neoadjuvant melanoma trials data collection and endpoint
TRANSCRIPT
Neoadjuvant Melanoma Trials Data Collection and Endpoint Selection
Christian Blank, MD, PhD, Netherlands Cancer Institute
November 6th, 2019

• Advisory role: BMS, MSD, Roche, Novartis, GSK, AZ, Pfizer, Lilly,GenMab, Pierre Fabre
• Research funding: BMS, Novartis, NanoString
• Stockownership: Uniti Cars, Neon Therapeutics, Forty Seven
Disclosures
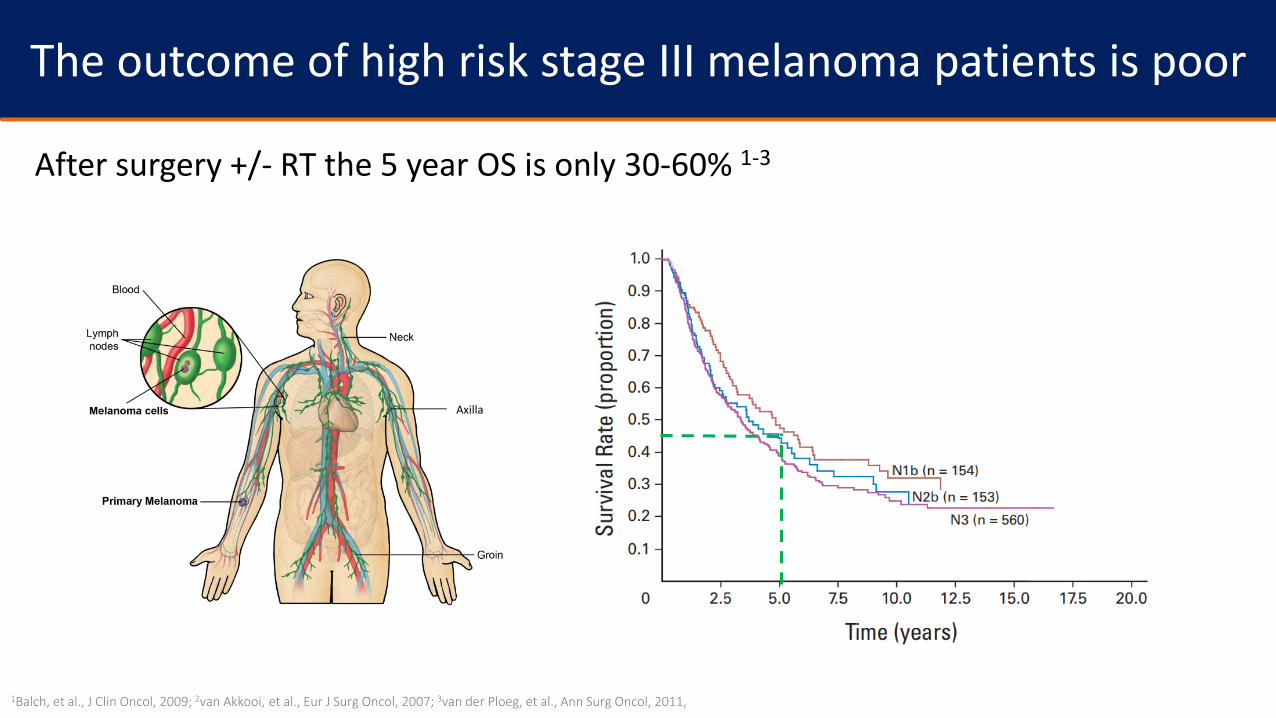
The outcome of high risk stage III melanoma patients is poor
After surgery +/- RT the 5 year OS is only 30-60% 1-3
Axilla
1Balch, et al., J Clin Oncol, 2009; 2van Akkooi, et al., Eur J Surg Oncol, 2007; 3van der Ploeg, et al., Ann Surg Oncol, 2011,

• Adjuvant therapy improved the RFS, but EFS remains poor 4,5
