP / Principal Jul-17 current 30.8.18
Medicare Medical
services LLP - Runs walk
in centre at Evergreen
Yes Yes Direct Director/Shareholder 2003 current 30.8.18
DM786 Limited
Property management
company
Yes Yes Direct Director 2002 current 30.8.18
DM786 Limited
Property management
company
Yes Yes Indirect Wife is a director, mother and
children are shareholders 2002 current 30.8.18
DM786 Health Ltd -
Health Consultancy (not
actively trading)
Yes Yes Direct Director 2012 current 30.8.18
DM786 Health Ltd -
Health Consultancy (not
actively trading)
Yes Yes Indirect Wife is a director, mother and
children are shareholders 2012 current 30.8.18
Prime Point Limited
Primary care medical
services provider
Yes Yes Direct Director / Shareholder 2012 current 30.8.18
Enfield Health
Partnership Limited,
Provider of community
gynaecology service
Yes Yes Direct Shareholder 2010 current 30.8.18
Enfield Healthcare
Alliance Ltd – runs
Chalfont Rd and
Boundary Court GP
Practices
Yes Yes Direct Shareholder 2014 current 30.8.18
South East Locality
Access hub Yes Indirect Wife is a locum GP 2016 current 30.8.18
Enfield Locum GPs
Yes Indirect Wife works in Enfield as a locum GP 2016 current 30.8.18
St George's Medical
Centre Yes Yes Direct GP Partner 1.3.17 30.10.17
Mo
Elected GP Representative and Governing Body Chair-Elect, Barnet CCG Charlotte Benjamin
Chair of Enfield CCG Governing Body
Chair of Enfield CCG Clinical Commissioning Group Abedi
Update Date
declared
Nature of Interest
Declared Interest-
(Name of the
organisation and
nature of business)
First NameCurrent position (s) held- i.e. Governing Body,
Member practice, Employee or other
Date of InterestType of Interest
Is the interest
direct or
indirect?
Second
Name
Voting Members
3

JFS, Brent Yes Direct School Governor 1.3.17 30.10.17
Chelsea and
Westminster NHS FT Yes Indirect Husband is clinical lead for ENT 1.3.17 30.10.17
Sorrel Brookes
Lay Vice Chair, Islington CCG
Member of Governing Body, Islington CCG
Strategy & Finance Committee, Islington CCG
PPP Committee, Islington CCG
Audit Committee, Islington CCG
Remuneration Committee, Islington CCG
NCL Primary Care Committee in Common
Trustee of Help on Your
Doorstep.Direct
Help on Your Doorstep is a
contractor for Islington CCG.
I take no part in contracting
decisions.
23.8.18
Muswell Hill Practice Yes Direct Practice Partner 15.3.18 7.11.18Muswell Hill Practice is
a member of
Federated4Health, the
pan-Haringey
federation of GP
practices.
Yes Direct Practice Partner 15.3.18 7.11.18
Muswell Hill Practice is
a member of WISH -
Urgent Care Centre
provider at Whittington
Hospital.
Yes Direct Practice Partner 15.3.18 7.11.18
Muswell Hill Practice
provides anticoagulant
care to Haringey
residents under a
contract with the CCG.
Yes Direct Practice Partner 15.3.18 7.11.18
The Hospital Saturday
Fund - a charity which
gives money to health
related issues.
Yes Direct Member 15.3.18 7.11.18
The Hospital Saturday
Fund - a charity which
gives money to health
related issues.
Yes Indirect (wife) Patron 15.3.18 7.11.18
The Lost Chord Charity -
organises interactive
musical sessions for
people with dementia
in residential homes.
Yes Indirect (wife) Patron 15.3.18 7.11.18
Haringey Health
Connected, the
federation of west
Haringey GP practices
Yes Indirect Practice Manager is Finance
Manager. 15.3.18 7.11.18
Salmons Brook
residents EdmontonYes Yes Direct
Non-Executive Director (flat owned
within the complex)2013 current 2.11.18
Elected GP Representative and Governing Body Chair-Elect, Barnet CCG Charlotte Benjamin
Peter Christian
Haringey CCG Chair, West GP Lead
GP Partner, Muswell Hill Practice
Member, Clinical Cabinet, Haringey CCG
Member, Health and Wellbeing Board
Member, Collaboration Board
Member, Remuneration Committee, Haringey CCG
Member, STP Clinical Cabinet and Transformation Board
Angela Dempsey Nurse Representative, Enfield CCG Governing Body
Chair, Quality and Safety Committee, Enfield CCG
Member, Clinical Commissioning Committee
4
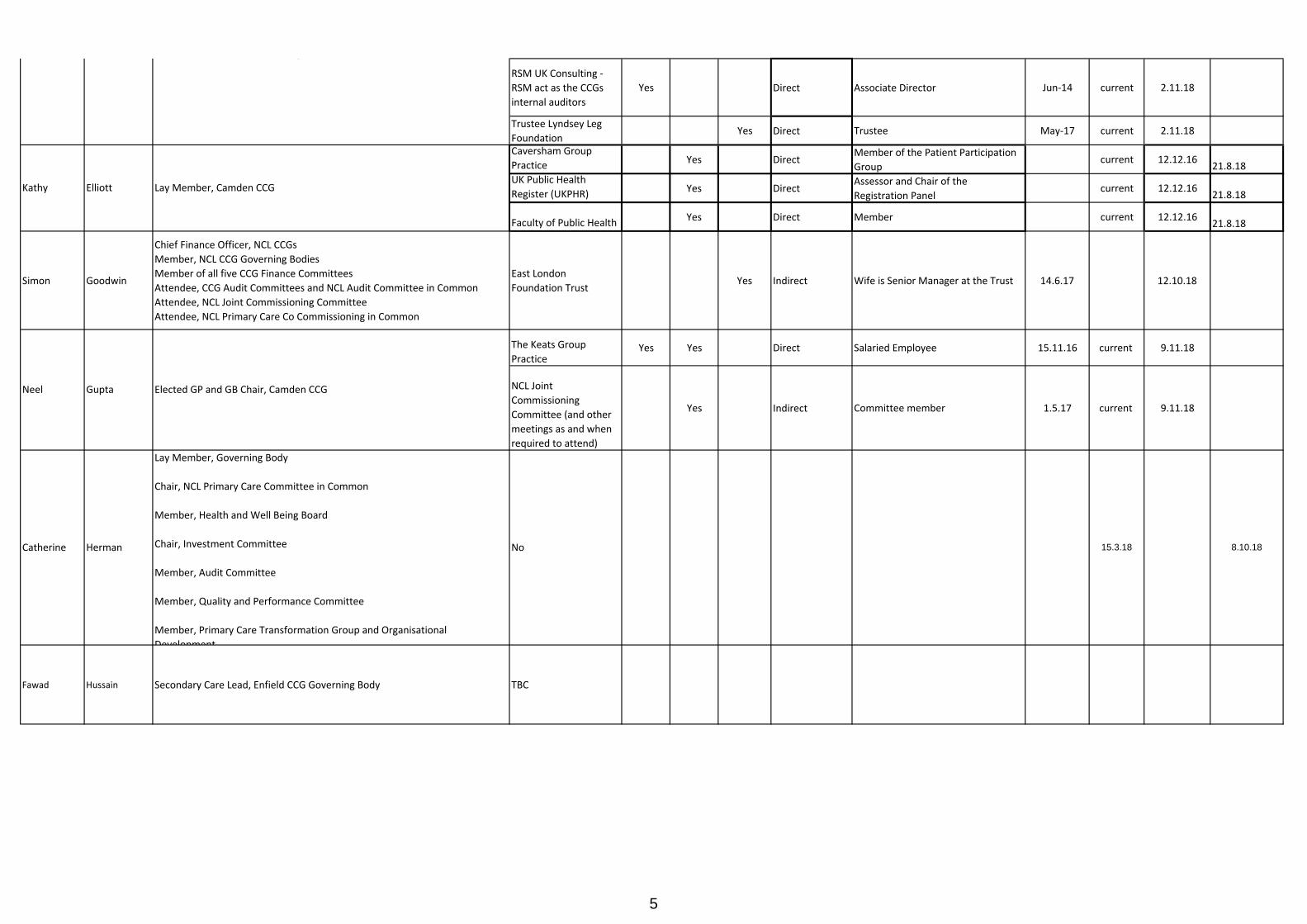
RSM UK Consulting -
RSM act as the CCGs
internal auditors
Yes Direct Associate Director Jun-14 current 2.11.18
Trustee Lyndsey Leg
Foundation Yes Direct Trustee May-17 current 2.11.18
Caversham Group
Practice Yes Direct
Member of the Patient Participation
Groupcurrent 12.12.16
21.8.18UK Public Health
Register (UKPHR) Yes Direct
Assessor and Chair of the
Registration Panelcurrent 12.12.16
21.8.18
Faculty of Public Health Yes Direct Member current 12.12.16
21.8.18
Simon Goodwin
Chief Finance Officer, NCL CCGs
Member, NCL CCG Governing Bodies
Member of all five CCG Finance Committees
Attendee, CCG Audit Committees and NCL Audit Committee in Common
Attendee, NCL Joint Commissioning Committee
Attendee, NCL Primary Care Co Commissioning in Common
East London
Foundation Trust Yes Indirect Wife is Senior Manager at the Trust 14.6.17 12.10.18
The Keats Group
PracticeYes Yes Direct Salaried Employee 15.11.16 current 9.11.18
NCL Joint
Commissioning
Committee (and other
meetings as and when
required to attend)
Yes Indirect Committee member 1.5.17 current 9.11.18
Fawad Hussain Secondary Care Lead, Enfield CCG Governing Body TBC
Neel Gupta Elected GP and GB Chair, Camden CCG
Kathy Elliott Lay Member, Camden CCG
Angela Dempsey Nurse Representative, Enfield CCG Governing Body
Chair, Quality and Safety Committee, Enfield CCG
Member, Clinical Commissioning Committee
Catherine Herman
Lay Member, Governing Body
Chair, NCL Primary Care Committee in Common
Member, Health and Well Being Board
Chair, Investment Committee
Member, Audit Committee
Member, Quality and Performance Committee
Member, Primary Care Transformation Group and Organisational
Development
No 15.3.18 8.10.18
5
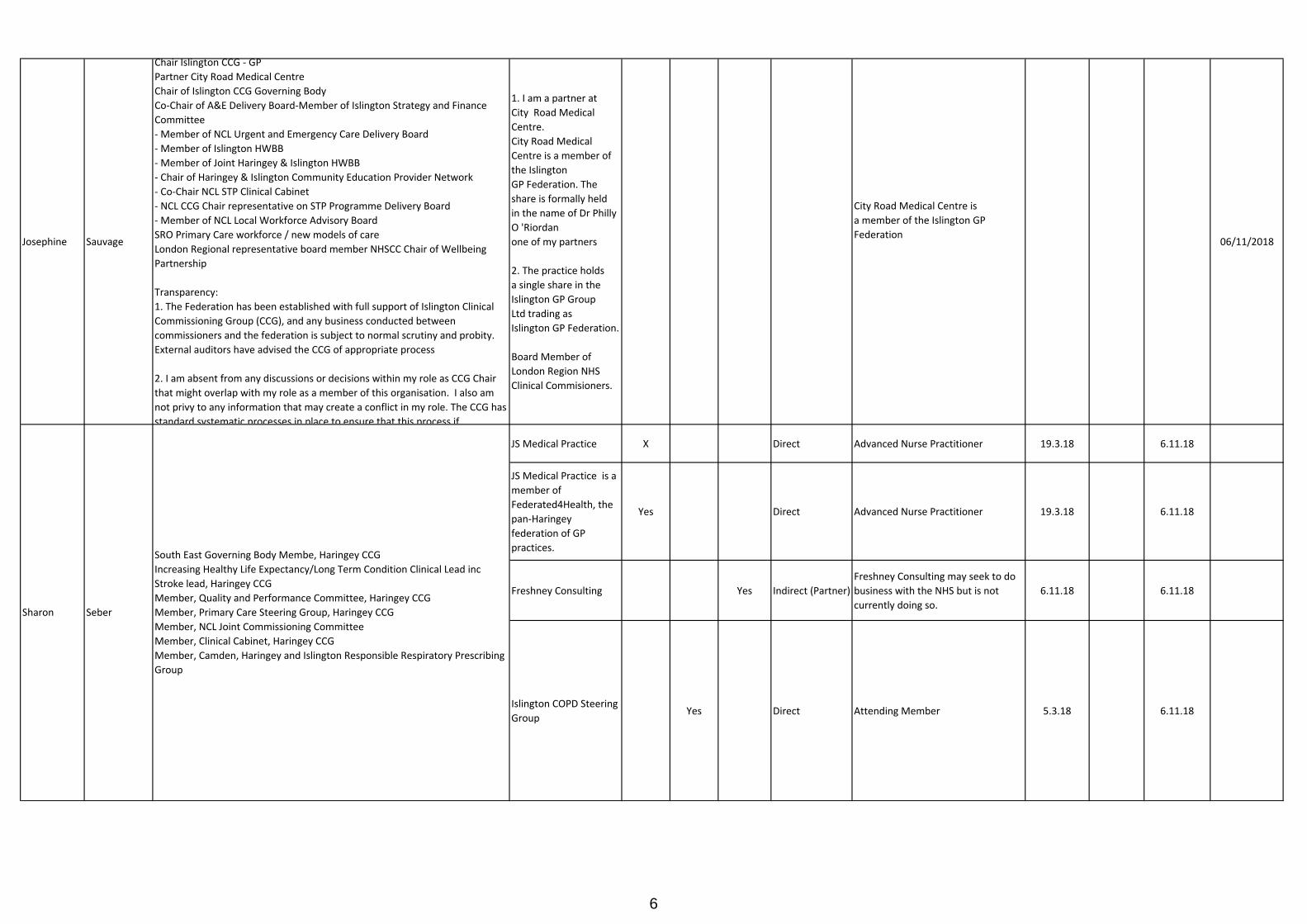
Josephine Sauvage
Chair Islington CCG - GP
Partner City Road Medical Centre
Chair of Islington CCG Governing Body
Co-Chair of A&E Delivery Board-Member of Islington Strategy and Finance
Committee
- Member of NCL Urgent and Emergency Care Delivery Board
- Member of Islington HWBB
- Member of Joint Haringey & Islington HWBB
- Chair of Haringey & Islington Community Education Provider Network
- Co-Chair NCL STP Clinical Cabinet
- NCL CCG Chair representative on STP Programme Delivery Board
- Member of NCL Local Workforce Advisory Board
SRO Primary Care workforce / new models of care
London Regional representative board member NHSCC Chair of Wellbeing
Partnership
Transparency:
1. The Federation has been established with full support of Islington Clinical
Commissioning Group (CCG), and any business conducted between
commissioners and the federation is subject to normal scrutiny and probity.
External auditors have advised the CCG of appropriate process
2. I am absent from any discussions or decisions within my role as CCG Chair
that might overlap with my role as a member of this organisation. I also am
not privy to any information that may create a conflict in my role. The CCG has
standard systematic processes in place to ensure that this process if
1. I am a partner at
City Road Medical
Centre.
City Road Medical
Centre is a member of
the Islington
GP Federation. The
share is formally held
in the name of Dr Philly
O 'Riordan
one of my partners
2. The practice holds
a single share in the
Islington GP Group
Ltd trading as
Islington GP Federation.
Board Member of
London Region NHS
Clinical Commisioners.
City Road Medical Centre is
a member of the Islington GP
Federation06/11/2018
JS Medical Practice X Direct Advanced Nurse Practitioner 19.3.18 6.11.18
JS Medical Practice is a
member of
Federated4Health, the
pan-Haringey
federation of GP
practices.
Yes Direct Advanced Nurse Practitioner 19.3.18 6.11.18
Freshney Consulting Yes Indirect (Partner)
Freshney Consulting may seek to do
business with the NHS but is not
currently doing so.
6.11.18 6.11.18
Islington COPD Steering
Group Yes Direct Attending Member 5.3.18 6.11.18
Sharon Seber
South East Governing Body Membe, Haringey CCG
Increasing Healthy Life Expectancy/Long Term Condition Clinical Lead inc
Stroke lead, Haringey CCG
Member, Quality and Performance Committee, Haringey CCG
Member, Primary Care Steering Group, Haringey CCG
Member, NCL Joint Commissioning Committee
Member, Clinical Cabinet, Haringey CCG
Member, Camden, Haringey and Islington Responsible Respiratory Prescribing
Group
6

Money Advice Trust
(a national debt advice
charity)
Yes Direct Chair 01.07.16 8.10.18
Enfield CCG X Direct Member, Audit Committee 10.1.14 8.10.18
Headway East London (HEL)
Yes Direct
Treasurer to HEL, which provides
services to people with acquired
brain injury
1.6.18 17.10.18
Healthcare People
Management
Association Yes Direct Honorary Treasurer 1.10.18 17.10.18
Haringey CCG Yes Yes Direct Member of Haringey CCG Audit
CommitteeApr-13 current 31.10.18
NHS England Performer
List Decision Panel
(outside of North
Central London)
Yes Direct Chair of Panels Apr-13 current 31.10.18
Broxbourne School
HertfordshireYes Direct
Chair of the Governing Body
(previously Governing Body members
since Nov. 2004)
Jun-15 current 31.10.18
Wormley C of E Primary
School, HertfordshireYes Direct Chair of the Governing Body 2006 current 31.10.18
Lloyds Pharmacy
Clinical HomecareYes Indirect Son employed in operational role Apr-17 current 31.10.18
TkaczykDominic
Lay Vice Chair, Enfield CCG Governing Body
Lead for Governance and Audit, Enfield CCG
Member, Finance and Performance Committee, Enfield CCG
Member, Clinical Commissioning Committee, Enfield CCG
Member, Procurement Committee, Enfield CCG
TrewKaren
Non-Voting Members
Lay Member for Audit and Governance, Barnet CCG
Adam Sharples
Member, Governing Body, Haringey CCG
Chair, Audit Committee, Haringey CCG
Chair, NCL Audit Committee in Common
Chair, Remuneration Committee, Haringey CCG
Member, Strategy and Finance Committee, Haringey CCG
Member, Finance and Performance Partnership Board, Haringey CCG
Chair, IFR Panel, Haringey CCG
Member, NCL Joint Commissioning Committee
Member, Community Services Improvement Group
Member, CSU In-Housing Sub Group
Member, Employment and Health Working Group (run by Haringey Council)
Conflicts of interest Guardian, Haringey CCG
7

Parin Bahl Healthwatch representative, Enfield CCG Governing Body Enfield Healthwatch Yes Yes Direct
Chair: Healthwatch Enfield is run by a
Community Interest Company, called
Combining Opinions to Generate
Solutions CIC (COGS). COGS is
commissioned by the London
Borough of Enfield to provide the
statutory Healthwatch service for
Enfield. COGS also undertakes
commissioned work e.g. training or
engagement work.
2017 current 20.11.18 16.1.19
Islington Council Direct
Executive Member for Health &
Social Care & Deputy Leader of the
Council
26.10.17
The Advisory Group For
The Friendship
Network, Manor
Garden Welfare Trust
Direct Member 26.10.17
Unite Direct Member 26.10.17
Whittington Health NHS
TrustDirect Attendee at Board Meetings 1.3.18 28.3.18
Whittington Park
Community CentreDirect Trustee 26.10.17
Camden Council Direct
Cabinet member for Tackling Health
Inequality and Promoting
Independence
5.10.17 26.10.17
St Michael's Primary
SchoolDirect Governor 5.10.17 26.10.17
Unison Direct Member 5.10.17 26.10.17
Richard Cornelius Councillor, Barnet Council To be confirmed
Barnet Council Yes Direct DPH has a statutory duty to provide
‘core offer’ to Barnet CCG 3.5.18
Ravenscroft Medical
CentreYes Direct Patient 3.5.18
Public Voice CIC (a
Community Interest Yes Direct Chair of the Board 19.2.18 8.11.18
Healthwatch Haringey Yes Direct Chair, Steering Committee 19.2.18 8.11.18
Bernie Grant Arts
Centre Partnership Yes Direct Director 19.2.18 8.11.18
Bernie Grant Trust Yes Direct Director 8.11.18Independent Advisory
Group, Metropolitan
Police Haringey
Yes Direct Member 19.2.18 8.11.18
Parliamentary
researcher Yes Direct
Part-time-employment as a
Parliamentary Researcher on Health
issues for backbench Labour MP
19.2.18 8.11.18
London Borough of
Haringey Fairness
Commission
Yes Direct Member 8.11.18
Haringey Joint
Partnership Board Yes Direct Co-Chair 8.11.18
Consumers Association
(Which?)Yes Direct
Trustee and Director
(Unremunerated)19.2.18 8.11.18
Sarah James Councillor, Haringey Council To be confirmed
Tamara Djuretic Director of Public Health, Barnet Council
Councillor, Islington Council Burgess Janet
Councillor, Camden Council
Sharon Grant
Chair, Healthwatch Haringey
Haringey CCG Governing Body Observer (With Speaking Rights)
Callaghan Patricia
8

Eileen Fiori
Director of Acute Commissioning, NCL
Member, Senior Management Team
Attendee, Joint Commissioning Committee
No interests to declare. 6.10.18
NCL CCGs N/A N/A N/A N/AAcute Performance Management
Lead N/A N/A 12.10.18
NCL CCGs N/A N/A N/A N/A Cancer Commissioning Lead N/A N/A 12.10.18
NCL CCGs N/A N/A N/A N/A Assurance Lead N/A N/A 12.10.18
City and Hackney and
Waltham Forest MIND Yes Yes Direct
Trustee - the Charity has no interests
in NCL CCGs26.1.17 current 12.10.18
Ian Porter Director of Corporate Services, NCL NONE N/A N/A N/A N/A
Attends all 5 CCGs Governing Body
meetings, NCL Audit Committee in
Common and other meetings as and
when required.
N/A N/A 14.6.17 23.7.18
Sarah Rothenberg Acting PoD Director and Director of Finance, NELCSUAssociation of Jewish
Refugees Yes Direct
Finance Committee member (no
social care overlap in NHS role )29.11.18
Paul Sinden Director of Performance and Acute Commissioning, NCL NCL CCGs N/A N/A N/A N/A
Attends all 5 CCGs Governing Body
meetings, NCL Primary Care
Commissioning in Common.
N/A N/A 30.4.18
Attendees
Ed Nkrumah Director of Performance, NCL
9

1
NORTH CENTRAL LONDON (‘NCL’) JOINT COMMISSIONING COMMITEE Draft minutes of the meeting held in public on Thursday 6 December 2018, 2.30pm – 5pm
Council Chamber, Civic Centre, 255 High Road, Wood Green, London N22 8LE
Voting Members Present:
Ms Karen Trew (Chair) Governing Body Vice Chair and Lay Member, Enfield CCG
Dr Mo Abedi Governing Body Chair, Camden CCG
Dr Charlotte Benjamin Governing Body Chair-Elect, Barnet CCG
Ms Sorrel Brookes Governing Body Lay Member, Islington CCG
Dr Peter Christian Governing Body Chair, Haringey CCG
Ms Kathy Elliott (Vice Chair) Governing Body Lay Member, Camden CCG
Dr Debbie Frost Governing Body Chair, Barnet CCG
Mr Simon Goodwin NCL Chief Finance Officer, Barnet, Camden, Enfield, Haringey and Islington CCGs
Dr Neel Gupta Governing Body, Chair, Camden CCG
Ms Helen Pettersen Accountable Officer, Barnet, Camden, Enfield, Haringey and Islington CCGs
Dr Jo Sauvage Governing Body Chair, Islington CCG
Ms Catherine Herman Governing Body Lay Member, Haringey CCG
Mr Dominic Tkaczyk Governing Body Lay Member, Barnet CCG
Non-Voting Members Present:
Ms Sharon Grant Healthwatch Haringey
Ms Parin Bahl Healthwatch Enfield
Attendees:
Mr Paul Sinden NCL Director of Planning, Performance and Primary Care
Ms Eileen Fiori NCL Director of Acute Commissioning
Mr Ian Porter Director of Corporate Services, Barnet, Camden, Enfield, Haringey and Islington CCGs
Ms Jennie Williams Director of Nursing and Quality, Haringey CCG
Apologies:
Mr Adam Sharples Governing Body Lay Member, Haringey CCG
Ms Peray Ahmet Councillor, Haringey Council
Ms Janet Burgess Councillor, Islington Council
Ms Pat Callaghan Councillor, Camden Council
Ms Alev Cazimoglu Councillor, Enfield Council
Mr Richard Cornelius Councillor, Barnet Council
Ms Angela Dempsey Nurse Member, Enfield CCG
Ms Tamara Djuretic Director of Public Health, Barnet Council
Minutes
Mr Steve Beeho Board Secretary, Haringey CCG
1 Introduction
1.1 Apologies for absence
1.1.1
Apologies were received from Angela Dempsey, Sharon Seber, Adam Sharples (Catherine Herman attending), Tamara Djuretic, Peray Ahmet, Janet Burgess, Pat Callaghan, Alev Cazimoglu, and Richard Cornelius.
1.2 Declarations of Interests
10

2
1.2.1
There were no additional declarations of interests.
1.3 Declarations of gifts and hospitality
1.3.1
There were no declarations of gifts or hospitality offered or received.
1.4 Opening Remarks
1.4.1
The Chair welcomed everybody to the meeting, and noted that this would be last JCC meeting for Debbie Frost and Angela Dempsey as their Governing Body terms of office were coming to an end. The Committee thanked them both for their contribution to the work of the JCC, highlighting that Debbie Frost had been the first chair of the Committee.
1.5 Questions from the public
1.5.1
There were no questions from the public.
2. Governance
2.1 Minutes of Committee Meeting on 4 October 2018
2.1.1
The Committee APPROVED the minutes of the meeting as an accurate record, subject to the wording “This forecast also incorporated a range of non-acute activity” in the penultimate bullet point of section 3.1.3 being amended to “This forecast also incorporated a range of non-NCL activity”.
2.3 Action Log
2.3.1 2.3.2 2.3.3
The Committee reviewed the action log. The majority of the actions had been discharged, with three open actions due to be closed at the next meeting in February. Paul Sinden confirmed with regards to the overdue action to move to a single acute contract and single acute performance and quality report that will be used by the JCC and individual CCGs that this had now been trialled in Enfield, Haringey and Islington and would be implemented at the next JCC meeting. The Committee NOTED the action log.
3. Contracts and Planning
3.1 Acute Commissioning Report
3.1.1
Eileen Fiori introduced the month seven report, highlighting the following points:
The overall forecast outturn on all acute providers was £1,246m, against an annual plan of £1,206m;
Year-to-date over-performance was £22.1m and forecast outturn over-performance was £45.6m against CCG financial plans for the 4 main NCL acute providers. This represented an £8.4m favourable movement from the previous month’s outturn due to an increased yield from claims and challenges supported by external validation;
CCGs were reporting £3m over-performance on acute contracts outside NCL, a £2.4m adverse movement from the previous month;
11

3
3.1.2 3.1.3 3.1.4 3.1.5
For the year-to-date £19.9m (65%) of the planned £30.9m QIPP had been delivered. The forecast outturn position was £43.4m delivery, against a plan of £64.5m (67%);
The increase in the number of A&E attendances converted into hospital admissions, particularly at Royal Free London and NMUH, was under investigation supported by forthcoming clinical audits;
Elective care pathways service developments for Clinical Advice and Guidance (CAG) and tele-dermatology schemes had now been introduced (although behind schedule), following finalisation of respective service specifications and payment mechanisms. The current Royal Free London tele-dermatology contract would run alongside the new NCL service specification until the end of the financial year, whilst the Trust worked through the changes to the pathway required to introduce the new service model;
Actions highlighted in the acute contract report were followed up through contact meetings with providers, and progress regularly monitored by the NCL Contract Delivery Group, NCL Activity Review Group and A&E Delivery Boards;
Clinicians had been given advance notice by the Royal Free London of the cancellation of some outpatient appointments as a result of the implementing a new Electronic Patient Record system and these appointments were being rescheduled.
In response to the paper Committee members made the following comments:
The Committee found the new report format helpful;
As the tele-dermatology pilot at Royal Free London would be continuing, Barnet and Enfield residents could also be referred into the new tele-dermatology service run by the other NCL acute providers;
Clarification was sought as to whether the reported 3% increase in A&E attendance was largely attributable to demographic changes and/or repeat attenders. SDK work to validate activity would inform this and be included in future reports;
Any discussions with providers about year-end settlements, both Royal Free London and NMUH had expressed an interest, should only be negotiated within clear parameters. Any proposals would be brought back to CCGs for approval and would take into account the SDK report into changes in counting and coding by providers;
Work was underway to harmonise QIPP reporting, and estimates of QIPP delivery, across the CCGs. This would respond to Committee questions on reported QIPP delivery in areas of activity with an increasing underlying trend, and the acceleration of QIPP delivery in the final quarter of the financial year;
Detailed implementation plans were in place for all QIPP schemes and further information would be provided about the impact that the STP direct access workstream was having on planned care activity;
The Committee NOTED the Acute Commissioning Report. ACTION: Will Huxter to provide an update on what is being done to make QIPP reporting consistent across NCL. ACTION: Will Huxter to provide an update on the overall planned care position, including the impact of the STP direct access workstream.
3.2 Acute Performance and Quality Report
3.2.1
Paul Sinden introduced the report, highlighting the following key points:
12

4
3.2.2 3.2.3
Three Never Events were reported across NCL acute providers in September 2018 and were being investigated by each Trust in accordance with the Serious Incident procedure
Following the submission of each A&E Delivery Board Winter Resilience Plans, a series of winter system stocktakes had been held with NHS England and NHS Improvement to gain assurance that the system has the capacity to meet the NHS Constitution targets over the winter, and with both hospital and community capacity in place to meet winter surges in demand for non-elective pathways;
NMUH system A&E performance continued to show improvement compared to the previous year, whereas performance at UCLH remained below target. The Royal Free and Whittington Health had also missed their planned performance improvement trajectories. Recovery plans were in place for all A&E Delivery Boards;
Reducing the number of long-stay patients in hospital beds remained a priority, with NMUH and Whittington Health both on track to achieve a 25% reduction, whilst the position at UCLH and the Royal Free was more challenging;
There had been a decline in the aggregate performance of NCL providers against the 62-day cancer waiting time operational standard. However, it was anticipated that the overall target will be recovered by February 2018, with the prostate pathway being the key challenge to delivering treatment within the standard;
Overall, NCL CCGs did not meet the national referral to treatment (RTT) 18 week NHS Constitutional standard, primarily due to the reported positions at UCLH and the Royal Free London. An NCL RTT Delivery Group has been established to focus on maintaining waiting lists within March 2018 levels through mutual aid across providers, the implementation of STP initiatives and insourcing/outsourcing capacity;
Ambulance response times continued to be differential within NCL, with Barnet and Enfield experiencing longer response times. NCL CCGs were addressing this with London Ambulance Service (LAS) through increased ambulance capacity in Barnet, Enfield and Haringey, as well as the introduction of new rosters. LAS would also be curtailing “auto-dispatch”, which should ensure that more ambulances were retained in their originating boroughs;
The LCW Unscheduled Care Collaborative was continuing to meet the local specification and national key performance indicators within the NCL contract, with the service (supported by earlier in-year investment) being more resilient than elsewhere nationally.
In response to the report the Committee made the following comments:
It was imperative that the recovery plan for the prostate pathway focused on the pathway as a whole and not just the hospital element, and this would be fed back at the NCEL Cancer Performance Improvement Task and Finish group meeting the following day. The high volume of surgery being carried out at UCLH would be one of the items under discussion;
The commitment among Trusts to provide mutual support in aid of the RTT target was welcomed but assurance was sought that their focus would continue to be on patients, rather than internal processes. The terms of reference for the NCL group required and collaborative work to be in the best interests of patients;
A request that future versions of the report placed a greater emphasis on patient experience.
The Committee NOTED the Acute Performance and Quality Report.
13

5
4. Commissioning
4.1 Adult Elective Orthopaedic Services Review
4.1.1 4.1.2
Professor Haddad provided the background to the report, noting the following points:
The JCC had given approval in February 2018 to develop the clinical case for change for adult elective orthopaedic services;
Following publication of the draft case for change in August 2018 a comprehensive engagement programme had been undertaken with providers (including secondary care orthopaedic teams), CCGs and patients;
The engagement programme had been informed by a desktop Equality Impact Assessment;
The evolving model proposed an increased co-location of orthopaedic expertise, reduction in unwarranted variations in care and outcomes, and was mindful of clinical interdependencies including musculo-skeletal services, spinal surgery, paediatric orthopaedics and trauma;
Alongside the engagement activities, the Adult Elective Orthopaedic Services Review Group held five clinical design workshops between July and November 2018 to discuss the principles that should be used to develop the clinical model. These workshops helped to crystallise a number of design principles for the new service model and next steps, which it was believed would see increased partnership working across North Central London, resulting in less pressure on beds and fewer cancellations of procedures;
The paper requested a mandate to establish a clinical orthopaedic network for North Central London working alongside the existing musculo-skeletal (MSK) workstream.
Anna Stewart then provided an overview of the engagement process, the evaluation of which had been supported by Verve Communications, highlighting:
Over 500 stakeholders had been contacted through the engagement process, with contact driven by the equality baseline assessment;
There was considerable overlap between the feedback from each group, particularly in terms of welcoming the proposed creation of elective orthopaedic centre(s), the potential to improve patient experience and clinical outcomes and the opportunity for extensive consultation and engagement;
There was a desire for the drivers for change to be articulated clearly in the consultation, and a strong emphasis on travel times and the importance of sustainability;
Enfield Healthwatch were thanked for the additional engagement work that they carried out to support the overall process;
A positive session had been held with the Joint Health Overview and Scrutiny Committee the previous week. The Committee, in line with the engagement themes, had a strong focus on transport and travel times.
14

6
4.1.3 4.1.4 4.1.5 4.1.6 4.1.7
Rob Hurd noted that the case for change was based on national and international evidence, and had the aim to improve access and outcomes and reduce cancellations (improve resilience to winter pressures). The design principles developed had been supported by the outcome of the engagement process. Building on the above, on 3 January 2019, the Committee would receive an updated governance framework for the review for approval. The framework would reflect the next phase of the review which would require a commissioning led approach (options appraisal for future service provision accruing form the engagement process) from the collaborative approach used to establish the design principles. An additional formal Committee meeting would be held on 3 January 2019 to accommodate the required timings for the adult elective orthopaedic services review. The Committee then discussed the report, making the following points:
The evidence-based approach to the review and supporting engagement process were welcomed;
Regular discussions had been held with Orthopaedic Consultants from all providers during the engagement process and they had accepted and supported the case for change. Engagement would need to be maintained as the detail of service options was developed;
Building on the robust engagement process to date, on-going engagement would need to continue to be cognisant of the equality baseline assessment and reach out to hard to reach groups;
The need to consider service interdependencies that sat outside of the scope of the review including musculo-skeletal services, trauma, paediatric orthopaedic services, and spinal surgery, and build on examples of service models used elsewhere;
An offer was made to bring an update on services for Children and Young People, as a service interdependence, to a future meeting;
Noted that meetings had been held with the Lead Members for Health in each of the 5 Local Authorities during the engagement process;
Given the need for an additional formal Committee and the timing (3 January 2019) it was suggested that publicity for the meeting be maximised and personal invitations to the meeting on 3 January 2019 be sent to the five Councillor representatives on the Committee.
The Joint Commissioning Committee:
NOTED the themes and feedback accruing from the extensive engagement exercise having provided guidance on the areas requiring most attention;
ACCEPTED the emerging design principles and six areas of next steps emerging from the clinical design workshops;
AGREED that the Review Group should be given the mandate to work within the Sustainability and Transformation Plan (STP) system and with the existing
15

7
4.1.8
musculo-skeletal (MSK) workstream to explore how a clinical orthopaedic network could be developed;
AGREED to bring back for approval in January 2019 options for the next steps and governance of the review in the second stage.
ACTION: Steve Beeho to ensure that the January 2019 meeting is well promoted and that invitations to the meeting are sent to the Councillor representatives on the Committee.
4.2 Procedures of Limited Clinical Effectiveness 4.2.1 4.2.2
Nick Dattani provided the background to the amended policy, highlighting the following points:
NCL CCGs currently have differential policies relating to procedures of limited clinical effectiveness (PoLCE) and the aim was to remove these differentials;
A clinically-led review had therefore been undertaken, involving primary and secondary care, to reduce ambiguity in the current policy issued in July 2015;
The Committee was being asked to approve updates to the policy in 35 areas that either provided greater clarity on application of the existing policy, incorporated new evidence or guidance or incorporated areas already adopted by Enfield CCG through the adherence to evidence-based medicine programme following engagement with the public;
The CCGs had actively engaged with providers across NCL and taken their feedback into account;
The updates were informed by an equality impact assessment;
This represented a ‘living’ policy and would incorporate future guidance as appropriate;
Once approved, the new policy would be active across North Central London CCGs and a paper setting out the detailed implementation of this across the CCGs and Providers will follow for the committee in January 2019.
The Committee discussed the proposed changes, making the following points:
The clinically-led review and evidence-based approach was welcomed;
Renaming the policy should be considered as various titles were being used – the national programme was titled Evidence-Based Interventions, whereas the London programme was called Choosing Wisely. In addition the NCL branding could cause concern about intent locally;
Assurance was sought that each CCG will carry out the relevant data protection work;
The importance of ensuring that the policy was consistently applied and evidence based across NCL to avoid any postcode related inequalities, including roll-out of the earlier Enfield process to the rest of NCL. The latter was the case as the Enfield work was incorporated into the NCL policy update;
Agreed to share the Equalities Impact Assessment with Healthwatch, along with sharing these with the NCL Joint Health Oversight Scrutiny Committee;
Clarification was sought on whether the list of procedures was finite and if not, what the process was for making additions to the list. The policy would be a
16

8
4.2.3 4.2.4 4.2.5
“live” document and would change in the light of updated evidence. Updates would be brought to the Joint Commissioning Committee for approval;
Clarification was also requested on whether there is a right of appeal under the policy. This was in place through the Individual Funding Request process that could be initiated by a GP or Consultant providing care for the individual;
The need to stress that the policy focused on clinical effectiveness, evidence, and using public money cost-effectively and was not driven by funding problems;
Clarity was sought on the NCL Joint Health Overview Scrutiny Committee (JHOSC) view of consultation requirements for changes to the policy;
It was agreed that a clear local communications plan (roadshows, for example), would be organised to ensure that practitioners were aware of the implications of the policy, and that implications of the policy were therefore reviewed regularly across the five boroughs.
The Joint Commissioning Committee:
APPROVED the proposed updates to the policy listed in the paper;
AGREED that the POLCE policy would be implemented across North Central London CCGs, with a paper coming to the next meeting on 3 January 2019 setting out the proposed detailed implementation plan.
ACTION: Richard Dale to share the Equalities Impact Assessment with Healthwatch. ACTION: Richard Dale to confirm the NCL Joint Health Overview Scrutiny Committee JHOSC’s position on whether formal consultation is required.
5. Risk
5.1 NCL Joint Commissioning Committee Risk Register
5.1.1 5.1.2 5.1.3 5.1.4
Paul Sinden introduced the JCC Risk Register which had been developed to align with the NCL risk reporting format and to allow a greater focus on risks rated 12 and above. The risk report now included a risk tracker and risk heat map. It was recommended that risks 16, 17 and 19 should be closed as they will be picked up through the NCL Sustainability and Transformation Plan. It was also recommended that risks 8 and 17 should be closed to allow the JCC to focus on the most material risks within its remit. The Committee:
NOTED the report and the updates to the NCL JCC risk register
NOTED the changes to the NCL JCC risk register proposed for February 2019.
6. Items for Information
6.1 CCG Finance Report - Month 7
17

