nebraska perinatal quality improvement …nebraska perinatal quality improvement collaborative...
TRANSCRIPT

NEBRASKA PERINATAL QUALITY IMPROVEMENT
COLLABORATIVE WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED
HYPERTENSIVE DISORDERS
Target Audience
Physicians advanced practice providers and nurses specializing in family medicine obstetrics and pediatrics
Educational Objectives
bull Discuss various classifications of hypertensive disorders in pregnancy
bull Describe how to diagnose and manage women with hypertensive disorders of pregnancy
bull Identify preventive therapies for pregnancy-induced hypertension
REQUIREMENTS FOR SUCCESSFUL
COMPLETION
In order to receive continuing education credits or contact hours you must
bull Sign into ZOOM and attend the entire webinar
bull Complete the online evaluation by signing in to MY Account at wwwunmceducce
Go to Evaluate a coursePrint Certificate
Use CME Activity Code 36519
Save and print your certificate Retain certificate for future documentation Certificates are
available up to 60 days post activity upon completion of the evaluation
CREDITThe University of Nebraska Medical Center Center for Continuing Education is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians
The University of Nebraska Medical Center Center for Continuing Education designates this live activity for a maximum of 1 AMA PRA Category 1 Credittrade Physicians should claim only the credit commensurate with the extent of their participation in the activity
The University of Nebraska Medical Center College of Nursing Continuing Nursing Education is accredited with distinction as a provider of continuing nursing education by the American Nurses Credentialing Centerrsquos Commission on Accreditation This activity is provided for 10contact hour under ANCC criteria
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the American Nurses Credentialing Centerrsquos Commission on Accreditation (ANCC) through the joint providership of the University of Nebraska Medical Center College of Nursing Continuing Nursing Education (UNMC CON CNE) (provider) University of Nebraska Medical Center Center for Continuing Education (UNMC CCE) and Nebraska Perinatal Quality Improvement Collaborative (NPQIC)
DISCLOSURE DECLARATIONAs a provider accredited by ACCME the University of Nebraska Medical Center Center for Continuing Education the
University of Nebraska Medical Center College of Nursing Continuing Nursing Education and the American Nurses
Credentialing Centerrsquos Commission on Accreditation must ensure balance objectivity independence and scientific
rigor in its educational activities Faculty are encouraged to provide a balanced view of therapeutic options by utilizing
either generic names or the trade names of several to ensure impartiality
All speakers planning committee members and others in a position to control continuing medical education content
participating in a University of Nebraska Medical Center Center for Continuing Education University of Nebraska
Medical Center College of Nursing Continuing Nursing Education and American Nurses Credentialing Centerrsquos
Commission on Accreditation activity are required to disclose relationships with commercial interests A commercial
interest is any entity producing marketing re-selling or distributing health care goods or services consumed by or
used on patients Disclosure of these commitments andor relationships is included in these course materials so that
participants in the activity may formulate their own judgments in interpreting its content and evaluating its
recommendations
This activity may include presentations in which faculty may discuss off -label andor investigational use of
pharmaceuticals or instruments not yet FDA-approved Participants should note that the use of products outside
currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing
information for FDA-approved indications
All materials are included with the permission of the authors The opinions expressed are those of the authors and
are not to be construed as those of the University of Nebraska Medical Center Center for Continuing Education
University of Nebraska Medical Center College of Nursing Continuing Nursing Education or American Nurses
Credentialing Centerrsquos Commission on Accreditation
FACULTY AND PLANNING COMMITTEE
DISCLOSURES
All faculty and planning committee members have no financial relationships to disclose
Ann Anderson-Berry MD PhD FAAP
Robert Bonebrake MD FACOG
Peggy Brown DNP RN CPHQ (Course Director)
Heidi Keeler PhD RN
Renee Paulin MSN RN CWOCN
Hemant Satpathy MD
Sara Weber MSW CHES CBE
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
REQUIREMENTS FOR SUCCESSFUL
COMPLETION
In order to receive continuing education credits or contact hours you must
bull Sign into ZOOM and attend the entire webinar
bull Complete the online evaluation by signing in to MY Account at wwwunmceducce
Go to Evaluate a coursePrint Certificate
Use CME Activity Code 36519
Save and print your certificate Retain certificate for future documentation Certificates are
available up to 60 days post activity upon completion of the evaluation
CREDITThe University of Nebraska Medical Center Center for Continuing Education is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians
The University of Nebraska Medical Center Center for Continuing Education designates this live activity for a maximum of 1 AMA PRA Category 1 Credittrade Physicians should claim only the credit commensurate with the extent of their participation in the activity
The University of Nebraska Medical Center College of Nursing Continuing Nursing Education is accredited with distinction as a provider of continuing nursing education by the American Nurses Credentialing Centerrsquos Commission on Accreditation This activity is provided for 10contact hour under ANCC criteria
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the American Nurses Credentialing Centerrsquos Commission on Accreditation (ANCC) through the joint providership of the University of Nebraska Medical Center College of Nursing Continuing Nursing Education (UNMC CON CNE) (provider) University of Nebraska Medical Center Center for Continuing Education (UNMC CCE) and Nebraska Perinatal Quality Improvement Collaborative (NPQIC)
DISCLOSURE DECLARATIONAs a provider accredited by ACCME the University of Nebraska Medical Center Center for Continuing Education the
University of Nebraska Medical Center College of Nursing Continuing Nursing Education and the American Nurses
Credentialing Centerrsquos Commission on Accreditation must ensure balance objectivity independence and scientific
rigor in its educational activities Faculty are encouraged to provide a balanced view of therapeutic options by utilizing
either generic names or the trade names of several to ensure impartiality
All speakers planning committee members and others in a position to control continuing medical education content
participating in a University of Nebraska Medical Center Center for Continuing Education University of Nebraska
Medical Center College of Nursing Continuing Nursing Education and American Nurses Credentialing Centerrsquos
Commission on Accreditation activity are required to disclose relationships with commercial interests A commercial
interest is any entity producing marketing re-selling or distributing health care goods or services consumed by or
used on patients Disclosure of these commitments andor relationships is included in these course materials so that
participants in the activity may formulate their own judgments in interpreting its content and evaluating its
recommendations
This activity may include presentations in which faculty may discuss off -label andor investigational use of
pharmaceuticals or instruments not yet FDA-approved Participants should note that the use of products outside
currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing
information for FDA-approved indications
All materials are included with the permission of the authors The opinions expressed are those of the authors and
are not to be construed as those of the University of Nebraska Medical Center Center for Continuing Education
University of Nebraska Medical Center College of Nursing Continuing Nursing Education or American Nurses
Credentialing Centerrsquos Commission on Accreditation
FACULTY AND PLANNING COMMITTEE
DISCLOSURES
All faculty and planning committee members have no financial relationships to disclose
Ann Anderson-Berry MD PhD FAAP
Robert Bonebrake MD FACOG
Peggy Brown DNP RN CPHQ (Course Director)
Heidi Keeler PhD RN
Renee Paulin MSN RN CWOCN
Hemant Satpathy MD
Sara Weber MSW CHES CBE
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