1Balch, et al., J Clin Oncol, 2009; 2van Akkooi, et al., Eur J Surg Oncol, 2007; 3van der Ploeg, et al., Ann Surg Oncol, 2011; 4Combi-AD - Long SMR 2017; 5Checkmate-238 - Weber ESMO 2019
Adapted from Menzies et al ASCO 2019
macromets
Dabrafenib + Trametinib Nivolumab
- 3m Months0
0
10
20
30
40
50
60
70
80
90
100
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50
RFS
(%)
52
3y, 58%2y, 67%
~15-25% screen failures, majority due to
PD
- 3m
RFS
(%)
Months
0102030405060708090
100
0 6 12 18 27 453 9 15 21 3024
3y, 60%2y, 64%
33 36 39 42
~15-25% screen failures, majority due to
PD
Stage IIIB/C
The EFS outcome of high risk stage III melanoma patients is poor

Neoadjuvant versus adjuvant checkpoint inhibition (IPI+NIVO) in macroscopic stage III melanoma – OpACIN
Adjuvant arm
Neo-adjuvant arm
designed by TN Schumacher and CU Blank in 2014
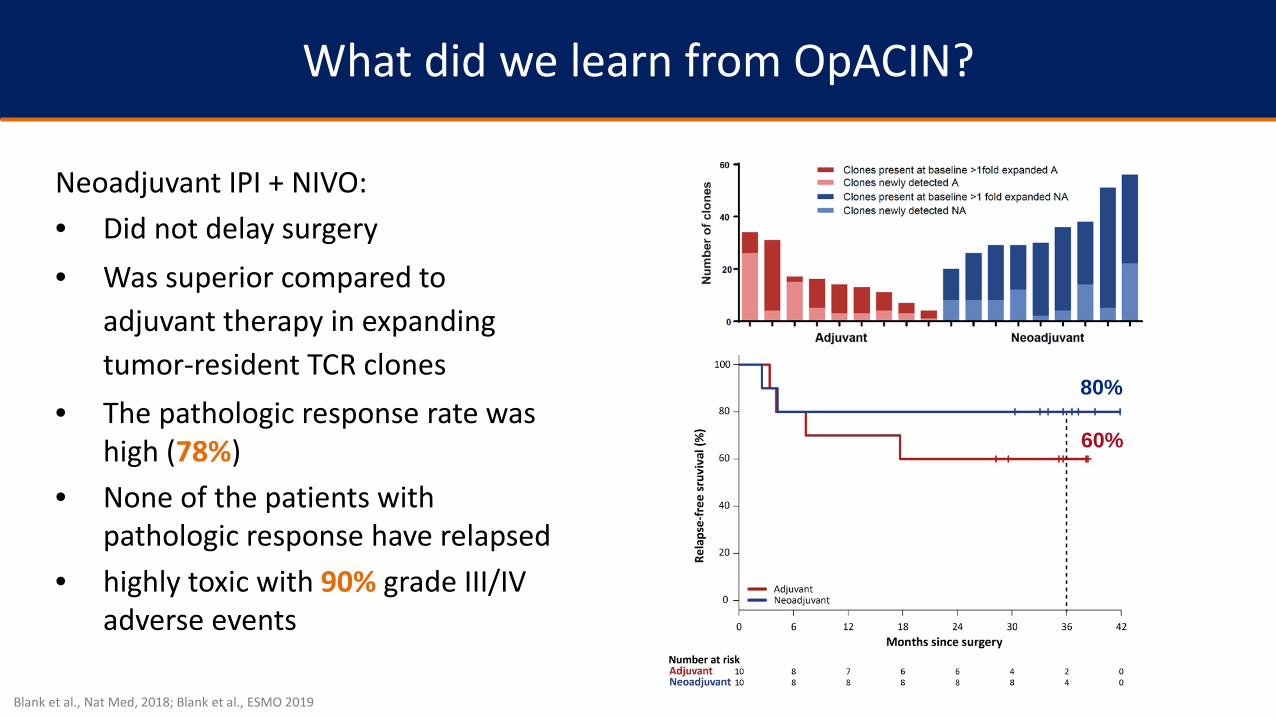
What did we learn from OpACIN?
