neonatal cardiac emergency
TRANSCRIPT

Neonatal Cardiac EmergenciesDr Neeraj Aggarwal
Consultant Pediatric CardiologyDepartment of Pediatric Cardiac Sciences
Sir Ganga Ram Hospital

Neonatal Presentations
1. Cyanosis2. Shock3. CHF 4. Arrhythmias • Septicemia, respiratory disorders, persistent
pulmonary hypertension of newborn (PPHN),inborn errors of metabolism and so on

Case 1
• Asymptomatic neonate was discharged on breast feeds
• Suddenly presents at 3 days of life with bluish discoloration
• Sats 70,mild tachypnoea and minimal distress• soft ESM• No response to oxygen• Ventilation –mild increase in saturations (75%)

Oligemic lung fields and no cardiomegaly

Plan
• Start Prostaglandin E1 and get Echo
• Could not find Prostin –referred • Team went with prostin –shifted to SGRH

• Why prostin started • Can we do it without echo • What is the probable DD• What is the prognosis• Expenses

Diagnosis
• ECHO at SGRH –• Pulmonary atresia with VSD • PDA

Neonatal cyanosis (cardiac causes)
PDA dependent pulmonary circulation
• Pulmonary Atresia ,Intact Ventricular Septum • Pulmonary Atresia, VSD and PDA • Pulmonary Atresia with Single Ventricle• Severe forms of Ebsteins anomaly

What is common to all these lesions
• Oligemia of lung fields on CXR


Pulmonary atresia

Neonatal cyanosis (cardiac causes)
Admixture lesions • Transposition of Great Arteries, intact
Interventricular septum• Total Anomalous Pulmonary venous connection• Truncus Arteriosus • Double Outlet Right Ventricle with VSD• Single ventricle anomalies with or without
Pulmonary stenosis

TGA

Neonatal cyanosis (cardiac causes)
Critical Right ventricular outflow tract obstruction with intracardiac shunt
• Critical Pulmonary Stenosis with interatrial
communication• Tetralogy of Fallot with Critical Pulmonary
Stenosis

Non Cardiac causes of Cyanosis Pulmonary
Primary lung disease• Respiratory distress
syndrome• meconium aspiration • PPHN• Pneumonia• Tracheo- esophageal
fistula
• Airway obstruction• Choanal atresia, laryngo-
tracheomalacia,laryngeal web, vocal cord paralysis
• Extrinsic compression of the lungs
• Pneumothorax• Chylothorax, Hemothorax• Diaphragmatic Hernia,
Space occupying lesions

Non Cardiac causes of Cyanosis Neurologic
• Drug-induced depression of respiratory drive, intracranial haemorrhage,post asphyxial cerebral dysfunction, or central apnea
• Respiratory neuromuscular dysfunction --spinal muscular atrophy, infant botulism, or neonatal myasthenia gravis

Non Cardiac causes of Cyanosis Hematologic
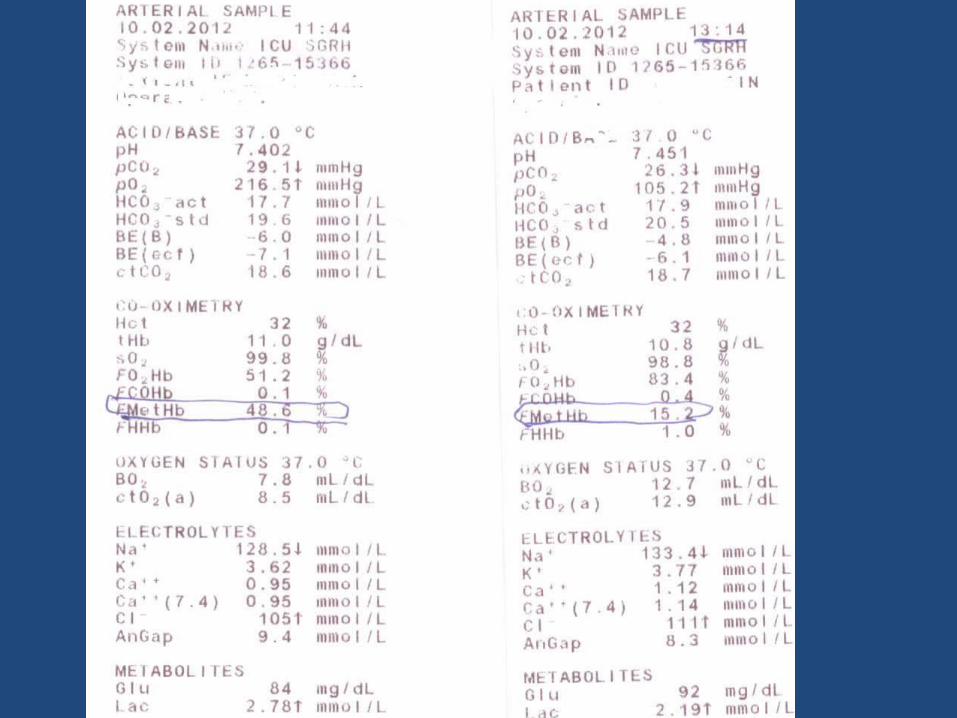
Methemoglobinemia or polycythemia cyanotic with normal Pao2

Importance CXR


Situs Solitus, Dextrocardia

• How to identify cardiac vs resp causes of cyanosis

DD of cyanosis

Hyperoxia test
• Differentiate mainly cardiac from respiratory cyanosis
• If resting saturations are less than 95 %.

