neonatal death associated with maternal methamphetamine abuse susan r. howe, phd joyce y. ho, bs...
TRANSCRIPT

Neonatal Death Associated with Maternal Methamphetamine Abuse
Susan R. Howe, PhDJoyce Y. Ho, BSCarl Wigren, MD
December, 2006

Topics for Today
• Two cases of neonatal death– History of maternal methamphetamine use
• Children and methamphetamine
• Methamphetamine analysis in the lab
• Pathology of neonatal death with maternal methamphetamine use

What is Methamphetamine?
• CNS Stimulant
• Extremely addictive
• 6-8 hr high (or longer)
• Easy to produce
• Inexpensive

Pleasurable Effects
• Nearly immediate “flash” or “rush”
• Euphoria, alertness
• Increased energy
• Increased libido

Undesirable Effects• Used in “binge and crash” pattern• Leads to tolerance and abuse• Users forego food and sleep• Significant toxicity
– Increased heart rate – High blood pressure– Increase body temperature– Convulsions– Stroke– Death




Long Term Meth Use
• Violent behavior
• Psychotic symptoms
– Auditory hallucinations
– Mood disturbances
– Delusions and paranoia
• Changes to the brain

Current Perspective
National Drug Intelligence Center, 2005

Current Perspective
• 2005: 4.3% of US population > 12 has used methamphetamine
2005 National Survey on Drug Use and Health
• 2005: 4.5% of high school seniors have used methamphetamine
2005 Monitoring the Future Study, NIDA

Women and Meth
• 2003 Arrestee Drug Abuse Monitoring Program
– 4.7% of adult male arrestees test positive for meth at the time of arrest
– 8.8% of adult female arrestees test positive for meth at the time of arrest

Meth and Pregnancy• Infant Development, Environment, and
Lifestyle Study, 2006 (IDEAL)
– 5.2% of women have used meth at some time in their pregnancy
– Meth use during pregnancy associated with small birth weight babies
Meth and Pregnancy
• Fetal growth restriction– Long term effects?
• Ruptured placenta
• Preterm labor
• Disease (HIV, hepatitis)
• Poor prenatal care, nutrition

“Prenatal exposure to drugs of abuse is
the single largest preventable cause of
developmental compromise of American children today.”
Malanga and Kosofsky, Developmental Brain Research 147(1-2): 47-57, 2003

Compromised Parenting
• Neglect• Diverted resources• Physical/mental health problems• Lack of supervision• Access to meth and paraphernalia• Exposure to high risk population• Poor nutrition/living conditions• Poor preventive care/disease management