9
6.1.1 6.1.2 6.1.3
Simon Goodwin introduced the Finance Report providing an overview of the financial position for the five NCL CCGs as at month 7:
All NCL CCGs were reporting forecast year-end outturn to plan, with the exception of Enfield CCG;
The reported position identified £46m net risk across the CCGs, with only Islington having a balance of opportunities and risks impacting on the year-end position. Underlying risks had been reported consistently to NHS England throughout the year;
The underlying position for NCL CCGs was a recurrent gap of £38.1m, making the financial challenge in 2019/20 at least commensurate to the challenge in 2018/19.
The following points were then made in the Committee feedback to the report:
Enfield CCG starting point for the current financial year was more challenging than for the other NCL CCGs due greater exposure to financially challenged Trusts and having less balance sheet flexibility given prior year financial pressures;
CCG actions and recovery plans were considered by respective Strategy and Finance Committees, and more high-level updates provided at Governing Body meetings;
Although all London STP areas contained CCGs with financial difficulties, NCL was in the unusual position of only having one CCG with a possibility of a surplus position;
To assist with planning and financial forecasts there was now a greater commonality of reporting and risk assessment of QIPP delivery across the CCGs, with this being followed up in respective Strategy and Finance Committees;
£38m of the £46m net risks identified to CCG reported outturn positions fell within the remit of the Committee, as covered in greater detail in the Acute Contract Report (item 3.1).
The Committee NOTED the NCL CCGs’ Financial Position as at month 7.
7. Questions from Public
7.1 Question and Answer Session
7.1.1
There were no questions from the public.
8. Any Other Business
8.1 Forward Planner 2018/19
8.1.1
The Committee NOTED the Forward Planner.
8.2 Deadline for Submission of Reports
8.2.1
The Committee NOTED that reports for the JCC meeting on 7 February 2019 should be sent to Paul Sinden by 28 January 2019.
8.3 Debbie Frost
8.3.1
Debbie Frost commented on the development of the Committee over the past two years and wished Committee members all the best for the future.
9. Date of Next Meeting
18

10
9.1
The next Committee meeting would be on 3 January 2019, with the planned Seminar taking place immediately afterwards.
19

1
NORTH CENTRAL LONDON (‘NCL’) JOINT COMMISSIONING COMMITEE Draft minutes of the meeting held in public on Thursday 3 January 2019, 15:00-16:30
Seminar Room 2, Resource for London, 356 Holloway Road, London N7 6PA
Voting Members Present:
Ms Karen Trew (Chair) Governing Body Vice Chair and Lay Member, Enfield CCG
Dr Mo Abedi Governing Body Chair, Enfield CCG
Dr Charlotte Benjamin Governing Body Member, Barnet CCG
Ms Sorrel Brookes Governing Body Lay Member, Islington CCG
Dr Peter Christian Governing Body Chair, Haringey CCG
Ms Kathy Elliott (Vice Chair) Governing Body Lay Member, Camden CCG
Mr Simon Goodwin NCL Chief Finance Officer, Barnet, Camden, Enfield, Haringey and Islington CCGs
Dr Neel Gupta Governing Body, Chair, Camden CCG
Ms Helen Pettersen Accountable Officer, Barnet, Camden, Enfield, Haringey and Islington CCGs
Dr Jo Sauvage Governing Body Chair, Islington CCG
Mr Adam Sharples Governing Body Lay Member, Haringey CCG
Mr Dominic Tkaczyk Governing Body Lay Member, Barnet CCG
Non-Voting Members Present:
Ms Parin Bahl Healthwatch Enfield
Attendees:
Mr Paul Sinden NCL Director of Planning, Performance and Primary Care,
Ms Eileen Fiori NCL Director of Acute Commissioning
Ms Sarah Rothenberg NCL POD Director, Northeast London Commissioning Support Unit
Mr Ian Porter Director of Corporate Services, Barnet, Camden, Enfield, Haringey and Islington CCGs
Ms Anna Stewart Programme Director, North London Partners in Health and Care
Mr Richard Dale Director of Programme Delivery, STP, NCL
Mr Will Huxter Director of Strategy, NCL CCGs
Apologies:
Ms Angela Dempsey Nurse Representative Enfield CCG
Ms Janet Burgess Councillor, Islington Council
Ms Sharon Seber Nurse Representative Haringey CCG
Ms Sharon Grant Healthwatch Haringey
Ms Pat Callaghan Councillor, Camden Council
Ms Alev Cazimoglu Councillor, Enfield Council
Mr Richard Cornelius Councillor, Barnet Council
Dr Tamara Djuretic Director of Public Health, Barnet Council
Mr Edmund Nkrumah NCL Director of Performance, Barnet, Camden, Enfield, Haringey and Islington CCGs
Minutes
Mr Andrew Tillbrook Deputy Board Secretary, NCL CCGs
20

2
1 Introduction
1.1 Apologies for absence
1.1.1
Apologies had been received from Ms Angela Dempsey, Ms Janet Burgess, Ms Sharon Seber, Ms Sharon Grant. Ms Pat Callaghan, Ms Alev Cazimoglu, Mr Richard Cornelius Dr Tamara Djuretic and Mr Edmund Nkrumah (later note: Ms Peray Ahmet, Haringey, had been stood down as Councillor).
1.2 Declarations of Interests
1.2.1
There were no additional declarations of interests.
1.3 Declarations of gifts and hospitality
1.3.1
There were no declarations of gifts or hospitality offered or received.
1.4 Opening Remarks
1.4.1
The Chair welcomed all members of the Committee and members of the public for attending.
1.5 Questions from the public
1.5.1
Some questions from members of the public had been received in advance of the meeting and also tabled at the meeting. Those questions tabled included:
With regard to Procedures of Limited Clinical Effectiveness (PoLCE), to seek clarity on the implementation process, taking account of the provisions in the 2010 Equality Act and statutory obligations on CCGs to improve health equality of patients in protected groups and also to narrow the gap between the best and worst health outcomes. Examples of potential differences included: whether patients were in manual or sedentary work, some gynaecological conditions and BMI scores typically linked to poverty and other social markers.
In addition, if guidance is given to GPs to account for variations as exemplified above, what will be the cost of the administrative system and if it is likely to cost be less than the anticipated annual saving of £2m?
1.5.2 In considering the question posed, the following responses were provided:
From a primary care perspective, it would be useful to assess the process that is being proposed and initial understanding of the implementation plan of PoLCE would include an Equalities Impact Assessment (EIA) to ensure fairness
The review would continue to be receptive to concerns as and when they arose
The PoLCE policy took account of patient thresholds based on their symptoms and so should not prejudice the applicant based on their working background (manual or sedentary jobs)
With regards to patients with a high level of BMI (Body Mass Index), access to treatment was not restricted in itself, rather, constraints were imposed where there were operative risks to the patient where issues such as wound infection, cardio-vascular complications, respiratory complications can be a significant element
21

3
Decisions of undergoing an operative procedure are based on discussion between a patient and clinician and take into account the best decision which would consider a range of medical factors.
1.5.3 It was important to ensure that the review and intentions of the proposed implementation of the PoLCE policy was communicated to patients and clinicians alike to ensure it was understood by all stakeholders, and, where a patient remained concerned about a decision regarding their treatment, to enable further communication between patient and clinician.
1.5.4 Further verbal comments from members of the public present suggested that consideration should be given as to how the Orthopaedics Services Review was being conducted. It was noted that in the view of the member of the public that some patient groups were unaware of the review and that there should be a widening of methods of communicating by word, letter and meetings in addition to internet and email as not all patients had access to computers.
1.5.5 In response to the question the following points were made:
The meeting noted that at the last Joint Commissioning Committee a report was considered which included the degree of engagement with patients, residents and other stakeholders. In particular:
o The engagement part of the review had been prefaced with a desktop EIA and several pensioner groups in Islington (including the St Luke’s Community Centre). In total about 500 people had been engaged in the review in face-to-face meetings. The groups selected had been based on those who were most likely to utilise the services under review
o If further and specific proposals were brought to light, a full-scale consultation exercise would need to be implemented, which would require a deeper level of engagement
o However, in the interim, it was suggested that contact details all pensioners’ forums in Islington and the National Pensioners Convention could be shared so that they can be included in future engagement around the review.
2. Commissioning
2.1 Adult Elective Orthopaedic Services Review: Governance and Process for Stage Two of the Review
2.1.1 The Committee noted that the report presented sets out the next stage in the governance processes proposed for the approach. The report which was taken as read, set out details of a two stage governance process:
Stage one – a clinically led process led by a Review Group focusing on engagement following publication of a draft case for change and co-creation of a proposed outline model of care (which had been undertaken in 2018), and
Stage two – a clinical commissioner led process delivering an options appraisal and creation of a pre-consultation business case (PCBC) (which was about to commence).
It was noted that the Committee were being asked to agree three recommendations on behalf of the five north central London CCGs: This paper sets out three things for the Joint Commissioning Committee to agree:
i) a more overtly commissioning led process to formally oversee stage two of the review;
22

4
ii) sign-off the decision making process up until public consultation, including carrying out an options appraisal process and the creation of a pre-consultation business case (PCBC); and
iii) that in taking forward the second stage of the review and any options appraisal process that the services should remain within the NHS by way of variations to existing annual contracts.
2.1.2 The Committee’s attention was drawn to the main components of the report. The Governance and Process Stage part of the report which set down the following elements: The proposed timeline indicated the following decision-points for the JCC (these may be subject to change):
March/April 2019 – agreement of the clinical model and options appraisal criteria; (which would be brought back to this committee for consideration and approval)
June/July 2019 – agreement of PCBC.
Contract form The Committee were reminded that a number of design principles had been agreed at the last meeting of this Committee (December 2018) alongside six areas of next steps. These were the outputs from the five clinical design workshops, details of which were set out in the report. This work, alongside the extensive pre-consultation engagement had evidenced the inter-connectedness between trauma and elective services and the conclusion that it would be difficult to disaggregate the two services without a significant impact on emergency services and recruitment and retention of key clinical staff, particularly orthopaedic surgeons. It was therefore recommended in the paper that that the services should remain within the NHS by way of variations to existing annual contracts. The Governance process The Committee were asked to note that stage two of the review would require a new governance framework, with more overt clinical commissioner leadership. A number of areas were noted:
Potentially commissioning responsibility should be widened to enable commissioners outside the NCL to part of the decision-making process. NHS England would provide further definitive advice in this area.
The review process had received positive leadership from the current SRO, (the Chief Executive of the Royal National Orthopaedic Hospital). To strengthen the commissioning aspect of this service, it was noted that Will Huxter, Director of Strategy for the five NCL CCGs, would become the joint SRO.
A Programme Board would be established to oversee three key workstreams, clinical, finance and activity modelling, and communications and engagement.
An independent clinical advisor would be appointed to provide, as required, additional assurance to both the Programme Board and the Joint Commissioning Committee
Mechanisms would be put into place to monitor potential and actual conflicts to ensure they were managed appropriately.
2.1.3 In considering the report and presentation the following observations and comments were made by members of the Committee:
How CCGs might wish to support and triage the community elements of the service, to which, particularly for Enfield CCG, with regard to the commissioning
23

5
aspect of the service, would look to incorporate QIPP schemes. Further detail was requested about potential financial partnership models;
The importance of ensuring appropriate communications were in place to disseminate the progress of this scheme to the five CCG Governing Bodies along with cascading information to patient groups and other stakeholders such as Healthwatch;
To clarify how the design principles shape the service model – was it correct that the elective hospitals would be responsible for operative care whilst the base hospital would look after the patient pre and post-operative care? Confirmation was requested about the areas of the clinical model that had not yet been determined;
The engagement approach was broadly supported as well as noting that current clinical models of care (such as South West London Elective Orthopaedic Centre (SWLEOC) were being reviewed, with the objective that the most appropriate clinical model would be devised and implemented for the benefit of health care arrangements in north central London;
The risks listed, which included the potential of stakeholder and patient concerns causing delays were noted; including the mitigations around ensuring robust patient and public engagement and the co-creation of the clinical model with both clinicians and patient representatives;
The Review Team were asked to look at how they could link more clearly the design principles and evidence (patient engagement feedback);
To clarify why the service model and design principles mean that the services needed to stay within the NHS by way of variations to existing contracts.
2.1.4 The Committee noted that:
The clinical design work had paid particular attention to the community elements of the service and how the acute element sat within the overall patient pathway. It was also a key theme from the patient and public engagement. There were opportunities through the development of the orthopaedic clinical network to look at key elements of the whole pathway to achieve consistency across NCL CCGs;
Financial partnership modelling options remained as work in progress to determine what would be the most beneficial model to work across NCL. As per the decision that the Committee were being asked to make any partnership arrangements would be achieved via variation to existing NHS annual contracts, rather than a standalone contract for these services. The high level proposed arrangement would need to be set out in the pre-consultation business case.
The importance of good communications with CCG Governing Bodies and patient stakeholder groups, particularly Healthwatch, was agreed;
The service model was clarified. It was confirmed that it was correct that the elective hospitals would be responsible for operative care whilst the base hospital would look after the patient pre and post-operative care. It was noted that some areas of the case-mix have not yet been finalised. There were likely to be a small number of complex cases where patients remained at one site for their care because of clinical specialisms (e.g. haemophiliacs were likely to remain at the Royal Free Hospital because of their clinical specialism in this area). Further work was also required to determine where day-case activity should sit in the model and also where pre-operative assessment and Joint School should sit in the model;
24

6
It was agreed that the approach was to draw on learning from SWLEOC not to replicate the approach wholesale in north central London; the model of care needed to fit our own geography and specific needs;
It was noted that there would be a strong patient engagement in the next stage of the review;
In relation to the risks and mitigations it was noted that there had been strong patient engagement in the approach to developing the design principles, in addition to clinical co-creation. All Healthwatch groups had been invited to nominate additional representatives to attend the workshops and these individuals had made a really positive contribution to the outputs. It was agreed that Healthwatch would be invited to provide to support these engagement exercises at future stages of this review;
It was agreed that as part of the development of the pre-consultation business case there would need to be an explicit link between the themes coming from the design workshops and engagement and the final service model. In particular patient transport services was acknowledged as requiring more work (and this would form part of the next review stage) to see if there were mitigations that could be made in the model to reduce any potential impact on patient travel times;
Finally, in relation to the clarity required with regard to the recommendation of retaining services within the NHS and the strength of the rationale for this. This is primarily based on clinical considerations, and the impact on both trauma and elective services if there were entirely separate providers for planned and elective care. The services defined in the design principles were so intertwined with existing NHS services, it was recommended that a separate specification for orthopaedic services could not be as clinically effective and be value for money. Separately procuring the elective centres, could lead to splitting medical teams and affecting recruitment and retention and clinical capacity. This could undermine trauma work and impact on emergency departments resilience, as well as the ability to establish ring-fenced capacity to ensure quality and continuity of service for the benefit of patient care.
2.1.5 ACTION: Anna Stewart to clarify the reference to patients in the co-creation of the programme with clinicians.
2.1.6 Anna Stewart and Will Huxter were thanked for their work to date from which the resolutions were agreed below, taking account of the discussion above.
2.1.7 The Joint Commissioning Committee:
AGREED a more overtly led process to formally oversee stage two of the review;
AGREED the decision making process up until public consultation, including carrying out an options appraisal process and the creation of a pre-consultation business case (PCBC); and
AGREED that in taking forward the second stage of the adult elective orthopaedic services review and any options appraisal process that the services should remain within the NHS by way of variations to existing annual contracts.
2.2 Implementing the NCL wide Procedures of Limited Clinical Effectiveness
2.2.1 Mr Dale introduced the above which was taken as read. The Committee noted that Dr Nick Dattani was unable to attend and present the report due to clinical engagement and so Dr Jo Sauvage (Clinical Chair of the PoLCE Steering Group) presented in his
25

7
absence. Mr Dale recapped the purpose of the report, which followed on from the implementation plan for the PoLCE policy, approved by this committee in December 2018 and to endorse the work to develop a proposal for a single contractual approach and management of referrals.
2.2.2 In consideration of a question raised by a member of the public as to the anticipated cost of the referral management processes including the cost of creating such as from scratch for Islington – and will these costs be less than the anticipated annual saving of £2m. The Committee was advised that the £2m savings mentioned in the report is what was thought to be achievable and subject to undertaking a high level options appraisal across the five CCGs which would include a range of criteria:
Reducing bureaucracy and ensuring value for money
Increasing transparency of the process
The service is clinically led and evidenced based.
2.2.3 Account would also be taken of national guidance to help provide options for a more consistent and equitable approach across the NCL area.
2.2.4 Some further questions raised in advance and submitted by Mr Richards were presented: Why is NCL proposing to continue circumcision as a procedure in its PoLCE policy when noted at the December meeting that it is an effective operation procedure with a range of medical conditions (and NHSE guidance does not include circumcision)? In response, the Committee noted that there had been a wider variation of how some procedures have been carried out over the years across NCL. Work on reviewing PoLCE has been conducted by different entities regionally and nationally, taking account of new evidence and have reached slightly different conclusions Currently, the work carried out at national level is reflected in the NCL proposals and it was noted that such work was subject to regular review. Assurance was provided by clarifying that circumcision procedures would continue to be undertaken, where there is a clinical value. There are clear clinical criteria to support this and the thresholds are applied. However, where circumcision is not required for medical and clinical reasons, the threshold would not be reached. It was confirmed that where local policies differ from national guidance, local conditions would prevail as they had been approved locally and subject to due diligence but where there are national policies, CCGs are duty bound to refer to those policies, take an opinion and include them in the work at local level. Ultimately, there is a national initiative to create consistency for commissioners as well as for providers.
2.2.5 The second question from Mr Philips concerned future decisions made about patients held with a referral pathway who have been referred with an expectation of an intervention prior to the approval of evidence based thresholds and if that future decision would renege on the earlier commitment and if the patient could appeal to the JHOSC? In response, it was confirmed any referrals prior to changes in threshold would be honoured. Potential future changes to thresholds would be developed, working with the JHOSC, taking account of EIAs which would determine the level of appropriate engagement.
26
8
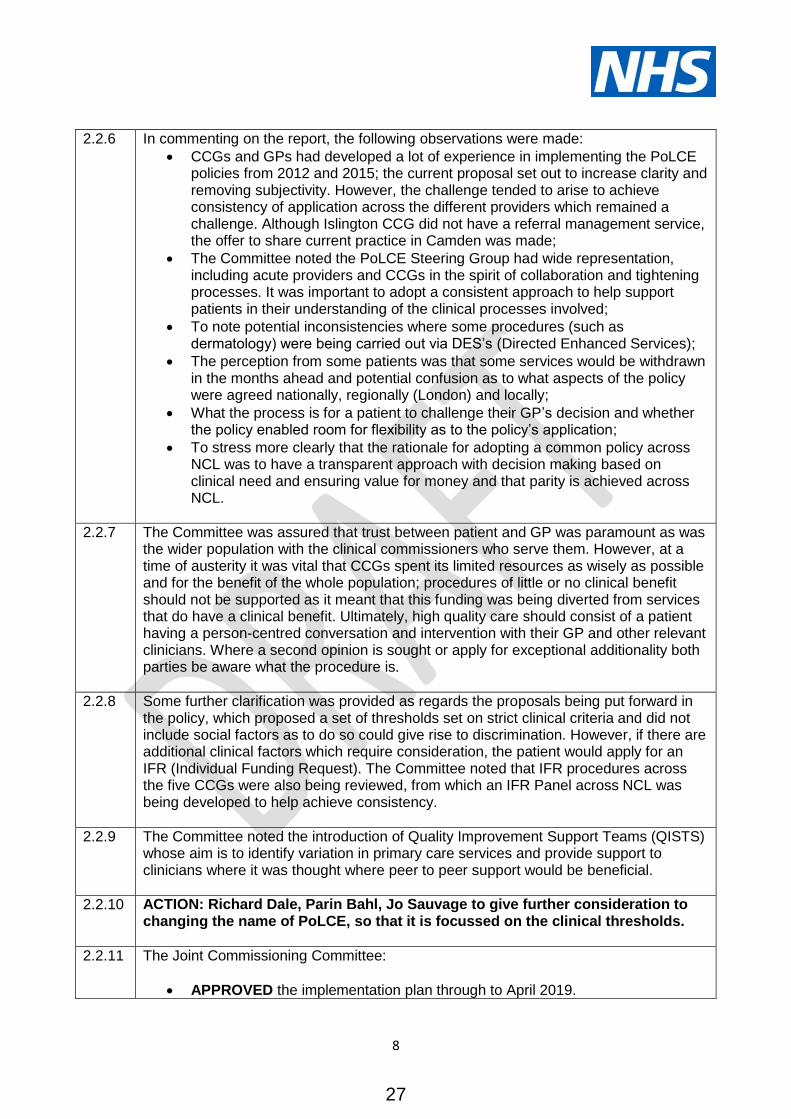
2.2.6 In commenting on the report, the following observations were made:
CCGs and GPs had developed a lot of experience in implementing the PoLCE policies from 2012 and 2015; the current proposal set out to increase clarity and removing subjectivity. However, the challenge tended to arise to achieve consistency of application across the different providers which remained a challenge. Although Islington CCG did not have a referral management service, the offer to share current practice in Camden was made;
The Committee noted the PoLCE Steering Group had wide representation, including acute providers and CCGs in the spirit of collaboration and tightening processes. It was important to adopt a consistent approach to help support patients in their understanding of the clinical processes involved;
To note potential inconsistencies where some procedures (such as dermatology) were being carried out via DES’s (Directed Enhanced Services);
The perception from some patients was that some services would be withdrawn in the months ahead and potential confusion as to what aspects of the policy were agreed nationally, regionally (London) and locally;
What the process is for a patient to challenge their GP’s decision and whether the policy enabled room for flexibility as to the policy’s application;
To stress more clearly that the rationale for adopting a common policy across NCL was to have a transparent approach with decision making based on clinical need and ensuring value for money and that parity is achieved across NCL.
2.2.7 The Committee was assured that trust between patient and GP was paramount as was the wider population with the clinical commissioners who serve them. However, at a time of austerity it was vital that CCGs spent its limited resources as wisely as possible and for the benefit of the whole population; procedures of little or no clinical benefit should not be supported as it meant that this funding was being diverted from services that do have a clinical benefit. Ultimately, high quality care should consist of a patient having a person-centred conversation and intervention with their GP and other relevant clinicians. Where a second opinion is sought or apply for exceptional additionality both parties be aware what the procedure is.
2.2.8 Some further clarification was provided as regards the proposals being put forward in the policy, which proposed a set of thresholds set on strict clinical criteria and did not include social factors as to do so could give rise to discrimination. However, if there are additional clinical factors which require consideration, the patient would apply for an IFR (Individual Funding Request). The Committee noted that IFR procedures across the five CCGs were also being reviewed, from which an IFR Panel across NCL was being developed to help achieve consistency.
2.2.9 The Committee noted the introduction of Quality Improvement Support Teams (QISTS) whose aim is to identify variation in primary care services and provide support to clinicians where it was thought where peer to peer support would be beneficial.
2.2.10 ACTION: Richard Dale, Parin Bahl, Jo Sauvage to give further consideration to changing the name of PoLCE, so that it is focussed on the clinical thresholds.
2.2.11 The Joint Commissioning Committee:
APPROVED the implementation plan through to April 2019.
27

9
NOTED the local work required by lead commissioners on behalf of NCL CCGs for any patients who have already received a referral for a treatment that is no longer routinely funded.
ENDORSED the work to develop a proposal for a single contractual approach and management of referrals.
Would ESTABLISH a set of principles to support understanding of the policy and appropriate communication to stakeholders.
3 Questions from Public
3.1 Professor Richards advised the Committee that when NHS England undertook the consultation exercise about PoLCE, it iterated that the review was the first stage of a longer-term process and there was some mistrust as to the wider intentions of NHSE. Coupled with this aspect was the perception that the trust between patient and doctor may be challenged if it was felt that recommendations for health care were not entirely clinically based. The meeting was assured that all doctors are duty bound by good medical practice set down by the General Medical Council – above all, that no harm should come to the patient and, within general practice, being an advocate for the patient.
4. Any Other Business
4.1 There was no any other business to conduct.
5. 5.1
Date of Next Meeting The next Committee meeting would be on Thursday, 7 February 2019, 2:30 to 5pm at Hendon Town Hall, The Burroughs, Barnet, NW4 4BG.
28

Agenda Item: 2.2
JOINT COMMISSIONING COMMITTEE
7 DECEMBER 2018 and 3 JANUARY 2019 - ACTION LOG
Meeting Date Action No. Action Lead Deadline Update
7 June 2018
25 To feed back to the Senior Management Team the issues raised about future performance monitoring from which a proposal for performance reporting would be developed.
Paul Sinden December 2018
A new approach has been agreed and will be implemented in the March 2019 reporting round.
4 October 2018
47 To bring a report on the London Ambulance Service to the JCC meeting, which will look at the disparity in performance in Barnet, Enfield and Haringey and include average waits as benchmarking.
Paul Sinden February 2019
This has been included in the February 2019 Acute Performance and Quality Report.
4 October 2018
51 To include case studies in the next TCP update to the JCC.
Kath McClinton February 2019
These have been included in the paper on today’s agenda.
4 October 2018
54 To produce a glossary of acronyms. Paul Sinden/ report authors
February 2019
A glossary is appended to this action log.
7 December 2018
55 To provide an update on what is being done to make QIPP reporting consistent across NCL.
Will Huxter February 2019
Work is underway to standardise QIPP reporting across CCGs. A monthly meeting of NCL QIPP directors is in place to review consistency of reporting against schemes. 2019/20 planning approach designed to ensure consistency.
7 December 2018
56 To provide an update on the overall planned care position, including the impact of the STP direct access workstream.
Will Huxter February 2019
A verbal update will be provided at the meeting.
29

Agenda Item: 2.2
7 December 2018
57 To ensure that the January 2019 meeting is well promoted and that invitations to the meeting are sent to the Councillor representatives on the Committee.
Steve Beeho February 2019
An invitation to the meeting was sent to all non-voting JCC members on 6 December 2018. A news story about the meeting was published prominently on all of the CCG websites in December 2018. The respective CCG communications teams also highlighted the meeting on Twitter and shared details with Healthwatch to promote through their networks.
7 December 2018
58 To share the PoLCE Equalities Impact Assessment with Healthwatch.
Richard Dale February 2019
These were shared with Healthwatch colleagues in January 2019.
7 December 2018
59 To confirm the NCL Joint Health Overview Scrutiny Committee JHOSC’s position on whether a formal consultation is required on PoLCE changes.
Richard Dale February 2019
For the December update the JHOSC recommended clinical stakeholder engagement which was undertaken. For future policy updates, the EQIAs and engagement will be presented to the JHOSC for a decision as to whether formal consultation is required.
3 January 2019
60 To clarify the reference to patients in the co-creation of the programme with clinicians.
Anna Stewart April 2019 An update will be provided at the next JCC meeting.
3 January 2019
61 To give further consideration to changing the name of PoLCE so that it is focussed on the clinical thresholds.
Jo Sauvage/ Parin Bahl/
Richard Dale
April 2019 A meeting has been booked with Parin Bahl and Sharon Grant to discuss this further.
30

Appendix 1
Glossary of Acronyms
The following key acronyms are used in the February JCC meeting papers.
BRS - Building the Right Support
CAG - Clinical Advisory Group
CETR - Community Education and Treatment Review
CRC - Colorectal cancer
CQUIN - Commissioning for Quality and Innovation
DG - Diagnostic Guidance
EDIS - Eating Disorder Intensive Service
EHCNMB - Education, Health and Care Needs Management Board
FIT - Faecal Immunochemical Test
FRF - Financial Recovery Fund
HCHJC - Head of Children’s Health Joint Commissioning
HEE - Health Education England
ICS - Integrated care system
LCW - London Central West Unscheduled Care Collaborative
LeDeR - Learning from Deaths report
MFF - Market Forces Factor
NCEL - North Central and Northeast London
NG – NICE Guidance
NLP - North London Partners
OT – Occupational Therapy
POD - Point of Delivery
SCAN - specialist CAMHS team for children and young people with learning
disabilities and neuro-developmental disorders
TCPs - Transforming Care Partnerships
TCST - Transforming Cancer Support Team
UEC - Urgent and Emergency Care
2ww - Two week wait
31
1
NCL Joint Commissioning Committee Thursday, 7 February 2019
Report Title Acute Contract Report (Month 9) Date of report 24 January 2019
Agenda Item
3.1
Lead Director /
Manager
Eileen Fiori Director of Acute Commissioning for NCL CCGs
Tel/Email [email protected]
GB Member Sponsor
Ms Karen Trew (Chair) Governing Body Vice Chair and Lay Member, Enfield CCG
Report Author
Eileen Fiori & Sarah Rothenberg Director of Finance NELCSU
Tel/Email [email protected]
Report Summary
This report sets out the Financial and Activity performance for NCL Commissioners at our Acute Hospital Providers for the reporting Month 9 (December) 2018. Actions being taken are included in the main body of the report as detailed below.
Recommendation The Joint Commissioning Committee is asked to:
APPROVE the report and
ADVISE on areas where further action could be taken by CCGs to mitigate key risks.
Identified Risks
and Risk
Management
Actions
Under-delivery of QIPP, activity within the emergency care pathway and the increasing costs at acute providers, where there is no corresponding increase in acuity, continue to present the greatest risks to delivering the financial plans.
These risks are monitored within the CCG Finance and Performance Committees.
Counting and coding behaviour is captured, challenged and monitored by the contracts and claims teams and further validation has now been completed. This has validated the current challenges as correct and in place and increased the level of confidence in the values attributed to these challenges.
Conflicts of Interest
Not applicable.
32
2
Resource
Implications
Annual budgets held by each CCG.
Engagement
The report is presented to the NCL Joint Commissioning Committee which includes elected GP representatives, lay members, Healthwatch, Public Health and representatives from each NCL London borough.
Equality Impact
Analysis
This report was written in accordance with the provisions of the Equality Act 2010.
Report History and
Key Decisions
This is a standard report provided for the Joint Commissioning Committee.
Next Steps Ongoing monitoring of performance and actions detailed below. Complete clinical audits in Non Elective admissions and A&E attendances at NMUH and RFL. Adjust Claims and challenge opportunities for each CCG based on the additional validation. A sharing of the activity, counting and coding issues noted at the Royal Free London will be shared through the Contract Meetings.
Appendices Full Finance and Activity pack is circulated with this summary report. See Appendix 1 - Full Finance and Activity pack.
Which CCG does this relate to
Barnet CCG, Camden CCG, Enfield CCG, Haringey CCG, Islington CCG.
33

3
1. Finance
1.1 NCL Acute Contracts
The overall forecasted outturn on all acute providers is £1,277m against an annual
plan of £1,215m. This expected adverse variance of £49.3m on Provider Contracts
predominantly relates to the four main NCL acute providers.
When monitoring against CCG financial plans for the main NCL acute providers
there is a reported year-to-date over performance of £31.9m and forecast outturn
over performance of £45.9m. This represents a £0.4m adverse movement from last
month’s outturn of which: £2.8m is at North Middlesex, which is offset by favourable
movements of £1.8m at Royal Free, £0.3m at the Whittington and £0.2m at
University College London.
The primary driver behind the improvement at the Royal Free, Whittington and UCLH is an upward revision in level of challenges assigned against contract data.
The deterioration at North Middlesex is split into two areas:
£1.0m increased activity in Elective and Non Elective PODs
£1.8m due to revisions in the estimated level of QIPP to be delivered later in the year.
1.2 Non NCL Acute Contracts:
We have a £3.4m over performance on acute contracts outside NCL. This is a £0.6m
adverse movement from last month.
Adverse movement is seen in the main at: Kings £0.2m; Imperial £0.1m; RNOH
£0.1m and Guys £0.1m.
Overall the Out of Sector Providers are currently expected to be 2.6% over the
financial annual plan.
Action: For Homerton, whilst this contract is the responsibility of City
and Hackney CCG, the CSU are supporting that commissioning team by
preparing a reconciliation statement to close the outstanding
contractual issues and challenges. Any adjustments to the position will
be pre-approved by NCL CCGs at Working Day 4 financial meetings.
Monthly.
Action: For Barts, a tele-conference is in place to inform all adjustments
and the reasons for this challenge, including mitigating actions such as
planned audits in Non-Elective activity and challenges. This is
discussed at the Working Day 4 financial meeting. Monthly.
Action: For Imperial, we are in ongoing discussions with the host
commissioners to resolve outstanding challenges and mitigating
actions. This month an escalation letter has been sent to the Trust to
support these discussions. A reconciliation statement has been
prepared and shared with the Trust. Monthly.
34

4
Action: Associate meetings in place with lead commissioners to monitor
actions being taken to mitigate over performance. Weekly.
1.3 Claims and Challenges (open)
The five largest open queries for the NCL CCGs at all providers are: • Aggregate claims £12m
• Misattribution Checks (incorrectly identified) £5.9m
• Provider not Lead for Maternity Pathway £1.4m
Aggregate contract claims are multiple manual challenges where there appear to
have been systematic problems affecting a group of charges.
Further Counting and Coding Opportunities
The work undertaken on counting and coding changes plus the claims and challenge
processes across the four main NCL Acute Providers in NCL was presented to CCG
finance and contract Directors on 5th
December.
Contract teams have been working to further understand and clarify the backing data
and to understand which opportunities have already described as part of the
standard claims and challenge process and those which are new areas for
challenge.
It is clear from this work that there has been a benefit in increasing the confidence
level on the possible return on the challenges already in the system at the Royal
Free.
The predicted return on the challenge opportunity increased by circa £2m for 18/19
at Royal Free. The report for UCLH gave further strength to the challenge already in place regarding a haematology counting and coding change that was evident in the first
quarter of the year. This was already planned for and there is no further increase in value.
Action: Full year effect opportunities to be built into the 2019/20
contracting round.
1.4 Claims and Challenges (accepted)
To date, £7.5m of claims raised at month 7 have been accepted by acute providers.
Breakdown of accepted claims by CCGs is shown below:
• Barnet £1,515,987
• Camden £1,365,601
• Enfield £1,991,517
35

5
• Haringey £1,557,594
• Islington £1,092,905
1.5 QIPP
At month nine, £20.5m of the planned £43.3m has been delivered (47%). The forecast
outturn position is expected to be £30.3m delivery against a plan of £64.5m (47%). This is a £7m slippage on the reported forecast at month eight. This slippage is due to under delivery on QIPP schemes and due to revised savings
plans now predicted to be at lower levels than originally expected. We are continuing to work on current schemes that will help prevent further deterioration and work on the development of additional QIPP plans to bridge the shortfall.
Camden, Enfield and Haringey CCGs account for a significant proportion of the total under delivery at month nine (circa £23m) while Haringey (£7.3m) and Enfield (£12.6m) CCGs are forecasting the greatest year-end under performance.
Health and Care Closer to Home
The NCL CCGs are reporting a £2m year-to-date delivery at month nine and £3.5m at year end (30% of plan), which is a deterioration on last month’s position. The main areas of under delivery are: the expected impact of
extended primary care access on Accident and Emergency attendances, Haringey QISTs (Quality Improvement Support Teams) and Enfield CCG’s Single Offer within primary care.
Urgent and Emergency Care
Overall, UEC schemes are reporting a £7.8m year-to-date delivery at month nine (49% of plan). The main areas of under-delivery relate to Ambulatory Care, Reducing Non-Elective Admissions for Children, Integrated Urgent
Care, Adult Admission Avoidance and Simplified Discharge. Under delivery of Ambulatory Care has been attributed to delays around agreeing counting and coding and tariff, particularly at RFL. Under delivery
relating to reducing children’s Non-Elective admissions is largely at NMUH, affecting Enfield CCG. This is due to ongoing negotiations relating to investment in a revised staffing model. Integrated Urgent Care and Adult Admission Avoidance aim to reduce Accident and Emergency attendances
and non-elective admissions by diverting patients to alternative services but activity increases have been seen across NCL. Overall, UEC schemes are forecast to deliver £10.5m of QIPP by year end,
which is 45% of the original plan. Planned Care
The NCL CCGs are reporting a £6.1m year-to-date delivery at month eight
which is 37% of plan.
36
6
The main area of slippage relates to Direct Access Pathology. This is due to delays caused by the robust governance processes required to implement new guidance for GP pathology, challenges and use of electronic ordering
systems across the patch. As a consequence, full savings for 2018/19 are delayed, resulting in a greater impact for 2019/20 than initially proposed. The Planned Care schemes overall are forecast to deliver £10.1m (41%) of
planned QIPP by year-end.
Action: Regular QIPP workshops to peer review performance and
opportunities to establish short, medium and long term pathway
changes that not only deliver in-year savings, but also contribute to 19-
20 plans. Next planned workshop: 24 January.
1.6 Year End Discussions
Both the Royal Free Hospitals and North Middlesex have made early indications that
they wish to commence discussions on finalising an income number for 2018/19.
Action: All contractual and financial discussions for 18/19 closedown
coordinated through the NCL CFO for Royal Free and the Director of
Acute Contracts for North Middlesex.
2. Activity
2.1 Overall Referral Trends
Overall, the ongoing trend for GP referred activity is down across the four NCL acute
providers. The annualised trend indicates a 2% decrease in referrals although referrals using the 2 week wait cancer routes continue to rise.
Action: CCGs are undertaking peer review of GP referral activity. This
will be reported back to the Activity Review Group that is chaired by Eileen Fiori, NCL Director of Acute Commissioning and is attended by a
Director from each CCG. This group will assist in identifying further opportunities at a local level. Monthly.
At Trust level, there have been reductions at North Middlesex, Royal Free London
and Whittington Health with a small increase seen at University College London. However there is a risk that an increasing number of referrals go to providers outside of NCL.
Action: CCGs are undertaking a review of out of sector activity. This will
be reported within each of the CCG contracting and QIPP meetings.
37