At Fio2= 0.21Pao2 (saturation %)
At Fio2 =1.00Pao2 (saturation %)
PaCo2
Normal >70 (>95) >300 (100) Normal
Pulmonary disease
50 (85) >150 (100) High
Neurological disease
50 (85) >150 (100) High
Methemoglobinemia
>70 (<85) >200 (<85) Normal
Cardiac disease
40-60 (75-93) <150 (<93 ) Normal
PPHN Preductal 40-70 (75-95)Post ductal <40 (75)
VariableVariable
Normal/high

Interpretation of hyperoxia test
• PaO2 more than 250 mmHg excludes cyanotic congenital heart disease
• PaO2 is more than 150, cyanotic CHD unlikely
• Pao2 less than 150 Cyanotic CHD
Limitations of Hyperoxia Test
False positive
TAPVC and HLHS may respond to oxygenation
–False negative – Pulmonary disease with a massive intrapulmonary shunt may not
respond to oxygenation.
– Failed hyperoxia test will not differentiate cardiac disease from PPHN

Differential cyanosis
• Preductal saturation > Post-ductal saturation
• Persistent Pulmonary Hypertension of the newborn (PPHN)
• Left ventricular outflow tract obstruction- interrupted aortic arch, critical coarctation of the aorta and critical aortic stenosis.
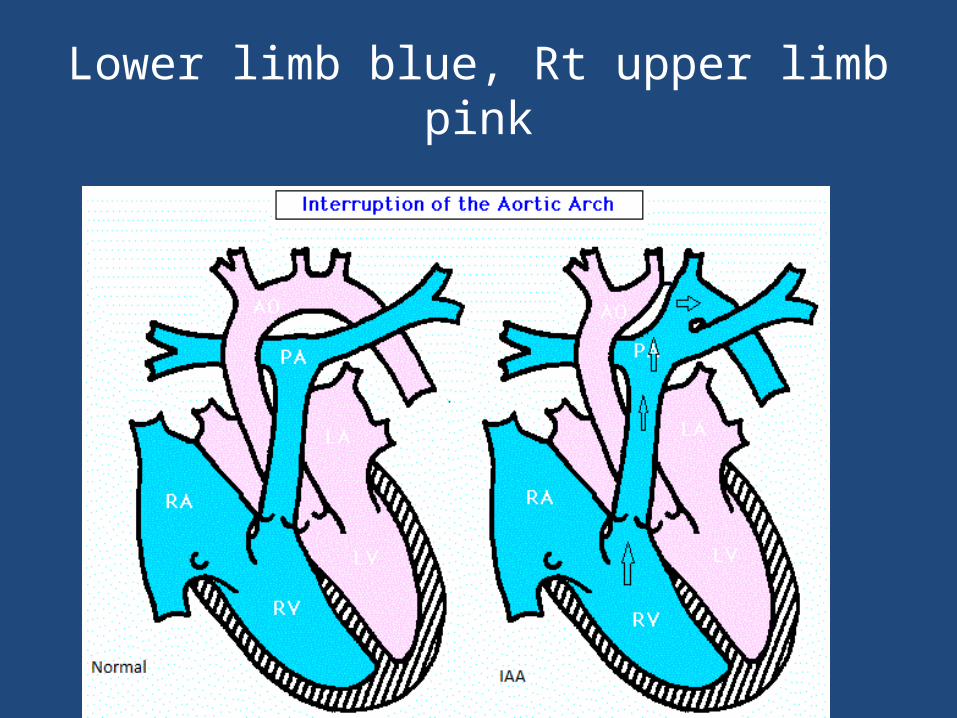
Lower limb blue, Rt upper limb pink
Pink Lower limb , blue upper limb Reverse differential cyanosis
• The postductal saturation higher than the preductal saturation
• TGA with left ventricular outflow obstruction (i.e., critical coarctation of the aorta, interrupted aortic arch, critical aortic stenosis)
• TGA with PPHN.

Cardiac causes of cyanosis
• Healthy neonates who present with sudden onset of cyanosis after being well for 2-3 days when PDA starts constricting
• Soft faint murmur of PDA • TGA -mild tachypnoea without respiratory
distress with saturation of around 90 %• PULSE OXIMETRY

Cardiac causes of cyanosis
• There is obviously no response to oxygen in such cases and hyperoxia test fails
Classification of Cyanotic CHD
• DECREASED PBF– TOF– TGA VSD PS– DORV VSD PS– TA VSD PS– SV PS– Pulmonary
atresia
• INCREASED PBF–TGA VSD–TRUNCUS–TAPVC
(ADMIXTURE)–SV WITHOUT PS–TA VSD NO PS