Meth Manufacture
• An excerpt from the Betty Cranker Cookbook:
“Take a pinch of red phosphorous, a smidgen of ephedrine, a dash of iodine and a skosh of lye. Add some distilled water and simmer for a few hours and hope it doesn’t explode and kill you.”
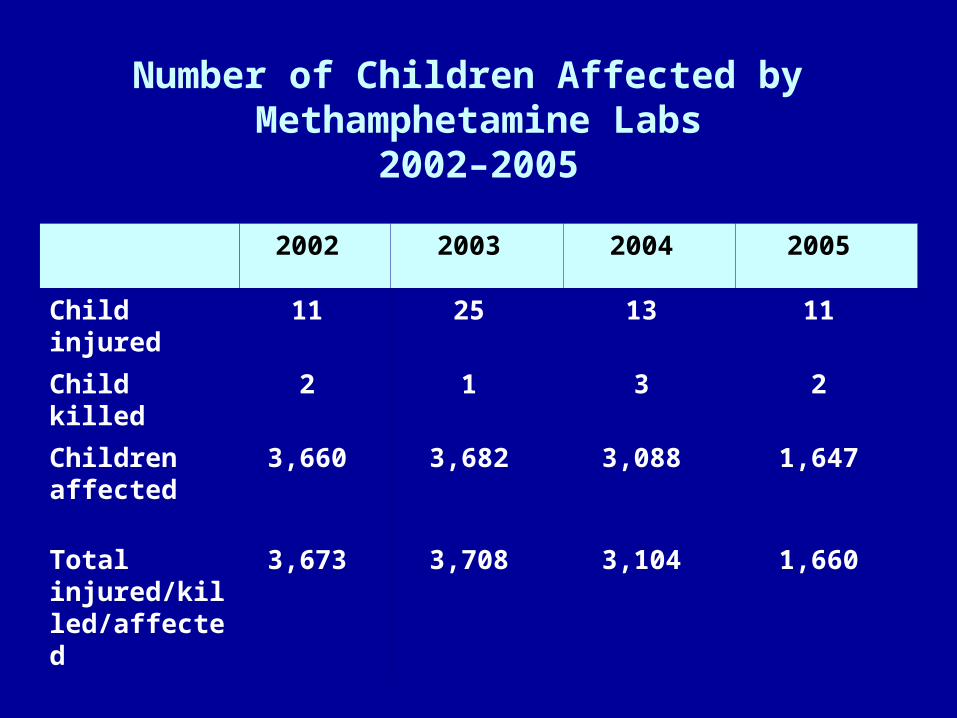
Number of Children Affected by Methamphetamine Labs
2002–2005
2002 2003 2004 2005
Child injured 11 25 13 11
Child killed 2 1 3 2
Children affected
3,660 3,682 3,088 1,647
Total injured/killed/affected
3,673 3,708 3,104 1,660

Meth Lab Hazards to Children
• Accidental methamphetamine ingestion
• Chemical and physical hazards
• Neglect and abuse
• Increased risk of accidents


Medical Examiner’s Case 1
• Hispanic Female admitted to hospital for
vaginal bleeding
• Emergency hysterectomy performed
after delivery
• Later pronounced at the hospital

Toxicology Report Case 1
• Aorta Blood Amphetamine TDX Positive
• Hospital Blood Amphetamine 33.7 ng/ml• Hospital Urine Amphetamine Positive• Hospital Blood Methamphetamine 109.0 ng/ml• Hospital Urine Methamphetamine Positive

Case 2Companion Case to Case No.1
• Full term fetal demise pronounced upon delivery
• Mother tested positive for Amphetamine Screen at the hospital

Toxicology Report Case 2
• Urine Amphetamine TDX Positive
• Aorta Blood Amphetamine 104.5 ng/ml• Urine Amphetamine Positive• Meconium Amphetamine 422.0 ng/ml• Aorta Blood Methamphetamine 299.2 ng/ml• Urine Methamphetamine Positive• Meconium Methamphetamine 1468.4 ng/ml
Case 3
• Full term stillborn infant delivered by cesarean section
• Mother had normal pregnancy
• Mother denied drug usage
• Urine drug screen on mother tested positive

Toxicology Report Case 3
• Urine Amphetamine TDX Positive• Aorta Blood Amphetamine 45.1 ng/ml• Urine Amphetamine Positive• Meconium Amphetamine 266.0 ng/ml• Aorta Blood Methamphetamine 235.5 ng/ml• Urine Methamphetamine Positive• Meconium Methamphetamine 1816.0 ng/ml

Chief Medical Examiner
Crime Lab Toxicology Human ID
DNA
Firearms
TraceEvidence
ForensicToxicology
Drug Chemistry
ForensicDentistry
Fingerprints
Anthropology/Radiology

Toxicology Laboratory Goals:
– assist the medical examiner in evaluating the role of toxicants as a determinant or contributory factor in the cause and manner of death
– aid law enforcement agencies in the investigation of criminal activities