7
At Royal Free, there is a decrease in referrals of 7.4% (a change from 8.1% over the last 2 months) for NCL CCGs. A correction to data submitted by Royal Free, which was counting Diagnostics Tests as a GP referral, explains the majority of this
decrease. There is evidence of actual referral decrease for Cardiology, Orthopaedics, Paediatrics, ENT and Urology specialties. Haringey and Enfield CCGs have both seen an increase in Target (Two Week Wait)
referrals particularly in Urology, Breast Surgery, Dermatology, Gynaecology and Colorectal Surgery.
The small rise in referrals at University College London is seen in Dermatology,
Trauma and Orthopaedics and Breast Surgery. A common theme across NCL is the increase in Two Week Wait (Suspected Cancer) demand. The cancer waiting times dataset shows a 17% year on year increase in
Two Week Wait activity. Analysis of First Outpatient First Attendance data shows particular increases in Breast Surgery, Urology and Dermatology activity.
Action: CCG GPs requested to investigate the reasons for the rise in two
week wait referrals and to be presented at the monthly Local Delivery Team meetings. Ongoing. Action: Director of Performance to confirm planning assumptions for
19/20 contracts.
2.2 First attendance Outpatients
First attendance outpatient activity has been above plan throughout 2018/19.
Although the 2018/19 monthly data is showing NCL level demand from primary care
is falling the attendance activity is not down on the same period as last year. This suggests that activity is driven by individual Trust waiting list management and the
increasing trend in suspected cancer referrals.
CAG was agreed in contracts in August 2018, therefore the impact of the service in avoiding referrals converting to first attendances should begin to be seen from
September onwards. Although there has been a delay there are now more specialties included in this service than were previously planned for. National IT systems do not support tracking of CAG onward referrals and a clinical audit is suggested.
Action: The CAG impact is being monitored by the planned care
workstream. Monthly.
Action: Individual contract Local Delivery Teams to manage the increase
in specialties offering advice and guidance and also the performance against CAG performance indicators. Monthly meetings.
38

8
Action: Request for local audits on CAG onward referrals to be undertaken.
In terms of Tele-dermatology, University College London and the Whittington have
agreed to convert their services to deliver to the NCL specification from the 2nd January 2019. This service will be subject to close review to test out the viability of the model over the remainder of the financial year.
Discussions have commenced with NMUH to join this approach as the NCL Tele-
dermatology specification is included in their subcontracted service with Concordia. The Trust’s feedback on the service specification has been positive, however
implementation of the service has been deferred until April 2019 (post the initial NCL proof-of-concept phase). Enfield continue to use the Tele-dermatology service (utilising medical photographers) at the Royal Free.
Following a meeting with Royal Free in early December the Trust have agreed to
participate in the NCL Tele-dermatology scheme. Commissioners are aiming for
implementation of this by 31st January 2019, however due to staffing issues in the
Trust IT team this could be delayed until mid-February 2019. In order to assist with
pressures UCLH are publishing their service via the e-referral system.
Action: Contract teams for North Middlesex to continue to work with the Trust to aim for the April implementation date.
Action: CCGs to monitor own use of CAG and Tele-dermatology
services through Local Delivery Team meetings. Monthly.
2.3 Follow ups
Monthly activity for follow ups has been broadly in line with CCG plans until month
five where a larger than expected reduction in follow ups had been seen. There is a
downward trend of 1% compared to last year.
Royal Free activity reduced by 6% using a year-on-year comparison. This was primarily due to a number of outpatient clinics at the Royal Free site closing for two
weeks in previous months as part of the planned move of these clinics to the re-opened Chase Farm site. The Royal Free planned to recover this activity and there is some evidence that this is the case as the trend two months ago was 8%. The main specialty affected was Paediatrics.
The Whittington remains the only NCL provider that reported an increase year on
year (+2%). This is driven by Plastic Surgery and Neurology. These services, although small in size, have continued to show historic rises.
Action: Local Delivery Teams monitor Provider activity that looks at first to follow up ratios and act on areas where variance describes opportunity. Monthly.
39

9
2.4 Planned Care
Year to date the activity is 2.3% above CCG plan. The level of activity has slightly increased by circa 1% when looking at year on year comparisons.
Royal Free is showing the greatest fall in activity of 8% compared to last year. Whilst the Trust has stated its desire to recover this position there is no evidence that capacity is in place to support this. The implementation of a new Electronic Patient Record system is also having an impact where existing patients need rebooking.
Fortnightly telephone calls are in place between Commissioners and Royal Free to update on RTT performance issues, in addition to a monthly RTT steering group meeting and Performance group meeting. A clinical harm review process is also in
place. There is an increase in planned care compared to last year for the other providers. Both UCLH and the Whittington are both undertaking increasing levels of activity in
day case and diagnostic procedures in specialties that are influenced by the number of suspected cancer referrals in Gastroenterology and Breast.
Action: The NCL wide RTT Performance Group monitors performance
and impact on patients waiting times in line with March 2018 waiting list positions. This is chaired by Paul Sinden, NCL Director of Planning, Performance and Primary care and attended by senior performance managers from the four acute providers.
Action: CQRGs monitor any patient impact through harm reviews, clinical incident reporting. Monthly.
Action: Activity Review Group reviewing activity to assess if this is taking place in the lowest cost environment. Monthly. Action: PoLCE data review taking place at Royal Free. Findings to be
presented at Contract Delivery Group. February.
Action: Review of Referral Management Systems across NCL being
undertaken through the Planned Care STP Workstream.
2.5 Non Elective Admissions
Year to date the Non Elective activity is 5.7% above plan.
This is 4.2% higher than the same period last year. This is a rise of 3300+ patients and is largely driven by the Royal Free and North Middlesex Hospitals. The largest change is seen at the Royal Free where Barnet CCG had 1600 more admission than the same period last year. A contributing factor has been as increase
of 20 Acute Assessment beds that had not been agreed with commissioners. This has resulted in an increase in short stay admissions.
40

10
Action: Barnet lead commissioner to secure response from the Provider about notification/corresponding drop in beds elsewhere. There is a
clinical audit on the 13th February to understand these changes to patient pathways.
Overall the system is showing a 13% increase in zero length of stay admissions and
North Middlesex Hospital are showing increases in Non Elective Short Stay admissions (adults and paediatrics) and Ambulatory Care admissions. Both will be driving an increase in the cost of the emergency care pathway that commissioner made no provision for.
Action: The contracts and clinical teams are in the process of planning audits of all activity within the emergency pathways at North Middlesex and Royal Free Hospitals, this will review Ambulatory Care and Non
Elective admissions in particular. To commence in February 2019. Action: findings described in the counting, coding and case mix review to be shared with providers as part of the challenge process.
At North Middlesex University Hospital, two new paediatric consultants have been recruited to reduce the level of NEL admissions at the Trust.
Action: The anticipated reduction in paediatric admissions will be monitored and discussed at the associated contract meetings. Monthly.
Work is underway at the LAS Demand Management Forum and will focus on
demand management schemes as well as targeting attendances and admissions for frailty patients. The group will also work towards maximising the uptake of Appropriate/Alternative Care Pathways and the impact on the associated calls and conveyances.
Action: This will be reported through the Urgent and Emergency Care STP workstream on delivering the demand management schemes across NCL. All CCGs are participating in this work. Monthly.
2.6 A&E attendances
Year to date the Accident and Emergency activity is 12.3% above plan and a year on year growth of 2.8%. Overall this is more than 13000 attendances that we did not plan for.
Each CCG is at least experiencing a 2% increasing trend with Enfield reaching 4%. Overall, the Urgent and Emergency Care STP QIPP schemes are reporting 49%
achievement against plan. LAS journeys are nor showing a rise in activity but the demand management schemes are not having the anticipated impact.
41

11
Schemes supporting A&E demand management include:
Redirection implemented at Barnet and Royal Free Hampstead Hospitals’
Emergency Departments and at Whittington Health from December 2018.
Collective approach on the Care Homes poster "are you concerned about
a resident" details which services are available and how to access them
111 *6 line is in place to enable staff to have access to clinical advice
rather than phoning emergency services.
The boroughs of Enfield, Barnet and Haringey are implementing
‘Significant 7’ across some of their care homes to help staff spot early
signs of deterioration
Extended Access contracts have now been agreed in primary care with
that adds as additional 10,000 appointments.
Action: Each CCG is working alongside the UEC STP workstream on
delivering the demand management schemes across NCL. For 2019/20, there should be a priority focus on optimising any non-elective tariff changes to realise efficiencies from ambulatory care. Ongoing.
Action: Urgent Treatment Centre (UTC) model remains in development and is being picked up by the RF UEC transformation board. Commissioners considered procurement but in the interim are negotiating a short - middle term solution with the current provider.
Action: Following completion of mapping exercise of care homes against the ‘Enhanced Health in Care Homes’ framework, a Draft Enhanced Care in Care Homes Framework is being developed.
Completion of draft for review is planned for March. Being led by Director of Quality at ECCG who will make recommendations on next steps.
Action: The STP engagement CQUIN with LAS will be focusing on
reduction of conveyances in Quarters 3 & 4 of 18/19.
42

Acute Commissioning Report
Month 9 Finance and Activity
December 2018
43
Financial Performance
244

Performance Against CCG Contract Plans
3
Overall Summary:
The Committee is asked to note the following when considering the NCL CCG finance and activity position for acute contracts, as at month
nine:
• Data submitted by all Providers was of sufficient quality to enable reporting of financial performance of actual activity and forecast outturn for the four main NCL acute Providers.
• When monitoring against CCG financial plans, the four main NCL acute providers reported year-to-date over performance of £31.9m and
forecast outturn over performance of £45.9m. This outturn includes the benefit of £3.3m from applying the Marginal Rate calcu lation.
Variance in YTD and Forecast over performance has deteriorated from month eight ,YTD by £3.8m and the Forecast by £0.4m. This YTD
adverse movement is driven by in-month activity increases including a lower level of QIPP achievement than planned. This has not been
reflected by a corresponding adverse forecast outturn primarily due to the fact there are mitigations in the annual position. The £0.4m
deterioration in the Forecast outturn comprises favourable movements of £1.8m at Royal Free, of £0.3m at The Whittington and £0.2m at
UCLH, offset by adverse movement of £2.8m at North Middlesex.
• The primary driver behind the improvement at the Royal Free, Whittington and UCLH is a upward revision in level of challenges assigned against contract data.
• The deterioration at North Middlesex is split into two areas:
• £1.0m increased activity in Elective and Non Elective PODs• £1.8m due to revisions in the estimated level of QIPP to be delivered later in the year.
• Commissioners have planned for a £3.3m over performance on acute contracts outside NCL which is 2.6% over the financial annua l plan.
This is a £0.6m deterioration from last month forecast across all contracts outside NCL.(See slide 7 for the Trust breakdown) .
45

Performance Against CCG Contract Plans
4
Adjustments:
The Committee is asked to note that NCL CCGs have included the following adjustments in their year-end forecasts for acute contracts:
• Seasonality: An adjustment has been made for the estimated activity levels later in the year, this is based on the historic trends.
• Estimated QIPP delivery: CCGs have made an adjustment for the estimated delivery of QIPP later in the year above trend. • Marginal Rate: Has been applied according to the specification agreed within each signed contract.
• Corrections to provider data: Where providers have billed items that should sit outside of the contract this expenditure has been removed, for example, MSK and Rehab at RFL. Estimates have also been added for any costs not included with the provider data, for
example Commissioning for Quality and Innovation (CQUIN).• Challenges: Claims and challenges considered likely to be successful are included within the reported positions.
Risks:
• Material QIPP delivery is required to meet CCG Financial Plans.
• More granular and accurate coding by Trusts could increase the acuity and therefore tariff charged by Providers.• Forecasting for winter months is based on historic trends. There is no provision for activity in winter months in excess of historic trends.
• If Referral to Treat (RTT) backlogs were reduced this would increase costs in contrast to the planned position of maintaining the RTT backlog at current levels. This could happen under instructions from NHSE and communications have been received by providers and
commissioners to undertake a detailed activity and performance review. Further details on RTT are included in the Performance and Quality paper.
• There has been a change to the Emergency Care Data Set (ECDS) in 2018/19 which is planned to be cost neutral. Indicative analysis suggests this to be true but will require ongoing monitoring.
• UCLH will be migrating to a new Patient Administration System (PAS) system in April 2019, currently there is not expected to be a risk to the 18/19 financial year, but this is being closely monitored.
46

Month 9 Acute Performance against
CCG Plans
5
The table below report the acute financial performance against CCG plans:
CCG plans assume delivery of a higher QIPP value, i.e., more savings, than the value of QIPP included in the signed
contracts.
Adverse / (Favourable)
Commissioner Provider YTD CCG Plan YTD Actual YTD Variance Annual CCG
Plan Annual Actual
Annual
Variance
Movement
from last
month
NHS Barnet CCG North Middlesex University Hospital NHS Trust 1,763,863 1,829,250 65,387 2,289,983 2,424,951 134,968 (29,451)
Royal Free London NHS FT 144,205,224 145,480,321 1,275,096 189,497,391 193,103,476 3,606,085 (1,075,718)
University College London Hospitals NHS FT 19,197,613 19,374,266 176,653 25,358,005 25,876,830 518,825 (1,036,299)
Whittington Health NHS Trust 8,428,680 8,284,083 (144,597) 11,117,575 10,972,489 (145,086) (529,152)
NHS Barnet CCG Total 173,595,380 174,967,920 1,372,539 228,262,954 232,377,745 4,114,791 (2,670,620)
NHS Camden CCG North Middlesex University Hospital NHS Trust 218,264 217,607 (657) 290,131 291,436 1,305 16,541
Royal Free London NHS FT 47,564,830 51,152,965 3,588,135 62,922,137 67,071,379 4,149,242 (875,571)
University College London Hospitals NHS FT 48,418,713 53,872,971 5,454,258 64,106,947 71,489,977 7,383,030 52,410
Whittington Health NHS Trust 7,558,285 8,221,553 663,268 10,014,047 10,932,367 918,320 30,941
NHS Camden CCG Total 103,760,092 113,465,096 9,705,005 137,333,262 149,785,158 12,451,896 (775,679)
NHS Enfield CCG North Middlesex University Hospital NHS Trust 81,109,377 85,950,655 4,841,278 108,145,838 114,297,794 6,151,955 2,644,592
Royal Free London NHS FT 58,326,849 61,771,575 3,444,726 77,769,137 81,985,845 4,216,708 (128,298)
University College London Hospitals NHS FT 12,239,973 12,289,552 49,580 16,319,969 16,523,928 203,958 106,369
Whittington Health NHS Trust 3,554,922 3,699,037 144,115 4,739,911 4,903,889 163,978 2,350
NHS Enfield CCG Total 155,231,121 163,710,819 8,479,699 206,974,855 217,711,455 10,736,600 2,625,013
NHS Haringey CCG North Middlesex University Hospital NHS Trust 58,965,337 62,912,857 3,947,519 77,145,845 82,627,469 5,481,624 141,777
Royal Free London NHS FT 16,162,128 16,318,579 156,451 21,157,207 21,605,528 448,321 120,170
University College London Hospitals NHS FT 16,723,641 17,776,457 1,052,816 21,879,963 23,869,162 1,989,199 (97,190)
Whittington Health NHS Trust 63,021,482 64,990,142 1,968,661 82,428,983 86,375,008 3,946,025 80,618
NHS Haringey CCG Total 154,872,588 161,998,035 7,125,447 202,611,998 214,477,167 11,865,169 245,375
NHS Islington CCG North Middlesex University Hospital NHS Trust 440,931 653,341 212,410 567,158 871,150 303,992 (17,519)
Royal Free London NHS FT 9,241,628 9,721,337 479,709 12,299,026 12,798,061 499,035 145,425
University College London Hospitals NHS FT 53,176,246 55,832,466 2,656,220 70,860,943 74,603,773 3,742,830 783,697
Whittington Health NHS Trust 74,779,528 76,633,568 1,854,040 99,492,696 101,693,613 2,200,917 72,293
NHS Islington CCG Total 137,638,333 142,840,712 5,202,379 183,219,823 189,966,597 6,746,774 983,896
Grand Total 725,097,514 756,982,581 31,885,068 958,402,892 1,004,318,122 45,915,230 407,984
47

Month 9 Acute Performance
(includes Out of Sector)
6
The table below reports the acute financial performance by provider against CCG plans:
For information, ‘Other Acute’ contains i) Private Providers ii) Overseas iii) London Ambulance Service (LAS) contract iv) Non
Contract Activity v) Service Level Agreement exclusions (e.g. activity at RFL outside the main contract) vi) Prior Year Impacts and
vii) Acute demand reserves.
The Acute £21.6m deterioration from last month is shown predominantly within ‘Other Acute’ and relates to a £15.7m adverse
change to Acute Demand Reserves and a £4.4m movement relating to Prior Year Acute Contracts.
The forecast outturn of £45.9m over performance across the four main acute contracts for the five CCGs is after the application
of marginal rates allowed for in contracts. At month nine marginal rates are forecast to yield £3.3m benefit to the CCGs in
2018/19. The underlying year-end over performance in acute providers on a full Payment by Results (PbR) tariff would therefore
be £49.2m at month nine.
Adverse / (Favourable)
ServiceProviderDescription
YTD Variance Annual CCG
Plan Annual Actual
Annual
Variance
Movement
from last
month
North Middlesex University Hospital NHS Trust 9,065,938 188,438,955 200,512,799 12,073,843 2,755,940
Royal Free London NHS FT 8,944,118 363,644,898 376,564,288 12,919,390 (1,813,992)
University College London Hospitals NHS FT 9,389,526 198,525,827 212,363,670 13,837,843 (191,014)
The Whittington Hospital NHS Trust 4,485,487 207,793,212 214,877,366 7,084,154 (342,950)
Sub Total 31,885,068 958,402,892 1,004,318,122 45,915,230 407,984
Other Provider Contracts 2,640,449 125,900,220 129,285,938 3,385,719 634,646
Other Acute 8,414,826 130,636,433 143,665,320 13,028,886 20,530,222
Grand Total 42,940,343 1,214,939,545 1,277,269,380 62,329,835 21,572,853
Commissioner FOT Marginal Rate Adjustment £
NHS Barnet CCG (318,528)
NHS Camden CCG (51,512)
NHS Enfield CCG (124,543)
NHS Haringey CCG (2,519,529)
NHS Islington CCG (274,042)
Grand Total (3,288,154)
48

Month 9 Acute Performance
(Other Providers)
7
The table below reports the acute financial performance at all NHS contracted acute providers, excluding the main four, this
includes out of sector providers:
Adverse / (Favourable)
ServiceProviderDescription
YTD Variance Annual CCG
Plan Annual Actual
Annual
Variance
Movement
from last
month
Barts Health NHS Trust 361,734 25,341,378 26,009,571 668,193 1,889
Moorfields Eye Hospital NHS Foundation Trust 333,813 19,959,505 20,506,593 547,088 32,353
Royal National Orthopaedic Hospital NHS Trust (174,133) 7,597,704 7,387,155 (210,549) 108,255
Barking, Havering and Redbridge University Hospitals NHS Trust 163,367 785,795 1,005,548 219,753 21,195
Imperial College Healthcare NHS Trust (207,146) 18,312,456 18,067,438 (245,017) 106,069
Royal Brompton & Harefield NHS Foundation Trust 208,917 1,920,724 2,123,467 202,743 0
The Royal Marsden NHS Foundation Trust 140,113 960,239 1,130,714 170,475 7,264
King's College Hospital NHS Foundation Trust 273,699 2,149,530 2,437,560 288,031 155,447
Great Ormond Street Hospital for Children NHS Foundation Trust 101,673 2,902,556 3,048,362 145,806 25,704
Chelsea and Westminster Hospital NHS Foundation Trust 397,415 3,297,467 3,811,672 514,205 (11,403)
The Princess Alexandra Hospital NHS Trust 72,567 586,188 680,865 94,676 24,444
Homerton University Hospital NHS Foundation Trust 207,558 13,427,972 13,534,801 106,829 20,901
West Hertfordshire Hospitals NHS Trust 79,501 1,303,000 1,411,339 108,339 27,710
Guy's and St Thomas' NHS Foundation Trust 199,643 12,829,560 12,985,247 155,687 90,381
St George's University Hospitals NHS Foundation Trust 90,508 1,072,978 1,174,895 101,917 (10,390)
London North West University Healthcare NHS Trust 391,221 13,453,168 13,970,712 517,544 34,829
Grand Total 2,640,449 125,900,220 129,285,938 3,385,719 634,646
49

Total QIPP (in and out of contract values)
at NCL Main Acute Providers
8
There is £13.5m QIPP included in the main four NCL acute Provider contracts and a further £50.9m acute QIPP planned at
these Providers by CCGs that has not been included within the contracts. Together, QIPP and QIPP out of contract total
£64.5m. Providers are committed to varying contracts on a QIPP by QIPP basis should they become satisfied further
QIPPs can be delivered. £36.4m of the planned QIPP is STP-wide QIPP and £28.1m represents CCGs’ local QIPP plans.
The table below shows the level of planned QIPP at each provider by CCG.
Provider Barnet Camden Enfield Haringey Islington Provider Total
Royal Free 9,946,850 5,569,831 7,681,395 1,289,000 533,167 25,020,242
NMUH 184,347 18,101 9,586,540 6,238,000 333,087 16,360,075
UCLH 598,372 7,062,966 283,960 1,124,000 4,070,188 13,139,486
Whittington 300,787 299,616 0 4,452,000 4,898,027 9,950,431
CCG Total 11,030,356 12,950,514 17,551,895 13,103,000 9,834,469 64,470,233
50
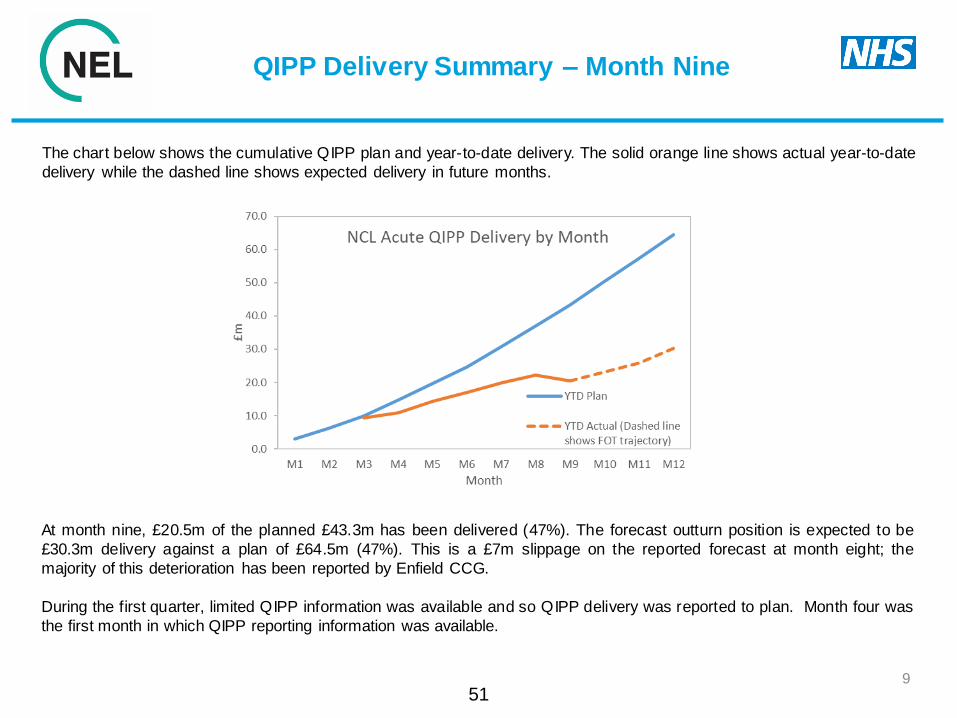
QIPP Delivery Summary – Month Nine
9
The chart below shows the cumulative QIPP plan and year-to-date delivery. The solid orange line shows actual year-to-date
delivery while the dashed line shows expected delivery in future months.
At month nine, £20.5m of the planned £43.3m has been delivered (47%). The forecast outturn position is expected to be
£30.3m delivery against a plan of £64.5m (47%). This is a £7m slippage on the reported forecast at month eight; the
majority of this deterioration has been reported by Enfield CCG.
During the first quarter, limited QIPP information was available and so QIPP delivery was reported to plan. Month four was
the first month in which QIPP reporting information was available.
51

QIPP Delivery by CCG
10
The table below shows delivery of gross QIPP at the four main NCL acute providers at month nine and the forecast outturn,
split by CCG. This is based on CCG reported positions.
At month nine, £20.5m of the planned £43.3m has been delivered (47%) with under delivery by worksteam detailed on the slide
after next.
All CCGs have reported a deterioration to their acute position compared to month eight with the greatest slippage reported by
Enfield CCG.
CCG Gross YTD Plan £ Gross YTD Actual £ Gross YTD Variance £ Gross FOT Plan £ Gross FOT Actual £ Gross FOT Variance £
Barnet CCG 6,446,773 5,436,060 -1,010,713 11,030,356 8,145,230 -2,885,126
Camden CCG 8,459,092 4,079,882 -4,379,210 12,950,514 7,672,410 -5,278,104
Enfield CCG 11,985,256 3,681,891 -8,303,364 17,551,895 4,909,189 -12,642,706
Haringey CCG 9,827,250 4,264,360 -5,562,890 13,103,000 5,869,649 -7,233,351
Islington CCG 6,593,298 3,030,548 -3,562,751 9,803,448 3,696,494 -6,106,954
Total 43,311,669 20,492,741 -22,818,928 64,439,212 30,292,971 -34,146,241
52

QIPP Delivery by Provider and by
Worksteam
11
The first table below shows delivery of gross QIPP at the four main NCL acute providers and the second table shows it by
Workstream. Both show the month nine position and forecast outturn based on the CCGs’ reported position.
At month nine, QIPP is under delivering at all providers by at least 40%.
Provider Gross YTD Plan £ Gross YTD Actual £Gross YTD Variance
£Gross FOT Plan £ Gross FOT Actual £
Gross FOT Variance £
North Middlesex University Hospital NHS Trust 11,767,773 4,173,836 -7,593,937 16,350,966 5,800,073 -10,550,893
Royal Free London NHS Foundation Trust 16,000,858 8,765,363 -7,235,495 25,021,233 13,324,926 -11,696,306
University College London Hospitals NHS Foundation Trust 8,569,502 4,943,407 -3,626,096 13,112,621 7,748,700 -5,363,921
Whittington Health NHS Trust 6,973,536 2,610,135 -4,363,401 9,954,392 3,419,272 -6,535,121
Total 43,311,669 20,492,741 -22,818,928 64,439,212 30,292,971 -34,146,241
Workstream Gross YTD Plan £ Gross YTD Actual £ Gross YTD Variance £ Gross FOT Plan £ Gross FOT Actual £ Gross FOT Variance £
Health and Care Closer to Home 7,900,849 2,008,756 -5,892,094 11,781,588 3,518,405 -8,263,183
Urgent and Emergency Care 15,862,133 7,763,100 -8,099,033 23,061,088 10,490,956 -12,570,132
Planned Care 16,628,368 6,145,477 -10,482,891 24,893,421 10,111,575 -14,781,846
Other Acute Schemes 2,920,319 4,575,408 1,655,089 4,703,115 6,172,035 1,468,920
Total 43,311,669 20,492,741 -22,818,928 64,439,212 30,292,971 -34,146,241
Schemes relating to Urgent and Emergency Care (UEC) and Planned Care are showing the greatest under delivery. Further
detail relating to each scheme is shown on the following slides.53

Activity Trend Analysis
1254

Demand: GP Referred Activity
13
Overall Referral Trends
Published data indicates a decrease in GP referrals to NCL providers, but data issues and service changes at individual
providers make overall comparisons difficult. Commissioners receive local datasets from Trusts to allow analysis at specialty
and GP practice level. The annualised trend indicates a 2% decrease in referrals.
At Trust level, there have been reductions at North Middlesex University Hospital, Royal Free London and Whittington Health
with an increase seen at University College London Hospital. There has also been an increase in referrals to out-of-sector
providers, particularly to Barts Health and BMI.
A common theme across NCL is the increase in Two Week Wait (Suspected Cancer) demand. The cancer waiting times
dataset shows a 17% year on year increase in Two Week Wait activity. Analysis of First Outpatient First Attendance data shows
particular increases in Breast Surgery, Urology and Dermatology activity. Increases are thought to be due to a change in clinical
referral guidelines and increased public awareness. However, conversion rates from referral for suspected cancer to cancer
diagnosis have remained proportional, indicating that this increase in referral levels is appropriate.55

Outpatients: First Attendances
14
Month 8 YTD Position:
2017/18 Actuals 467,893
2018/19 YTD Operating Plan 486,140
2018/19 YTD CCG Plans with QIPP 454,453
2018/19 CCG Plans Without QIPP 488,396
2018/19 YTD Actuals 485,248
Year on Year Growth 17,355
Year on Year Growth % 3.7%
National Growth Expectation 6.4%
Operating Plan Variance -0.2%
CCG Plan Variance 6.8%
Treatment Functions with Greatest Year on Year Increases and Decreases HRG Subchapters with Greatest Year on Year Increases and Decreases
Treatment Function 17/18 YTD 18/19 YTD Change % Change Subchapter 17/18 YTD 18/19 YTD Change % Change
Diagnostic Imaging 123,276 130,330 7,054 6% HN - Orthopaedic Non-Trauma Procedures 1,655 1,780 125 8%
Ophthalmology 20,846 22,754 1,908 9% FZ - Digestive System Procedures and Disorders 1,782 1,977 195 11%
Colorectal Surgery 9,267 10,394 1,127 12% LB - Urological and Male Reproductive System Procedures and Disorders 1,981 2,284 303 15%
ENT 14,689 15,632 943 6% MA - Female Reproductive System Procedures 14,742 15,599 857 6%
General Medicine 9,669 10,765 1,096 11% WF - Non-admitted Consultations 393,502 414,312 20,810 5%
Clinical Neuro-Physiology 2,711 2,294 -417 -15% BZ - Eyes and Periorbita Procedures and Disorders 6,539 5,431 -1,108 -17%
Gynaecological Oncology 3,457 2,793 -664 -19% CA - Ear, Nose, Mouth, Throat and Neck Procedures 7,809 7,138 -671 -9%
Neurology 7,780 7,289 -491 -6% EY - Interventional Cardiology for Acquired Conditions 16,481 16,014 -467 -3%
Respiratory Physiology 4,787 4,223 -564 -12% JC - Skin Procedures 10,799 10,339 -460 -4%
Vascular Surgery 4,091 3,527 -564 -14% NZ - Obstetric Medicine 4,303 3,866 -437 -10%
Total (All Treatment Functions) 467,893 485,248 17,355 3.7% Total (All HRG Subchapters) 467,893 485,248 17,355 3.7%
Provider Summary CCG Summary
Provider 17/18 YTD 18/19 YTD Change % Change CCG 17/18 YTD 18/19 YTD Change % Change
Royal Free London 162,046 158,119 -3,927 -2% Barnet 106,063 108,389 2,326 2%
North Middlesex 54,227 54,715 488 1% Camden 82,004 79,989 -2,015 -2%
UCLH 74,094 74,847 753 1% Enfield 91,536 97,834 6,298 7%
Whittington 89,126 94,995 5,869 7% Haringey 99,044 106,512 7,468 8%
Other Providers 88,400 102,572 14,172 16% Islington 89,246 92,524 3,278 4%
Total 467,893 485,248 17,355 4% Total 467,893 485,248 17,355 4%
48,000
50,000
52,000
54,000
56,000
58,000
60,000
62,000
64,000
66,000
68,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient First Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans 18/19 Actuals
48000
50000
52000
54000
56000
58000
60000
62000
64000
66000
68000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient First Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans 18/19 Actuals
56

Outpatients: Follow ups
15
Month 8 YTD Position:
2017/18 Actuals 775,224
2018/19 YTD Operating Plan 803,830
2018/19 YTD CCG Plans with QIPP 783,161
2018/19 CCG Plans Without QIPP 806,692
2018/19 YTD Actuals 769,446
Year on Year Growth 5,778-
Year on Year Growth % -0.7%
National Growth Expectation 4.1%
Operating Plan Variance -4.3%
CCG Plan Variance -1.8%
Treatment Functions with Greatest Year on Year Increases and Decreases HRG Subchapters with Greatest Year on Year Increases and Decreases
Treatment Function 17/18 YTD 18/19 YTD Change % Change Subchapter 17/18 YTD 18/19 YTD Change % Change
Diagnostic Imaging 92,619 95,073 2,454 3% AB - Pain Management 3,209 3,411 202 6%
Ophthalmology 80,457 82,732 2,275 3% BZ - Eyes and Periorbita Procedures and Disorders 41,007 44,117 3,110 8%
Colorectal Surgery 9,923 10,886 963 10% FZ - Digestive System Procedures and Disorders 858 1,200 342 40%
Urology 34,865 36,301 1,436 4% LB - Urological and Male Reproductive System Procedures and Disorders 6,638 7,265 627 9%
Gastroenterology 26,481 27,315 834 3% NZ - Obstetric Medicine 5,453 5,619 166 3%
Anticoagulant Service 75,255 64,893 -10,362 -14% CA - Ear, Nose, Mouth, Throat and Neck Procedures 9,683 8,459 -1,224 -13%
ENT 22,464 20,904 -1,560 -7% DZ - Respiratory System Procedures and Disorders 3,653 3,295 -358 -10%
General Medicine 19,858 18,833 -1,025 -5% JC - Skin Procedures 23,458 22,119 -1,339 -6%
Paediatrics 13,466 11,749 -1,717 -13% WF - Non-admitted Consultations 657,472 652,411 -5,061 -1%
Trauma & Orthopaedics 59,138 58,094 -1,044 -2% YR - Vascular Imaging Interventions 660 445 -215 -33%
Total (All Treatment Functions) 775,224 769,446 -5,778 -0.7% Total (All HRG Subchapters) 775,224 769,446 -5,778 -0.7%
Provider Summary CCG Summary
Provider 17/18 YTD 18/19 YTD Change % Change CCG 17/18 YTD 18/19 YTD Change % Change
Royal Free London 269,325 253,377 -15,948 -6% Barnet 192,233 188,469 -3,764 -2%
North Middlesex 138,551 139,105 554 0% Camden 123,393 122,238 -1,155 -1%
UCLH 168,854 169,632 778 0% Enfield 177,404 175,758 -1,646 -1%
Whittington 90,771 92,718 1,947 2% Haringey 154,806 156,534 1,728 1%
Other Providers 107,723 114,614 6,891 6% Islington 127,388 126,447 -941 -1%
Total 775,224 769,446 -5,778 -1% Total 775,224 769,446 -5,778 -1%
60,000
65,000
70,000
75,000
80,000
85,000
90,000
95,000
100,000
105,000
110,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient Follow Up Activity
Series1 Series2 Series4
80,000
85,000
90,000
95,000
100,000
105,000
110,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient Follow Up Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans with QIPP 18/19 Actuals
60000
65000
70000
75000
80000
85000
90000
95000
100000
105000
110000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient Follow Up Activity
Series1 Series2 Series4
80000
85000
90000
95000
100000
105000
110000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Outpatient Follow Up Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans with QIPP 18/19 Actuals
57

Elective Activity: Planned Care
Month 8 YTD Position:
2017/18 Actuals 104,653
2018/19 YTD Operating Plan 106,501
2018/19 YTD CCG Plans with QIPP 103,417
2018/19 CCG Plans Without QIPP 108,312
2018/19 YTD Actuals 105,777
Year on Year Growth 1,124
Year on Year Growth % 1.1%
National Growth Expectation 3.6%
Operating Plan Variance -0.7%
CCG Plan Variance 2.3%
Treatment Functions with Greatest Year on Year Increases and Decreases HRG Subchapters with Greatest Year on Year Increases and Decreases
Treatment Function 17/18 YTD 18/19 YTD Change % Change Subchapter 17/18 YTD 18/19 YTD Change % Change
Ophthalmology 7,783 8,437 654 8% JA - Breast Procedures and Disorders 1,596 1,854 258 16%
Dermatology 4,712 5,470 758 16% JC - Skin Procedures 5,413 6,095 682 13%
Gastroenterology 21,924 23,708 1,784 8% BZ - Eyes and Periorbita Procedures and Disorders 7,643 8,277 634 8%
General Medicine 304 500 196 64% FZ - Digestive System Procedures and Disorders 28,939 30,482 1,543 5%
Medical Oncology 5,159 5,743 584 11% SA - Haematological Procedures and Disorders 5,057 5,496 439 9%
Colorectal Surgery 3,888 3,667 -221 -6% HN - Orthopaedic Non-Trauma Procedures 6,246 5,611 -635 -10%
General Surgery 5,389 4,885 -504 -9% LB - Urological and Male Reproductive System Procedures and Disorders 7,952 7,313 -639 -8%
Gynaecology 4,677 4,375 -302 -6% MA - Female Reproductive System Procedures 3,996 3,719 -277 -7%
Trauma & Orthopaedics 8,444 7,330 -1,114 -13% SB - Chemotherapy 7,725 7,524 -201 -3%
Urology 7,728 6,947 -781 -10% YR - Vascular Imaging Interventions 2,815 2,433 -382 -14%
Total (All Treatment Functions) 104,653 105,777 1,124 1.1% Total (All HRG Subchapters) 104,653 105,777 1,124 1.1%
Provider Summary CCG Summary
Provider 17/18 YTD 18/19 YTD Change % Change CCG 17/18 YTD 18/19 YTD Change % Change
Royal Free London 33,341 30,738 -2,603 -8% Barnet 25,387 24,689 -698 -3%
North Middlesex 18,230 18,820 590 3% Camden 15,665 15,376 -289 -2%
UCLH 25,424 26,351 927 4% Enfield 25,731 26,337 606 2%
Whittington 11,478 12,001 523 5% Haringey 21,188 22,583 1,395 7%
Other Providers 16,180 17,867 1,687 10% Islington 16,682 16,792 110 1%
Total 104,653 105,777 1,124 1% Total 104,653 105,777 1,124 1%
(The LOS is from 'raw' SUS data rather than the NCDR 'Operating Plan' dataset so totals will not match with the above)
Length of Stay
Length of Stay 17/18 YTD 18/19 YTD Change % Change
0 Days 89,146 91,908 2,762 3%
1 Day 5,455 4,982 -473 -9%
2-7 Days 4,747 4,591 -156 -3%
8-20 Days (Stranded Patients) 848 684 -164 -19%
Over 21 Days (Super Stranded Patients) 384 310 -74 -19%
Total 100,580 102,475 1,895 2%
8,500
9,500
10,500
11,500
12,500
13,500
14,500
15,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Elective Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans with QIPP 18/19 Actuals
58