Chest X ray
• Rule out respiratory issues • Assess pulmonary blood flow and presence of
Cardiomegaly
INCREASED PBF FEATURES ON CXR
• CARDIOMEGALY
• INCREASED VASCULARITY–> 5 END VESSELS IN EITHER OF LUNG
FIELD–> 6 VESSELS TRACEABLE TO LATERAL
1/3rd

INCREASED pulmonary blood Flow
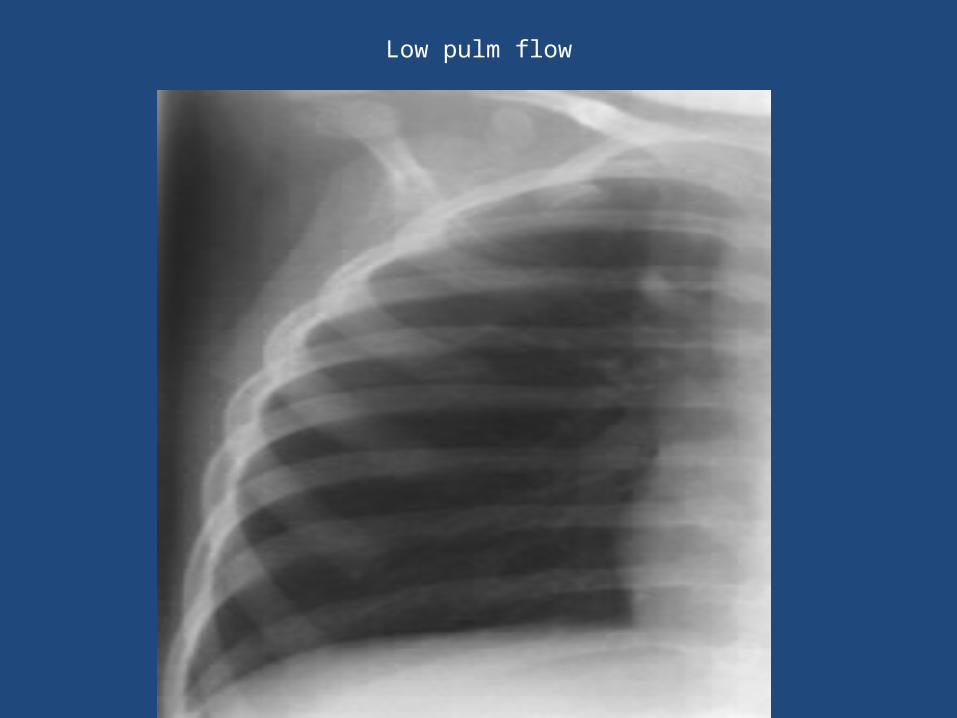
Low pulm flow

INCREASED PBF

Truncus

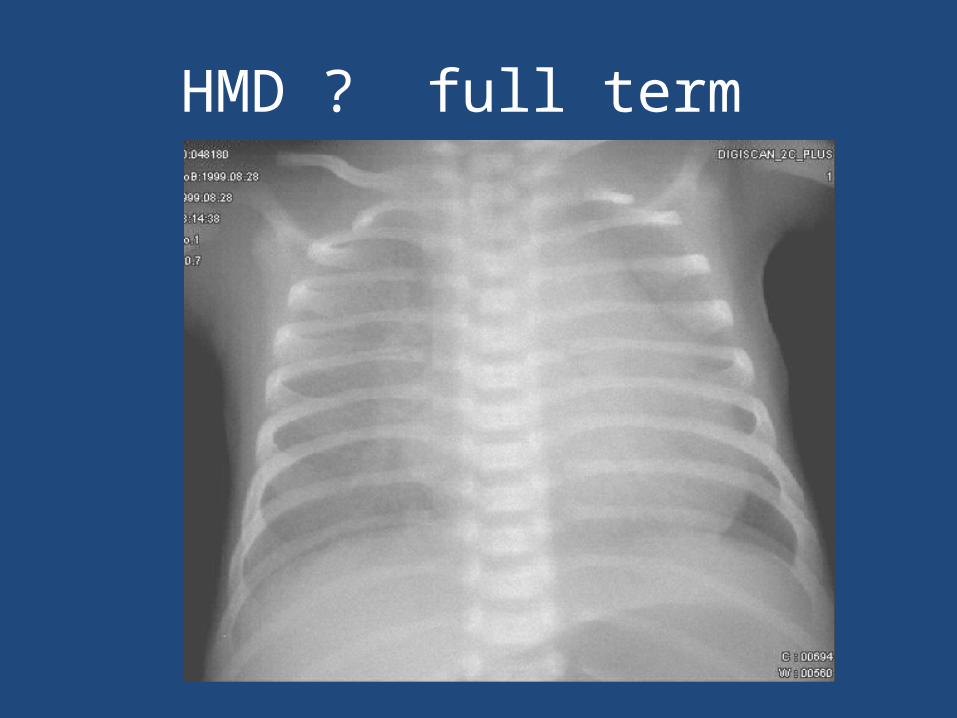
HMD ? full term


Reduced Pulmonary blood flow
No or minimal cardiomegaly • Duct dependent pulmonary circulation • Critical RVOT obstructions with intracardiac
mixing Massive Cardiomegaly with reduced
pulmonary blood flow will suggest a diagnosis of Ebstein anomaly

