neuro opthal
DESCRIPTION
OpthalmologyTRANSCRIPT
NEURO - OPTHALGROUP 2 A1
OBJECTIVES1. Clinical anatomy of extraocular muscles
2. Clinical anatomy of the cranial nerves III,IV,VI
3. Action of extraocular muscles
4. Assessment of ocular deviations:
a. Hirschberg’s test
b. Extraocular movement
5. Cranial nerve palsies ( cause and management)
a. Oculomotor nerve palsy
b. Trochlear nerve palsy
c. Abducent nerve palsy
6. Visual pathway
a. Normal visual pathway
b. Visual field defects due to lesions along the pathway
7. Normal Pupil light reflex pathway
MBBS 0910 GROUP 2A1 2

ANATOMY OF EXTRAOCULAR
MUSCLES
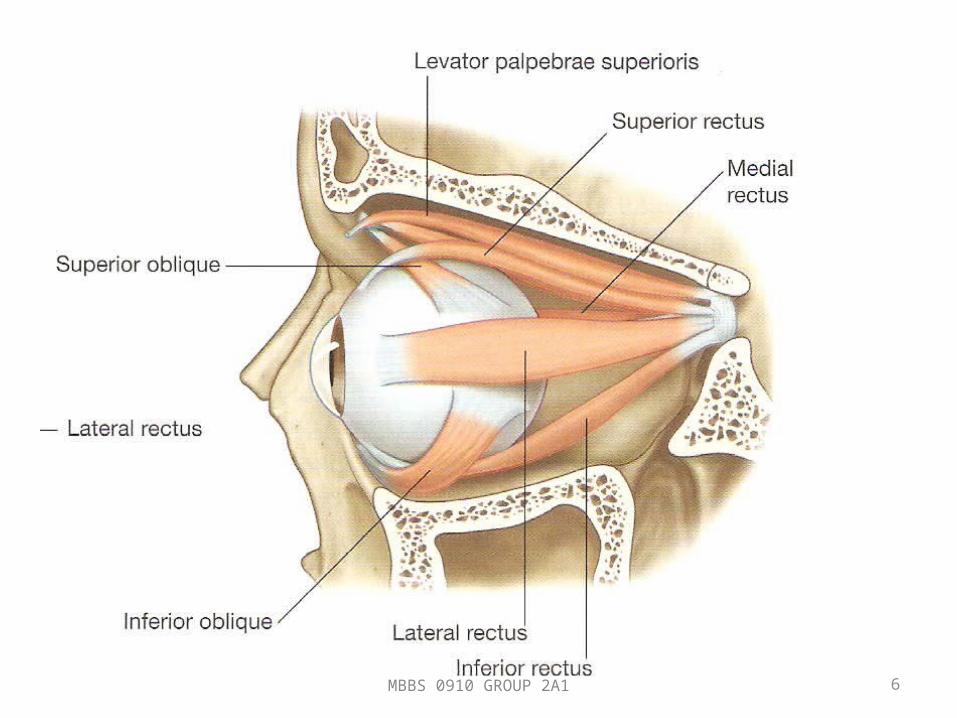
EXTRAOCULAR MUSCLES
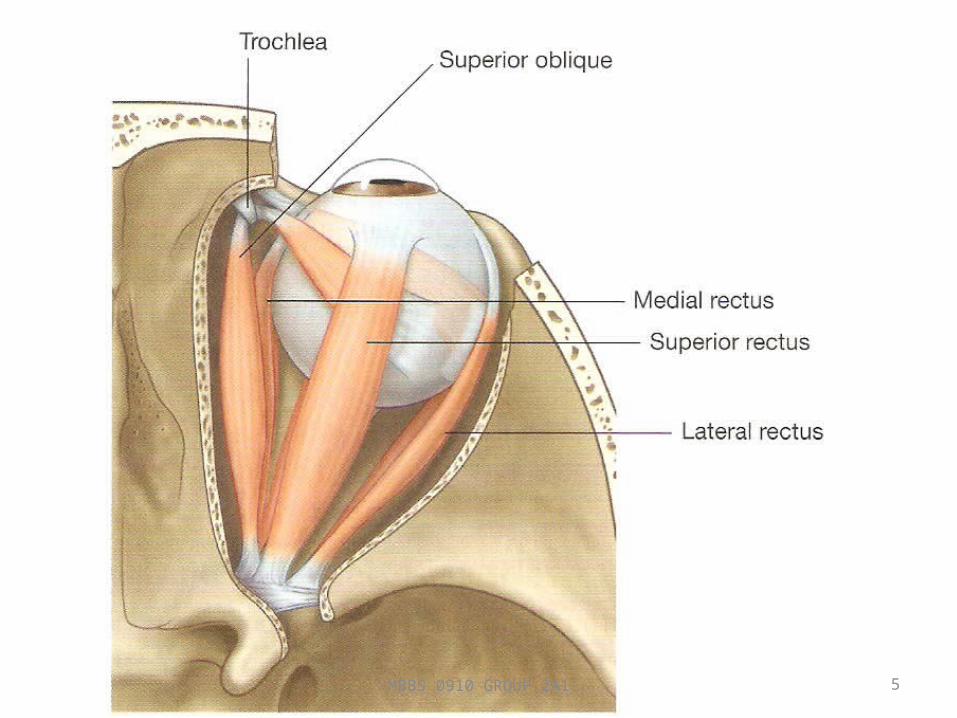
• Consist of 4 recti and 2 oblique muscles.
1. Lateral rectus
2. Medial rectus
3. Inferior rectus
4. Superior rectus
5. Inferior oblique
6. Superior oblique
• The annulus of Zinn (common tendinous ring) is a ring of fibrous tissue surrounding the optic nerve at its entrance at the apex of the orbit.
• The extraocular muscles are supplied mainly by branches of the ophthalmic artery.
MBBS 0910 GROUP 2A1 4
MBBS 0910 GROUP 2A1 5
MBBS 0910 GROUP 2A1 6
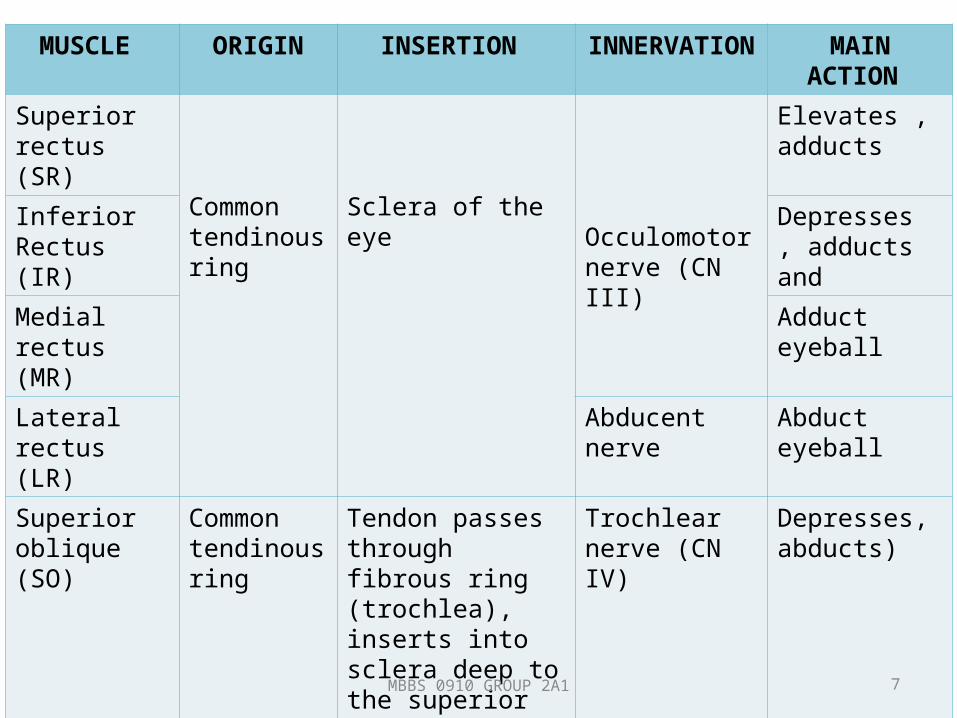
MUSCLE ORIGIN INSERTION INNERVATION MAIN ACTION
Superior rectus (SR)
Common tendinous ring
Sclera of the eyeOcculomotor nerve (CN III)
Elevates , adducts
Inferior Rectus (IR)
Depresses , adducts and
Medial rectus (MR)
Adduct eyeball
Lateral rectus (LR)
Abducent nerve Abduct eyeball
Superior oblique (SO)
Common tendinous ring
Tendon passes through fibrous ring (trochlea), inserts into sclera deep to the superior rectus muscle .