CREDITThe University of Nebraska Medical Center Center for Continuing Education is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians
The University of Nebraska Medical Center Center for Continuing Education designates this live activity for a maximum of 1 AMA PRA Category 1 Credittrade Physicians should claim only the credit commensurate with the extent of their participation in the activity
The University of Nebraska Medical Center College of Nursing Continuing Nursing Education is accredited with distinction as a provider of continuing nursing education by the American Nurses Credentialing Centerrsquos Commission on Accreditation This activity is provided for 10contact hour under ANCC criteria
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the American Nurses Credentialing Centerrsquos Commission on Accreditation (ANCC) through the joint providership of the University of Nebraska Medical Center College of Nursing Continuing Nursing Education (UNMC CON CNE) (provider) University of Nebraska Medical Center Center for Continuing Education (UNMC CCE) and Nebraska Perinatal Quality Improvement Collaborative (NPQIC)
DISCLOSURE DECLARATIONAs a provider accredited by ACCME the University of Nebraska Medical Center Center for Continuing Education the
University of Nebraska Medical Center College of Nursing Continuing Nursing Education and the American Nurses
Credentialing Centerrsquos Commission on Accreditation must ensure balance objectivity independence and scientific
rigor in its educational activities Faculty are encouraged to provide a balanced view of therapeutic options by utilizing
either generic names or the trade names of several to ensure impartiality
All speakers planning committee members and others in a position to control continuing medical education content
participating in a University of Nebraska Medical Center Center for Continuing Education University of Nebraska
Medical Center College of Nursing Continuing Nursing Education and American Nurses Credentialing Centerrsquos
Commission on Accreditation activity are required to disclose relationships with commercial interests A commercial
interest is any entity producing marketing re-selling or distributing health care goods or services consumed by or
used on patients Disclosure of these commitments andor relationships is included in these course materials so that
participants in the activity may formulate their own judgments in interpreting its content and evaluating its
recommendations
This activity may include presentations in which faculty may discuss off -label andor investigational use of
pharmaceuticals or instruments not yet FDA-approved Participants should note that the use of products outside
currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing
information for FDA-approved indications
All materials are included with the permission of the authors The opinions expressed are those of the authors and
are not to be construed as those of the University of Nebraska Medical Center Center for Continuing Education
University of Nebraska Medical Center College of Nursing Continuing Nursing Education or American Nurses
Credentialing Centerrsquos Commission on Accreditation
FACULTY AND PLANNING COMMITTEE
DISCLOSURES
All faculty and planning committee members have no financial relationships to disclose
Ann Anderson-Berry MD PhD FAAP
Robert Bonebrake MD FACOG
Peggy Brown DNP RN CPHQ (Course Director)
Heidi Keeler PhD RN
Renee Paulin MSN RN CWOCN
Hemant Satpathy MD
Sara Weber MSW CHES CBE
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