Pulmonary atresia, VSD
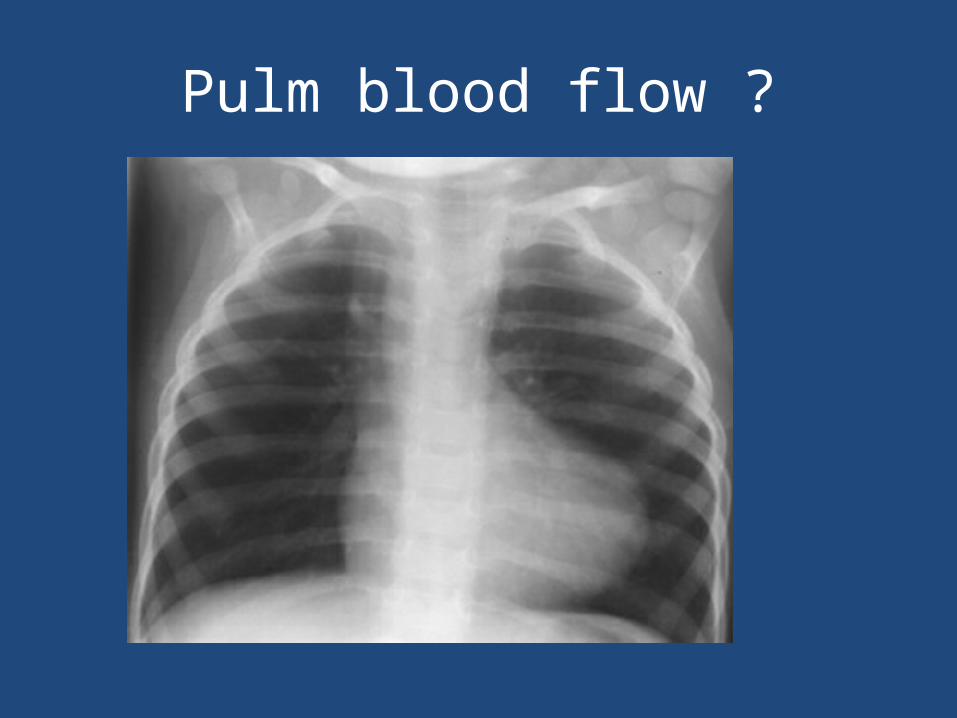
Pulm blood flow ?

Pulm blood flow ? Cardiac size ?

TRICUSPID ATRESIA,PS
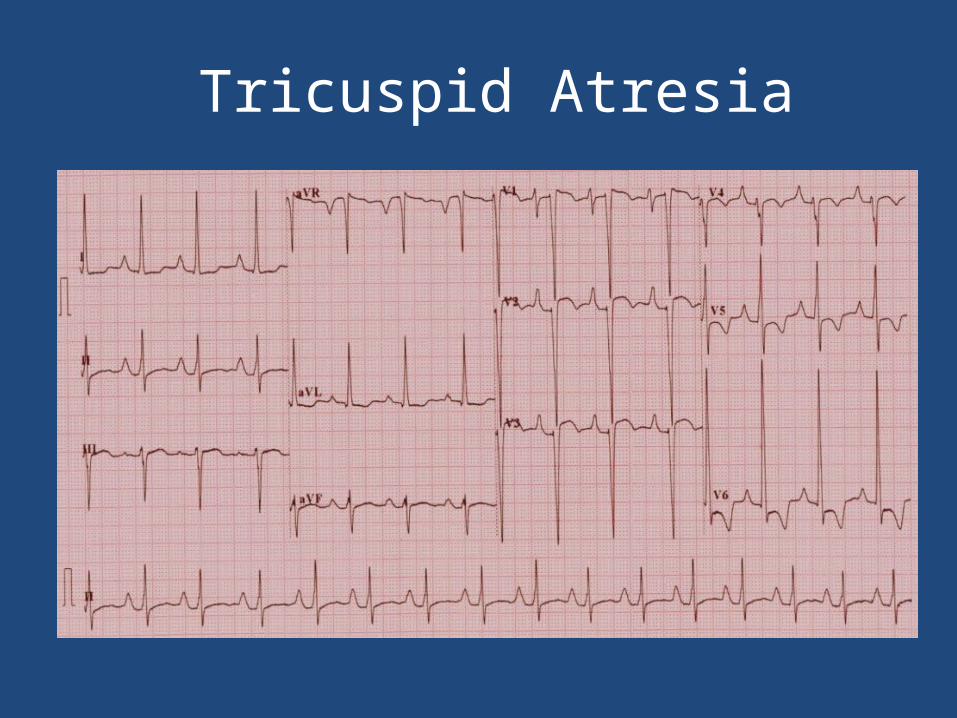
Tricuspid Atresia

Ebstein

Case 2
• D3 old baby –suddenly sick• Poor feeding , Not passing urine • Colour not Looking good –pale • Cold peripheries ,Tachypnoea , tachycardia• poor pulses ,BP 32/20, metabolic
acidosis ,raised lactates Shock

Neonatal shock
• Ventilated • Fluid challenge oliguria unresponsive• Inotropes high doses hypotension persists
• Non cardiac- Sepsis ???