Trochlear nerve (CN IV)
Depresses, abducts)
Inferior oblique (IO)
Anterior part of floor of orbit
Sclera deep to lateral rectus muscle.
Occulomotor nerve (CN III)
Elevates, abducts
MBBS 0910 GROUP 2A1 7
CLINICAL ANATOMY OF CRANIAL NERVE III, IV &
VI
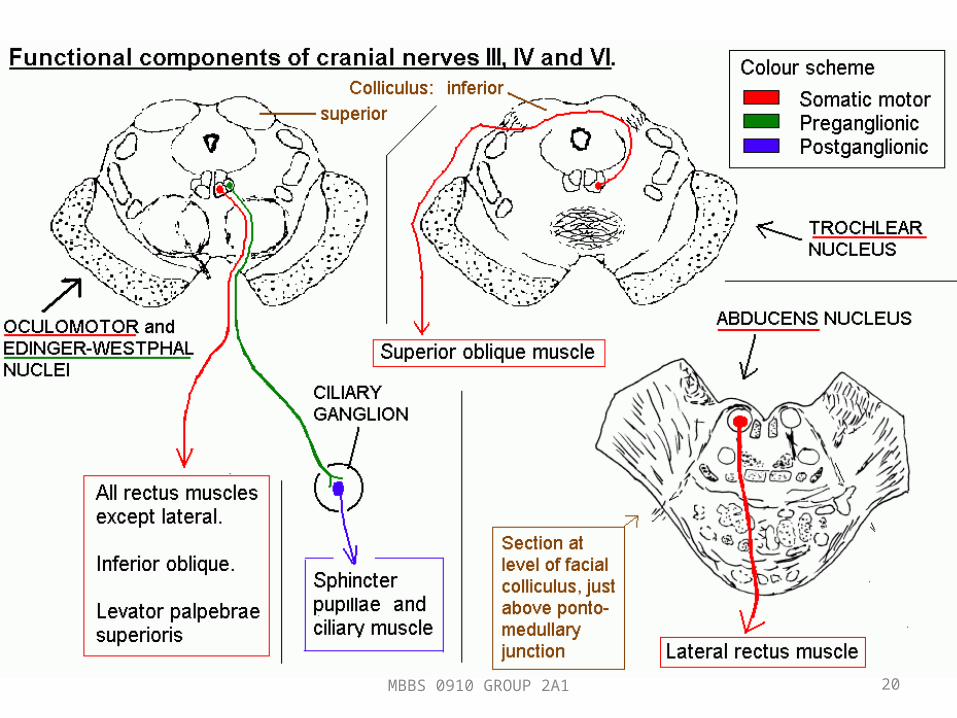
CRANIAL NERVE III (OCULOMOTOR)
• Entirely MOTOR in function.• Has two motor nuclei
1. Main motor nucleus2. Accessory parasympathetic nucleus
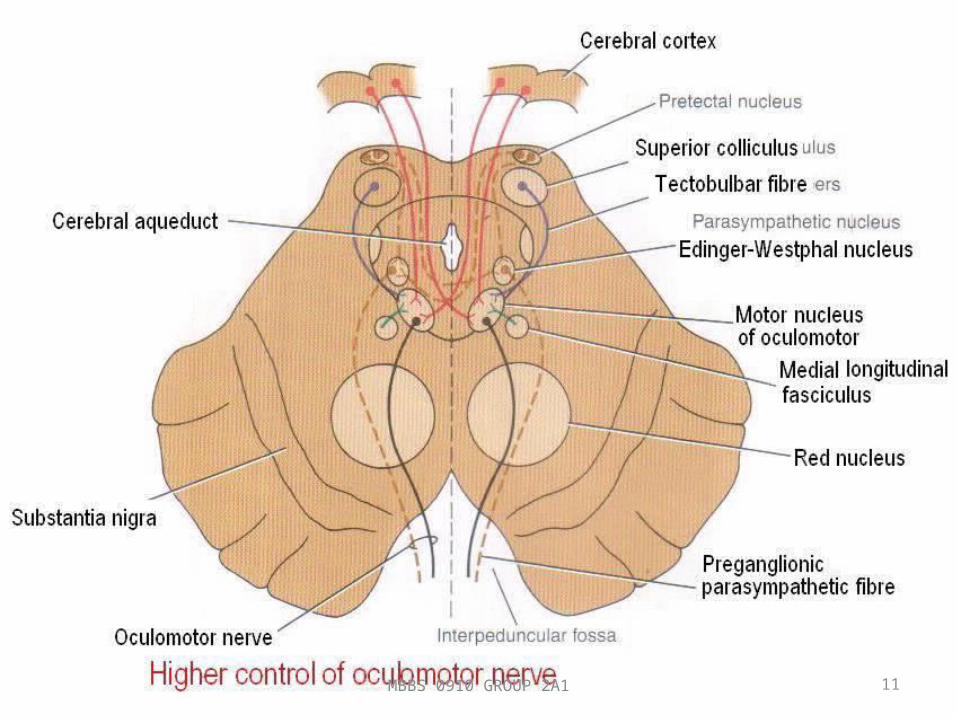
• Main motor nucleus located at anterior part of gray matter surrounding the cerebral aqueduct of the midbrain
• Lies at the level of superior colliculus• Supply ALL extrinsic muscle of the eye EXCEPT superior oblique
& lateral rectus.• Outgoing nerve emerge at interpeduncular fossa• The accessory parasympathetic nucleus (Edinger – Westphal
nucleus) is situated posterior to the main oculomotor nucleus.
MBBS 0910 GROUP 2A1 9
• Preganglion axon accompanied the oculomotor fibers then synapse in ciliary ganglion
• Postganglionic fibers pass through short ciliary nerves to constrictor pupillae of the iris & the ciliary muscles.
• Received fiber – From corticonucleus : accomodation reflex– From pretectal nucleus : direct & consensual light
reflex.