DISCLOSURE DECLARATIONAs a provider accredited by ACCME the University of Nebraska Medical Center Center for Continuing Education the
University of Nebraska Medical Center College of Nursing Continuing Nursing Education and the American Nurses
Credentialing Centerrsquos Commission on Accreditation must ensure balance objectivity independence and scientific
rigor in its educational activities Faculty are encouraged to provide a balanced view of therapeutic options by utilizing
either generic names or the trade names of several to ensure impartiality
All speakers planning committee members and others in a position to control continuing medical education content
participating in a University of Nebraska Medical Center Center for Continuing Education University of Nebraska
Medical Center College of Nursing Continuing Nursing Education and American Nurses Credentialing Centerrsquos
Commission on Accreditation activity are required to disclose relationships with commercial interests A commercial
interest is any entity producing marketing re-selling or distributing health care goods or services consumed by or
used on patients Disclosure of these commitments andor relationships is included in these course materials so that
participants in the activity may formulate their own judgments in interpreting its content and evaluating its
recommendations
This activity may include presentations in which faculty may discuss off -label andor investigational use of
pharmaceuticals or instruments not yet FDA-approved Participants should note that the use of products outside
currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing
information for FDA-approved indications
All materials are included with the permission of the authors The opinions expressed are those of the authors and
are not to be construed as those of the University of Nebraska Medical Center Center for Continuing Education
University of Nebraska Medical Center College of Nursing Continuing Nursing Education or American Nurses
Credentialing Centerrsquos Commission on Accreditation
FACULTY AND PLANNING COMMITTEE
DISCLOSURES
All faculty and planning committee members have no financial relationships to disclose
Ann Anderson-Berry MD PhD FAAP
Robert Bonebrake MD FACOG
Peggy Brown DNP RN CPHQ (Course Director)
Heidi Keeler PhD RN
Renee Paulin MSN RN CWOCN
Hemant Satpathy MD
Sara Weber MSW CHES CBE
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
FACULTY AND PLANNING COMMITTEE
DISCLOSURES
All faculty and planning committee members have no financial relationships to disclose
Ann Anderson-Berry MD PhD FAAP
Robert Bonebrake MD FACOG
Peggy Brown DNP RN CPHQ (Course Director)
Heidi Keeler PhD RN
Renee Paulin MSN RN CWOCN
Hemant Satpathy MD
Sara Weber MSW CHES CBE
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
6
Dr Hemant K Satpathy
Perinatologist
Methodist Womenrsquos Hospital
NEBRASKA PERINATAL QUALITY IMPROVEMENT COLLABORATIVE
WEBINAR SERIES
MANAGEMENT OF PREGNANCY RELATED HYPERTENSIVE
DISORDERS
7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

7Maternal Mortality Rate
8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

8
9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

9
CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

CLASSIFICATION OF HYPERTENSIVE DISORDERS OF
PREGNANCY
10
1 Gestational HTN
2 Preeclampsia and eclampsia
-without severe features
-with severe features
3 Chronic HTN
-without superimposed preeclampsia
-with superimposed preeclampsia
11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

11
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
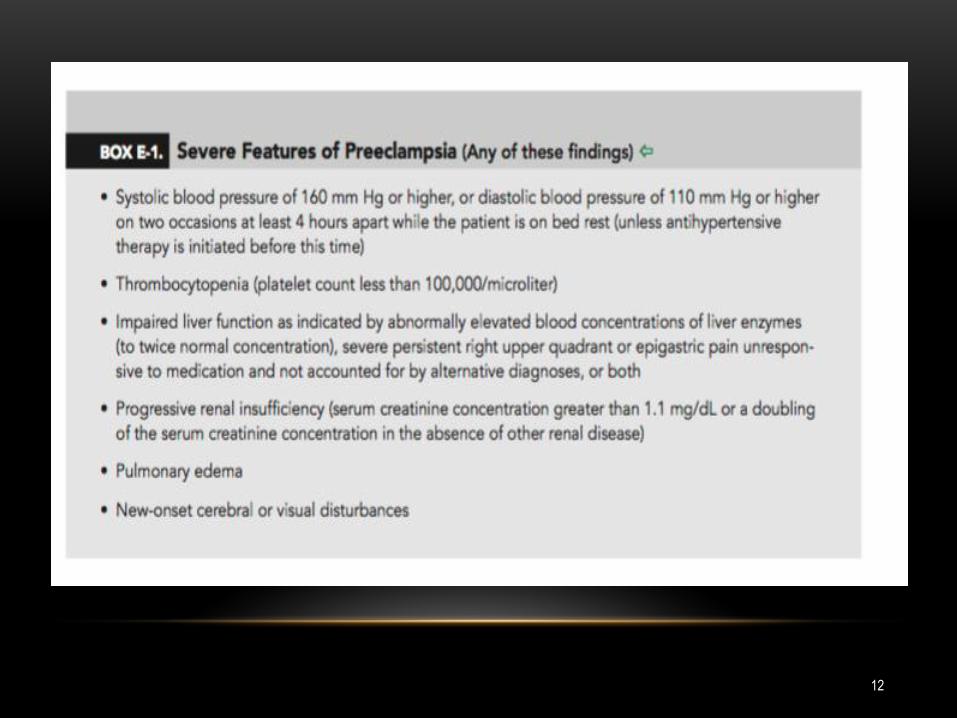
12
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
PROTEINURIA
bull Task force eliminated dependence on proteinuria for diagnosing
preeclampsia
bull Severe range proteinuria not a severe feature of preeclampsia
13
14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