Activity Deep Dive
Unplanned Care : Non-elective Admissions
Month 8 YTD Position:
2017/18 Actuals 80,917
2018/19 YTD Operating Plan 85,255
2018/19 YTD CCG Plans with QIPP 79,748
2018/19 CCG Plans Without QIPP 86,541
2018/19 YTD Actuals 84,315
Year on Year Growth 3,398
Year on Year Growth % 4.2%
National Growth Expectation 2.3%
Operating Plan Variance -1.1%
CCG Plan Variance 5.7%
Treatment Functions with Greatest Year on Year Increases and Decreases HRG Subchapters with Greatest Year on Year Increases and Decreases
Treatment Function 17/18 YTD 18/19 YTD Change % Change Subchapter 17/18 YTD 18/19 YTD Change % Change
Accident & Emergency 16,527 19,216 2,689 16% HD - Musculoskeletal and Rheumatological Disorders 1,550 1,902 352 23%
Cardiology 1,604 1,800 196 12% LA - Renal Procedures and Disorders 3,096 3,632 536 17%
General Medicine 23,525 23,968 443 2% DZ - Respiratory System Procedures and Disorders 6,919 7,400 481 7%
General Surgery 6,911 7,226 315 5% EB - Cardiac Disorders 6,871 7,238 367 5%
Neurology 569 938 369 65% LB - Urological and Male Reproductive System Procedures and Disorders 2,331 2,732 401 17%
Diabetic Medicine 70 22 -48 -69% HT - Orthopaedic Trauma Procedures 2,013 1,839 -174 -9%
Medical Oncology 837 775 -62 -7% PB - Neonatal Disorders 3,142 2,424 -718 -23%
Neonatology 2,851 2,155 -696 -24% PW - Paediatric Infectious Diseases 2,737 2,549 -188 -7%
Rehabilitation 359 171 -188 -52% PX - Paediatric Medicine 1,895 1,734 -161 -8%
Respiratory Medicine (Also Known as Thoracic Medicine) 670 485 -185 -28% WJ - Infectious Diseases and Immune System Disorders 2,496 1,947 -549 -22%
Total (All Treatment Functions) 80,917 84,315 3,398 4.2% Total (All HRG Subchapters) 80,917 84,315 3,398 4.2%
Provider Summary CCG Summary
Provider 17/18 YTD 18/19 YTD Change % Change CCG 17/18 YTD 18/19 YTD Change % Change
Royal Free London 25,836 28,309 2,473 10% Barnet 20,076 21,729 1,653 8%
North Middlesex 20,289 21,359 1,070 5% Camden 11,936 12,145 209 2%
UCLH 12,217 12,206 -11 0% Enfield 19,770 20,897 1,127 6%
Whittington 11,600 11,079 -521 -4% Haringey 16,197 16,671 474 3%
Other Providers 10,975 11,362 387 4% Islington 12,938 12,873 -65 -1%
Total 80,917 84,315 3,398 4% Total 80,917 84,315 3,398 4%
(The LOS is from 'raw' SUS data rather than the NCDR 'Operating Plan' dataset so totals will not match with the above)
Length of Stay
Length of Stay 17/18 YTD 18/19 YTD Change % Change
0 Days 25,891 29,303 3,412 13%
1 Day 17,730 17,610 -120 -1%
2-7 Days 24,916 25,058 142 1%
8-20 Days (Stranded Patients) 9,097 9,332 235 3%
Over 21 Days (Super Stranded Patients) 4,414 4,021 -393 -9%
Total 82,048 85,324 3,276 4%
8,500
9,000
9,500
10,000
10,500
11,000
11,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL Elective Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans with QIPP 18/19 Actuals
59

Activity Deep Dive
Unscheduled Care : Accident & Emergency (A&E)
Month 8 YTD Position:
2017/18 Actuals 483,671
2018/19 YTD Operating Plan 492,607
2018/19 YTD CCG Plans with QIPP 442,623
2018/19 CCG Plans Without QIPP 497,312
2018/19 YTD Actuals 497,025
Year on Year Growth 13,354
Year on Year Growth % 2.8%
National Growth Expectation 1.1%
Operating Plan Variance 0.9%
CCG Plan Variance 12.3%
HRG Code with Greatest Year on Year Increases and Decreases Provider Summary
HRG Code/Description 17/18 YTD 18/19 YTD Change % Change Provider 17/18 YTD 18/19 YTD Change % Change
UZ01Z - Data Invalid for Grouping 0 405 405 130% Royal Free London 129,053 136,291 7,238 6%
VB01Z - Emergency Medicine, Any Investigation with Category 5 Treatment 308 191 -117 -38% North Middlesex 100,352 102,323 1,971 2%
VB02Z - Emergency Medicine, Category 3 Investigation with Category 4 Treatment 6031 5778 -253 -4% UCLH 55,925 56,758 833 1%
VB03Z - Emergency Medicine, Category 3 Investigation with Category 1-3 Treatment 20151 22318 2167 11% Whittington 58,657 62,112 3,455 6%
VB04Z - Emergency Medicine, Category 2 Investigation with Category 4 Treatment 20829 20328 -501 -2% Other Providers 139,684 139,541 -143 0%
VB05Z - Emergency Medicine, Category 2 Investigation with Category 3 Treatment 7591 5969 -1622 -21% Total 483,671 497,025 13,354 3%
VB06Z - Emergency Medicine, Category 1 Investigation with Category 3-4 Treatment 14118 11947 -2171 -15% CCG SummaryVB07Z - Emergency Medicine, Category 2 Investigation with Category 2 Treatment 36887 46915 10028 27%
VB08Z - Emergency Medicine, Category 2 Investigation with Category 1 Treatment 106658 121028 14370 13% CCG 17/18 YTD 18/19 YTD Change % Change
VB09Z - Emergency Medicine, Category 1 Investigation with Category 1-2 Treatment 165236 183511 18275 11% Barnet 133,205 135,245 2,040 2%
VB10Z - Emergency Medicine, Dental Care 164 121 -43 -26% Camden 80,694 82,514 1,820 2%
VB11Z - Emergency Medicine, No Investigation with No Significant Treatment 105633 78453 -27180 -26% Enfield 109,523 114,339 4,816 4%
VB99Z - Emergency Medicine, Patient Dead On Arrival 65 61 -4 -6% Haringey 90,895 93,750 2,855 3%
Total 483,671 497,025 13,354 3% Islington 69,354 71,177 1,823 3%
Total 483,671 497,025 13,354 3%
50,000
52,000
54,000
56,000
58,000
60,000
62,000
64,000
66,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NCL A&E Activity
18/19 Op Plan 2018/19 CCG Plans Without QIPP 2018/19 CCG Plans with QIPP 18/19 Actuals
60

1
NCL Joint Commissioning Committee Thursday, 7 February 2019
Report Title NCL Acute Services Quality & Performance Report – as at January 2019
Date of report: 28 January 2019
Agenda Item
3.2
Lead Director /
Manager
Paul Sinden Director of Performance, Planning and Primary Care for NCL CCGs
Tel/Email [email protected]
GB Member Sponsor
Not Applicable
Report Author
Helen Boswell Associate Director Performance Improvement and Service Transformation NEL CSU Ed Nkrumah Director of Performance for NCL CCGs
Tel/Email [email protected] [email protected]
Report Summary
This report provides a summary of the operational performance across NCL acute providers and the actions to address areas for improvement in 2018/19. The report also includes updates on patient safety, patient experience and service quality impacted by operational service performance. The exception reports summarise the key issues impacting across NCL and individual CCGs for the following providers:
North Middlesex University Hospital;
Royal Free London Hospital; University College London Hospital;
Whittington Health;
Royal National Orthopaedic Hospital and Moorfields Eye Hospital London Central and West Unscheduled Care Collaborative - Integrated Urgent Care service (NHS 111 and GP out-of-hours) provider;
London Ambulance Service. The detailed NCL Acute Services Quality and Performance Report for November 2018 is available here.
Recommendation The NCL Joint Commissioning Committee is asked to:
COMMENT on the actions being taken to deliver improvements in service quality and operational performance across NCL;
APPROVE the NCL JCC Quality and Performance Report, January 2019.
Identified Risks
and Risk
The main risks and mitigations to note are included in the risk register for the Joint Commissioning Committee and include:
61

2
Management
Actions
Performance risks to delivery of NHS Constitution Standards for Accident and Emergency, Cancer 62-days and Referral to Treatment (Royal Free London in particular) in 2018/19;
The increasing number of never events at Royal Free London.
Conflicts of Interest Conflicts of interest are managed robustly and in accordance with the NCL Conflicts of Interest Policy.
Resource
Implications
Not applicable.
Engagement The report is presented to the NCL CCG Joint Commissioning Committee which includes elected GP representatives, lay members, Healthwatch, Public Health and representatives from each NCL London Borough.
Equality Impact
Analysis
This report was written in accordance with the provisions of the Equality Act 2010.
Report History and
Key Decisions
Not applicable.
Next Steps The NCL Acute Performance and Quality Report will now be used at individual CCG Committee and Governing Body meetings to provide an overview of performance and quality with NCL CCGS and acute providers. The report will be further developed in response to feedback from the Joint Commissioning Committee and CCG Committees.
Appendices
Full report available on request.
62

3
NCL Acute Quality & Performance Summary Report
January 2019
1. Introduction
This paper focuses on progress being made in addressing operational performance and quality of
service issues in the following key areas:
Patient Experience
Never Events & Serious Incidents
Urgent and Emergency Care
Referral to Treatment Waiting Times
Cancer Waiting Times
Diagnostics Waiting Times
2. Patient Experience
North Middlesex University Hospital continues to report the lowest Friends and Family Test A&E
score in London. Trust score declined further in November 2018 (66%) compared to previous month
(68%). The Trust’s Patient Experience Improvement Plan is monitored at the monthly Clinical Quality
Review Group meetings with commissioners. The Plan focuses on embedding pathway changes to
improve patient experience as well as improving response rates, which is currently below 10%,
through text messages and electronic surveys. It is anticipated that the rebuild of the emergency
department will have a positive impact on patients’ experience of the service. The Clinical Quality
Review Group is also overseeing the improvement plan for outpatient patient experience which
continues to track below the NCL average of 92%.
The London and NCL Cancer Commissioning Boards have reviewed the recently published national
cancer patient experience survey results for 2017. The survey shows NCL providers maintaining high
scores or improving on their overall scores from previous year, with the exception of Royal Free
London (RFL) which reported a decline. RFL has started a process of analysing the results in detail
to inform their improvement plan which will be monitored at a local and STP level. Further targeted
work on patient communication which is a recurring issue across primary and secondary care will be
undertaken across NCL.
3. Never Events & Serious Incidents
Two Never Events were reported by NCL acute providers in December 2018 – a wrong site surgical
procedure at Whittington Health (discovered before surgery was performed) and wrong site surgery
at Royal Free London. These events will be investigated by each Trust as per the Serious Incident
procedure which includes producing a final written investigation report and associated action plan.
This brings the total number of Never Events reported in 2018/19 at Royal Free London to ten. The
Trust presents progress against the Never Events Assurance Plan at each Clinical Quality Review
Group meeting. The Trust Executive Team, Barnet CCG (as lead commissioner) and NHS
Improvement are working together to deliver sustained improvements.
4. Accident & Emergency Performance and Winter Resilience
Performance against the 4-hour A&E waiting time standard in 2018/19 has been variable with a
marginal deterioration in December 2018, coinciding with the start of winter. In spite of recent
challenges at North Middlesex and Barnet Hospitals, the system has worked together well and
responded better to operational challenges this year resulting in fewer escalations compared to
previous years. All NCL Trusts have also delivered improvements in ambulance handovers, reducing
63
4
the number of 30 and 60-minute delays by 30% and 70% respectively over the last 12 months.
Commissioners will be working with stakeholders in the coming months on a trajectory to eliminate
handover delays in line with national guidance.
Local A&E Delivery Boards are maintaining a strong focus on improving discharge rates by
supporting “stranded patients” (hospital stays beyond 21 days) and redirection to primary care
access hubs to reduce demand where possible.
5. London Ambulance Service (LAS)
Ambulance response times across North Central London have been poor over the last six months,
especially for Barnet, Enfield and Haringey patients requiring an emergency (category 2) or urgent
(category 3) response. The Trust cites the relative distance between these outer-London boroughs
and the specialist centres located in central London, where patients are often conveyed to, as one of
the key reasons for the limited availability of ambulances locally to respond prompt ly to call-outs.
At an aggregate level, response times in NCL declined in December 2018 with only the Category 1
(life threatening) standards being met. Actions being taken by LAS to improve performance and
reduce variation across NCL include:
• Providing an additional overlay vehicle in the boroughs of Enfield, Haringey and Barnet.
• From February 2019 a new layer of rosters will be introduced in Camden and Islington . This is
aimed at allocating resources more evenly across the five NCL boroughs to reduce variation
in performance.
• Local Recovery Plans and a designated Location Group Manager for NCL to be appointed to
look at specific local recovery plans for categories 2 and 3 standards.
• Resource modelling is being developed to improve admission avoidance.
6. Integrated Urgent Care (NHS 111 and Out-of-Hours Service)
London Central West Unscheduled Care Collaborative (LCW) met all but one of the agreed national
and local performance indicators. The local NCL roadmap standard of 85% for calls answered within
60 seconds was marginally missed in December 2018 (84.1%) due primarily to an increase in calls
by 3,440 to 27,837. The service was also adversely impacted, particularly during call surges, by high
incidence of staff sickness.
However, between 15th December 2018 and 1 January 2019, the provider achieved a service level of
89.6% on average and above 95% on some days during of the bank holiday period. There has been
a significant increase in staff recruited to cover the winter period and further recruitment has
recommenced following the Christmas break.
7. Referral to Treatment Waiting Times
Overall, NCL CCGs did not meet the national referral to treatment NHS Constitutional standard of
ensuring that 92% of patients wait no longer than 18 weeks from referral to treatment. This under-
performance was primarily due the reported positions at University College London Hospital (90%)
and Royal Free London (76%). UCLH’s plan to return to compliance by March 2019 is being closely
monitored. Harm review processes are in place for patients waiting longer the 52 weeks to start
treatment.
NCL providers are on track to deliver the national ambition to maintain waiting lists within March 2018
levels with the exception of Royal Free London due to their data quality issues.
64

5
The Royal Free London Trust board has been considering the next steps following the review of their
RTT data which confirmed the data quality issues with current reports were material and
recommended a programme of work to resolve the issues identified, including an extensive data
validation exercise. The board plans to make a decision in February 2019 on whether or not to stop
RTT reporting nationally based on their assessment of the risks and implications of the options that
are available to them. Commissioners continue to work closely with the Trust and regulators to
ensure risk to patients are minimised and validations can be commenced as soon as possible.
The NCL RTT Delivery Group continues to focus on facilitating mutual aid with regard to elective
capacity between providers. The group is supporting the implementation of the Capacity Alert
System on the national electronic referral system for pain management service at Royal Free
London. The alert will offer UCLH pain management service as an alternative for a limited period to
reduce the pressure on the service at Royal Free London.
8. Cancer Waiting Times
In November 2018, NCL providers achieved aggregate performance of 74% against the 85% 62 -day
cancer waiting time operational standard, an improvement on previous month (72% in October 2018)
and 34 breaches from target. Of particular concern was a sharp decline in performance at UCLH to
58%, raising further concerns about the Trust’s operational resilience to recover performance.
The prostate pathway, with UCLH as the specialist centre for NCL, remains a major contributory
factor to the poor performance and an ongoing risk to recovery. Patients on a prostate cancer
pathway (often transferred between Trusts) accounted for approximately half of all breaches in
November 2018. A significant proportion of breaches in other tumour sites, in particular, breast,
gynaecology and head and neck were also associated with shared pathways.
Improvement actions focused on streamlining pathways and increasing capacity are being
progressed at provider and sector level, overseen by the newly established Task and Finish Group
for North Central and East London STPs. Commissioners will be writing to UCLH to seek further
assurance on their recovery plans and trajectories in light of the recent deterioration in performance.
A governance review of the UCLH Cancer Collaborative, hosted by UCLH is also underway. Detailed
review of recovery plans and modelling to establish when NCL will return to compliance is being
undertaken.
9. Diagnostics Waiting Times
NCL CCGs, on aggregate, marginally missed the diagnostic standard in November 2018 with
performance of 98.9% against the target of 99.0%. This was primarily due to capacity pressures at
the Royal Free London in echocardiography and endoscopy. The Trust have reported that
endoscopy services are moving to a joint leadership structure in order to improve service delivery
and optimise capacity across the different hospital sites. Cardiology services are also preparing a
business case for the Trust Board to expand echocardiography services.
65

6
Table 1 - NCL CCG Performance Scorecard
Data Source: NHS Digital via North East London Information Exchange
Table 2 - NCL Provider Scorecard
Data Source: NHS Digital via North East London Information Exchange
Measure Date%Const
Standard
Referral to Treatment: 90% admitted
performance n/a 75.77% 80.70% 71.48% 78.11% 82.10% 76.84%
Referral to Treatment: 95% non-admittedn/a 87.07% 90.89% 87.53% 91.24% 91.92% 89.54%
Referral to Treatment: 92% incomplete92% 80.03% 86.84% 81.45% 90.27% 91.40% 85.06%
Cancer waits: 2 week All Cancers93% 91.10% 93.80% 89.90% 93.80% 93.60% 92.20%
Cancer waits: 2 week breast symptomatic 93% 95.60% 87.50% 95.00% 95.40% 93.90% 93.80%
Cancer waits: 31 days diagnosis to
treatment 96% 99.00% 97.80% 95.80% 100.00% 97.70% 97.90%
Cancer waits: 31 days diagnosis to
treatment subsequent drug treatment 98% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Cancer waits: 31 days diagnosis to
treatment subsequent surgery 94% 85.20% 85.70% 100.00% 100.00% 100.00% 91.70%
Cancer waits: 31 days treatment
subsequent radiotherapy 94% 89.70% 100.00% 90.00% 91.30% 95.50% 93.10%
Cancer waits: 62 days referral to treatment85% 78.10% 95.50% 70.30% 82.10% 65.60% 76.50%
Cancer waits: 62 days referral to treatment
- referral from screening90% 0.00% 85.70% 66.70% 83.30% n/a 73.90%
Cancer waits 62 days upgraden/a 88.90% 100.00% 91.70% 100.00% 100.00% 93.80%
Diagnostic waits less than 6 weeks99% 97.88% 99.61% 99.00% 99.36% 99.17% 98.90%
Nov-18
NCL STPIslingtonHaringeyEnfieldBarnet Camden
MeasureDate %Const
StandardFour-hour max wait in A&E Dec-18 99.17% 85.30% 83.20% 82.80% 88.52% 85.90%
RTT: 90% admitted performance n/a 83.45% 78.75% 81.62% 70.83% 73.53% 81.16% 69.02% 77.53%
RTT: 95% non-admitted n/a 89.95% 93.86% 94.08% 85.09% 86.32% 90.74% 91.41% 90.41%
RTT: 92% incomplete 92% 92.13% 94.63% 95.81% 90.28% 75.51% 90.45% 92.11% 86.31%
Cancer waits: 2 week All Cancers 93% 87.50% 94.30% 93.70% 89.70% 93.90% 93.70% 91.80%
Cancer waits: 2 week breast symptomatic 93% 93.20% 94.10% 90.20% 100.00% 93.40%
Cancer waits: 31 days 1st Definitive
Treatment 96% 100.00% 100.00% 97.50% 100.00% 98.10% 96.00% 100.00% 97.30%
Cancer waits: 31 days diagnosis to treatment
subsequent drug treatment 98% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% Cancer waits: 31 days diagnosis to treatment
subsequent surgery 94% 77.20% 100.00% 100.00% 100.00% 96.10% 89.40% 100.00% 91.50%
Cancer waits: 31 days treatment subsequent
radiotherapy 94% 92.60% 100.00% 91.50% 93.20%
Cancer waits: 62 days referral to treatment85% 76.30% 83.30% 80.60% 58.10% 93.30% 73.60%
Cancer waits: 62 days referral to treatment -
referral from screening 90% 66.70% 79.10% 100.00% 75.00% 80.00%
Cancer waits 62 days upgrade n/a 100.00% 97.40% 100.00% 84.30% 84.70% 100.00% 90.10%
Diagnostic waits > 6 wks 99% 97.10% 100.00% 99.70% 99.60% 98.20% 99.20% 99.10% 98.70%
Nov-18
NCL
STP WhittGOSH Moorfields NMUH RNOH RFL UCLH
66
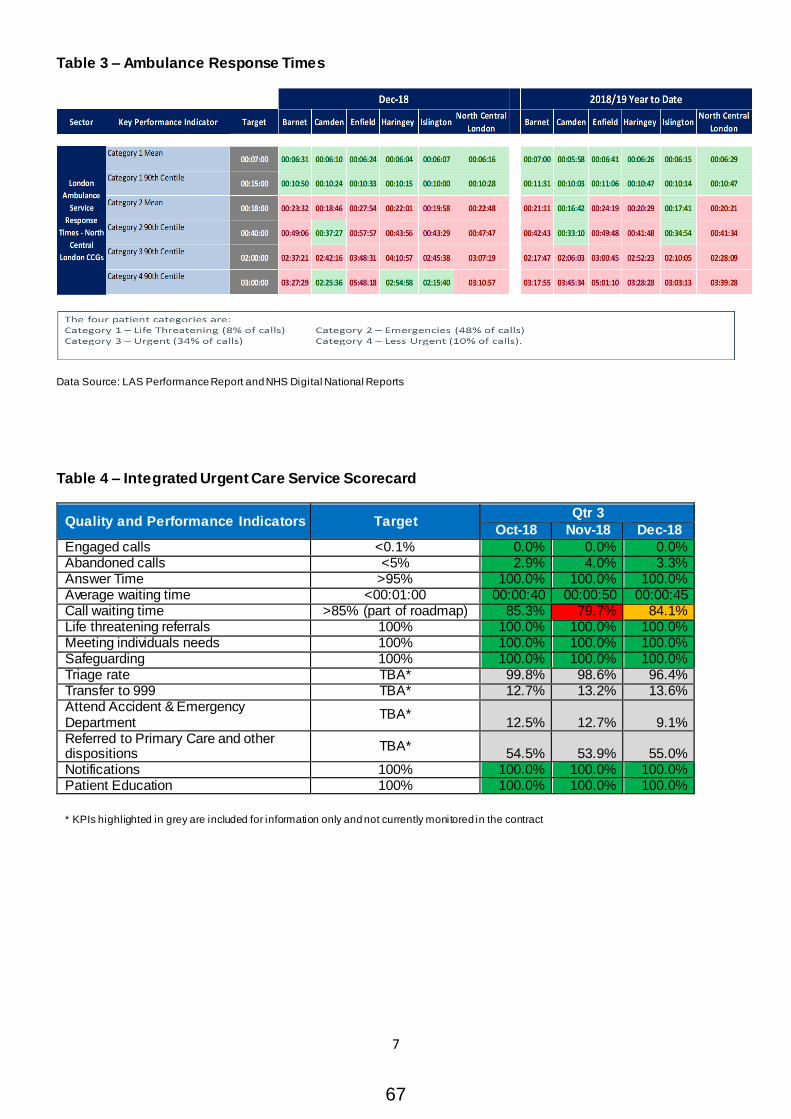
7
Table 3 – Ambulance Response Times
Data Source: LAS Performance Report and NHS Digital National Reports
Table 4 – Integrated Urgent Care Service Scorecard
Quality and Performance Indicators Target Qtr 3
Oct-18 Nov-18 Dec-18
Engaged calls <0.1% 0.0% 0.0% 0.0% Abandoned calls <5% 2.9% 4.0% 3.3% Answer Time >95% 100.0% 100.0% 100.0% Average waiting time <00:01:00 00:00:40 00:00:50 00:00:45 Call waiting time >85% (part of roadmap) 85.3% 79.7% 84.1% Life threatening referrals 100% 100.0% 100.0% 100.0% Meeting individuals needs 100% 100.0% 100.0% 100.0% Safeguarding 100% 100.0% 100.0% 100.0% Triage rate TBA* 99.8% 98.6% 96.4% Transfer to 999 TBA* 12.7% 13.2% 13.6% Attend Accident & Emergency Department
TBA* 12.5% 12.7% 9.1%
Referred to Primary Care and other dispositions
TBA* 54.5% 53.9% 55.0%
Notifications 100% 100.0% 100.0% 100.0% Patient Education 100% 100.0% 100.0% 100.0%
* KPIs highlighted in grey are included for information only and not currently monitored in the contract
67

1
NCL Joint Commissioning Committee Thursday, 7 February 2019
Report Title Transforming Care Programme Update
Date of
report 7 February 2019
Agenda
Item
3.3
Lead Director /
Manager
Paul Sinden Director of Performance, Planning and Primary Care NCL
Tel/Email [email protected]
GB Member
Sponsor
Report Author
Kath McClinton Assistant Director Islington CCG: Senior Responsible Officer (SRO) Transforming Care Programme
Tel/Email [email protected] 02036882921
Report Summary
Transforming Care is a national programme aimed at supporting people with learning disabilities to lead rewarding and fulfilling lives in the community and prevent the need for long term hospital care. North Central London is required to reduce the number of inpatient beds commissioned for people with a learning disability and/or autism from 81 to 48 or under by the end of March 2019, when the programme is due to end. This report updates the Committee on:
North Central London’s (NCL) improved performance against
the bed reduction trajectory. At the end of Quarter 3 there are
56 inpatients against a trajectory of 55 and it is estimated
NCL will end the programme in the region of 53 inpatients.
This represents a sustainable bed reduction of 35%
A £0.5m increase to the pressure reported to the Joint
Commissioning Committee in October 2018, from
Specialised Commissioning discharges
Confirmation that the Transforming Care Programme will be
extended beyond March 2019. Further detail on programme
requirements is awaited from NHS England, specifically in
relation to funding flows into 2019/20, and will be reported to
the Joint Commissioning Committee in the next update
report.
Recommendation The Joint Commissioning Committee is asked to NOTE the report.
68

2
Identified Risks
and Risk
Management
Actions
Failure to meet the bed reduction target by the end of March 2019; current programme management oversight of discharge planning will continue and support the resolution of barriers to discharge where practicable
Financial risk arising through the discharge of patients from Specialised Commissioning into locally funded care packages who are not eligible for funds to transfer under the NHS England Funding Transfer Agreement.
Conflicts of Interest
Any Conflicts of Interest are managed robustly and in accordance with the NCL Conflict of Interests Policy.
Resource
Implications
There is a £0.5m increase to the pressure reported to the Joint Commissioning Committee in October 2018. Recurrent impact from Specialised Commissioning discharges £3.8m, offset by £2.0m funding flowing in from NHS England. Net potential impact £1.8m ((£1.3m reported previously).
Engagement
The Transforming Care Board oversees implementation of the programme, with membership of the Board including CCG and Local Authority representatives; Mental Health Trusts; Primary Care; Family Carers and Healthwatch.
Equality Impact
Analysis
Not applicable to this report.
Report History
and Key
Decisions
This is a regular update to the North Central London Joint Commissioning Committee.
Next Steps The next steps for the Transforming Care Programme are to:
Continue with the current arrangements to support the timely
discharge of inpatients as planned to meet NCL’s trajectory;
Development of the programme structure 2019/20 once
further detail is confirmed by NHS England.
Appendices
Appendix 1: RAG rated discharge summary by Borough Appendix 2: Case studies
Which CCG does
this relate to
Barnet CCG, Camden CCG, Enfield CCG, Haringey CCG, Islington CCG
69

3
1. Introduction
Transforming Care is a national programme aimed at supporting people with learning disabilities to live rewarding and fulfilling lives in the community and prevent the need for long term hospital care.
The three-year programme, established by NHS England in the wake of the abuse scandal at Winterbourne View Hospital, is due to end in March 2019. By the end of the Programme Transforming Care Partnerships (TCPs) will be expected to have met their targets for hospital bed reduction as set out by NHS England.
NCL partnership has 81 patients defined as being in the Transforming Care cohort and we are required to achieve a net reduction of 33 beds to arrive at a total of 48 inpatient beds or less by 31 March 2019. Patients in scope fall into two separate cohorts; one group is funded by the CCGs and the second group by NHS England through Specialist Commissioning. This report updates the Joint Commissioning Committee on North Central London’s Transforming Care Programme including current performance against the bed reduction trajectory; an overall summary of programme activity including six case studies; an updated projected financial impact of Specialised Commissioning discharges and a summary of programme priorities beyond March 2019.
2. Performance
As at 31 December 2018, the performance of the NCL Transforming Care Programme is closely aligned with trajectory (56 inpatients against a target of 55 for Q3), as illustrated in the table below. This is a significant improvement on the previously reported position, and whilst meeting the final Programme trajectory of 48 inpatients by March 2019 continues to be challenging, the progress so far represents a 31% reduction in inpatient bed use across NCL. This is in comparison with a national reduction of 18%. Admissions continue to occur (approximately 2 per month) and as performance is determined by the net inpatient figure, new admissions do impact on overall performance, and will continue to pose a risk to NCL’s performance through to the end of March. In November, NHSE introduced a fortnightly return which captures whether CCGs were aware of the risk of an individual being admitted, and whether any action (i.e. a Care and Treatment Review) was taken to try and prevent the admission. CCGs are further scrutinised where these two criteria have not been met. To date, NCL have not had any admissions where the individual was not known, or where action was not taken to try and prevent the admission.
In addition to the overall trajectory, performance is also measured against those patients identified as ‘long-stay’ i.e. those who have been in inpatient settings for at least five years. NCL has discharged three long-stay patients in Q3, which is a significant achievement when taking into consideration the
81 80 7885 82
70 67 65 62 60
57
5548
81 79 7680
71 6864 64 63 61
62
5641 4137 39 37 35 38 35 33 32 31 29
40 3833
4134 33 32 29 30 29 31
27
0
10
20
30
40
50
60
70
80
90
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Year 0 Year 1 (2016/17) Year 2 (2017/18) Year 3 (2018/19)
Nu
mb
er o
f In
pa
tiie
nts
NCL TCP Performance as at 31 December 2018
All Patients - Targets All Patients - Actual NCL CCG's NHSE
70
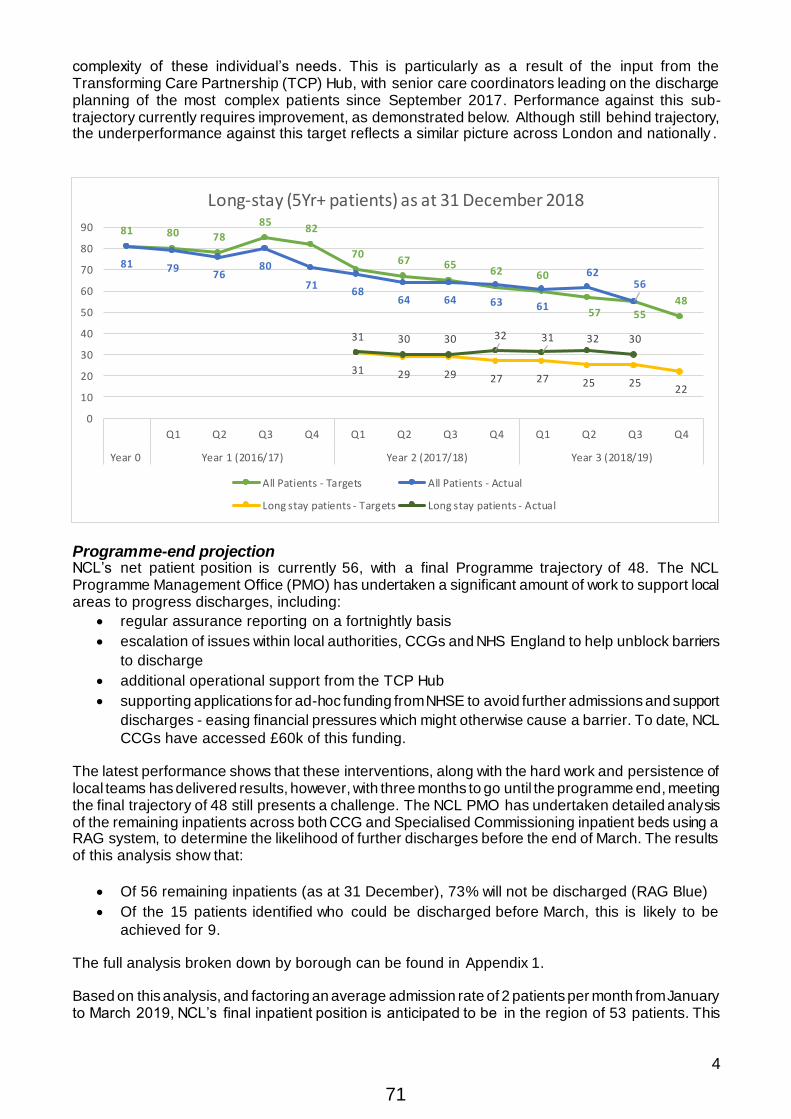
4
complexity of these individual’s needs. This is particularly as a result of the input from the Transforming Care Partnership (TCP) Hub, with senior care coordinators leading on the discharge planning of the most complex patients since September 2017. Performance against this sub-trajectory currently requires improvement, as demonstrated below. Although still behind trajectory, the underperformance against this target reflects a similar picture across London and nationally .
Programme-end projection NCL’s net patient position is currently 56, with a final Programme trajectory of 48. The NCL Programme Management Office (PMO) has undertaken a significant amount of work to support local areas to progress discharges, including:
regular assurance reporting on a fortnightly basis
escalation of issues within local authorities, CCGs and NHS England to help unblock barriers
to discharge
additional operational support from the TCP Hub
supporting applications for ad-hoc funding from NHSE to avoid further admissions and support
discharges - easing financial pressures which might otherwise cause a barrier. To date, NCL
CCGs have accessed £60k of this funding.
The latest performance shows that these interventions, along with the hard work and persistence of local teams has delivered results, however, with three months to go until the programme end, meeting the final trajectory of 48 still presents a challenge. The NCL PMO has undertaken detailed analysis of the remaining inpatients across both CCG and Specialised Commissioning inpatient beds using a RAG system, to determine the likelihood of further discharges before the end of March. The results of this analysis show that:
Of 56 remaining inpatients (as at 31 December), 73% will not be discharged (RAG Blue)
Of the 15 patients identified who could be discharged before March, this is likely to be
achieved for 9.
The full analysis broken down by borough can be found in Appendix 1. Based on this analysis, and factoring an average admission rate of 2 patients per month from January to March 2019, NCL’s final inpatient position is anticipated to be in the region of 53 patients. This
81 80 78
8582
7067 65
62 60
57 5548
81 7976
80
7168
64 64 63 61
6256
31 29 29 27 27 25 2522
31 30 30 32 31 32 30
0
10
20
30
40
50
60
70
80
90
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Year 0 Year 1 (2016/17) Year 2 (2017/18) Year 3 (2018/19)
Long-stay (5Yr+ patients) as at 31 December 2018
All Patients - Targets All Patients - Actual
Long stay patients - Targets Long stay patients - Actual
71

5
would equate to an overall reduction in the use of inpatient beds of 35%, for people with a Learning Disability and/or Autism.
Changes in the Learning Disability population Whilst the projections for inpatients in March 2019 fall below the target for NCL, there are two significant factors worth noting in relation to the targets set by NHSE for the Transforming Care Programme.
The national Programme target for the maximum number of TCP inpatients, as set out in
Building the Right Support1, equates to “10-15 inpatients per million population in CCG
commissioned beds, and 20-25 inpatients per million population in NHS England-
commissioned beds”2 – known as the ‘BRS target’. For NCL, the overall BRS target is 48
inpatients. This means that if NCL were to achieve an inpatient figure of 48 by 31 March,
national standards will have been met.
The population figures used to calculate the BRS target are taken from the NHS 2015-16 GP
Registered Population data. This has not been updated, despite annual increases in the
population, which in turn will impact on the comparative number of people within the TCP
cohort, and the number of inpatients. Across NCL, the 2018/19 GP registered population (as
at 30 September 2018) stands at 1,625,8033 – a 6.2% increase since 2015/16. If the BRS
target were therefore applied to the most up-to-date population data, NCL’s BRS target would
increase to 65 inpatients – a figure which has already been met. The NCL PMO has raised
the issue of using out-of-date population data to judge the current performance of TCPs with
NHSE, however, there are no plans for the BRS figure to be updated before the end of March,
and TCPs will continue to be held to account against the 2015-16 population.
3. Summary of Programme Activity
As we near the end of this three year programme it is opportune to reflect not solely on the numbers but also on some of the individuals behind the numbers, and the positive outcomes that have been achieved. Six case studies are appended (Appendix 2) to this report, which highlight in some detail the work of the TCP Hub in discharging several long-stay patients and young people, as well as supporting proactive admission avoidance activity to ensure those individuals remain out of hospital. The complexity of these cases is apparent, as is the ongoing challenge faced by local teams to identify appropriate, sustainable community support for each individual. In the cases of the young people, the impact that a young person’s needs can have on the wider family is also clear. Overall Programme activity highlights include:
A total of 178 admissions have been reported as part of the Programme across NCL, since
April 2016, with 122 discharges as at 31 December 2018. As the monthly reporting to NHS
England reflects the net inpatient position, a large number of these admissions and discharges
will not be highlighted, particularly where admission and discharge occurs within the same
month.
Of these, 28 admissions were children and young people (CYP), with 24 discharged to date.
Almost half of these young people were discharged home and almost the same number were
discharged to residential care away from home.
Of the 67 adult discharges from CCG-funded inpatient settings, 55 were from a London
hospital, meaning the majority of these individuals were kept close to home during their
admission. However, of the remaining 29 CCG-funded patients awaiting discharge, 21 are in
hospitals outside of London (including 10 at Harperbury hospital in Hertfordshire). This reflects
1 Building the Right Support 2015 2 Building the Right Support 2015 , pg 6 3 https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/general-practice-data-hub/patients-registered-at-a-gp-practice
72
6
the complexity of the majority of these individuals, who have been p laced out of London due
to local hospitals not having either the capacity or the skills to meet their presenting needs. A
workstream led by NHS England London Region is assessing the capacity needs across
London in order to reduce the number of out-of-area admissions that take place in the future.
Of all admissions, seven were readmissions within the life of the Programme. Six of these
were for individuals supported locally, who were admitted to CCG-commissioned inpatient
settings.
Approximately 16 individuals who have been inpatients for more than five years have been
successfully discharged from hospital, with two readmitted. Of these, the longest length of
stay was 21 years. A number of these individuals had never lived in the community as adults
(as demonstrated in some of the attached case studies). Work is also underway to discharge
two patients currently placed at Harperbury hospital. Individuals at Harperbury, whilst coun ted
as part of TCP, have not been subject to the same activity during the Programme due to legal
restrictions. The average length of stay for patients at Harperbury is 49 years.
4. Funding update
There is a change to the position reported to the Joint Commissioning Committee in October 2018. The recurrent impact from Specialised Commissioning discharges over the lifetime of the Programme is expected to be £3.8m, offset by a £2.0m funding flowing in from NHS England. The net impact is £1.8m (full-year effect from April 2019) with these costs already in the system and funded across the 5 CCGs and respective Social Care services according to local risk share arrangements. Some of these costs would have been incurred across NCL as individuals were discharged fr om placements including CAMHs Tier 4 beds and from low secure forensic placements into the community. The Transforming Care programme has accelerated the pace of discharges back into the community by placing a greater emphasis on care closer to home particularly for those people with long lengths of stay in inpatient beds. The patient case studies appended to the report identify the positive outcomes for individuals discharged back into the community. This is an increased impact of £0.5m and arises from the discharge of 3 additional patients:
£150k impact arising through discharge of a 20 year stay Islington inpatient with no previously
expected discharge date
£130k impact arising through discharge of a 17 year stay Islington inpatient who had been
expected to be discharge post programme
£250k impact arising through discharge of a Barnet Child recently added to this patient cohort
There is additional risk of further patients being included in the patient cohort (growth) and the discharge of patients not currently on a discharge pathway. 5. Future of the Transforming Care Programme
The NHS Long-Term Plan, published in early January, contained a strong a commitment to raise the profile of people with a learning disability or autism, with particular focus on:
New impatient reduction targets over the next two years
Target numbers have been recalculated with a separation of adult and children numbers;
these are yet to be confirmed locally
Monitoring against a 12 point discharge plan for inpatients
Strengthening of the Community (Education) Treatment Review process
Annual Health check target 75%
73