MBBS 0910 GROUP 2A1 10
MBBS 0910 GROUP 2A1 11
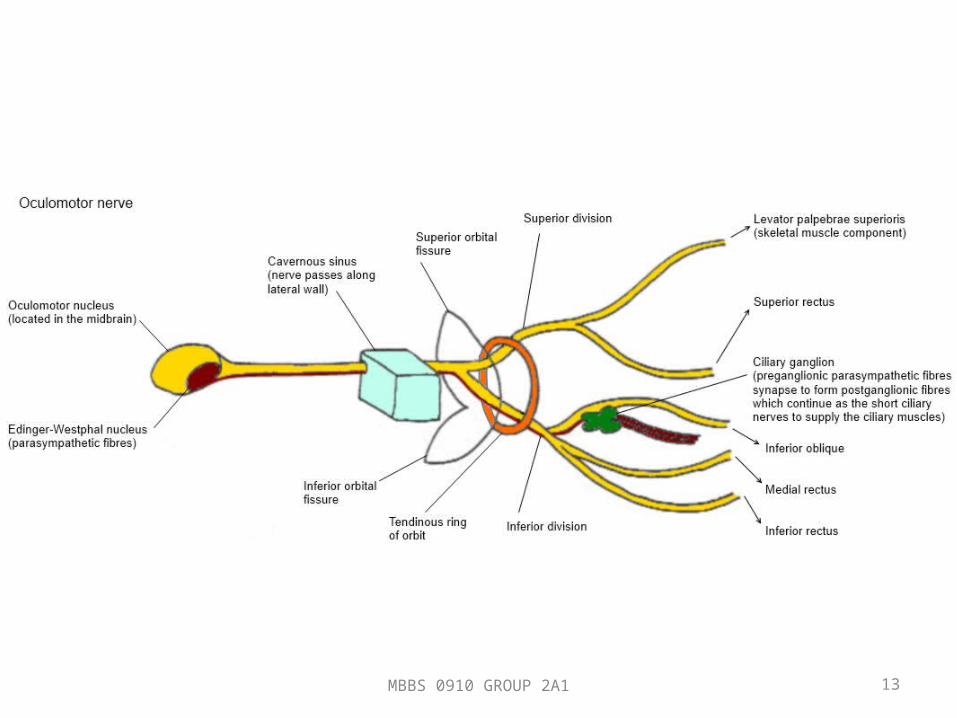
• Supplies extrinsic muscle of the eye: levator palpebrae superioris, superior rectus, medial and inferior rectus & inferior oblique.
• Also supplies intrinsic muscles: the constrictor pupillae of the iris & ciliary muscle.
• Responsible for:– Lifting upper eyelid– Turning the eye upward, downward & medially– Constricting pupil– Accommodating the eye
MBBS 0910 GROUP 2A1 12
MBBS 0910 GROUP 2A1 13
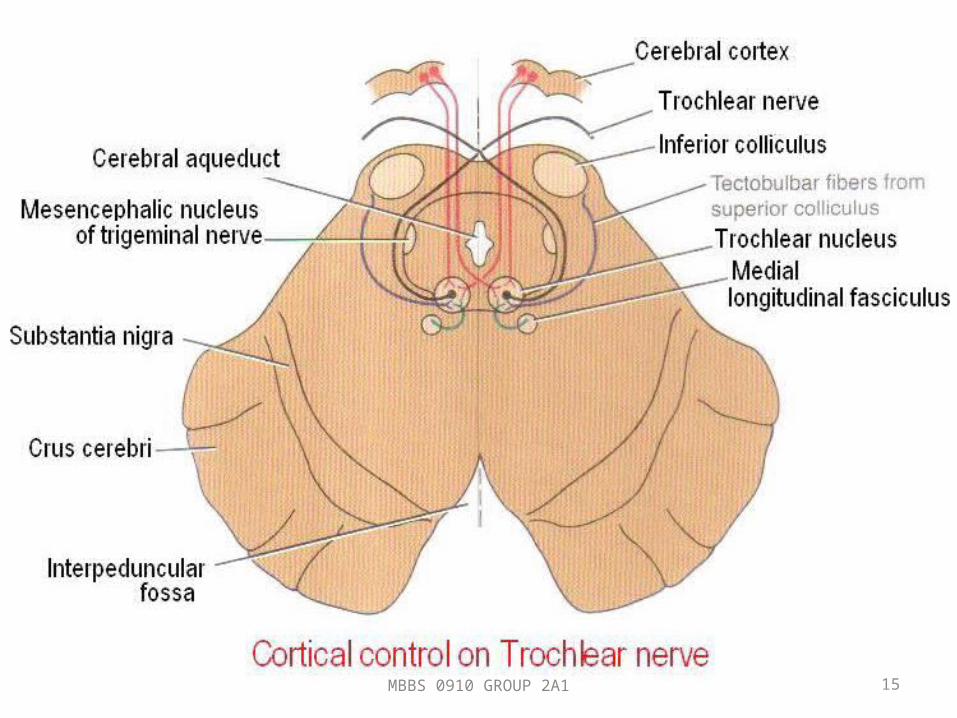
CRANIAL NERVE IV (TROCHLEAR)
• Entirely MOTOR in function.• Located at anterior part of gray matter surrounding the cerebral
aqueduct of the midbrain• Inferior to ocular motor nucleus at level of inferior colliculus• Leave the posterior surface of brainstem, emerges from