14
15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

15
SCREENING FOR PREECLAMPSIA
16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

16
FETAL MEDICINE FOUNDATION
17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

17
FETAL MEDICINE FOUNDATION
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
PREVENTION OF PREECLAMPSIA
18
bull ASA
bull Calcium
bull Pravastatin
19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

19
PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

PREVENTION OF PREECLAMPSIA
bull Low dose ASA in high risk patients to be initiated between 12-16 weeks
bull Indications (ACOG)
preeclampsia and PTD lt 34 07 weeks
preeclampsia gt1 prior pregnancy
20
PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

PREVENTION OF PREECLAMPSIA
bull USPTF indications for ASA
bull CHTN
bull CKD
bull SLE
bull AMA gt40
bull IVF pregnancy
bull Obesity
bull Pregestational DM
bull Multifetal pregnancy
bull Family history of preeclampsia
bull Primigravida
bull Thrombophilia
21
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
22
Aspirin prevents preeclampsia
In the ASPRE study women were screened for preeclampsia (PE) at 11 to 13 weeks by the
FMF algorithm In the high risk group (risk of gt1 in 100) use of aspirin (150mgday) from 12
until 36 weeks of gestation reduced the incidence of PE before 34 weeks by gt80 and PE
before 37 weeks by gt60
NEJM 2017 377613-622
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
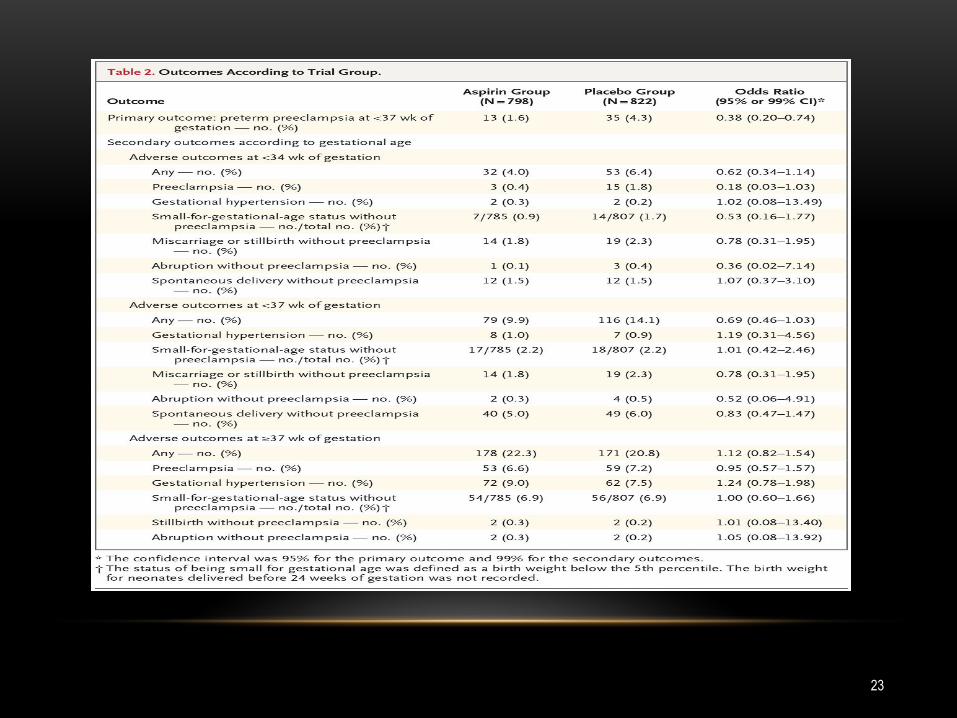
23
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
- Outpatient management
- 2week BP check
- Weekly PIH labs
- Weekly antepartum testing
- Serial fetal growth scan
- Strict bred rest not recommended
- Antihypertensive not indicated in absence of severe range BP or end organ damage
- Magnesium not indicated for seizure prophylaxis
- Delivery recommended at 37 07 weeks
24
Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

Lancet 2009 Sep 19374(9694)979-88 doi 101016S0140-6736(09)60736-4 Epub
2009 Aug 3
Induction of labour versus expectant monitoring for gestational hypertension or
mild pre-eclampsia after 36 weeks gestation (HYPITAT) a multicentre open-label
randomised controlled trial
Koopmans CM1 Bijlenga D Groen H Vijgen SM Aarnoudse JG Bekedam DJ van den
Berg PP de Boer K Burggraaff JM Bloemenkamp KW Drogtrop AP Franx A de Groot
CJ Huisjes AJ Kwee A van Loon AJ Lub A Papatsonis DN van der Post JA Roumen
FJ Scheepers HC Willekes C Mol BW van Pampus MG HYPITAT study group
FINDINGS
756 patients were allocated to receive induction of labour (n=377 patients) or expectant
monitoring (n=379) 397 patients refused randomisation but authorised use of their
medical records Of women who were randomised 117 (31) allocated to induction of
labour developed poor maternal outcome compared with 166 (44) allocated to
expectant monitoring (relative risk 071 95 CI 059-086 plt00001) No cases of
maternal or neonatal death or eclampsia were recorded
INTERPRETATION
Induction of labour is associated with improved maternal outcome
and should be advised for women with mild hypertensive disease
beyond 37 weeks gestation25
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
MANAGEMENT OF PREECLAMPSIA WITHOUT SEVERE FEATURES MILD
GHTN AND CHTN WITH SUPERIMPOSED PREECLAMPSIA WITHOUT
SEVERE FEATURES
bull Indications for delivery after 34 weeks
bull PPROM
bull Oligohydramnios
bull Severe IUGR
bull Persistent BPP lt610
26
ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