7
The improvement of community support for people with a learning disability or autism,
particularly in relation to crisis provision and community forensic support.
Stopping the over medication of people with a learning disability
Learning Disability and autism awareness training for all NHS staff
Continuation of the Learning Disability Mortality Review (LeDeR) Programme.
In light of the above, the NCL Transforming Care Programme will continue beyond March 2019 although more detail is needed from NHS England including confirmation of funding flows. A full work programme will be developed following more information on the planning guidance but NCL priorities will include:
Continuation of the NCL-wide strategic arrangements to ensure the needs of people with a
Learning Disability and Autism remain in focus
Driving improvements in hospital admissions avoidance. This will include further embedding
of the delivery of Care (Education) Treatment Reviews (C(E)TRs), particularly within the
community, and more stringent governance across NCL to ensure that admission avoidance
is prioritised through the use of robust Admission Avoidance registers
Supporting Community Mental Health Teams to embed TCP practice within their services to
reflect the offer within Learning Disability services
Workforce development relating to Positive Behaviour Support and Autism; continuation of
work within NCL children’s services to deliver autism training to various front-line staff, using
funding provided by NHSE in 2018/19. It is hoped that further funding will be made available
so this training can be rolled out to colleagues in adult services.
Development of robust transition arrangements for young people approaching adulthood
Continuation of work with local authorities to explore and deliver a pilot that enables people
with a learning disability or autism to access different housing options
Embedding of the community forensic pathway across NCL, a new service funded by NHS
England for two years
Continuation of the workstream to develop an enhanced crisis pathway for people with a
learning disability or autism.
Understanding the needs of young people in 52 week residential care
Discharge the remaining inpatients including a focus on the patients at Harperbury hospital
Continued focus on the sustainability of good practice across the patch
The delivery of some of these priorities is dependent on whether additional funding can be secured from NHS England to support delivery in 2019/20, an issue raised regularly at the monthly assurance meetings.
6. Conclusion
As at the end of December 2018 performance has improved with a total number of inpatients of 56 against a target of 55 for the end of Quarter 3. It is estimated NCL will end the programme in the region of 53 patients and, whilst this number falls short of the overall target of 48, it represents a sustained hospital bed use reduction of 35%, against a national average of 18%. The Transforming Care Programme will be extended beyond March 2019 and the detail will be reported to the next Joint Commissioning Committee update, once this is known from NHS England. 7. Recommendations
The Joint Commissioning Committee is asked to NOTE this report.
74

1
Transforming Care Partnership
North Central London
Joint Commissioning Committee
7 February 2019
TCP Update - Appendix 1
NCL Transforming Care Trajectory Update – December 2018
The discharge plans of current inpatients have been reviewed, with assurance provided via meetings
with CCG commissioners and colleagues from NHS England Specialised Commissioning.
Overall, NCL is expected to reduce the number of inpatients to 48 by March 2019. As a result of the
review, the likely performance against the planned trajectory for NCL has been revised. Discharge
plans for each patient have been RAG rated at the end of each month since April 2018; this report
includes the update as at 31 December:
Blue Patients in Harperbury and those not clinically ready for discharge before the end of the Programme
Red Patient not expected to be discharged before end of Programme: significant barriers to discharge
Amber Amber-Red Patient could be discharged before end of Programme, with a number of challenges to overcome to develop/deliver the discharge plan
Amber-Green Patient could be discharged before end of Programme, with few challenges to overcome to deliver the discharge plan
Green Patient expected to be discharged before end of Programme, with discharge plan progressing well
As at end of December:
NCL TCP Cases – Discharge Plan RAG Local Area
CCG-Funded Patients NHSE-Funded Patients Total
Barnet 9 2 2 13 Camden 3 1 2 2 8 Enfield 1 1 3 1 6
Haringey 4 1 3 5 13 Islington 5 2 2 7 16
Total 22 2 6 2 19 5 56
End-of-Programme RAG:
As part of increased assurance by NHSE, NCL TCP have been asked to report on how many
inpatients are expected to remain at the end of the Programme (31 March 2019). Further work has
therefore been undertaken to ascertain how many of those with a Green, Amber or Red rating should
definitely be discharged by the end of March, regardless of any delays:
Area CCG-funded patient NHSE-funded
Total (as at 31 Dec)
Expected to discharge by March
Total (as at 31 Dec)
Expected to discharge by March
Barnet 9 0 4 1 Camden 4 0 4 1
Enfield 2 1 4 1 Haringey 8 1 5 0 Islington 9 4 7 0
Total 32 6 24 3
75

2
As the above shows, the majority of patients remaining are unlikely to be discharged before the end of
March, and this is also reflected in the high proportion who are RAG’d Blue (73% of all current
inpatients). The majority of these patients remain unwell and therefore cannot be safely discharged
before the end of the Programme.
Projection as at 31 December 2018:
Based on the December inpatient total of 56, it is expected that 9 patients should be discharged
before the end of March, even accounting for further delays to individual discharge plans. In order to
be pragmatic, an admission rate of 2 per month has also been factored into the projection, from
January to March 19. Therefore, by the end of March, it is projected that NCL should end the
Programme in the region of 53 patients, which would fall some way short of trajectory. However, it
should be noted that in terms of a reduction in the use of inpatient beds for NCL’s TCP cohort, a total
of 53 inpatients remaining would equate to a 35% reduction, which would be a significant
achievement.
76

1
Joint Commissioning Committee
7 February 2019
TCP Update - Appendix 2
NCL Transforming Care Hub Case Studies: June – December 2018
The following case examples showcase the complexities of avoiding admissions and successfully discharging patients within the NCL Transforming Care cohort, and the positive outcomes that have been achieved for these individuals as a result. All cases have been supported or led by Senior Care Coordinators within the NCL Transforming Care Hub, a fixed-term resource funded via grant funding from NHSE. Any identifying information has been removed, and permission has been sought to share direct comments.
CASE 1 – Person ‘A’ (Young Person) Presenting Needs / Diagnosis: Autism, Eating Disorder Length of stay in hospital N/A – MH admission avoided
What the person wanted for the future
Parent view – avoid Tier 4 admission, intensive support for summer period, commence at new school in September.
Challenges contributing to risk of admission and how these were overcome:
13 year old male with autism and an eating disorder (ED) on a paediatric ward due
to ED related deterioration in physical status appeared to require Tier 4 admission.
Perception of Community Education and Treatment Review was to work towards
stabilising the young person in the community over the summer period to give him
the best opportunity to start at a new autism specific school in September.
Young person had been educated via a home tuition programme for almost two
academic years prior and a Tier 4 admission would have disrupted his opportunity
to transition into a new school setting in September as originally planned.
Challenges overcome via:
Head of Children’s Health Joint Commissioning (HCHJC) agreed on the spot to
fund a place for the young person at the Eating Disorder Intensive Service (EDIS).
Senior Care Coordinator (SCC) arranged for consultation with specialist MH
autism service to support ED input, through contract identified by HCHJC.
CETR panel recommended need for 1:1 support worker to engage young person
in meaningful activities over the summer holidays and lessen the strain on parent.
SCC liaised with parent who identified tutor who had pre-existing relationship with
young person through his home tuition programme.
SCC liaised with Pupil Services Strategy and Commissioning Manager to utilise
pre-existing arrangements for support from tutor funded through personal budget.
Case brought to local Education, Health and Care Needs Management Board
(EHCNMB) by HCJC and TCC within three working days of CETR.
77

2
Funding later agreed for 30 hours per week of 1:1 support through existing Short
Breaks Personal Budget with excess to be funded through health by HCJC.
1:1 worker provided support for remainder of summer holidays, overlapping and
working in conjunction with the EDIS input.
Agencies involved in the process:
NCL TCP Hub Senior Care Coordinator
Head of Children’s Health Joint Commissioning
CAMHS ED Service
Pupil Services Strategy and Commissioning Manager
Current status/outcomes achieved:
By the end of the summer, Tier 4 admission avoided with young person gaining
weight and starting at new school in September.
Young person attending school Monday to Friday and accessing EDIS seven days
per week, receiving multi-disciplinary input from key workers, nursing, dietetics,
family therapy, psychology and psychiatry.
Social care referral recommended by initial CETR led to allocation of Family
Outreach Support Worker.
Follow up CETR in October chaired by TCC included input from new school
through attendance from head teacher and speech and language therapist (SLT).
Due to significant progress made in relation to ED, outcome of follow-up CETR
centred upon gradual transition away from EDIS towards community CAMHS ED
support, further educational input and accessing meaningful activities.
CETR actions included young person to start attending an after -school club, SLT
input, and access to meaningful activities via TC specific top-up of personal budget
from Choice & Control Commissioner.
Young person accessing SLT input through school: talking to more adults and
students, setting and reviewing his own targets and plan is to attend social games
group with peers.
Feedback from individual/ family/professionals
RC fed back that admission would not have been avoided without Transforming
Care input.
Parent reported that young person is ‘doing really well’ and grateful for the
instigation of the CETR process.
CETR independent reviewers (‘Expert by Experience’ and ‘Clinical Expert’)
provided by NHS England fed back that they had not seen a positive turn around
happen as quickly before and were impressed with the autism-friendly approach
from the ED service.
78

3
CASE 2 – Patient ‘B’ (young person)
Presenting Needs / Diagnosis: Patient recovering from an acute psychotic episode.
Past diagnosis of Selective Mutism. Mild learning
disability and Epilepsy.
Length of stay in hospital 17 months
What the person wanted for the
future
To live in their own home, with family. To access the
community and take part in activities and to go to a
local school
Barriers to discharge and how these were overcome:
There were no local schools that would support ‘B’, due to their mental health
diagnosis
Concerns regarding the risk of ‘B’ leaving their home without supervision when
experiencing a seizure-type episode. Previous incidents of trying to jump over the
landing stairwell.
Damage to furniture. An OT assessment was requested, but was delayed for 6
weeks before being completed. OT recommendations required further adjustment
to conform to fire regulations. This further delayed the discharge process by 8
weeks.
Transport arrangements to enable the young person to attend school.
No agreement via mental Health Act Section 117 ensure an appropriate care
package could provide support in the community.
Barriers overcome via:
NCL Hub Senior Care Coordinator provided an increased level of support to the
family via almost daily contact, including supporting the patient’s mother to ensure
she was able to support both the patient and siblings.
OT assessment recommended adaptations to be made to the individual’s home to
reduce risk of leaving the property without supervision, including alarms that alert
the family to doors being opened. ‘Tuff Furniture purchased to prevent future
damage to furniture.
79

4
Senior care Coordinator led on facilitating contact between all relevant agencies
involved in the young person’s care, chasing actions, and ensuring a person-
centred approach to the implementation of discharge plans.
Engagement from Barnet CCG in the discharge process, who provided support
through escalating concerns around delays, funding the OT assessment and the
purchase of bespoke ‘Tuff Furniture’ to meet the needs of the individual upon
discharge home.
A personal health Budget agreed to ensure support is available for the young
person in the community. This has been used recently for increased support to
access school social clubs.
Agencies involved in the process:
NCL TCP Hub Senior Care Coordinator
Social Worker
Local SCAN team (specialist CAMHS team for children and young people with
learning disabilities and neuro-developmental disorders) Care Coordinator
Housing department
CCG/Local Authority Joint Commissioners
Education services
Hospital
NHSE Specialised Commissioning Team (CAMHS)
NCL TCP Programme Management Office
Current status/outcomes achieved since discharge :
‘B’ is at home and settling well. A SCAN care coordinator in place, and is carrying out
follow-up visits. A Personal Health Budget is in place, and will be reviewed as required.
Feedback from professionals and family:
‘B’s’ mother has shared she is happy with the agreement that her child can now live back
at home, with the safety issues minimised.
CASE 3 – Patient ‘C’
Presenting Needs / Diagnosis: Severe Learning Disability, Autism, Epilepsy,
Diabetes Type 1, PICA (eating disorder)
Length of stay in hospital 6 years (whole adult life)
80

5
What the person wanted for the
future
To live in their own home, near their family. To access
the community and take part in activities.
Barriers/challenges relating to discharge and how these were overcome:
‘C’ has physical health conditions which are difficult to manage alongside needs
relating to Learning Disability and Autism.
In particular Diabetes Type 1 is complicated to manage alongside PICA (which
causes extreme food seeking behaviours).
Because of reduced understanding and communication relating to Autism and
Learning Disability, restrictions on food seeking and food intake can cause
challenging behaviour.
As a result of this complex physical and mental health presentation, ‘C’s needs
had been managed in residential school setting from age of 11 and subsequently
in hospital from age of 18. There was little evidence to understand how his needs
could be met in a community setting.
Barriers overcome via:
Bespoke, person centred and intensive care coordination by TCP Senior care
Coordinator, including weekly reviews of the transition with the hospital and care
provider to ensure that ‘C’s needs were fully understood and reflected in the care
planning documentation. This included close working with GP and Community
Diabetes Service to ensure that reasonable adjustments were made.
Appropriate levels of 2:1 staff support commissioned in community care provision.
Development of a detailed Positive Behaviour Support Plan.
Identification of a suitable property being located and furnished specifically to
safely meet ‘C’s needs (complicated by the fact that ‘C’ had to have his own
kitchen that was locked so he could not access, authorised by DOLS).
Regular contact between the Care Coordinator and the family to support them
through the process and ensure that all of their concerns were taken into account.
Agencies involved in the process:
NCL TCP Hub Senior Care Coordinator.
Local Community Learning Disability Team (joint health and social care)
Local Authority Legal department, supporting various court applications to enable
safe discharge to the community.
Hospital
81

6
Local Commissioners
Community provider
NCL TCP Programme Management Office
GP
Community Diabetes Service
Current status/outcomes achieved since discharge:
Over 6 months since ‘C’ discharged – successfully living in new home
‘C’ is now displaying a calm and settled mental state and instances of challenging
behaviour have drastically reduced. As presenting needs changed and developed
over time, the Positive Behaviour Support Plan has also been revised to ensure
the right support is provided.
Instances of food seeking have drastically reduced. ‘C’ is now able to access his
kitchen, serve his own food, and eat his meals with his family (which he was
unable to for a number of years previously). ‘C’ also has independent access to
their own snack cupboard.
The care provider worked closely with the MDT to support ‘C’ to improve their
behaviour. This has now been successfully handed over from the funding borough
to the borough ‘C’ lives in.
Level of sensory needs have reduced.
‘C’ hosts regular visits from family, and visits them in their home. His level of
contact and quality time spent with family has greatly increased since discharge.
Feedback from professionals and family:
‘C’s family report that he is ‘very happy’.
Care provider state they are ‘very impressed with his progress’.
82

7
CASE 4 – Patient ‘D’
Presenting Needs / Diagnosis: Mild Learning Disability, Autism, Mood Disorder
Length of stay in hospital 21 years (whole adult life, inpatient since age 14)
What the person wanted for the
future
To live in their own home, near their family. To access
the community and take part in activities.
Barriers/challenges relating to discharge and how these were overcome:
‘D’ demonstrates complex challenging behaviour which poses a risk to himself
(e.g. tying ligatures, burning self, absconding) and others (e.g. verbal threats of
violence, rape, and a preoccupation with animals and children, damage to
property).
‘D’ was institutionalised after spending such a long time in hospital. He had lived in
the last hospital setting for 13 years and had a complex attachment to his bedroom
door, bedroom, and staff.
The hospital was CQC rated as ‘requires improvement’ and was reluctant to work
in partnership with the community team or care provider to progress the patient to
be ready for discharge.
The patient refused to take part in a transition with community care provider so
they could gain experience in meeting his needs, and became overwhelmed with
any more than one visit per week.
‘D’s mother is closely involved in his care and purchased the community property
where he was to be discharged too. She suffers from anxiety and became very
overwhelmed by the process.
Barriers overcome via:
Bespoke, person centred and intensive care coordination by TCP Senior Care
Coordinator, including weekly reviews of the transition with the hospital, care
provider and MDT to ensure that ‘D’s needs were fully understood and reflected in
the care planning documentation. This included close working with Psychology
team to understand his complex attachment to hospital and boundary testing
behaviours.
Tri-borough ‘Unmanaged Risk Forum’ (led by local Mental Health Trust) attended
to ensure that all measures to assess risk had been considered and implemented .
Legal advice sought on actions to be taken if patient refused to leave hospital.
83

8
Appropriate levels of 2:1- 3:1 staff support commissioned in community care
provision.
‘D’s mother was supported by OT to purchase suitable property and NCL TCP
Capital Fund funding grant obtained for £55,000.00 to ensure that this was safe
for ‘D’ to live in (bedroom and en-suite were ligature free, windows and fencing
reinforced to reduce opportunities to escape, and elements of hospital such as
bedroom door were replicated).
Development of a detailed Positive Behaviour Support Plan.
Regular contact between the Care Coordinator and ‘D’s mother to support her
through the process and ensure that all of her concerns were taken into account.
Agencies involved in the process:
NCL TCP Hub Senior Care Coordinator.
Local Community Learning Disability Team (joint health and social care)
Local Authority Legal department, supporting various court applications to enable
safe discharge to the community.
Hospital
Local Commissioners
Community provider
NCL TCP Programme Management Office
Current status/outcomes achieved since discharge :
8 weeks since ‘D’ was discharged – successfully living in new home.
‘D’ continues to test boundaries with new support staff which is considered to be
part of the process of him becoming more settled in his new home. As presenting
needs changed and developed, the Positive Behaviour Support Plan has also
been revised to ensure the right support is provided.
‘D’ has accessed community activities of his choice including shopping, the Zoo
and attending a local disco to socialise with peers.
The care provider continues to work closely with the MDT to support ‘D’ to improve
their behaviour.
‘D’s mother has spent a lot of time with him in his home and supporting him to
access the community. His level of contact and quality time spent with family has
greatly increased since discharge.
84

9
Feedback from professionals and family:
‘D’ reports ‘I can’t believe I did it’ in relation to leaving hospital, rates his new home as ‘100
out of 10’ and states ‘it is much better than hospital’.
His mother reports she feels he is doing ‘very well’ and that he is ‘very happy’.
Community care provider service manager states she feels the discharge process has
gone ‘so much better than I could have expected’.
CASE 5 – Patient ‘E’
Presenting Needs / Diagnosis: Moderate Learning Disability and Autism
Length of stay in hospital 8 years (whole adult life)
What the person wanted for the
future
To live in their own home, near their family. To access
the community and take part in activities.
Barriers/challenges relating to discharge and how these were overcome:
‘E’ demonstrates challenging behaviour in the form of banging his head against
hard or sharp objects to injure himself, and also targets others to injure by hitting
them with his head. This has been of such severity in the past that it has caused
him to develop two haematomas which were surgically removed.
‘E’ struggles with auditory, visual, vestibular, touch and multisensory processing
which means he is sensitive to noise, light, touch and struggles when his feet leave
the ground. Overstimulation to these sensitivities can cause him to bang his head.
‘E’ has struggled to adjust to new care settings in the past, causing him to
demonstrate a higher level of challenging behaviour and distress.
‘E’s mother is closely involved in his care, with a clear idea of the care she would
like for her son, which may not always match with professional views.
Barriers overcome via:
Bespoke, person centred and intensive care coordination by TCP Senior care
Coordinator, including weekly reviews of the transition with the hospital, care
85

10
provider and MDT to ensure that E’s needs were fully understood and reflected in
the care planning documentation.
Appropriate levels of 2:1 – 4:1 staff support commissioned in community care
provision.
Purchase of suitable house and completed a large renovation project jointly
funded by the NCL TCP Capital Fund and NHSE totalling £200,000. This padded
or replaced as many trigger points for ‘E’ to target as possible such as radiators,
taps, corners and sharp edges. In addition, two of the rooms have been
completely padded.
Development of a detailed Positive Behaviour Support Plan with community care
organisation’s PBS Lead on site full time for three months.
Regular contact between the Care Coordinator and ‘E’s mother to support her
through the process and ensure that all of her concerns were taken into account.
Agencies involved in the process:
NCL TCP Hub Senior Care Coordinator.
Local Community Learning Disability Team (joint health and social care)
Local Authority Legal department, supporting various court applications to enable
safe discharge to the community.
Hospital
Local Commissioners
Community provider
NCL TCP Programme Management Office
NHS England
Current status/outcomes achieved since discharge :
6 weeks since ‘E’ was discharged – successfully living in new home.
‘E’ continues to display a high level of challenging behaviour and additional staffing
remains in place to support him. As presenting needs changed and developed, the
Positive Behaviour Support Plan has also been revised to ensure the right support
is provided.
The care provider continue to work closely with the MDT to support ‘E’ to improve
their behaviour.
86

11
‘E’ has accessed their local shop to purchase items of their choice, prepared their
own food, been for walk in their community, and successfully attended outpatient
health appointments at GP and local hospital.
‘E’s mother has spent a lot of time with him in his home and supporting him to
accessing the community. His level of contact and quality time spent with family
has greatly increased since discharge.
Feedback from professionals and family:
‘E’s mother reports that she feels ‘free as my son is no longer locked up’.
‘E’s community care provider report that he has a great sense of humour and continues to
settle into his new home well.
When care coordinator asked ‘E’ if he likes his new home during a visit last week ‘E’
smiled.
CASE 6 – Patient ‘F’ (Young person)
Presenting Needs / Diagnosis: Severe Learning Disability and Autism
Patient can display behaviours of concerns:- such as,
hitting, scratching, hair pulling, breaking of furniture,
doors, TV, mirrors, kicks walls and can run away from
his support worker.
Length of stay in hospital 10 months
What the person wanted for the
future
To live in his family home, near family, to access the
community and school, to take part in activities such
as trampolining, swimming and shopping
Barriers to discharge and how these were overcome:
Challenges around F’s mother’s understanding of his needs, how this impacts on
his interpretation of the world around him, and how to provide appropriate support
at home. This impacted heavily on the discharge process.
87

12
Barriers overcome via:
A section 20 (Children’s Act) application requested and agreed, along with a Child
in Need Assessment. This resulted in F’s being placed under the care of local
authority, within a residential school placement.
Advocate support for family in light of decision around F’s care. Family agreed this
was the best option for F.
The NCL TCP Hub Senior Care Coordinator ensured that communication was
transparent for AA’s Mother and Siblings and care plans were person centred. This
included carrying out two-weekly reviews with the residential school, the hospital
and the family.
Once a residential education placement identified, the NCL TCP Hub Senior Care
Coordinator supported the school team to ensure Positive Behavioural Support
training had been undertaken, to support F to transition and settle into the new
environment. This helped to address F’s increase in anxiety and behaviours of
concern. The Senior Care Coordinator also kept in daily contact with the new
provider upon discharge during the period whilst F settled in.
Agencies involved in the process:
NCL TCP Hub Senior care Coordinator
Barnet Looked After Children’s Team,
Barnet Tripartite Panel
Community Provider
Hospital
Barnet CCG/Local Authority Children’s Commissioners
NHSE Specialised Commissioning (CAMHS)
NCL TCP Programme Office
Current status/outcomes achieved since discharge :
F has settled into the school, his access to the community has increased. Contact with his
family has now been agreed and a consistent visiting time, along with the finances for his
family to visit him twice a month.
Feedback from professionals and family:
F’s mother is still quite worried about her son being far away from her and his sisters, but
happy she can see him twice a month. His sister shared she thinks this is the best
arrangement for her brother at this time.
88

13
The care provider provided the feedback:
“You have shown great support and guidance to us as a team and this is gratefully
appreciated.”
89

1
NCL Joint Commissioning Committee
Thursday, 7 February 2019
Report Title Full Business Case for Faecal Immunochemical Test (FIT) implementation in NCL
Date of report: 29 January 2019
Agenda Item
4.1
Lead Director /
Manager
Paul Sinden Director of Performance, Planning and Primary Care for NCL CCGs
Tel/Email [email protected]
GB Member Sponsor
Not applicable.
Report Author
Ed Nkrumah Director of Performance for NCL CCGs
Tel/Email [email protected]
Report Summary
This full business case is for the implementation of Faecal Immunochemical Test (FIT, also known as quantitative FIT or qFIT) for patients who present in primary care with symptoms suggestive of colorectal cancer. This non-invasive, inexpensive and highly sensitive test detects hidden blood in a stool sample, is already in use across various areas in England and Scotland. This is also due to be rolled out for the national bowel cancer screening programme in the next few weeks. The attached business case which is backed by NICE guidance and clinical studies, sets out the clinical and financial case for implementing FIT across NCL and the work undertaken so far to deliver the service subject to approval. The test is expected to deliver the following key benefits:
Early (stages 1 and 2) detection and diagnoses of colorectal
cancer after clinical presentation
Better patient experience of care compared to colonoscopies
More efficient use of limited endoscopy capacity across NCL
which will also deliver financial savings to the local health
economy. We propose that the service is commissioned through a variation to NHS Standard Contract with NCL providers who currently provide pathology services to CCGs and rolled out in two phases.
Recommendation The NCL Joint Commissioning Committee is asked to APPROVE this business case for implementing FIT across NCL in a 2- phased approach: Phase 1- APPROVE immediate implementation of Phase 1 – FIT for symptoms described in NICE Diagnostic Guidance 30 (DG30).
90

2
Phase 2 – JCC to receive an updated business case for APPROVAL for implementing Phase 2 – FIT for other symptoms described in NICE Guidance 12 (NG12). The clinical and financial case will be based on evidence from the publication of an ongoing pilot study by UCLH Cancer Collaborative. The case will be presented once findings from the study are released.
Identified Risks
and Risk
Management
Actions
The main risk relate lack of clinical (primary and secondary care) engagement. This is being mitigated through extensive clinically-led engagement plan. Further communication and engagement will be undertaken if business case is approved.
Conflicts of Interest
None identified.
Resource
Implications
Estimated annual investment: £50k for FIT testing with net savings
of £2m from reduced spend on colonoscopies.
Engagement
Project stakeholder engagement plan being implemented includes:
Presentations to GP Educational events in Haringey, Camden and Enfield with sessions planned for Islington and Barnet in January 2019.
Face to face meetings and presentation by Dr Edward Seward, Consultant Gastroenterologist at UCLH, to clinical teams at Royal Free London Hospital, Whittington Hospital, University College London Hospital and North Middlesex Hospital
Shared learning and benchmarking with other London STPs.
Business case has the support of London and NCL Cancer Commissioning Board and UCLH Cancer Collaborative. Patient representatives have been engaged through these group.
Local activities have confirmed strong support from GPs and secondary care clinicians and operational teams across the NCL.
Equality Impact
Analysis
Equality Impact analysis – approved by Senior Equality, Diversity and Inclusion Manager North Central London CCGs. Quality Impact Assessment- approved by Directors of Quality NCL CCGs. Data Protection Impact Assessment –sign off expected w/e 1 February 2019.
Report History and
Key Decisions
10 July 2018 - Pan-London Outline Business Case produced by Transforming Cancer Support Team (TCST) for London.
91

3
16 July 2018 – Pan-London Outline Business Case supported by London Cancer Commissioning Board. 2 August 2018 - London Cancer Commissioning Board supported Pan-London Outline Business Case. 18 September 2018 - NCL Senior Management Team supported Pan-London Business Case and approve the set-up of a project group to develop the full business case. 24 September 2018 – NCL Cancer Commissioning Board supported the case for implementing FIT for higher risk symptoms based on preliminary findings from pilot study led by UCLH Cancer Collaborative. 11 January 2019 – Local Tariff for FIT Test shared with NCL Payment Mechanism Group for information and comments. 21 January 2019 – Full Business Case sign-off by Task and Finish Group. 29 January 2019 – Full Business Case presented to NCL Senior Management Team for review.
Next Steps Mobilisation of service.
Appendices
Faecal Immunochemical Test (FIT) – NCL Full Business Case
92
1 | P a g e
Faecal Immunochemical Test (FIT) - NCL Full Business Case
Project Name Faecal Immunochemical Test (FIT) for Symptomatic Patients
SRO Paul SINDEN, Director of Performance, Planning and Primary Care, NCL CCGs
Clinical Lead Dr Clare STEPHENS, Cancer Clinical Lead, NCL STP
Project Lead Ed NKRUMAH, Director of Performance, NCL CCGs
Project Manager Bashir RAMZAN, NCL Cancer Project Manager
Project Classification
Transactional Transitional Transformational
Executive Summary North Central London Clinical Commissioning Groups (CCGs) are seeking to commission a pathology service for Faecal Immunochemical Test (FIT) (also known as quantitative FIT or qFIT) for symptomatic patients. This is a non-invasive, inexpensive and highly sensitive test that detects hidden blood in a stool sample that could be suggestive of colorectal cancer (CRC). This paper sets out the clinical and financial case for implementing FIT across NCL and the work undertaken so far to deliver the service subject to approval. The test is expected to deliver the following key benefits:
Early (stages 1 and 2) detection and diagnoses of colorectal cancer after clinical
presentation
Better patient experience of care compared to colonoscopies
More efficient use of limited endoscopy capacity across NCL which will deliver
financial savings
The national Bowel Cancer Screening Programme will also be rolling our FIT in the next few months using a higher threshold compared to that of the symptomatic patient group. We propose that the service is commissioned through a variation to NHS Standard Contract with NCL providers who currently provide pathology services to CCGs. The NCL Joint Commissioning Committee is asked to approve this business case including the service specification and pathway for implementing FIT across NCL in 2 phases; Phase 1 – Immediate implementation of FIT for symptoms described in NICE Diagnostic Guidance 30 (DG30). Phase 2 – Implementation of FIT for other symptoms described in NICE Guidance 12 (NG12) when the findings from the pilot study by UCLH Cancer Collaborative is released and the NCL Cancer Commissioning Board determines there is sufficient evidence to support the proposed expansion
93

2 | P a g e
Strategic Objectives & Outcomes Objectives Outcome metrics
Detect CRC at an earlier stage of disease Percentage new CRC diagnosed at stage 1 & 2 Improved percentage <60 at stage 1 & 2 CRC
Diagnose CRC more rapidly after clinical presentation
Increased percentage CRC diagnosed via 2ww
Reduced percentage CRC diagnosed as emergency
Improve patient experience of care Improved National Cancer Patient Experience Survey metrics for early diagnosis and service coordination
Improve achievement of waiting times standards
Improved cancer waiting times to treatment, principally the 2-week and 62-day waiting time standards
More efficient use of NHS care Reduced demand for endoscopy
Increased percentage of endoscopies which yield diagnosis of CRC
Reduced demand for OPD gastroenterology and colorectal surgery
Contribute to CCGs QIPP savings and quality improvements – and their contribution to CCGs corporate objectives
Annual QIPP Savings Plan
Barnet CCG
Camden CCG
Enfield CCG
Haringey CCG
Islington CCG
NCL CCGs
Reduction in scopes (cost)
£510,503 £373,213 £431,831 £479,844 £330,277 £2,125,668
Cost of FIT £12,935 £9,456 £10,942 £12,158 £8,368 £53,859
Net Savings £497,568 £363,756 £420,890 £467,686 £321,909 £2,071,809
Please see appendices 1 (a – c) for detailed breakdown including modelling assumptions and
local tariff assessment.
Background & Case for Change Colorectal cancer (CRC) is the fourth most common malignancy in the UK, accounting for 12%
of all new cancers. In London, approximately 3,500 people are diagnosed with and around
1,250 die from CRC each year. Over 20% of new cases in London are in people under 60 years
old. The number of people in London and England diagnosed annually with CRC has increased
steadily over the past decade, largely due to age-related demographic growth. Mortality has
fallen progressively in the same period, reflecting improvements in diagnosis and treatment.
9 in 10 people diagnosed with the earliest stage (stage 1) of CRC survive for five years or
more; less than 1 in 10 people with the latest stage (stage 4) do. Over half of all cases in
England and almost 60% of cases in London are diagnosed at Stages 3 and 4. Worryingly,
people under 60 years are less likely to be diagnosed with early stage CRC (37%) compared to
94

3 | P a g e
those over 60 years (44%). Around a quarter of all patients in London are diagnosed via an
emergency route; only a third of these are alive after 5 years. This compares to 69% for those
diagnosed via 2ww or routine referral.
Although the proportion of cases diagnosed as an emergency has fallen over the past decade,
in North Central and East London this decrease has been only marginal (less than 1%).
Similarly, there have been relatively small improvements in the proportions of patients
diagnosed with early stage CRC over the most recently recorded period (2012-16).
CRC is usually diagnosed by colonoscopy, sigmoidoscopy or CT colonography (henceforth
these will be referred to collectively as “endoscopy”). National guidelines (NICE NG12)
recommend referral of symptomatic patients for endoscopy determined by an assessment of
whether the patient is at “high” or “low” risk of CRC. This should be based on a person’s age,
sex, the nature and duration of their symptoms, and basic laboratory test results. High risk
patients (considered to have a risk of cancer > 3%) should be referred urgently via a 2WW
pathway. Low risk patients (< 3%) should be managed according to clinicians’ discretion using
qualified reassurance, follow up and safety netting and - for certain groups - testing for occult
blood in the stool. The strength of this distinction is that patients with the highest risk can be
referred quickly for investigation. However, in real world clinical practice it is not always easy
to distinguish between those with a greater or less than 3% risk, and regardless of this many
people with CRC present with a “low risk” clinical picture that does not initially meet NG12
criteria for urgent referral. This means that people may be incorrectly judged to not need
endoscopy and their diagnosis delayed.
An abnormal faecal blood test result suggests that there may be bleeding within the
gastrointestinal tract, which requires further investigation, usually via endoscopy. At the time
NG12 was published the only test widely available was a guaiac based Faecal Occult Blood
Test (gFOBt). This has no specificity for human haemoglobin, leading to false positives from
dietary sources of haemoglobin and antioxidants or peroxidase activity from food and drugs.
As a result, practitioners lost confidence in this test and it was gradually withdrawn. In
response, the pan London NG12 colorectal clinical reference group decided to “upgrade”
patients for which NG12 guidelines recommended a gFOBt to a suspected cancer referral
(2ww); therefore, London pathways encouraged referral of greater numbers of people via a
2ww suspected lower gastroenterology (GI) cancer route than are specified within the NG12
guidelines. This means that implementing FIT in line with DG30 guidance will lead to many
people currently being referred via 2ww being reassured they are very low risk and do not
need referral for endoscopy.
In July 2018 the NCL Cancer Commissioning Board considered and supported the London-wide
business case for the introduction of FIT. From the implementation options presented (see
appendix 2), the board favoured option 4 - to deliver a phased implementation approach;
starting with eligible patients under current NICE Guidance (DG30) (phase 1) and followed by
other symptoms (phase 2) if supported by the evidence of the ongoing pilot studies at UCLH
Cancer Collaborative and other cancer vanguards.
A project group, co-led by STP Cancer Clinical Lead and NCL Director of Performance, was
subsequently set up to oversee the roll out of FIT service in two phases. Phase 1 is shown in
green on the services pathway (appendix 3). Phase 2, commencing later, will build on the
95

4 | P a g e
learning from phase 1 and see FIT offered to some patients presenting with symptoms that
currently meet the criteria for a 2-week wait referral.
Progress Update The project group has representation from CCGs/NCLCCGs, providers (clinical and laboratory
managers), UCLH Cancer Collaborative, Transforming Cancer Services Team, and Cancer
Research UK. Patient input has been received through the London and NCL Cancer
Commissioning Boards.
Since the formation of group, a broad programme of stakeholder engagement activity has
been and continues to be undertaken. Some of the key activity undertaken to date include:
Production of briefing notes, frequently asked questions, educational resources for
GPs, patients, primary care leads and secondary care providers.
Presentations to GP Educational events in Haringey, Camden and Enfield with sessions
planned for Islington and Barnet in January 2019.
Face to face meetings and presentation by Dr Edward Seward, Consultant
Gastroenterologist at UCLH, to clinical teams at Royal Free London Hospital,
Whittington Hospital, University College London Hospital and North Middlesex
Hospital
Other London STPs to share learning and benchmark information
Engagement with CCG commissioning Teams and STP Planned Care work stream
Local activities have confirmed strong support from GPs and secondary care clinicians and
operational teams across the NCL.
Commissioning Approach
Implementation of FIT will require the commissioning FIT kit (tube), transportation of samples
from GP practices to test laboratory, testing and reporting. Our proposed approach,
recommended by NEL CSU Procurement Team, is to include FIT testing to the existing suite of
pathology tests commissioned with NCL acute providers by varying the existing NHS standard
contracts. The approach benefits from use of existing pathology providers with established
supply chain - transportation links, IT infrastructure, and therefor speed of implementation.
The approach also offers benefits to all NCL providers who are currently struggling with
endoscopy capacity and are having to run extra clinics, insourced or outsource to meet
demand, and paying a premium (in excess of tariff) in the process. These challenges are noted
on some provider risk registers.
The service specification (appendix 3) sets out commissioners’ requirements of providers for
the service.
In recognition of the concerns with implementing FIT for NG12 prior to the release of the pilot
study results, we propose that NCL implements FIT in two phases.
Phase 1 – Immediate implementation of FIT for symptoms described in NICE Diagnostic Guidance 30 (DG30). The guidance recommends that adults are offered FIT if they do not have rectal bleeding but are:
aged 50 and over with unexplained abdominal pain or weight loss, or
96