midbrain & decussates with the nerve of the opposite site.• Responsible for turning the eye downward & laterally
MBBS 0910 GROUP 2A1 14
MBBS 0910 GROUP 2A1 15

MBBS 0910 GROUP 2A1 16
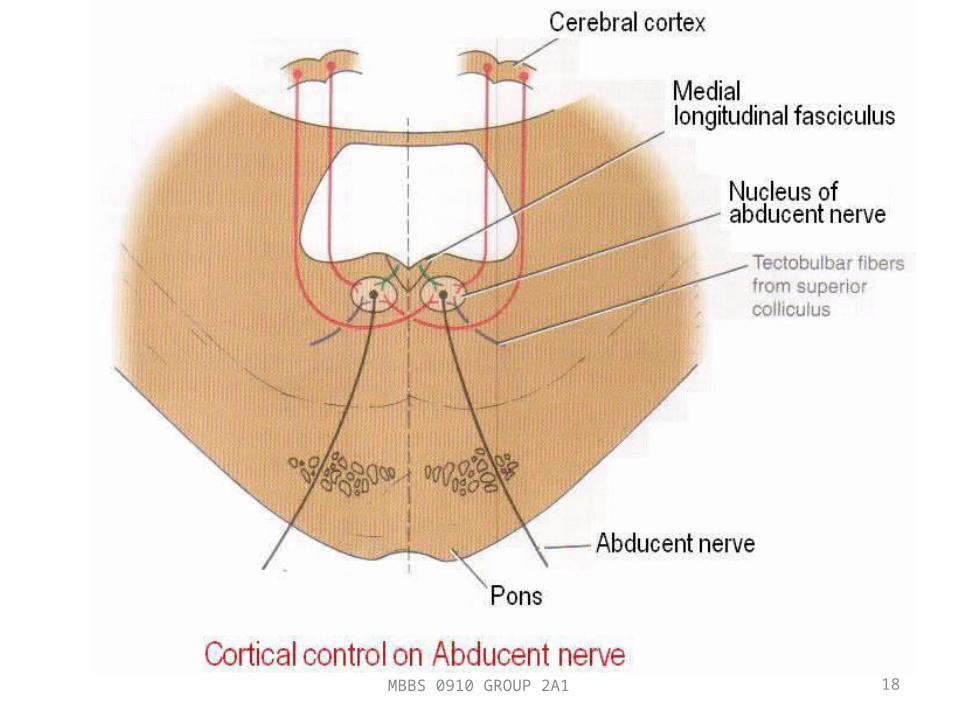
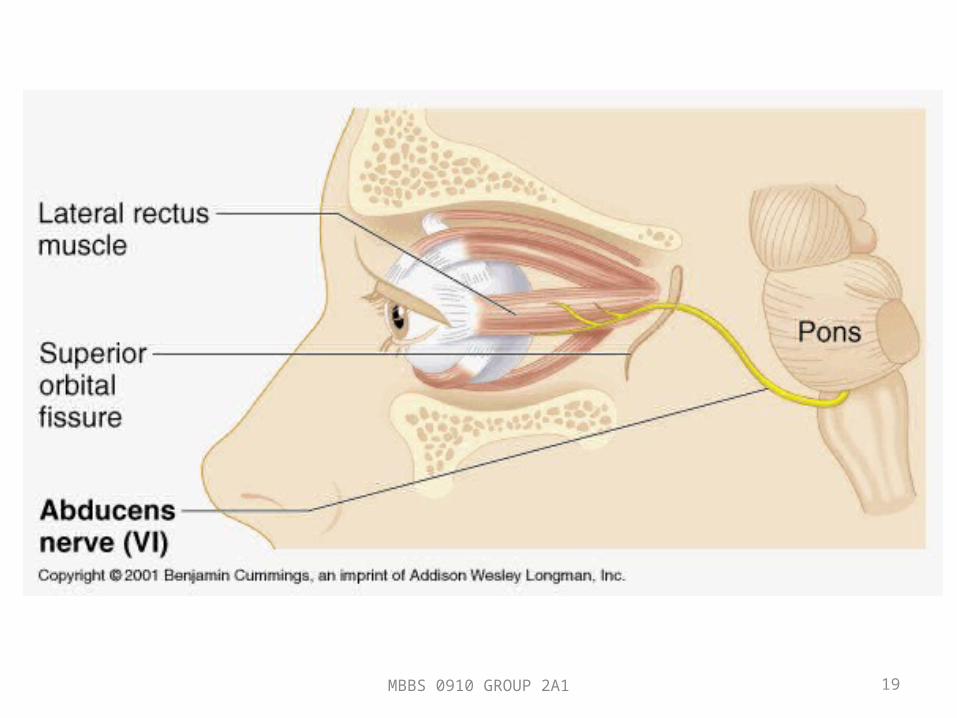
CRANIAL NERVE VI (ABDUCENT)
• Small motor nerve supplies the lateral rectus muscle.• Its nucleus situated beneath the floor of the upper part of 4th
ventricle, close to midline & beneath colliculus facialis.• Pass anteriorly through pons & emerge in the groove between
lower border of pons & medulla.• Entirely MOTOR• Responsible for turning the eye laterally.
MBBS 0910 GROUP 2A1 17
MBBS 0910 GROUP 2A1 18
MBBS 0910 GROUP 2A1 19
MBBS 0910 GROUP 2A1 20
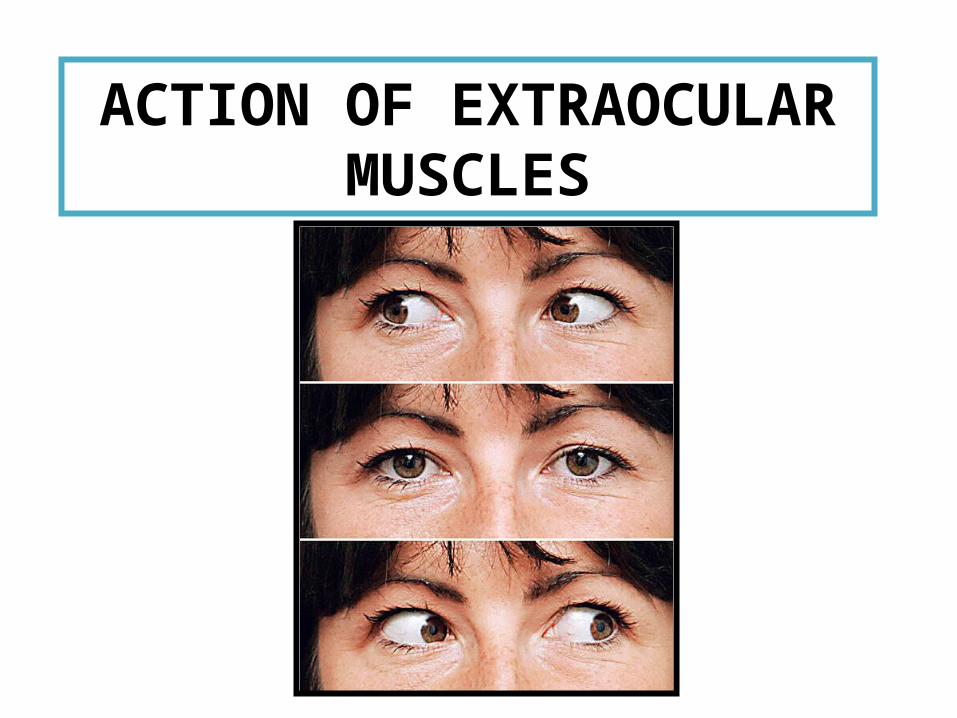
ACTION OF EXTRAOCULAR
MUSCLES