ECLAMPSIA
27
bull Eclampsia is defined as the presence of new onset seizure with
or without coma in a women with preeclampsia
ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

ECLAMPSIA
28
bull Incidence 2-310000
bull Antepartum 40-50
bull Intrapartum 10-35
bull Postpartum 10-40
bull 15 without HTN or proteinuria
29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

29
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
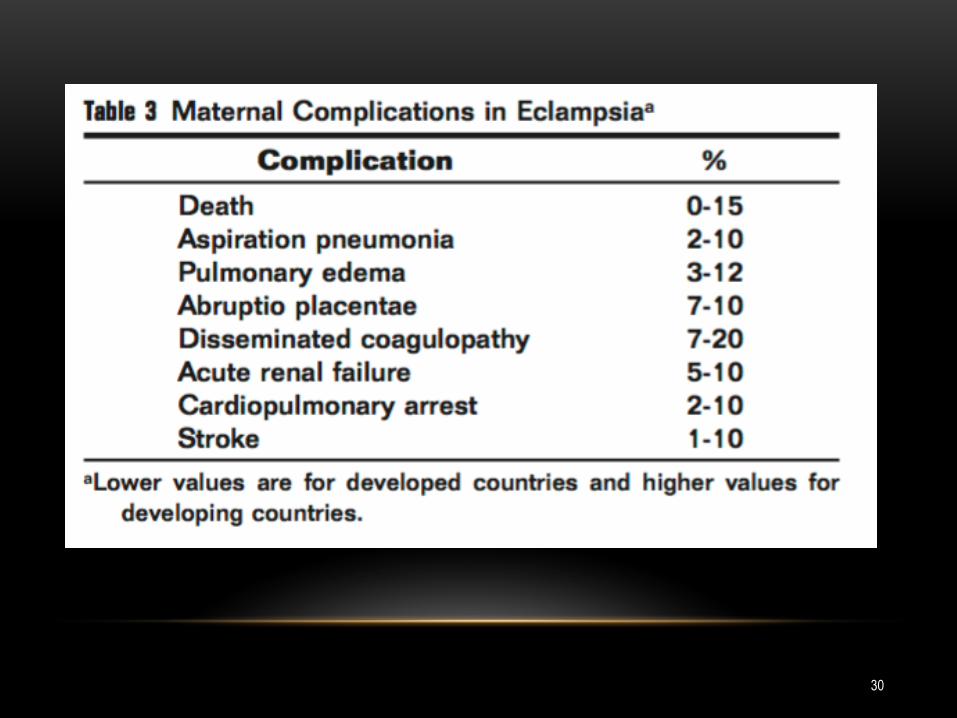
30
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
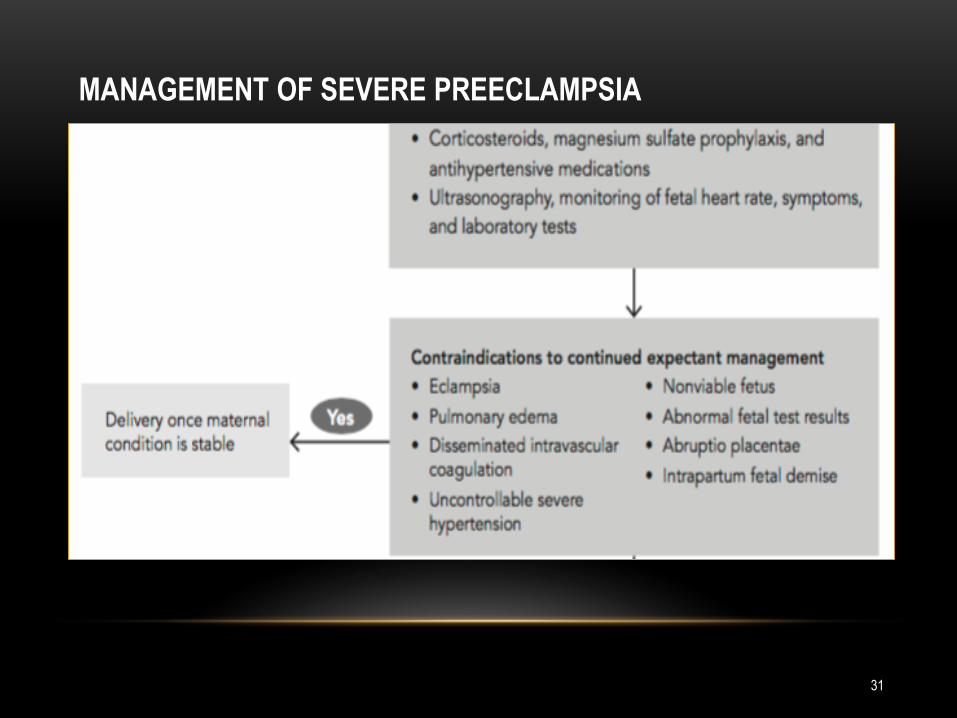
31
MANAGEMENT OF SEVERE PREECLAMPSIA
MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