5 | P a g e
aged under 60 with changes in their bowel habit or iron-deficiency anaemia, or aged 60 and over and have anaemia even in the absence of iron deficiency.
Although the test will be offered in primary care, secondary care clinicians will be encouraged to offer the test to eligible patients who present on secondary care without the test. The finance and activity modelling of the reduction in colonoscopies and flexi sigmoidoscopies (the two main diagnostic tests for detecting CRC) the estimated net savings are approximately £2.0 million per year across all NCL CCGs. A detailed breakdown is given in appendix 1a. Phase 2 – Implementation of FIT for other symptoms described in NICE Guidance 12 (NG12) and beyond the scope of DG30 but excluding ‘red flag’ symptoms such as rectal or abdominal mass and marked unexplained weight loss. The current guidance for a 2-week wait referral is as follows;
o aged 40-49 with unexplained weight loss and abdominal pain or o aged 50 or over with unexplained rectal bleeding or o aged 60 or over with iron-deficiency anaemia or changes in their bowel habit
or o people with a rectal or abdominal mass or o adults aged under 50 with rectal bleeding and any of the following
unexplained symptoms or findings: abdominal pain change in bowel habit weight loss iron-deficiency anaemia.
FIT for NG12 symptoms will be introduced in phase 2 if the following conditions are met;
1. UCLH Cancer Collaborative completes and releases the final results of its pilot study of FIT for NG12 symptoms. This is one of the largest observational studies to evaluate the effectiveness of FIT as a rule-out test for patients who are currently eligible for a 2-week wait referral under NICE Guidance.
2. NCL Cancer Commissioning Board considers the evidence and findings of the study to ensure consistency with the proposed pathway for NCL.
3. Finance and activity modelling is undertaken and signed-off by NCL Senior Management Team
4. Plans are put in place to audit the pathway after 3 months of implementation
Risk Risk
Rating
Mitigation
1. Trusts do not engage as they are
concerned FIT testing for DG30
but not NG12 will increase
endoscopy demand and exceed
capacity
Medium Clinically-led engagement has taken place
to assure Trusts of the expected impact.
Extensive activity modelling has also been
undertaken with clinical input at National
(Cancer Alliance Data, Evidence and
97
6 | P a g e
Analysis Service, CADEAS), London (TCST)
and STP/Alliance level. All scenarios have
shown a reduction in endoscopy demand.
2. GPs do not engage as unaware of
pathway, unsure about how to
implement in practice and/or
concerned about safety netting
Medium Core training materials, videos and
communication strategy in place/safety
netting pathway in place with materials
available to support safety netting in
practices. Strategy includes utilising GP
education events and CRUK (Cancer
Research UK) Facilitators in primary care
3. Patients do not engage due to
cultural beliefs or preference for
colonoscopy
Low Health Equalities Assessment undertaken.
Patient information in place and available
in top 11 London languages and in easy
read format/videos in place for
patients/pathway adapted in line with
recommendations from HEA for patients
who may not wish to engage in a FIT test
Studies show this should not be an issue if
clearly explained to patients
Recommendations The NCL Joint Commissioning Committee is asked to approve this business case for implementing FIT across NCL in a 2- phased approach: 1. Approve Immediate implementation of Phase 1 – FIT for symptoms described in NICE
Diagnostic Guidance 30 (DG30). 2. Recommend a way forward for implementing Phase 2 –FIT for other symptoms described
in NICE Guidance 12 (NG12). The clinical and financial case will be based on evidence from
the ongoing pilot study by UCLH Cancer Collaborative. The suggested options being;
a. JCC to receive an updated business case for approval when findings from study
are released OR
b. delegate decision –making to the NCL SMT and NCL Cancer Commissioning Board.
This will be informed by findings from the study
98
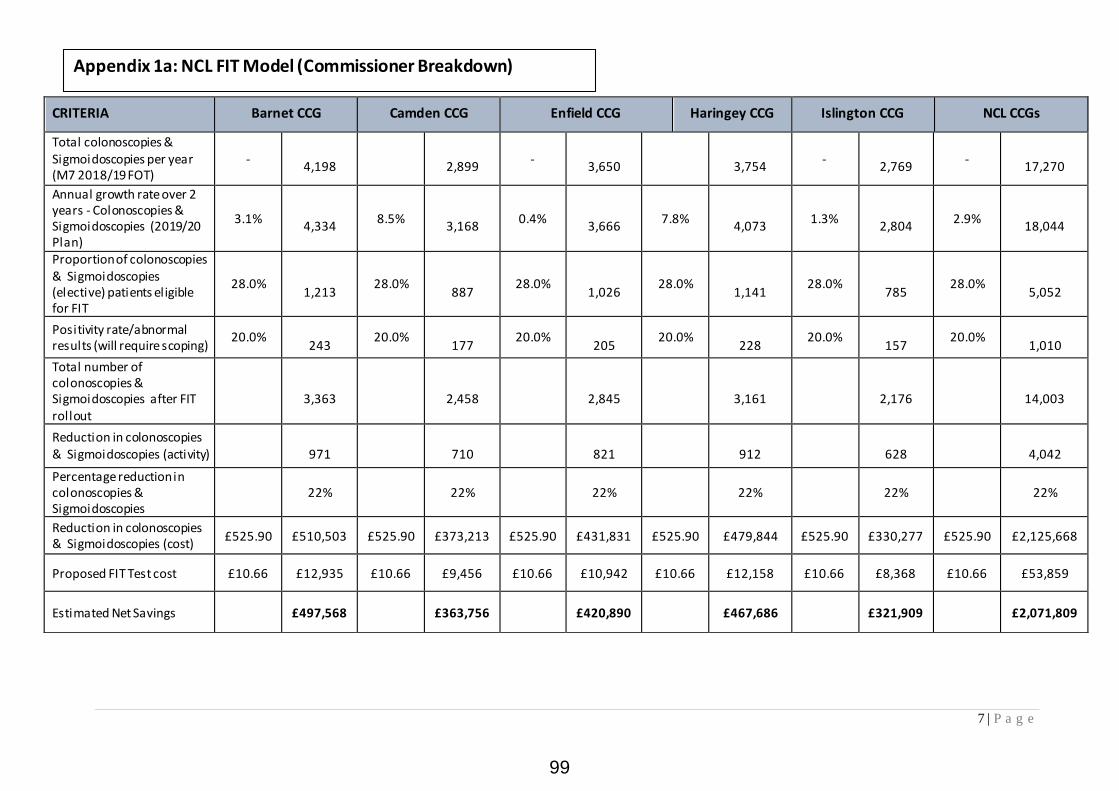
7 | P a g e
CRITERIA Barnet CCG Camden CCG Enfield CCG Haringey CCG Islington CCG NCL CCGs
Total colonoscopies & Sigmoidoscopies per year (M7 2018/19 FOT)
-
4,198
2,899
-
3,650
3,754
-
2,769 -
17,270
Annual growth rate over 2 years - Colonoscopies & Sigmoidoscopies (2019/20 Plan)
3.1%
4,334 8.5%
3,168
0.4%
3,666 7.8%
4,073
1.3%
2,804 2.9%
18,044
Proportion of colonoscopies & Sigmoidoscopies (elective) patients eligible for FIT
28.0%
1,213 28.0%
887
28.0%
1,026 28.0%
1,141
28.0%
785 28.0%
5,052
Positivity rate/abnormal results (will require scoping)
20.0%
243 20.0%
177
20.0%
205 20.0%
228
20.0%
157 20.0%
1,010
Total number of colonoscopies & Sigmoidoscopies after FIT rollout
3,363
2,458
2,845
3,161
2,176
14,003
Reduction in colonoscopies & Sigmoidoscopies (activity)
971
710
821
912
628
4,042
Percentage reduction in colonoscopies & Sigmoidoscopies
22% 22% 22% 22% 22% 22%
Reduction in colonoscopies & Sigmoidoscopies (cost)
£525.90 £510,503 £525.90 £373,213 £525.90 £431,831 £525.90 £479,844 £525.90 £330,277 £525.90 £2,125,668
Proposed FIT Test cost £10.66 £12,935 £10.66 £9,456 £10.66 £10,942 £10.66 £12,158 £10.66 £8,368 £10.66 £53,859
Estimated Net Savings £497,568 £363,756 £420,890 £467,686 £321,909 £2,071,809
Appendix 1a: NCL FIT Model (Commissioner Breakdown)
99

8 | P a g e
Appendix 1b: NCL FIT Model (Provider Breakdown)
2018/19 (M1-M7
Actual)
2018/19 (M1-M7
Actual)
2018/19 Activity
Forecast
Average activity
growth over 2 Yrs
Annual growth rate
over 2 years -
Colonoscopies &
Sigmoidoscopies
(2019/20 Plan)
Proportion of
colonoscopies &
Sigmoidoscoies
(elective) patients
eligible for FIT
Positivity
rate/abnormal
results (will
require scoping)
Total number of
colonoscopies &
Sigmoidscopies
after FIT rollout
Reduction in
colonoscopies &
Sigmoidscopies(acti
vity)
Percentage
reduction in
colonoscopies &
Sigmoidscopies
Reduction in
colonoscopies &
Sigmoidscopies(cost)
Proposed Unit cost
of FIT
Net Saving
CommissionerName Provider Sum of Activity Sum of Cost 0.0% 28.0% 20.0% 0.0% 0.0% 0.0% £525.90 £10.66 £0.00
NHS Barnet CCG 1. Royal Free 1,655 £858,904 2,837 -1.6% 2,793 782 156 2,167 626 22.4% £329,034 £8,337 £320,698
NHS Barnet CCG 2. UCLH 327 £190,182 561 7.8% 604 169 34 469 135 22.4% £71,181 £1,804 £69,377
NHS Barnet CCG 3. Whittington 147 £73,459 252 2.7% 259 72 14 201 58 22.4% £30,493 £773 £29,721
NHS Barnet CCG 4. North Mid 34 £16,325 58 33.3% 78 22 4 60 17 22.4% £9,150 £232 £8,918
NHS Barnet CCG 5. Other 286 £148,762 490 22.3% 600 168 34 465 134 22.4% £70,644 £1,790 £68,854
NHS Barnet CCG Total 2,449 £1,287,632 4,198 0.0% 4,334 1,213 243 3,363 971 22.4% £510,503 £12,935 £497,568
NHS Camden CCG 1. Royal Free 626 £317,433 1,073 0.6% 1,079 302 60 838 242 22.4% £127,141 £3,221 £123,920
NHS Camden CCG 2. UCLH 854 £479,167 1,464 15.5% 1,691 474 95 1,313 379 22.4% £199,249 £5,048 £194,201
NHS Camden CCG 3. Whittington 57 £29,241 98 -7.5% 90 25 5 70 20 22.4% £10,646 £270 £10,376
NHS Camden CCG 4. North Mid 1 £375 2 -21.4% 1 0 0 1 0 22.4% £159 £4 £155
NHS Camden CCG 5. Other 153 £79,376 262 16.6% 306 86 17 237 68 22.4% £36,017 £913 £35,105
NHS Camden CCG Total 1,691 £905,592 2,899 0.0% 3,168 887 177 2,458 710 22.4% £373,213 £9,456 £363,756
NHS Enfield CCG 1. Royal Free 1,002 £527,533 1,718 3.2% 1,772 496 99 1,375 397 22.4% £208,784 £5,290 £203,494
NHS Enfield CCG 2. UCLH 213 £124,561 365 -1.2% 361 101 20 280 81 22.4% £42,505 £1,077 £41,428
NHS Enfield CCG 3. Whittington 40 £20,632 69 10.2% 76 21 4 59 17 22.4% £8,898 £225 £8,672
NHS Enfield CCG 4. North Mid 756 £387,618 1,296 -3.1% 1,256 352 70 975 281 22.4% £147,972 £3,749 £144,223
NHS Enfield CCG 5. Other 118 £61,085 202 -0.7% 201 56 11 156 45 22.4% £23,672 £600 £23,072
NHS Enfield CCG Total 2,129 £1,121,429 3,650 0.0% 3,666 1,026 205 2,845 821 22.4% £431,831 £10,942 £420,890
NHS Haringey CCG 1. Royal Free 173 £89,858 297 14.8% 340 95 19 264 76 22.4% £40,091 £1,016 £39,075
NHS Haringey CCG 2. UCLH 321 £174,817 550 26.2% 695 194 39 539 156 22.4% £81,819 £2,073 £79,746
NHS Haringey CCG 3. Whittington 825 £405,585 1,414 7.7% 1,523 426 85 1,182 341 22.4% £179,398 £4,546 £174,853
NHS Haringey CCG 4. North Mid 654 £330,515 1,121 -10.8% 1,000 280 56 776 224 22.4% £117,810 £2,985 £114,825
NHS Haringey CCG 5. Other 217 £112,694 372 38.6% 515 144 29 400 115 22.4% £60,725 £1,539 £59,186
NHS Haringey CCG Total 2,190 £1,113,469 3,754 0.0% 4,073 1,141 228 3,161 912 22.4% £479,844 £12,158 £467,686
NHS Islington CCG 1. Royal Free 76 £39,806 130 -2.1% 128 36 7 99 29 22.4% £15,025 £381 £14,645
NHS Islington CCG 2. UCLH 687 £393,824 1,178 1.7% 1,198 336 67 930 268 22.4% £141,157 £3,577 £137,581
NHS Islington CCG 3. Whittington 647 £329,250 1,109 -3.1% 1,075 301 60 834 241 22.4% £126,580 £3,207 £123,373
NHS Islington CCG 4. North Mid 2 £976 3 -25.5% 3 1 0 2 1 22.4% £301 £8 £293
NHS Islington CCG 5. Other 203 £105,893 348 15.2% 401 112 22 311 90 22.4% £47,213 £1,196 £46,017
NHS Islington CCG Total 1,615 £869,749 2,769 0.7% 2,804 785 157 2,176 628 22.4% £330,277 £8,368 £321,909
Grand Total 10,074 £5,297,871 17,270 0.0% 18,044 5,052 1,010 14,003 4,042 22.4% £2,125,668 £53,859 £2,071,809
100

9 | P a g e
Appendix 1c: NCL FIT Modelling Assumptions
Project Name
FIT for Symptomatic
Data Source
Secondary Uses Service (SUS)
POD
Elective day case
Age group
18+
Specialty (Treatment Function Code) All- (majority recoded under Gastroenterology & Colorectal Surgery)
HRG Description All activity where dominant HRG description contains colonoscopy or sigmoidoscopy
HRG Codes FZ51Z, FZ52Z, FZ53Z, FZF54Z, FZ55Z, FZ56Z, FZF57Z
% positive FIT who will then be referred on 2WW for a scope
28%
Est tariff for FIT- (HSL supplied price)
£10.66 per test based on HSL (provider of pathology services to RFL, UCLH and NMUH through a subcontracting arrangement}
Data period 2017/18 to 2018/19 Month 7
Forecast method Straight line forecast from Month 1 to 7 of 2018/19 data
Providers NCL (UCLH, WH, NMU, RFH) and all other acute Trusts
Exclusion Specialised commissioning activity, Ambulatory Emergency Care activity, Non-consultant led speciality e.g. Midwife, Nursing, AHP episodes, Well babies and maternity,
Category
Criteria
Data Source
Secondary Uses Service (SUS)
POD
Elective day case
Age group
18+
Specialty (Treatment Function Code)
All- (majority recorded under Gastroenterology & Colorectal Surgery)
HRG Description All activity where dominant HRG description contains colonoscopy or sigmoidoscopy
HRG Codes & Descriptions FZ51Z - Diagnostic Colonoscopy , 19 years and over FZ52Z- Diagnostic Colonoscopy with Biopsy, 19 years and over FZ53Z- Therapeutic Colonoscopy , 19 years and over FZ54Z- Diagnostic Flexible Sigmoidoscopy, 19 years and over FZ55Z- Diagnostic Flexible Sigmoidoscopy with Biopsy, 19 years and over FZ56Z- Therapeutic Flexible sigmoidoscopy, 19 years and over FZ57Z- Diagnostic or Therapeutic Rigid Sigmoidoscopy, 19 years and over
% positive FIT who will then be referred on 2WW for a scope
28%
FIT positivity rate/abnormal results (will require scoping)
20%
Negotiated Tariff for FIT
£10.66 per test, including test kit, transport and reporting
Data period 2017/18 to 2018/19 Month 7
Forecast method Straight line forecast from Month 1 to 7 of 2018/19 data
Providers NCL (UCLH, WH, NMU, RFH) and all other acute Trusts
Exclusion Specialised commissioning activity, Ambulatory Emergency Care activity, Non-consultant led speciality e.g. Midwife, Nursing, AHP episodes, Well babies and maternity
101

10 | P a g e
Appendix 2 - Options for implementing FIT for symptomatic patients
OPTION PROS CONS 1. DG30 / low risk alone and await national guidance on high risk
In keeping with national guidance and London position
GP learning in use of FIT for low risk in prep for use in high risk
Likely easy adaption to recommendation for use in high risk
Should reduce demand for endoscopy via element of “rule out”
In keeping with implementation in many other areas
Requires investment for FIT testing and implementation of new pathway
Risk of increasing demand for endoscopy through “rule in”
Likely to be 2nd stage implementation once recommendations on use in high risk available
2. Delay all implementation until there is recommendation on use in high and low risk symptomatic patients
Delays implementation until there is clarity about use in high as well as low risk patients, so potentially one step implementation
No investment required Potential to implement “final
state” pathway for low and high-risk patients in one stage, so minimising complexity
No risk of increasing demand for endoscopy through creation of new “rule in” FIT pathway
Risks lengthy delay in introducing national guidance
May be lengthy period before national recommendation on use in high risk available
Low risk patients can’t receive test so no clinical benefits
No learning in use by GPs possible in this time, will all have to be learnt when “final state” recommendations available
No opportunity to curtail trend to rising demand for endoscopy via new “rule out” FIT pathway
Implementation costs will eventually be required
Will be out of sync with other areas in London that implement FIT / DG30 – inequity for patient populations
3. Low and High-risk implementation at same time
Emerging evidence from pilot studies supports this
Likely direction of travel for use of FIT in future
Likely greatest reduction in demand for endoscopy
Likely greatest financial savings
Outside current national guidelines
Greatest investment costs Requirement to introduce as
part of NHSE pilot programme – will require broad clinical support
4. DG30 and prepare actively for inclusion of high-risk patients
Same benefits as option 1 Able to implement in high risk
early when ready to, where greatest benefits for reducing demand likely to be seen
National recommendation in high risk may be different to that prepared for locally
May divert attention from implementation in low risk cohorts
102

11 | P a g e
SCHEDULE 2 – THE SERVICES
A. Serv ice Spec if ications
Service Specification No. NCL_FIT_01
Service Faecal Immunochemical Test
Commissioner Lead North Central London Clinical Commissioning Groups (NCL
CCGs)- NHS Camden CCG (UCLH¹), NHS Haringey CCG (NMUH¹), NHS Barnet CCG (RFL¹), NHS Islington CCG (WH¹), NHS Enfield
CCG (RFL¹) Provider Lead Not applicable
Period 2018/19 and 2019/20
Date of Review December 2019
1 . Population Needs
1.1 National/local context and evidence base
Colorectal cancer (CRC) is one of the most common cancers in England and the second commonest cause of cancer death. Diagnosis in symptomatic patients relies on identification of people with a
high risk of having cancer who should be referred for specialist investigations. This approach has limitations as many people with cancer present initially with low risk symptoms so diagnosis may be
delayed. Over half of all CRC is detected once the cancer has spread and a quarter after an emergency presentation to A&E, which are associated with poorer survival rates.
Quantitative Faecal Immunochemical Testing (qFIT or FIT) is a stool test that is highly sensitive for identifying bleeding in the gastrointestinal tract, a sign of CRC. FIT offers an improved method for
identifying people with significant risk of CRC who should be referred for investigation. Recently launched, NICE guidance DG30 recommends use of FIT in groups of symptomatic patients not
considered to have a > 3% risk of cancer – the threshold that should trigger an urgent suspected cancer (USC or 2 week wait) referral.
In London these patients are already included in 2ww referral recommendations due to the
limitations of the previously available stool test (guaiac FOBt). With the commissioning of FIT, they could now be offered this test first.
Use of FIT in people with symptoms suspicious of CRC is likely to lead to an increase in the speed of
CRC diagnosis for many patients, with a substantially higher proportion diagnosed via an USC route. Modelling also suggests there may be improvements in the number of people diagnosed with early
stage cancer and the proportion of patients satisfied with the time taken to diagnose them after they first present.
¹ Note UCLH- University College London Hospitals NHS Foundation Trust
NMU-North MIDDLESEX University Hospital NHS Trust
RFH- Royal Free London Hospital NHS Foundation Trust
WH- Whittington Hospital NHS Trust
Appendix 3 - Service Specification
103

12 | P a g e
2. O utcomes
2 .1 NHS Outcomes Framework Domains & Indicators
Domain 1 Preventing people from dying prematurely Yes
Domain 2 Enhancing quality of life for people with long-term conditions Yes
Domain 3 Helping people to recover from episodes of ill-health or
following injury
No
Domain 4 Ensuring people have a positive experience of care Yes
Domain 5 Treating and caring for people in safe environment and
protecting them from avoidable harm
Yes
2.2 Locally defined outcomes
O bjectives O utcome metrics
Detect CRC at an earlier stage of
disease
Percentage new CRC diagnosed at stage 1 & 2
Improved percentage <60 at stage 1 & 2 CRC
Diagnose CRC more rapidly after
c l inical presentation
Increased percentage CRC diagnosed via 2ww
Reduced percentage CRC diagnosed as emergency
Improve patient experience of
care
Improved NCPES* metrics for early diagnosis and
service coordination
Improve achievement of waiting
times standards
Improved CWT† performance, principally 2ww and
62d waiting times
More efficient use of NHS care Reduced unnecessary demand for endoscopy
Increased percentage of endoscopies which yield
diagnosis of CRC
Reduced demand for OPD gastroenterology and
colorectal surgery
*National Cancer Patient Experience Survey
3. Scope
3 .1 Aims and objectives of service
North Central London CCGs are seeking to commission Quantitative Faecal Immunochemical Test (FIT) service for colorectal cancer across North Central London STP footprint. A pathology service will deliver a comprehensive (end-to-end) FIT testing service, which will include:
Supply of sample test kit, Sample collection and transportation, Analyses of sample Reporting results to requesting clinicians in primary and secondary care settings using
systems that are compatible with existing patient administrative systems (EMIS, tQuest systems etc.).
The service will be delivered with secondary care providers across NCL (UCLH, NMU, RFH, WH) working consistently to the same quality standards, turnaround times and using the same analyser.
104

13 | P a g e
Offering the FIT test in primary care is expected to:
Improve early detection and diagnosis of colorectal cancer Supports primary care clinicians in decision making when referring patients on the 2ww
urgent pathway. Reduce outpatient appointments and demand on endoscopy services
Deliver care closer to home and avoid the need for onward referral for patients where
appropriate (i.e. patients with negative FIT result). Improve patient experience of primary and secondary care Reduce the number of repeat tests needed Improve patient compliance with test in primary and secondary care Deliver financial efficiency savings for providers and commissioners.
3 .2 Service description/care pathway
The service provider will:
Provide sample test kits including ‘how to’ leaflet and form for collecting patient
information to all GP Practices across NCL CCGs. Collect samples from GP Practices across NCL CCGs on a regular and at frequency to
ensure samples are suitable for analysis. Deliver the FIT test kit to GPs practices upon request. Analyse samples Communicate results in agreed format to requesting GP practice within five (5) working
days of collection of sample by laboratory transport.
Respond within 24 hours to any queries from primary care (GP practices)
3 .3 Population covered
The service outlined in this specification is for adult patients ordinarily resident of NCL CCGs as give
below ;
CCG Population NHS Barnet CCG 423,130 NHS Camden CCG 284,506 NHS Haringey CCG 318,151 NHS Islington CCG 252,200 NHS Enfield CCG 339,861 NCL CCGs Total 1,617,848
3 .4 Administering the test
NICE have recommended three technologies - The OC Sensor, HM-JACKarc and FOB Gold quantitative faecal immunochemical tests for adoption in primary care. Positive results should be reported using a threshold of 10 micrograms of haemoglobin per gram of faeces.
For consistency, all laboratories delivering the service across NCL CCGs will be required to adopt the same NICE- recommended analyser.)
3.5 Exclusion criteria • Samples / requests received from GPs outside NCL footprint will not be funded by NCL
CCGs
• FIT for Screening for National Bowel Screening Programme
105

14 | P a g e
3.6 Supplies
• The service provider will be responsible for supplying FIT kits to and collecting samples from all GP Practice premises in NCL footprint.
• FIT kits to include sample collection device, GP request form, and patient information leaflet on how to collect a sample.
• Supplier to monitors volume of FIT Kits used against supplied to GP practices to indicate when
supplies are running low.
• GPs practices to request supplies via existing mechanisms for ordering pathology consumables.
• All supplies are delivered within 5 days of receiving request.
3 .7 Interdependence with other services/providers
FIT testing for symptomatic patients in primary care is expected to impact on:
Endoscopy services
Lower GI Straight to Test pathways
There is interdependency with FIT for bowel cancer screening mainly in terms of patient and primary care education
3 .8 Record Keeping
The Provider MUST maintain adequate electronic records of the FIT tests provided. Full records should be maintained in line with data governance legislations and available to referrers, commissioners and regulators where appropriate.
Accurate, clearly formatted and complete data will be transmitted electronically to referring primary care clinicians to support their decision-making
For the contracted period, the provider MUST be able to provide patient level reports of all activity. These must cover a minimum data set to be agreed but must include the following:
Patient NHS number GP Practice/Practice Code Test results – value, positive / negative Turnaround time CCG of registration
Aggregated monthly reports on the above information will be required.
4 . Applicable Service Standards
4 .1 Applicable national standards (e.g. NICE)
The service will operate under the highest industry standards for FIT.
4 .2 Applicable standards set out in Guidance and/or issued by a competent body (e.g. Royal Colleges)
The service will operate under the standards for laboratories providing services to the NHS
106
15 | P a g e
4 .3 Applicable local standards To be confirmed
4 .4 Governance and Security As per other applicable pathology services
5 . Applicable quality requirements
5.1 Applicable Quality Requirements
The provider will be accredited to UKAS ( United kingdom accreditation service) under the International standard ISO 15189 Medical laboratory accreditation
Provider laboratories will be required to participate in an External Quality Assurance scheme for qFIT and be able to demonstrate acceptable performance of the test in the scheme
The method used should be CE marked and fit for the intended clinical purpose. Provider should refer to the implementation guidance in of NICE Guidance NG12 and
Diagnostic Guidance DG 30 to ensure compliance.
5 .1.1 Continuous Improvement
The NCL CCGs will seek to collect data and work with service providers to develop continuous improvement plans.
5 .1.2 Reporting
The provider will be expected to provide accurate, timely and comprehensive reports to commissioners to support payment and service evaluation and service development. Reports will include, but not limited to, the following details;
Number of requests by
Requester Code (GP Practice or Provider)
Month of request
Test kits issued and returned samples
Test Results (positive and negative)
Test result breakdown
% of successful test request per number of test kits per practice
FIT Read Code
Patients offered repeat tests
Report on number of complaints received and how they have been managed in line with NHS Standard Contract requirements
Turnaround times for sample collection and reporting Reports for Referrers
The service provider must supply the information requested by the commissioner in an agreed format and within agreed timescales. There will be occasions when the CCG(s) requests additional information or reports. The CCG(s) will indicate the purpose and priority of information requested, the service will respond to the CCG(s) within 24 hours. As a minimum, this will include:
Patient NHS number
107
16 | P a g e
GP Practice/Practice Code Test result (positive / negative ) READ Codes
5 .1.3 Suspension
The service may be suspended if service quality requirements are not met and provider is unable to deliver on an agreed rapid recovery plan.
5 .1.4. Exit Arrangements
Either party can exit this agreement by providing a minimum of 3 months written notice to exit the scheme.
Before issuing an exit notice, the parties will meet to discuss the reason for termination.
If, after this meeting, the reason for terminating is not resolved, then the relevant party will issue an exit notice.
This contract runs for the duration specified at the front of the document. Termination is possible through a three (month written notification by either party). The commissioner may initiate
termination on performance grounds at any stage subject to an agreed recovery plan.
5.2 Applicable CQUIN goals TBA
6 . Location of Provider Premises
The Provider’s Premises are located at: TBC
6 .1 Business Continuity
The service provider will maintain an effective business continuity plan detailing how, in the event of a major failure of the services, facilities or equipment the service can continue without disruption to CCG and GP Practices. The service provider will ensure that contingency arrangements are in place to ensure adequate available cover in the case of any planned or unplanned increases in workload and staff absences caused by sickness or travel disruptions.
Contingency arrangements are required for periods of IT system downtime which cannot be fixed within the contracted fix time standard and will subsist and therefore require alternative temporary arrangements to be put in place.
The service provider will use IT systems that are designed and configured to provide a high level of
fault tolerance. The service providers Information Technology department is required to constantly monitor system performance and service disruption on all systems.
No failure of NHS Digital or any other subcontractor supplying IM&T services or infrastructure will relieve the service of their responsibility for delivering services. Therefore, the service must have
108

17 | P a g e
an IM&T Systems disaster recovery plan to ensure service continuity and prompt restoration of all IM&T Systems in the event of major systems disruption or disaster.
7 . Individual Service User Placement
N/A
8 . Key Performance Indicators (KPI)
KPI Threshold By (Source) Time taken from receipt of test by lab to send result back to GP practice
5 working days Lab provider
Turnaround time for responding to queries
24 hours Lab provider
9. Activity Levels for the service
Indicative CCG Activity to be commissioned NCL CCG Barnet
CCG Camden CCG
Enfield CCG
Haringey CCG
Islington CCG
Total NCL CCGs
*Indicative 2019/20 annual ac tivity (DG30)
1,213 887 1,026 1,141 785 5,052
*Indicative activity numbers based on NCL modelling data
Indicative Provider Activity to be provided
Provider RFH UCLH WH NMU O ther Total
Indicative 2019/20 Activity *DG30)*
1,712
1,274
846
655
566
5,052
10. Finance for the service
10.1 Indicative service line budget for 2019/20 is £ indicative activity X local tariff for FIT 10.2 The NCL will pay the service provider £10.66 per FIT test carried out
109

18 | P a g e
Proposed lower GI pathway incorporating the FIT test for symptomatic
patients in North Central London
+ +
Higher risk
Red flag symptoms: Any of; Over 60 with iron deficiency anaemia
Rectal/abdominal mass
marked weight loss ‘gut feeling’
Lower risk
All other symptomatic (incl DG30). Any of; • Over 50 with unexplained abdominal pain or weight loss
• Under 60 with changes in bowel habit or iron-deficiency anaemia • 60 or over with anaemia without iron deficiency
+ve
Unexplained PR Bleeding
Patient not
compliant*
FIT Test
2WW Referral
STT Colonoscopy
<50 years
old
<50 yearss
old STT Sigmoidoscopy
<50 yearss old
STT Colonoscopy
<50 yearss old
Reassurance of
99% chance of no
cancer
<50 yearss old
GP safety netting
<50 yearss old
STT Colonoscopy
<50 yearss old
FIT Test
2WW Referral
Identify symptoms
FIT Test
2WW Referral
-ve
Patient with lower GI symptoms
V0.10
Last updated: 03 Jan 2019
≥50 years
old
<50
yearss old
GP safety netting
<50 yearss old
*If the patient remains non FIT compliant and
their symptoms progress causing increase GP
concern, then the patient is moved onto the
red flag pathway.
• Data collection & evaluation from each p/w will contribute to the national FIT pilot studies
• Low risk Green pathway patients referred to the symptomatic blue / red pathway without
FIT, will be assessed with FIT @ a face-to-face appointment by secondary care. If negative,
they will return to the green pathway.
Green = Phase 1 (early 2019) Red / Blue = Phase 2 (April 2019)
Suspected lower GI cancer
Suspected IBS/IBD Refer to your local
IBS/IBD pathway
including using
calprotectin test
FIT & Calprotectin
Have different roles in the patient with
colorectal symptoms.
• FIT detects red cells to help decision making in suspected colorectal cancer
• Calprotectin detects white cells to help decide between IBS & IBD, a
negative calprotectin is 98% predictive for the absence of IBD. It is not helpful if colorecta l
cancer is suspected
FIT for Bowel Screening is separate and not delivered through GPs
110

1
NCL Joint Commissioning Committee
Thursday, 7 February 2019
Report Title Summary of Moorfields Eye Hospital Consultation Programme
Date of report 25 January 2019
Agenda Item
4.2
Lead Director /
Manager
SRO Sarah Mansuralli Chief Operating Officer Camden CCG
Tel/Email [email protected]
GB Member Sponsor
Helen Pettersen Accountable Officer
Report Author
Denise Tyrrell Programme Director and Sarah Murray Programme Manager
Tel/Email [email protected]
Report Summary
This briefing updates the NCL JCC on the progress of the programme and pre-consultation engagement activities for the proposed relocation of Moorfields Eye Hospital from its City Road site - the proposal is known as Oriel.
Recommendation The Joint Commissioning Committee is asked to:
APPROVE the Committees in Common process. APPROVE delegated authority of nominated
representatives to attend the Committees in Common to formally launch the public consultation to inform the relocation proposal decision-making.
Identified Risks
and Risk
Management
Actions
The two most significant risks that have been identified are:
14 lead CCG Governing Bodies do not approve Committees in Common approach leading to delay
Stakeholder objections lead to delays These risks are to be expected on a programme of this size and complexity. They are being managed through stakeholder communications and engagement.
Conflicts of Interest
None noted at this stage.
Resource
Implications
Programme resource implications are being worked up in the Pre-Consultation Business Case (PCBC) which is being submitted to NHS England for assurance in spring 2019. The PCBC will be available to inform decision making for the Committees in Common.
111
2
Engagement
Through Oriel, Moorfields has been engaging with patient staff and public since 2012. Further pre-consultation engagement activities are being undertaken through 2018/ 2019.
Equality Impact
Analysis
An initial EQIA is in development to inform the PCBC. This will be available for review at the proposed Committees in Common meeting. Further detailed EQIA analysis will be undertaken through the programme phases.
Report History and
Key Decisions
NCL Joint commissioning Committee, Thursday 3 January 2019 NOTE programme activities to date AGREE agenda item for February JCC NCL Joint Commissioning Committee Thursday, 4 October 2018 4.1 Clinical Case for Change – Moorfields City Road Site Move Committees in Common process approved to date at: North East London Joint Commissioning Committee 9/1/19 Ealing CCG Governing Body 23/1/19 East and North Hertfordshire CCG Governing Body 24/1/19
Next Steps The programme team will work with the nominated representatives in preparation for the Committees in Common meeting. This meeting will take place once the Pre-Consultation Business Case assured by NHS England and the Consultation Document prepared.
Appendices
Summary of Moorfields Eye Hospital Relocation Proposal Programme Progress report.
Which CCG does this relate to
Barnet CCG, Camden CCG, Enfield CCG, Haringey CCG, Islington CCG
112

Summary of Moorfields Eye Hospital
Consultation Programme
NCL Joint Commissioning Committee
Thursday, 7 February 2019
V0.3_20 Dec 2018 MASTER
113

Introduction
This briefing updates the NCL JCC on the progress of programme and pre-consultation engagement activities for the
proposed relocation of services from Moorfields Eye Hospital on City Road - the proposal is known as Oriel.
In preparation for the establishment of a Committees in Common with the fourteen lead CCGs and NHSE Specialised
Commissioning, NCL JCC are asked to delegate authority of nominated representatives to attend the Committees in
Common to formally launch the public consultation to inform the relocation proposal decision making.
Background
For approximately five years, Moorfields has been exploring the opportunity to move from its current premises in City
Road to a state-of-the-art, purpose-built facility, which would offer significant potential to enhance the experience for
patients currently seen at its City Road premises.
Moorfields’ services are commissioned by CCGs across England, as well as NHS England, with some 14 London
commissioners holding significant contracts. NHS Camden CCG, on behalf of NHS Islington CCG as lead commissioner,
is representing commissioners across the country in this development.
The programme plans to continue engaging with patients, residents and other stakeholders in spring 2019 to get their
feedback on the proposed option to move Moorfields City Road to St Pancras and gather feedback on what is important
to them of any new development. This will help us refine our proposals and ensure these opinions inform future
development of Moorfields.
2114

There are a number of national, regional and local factors driving the need for change
• More patients will need treatment for eye conditions in the future , placing increased pressure on services
and facilities. This requires organisations to be agile, adapting their service models in response to changing
clinical and technological advances
• The rising incidence of eye disease requires the development of new techniques and technology to diagnose
and treat conditions. The City Road site constrains scientists and clinicians, with ageing facilities and a
configuration that hinders rather than facilitates innovation and interaction
• Patient feedback from the Friends and Family test and other sources has also highlighted factors associated
with the environment and specifically waiting times in clinics
• The Care Quality Commission (CQC) highlighted the impact of the current ageing estate at City Road on
patient experience, specifically in relation to privacy and dignity
• Exemplar organisations have demonstrated opportunities to generate efficiency and financial benefits by
tackling unwarranted variation in care across hospital eye services
• Commissioners, Moorfields Eye Hospital and its partners have set out a strategy outlining the drive to increase
patient satisfaction and create a joint research and medical facility to benefit both staff and patients
• This would place a centre for eye care, research and education in London with local, national and
international accessibility, close to the King’s Cross St Pancras International transport hub. It would be located
in the emerging MedCity1 knowledge zone, home to UCL’s world-renowned research community, Francis Crick 1 Institute, Wellcome Trust and more.
3
The Case for Change
1 MedCity London:, a collaboration between the Mayor of London and London’s health science centres of Imperial College London, King's College London and University College London.
115

Health and social care services in north London have
become ‘partners in health and care’ to improve the
access and quality of services, and to make the system
more efficient.
To achieve this, in June 2017 the North London Partners
(NLP) outlined a programme of transformation with four
elements:
Prevention: We will increase our efforts on prevention
and early intervention to improve health and wellbeing
outcomes for our whole population
Service transformation: To meet the changing needs of
our population we will transform the way that we deliver
services
Productivity: We will focus on identifying areas to drive
down unit costs, remove unnecessary costs and achieve
efficiencies, including working together across
organisations to identify opportunities to deliver better
productivity at scale
Enablers: We will build capacity in digital, workforce,
estates and new commissioning and delivery models to
enable transformation
North London Partners in Health and Care: working together for better health and care
4
This NLP vision for care services seeks to improve the
health and wellbeing of our population through
reduced health inequalities, addressing the wider
determinants of health and supporting care closer to
home, ensuring that when hospital care is needed, it
takes place in high quality buildings in the right
configuration.
A programme workstream is looking at ophthalmology,
and how North London Partners could improve patient
and staff experience and deliver better inpatient and
outpatient services across north central London, reducing
unwarranted variation in the services residents receive.
Estates is a core enabler to the delivery of this vision.
NLP wants to work towards a high quality, flexible and
accessible estate, which is appropriately utilised. Estates
can have a truly positive impact on the physical and
mental health and wellbeing of our communities and
staff.
NLP recognises the task ahead will be challenging, there
is considerable work still to do to continue to develop our
strategy and implementation plan for care in detail,
including working with our communities and residents to
develop plans.
116

Capital funding
North London Partners currently has two projects requiring capital funding that could affect residents and patients. These
were recently allocated £18m and £86m respectively by the Department of Health and Social Care (subject to the
outcome of consultation).
• Services currently provided at St Pancras Hospital for Camden and Islington Mental Health NHS Trust would
move to the Whittington Hospital site, as well as further investment in community hubs, long lease/sale of a substantial
part of the SPH site and construction of a new clinical (outpatient) facility for the trust at SPH, along with the
development of the Institute of Mental Health to be delivered in partnership between the Trust and University College
London.
• Of the land released, up to two acres of the St Pancras site could be sold to Moorfields Eye Hospital (MEH) for
the development of a new eye care, research and education facility with the UCL Institute of Ophthalmology (IoO)
known as Oriel. MEH would partially fund the move from the release of their Old Street site.
• The St Pancras Transformation Programme is not reliant on Oriel, but Oriel is reliant on the St Pancras
Transformation programme.
• Moorfields Eye Hospital NHS Foundation Trust, its research partners, the UCL Institute of Opthalmology and
Moorfields Eye Charity propose moving from City Road and Bath Road to the St Pancras hospital site by 2025/26. This
proposed move to the Kings Cross area would further enhance the Trust’s international reputation as a provider of
world-class patient care and clinical education, driving recruitment and providing a facility that will enable exceptional
training for the next generation of experts on national and global scale.
• Moorfields Eye Hospital is dedicated to improving patient and staff experience, and these proposals would deliver
an environment which would enable the Trust to deliver, and build on, its objectives through investing in the
clinical and educational experience of patient and staff.
Links with other North Central London proposals
5117