Neoadjuvant IPI + NIVO:• Did not delay surgery• Was superior compared to
adjuvant therapy in expanding tumor-resident TCR clones
• The pathologic response rate was high (78%)
• None of the patients withpathologic response have relapsed
• highly toxic with 90% grade III/IV adverse events
Blank et al., Nat Med, 2018; Blank et al., ESMO 2019
80%
60%
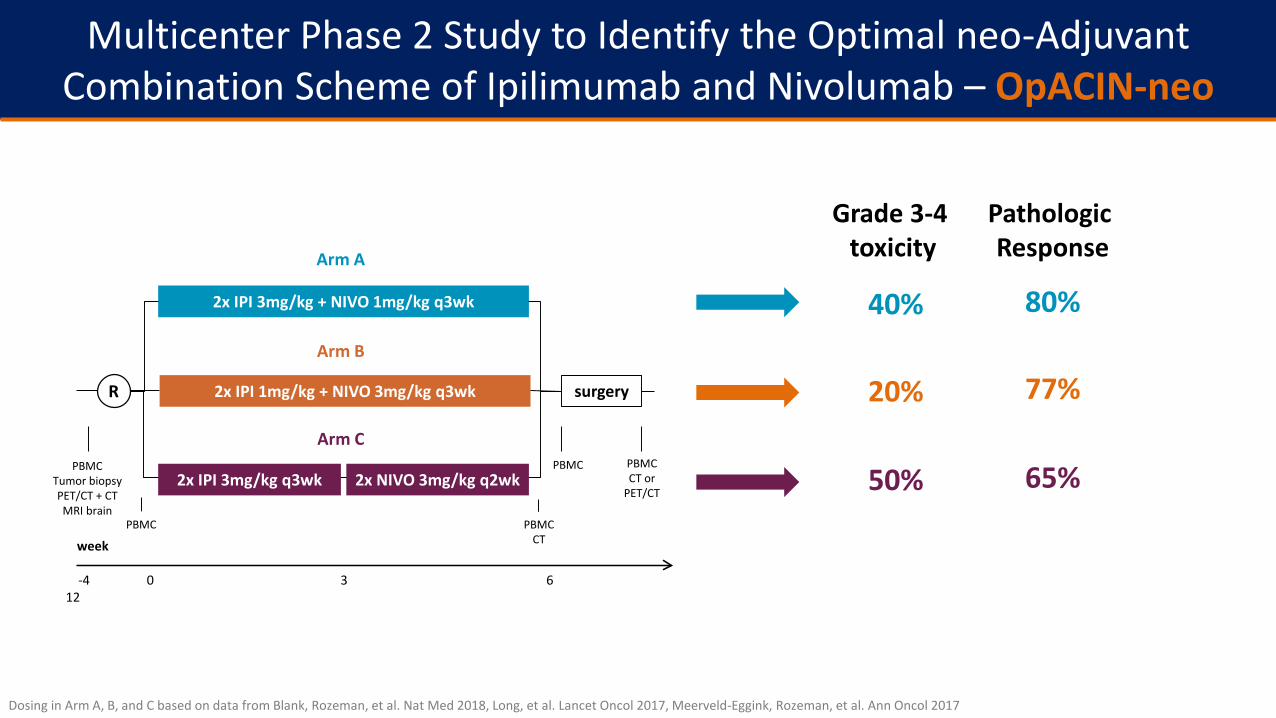
Multicenter Phase 2 Study to Identify the Optimal neo-Adjuvant Combination Scheme of Ipilimumab and Nivolumab – OpACIN-neo
Dosing in Arm A, B, and C based on data from Blank, Rozeman, et al. Nat Med 2018, Long, et al. Lancet Oncol 2017, Meerveld-Eggink, Rozeman, et al. Ann Oncol 2017
-4 0 3 6 12
PBMC
PBMCTumor biopsyPET/CT + CTMRI brain
PBMCCTweek
PBMC
R surgery
2x IPI 3mg/kg q3wkPBMCCT or
PET/CT2x NIVO 3mg/kg q2wk
2x IPI 1mg/kg + NIVO 3mg/kg q3wk
2x IPI 3mg/kg + NIVO 1mg/kg q3wk
Arm A
Arm B
Arm C
40%
20%
50%
Grade 3-4 toxicity
Pathologic Response
80%
77%
65%
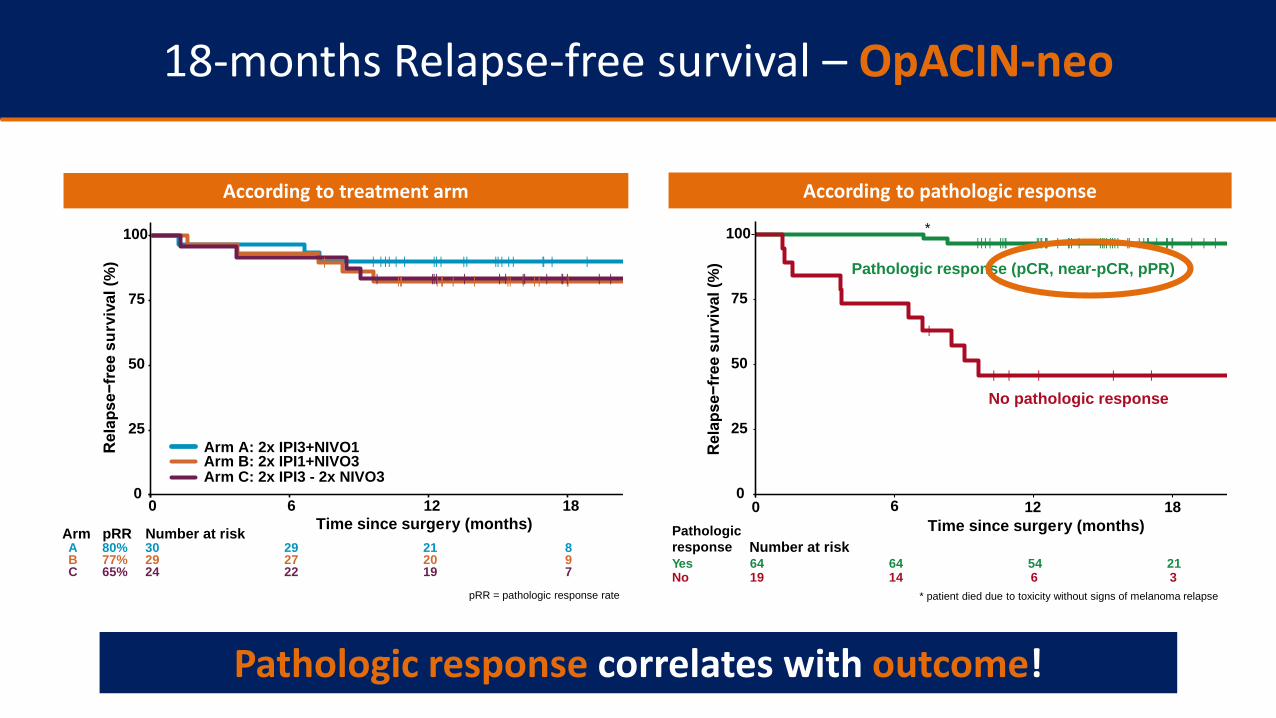