MANAGEMENT OF SEIZURE
32
bull Airway breathing and circulation
bull Avoid injury
bull Pulse oximetry
bull Labs and imaging
bull Continuous fetal monitoring
bull Magnesium (4-6 gm loading dose 1-3 gmhr maintenance dose)
bull Expeditious delivery once the mother is stable
bull Antihypertensives
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
33
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
34
35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

35
MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

MAGPIE
MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

MAGPIE
38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

38
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

39
INDICATIONS FOR MGSO4 FOR SEIZURE PROPHYLAXIS
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
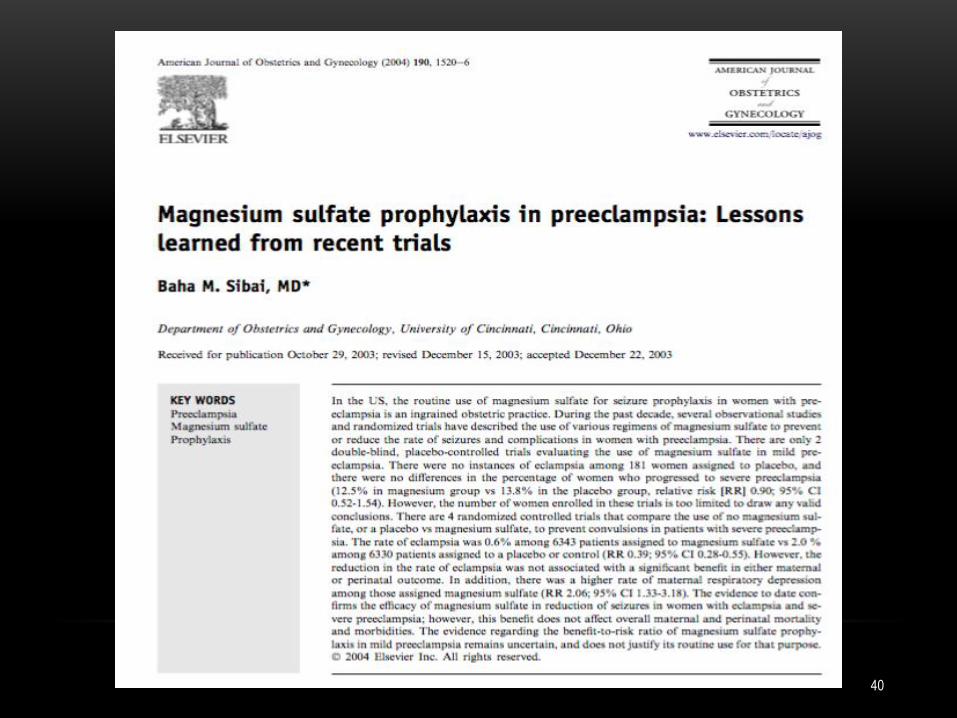
40
41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

41
42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

42
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
ECLAMPSIA MANAGEMENT
43
bull Indications for checking magnesium level
bull Renal disease
bull Signs and symptoms of magnesium toxicity
bull Recurrent seizure while on magnesium infusion
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
ECLAMPSIA MANAGEMENT
44
bull Contraindications for MgSO4
bull Myasthenia gravis
bull Impaired renal function (creatinine lt12 12-25 gt25 mgdl)
ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

ECLAMPSIA MANAGEMENT
bull Hypocalcemia
bull while receiving MgSO4 does not require treatment
CHOLST IN ET AL THE INFLUENCE OF HYPERMAGNESEMIA ON SERUM CALCIUM AND PARATHYROID HORMONE LEVELS IN HUMAN
SUBJECTS NEJM 19843101221
ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

ECLAMPSIA MANAGEMENT
46
bull Indications for head imaging
bull Onset gt48 hrs postpartum
bull Seizure refractory to magnesium
bull Focal neurological deficits
bull Coma
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
ECLAMPSIA MANAGEMENT
47
bull Recurring seizure
bull Head imaging
bull Check magnesium level
bull Treatment
bull 2 gm magnesium bolus IV
bull Others 5-10 mg IV diazepam 2-4 mg IV lorazepam 1-2
mg midazolam 500 mg IVPO levetiracetam IV
hydantoin 250 mg IV sodium amobarbital
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
48
49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