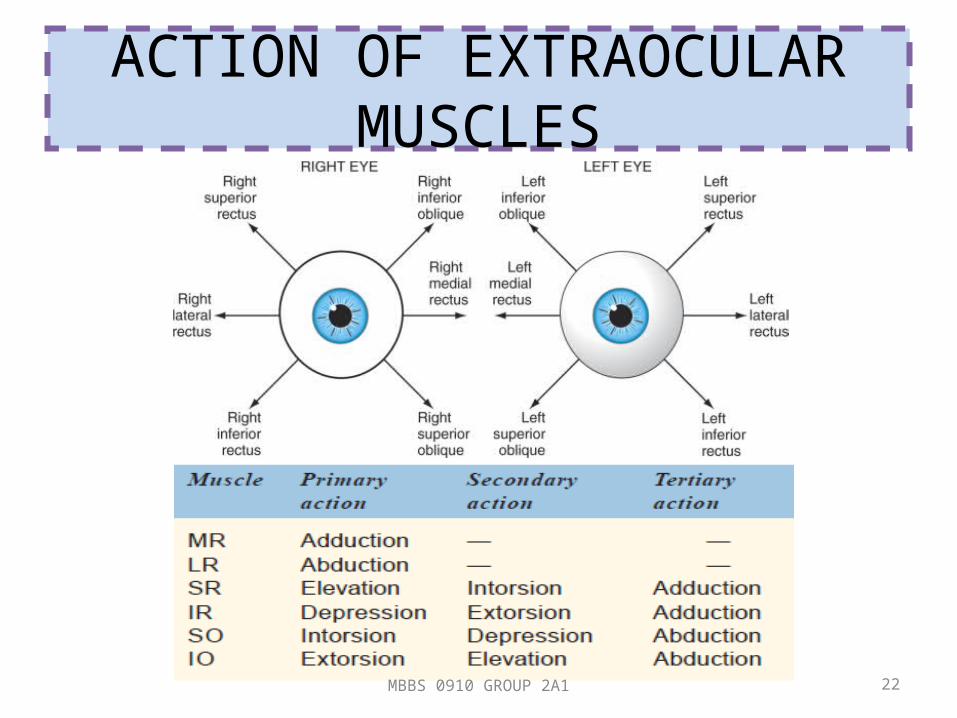
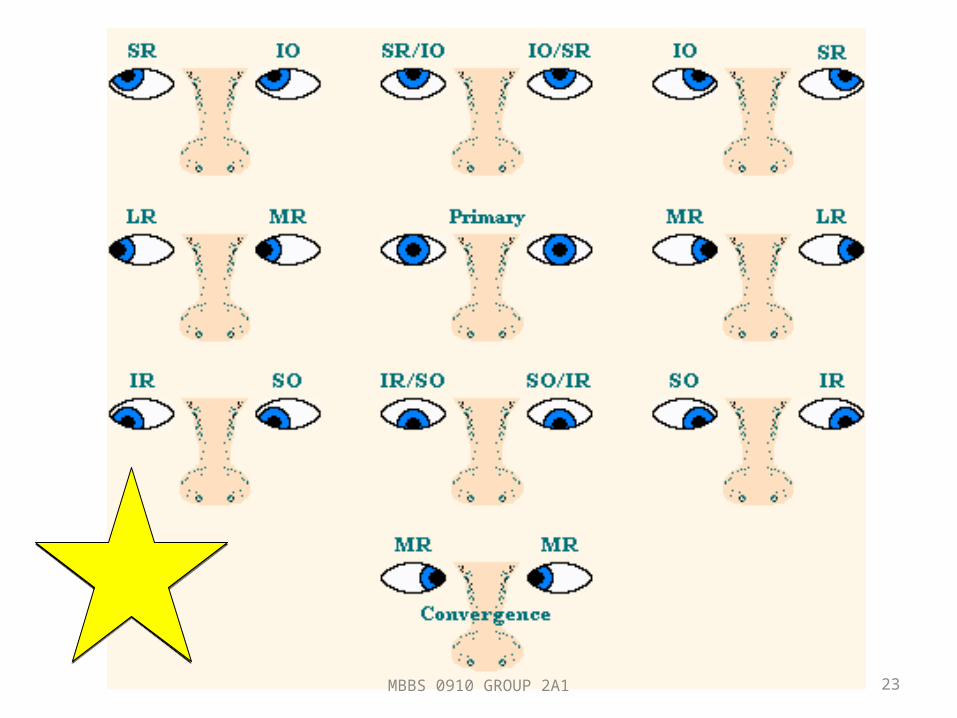
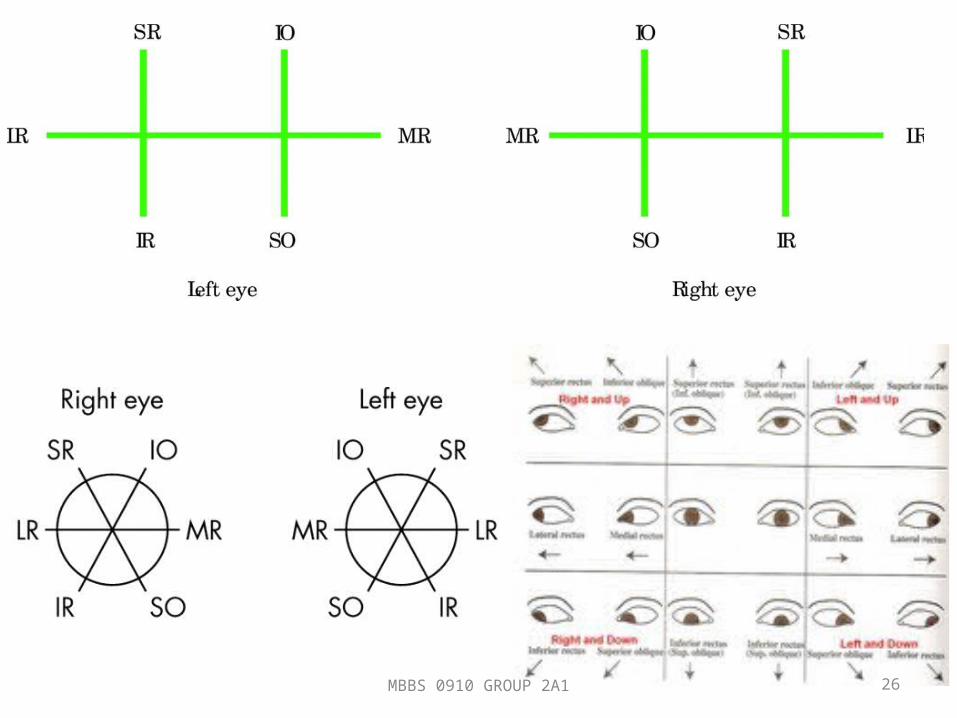
ACTION OF EXTRAOCULAR MUSCLES
MBBS 0910 GROUP 2A1 22
MBBS 0910 GROUP 2A1 23
OCULAR DEVIATION
EXTRAOCULAR MOVEMENT
1. Test by asking patient to follow finger movement directed in the full range of the normal muscle movement
2. Ask to look in all directions without moving their head and ask them if they experiences any double vision.
3. Test convergence movements by having the patient fixate on an object as it is moved slowly towards a point right between the patient's eyes.
4. Also, observe the eyes at rest to see if there are any abnormalities such as spontaneous nystagmus or dysconjugate gaze (eyes not both fixated on the same point) resulting in diplopia .