18-months Relapse-free survival – OpACIN-neo
According to treatment arm According to pathologic response
| | | | |||| |||| ||| | ||| | |||| |||| || | | || | || || | | |
|
| | | | |
0
25
50
75
100
0 6 12 18Time since surgery (months)
Rel
apse
−fre
e su
rviv
al (%
)
64 64 54 2119 14 6 3No
YesNumber at risk
No pathologic response
Pathologic response (pCR, near-pCR, pPR)
Pathologicresponse
* patient died due to toxicity without signs of melanoma relapse
| | | | | | || | || || | | | || | ||||| | || | | || | | | ||| ||| | | | || | || | | |
0
25
50
75
100
0 6 12 18Time since surgery (months)
Rel
apse
−fre
e su
rviv
al (%
)
30 29 21 829 27 20 924 22 19 7 C
B A
Number at risk
Arm A: 2x IPI3+NIVO1Arm B: 2x IPI1+NIVO3Arm C: 2x IPI3 - 2x NIVO3
Arm pRR
65%77%80%
pRR = pathologic response rate
*
Pathologic response correlates with outcome!
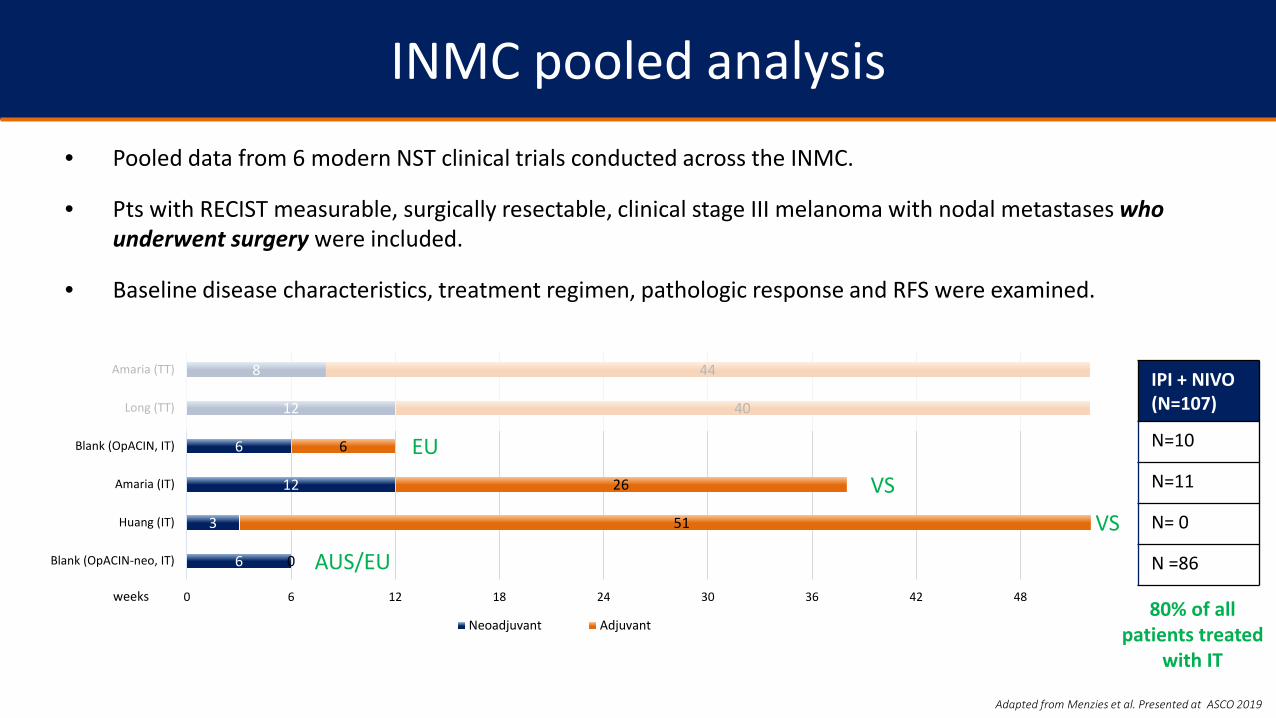
INMC pooled analysis• Pooled data from 6 modern NST clinical trials conducted across the INMC.