1.Shock1. Duct dependent systemic circulation and Left
ventricular outflow Tract obstructions
• Critical Aortic stenosis and coarctation , Interrupted aortic arch
• Hypoplastic Left Heart Syndrome (HLHS)
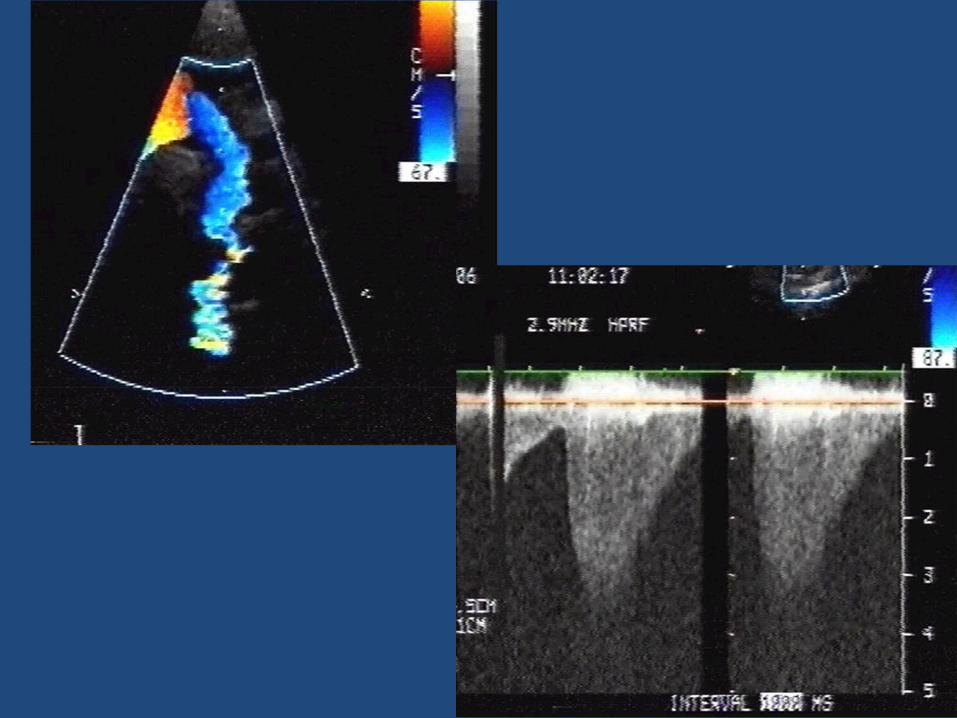
2. Obstructive TAPVC
3. Rhythm disturbances
Tachyarrhythmias and Brady arrhythmias (e.g. Complete heart block)

Clinical presentation
• A healthy newborn who presents after 48-72 hrs of life with sudden onset of pallor, grey appearance and breathing difficulty.
• Not passing urine and not taking feeds over last 4-6 hrs
• Metabolic acidosis• Start prostaglandin E1 suspecting duct dependent
systemic circulation ??• Other measures to stabilize including ventilation
and inotropes (unless echo rules out cardiac lesion)

Clinical clues
• Harsh systolic murmur - obstructive lesion (aortic stenosis or pulmonary stenosis).
• Differential cyanosis with lower limb showing desaturation compared to upper limb should prompt for the cause of PDA shunting right to left (e.g. interrupted aortic arch ,severe Coarctation of aorta or PPHN)
• Differential Pulse –good upper limb and feeble lower limb-Coarctation /IAA
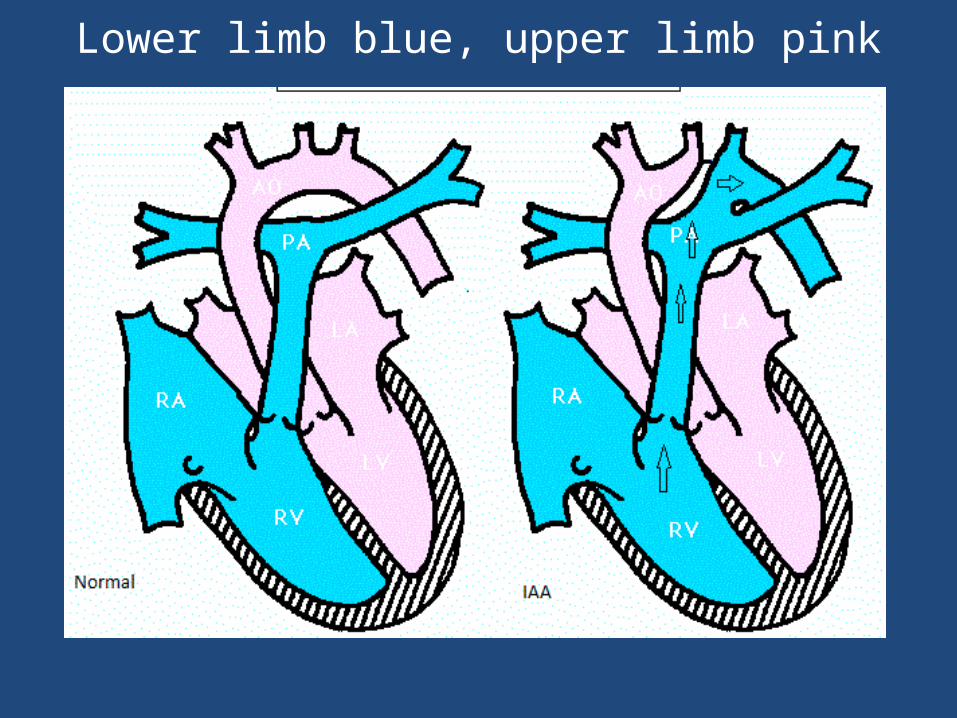
Lower limb blue, upper limb pink