MBBS 0910 GROUP 2A1 25
MBBS 0910 GROUP 2A1 26
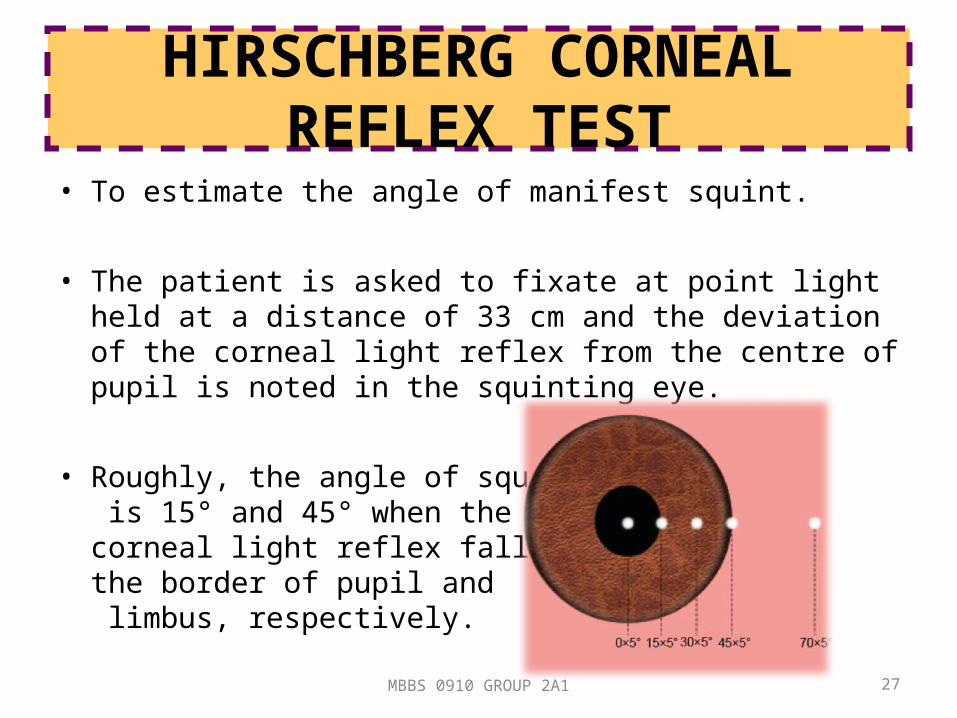
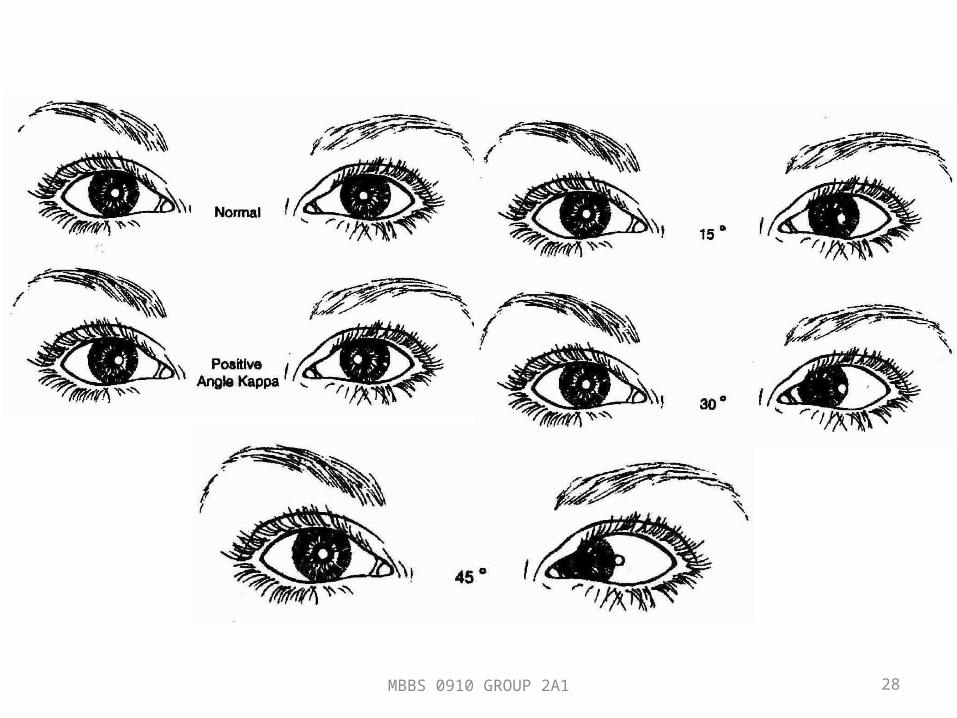
HIRSCHBERG CORNEAL REFLEX TEST
• To estimate the angle of manifest squint.
• The patient is asked to fixate at point light held at a distance of 33 cm and the deviation of the corneal light reflex from the centre of pupil is noted in the squinting eye.
• Roughly, the angle of squint is 15° and 45° when the corneal light reflex falls on the border of pupil and limbus, respectively.
MBBS 0910 GROUP 2A1 27
MBBS 0910 GROUP 2A1 28
CRANIAL NERVE PALSIES

SO4, LR6, the rest is 3
OCULOMOTOR NERVE PALSY (ALL 3)
• Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae superioris, ciliary muscle, and iris sphincter.
• Clinical features:
1. Ptosis due to paralysis of the LPS muscle.
2. Deviation. Eyeball is turned down, out and slightly intorted due to actions of the lateral rectus and superior oblique muscles.
3. Ocular movements are restricted in all the directions except outward.
4. Pupil is fixed and dilated due to paralysis of the sphincter pupillae muscle.
5. Accommodation is completely lost due to paralysis of the ciliary muscle.
6. Crossed diplopia is elicited on raising the eyelid.
7. Head posture may be changed if pupillary area remains uncovered.
MBBS 0910 GROUP 2A1 31
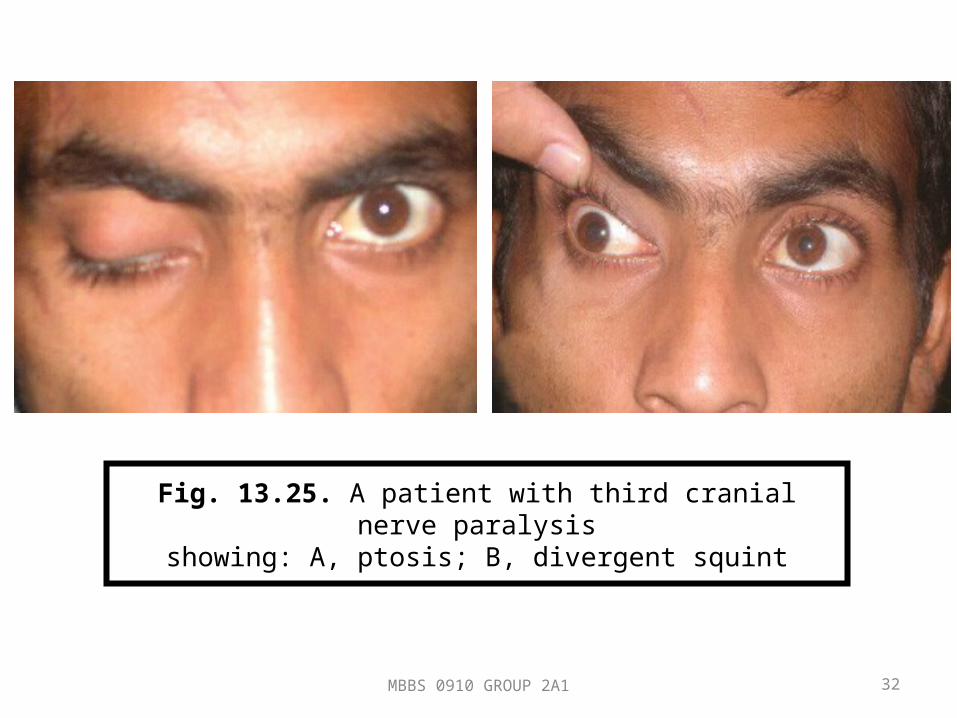
Fig. 13.25. A patient with third cranial nerve paralysisshowing: A, ptosis; B, divergent squint
MBBS 0910 GROUP 2A1 32

MBBS 0910 GROUP 2A1 33

CAUSES• Causes of 3rd nerve palsy:
– Diabetes mellitus type II– Atherosclerosis – Head injury– Aneurysm of the
posterior communicating artery
– Cavernous sinus thrombosis
– Space occupying lesion especially in the midbrain
– Multiple sclerosis
PROGNOSIS• Fortunately, nearly all
patients undergo spontaneous remission of the palsy, usually within 6-8 weeks.
• Medical management is actually watchful waiting, since there is no direct medical treatment that alters the course of the disease.