• Pts with RECIST measurable, surgically resectable, clinical stage III melanoma with nodal metastases who underwent surgery were included.
• Baseline disease characteristics, treatment regimen, pathologic response and RFS were examined.
Adapted from Menzies et al. Presented at ASCO 2019
6
3
12
6
12
8
0
51
26
6
40
44
0 6 12 18 24 30 36 42 48
Blank (OpACIN-neo, IT)
Huang (IT)
Amaria (IT)
Blank (OpACIN, IT)
Long (TT)
Amaria (TT)
Neoadjuvant Adjuvant
weeks
IPI + NIVO(N=107)
N=10
N=11
N= 0
N =86
80% of all patients treated
with IT
EU
AUS/EU
VS
VS
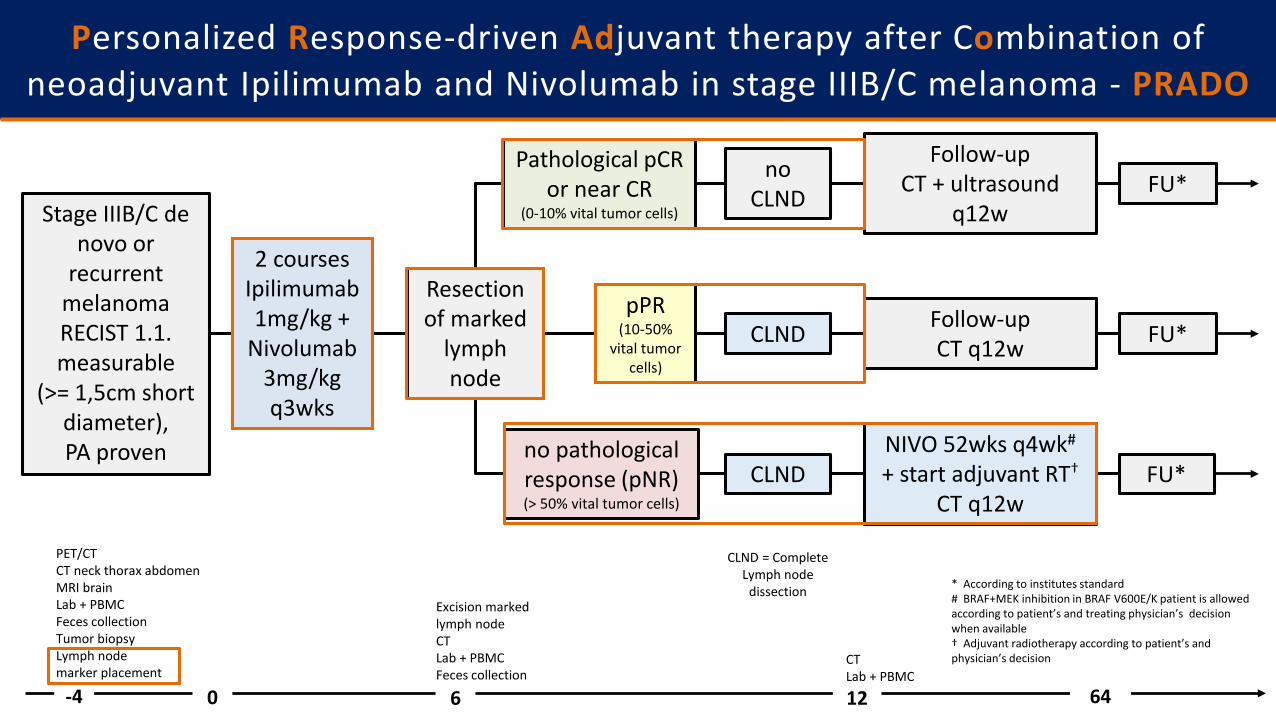
Personalized Response-driven Adjuvant therapy after Combination of neoadjuvant Ipilimumab and Nivolumab in stage IIIB/C melanoma - PRADO
Stage IIIB/C de novo or
recurrent melanomaRECIST 1.1. measurable
(>= 1,5cm short diameter),PA proven
Follow-upCT + ultrasound
q12w
-4 60 12 64
CLND = Complete Lymph node
dissection
CLND
FU*
FU*
no CLND