6
2011 to 2018 2018 2019 2020 to 2025/26
Trust-led activities to
initiate the proposed
Oriel programme
Public and patient
engagement to test
potential options.
Strengthened programme
leadership with
commissioner
involvement
London Clinical Senate
review that there is clear,
clinical evidence for the
proposals.
Strengthened patient
public and stakeholder
engagement
Consulting and involving a
wide range of patients,
local residents and
national service users who
use the specialist
services, including them in
developing the design
criteria for the potential
site.
Development of
preferred option from
engagement and
consultation feedback
Subject to consultation
outcome, further NHS
assurance would be
sought, and
implementation of the
proposed move to
create a centre for eye
care, research and
education in London
with local, national and
international
accessibility.
Timeline to date and proposed future timelines
118

7
Expected programme benefitsBuilt in partnership with patients, staff and students, this proposed new, integrated facility would improve patient
experience and enable clinicians and researchers to collaborate more freely, both in the UK and beyond.
A critical requirement would be to operate from a more flexible space given the way that patients navigate ophthalmic
care pathways now and in the future. The pace of innovation and change would continue to be rapid, with the
development of more sophisticated technologies. Patients must have access to facilities that would be more easily
adapted to these changes and developments in ways that are not possible at the City Road hospital in buildings over
100 years’ old.
Benefits to
residents, patients
and carers
• Improved, easier
and more
comfortable
patient experience
• Improved access
to counselling
services and
patient support
groups
• Access to other
care and support
services
• Improved care
pathway
Benefit to staff:
• Better working
environment
aiding recruitment
and retention
• Developing new
care pathways
would offer new
job opportunities
and the ability to
develop new roles
and approaches to
enhance career
opportunities
Benefit to future
research
New facilities would
broaden the scope
and scale of
research, securing
the availability and
access to the top
research talent and
better integrating
research with service
delivery so that the
benefits of research
are translated more
speedily into patient
care.
Benefit to training
and education
Integrating teaching
facilities alongside
UCL and service
delivery would
enhance and expand
the education and
training capability.
This would support
the development of
staff and students
that can meet the
increased demand
for eye care
professionals in the
future.
Benefit to the NHS:
Improving operating
efficiency is vital as
demand for services
increases. Efficient
care pathways will
be vitally important
for patients who still
need to come to
hospital, together
with services being
provided in the
community and in
primary care.
119

8
Process for NHS CCGs to consider proposals for City Road site move
Legal advice has been sought on the decision-making process. A full governing body of all fourteen CCGs is too large
and unwieldy to conduct an effective decision-making meeting. We therefore propose each CCG delegates the decision-
making function to a small committee, and that these then meet in common. This would minimise associated risks with
decision-making, such as:
• Ensuring that all decision-makers have access to the same information both in terms of documentation and also any
verbal presentations prior to making their decisions
• Sequencing decisions in such a way that all decision-makers are able to make decisions with an open mind
Legal considerations
Committees in Common
These committees of commissioners would
review the material and evidence for the
proposed site move and consult health scrutiny
in line with national legislation and guidance
120
9
Next steps
• Pre-consultation engagement
• Patients and residents
• Health, overview and scrutiny
• Staff
• Preparations for CCGs and JCC to run Committees in Common
• Committees in Common to review evidence and consult with health, overview and scrutiny
The NCL JCC are asked to delegate authority of nominated representatives to attend the Committees in
Common to formally launch the public consultation to inform the relocation proposal decision making.
Approval
121

NCL Joint Commissioning Committee Thursday, 7 February 2018
Report Title Risk Register for the Joint Commissioning Committee
Date of report 29 January 2019
Agenda Item
5.1
Lead Director /
Manager
Paul Sinden Director of Performance, Planning and Primary Care
Tel/Email [email protected]
Committee Member Sponsor
Not Applicable
Report Author
Paul Sinden, Director of Performance, Planning and Primary Care
Tel/Email [email protected]
Report Summary
North Central London Joint Commissioning Committee Risk Register
1. Introduction This paper provides an overview of the updated risk register for the North Central London CCG Joint Commissioning Committee. The risk register covers areas of commissioning delegated to the Committee by the five North Central London CCGs in November 2016. The risk register for the Committee, as at February 2019, is presented in accordance with the proposals agreed by the Committee in December 2018. The paper provides:
Updates made to the register for February 2019 compared to the last update in December 2018;
Risk scores including any changes.
2. Risks The Committee is asked to note the most material risks, with mitigated risk scores of 12 and above. Section 3 of the risk report provides an update on actions to mitigate risks:
Risk Mitigated score February 2019
28. System financial recovery from deficit position 20
13. Management of winter pressures 16
1. Delivery of 62-day waiting time standard 12
2. Delivery of 4-hour waiting time standard for A&E 12
20 Delivery of RTT waiting time standard 12
25. Ensuring effective contract management 12
26. Ensuring service delivery to support contract management 12
122

Recommendation The NCL Joint Commissioning Committee is asked to:
NOTE the report and updates to the Committee risk register as set out in section 3 of the risk report;
PROVIDE FEEDBACK on the risks included;
ADVISE on further development of strategic risks falling within the remit of the Committee;
APPROVE the changes to risk scores for JCC20, JCC21, and JCC22 as set out in section 2.1 of the risk report;
APPROVE the changes to the Committee risk register proposed for February 2019 onwards as set out in section 2 of the risk report.
Identified Risks
and Risk
Management
Actions
The risk register will be a standing item for each meeting of the Committee.
Conflicts of Interest
Conflicts of interest are managed robustly and in accordance with the NCL Conflicts of Interest Policy.
Resource
Implications
The risk register focuses on risks relating to delivery of the strategic objectives of the five CCGS in North Central London delegated to the Joint Commissioning Committee:
Commission the delivery of NHS constitutional rights and pledges;
Improve the quality and safety of commissioned services;
Improve health outcomes, address inequalities and achieve parity of esteem;
Maintain financial stability and ensure sustainability through robust planning and commissioning of value-for- money services.
Engagement
The report is presented to the NCL Joint Commissioning Committee which includes elected GP representatives, lay members, Healthwatch, Public Health and representatives from each NCL London borough.
Equality Impact
Analysis
This report was written in accordance with the provisions of the Equality Act 2010.
Report History and
Key Decisions
The initial risk register for the Joint Commissioning Committee has been developed with reference to existing risk registers from individual CCGs, and then updated for actions to mitigate existing risks and the addition of new emerging risks.
Next Steps Work is underway to streamline risk reporting across North Central London, with registers across the Sustainability and Transformation Plan, CCGs, the Joint Commissioning Committee and NCL CCG Primary Care Committee-in-Common.
Appendices
Joint Commissioning Committee Risk Register
123

North Central London Joint Commissioning Committee Risk Register
1. Introduction This paper provides an overview of the updated risk register for the North Central London CCG Joint Commissioning Committee. The risk register covers areas of commissioning delegated to the Committee by the five North Central London CCGs in November 2016. The risk register for the Committee, as at February 2019, is presented in accordance with the proposals agreed by the Committee in December 2018. The paper provides:
Updates made to the register for February 2019 compared to the last update in December 2018;
Risk scores including any changes.
2. Development of the risk register In December 2018 the Committee agreed to updates to the Committee risk register and within this that the risks to be reported on in February 2019 would be as per the table below. The table has been updated to incorporate mitigated risk scores for February 2019:
Risk Unmitigated risk score
Mitigated risk score Oct 2018
Mitigated risk score Dec 2018
Mitigated risk score Feb 2019
1 Delivery of 62-day waiting time standard 16 12 12 12
2 Delivery of 4-hour waiting time standard for A&E 16 12 12 12
3 Transforming Care -reducing inpatient care 9 9 9 9
9 Provider relationship to enable contract delivery 12 8 8 8
12 Ensuring quality of Transforming Care community packages
6 6 6 6
13 Management of winter pressures 20 16 16 16
20 Delivery of RTT waiting time standard 16 9 12 12
21 Effective integrated urgent care service 12 8 6 6
22 Successful in-housing of NELSCU contracts function 8 2 6 6
24 Delivering prevention whilst on PbR construct 12 8 8 8
25 Ensuring effective contract management 16 12 12
26 Ensuring service delivery to support contract management
16 12 12
27 Ensuring clarity in role of the JCC within overall CCG governance processes
12 4 4
28 Supporting system financial recovery through contracts 20 16 20
2.1 Risk scores Risk scores remain unchanged from December 2018 to February 2019 with the exception of JCC28: Supporting system financial recovery through contracts – the score has increase to 20 from 16 given the deficit positions reported by Barney, Enfield and Haringey CCGs in 2018/19 alongside provider deficits.
3. Updates to the risk register The Committee is asked to note that following updates to the existing risk register for December 2018 compared to October 2018: JCC 1: Delivery of the 62-day cancer waiting time standard. Delivery of the performance standard has been further supported recently by:
Development of a refreshed recovery plan across the UCLH Cancer Alliance covering North Central and Northeast London (NCEL) in November 2018 focusing on pathways with the most frequent breaches – prostate (urology) and bowel (lower GI). Recovery further supported by establishing the NCEL Task and Finish Group with decision-making membership from commissioners and providers;
Additional capacity in place for urology pathways (at UCLH) and bowel pathways (Royal Free London and North Middlesex University Hospital;
124

Follow-up with providers on areas of high risk – letter to UCLH requesting further assurance on management of the prostate pathway and investigation into the rising waiting list backlog at Royal Free London.
JCC2: Delivery of the 4-hour waiting time standard for A&E. Each A&E Delivery Board has implemented plans for winter 2018/19, with the plans focusing on maintaining emergency care pathway flow (with all systems showing a reduction in long lengths of stay in hospital beds and reduced ambulance delays), and ensuring capacity to deliver the waiting time standards for cancer and referral-to-treatment. All units have been under pressure over the winter period, particularly Barnet Hospital and North Middlesex University Hospital, but system winter plans have helped reduce the need for escalation calls (A&E Delivery Boards managing pressure locally). JCC3: Transforming Care – reducing inpatient care. The programme will continue into 2019/20 to support people with learning disabilities transfer into community packages of care from inpatient placements. The paper to the Committee in February 2019 demonstrates a reduction in inpatient placements with further progress with discharge of short-term admissions in January and February (admissions of much shorter duration than on prior occasions). JCC9: Relationships with providers not strong enough to support contract delivery. Work undertaken to strengthen relationships within NCL includes:
Borough-based “Intergreat” events held in January and February 2019 following the NCL event held in October 2018 to simulate an integrated care system;
Joint planning for 2019/20 underway through STP Directors of Finance Group including the approach to activity plans for 2019/20 submitted in January 2019. Initial operating plan submissions have focused on activity plans for 2019/20 (and as a baseline forecast outturn for 2018/19).
JCC12: Assuring the quality of Transforming Care Programme community packages of care. In February 2019 the Committee has received further patient case studies demonstrating the positive outcome of transferring care from inpatient placements into the community. JCC13. Ensuring that management of winter pressures supports recovery of waiting time standards for A&E and cancer and protects capacity for elective pathways. See update for JCC2 above. Surge hub support, provided by Northeast London Commissioning Support Unit (NELSCU), has been extended from 5 days to 7 days for the winter period. The surge hub support delivery of escalation actions as urgent and emergency care system pressure increases. JCC20: Delivery of referral-to-treatment (RTT) waiting time standard. All providers in NCL, with the exception of Royal Free London, are now maintaining their patient tracking list (waiting list) within March 2018 levels. Work to achieve this includes:
Establishment of NCL RTT Delivery Group to provide system-wide solutions to maintaining waiting lists within March 2019 levels. Providers have undertaken initial demand and capacity work to identify areas of deficit and surplus capacity to support NCL-wide work, and through this group capacity alerts have been put in place for pain management services at Royal Free London;
The introduction of clinical advice and guidance and tele-dermatology as an alternative to outpatient referral;
The on-going recovery plan at Royal Free London.
JCC21: Integrated Urgent Care service operates as an effective part of the overall urgent and emergency care system. Increased clinical triage built into the service specification and agreement of a sustainable contract for 2018/19 to carry forward into 2019/20. The NCL integrated urgent care service has shown greater resilience over the winter period than comparable services elsewhere in London. JCC24: Delivering prevention whilst on payment-by-results contract construct with acute hospitals. Work underway to support investment in prevention includes:
Work with acute providers on alternative contract forms and payment mechanisms;
Establishment of NCL Payment Mechanism Group, across commissioners and providers, to agree prices for new service developments;
Invest-to-save cases to reduce activity into acute hospitals including the FIT business case for bowl cancer screening (to JCC in February 2019).
125
JCC25: Ensuring effective contract management. Contract performance in 2018/19 will be monitored against CCG financial plans as well as contract baselines for each contract, as not all acute QIPP is contained within provider contract baselines. JCC reports have been established on this basis. Activity trend reports have been developed to help evaluate run-rates, the impact of Sustainability and Transformation Plan and QIPP interventions, and identify changes to counting and coding by providers. External support has been procured to maximise the yield from claims and challenges. JCC26: Ensuring service delivery to support contract management. Additional mitigations underway include:
A contract framework for 2019/20 has been developed to consider opportunities for using alternative contract forms and system incentives in support of STP delivery. Supporting contract negotiation strategies for the 2019/20 planning round have been developed for each provider;
Discussions on contract form for 2019/20 are underway with providers through the STP Directors of Finance and with the main acute providers;
A Payment Mechanism Group with providers has been established to agree local tariffs for Sustainability and Transformation Plan interventions where required including for tele-dermatology and Clinical Advice and Navigation;
Development of QIPP governance process across NCL to support delivery of interventions;
Streamlined reporting process for acute services agreed aligning reports to the Joint Commissioning Committee and CCG Committees to prevent duplication.
JCC28: Supporting system financial recovery through contracts. Mitigations underway include:
Publication of system intentions for 2019/20 with a focus on interventions that reduced overall system costs, and development of single delivery plans with providers;
This will be supported by the contract framework for 2019/20 and Payment Mechanism Group;
NCL-wide and Borough-based “Intergreat” events held with NCL STP stakeholders to simulate the introduction of local integrated care systems. The outcome will inform planning for 2019/20;
Establishment of Local Delivery Groups with providers to support delivery of QIPP and provider cost improvement programmes.
126

Risk ID Risk Title Risk Owner Strategic Update AUG OCT DEC FEB
JCC1
Delivery of Cancer 62-day
waiting time standard
(Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
Delivery of the performance standard has been further
supported recently by:
• Development of a refreshed recovery plan across the UCLH
Cancer Alliance covering North Central and Northeast London
(NCEL) in November 2018 focusing on pathways with the most
frequent breaches – prostate (urology) and bowel (lower GI).
Recovery further supported by establishing the NCEL Task and
Finish Group with decision-making membership from
commissioners and providers;
• Additional capacity in place for urology pathways (at UCLH)
and bowel pathways (Royal Free London and North Middlesex
University Hospital;
• Follow-up with providers on areas of high risk – letter to UCLH
requesting further assurance on management of the prostate
pathway and investigation into the rising waiting list backlog at
Royal Free London.
12 16 16 12 12
JCC2
Delivery of four-hour waiting
time standard for A&E
(Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
Each A&E Delivery Board has implemented plans for winter
2018/19, with the plans focusing on maintaining emergency care
pathway flow (with all systems showing a reduction in long
lengths of stay in hospital beds and reduced ambulance delays),
and ensuring capacity to deliver the waiting time standards for
cancer and referral-to-treatment. All units have been under
pressure over the winter period, particularly Barnet Hospital and
North Middlesex University Hospital, but system winter plans
have helped reduce the need for escalation calls (A&E Delivery
Boards managing pressure locally).
12 16 16 12 12
JCC13
Ensuring that management
of winter pressures supports
recovery of waiting time
standards for A&E and
cancer and protects capacity
for elective pathways
(Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
See update for JCC2 above. Surge hub support, provided by
Northeast London Commissioning Support Unit (NELSCU), has
been extended from 5 days to 7 days for the winter period. The
surge hub support delivery of escalation actions as urgent and
emergency care system pressure increases.
16 20 16 16 16
JCC Risks- Highlight Report2018/19
Movement From
Last Report
Target Risk
ScoreCurrent Risk Score
127

JCC20
Delivery of referral-to-
treatment (RTT) waiting time
standard (Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
All providers in NCL, with the exception of Royal Free London,
are now maintaining their patient tracking list (waiting list) within
March 2018 levels. Work to achieve this includes:
• Establishment of NCL RTT Delivery Group to provide system-
wide solutions to maintaining waiting lists within March 2019
levels. Providers have undertaken initial demand and capacity
work to identify areas of deficit and surplus capacity to support
NCL-wide work, and through this group capacity alerts have
been put in place for pain management services at Royal Free
London;
• The introduction of clinical advice and guidance and tele-
dermatology as an alternative to outpatient referral;
• The on-going recovery plan at Royal Free London.
9 16 16 12 9
JCC25
Ensuring effective contract
management (Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
Contract performance in 2018/19 will be monitored against CCG
financial plans as well as contract baselines for each contract, as
not all acute QIPP is contained within provider contract
baselines. JCC reports have been established on this basis.
Activity trend reports have been developed to help evaluate run-
rates, the impact of Sustainability and Transformation Plan and
QIPP interventions, and identify changes to counting and coding
by providers. External support has been procured to maximise
the yield from claims and challenges.
16 12 12
JCC26
Ensuring service delivery to
support contract
management (Threat
Paul Sinden, Director of
Performance, Planning and
Primary Care
Additional mitigations underway include:
• A contract framework for 2019/20 has been developed to
consider opportunities for using alternative contract forms and
system incentives in support of STP delivery. Supporting
contract negotiation strategies for the 2019/20 planning round
have been developed for each provider;
• Discussions on contract form for 2019/20 are underway with
providers through the STP Directors of Finance and with the
main acute providers;
• A Payment Mechanism Group with providers has been
established to agree local tariffs for Sustainability and
Transformation Plan interventions where required including for
tele-dermatology and Clinical Advice and Navigation;
• Development of QIPP governance process across NCL to
support delivery of interventions;
• Streamlined reporting process for acute services agreed
aligning reports to the Joint Commissioning Committee and
CCG Committees to prevent duplication.
16 12 12
128

JCC28
Supporting system financial
recovery through contracts
(Threat)
Paul Sinden, Director of
Performance, Planning and
Primary Care
Mitigations underway include:
• Publication of system intentions for 2019/20 with a focus on
interventions that reduced overall system costs, and
development of single delivery plans with providers;
• This will be supported by the contract framework for 2019/20
and Payment Mechanism Group;
• NCL-wide and Borough-based “Intergreat” events held with
NCL STP stakeholders to simulate the introduction of local
integrated care systems. The outcome will inform planning for
2019/20;
• Establishment of Local Delivery Groups with providers to
support delivery of QIPP and provider cost improvement
programmes.
20 20 16
Risk Key
Risk Improving ê
Risk Worsening é
Risk neither improving nor worsening but working towards target è
129

BAF Risk Heat Map
2 3 4 5
3
4
5
Consequence
Likelihood
2
1
1
Current Risk Score: Target Risk Score:x x
JCC 1JCC 1
JCC 2JCC 2
JCC 26
JCC 26
JCC 28
JCC 20
JCC 13
JCC 13
JCC 20
JCC 28JCC 25
JCC 25
130

1
NCL Joint Commissioning Committee Thursday, 7 February 2019
Report Title Planning for 2019/20
Date of report 24 January 2019
Agenda
Item
6.1
Lead Director /
Manager
Paul Sinden Director of Performance, Planning and Primary Care
Tel/Email [email protected]
Committee Member Sponsor
Report Author
Paul Sinden Director of Performance, Planning and Primary Care
Tel/Email [email protected]
Report Summary
1. Introduction This report provides an overview of the national framework for the planning round for 2019/20, and includes:
A summary of the NHS Long Term Plan published in January 2019;
A summary of the Planning Guidance for 2019/20 published in January 2019.
The planning guidance sets 2019/20 as being the foundation year for delivery of the NHS Long Term Plan. Guidance for 2019/20 therefore sets out a single operational planning process for commissioners and providers, service deliverables and operational standards for the year, and changes to the NHS finance system as the groundwork to delivering the NHS Long Term Plan. Within the planning guidance is a commitment to publish a clinical review of standards in spring 2019 that may change some of the operating plan deliverables. The overview of the planning guidance is supported by the following appendices:
Summary of operational standards for 2019/20; Summary of longer-term deliverables requiring preparatory work in 2019/20;
Timetable for the 2019/20 planning round, with provider contracts for next year to be signed by 21 March 2019.
CCG financial allocations have also been published and work is underway to cost the planning guidance requirements against those allocations and the uplift received by CCGs in 2019/20 compared to 2018/19. This includes the mandated uplifts to provider contracts, recovery of CCG deficits where required, and requirement to invest in mental health, primary care, and community services at least in line with CCG allocation uplifts. Access to the full versions of the NHS Long Term Plan and Planning Guidance are signposted in the paper.
131

2
Recommendation The Joint Commissioning Committee is asked to:
COMMENT on the NHS Long Term Plan and supporting national planning guidance for 2019/20;
IDENTIFY areas for priority, and of risk, for local planning for 2019/20.
Identified Risks
and Risk
Management
Actions
The main risks to delivering plans for 2019/20 are:
The need to align CCG and provider operating plans to support a reduction in system costs whilst delivering on operating plan priorities;
The need to better align system incentives to support delivery of Sustainability and Transformation Plan priorities and to reduce system costs;
Delivery of system plans within the resource envelopes of both CCGs and providers.
Conflicts of Interest
The report was prepared in accordance with conflicts of interest guidance.
Resource
Implications
Plans for 2019/20 will need to be developed within CCG resource envelopes and encompass run-rates from 2018/19 adjusted for demographic growth, the impact of Sustainability and Transformation Plan and local QIPP interventions, and the impact of national planning guidance.
Engagement
Plans should reflect the priorities identified through engagement with patients and public. Local CCG engagement timelines will be built into the process for generating plans, as well as being informed by on-going engagement structures.
Equality Impact
Analysis
This report was written in accordance with the provisions of the Equality Act 2010.
Report History and
Key Decisions
Planning for 2019/20 has been previously considered at STP Directors of Finance meetings and NCL CCG Contract Delivery Group. Local preparations for the 2019/20 planning round have been co-ordinated through the STP Directors of Finance meeting with both commissioner and provider leadership represented. CCG positions for the 2019/20 planning round will be co-ordinated through NCL CCG Senior Management Team.
Next Steps Plans for completing the planning round for 2019/20 will be will be further developed to account for:
Agreement of activity forecast outturn in 2018/19 and plans for 2019/20 with providers based on local STP and QIPP plans, and planning guidance priorities;
Borough-based “Intergreat” events being held in January and February 2019;
Delivery of operating plans and contracts in accordance with the national and local planning timetables.
Appendices
1. Summary of the NHS Long Term Plan; 2. Overview of national Planning Guidance for 2019/20 3. Overview of Sustainability and Transformation Partnership workstream
progress
132

3
The NHS Long-Term Plan
1. Overview of the plan This document provides a summary of the NHS Long Term Plan published in January 2019, building on the Five Year Forward View and addressing current concerns about the NHS (funding, staffing, increasing inequalities, and pressure from a growing and ageing population). The NHS Long Term Plan can be found here: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/01/nhs-long-term-plan.pdf and in summary form here: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/01/the-nhs-long-term-plan-summary.pdf
2. New Service Model for 21st Century Establishing new service model to give patients more options, better support, and joined up care at the right time and in the optimal care setting through a focus on: Boosting out of hospital care;
Reducing pressure on emergency hospital services;
Co-creation, empowerment and personalised care;
Digitally enabled primary and outpatient care; Population health and Integrated Care Systems.
Mechanisms to do this will include:
Greater use of on-line / digital access to GP consultations and outpatient appointments (reduce latter by up to 1/3);
Joined up care through primary care networks (30-50k populations);
New national standards for rapid response in community as alternative to hospitalisation, and increasing NHS support for people living in care homes;
Roll-out of social prescribing, personal budgets, and support for self-management of health in partnership with patient groups and the voluntary sector;
Backed by investment in primary care, community services, and mental health at a greater pace than growth in CCG allocations;
Establish urgent treatment centres, supported by national designation process and service specification, to relieve pressure on emergency departments;
Greater use of same-day emergency care to avoid overnight non-elective admissions;
New clinical standards for most serious emergencies; following work on trauma and stroke;
Continued focus with social care on reducing delayed transfers of care.
3. Focus on prevention and reducing health inequalities Aim to help people stay healthy and moderate demand on the NHS, with this being most effective with the NHS working with individuals, communities and broader economy (public and private). The plan therefore prioritises (funds) a series of evidence-based NHS prevention programmes focusing on reducing smoking, reducing obesity (in part through Type 2 diabetes prevention programmes), reduce alcohol related emergency admissions and lower air pollution.
Systems will be set measurable goals and mechanisms by which they will reduce health inequalities over the next 5 and 10 years, with this supported by changes to funding formulas to more accurately account for health inequalities and unmet need. Targets will include reducing smoking during pregnancy and for people with severe mental illness, better support for people with learning disabilities, autism, and who are homeless, finding employment for people with severe mental illness and improving the uptake of screening and early diagnosis of cancer.
4. Progress on care quality and outcomes Builds on existing improvements for safety in childbirth, cancer survival, reducing cardiovascular deaths, and lower male suicide rates. Given remaining unmet need and unwarranted variations in care and outcomes the plan goes beyond the priorities set out in the Five Year Forward View for cancer, mental
133

4
health, diabetes, multi-morbidity and healthy ageing including dementia to incorporate children’s health, cardiovascular and respiratory conditions, learning disabilities and autism.
5. Supporting NHS Staff NHS workforce implementation plan will be published later in 2019. A focus on matching workforce to rising demand, increasing the pipeline of training and university places to do this, improving access to, and funding for, clinical placements, expanding international recruitment, incentives for recruitment in hard to reach specialities and geographies, and creating flexible employment conditions to improve recruitment and retention (flexible rostering, funds for continuing professional development, support diversity and create culture of respect and fairness, create new roles and inter -disciplinary credential programmes; development of primary care networks, increasing the number of volunteers).
6. Digitally enabled care Investment in technology as an enabler for delivery of the NHS Long Term Plan with a focus on digital access to services, self-care by patients and carers, interoperability (access integrated health and care records), and access to decision support tools and Artificial Intelligence. Encourages the use of predictive techniques to plan and optimise care in integrated care systems and use of secure linked clinical, genomic and other data to support medical breakthroughs and consistent quality of care.
7. Value for money (taxpayers investment) Five year funding settlement from 2019/20 with average real-term annual funding increase of 3.4% to account for the current NHS financial pressures and then support the phased commitments in the plan to address ageing population and unmet need.
Funding uplift assumes the ability to invest in primary and community services and maintain recent investment trends in hospital services, but plan expects a reduction in hospital demand on implementation.
Delivery supported by changes to NHS financial architecture, payment systems and incentives. References reduction in admin costs – the 20% reduction in management costs, and annual 1.1% efficiency requirement.
8. Alignment with current transformation work: North Central London Sustainability and Transformation Partnership
There is strong alignment between the long term plan and the work already underway locally as part of the North Central London Sustainability and Transformation Partnership (STP). The clinical priorities set out in the plan are reflected through NCL wide programmes of work currently underway to improve outcomes and care for cancer, cardiovascular disease, maternity and mental health. This is combined with ongoing local work to redesign services as articulated in the plan. Locally we have made real progress already in: supporting the development of primary care networks (groups of practices typically covering 30–50,000 people); redesigning and simplifying emergency and urgent care services; and moving towards ‘digital first’ planned care services. The plans strong focus on both workforce and digital as drivers for change is also reflected in NCL work with dedicated programmes established locally to taking forward change in these areas. The STP programmes of work provide a strong foundation for further transformation work and have supported organisations working together in new ways. There is now an opportunity to review these areas of work and accelerate our plans through new commitments to system working in light of the move towards an integrated care system in North Central London. An overview of the work taking place in each STP programme and progress in quarter three of 2018/19 can be found in the appendix of this paper.
134

5
9. Next steps Next steps include:
Publication of clinical standards review and implementation framework for the plan in Spring 2019;
Establishing NHS Assembly in early 2019 to strengthen engagement on implementing the plan; Refresh of local systems plans by Autumn 2019 to support development of national implementation
programme;
Plan can be implemented without changes to primary legislation, but changes would support speed of delivery and being recommended;
Current legal framework allows creation of integrated care systems (ICS) by April 2021, working with local authorities at “place” level. ICS remove barriers referenced in Five Year Forward View – primary and specialist, physical and mental health, and health and social care.
135

6
NHS Operational and Planning and Contracting Guidance for 2019/20
1. Introduction The guidance sets 2019/20 as being the foundation year for delivery of the NHS Long Term Plan. The guidance for 2019/20 therefore sets out a single operational planning process for commissioners and providers, service deliverables and operational standards for the year, and changes to the NHS finance system as the groundwork to delivering the NHS Long Term Plan. F ive-year CCG allocations have also been published. The paper provides an overview of the planning guidance and is supported by the following appendices:
Summary of operational standards for 2019/20;
Summary of longer-term deliverables requiring preparatory work in 2019/20;
Timetable for the 2019/20 planning round. The full guidance for 2019/20 can be found at: https://www.england.nhs.uk/publication/preparing-for-2019-20-operational-planning-and-contracting/
2. System Planning The guidance states that a single operational planning process for commissioners and providers will be in place for 2019/20 with each system, whether a Sustainability and transformation Partnership (STP) or Integrated Care System (ICS) producing:
A system-level operating plan; and An aggregation of system data (for each individual CCG and provider) across finance, activity,
contracting and workforce to demonstrate system alignment. The guidance is designed to align commissioner and provider plans around collective priorities, with realistic assumptions for capacity and activity to provide the framework for individual organisational plans. The system focus is supported by system control totals (aggregate of individual commissioner and provider control totals) that can be moved across organisations on a net neutral basis (no change to overall system control total) if agreed with NHS England and NHS Improvement.
3. Finance Changes to the financial system in 2019/20 are designed to facilitate establishing Integrated Care Systems, with all areas of country targeted to be part of an Integrated Care System by April 2021. Payment reform
Tariff uplift 3.8%, subject to final consultation (final tariff published on 11 March 2019). Prices will be further uplifted by the transfer in of CQUIN funds (1.25%) and part of the provider sustainability fund into urgent and emergency care prices;
Efficiency factor 1.1%; Blended payment approach implemented for emergency care activity (marginal rate of 20% for
variances from plan) covering A&E attendances, non-elective admissions, ambulatory care and same day emergency care. Plans can be reset in-year for significant variances from plan – a “break-glass” clause;
Emergency tariffs further simplified by removing the marginal emergency rate tariff (MRET) and 30-day readmissions rules on a financially neutral basis between commissioners and providers;
CQUIN simplified and reduced to 1.25% in 2019/20 compared to 2.5% in 2018/19 (balance into provider prices);
Provider financial framework An overall focus on moving all providers to financial sustainability through:
Phased introduction of revised market forces factor payments to providers over a five -year period;
136

7
Balance of provider sustainability funds (net of transfer into urgent and emergency care prices) available to providers signing-up to their control total for the year). Sign-up also limits contract sanctions applicable to those providers;
Creation of new financial recovery fund (FRF) that providers can also access in 2019/20 on sign -up to their control totals. Access from 2020/21 will also require an agreed financial recovery plan to remove deficits. By 2023/24 no Trusts are expected to be in deficit. In 20201/21 the provider sustainability fund will be merged into the financial recovery fund;
Providers will receive rebased control totals for 2019/20 in January 2019 based on the above, with providers in a deficit position required to deliver an additional 0.5% efficiency over and above the national 1.1% requirement;
A review of cash regime for providers including interest payable on historic debt and new loans, and in some cases a restructuring of historic debts.
Commissioner financial framework
Allocations formulae updated to provide greater sensitivity to addressing health inequalities an unmet need, and accommodates updated needs assessments for mental health and community services;
CCG allocations for the next five years (from 2019/20) were published alongside the planning guidance, with work underway locally to calculate the cost of operating plan requirements against the allocations;
Headline growth in CCG allocations are summarised below. Allocations growth (alongside QIPP plans) will be used to cover operating plan applications including resolution of recurrent deficits.
Allocations % uplift
in 2019/20
Barnet Camden Enfield Haringey Islington NCL
Core CCG +6.1% +4.9% +5.9% +6.3% +5.4% +5.7%
Delegated primary
medical services
+6.8% +6.8% +6.5% +6.5% +7.1% +6.7%
Confirmation of 20% reduction in CCG running costs to be in place by April 2020 (plans prepared in 2019/20);
Specialised Commissioning
Plans to integrate specialist services into local systems to be developed during 2019/20; Funds for specialist services not included in system control totals for 2019/20. Productivity and efficiency
Minimum efficiency requirement of 1.1% per annum over the next five years;
To support productivity and efficient improvements the guidance references: System estates strategies to improve utilisation; NHS RightCare programme with a focus on cardiovascular and respiratory services; Use of Innovation and Technology Fund including the use of blood glucose monitoring devices for
people with Type 1 diabetes; National guidance on evidence based interventions for procedures and prescribing;
The guidance identifies areas of further work to improve productivity and efficiency in 2019/20 and future years: Transforming outpatient services by replacing up to 1/3 of face-to-face attendances into digitally-
enabled operating models; Use of mobile devices and digital services by staff to improve the productivity of community services
for both physical health and mental health; Improving the availability and deployment of clinical workforce through e-rostering and e-job
planning standards; Reducing unwarranted variations through the Getting It Right First Time (GIRFT) programme; Secure procurement savings by increasing standardisation and working collaboratively across
organisations including securing value from medicines and pharmacy, establishing pathology and imaging networks, and improving corporate services.
137
8
4. Operating plan requirements Appendix one provides a summary of operational standards for 2019/20, and appendix two sets out longer-term deliverables requiring preparation in 2019/20 for delivery in subsequent years. Emergency Care – Priorities for emergency services in 2019/20 include:
All emergency departments to operate a same day emergency care service (12 hours per day 7 days per week by September 2019) to increase the proportion of acute admissions discharged on the day of attendance;
Avoidable admissions to be prevented through hospitals setting up acute frailty services delivering comprehensive geriatric assessments in emergency departments and assessment units;
Continue to work with social care to reduce long-stay patients (in hospital for 21 days or more) and delayed transfers of care in line with Better Care Fund targets;
NHS 111 Clinical Assessment Services to be in place by April 2019 to support triage of patients to appropriate services;
Redesign urgent care services outside of emergency departments supported by national designation process for urgent treatment centres to be completed by December 2019;
Delivery of ambulance response programme standards;
Note the clinical standards review will develop new ways to focus on patients with the most serious illnesses and injuries.
Referral-to-treatment (RTT) times – in-year reduction in waiting lists is expected from all providers supported by:
Patients waiting in excess of 6 months being offered care from an alternative provider; Elimination of waits in excess of 52 weeks (fines for both providers and commissioners for breaches);
Roll-out of capacity alerts;
Redesign of outpatient pathways to accelerate the use of non-face-to-face interventions and alignment of diagnostic tests with appointments;
Cancer – all waiting time standards in the NHS Constitution remain in place, and providers will start to collect 28-day faster diagnosis standard data items in preparation for the introduction of the standard in 2020. Cancer Alliances established to bring commissioners and providers together to deliver a system-wide cancer plan covering operational performance and transformation (UCLH Cancer Alliance locally covering North Central and Northeast London). Mental Health – continue to implement five year forward view for mental health, and associated mental health investment standard, in 2019/10. Guidance indicates that CCG allocations for 2019/20 include funds for implementing NHS Long Term Plan priorities for mental health, and therefore progress with implementing service developments for community mental health teams for people with severe mental illness, enhanced crisis services for adults and for children and young people, and perinata l mental health services should be made. Learning disabilities – the Transforming Care Programme is extended to 2019/20 with a further reduction in inpatient care targeted for people with a learning disability and/or autism. Primary care and community health services - a focus on delivery of the General Practice Forward View (supported by investment) through:
Development of primary care networks to ensure full coverage by June 2019 supported by £1.50 per head investment (some investment already in place in NCL) and data analytics for population segmentation;
Investment in primary and community services over and above CCG allocations uplifts, with progress in implementing the new models of care set out in the NHS Plan new service models to be delivered in return including the urgent response standards for urgent community support (2 -hour rapid response service offer)
Development of primary care strategy to implement the above as part of local response to NHS Long Term Plan and required improvement to population health – general practice strategy for NCL developed in 2018/19;
138