49
50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

50
51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

51
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
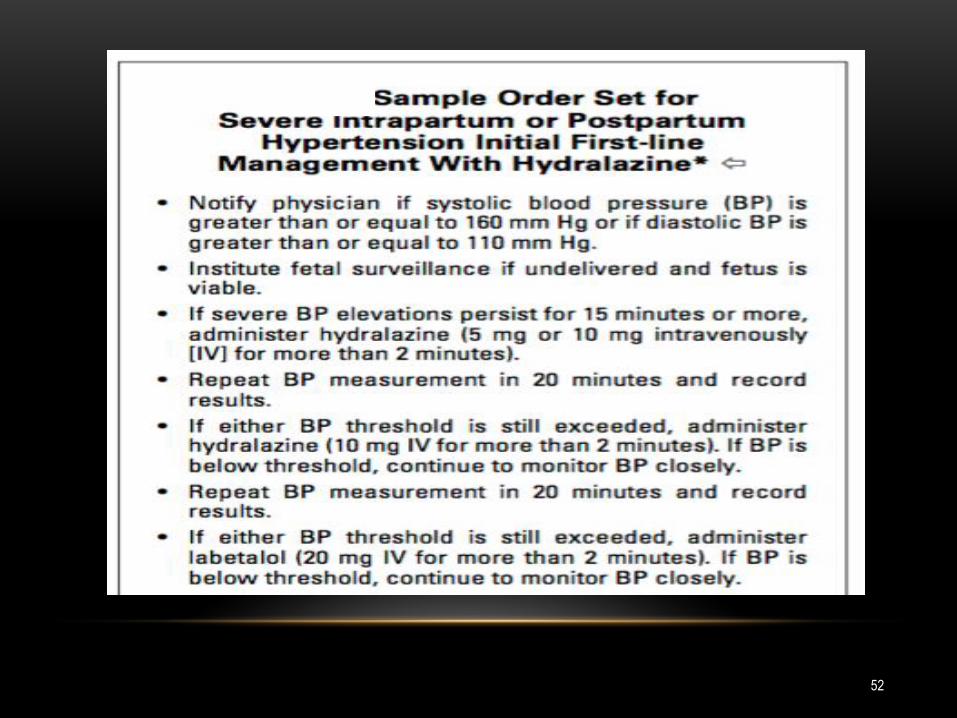
52
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
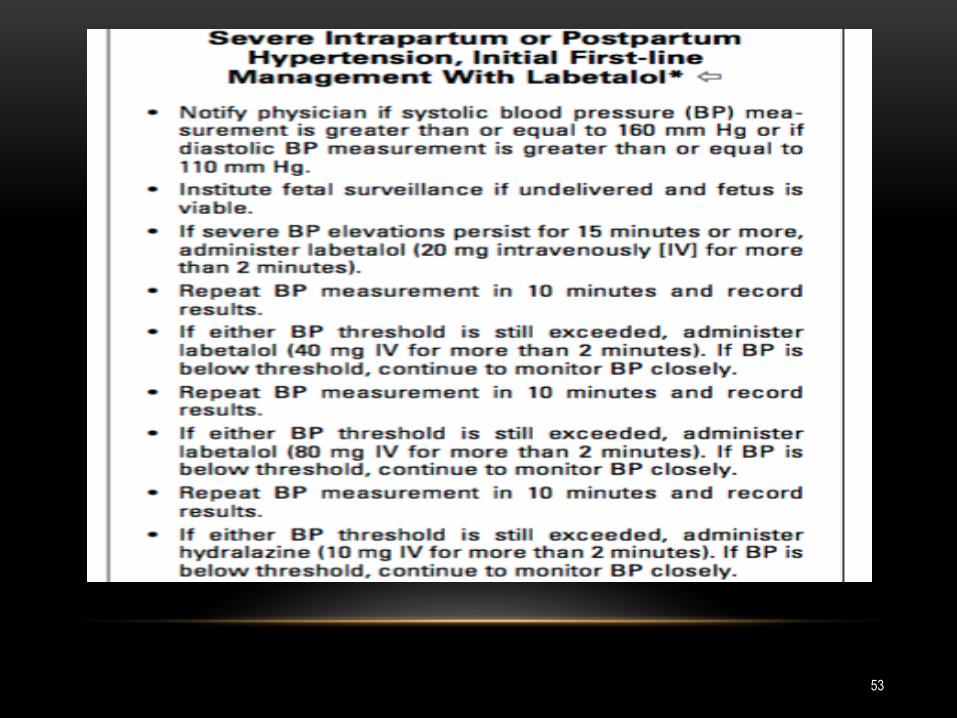
53
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
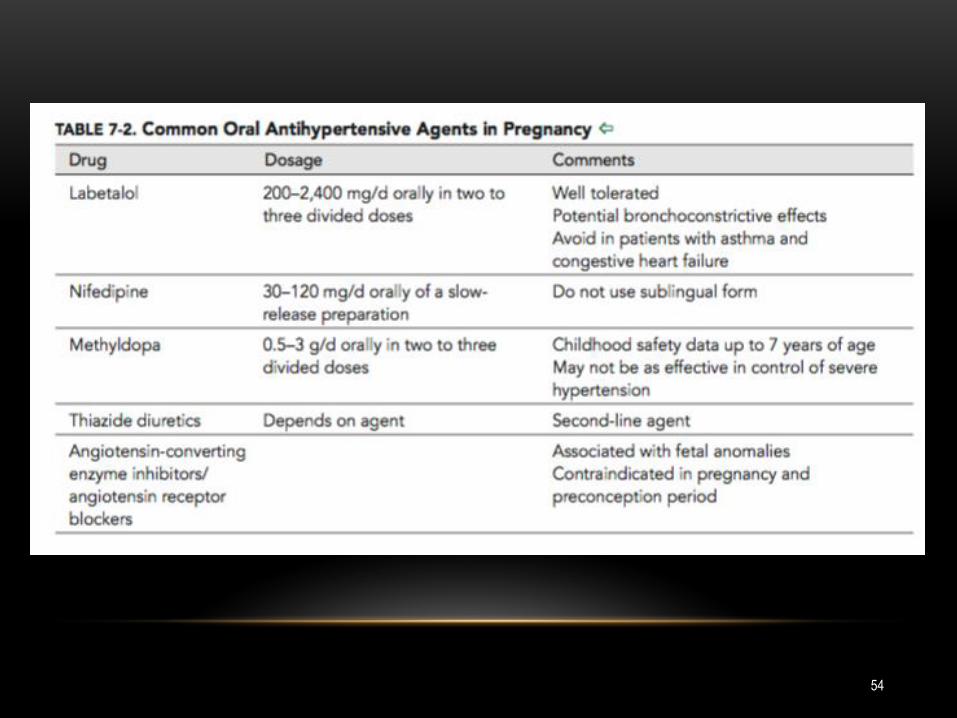
54
55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