Obstructed TAPVC

ECG
• Neonates presenting with shock to detect arrhythmias
• Supraventricular and ventricular tachycardia, or extreme bradycardia
• Pallor, diaphoresis, dizziness, and syncopal or pallid spells, all related to the decreased cardiac output



Case 3
• Apparently happy baby with mild cyanosis• Hyper dynamic chest , Mild tachypnoea ,sats
80’s (pulse ox)
Transposition physiology
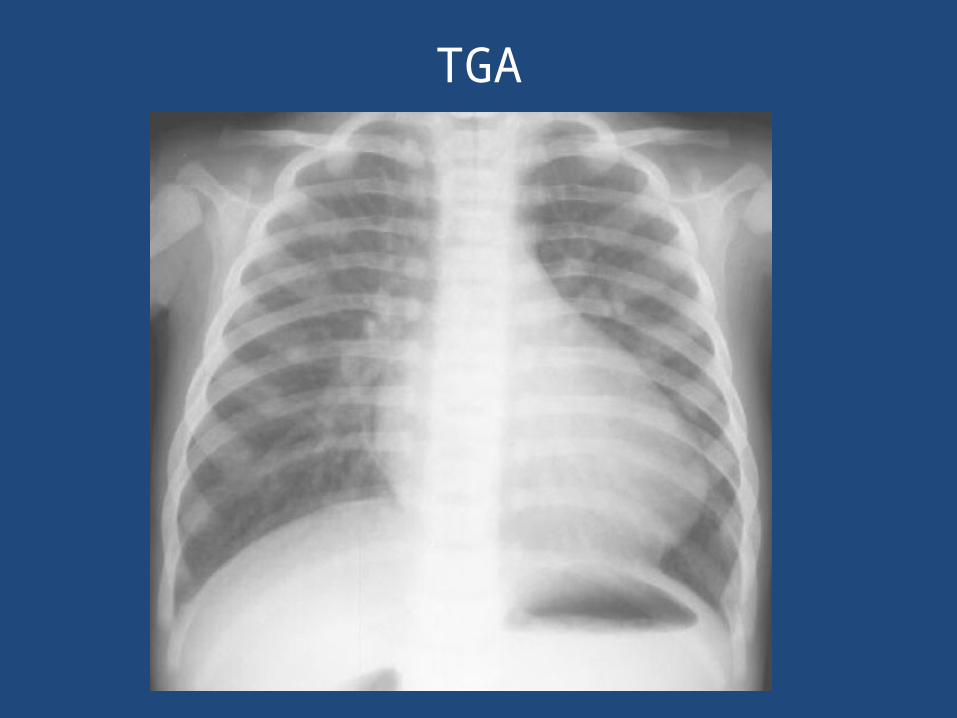
TGA


Parallel great vessels

Prostaglandin E1
• When to use • How to give • Doses and monitoring

How do we start Prostaglandin?
• Dose - 0.001-0.4 microgram/kg/min infusion• Higher doses 0.1 mic/kg/min should be used
to reopen the closed PDA (or if there is sudden onset of severe cyanosis or shock).
• Increments of 0.05 microgram /kg/min every 5-10 minutes
• Once the duct has opened, dose can be reduced to a minimum

Preparation
• 500 microgram per vial, dilute it in 50 ml of 5 % dextrose and start in infusion pump.
• According to formula (this formula can be used for any inotropes)
• 3×wt×microgram/kg/min divided by concentration (mg) in 50 ml =flow rate in ml/hr
• So for wt of 3 kg child and dose of 0.1mic/kg/min• 3x3x0.1/0.5=ml/hr ( 0.9/0.5) = 1.8 ml per hr
infusion will give you 0.1 microgram/kg/min.

Preparation
• Lower doses in the range of 0.01 microgram/kg/min till definitive surgical repair.
• With proper monitoring in ICU for saturations and under echocardiographic guidance (for PDA monitoring), dose can be reduced to 0.001 microgram/kg/min.