PET/CT CT neck thorax abdomenMRI brainLab + PBMC Feces collectionTumor biopsyLymph node marker placement
Excision marked lymph nodeCTLab + PBMCFeces collection
CTLab + PBMC
Pathological pCR or near CR
(0-10% vital tumor cells)
CLND
no pathological response (pNR)(> 50% vital tumor cells)
Resection of marked
lymph node
pPR(10-50%
vital tumor cells)
Follow-upCT q12w FU*
* According to institutes standard# BRAF+MEK inhibition in BRAF V600E/K patient is allowed according to patient’s and treating physician’s decision when available † Adjuvant radiotherapy according to patient’s and physician’s decision
NIVO 52wks q4wk#
+ start adjuvant RT†
CT q12w
2 courses Ipilimumab 1mg/kg +
Nivolumab 3mg/kgq3wks

2 courses IPI+NIVO
CLND
Schermers et al., BJS 2019
The pathologic response in the largest lymph node is representing the whole lymph node bed
(MeMaLoc substudy of OpACIN-neo)
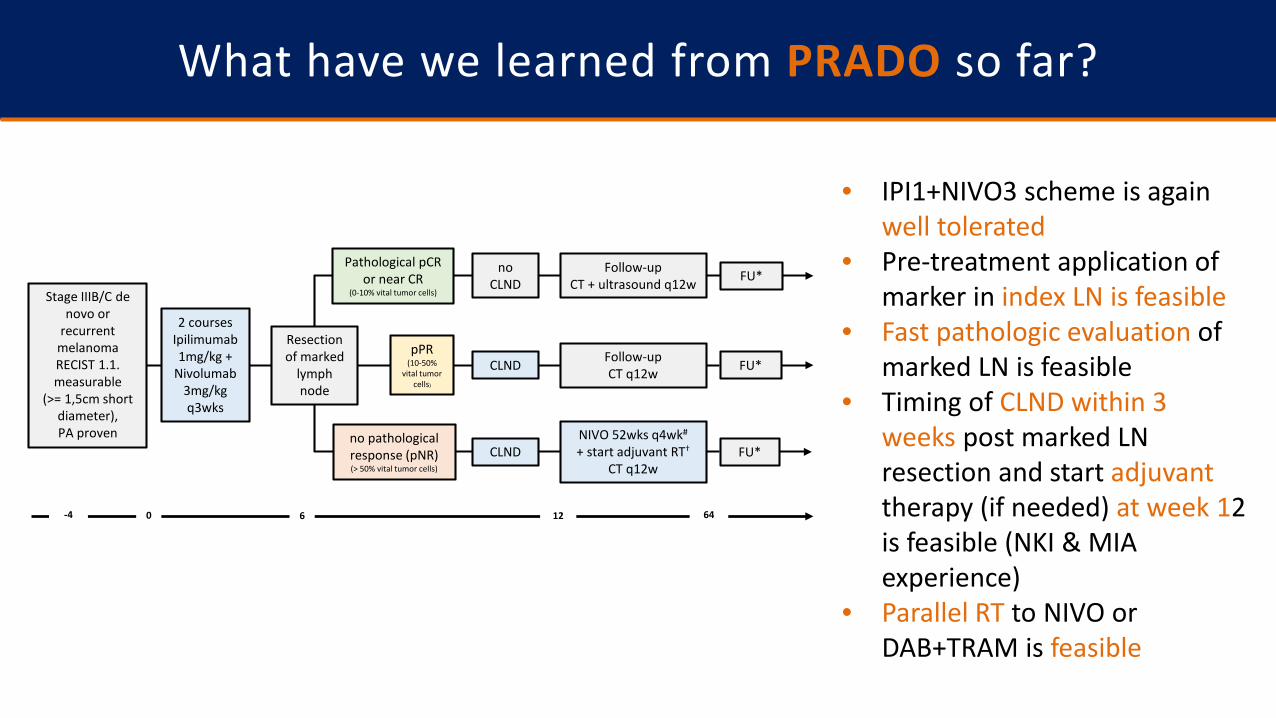
What have we learned from PRADO so far?