9
Internal audits into delegated commissioning of primary medical services (GP contracts) to ensure delegated authority undertaken effectively - 2 audits undertaken in 2018/19.
Workforce – develop workforce plans to address supply and retention and that align to finance and activity plans. Plans to explore new ways of working to help further reduce temporary staffing costs. Data and Technology – Providers will be required to submit all commissioning datasets to the Secondary Uses Service (SUS+) on a weekly basis from April 2019, continuing with existing requirements for other datasets. The guidance states that, during 2019, a number of core sta ndards will be mandated for technology in use across the NHS including addressing interoperability and cyber security. Commissioners and providers also requested to support national roll out of the NHS App and encourage use of the Diabetes Prevention Programme. Personal Health Budgets – increase the number of personal health budgets in place as per current operating plan trajectories. Longer-term deliverables – Appendix 2 sets out service developments prioritised in the NHS Long Term Plan requiring preparatory work in 2019/20.
5. Process and timescale
Appendix three provides a summary of the local timetable for the 2019/20 planning round that incorporates the deadlines set out in the national timetable included in the planning guidance, with provider contracts for 2019/20 to be signed by 21 March 2019.
139
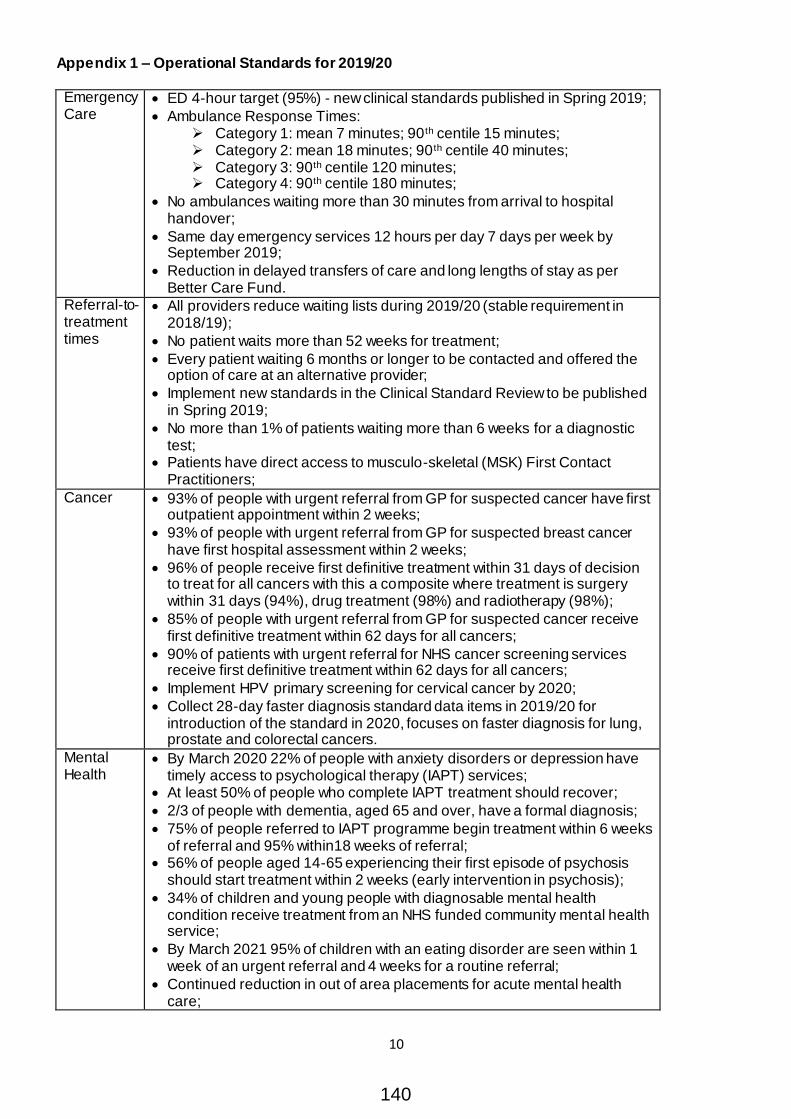
10
Appendix 1 – Operational Standards for 2019/20 Emergency Care
ED 4-hour target (95%) - new clinical standards published in Spring 2019;
Ambulance Response Times: Category 1: mean 7 minutes; 90 th centile 15 minutes; Category 2: mean 18 minutes; 90 th centile 40 minutes; Category 3: 90th centile 120 minutes; Category 4: 90th centile 180 minutes;
No ambulances waiting more than 30 minutes from arrival to hospital handover;
Same day emergency services 12 hours per day 7 days per week by September 2019;
Reduction in delayed transfers of care and long lengths of stay as per Better Care Fund.
Referral-to-treatment times
All providers reduce waiting lists during 2019/20 (stable requirement in 2018/19);
No patient waits more than 52 weeks for treatment;
Every patient waiting 6 months or longer to be contacted and offered the option of care at an alternative provider;
Implement new standards in the Clinical Standard Review to be published in Spring 2019;
No more than 1% of patients waiting more than 6 weeks for a diagnostic test;
Patients have direct access to musculo-skeletal (MSK) First Contact Practitioners;
Cancer 93% of people with urgent referral from GP for suspected cancer have first outpatient appointment within 2 weeks;
93% of people with urgent referral from GP for suspected breast cancer have first hospital assessment within 2 weeks;
96% of people receive first definitive treatment within 31 days of decision to treat for all cancers with this a composite where treatment is surgery within 31 days (94%), drug treatment (98%) and radiotherapy (98%);
85% of people with urgent referral from GP for suspected cancer receive first definitive treatment within 62 days for all cancers;
90% of patients with urgent referral for NHS cancer screening services receive first definitive treatment within 62 days for all cancers;
Implement HPV primary screening for cervical cancer by 2020;
Collect 28-day faster diagnosis standard data items in 2019/20 for introduction of the standard in 2020, focuses on faster diagnosis for lung, prostate and colorectal cancers.
Mental Health
By March 2020 22% of people with anxiety disorders or depression have timely access to psychological therapy (IAPT) services;
At least 50% of people who complete IAPT treatment should recover;
2/3 of people with dementia, aged 65 and over, have a formal diagnosis;
75% of people referred to IAPT programme begin treatment within 6 weeks of referral and 95% within18 weeks of referral;
56% of people aged 14-65 experiencing their first episode of psychosis should start treatment within 2 weeks (early intervention in psychosis);
34% of children and young people with diagnosable mental health condition receive treatment from an NHS funded community mental health service;
By March 2021 95% of children with an eating disorder are seen within 1 week of an urgent referral and 4 weeks for a routine referral;
Continued reduction in out of area placements for acute mental health care;
140

11
At least 60% of people with a severe mental illness should receive a full annual physical health check;
Co-location of mental health therapists in primary care to extend access to psychological therapies (supported by recruitment programme);
Other targets relate to perinatal mental health, all age crisis and liaison services, early intervention in psychosis, and reducing suicides.
Learning Disabilities and Autism
Reduce reliance on inpatient care for people with a learning disability and/or autism – to 37 inpatients per million adult population by March 2020 (Transforming Care Programme) - split 50/50 between CCG funded and specialist commissioning funded placements;
75% of people on the learning disability register have an annual health check;
CCGs undertaking Learning from Deaths report (LeDeR) reviews co-ordinated through a steering group, with named lead, with reviews carried out within 6 months of notification of death, with systems in place for analysing and addressing themes and recommendations from the reviews, and with the above summarised in an annual report presented to relevant committee for all statutory partners.
Personal Health Budgets
Increase the uptake of personal health budgets
141

12
Appendix 2 – Longer-Term Deliverables System architecture
All areas of country part of an Integrated Care System by April 2021
Health Inequalities
Establish plans in 2019 to reduce health inequalities by 2023/24 and 2028/29 including equity of access and equity of outcome
Maternity Continuity of carer model to improve outcomes for most vulnerable mothers and babies;
Smoking cessation support for all women who smoke during their pregnancy;
50% reduction in stillbirth, maternal and neonatal mortality, and serious brain injury by 2015;
By Spring 2019 all maternity and neonatal units to be part of National Maternal and Neonatal Health Safety Collaborative, supported by Local Learning Systems;
Roll-out Saving Babies Lives Care Bundle during 2019;
Extend the offer of maternity digital care records by October 2019; By March 2021 most women will receive continuity of the person caring for
them during pregnancy, during birth and post-natal care;
All maternity services not delivering accredited or evidence-based infant feeding programmes to start the accreditation process in 2019/20.
Mental health
By 2020/21 ensure more people living with severe mental health problems have their physical health needs met;
Deliver enhanced mental health services to children and young people; Roll-out mental health support teams working in schools and colleges;
Expand access to psychological therapy services (IAPT) for adults and older adults with common mental health problems, with a focus on those with long-term conditions;
Progress delivery of standards for early intervention in psychosis, IAPT, and eating disorder services for young people by 2021
Learning disability and autism
Expand programmes to stop the overmedication of people with learning disability and/or autism;
Further reduce the number of people with learning disability and/or autism in inpatient care.
Cancer Offer HPV vaccination to all boys aged 12 and 13 from September 2019 to prevent HPV related diseases;
Extend lung health checks from national pilot sites;
Roll-out of new Rapid Diagnostic Centres from 2019; Implement stratified follow-up for breast cancer in 2019 and for prostate
and colorectal cancers in 2020 with full roll-out for relevant cancers by 2023, aligned with introduction of quality life metric in 2019 to track and respond to the long-term impact of cancer.
142

13
Appendix 3 – Planning timetable
Step or Key Deliverable Completion Date
National / Local
deadline
Owners
Publication of planning guidance for 2019/20 and CCG allocations
21 Dec 2018 National
Agree methodology for 2018/19 activity outturn (for contracting purposes)
21 Dec 2018 Local CCGs/Trusts
Agree joint plan to deliver the contract baseline incorporating provider Cost Improvement Plans and CCG QIPP plans
7 Jan 2019 Local CCGs/Trusts
2019/20 – initial plan submission –activity rather than finance
14 Jan 2019 National CCGs/Trusts
Publication of NHS Long-Term Plan Jan 2019 National
Formal contract offers made to providers 21 Jan 2019 Local CCGs
Provider formal response to CCG contract offers 29 Jan 2019 Local Providers
Agree 2019/20 activity baselines 5 Feb 2019 Local CCGs/Trusts
2019/20 second cut operating plans submission 12 Feb 2019 National CCGs/Trusts
Aggregated system operating plan submissions and system operating plan narrative
19 Feb 2019 National CCGs/Trusts
Agree terms for any contract variations post planning and tariff guidance including any MFF changes
28 Feb 2019
Local CCGs/Trusts
Local escalation process for baselines not agreed 28 Feb to 18 March 2019
Local CCGs/Trusts
2019/20 national tariff published 11 March 2019
National
Agree HRG-level 2019/20 Indicative Activity Plans and Joint CIP/QIPP Plans (with phasing)
18 March 2019
Local CCGs/Trusts
2019/20 NHS Standard Contracts signed 21 March 2019
National CCGs/Trusts
Trust Board / CCG Governing Body approval of budgets for 2019/20
29 March 2019
National CCGs/Trusts
Final submission of operating plans for 2019/20 4 April 2019 National CCGs/Trusts
Aggregated system operating plan submissions and system operating plan narrative
11 April 2019 National CCGs/Trusts
143

North London Partners in Health and CareNorth Central London STPQuarterly update21 December 2018
144
Ambition for the STP is built on existing CCGs, Local Authorities
and Providers values and strategy
Improve the health and wellbeing of the local
population
Reduce health inequalities
Maximise out of hospital care and build resilient well
supported communities
A partnership of the NHS and local authorities, working together with the public and patients where it’s the most efficient and effective way to deliver improvements.
Ambitions of the STP 1.
145
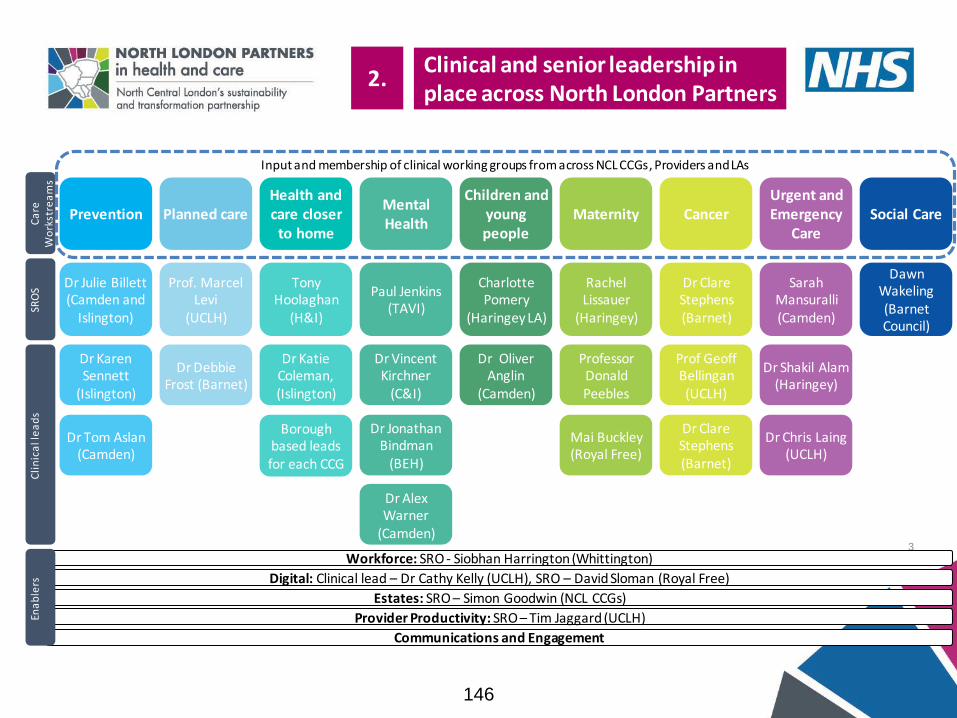
3
Prevention Planned care Mental Health
Maternity Urgent and Emergency
Care
Health and care closer
to home
Children and young people
Cancer
Dr Julie Billett(Camden and
Islington)
Prof. Marcel Levi
(UCLH)
Paul Jenkins(TAVI)
Rachel Lissauer
(Haringey)
Sarah Mansuralli(Camden)
Tony Hoolaghan
(H&I)
Charlotte Pomery
(Haringey LA)
Dr Clare Stephens(Barnet)
Dr Clare Stephens(Barnet)
Dr Karen Sennett
(Islington)
Dr Vincent Kirchner
(C&I)
Professor Donald Peebles
Dr Shakil Alam(Haringey)
Dr Katie Coleman, (Islington)
Dr Oliver Anglin
(Camden)
Prof Geoff Bellingan(UCLH)
Cli
nic
al l
ea
ds
Dr Tom Aslan (Camden)
Dr Jonathan Bindman
(BEH)
Dr Alex Warner
(Camden)
Mai Buckley(Royal Free)
Dr Chris Laing(UCLH)
Dr Debbie Frost (Barnet)
Borough based leads for each CCG
Social Care
Dawn Wakeling (Barnet Council)
Workforce: SRO - Siobhan Harrington (Whittington)
Digital: Clinical lead – Dr Cathy Kelly (UCLH), SRO – David Sloman (Royal Free)
Estates: SRO – Simon Goodwin (NCL CCGs)
Provider Productivity: SRO – Tim Jaggard (UCLH)
Communications and Engagement
SRO
SC
are
W
ork
stre
am
sEn
ab
lers
Clinical and senior leadership in place across North London Partners
2.
Input and membership of clinical working groups from across NCL CCGs, Providers and LAs
146

Working with our partners on integrated care:
• In October, we held a simulation event held to build our collective vision for integrated care systems and how this might work across the population of North Central London. Following this a national bid submitted to support next steps in our development.
• Proposed next steps: Sharing event write-up (Oct 2018); stakeholders, residents and orgs debate the principles from the event and provide initial feedback (Dec 2018), secure national and local funding to support ICS development (Nov 2018), plan and deliver further
‘Inter-great’ events (Nov 2018-Feb 2019 including borough-based events in Jan-Feb 2019), capture learning and develop potential options for how ICSs could be developed across NCL (Jan-Mar 2019), Apply for next wave of Aspirant ICS funding (TBC), start to discuss options widely with Trusts, Local Authorities, CCGs, patients etc (Spring 2019)
Urgent and Emergency Care:
• This winter providers across NCL are supporting more patients with immediate health or functional needs, and who would otherwise require an admission to hospital, to stay at home and receive care. Across NCL we have standardised elements of our admissionavoidance rapid response services to make it easier for clinicians to refer patients as well as discharge pathways. NCL is the first area in the country to launch 111 *9 which enables clinicians to directly access any rapid response service in NCL.
Planned Care • Standardised urology pathways implemented across primary and secondary care in the first half of 2018 have resulted in a 10%
reduction in outpatient activity and a high level of satisfaction amongst clinicians. The intention is to reduced unwarranted variation and improve quality of care. This works is believed to be unique to NCL and is attracting national interest.
• Significant progress in NCL is occurring on the implementation of the new advice and guidance service for GPs. The service allows GPS to securely submit clinical queries to consultants when considering a referral. Since April 2018 there has been over 4,500 submissions, 66% GP practices have used the service. The service seeks to reduce unwarranted referrals and provide specialist opinions seamlessly into primary care.
Orthopaedics review• The Orthopaedic review evaluation was reported to the December CCG Joint Commissioning Committee (JCC). In January, the JCC will be
asked to endorse the next steps and governance for the next phase of the review.• In parallel to this, a number of clinical design workshops have taken place, which began to explore in more detail how elective
orthopaedic services might be organised in the future, how services could be designed, the key interdependences and critical factors that need to be considered in the next stages of the review. Both the engagement exercise and design workshops have seen a wide range of participation and provide a strong foundation for next steps. Feedback from the engagement exercise is currently being independently evaluated and will be shared with the NCL CCG’s Joint Commissioning Committee
who will decide on the next steps for the review.
Headlines from across the programme
3.
147

Care home nurses and acute nurses trial exchange scheme
A CapitalNurse/HEE programme found that care home nurses feel misunderstood by their acute nursing colleagues and the reverse is also true. The misunderstandings have impacted on good collaboration on patient/resident care and on clinical outcomes.
A three month trial exchange scheme to share experiences is underway involving nurses from elderly medicine and UEC at Whittington Health and care home nurses working in three Islington homes run by Care UK.
Residents offer their views on challenges and opportunities in developing integrated care systems
Twenty six residents attended a workshop hosted by the North London Partners to get an understanding of what an integrated care system might mean for local people, identify potential challenges and benefits that such a system could offer.
The residents identified a number key benefits including: the potential to tailor services around individuals, provide a person-centred approach with a single point of access for all a patient’s health and care needs. Key challenges that were discussed included: lack of communication between organisations due to differences in culture and ways of working and systems not being in place to share information.
To further develop a case for integrated care the residents made a number of recommendations including: talking directly to patients and their families about what is working and to identify their requirements and getting out into the community to meet with disadvantaged groups. There will be follow up workshops across the NLP boroughs in 2019.
Digital work to transform health and care underway Our programme to join-up health and care records across our five boroughs is progressing well. There are two main strands to the programme: • Health Information Exchange (HIE) is an application that
will provide a summary of our residents’ health and social care information together in one easy-to-view real-time record.
• HealtheIntent is a tool which allows an increased collective ability to be more proactive in the care of our communities. The system takes elements of health and care information from different sources and enables us to manage groups of residents in relation to health or social condition. It will also give richer and more up-to-date information to help us plan future services.
Access to both tools, and the new ways of working that they enable, is being introduced gradually across the five boroughs, starting with a number of early adopter sites. Barnet has been identified as the early adopter for HIE, and we are currently working with primary care colleagues to agree on practices that will introduce the shared record by March 2019. Initially the shared record will contain primary care data alongside data from the main acute provider for the area, the Royal Free Hospital group.
We are in discussions with the Haringey and Islington Wellbeing Partnership about their becoming early adopters of HealtheIntent (focused on North Islington and North Tottenham).
Some examples of enabling transformation
4.
148

Health and
Care Closer to Home
SRO: Tony
Hoolaghan
Overall workstream objective
‘Place-based’ population health system of care; based around neighbourhoods of 50-80k; drawing together social, community, primary & specialist services; underpinned by a systematic focus on prevention & supported self-care.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• NCL GP strategy approved by all NCL CCG governing bodies • HCCH approved bids for primary care improvement grants for 18/19 and 19/20• Second tranche of primary care transformation funding (£800k) approved• Bid for further £500k to support foundations of integration (NHSE national) • Online consultation provider selected
• Priorities for integrated networks for 19/20 agreed with providers• Time for Change (mental health) collaborative rolled out
• Locally Commissioned Services approach agreed for 19/20
• Approval and mobilisation of social prescribing business case
Priority project Impact* Major Independencies Key Care Settings Partner involvement
CHIN/Neighbourhood C Workforce, Estates, Digital GP practices, social care, community Partners involved:• CCGs, GP, community pharm , Mental Health & Social CarePotential future commitments:• North Central London (NCL)-wide approach to Atrial Fibrillation
improvement • NCL model for social prescribing• Enhanced services review• Contracting for Care & Health Integrated Networks
Quality Improvement £, Q Workforce Virtual, GP practices
P. Care Commissioning £, Q, E CCGs, GPs
Social Prescribing £, Q Workforce GP practices, social care, community
Primary Care at Scale £, Q, P, E GP practices
* £ = Savings, Q = Quality, P=Performance, E=Efficiency, C=Clinical Outcomes
Planned
CareSRO:
Marcel Levi
Overall workstream objective
Deliver better value planned care through new models of care and reducing unwarranted variation across providers.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)
• Clinical advice and navigation live across all acute sites and specialities with 900 queries each month
• NCL CCGs signed off consistent evidence based POLCE policy
• Teledermatology service to go live using smartphone dermascope in primary care • Further work on POLCE to incorporate national Evidence Based Interventions guidance
Priority project Impact* Major Independencies Key Care Settings Partner involvement
POLCE £, Q, C - GPs, Providers Partners involved:• Acute Providers, CCGs, GPsPotential future commitments:• Implement Common NCL ‘Using NHS money wisely / Procedures
of Limited Clinical Effectiveness (PoLCE) Policy• Teledermatology and Advice and Navigation services
implemented across NCL• Involvement in orthopaedic review
Advice & Navigation £, Q, P, E, C Digital GPs
Dermatology £, Q, C Digital GPs, Acute Providers
Urology £, Q, C HCCH Acute Providers
Orthopaedic review £, Q - Acute Providers
UEC
SRO: Sarah Mansuralli
Overall workstream objective:
A consistent and reliable Urgent and Emergency Care (UEC) service by 2021 that is accessible to the public, easy to navigate, inspires confidence, promotes consistent standards in clinical practice and leads to a reduction in variation of patient outcomes. Key areas of work focus on admissions avoidance, ambulatory care, end of life care and discharge to assess.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• £315k in ‘UEC transformation funding’ has been approved by NHSE to support
timely discharge of mental health and delirium patients from A&E settings.• ‘Supporting patients’ choices to avoid delayed discharge’ policy launched in NCL. • NCL rapid response ‘core offer’ finalised and with CCGs for final approval.• 111*9 soft launch for ease of routing referrals to rapid response teams. • Stroke business case (to increase rehab in community settings) approved
• Acute hospitals working to increase ambulatory care • Implementation of Trusted Assessor and discharge to assess pathway across NCL • Implementation of revised Single Point of Access services for last phase of life care.
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Integrated urgent care £, Q, P, E, C Digital Acute, GPs, Pharmacies, NHS111 Partners involved:• Acute Trusts, Community services, MH providers GP Practices;
Care HomesPotential future commitments:• Last phase of life single point of access model
Admission avoidance £, Q, P, E, C Digital, Workforce Acute, GPs / Community
Simplified discharge £, Q, P, E, C Digital, Social Care Acute, Care Homes, Community
Last Phase of life £, Q, P, E, C Digital, Social Care Care Homes, NHS111, Remote
149

Health and
PreventionSRO: Julie
Billet
Overall workstream objective
Driving a system-wide approach to prevention and population health, working to enable success in the overall STP strategy for care
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• Submitted bid to Health Education England (HEE) for ‘Make Every Contact Count’
train the trainer pilot• Submitted bid to HEE for Mental Health employment support • Agreed funding for Public Health Consultant to work with providers to implement
prevention framework and improve clinical engagement with workstreams
• Coordinate approach with partners on ‘Multi-Professional Advanced Clinical Practice’ task and finish group • Work with UCLH Cancer Collaborative on opportunities for greater uptake of smoking cessation linked to
the new North Central and East London lung screening trial• Continue to embed the new integrated sexual health service
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Workforce for prevention E, P Workforce, Estates, Digital Acute, MH Trusts, Community Partners involved:• GP practices Potential future commitments:• Working towards healthier workplaces • Alignment of organisational strategies • Commitment to prevention (primary and secondary)
Healthier environment O Workforce Acute, MH Trusts, Community
Healthier choices C, Q Workforce All partners
Mental
HealthSRO: Paul
Jenkins
Overall workstream objective
• Working to address inequalities for those with Serious Mental Illness and provide consistent care. • Deliver services closer to home, reducing demand on the acute sector and mitigating the need for additional MH inpatient beds.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• NCL STP met the CYP access standard for 2017/18• MoU signed for Children and Young People’s Out of hours service• MH Liaison commissioning and delivery model proposal completed. • Submission of Dementia funding proposals to NHSE.• MH Workforce Delivery Plan received positive score from regulators.
• Plan agreed to scale up & implement new MHLS model in NCL A&Es (UCLH & NMUH already complete)• Agree NCL approach to Primary Care Mental Health to inform commissioning for 19/20 • Delivery of Mental Health workforce projects• Secure funding for post suicide intervention service (NCL wide) • Launch trailblazers for Children and Young People
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Improve acute care E HCCH, Social Care, UEC Acute, MH Trusts, Community Partners involved:• CCGs, Acute, GPs/CHINs, MH Trusts, HEEPotential future commitments:• Development of frontline mental health services across settings • Agree single approach to Psych Liaison services in Acute services• Expand workforce to ensure capacity to meet national targets for
improved access.
Improve CAMHS Q CYP Schools, GPs, Community, MH Trusts
MH Liaison services Q, P, £ UEC Acute, MH Trusts, Community
Primary Care MH inc. IAPT Q, P, £ HCCH, Digital, Estates (2) GPs, Community
MH Workforce Q, P, £ Workforce (3), Digital Acute, MH Trusts, Community, GPs
Maternity
SRO: Rachel Lissauer
Overall workstream objective
Delivery of the National Maternity Transformation programme through improved continuity and safety of perinatal care for women, working across professional and organisational boundaries todrive better patient experience and integrated care.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• NEL CSU Digital team commissioned to build a Single Point of Access website. • 2nd Community Services hub successfully launched
• Quality and Safety - Implementation of Serious Incident triggers• Single Point of Access: - Test phase of the website with a public launch planned for early March 2019.• Community Services Development - Develop plan for new model of delivery• NCL Collaborative working: Development of Pocket Book app
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Quality & Safety Q Digital Acute, community Partners involved:• Acute trusts
Potential future commitments:• Portability of staff across services • Single point of booking across NCL
Personalisation & choice Q Digital Acute, community
Single point of access £,Q Digital , Workforce Acute, community
Community services dvt Q HCCH Community settings
NCL collaborative working £, Q Workforce Acute, community
* £ = Savings, Q = Quality, P=Performance, E=Efficiency, C=Clinical Outcomes150

Cancer
SRO: Dr Claire
Stephens
Overall workstream objective
Delivery of improved survival, patient experience, efficiency of service delivery - including services closer to home; reduced costs £ financial sustainability; reduced variation.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• NCEL STPs and alliance submitted an improvement plan to NHSE and I. • Alliance & STP bids submitted to NHSE for share of 1.3m London funding • Lung study installation of CT scanners at UCH and Finchley complete. • Digital Image sharing project being reviewed in light of London level changes to
interoperability plans;
• Sustained achievement of 62 Day standards for patients living in NCL . Take action as required.• Quantitative Faecal Immunochemical Test (qFIT) implemented across the sector; • Lung screening study launched• Providing access to rehabilitation across cancer pathways
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Cancer waits Q, P Diagnostics capacity Acute, Primary Care , community Partners involved:• Acute providers, GPs
Early diagnosis Q, P HCCH, Prevention Acute, Primary Care , community
Living w & beyond cancer Q HCCH, Planned Acute, Primary Care , community
Digital
SRO: David Sloman
Notable progress made this reporting period (Q3 2018) Notable progress planned for next reporting period (Q4 2018)
• Revised Health Information Exchange & HealtheIntent delivery plans established• Completed ‘Health System Led Investment’ (HSLI) funding proposal process
• First Tranche of HIE connections • HealtheIntent Phase 1 initiated
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Health Information Exch Q, £ Clinical Workstreams All Partners involved: Acute Trusts, Primary Care, Commissioners, Pharmacy, Public Health, Local Authority
Pop Health Management Q, £ Clinical Workstreams All
Children
and YoungPeople
SRO:
Charlotte Pomery
Overall workstream objective
‘Right care, right place, right time’. Transformed health & social care services: equitable, accessible, efficient & delivers improved outcomes. Enabling high quality, responsive services for children, young people & families, delivered locally where possible, with a shared focus on promoting wellbeing, reducing health inequa lities & improving health & social outcomes.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• Continued engagement with system partners on detailed asthma plan• Delayed Transfers of Care (DTOC) brief complete and stakeholder workshop
scheduled for January 2019;• Agreed priorities and scope within complex needs work
• Refinement and agreement of System-Wide NCL Asthma plan, Inc. launch planning Q1 19/20• Children’s surgery: outline proposals, early engagement/consultation• Broader review of prevention opportunities for children and young people and their families• Develop project plan/initiation concerning children with complex needs
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Paediatric surgery Q Workforce, digital Acute trusts (GDH & Tertiary) Partners involved: Acute Trusts, Primary Care, Commissioners, Pharmacy, Public Health, Local AuthorityPotential future commitments:• System approach to managing & preventing asthma in C&YP• Developing a surgical network across NCL• Preventative approach to care & support for CYP & families
Asthma Q Prev, HCCH, workforce, digital Acute, Primary Care , community
Complex Needs £, Q UEC, HCCH, Mental Health Acute Trusts, LA Placements
Paed. admissions avoid. £, P, Q UEC, Prev, HCCH, workforce, digital Acute, Primary Care , community
Social Care
SRO: Dawn Wakeling
Overall workstream objective
Working to address care inequalities in provision and improving longer term strategic approach to workforce and care market.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• Workforce: Implementing Health Education England (HEE) funded schemes. • Workforce: Care home quality dataset shared with stakeholders for input• Markets: Received draft of care analytics work around sustainable price setting;• Markets: LPH care tiers for nursing care defined and putting in place performance
tracking with teams. • Markets: Principles for implementing a coordinated pricing structure; block
contracts and performance management developed.
• Independent care sector workforce: Pilot of Proud To Care launched. • Workforce: Improved career pathways developed.
• Social care markets: Agreed sites for developing capacity in sector and pricing strategy
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Ind. Care Sector Workforce £, E, Q HCCH, UEC, Workforce Home Care, Care Homes Partners involved: Local authorities, CCGs, care providersPotential future commitments: Joint commissioning strategy
Social Care Markets Q, £, E HCCH, UEC, MH, Workforce Home Care, Care Homes
* £ = Savings, Q = Quality, P=Performance, E=Efficiency, C=Clinical Outcomes151

Workforce
SRO:Siobhan
Harrington
Overall workstream objective
To attract people to live and work in NCL so we have the best possible workforce to deliver high quality services to our community
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)• Secured HEE funding for STP workforce priorities (£500k)• Portability: Confirmed all Trusts will work towards shared solution in 2019/20• Collaborative bank: seminar for all NLP partners to consider options
• Collaborative bank: All Trusts to consider and share their intention to join. Social and primary care and CYP workshop on developing bank option.
• Temp staff: work to start scoping outliers and inconsistencies in bank rates• Analytics and enablers: deliver on confirmed workforce observatory approach for orthopaedic review
Priority project Impact* Major Independencies Key Care Settings Partner involvement
UEC prep. winter 2019 P, Q UEC Acute, Community, Primary care Partners involved:• All Potential future commitments:• Standardisation of mandatory training to aid portability • Standardisation of employment contracts to aid portability
Portability (including passports, MAST)
P, Q, £ Prevention, HCCH Acute, Community, Primary care
Temporary Staffing £, Q, C - Acute and Community trusts
Social & Primary C/Community/Place based
£, P, Q UEC Community, Primary care
Analytics (WF planning) £ All
Estates
SRO: Simon Goodwin
Overall workstream objective
To provide a fit for purpose, cost-effective, integrated, accessible estate which enables the delivery of high quality health and social care services for our local population.
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)
• STP completed prioritisation of 2019/20 improvement grants. • Submitted STP investment pipeline (NCL Delivery Plan) to London Estates Board for
inclusion in London Capital Pipe-line. • Submitted Category 3 Estates and Technology Transformation Fund (ETTF) existing
schemes & support for 18/19 Cohort 1 ETTF schemes.
• Refresh estates strategy as clinical strategies completed• St Pancras Hospital - Initiate Final Business Case• Project Oriel - Launch public consultation and work on preparing Outline Business Case• St Ann’s - Commencement of main inpatient building construction • Void spaces: Submit Property Vacating Notices on voids in NHS PS properties under 100m2
Priority project Impact* Major Independencies Key Care Settings Partner involvement
NCL estates strategy £, Q All All STP partners Partners involved:• CCGs and TrustsPotential future commitments:• Partnership working on NCL estates strategy iteration
St Pancras devt. – C&I £, Q Mental Health C&I hospital site
St Ann’s devt.– BEH £, Q All BEH hospital site
Project Oriel Q - Moorfields, C&I hospital sites
Reducing void spaces £, Q All All STP partners
Provider Productivity
SRO: Tim
Jaggard
Overall workstream objective
To scope and take forward areas of savings requiring collaboration across providers
Notable progress made this reporting period (Q3 2018/19) Notable progress planned for next reporting period (Q4 2018/19)
• Imaging diagnostics workstream has completed a provider and commissioner data collection exercise across NCL providers & are considering future opportunities to repatriate activity.
• Workforce finance model for Mandatory and Statutory Training (MaST) completed
• Patient Transport, decontamination and automation updates planned for Dec-18. • Procurement brief update planned for Dec-18 CEOs meeting.• Medicine Optimisation team to brief Clinical cabinet on latest changes proposed by NHSE in respect of
biosimilar treatment potential risk
Priority project Impact* Major Independencies Key Care Settings Partner involvement
Workforce £ Workforce NHS Trusts Partners involved:• ProvidersPotential future commitments:• Consideration of collaborative bank option • Ongoing engagement in modelling, scoping and emerging
programme of work
Procurement £ - NHS Trusts
Facilities management £ - NHS Trusts
Diagnostics £, Q Planned Care NHS Trusts 152

Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Agenda Items
1. Standing Items
Apologies √ √ √ √ √ √
Declarations of Interests √ √ √ √ √ √
Register of Gifts and Hospitality √ √ √ √ √ √
Minutes of Last Meeting √ √ √ √ √ √
Action Log √ √ √ √ √ √
Forward Planner √ √ √ √ √ √
AOB √ √ √ √ √ √
2. Governance
Remit of the Committee
Terms of Reference- Annual Review
Appointment to Chair of the Committee
3. Activity and Performance
Acute Contract Report √ √ √ √ √ √
Acute Performance and Quality Report √ √ √ √ √ √
Integrated Urgent Care Report - within
acute reports √ √ √ √ √ √
Learning Disabilities- Transforming Care
Cohort √ √ √
In-Health Contract Update √
4. Commissioning
System Intentions 2019-20 √ √
Planning for 2018/19 √ √
Planning for 2019/20 √
5. Risk
NCL Joint Commissioning Committee Risk
Register √ √ √ √ √ √
6. Other Items
Procedures of limited clinical effectiveness √ √
Interdependent services including mental
health √
Specialist services not commissioned by
Specialist Commissioning - Cancer (June
18) / Maternity (Aug 18) √ √
7. Business Cases - dates to be
confirmed
Adult Elective Orthopaedics √ √ √
QFIT Business Case √
Moorfields Eye Hospital Clinical Case for
Change √ √
NCL Joint Commissioning Committee Forward Planner 2018/19
S
e
m
i
n
a
r
S
e
m
i
n
a
r
S
e
m
i
n
a
r
S
e
m
i
n
a
r
153
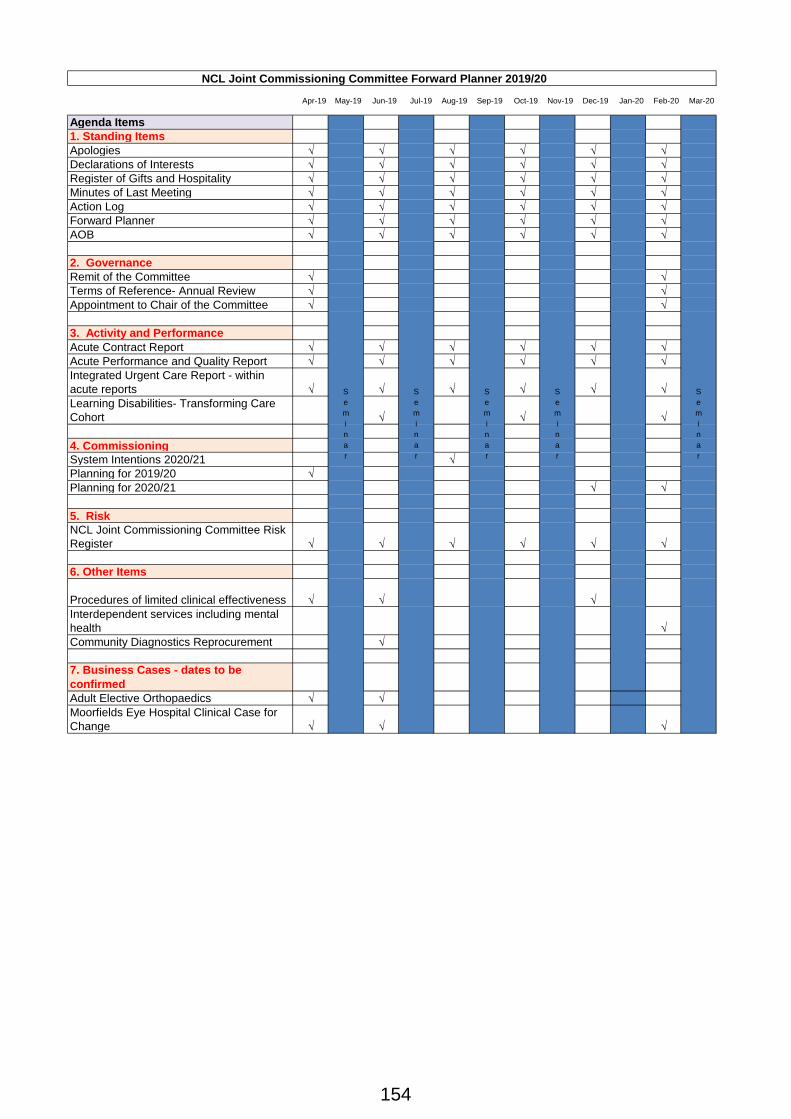
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Agenda Items
1. Standing Items
Apologies √ √ √ √ √ √
Declarations of Interests √ √ √ √ √ √
Register of Gifts and Hospitality √ √ √ √ √ √
Minutes of Last Meeting √ √ √ √ √ √
Action Log √ √ √ √ √ √
Forward Planner √ √ √ √ √ √
AOB √ √ √ √ √ √
2. Governance
Remit of the Committee √ √
Terms of Reference- Annual Review √ √
Appointment to Chair of the Committee √ √
3. Activity and Performance
Acute Contract Report √ √ √ √ √ √
Acute Performance and Quality Report √ √ √ √ √ √
Integrated Urgent Care Report - within
acute reports √ √ √ √ √ √
Learning Disabilities- Transforming Care
Cohort √ √ √
4. Commissioning
System Intentions 2020/21 √
Planning for 2019/20 √
Planning for 2020/21 √ √
5. Risk
NCL Joint Commissioning Committee Risk
Register √ √ √ √ √ √
6. Other Items
Procedures of limited clinical effectiveness √ √ √
Interdependent services including mental
health √
Community Diagnostics Reprocurement √
7. Business Cases - dates to be
confirmed
Adult Elective Orthopaedics √ √
Moorfields Eye Hospital Clinical Case for
Change √ √ √
S
e
m
i
n
a
r
NCL Joint Commissioning Committee Forward Planner 2019/20
S
e
m
i
n
a
r
S
e
m
i
n
a
r
S
e
m
i
n
a
r
S
e
m
i
n
a
r
154