No Response to prostaglandin Infusion
Diagnosis Management
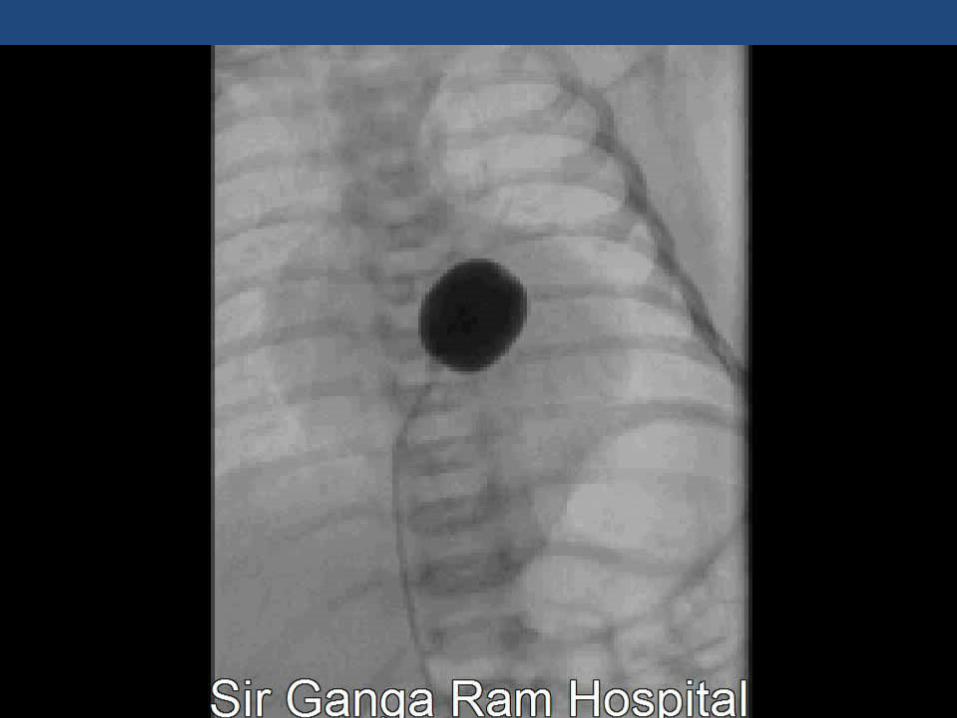
1. Transposition of Great Arteries with Intact Ventricular Septum and a restrictive interatrial communication
Needs emergency Balloon Atrial Septostomy
1. Obstructed TAPVC Emergency surgery
1. Non Cardiac Diagnosis Treatment of etiology
Congestive heart failure
Cyanotic heart disease with high pulmonary flow • Truncus Arteriosus • Single ventricle physiology without Pulmonary
Stenosis• Transposition of Great Arteries with VSD• Double Outlet Right Ventricle with VSD• Total Anomalous Pulmonary venous connection

Cyanotic heart disease with high pulmonary flow
• Not significantly cyanotic due to torrential pulmonary blood flow
• Saturation may vary in the range of 90’s.• Naked eyes will not pick up the cyanosis• Pulse oximetry -- early detection

Acyanotic Heart Disease with high pulmonary flow
• Preterm with significant post tricuspid shunt
lesions (e.g. VSD ,PDA ,Aorto- Pulmonary window)• Severe valvular regurgitant lesions (e.g. Mitral
regurgitation associated with AV canal defects)• Anomalous Left Coronary Artery from Pulmonary
Artery(ALCAPA)• Cardiomyopathy

Other causes of CHF
Rhythm disturbances • Tachyarrhythmias • Brady arrhythmias ( e.g. complete heart block, High
degree second heart block) Non Cardiac causes • High output states like anemia ,thyrotoxicosis ,
systemic Arteriovenous malformations (g.e.Vein of Galen )

Clinical features
• Difficulty in feeding ,sub costal indrawing, sweating with feeds ,tachypnoea, tachycardia, gallop rhythm and hepatomegaly .

Pulmonary blood flow –high
• Excessive sweating• Feeding difficulty (suck rest suck) • Chest infection• Failure to thrive• Hyperdynamic precordium• Shunt murmur and diastolic flow murmur• Cardiomegaly

Preterm PDA
• Steal phenomenon like cerebral steal (manifesting as apnea) or steal from gut (manifesting as necrotizing enterocolitis ).
• Bounding pulses along with wide pulse pressure should give a suspicion

Preterm PDA
• After surfactant therapy, they show improvement and ventilatory requirements go down .
• As Hyaline membrane disease improves and PVR falls, PDA shunt becomes significant and ventilatory requirements become higher again

Preterm VS Full term –CHF
• Preterm --Other post tricuspid lesions can also lead to CHF in preterm neonates (e.g. Large VSD, AP window)
• Full term --Usually don’t present in full term
neonates as PVR falls after 4-6 weeks and then shunt lesions start manifesting as CHF.