MBBS 0910 GROUP 2A1 34
MANAGEMENT
• Treatment during the symptomatic interval is by alleviating symptoms, mainly pain and diplopia.
• Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line treatment of choice for the pain. Diplopia is not a problem when ptosis occludes the involved eye.
• When diplopia is from large-angle divergence of the visual axes, patching one eye is the only practical short-term solution. When the angle of deviation is smaller, fusion in primary position often can be achieved using horizontal or vertical prism or both.
MBBS 0910 GROUP 2A1 35
TROCHLEAR NERVE PALSY (SO4)
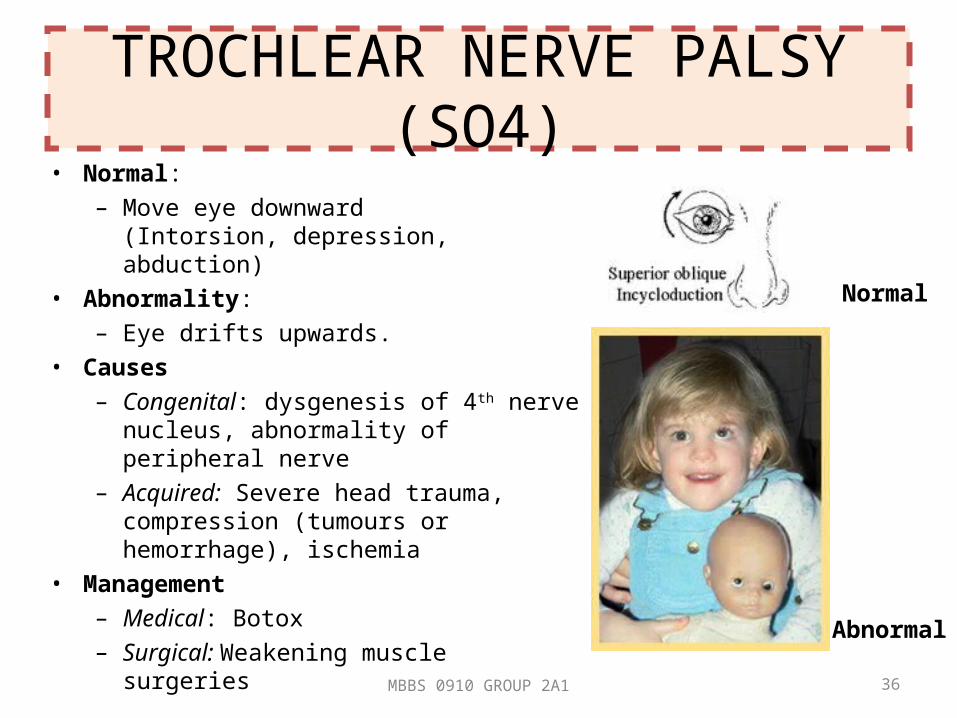
• Normal:– Move eye downward
(Intorsion, depression, abduction)• Abnormality:
– Eye drifts upwards. • Causes
– Congenital: dysgenesis of 4th nerve nucleus, abnormality of peripheral nerve
– Acquired: Severe head trauma, compression (tumours or hemorrhage), ischemia
• Management– Medical: Botox– Surgical: Weakening muscle surgeries Abnormal
Normal
MBBS 0910 GROUP 2A1 36
ABDUCENS NERVE PALSY (LR6)
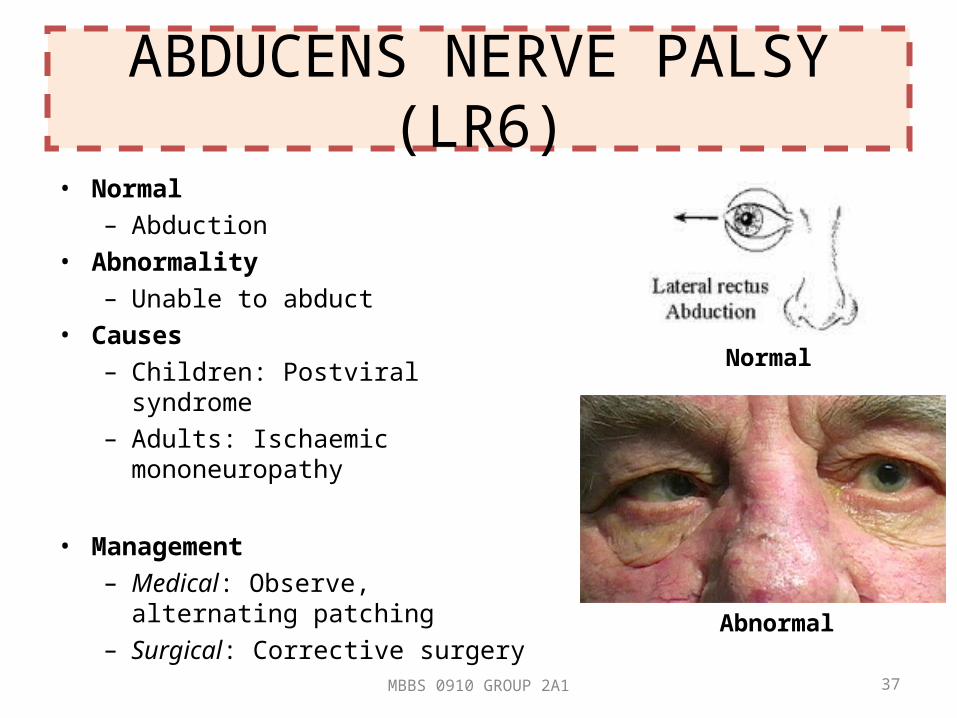
• Normal– Abduction
• Abnormality– Unable to abduct
• Causes– Children: Postviral syndrome– Adults: Ischaemic mononeuropathy
• Management– Medical: Observe, alternating
patching – Surgical: Corrective surgery
Abnormal
Normal
MBBS 0910 GROUP 2A1 37

VISUAL PATHWAY
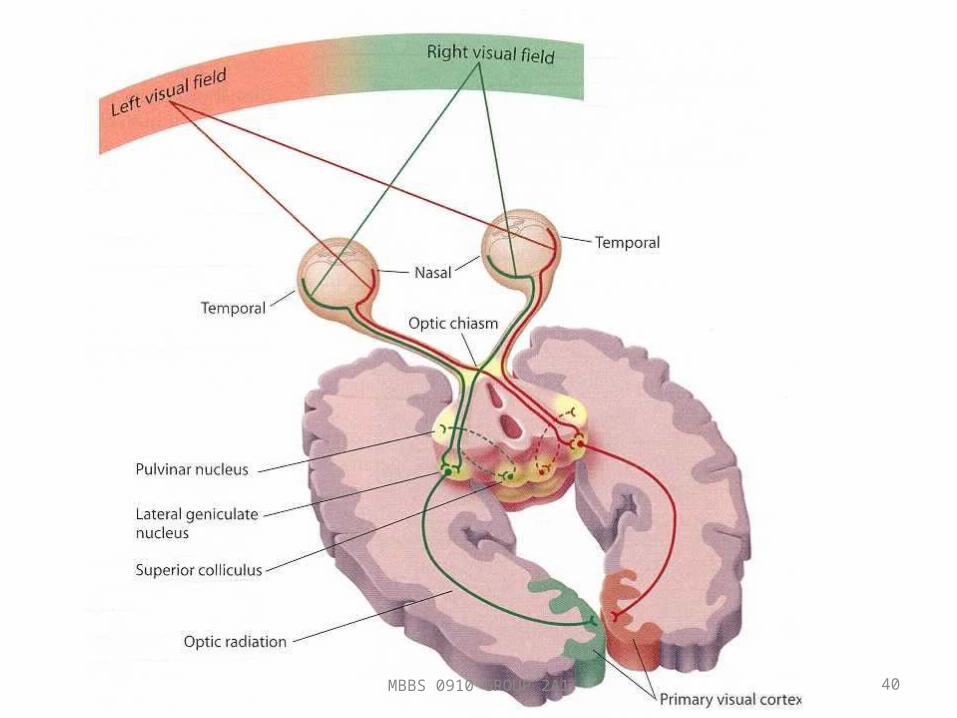
FORMED BY
1) Retina
2) Optic nerves
3) Optic chiasma
4) Optic tracts
5) Lateral geniculate bodies
6) Optic radiations
7) Visual cortex
MBBS 0910 GROUP 2A1 39
MBBS 0910 GROUP 2A1 40