• IPI1+NIVO3 scheme is again well tolerated
• Pre-treatment application of marker in index LN is feasible
• Fast pathologic evaluation of marked LN is feasible
• Timing of CLND within 3 weeks post marked LN resection and start adjuvanttherapy (if needed) at week 12 is feasible (NKI & MIA experience)
• Parallel RT to NIVO or DAB+TRAM is feasible
no pathological response (pNR)(> 50% vital tumor cells)
Stage IIIB/C de novo or
recurrent melanomaRECIST 1.1. measurable
(>= 1,5cm short diameter),PA proven
Follow-upCT + ultrasound q12w
-4 60 12 64
CLND
FU*
FU*
no CLND
Pathological pCR or near CR
(0-10% vital tumor cells)
CLND
Resection of marked
lymph node
pPR(10-50%
vital tumor cells)
Follow-upCT q12w FU*
NIVO 52wks q4wk#
+ start adjuvant RT†
CT q12w
2 courses Ipilimumab 1mg/kg +
Nivolumab 3mg/kgq3wks

|||||
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
0%
25%
50%
75%
100%
74 18 14 14 12 11 10 9 8 8 6 4 2 1 076 32 32 26 24 22 22 21 20 19 16 11 5 2 1 0
Surgery AloneT-VEC + Surgery
Number of Patients at Risk:
Arm 1 (T-VEC + Surgery, N = 76): 29.5%Arm 2 (Surgery Alone, N = 74): 16.5%Median Follow-up = 31.2 monthsOverall P = 0.070Overall HR (80% CI) = 0.75 (0.58, 0.96)
Study Month
Kap
lan-
Mei
er (K
M %
)
ITT Analysis Set: 150 patients enrolled and randomized
RFS is not advisable in neoadjuvant randomized trials: T-VEC neoadjuvant versus upfront surgery
Dummer, et al.
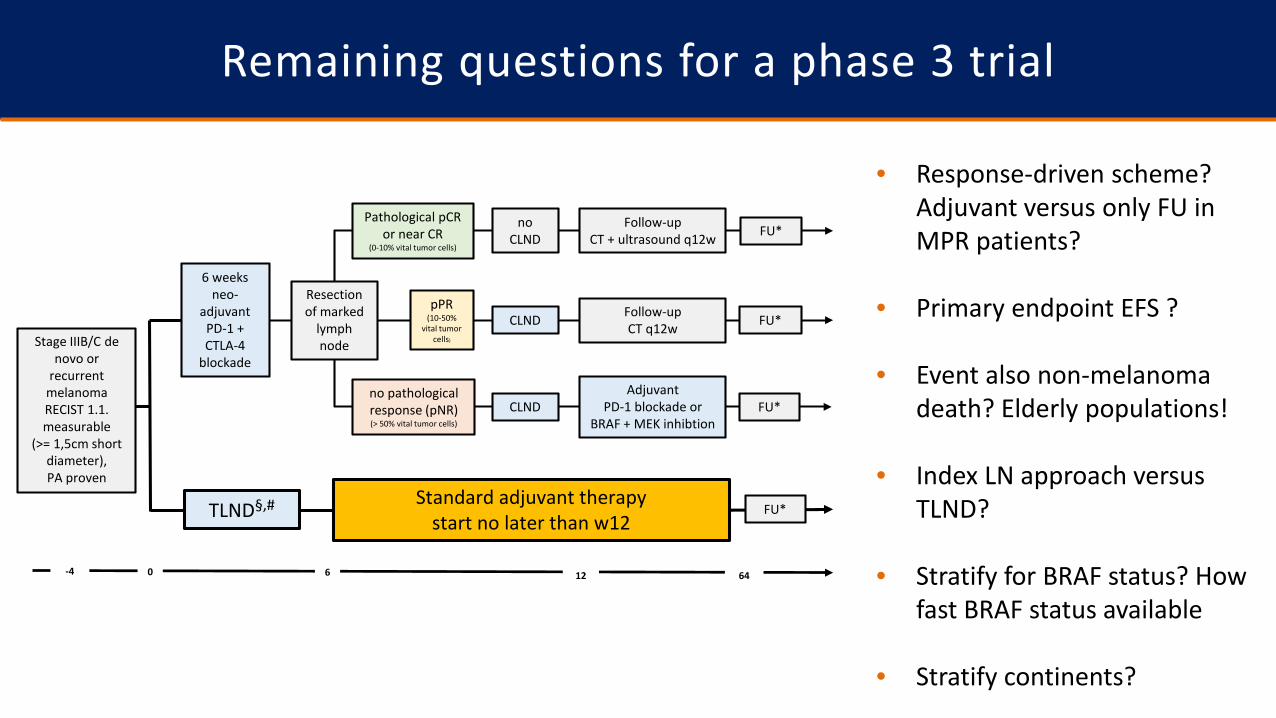
Remaining questions for a phase 3 trial
• Response-driven scheme? Adjuvant versus only FU in MPR patients?