CHF
• Chest X ray in such cases will show Cardiomegaly (cardiothoracic ratio >0.6).
• Thymic and extra cardiac shadows


ABSENT PULMONARY VALVE

TRUNCUS
Rhythm disturbances
• SVT • Brady arrhythmias with Long QTc

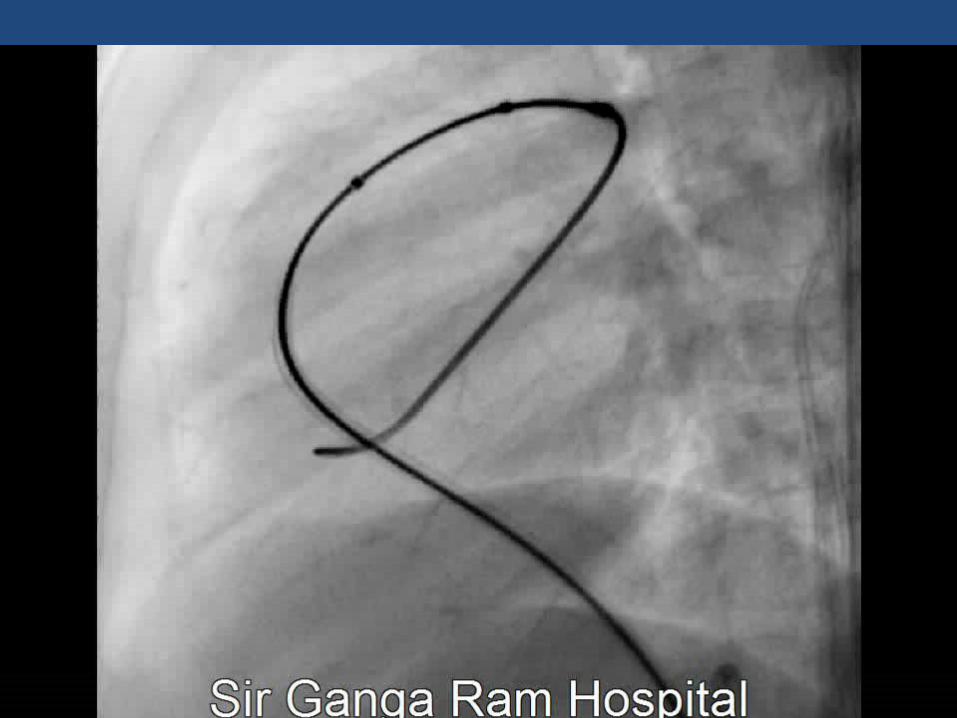
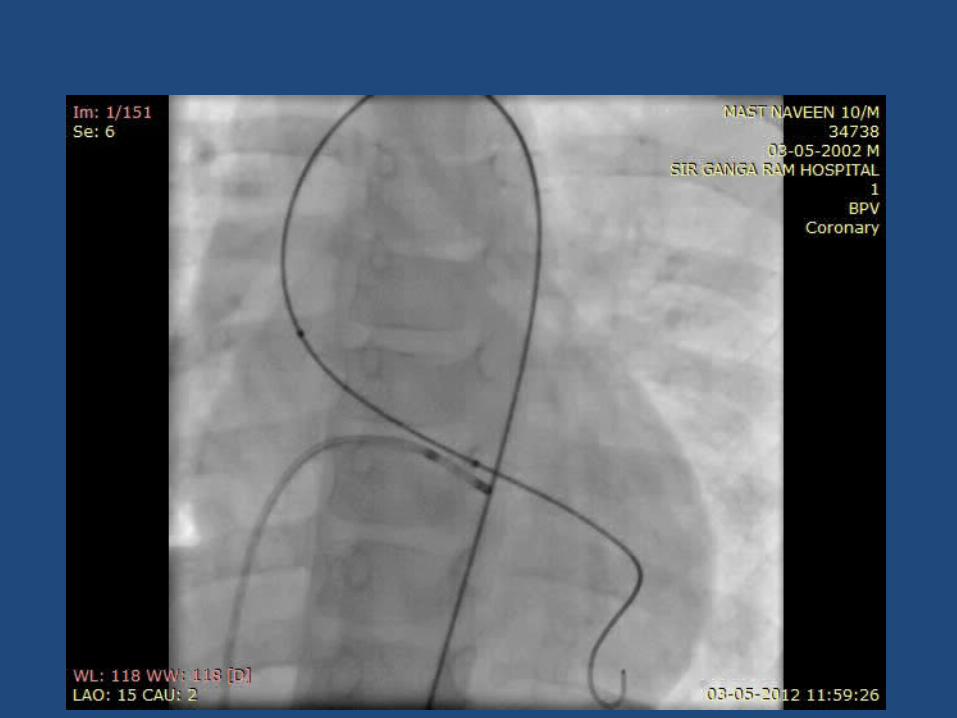
Neonatal Interventions
• BAS-Ballon atrial Septostomy• BPV-Ballon pulmonary valvuloplasty• BAV-Ballon aortic valvuloplasty• Ballon Coarct angioplasty • PDA stenting


Summary
• Right sided obstructive lesions-(cyanosis) - critical PS,pulmonary atresia
• Left sided obstructive lesions (Collapse) – critical AS, IAA, COA, HLHS

Summary
• Mixing lesions (cyanosis with CCF) – TGA
• ASD dependent lesions (cyanosis with CCF)- TAPVC, Tricuspid atresia

Probability of prostaglandin sensitive lesion is increased
• In a cyanosed neonate with failed hyperoxia test – murmur
• In a non -cyanosed neonate ,by abnormal
pulses • Whenever in doubt, Start PGE1 , though may not be effective in
certain lesions