TSQ

AMPHETAMINE/METHAMPHETAMINE CHROMATOGRAM
C:\Xcalibur\Data\AMPQCMIXOCT12 10/12/2006 1:20:37 PM
RT: 0.00 - 8.01
0 1 2 3 4 5 6 7 8Time (min)
0
100
MD
MA
0
100
MD
A
0
100
ep
he
dri
ne
0
100
me
th-d
5
0
100
me
th
0
100
am
p-d
5
0
100
am
p
RT: 4.494.487AA: 13185356SN: 2922
RT: 4.444.444AA: 3113532SN: 3269
RT: 5.115.113AA: 18874303SN: 4607
RT: 5.105.099AA: 6151323SN: 9271
RT: 3.723.721AA: 18380772SN: 4931
RT: 5.155.149AA: 1990057SN: 1947
RT: 5.615.606AA: 7288093SN: 1526
RT: 3.463.464AA: 241049SN: 22
RT: 6.536.533AA: 32367SN: 9
NL: 9.23E5TIC F: + c ESI SRM ms2 [email protected] [ 91.121-91.123, 119.125-119.127] MS ICIS AMPQCMIXOCT12
NL: 2.19E5TIC F: + c ESI SRM ms2 [email protected] [ 96.099-96.101] MS ICIS AMPQCMIXOCT12
NL: 1.46E6TIC F: + c ESI SRM ms2 [email protected] [ 91.120-91.122, 119.126-119.128, 133.140-133.142] MS ICIS AMPQCMIXOCT12
NL: 4.79E5TIC F: + c ESI SRM ms2 [email protected] [ 92.119-92.121] MS ICIS AMPQCMIXOCT12
NL: 1.13E6TIC F: + c ESI SRM ms2 [email protected] [ 148.157-148.159] MS ICIS AMPQCMIXOCT12
NL: 1.68E5TIC F: + c ESI SRM ms2 [email protected] [ 135.061-135.063] MS ICIS AMPQCMIXOCT12
NL: 6.48E5TIC F: + c ESI SRM ms2 [email protected] [ 135.061-135.063] MS ICIS AMPQCMIXOCT12

AMPHETAMINE/METHAMPHETAMINE SPECTRAC:\Xcalibur\Data\AMPQCMIXOCT12 10/12/2006 1:20:37 PM
RT: 0.00 - 8.01
0 1 2 3 4 5 6 7 8
Time (min)
0
10
20
30
40
50
60
70
80
90
100
am
p
RT: 4.494.487AA: 13185356SN: 2922
NL: 9.23E5
TIC F: + c ESI SRM ms2 [email protected] [ 91.121-91.123, 119.125-119.127] MS ICIS AMPQCMIXOCT12
AMPQCMIXOCT12 #1505 RT: 4.49 AV: 1 NL: 5.69E5F: + c ESI SRM ms2 [email protected] [ 91.121-91.123, 119.125-119.127]
91.122 91.123
m/z
119.125 119.126
m/z
0
10
20
30
40
50
60
70
80
90
100
Re
lative
Ab
un
da
nce
0
10
20
30
40
50
60
70
80
90
100
Re
lative
Ab
un
da
nce
91.12
119.13
RT: 0.00 - 8.01
0 1 2 3 4 5 6 7 8
Time (min)
0
10
20
30
40
50
60
70
80
90
100
me
tha
mp
RT: 5.115.113AA: 18874303SN: 4607
NL: 1.46E6
TIC F: + c ESI SRM ms2 [email protected] [ 91.120-91.122, 119.126-119.128, 133.140-133.142] MS ICIS AMPQCMIXOCT12
AMPQCMIXOCT12 #1707 RT: 5.09 AV: 1 NL: 1.35E6F: + c ESI SRM ms2 [email protected] [ 91.120-91.122, 119.126-119.128, 133.140-133.142]
91.122
m/z
119.126
m/z
133.140
m/z
0
10
20
30
40
50
60
70
80
90
100
Re
lative
Ab
un
da
nce
0
10
20
30
40
50
60
70
80
90
100
Re
lative
Ab
un
da
nce
0
10
20
30
40
50
60
70
80
90
100
Re
lative
Ab
un
da
nce
91.12
119.13
133.14