• Primary endpoint EFS ?
• Event also non-melanoma death? Elderly populations!
• Index LN approach versus TLND?
• Stratify for BRAF status? How fast BRAF status available
• Stratify continents?
no pathological response (pNR)(> 50% vital tumor cells)
Follow-upCT + ultrasound q12w
CLND
FU*
FU*
no CLND
Pathological pCR or near CR
(0-10% vital tumor cells)
CLND
Resection of marked
lymph node
pPR(10-50%
vital tumor cells)
Follow-upCT q12w FU*
Adjuvant PD-1 blockade or
BRAF + MEK inhibtion
Stage IIIB/C de novo or
recurrent melanomaRECIST 1.1. measurable
(>= 1,5cm short diameter),PA proven
6 weeksneo-
adjuvant PD-1 + CTLA-4
blockade
TLND§,# Standard adjuvant therapy start no later than w12
-4 60 12 64
FU*

Remaining questions for a phase 3 trial
• Timing of CLND within 3 weeks post marked LN resection feasible?
• Start adjuvant therapy (if needed) at week 12 broadly feasible?
• Pathology fast enough? pRR or MPR as surrogate markers?
• Adjuvant RT parallel NIVO or DAB+TRAM in NR patients?
• How to deal with change to other adjuvant therapy in non-MPR which will be reality
no pathological response (pNR)(> 50% vital tumor cells)
Follow-upCT + ultrasound q12w
CLND
FU*
FU*
no CLND
Pathological pCR or near CR
(0-10% vital tumor cells)
CLND
Resection of marked
lymph node
pPR(10-50%
vital tumor cells)
Follow-upCT q12w FU*
Adjuvant PD-1 blockade or
BRAF + MEK inhibtion
Stage IIIB/C de novo or
recurrent melanomaRECIST 1.1. measurable
(>= 1,5cm short diameter),PA proven
6 weeksneo-
adjuvant PD-1 + CTLA-4
blockade
TLND§,# Standard adjuvant therapy start no later than w12
-4 60 12 64
FU*
Department of Medical OncologyLisette RozemanJudith VersluisIrene ReijersMaartje RohaanMarnix Geukes FoppenSandra AdriaanszHenk MalloWilma UyterlindeJudith LijnsveltSofie WilgenhofHans van ThienenJohn Haanen
Department of Molecular Oncologyand Immunology Oscar KrijgsmanEsmée HoefsmitPetros DimitriadosTrieu My VanMesele ValentiPia KvistborgLorenzo FanchiMembers of the Blank groupDaniel Peeper
Ton Schumacher
Department of PathologyBart van de WielCarolien BiermanLinda Bosch
Department of Surgical OncologyAlexander van AkkooiMichel WoutersWinan van HoudtMartin KlopAnne Miek Koenen
Department of BiometricsKarolina Sikorska Alex TorresLindsay GrijpinkSteven VanhoutvinHarm van Tinteren
Department of RadiologyAnnemarie BruiningStijn Heijmink
CFMPBDennis PetersSten CornelissenLinde BraafAnnegien Broeks
Department of Psychosocial Research and EpidemiologyAnnelies BoekhoutLonneke van de Poll
Patients and their families Collaborators OpACIN-Neo trialGeorgina LongAlexander MenziesRichard ScolyerMIA surgical and trial teamJohan HanssonKarolinska Institute surgical and trial team
International Melanoma NeoadjuvantConsortiumMDA Cancer Center– Jennifer Wargo, Roda Amaria, Hussein Tawbi, Liz Burton, Michael TetzlaffMIA – Georgina Long, Alexander Menzies, Maria Gonzales, Richard ScolyerAll other members of the INMC https://melanoma-inc.org
BMSBauke StegengaAndrew EvansVikki GoodmanConstance PfeiferBrian Lamon
NanoStringSarah Warren
Acknowledgements