55
56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

56
STEROID FOR FETAL LUNG MATURITY
57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

57
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
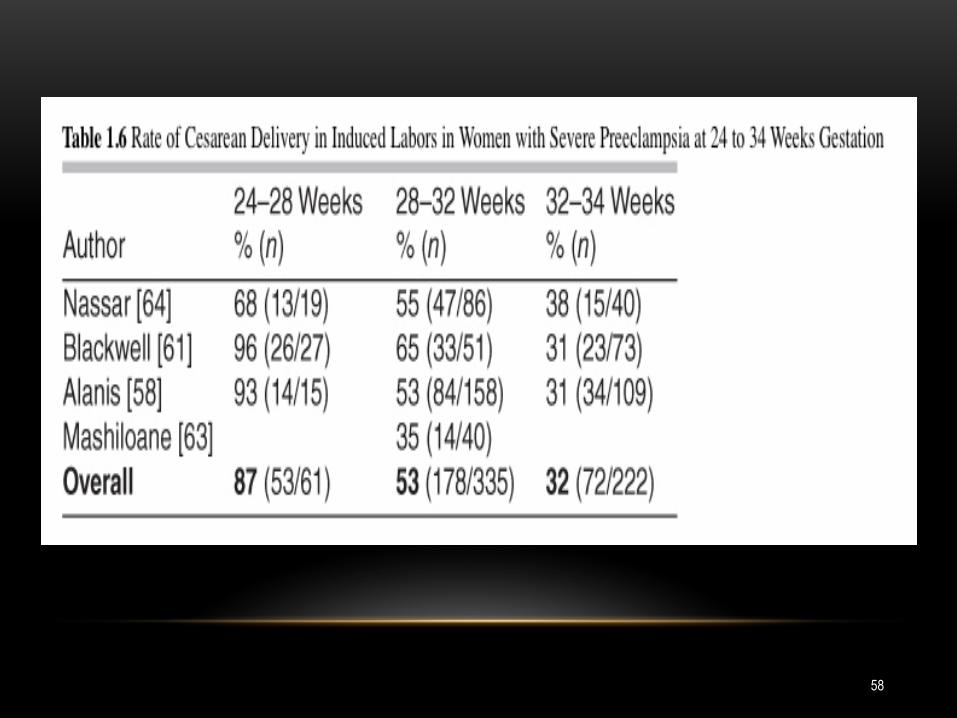
58
59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

59
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
ANESTHESIA CONSIDERATIONS
60
bull Preferred anesthesia -regional
bull Thrombocytopenia ndashno safe limit per ASA
bull Magnesium sulfate ndashcontinue during cesarean
ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

ANESTHESIA CONSIDERATIONS
bull The American Society of Anesthesiologists has not
recommended a safe limit for the platelet count in parturient
women with preeclampsia relying on the health care providerrsquos
judgment following review of the laboratory values
PRACTICE GUIDELINES FOR OBSTETRIC ANESTHESIA AN UPDATED RE- PORT BY THE AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC
ANESTHESIA AMERICAN SOCIETY OF ANESTHESIOLOGISTS TASK FORCE ON OBSTETRIC ANESTHESIA ANESTHESIOLOGY 2007106843ndash63
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS
62
Patients with preeclampsia with severe features undergoing
cesarean have lower threshold for seizure secondary to induction
of anesthesia and stress of labor In addition because of long half
life discontinuing magnesium in OR will not abate potential
interactions of magnesium with anesthetic agents and furthermore
the subtherapeutic level increases the risk of postpartum
eclampsia
TASK FORSE RECOMMENDATION
63THANKS
64
QUESTIONS

63THANKS
64
QUESTIONS

64
QUESTIONS