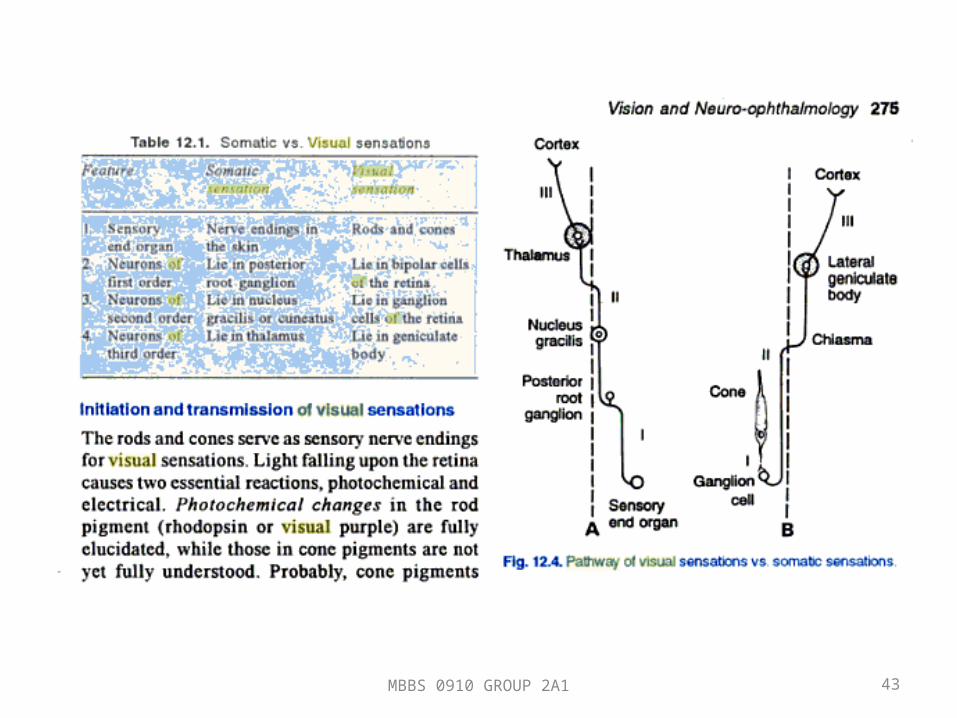
1. Optic nerves– It is a backward continuation of nerve fiber layer of the retina– Consists of axons, afferent fibers– Does not regenerate as it is not covered by neurilemma– Very fine (about 2-10 um), 47-50 mm in length;
• Intraocular part – (1 mm) passes through sclera as lamina cribrosa and finally appear as optic disc
• Intraorbital part – (30 mm) slightly sinous part as to allow eye movements. From back of the eyeball to the optic foramina. Posteriorly, it is closely surrounded by annulus of zinn and origin of 4 rectus muscles. Some fibers of superior rectus muscle adhere here, which account to painful ocular movement in retrobulbal neuritis.
MBBS 0910 GROUP 2A1 41
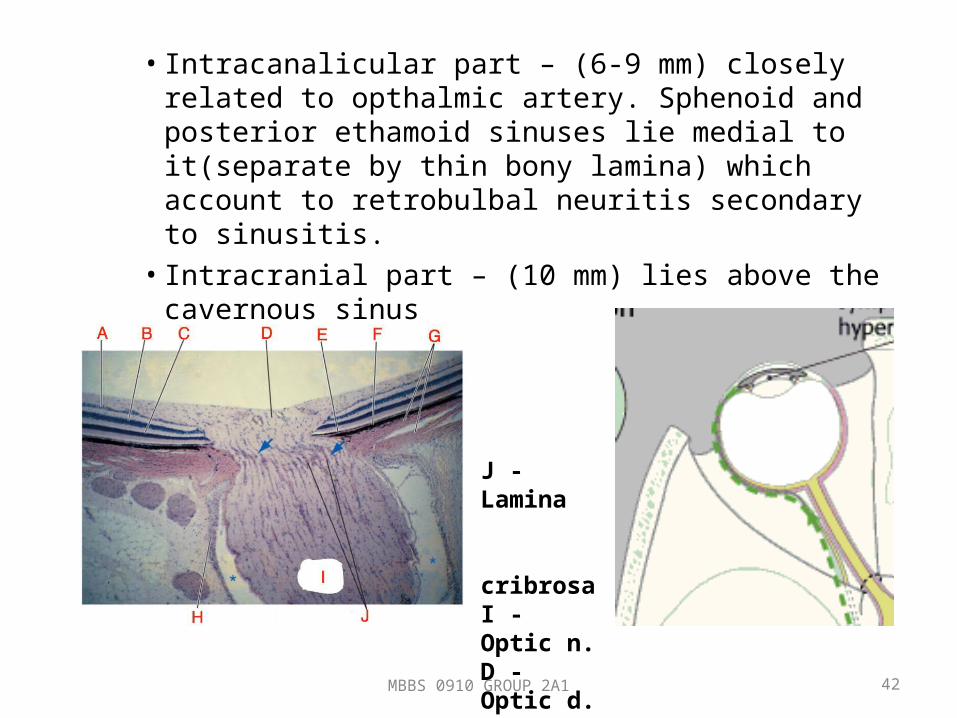
• Intracanalicular part – (6-9 mm) closely related to opthalmic artery. Sphenoid and posterior ethamoid sinuses lie medial to it(separate by thin bony lamina) which account to retrobulbal neuritis secondary to sinusitis.• Intracranial part – (10 mm) lies above the cavernous
sinus
MBBS 0910 GROUP 2A1 42
J - Lamina cribrosaI - Optic n.D - Optic d.G - Sclera
MBBS 0910 GROUP 2A1 43
2. Optic chiasma– 12 mm horizontally, 8 mm anteriorposteriorly– Lies below pituitary gland
2. Optic tract– Are cylindrical bundles of nerve fibers– Each optic tract consist of nerve fibers from same side
of temporal half and opposite side of nasal half
3. Lateral geniculate body– Each consist of 6 layers of neurons– The fibers of second order neurons coming via optic
tracts relay in these neurons
MBBS 0910 GROUP 2A1 44
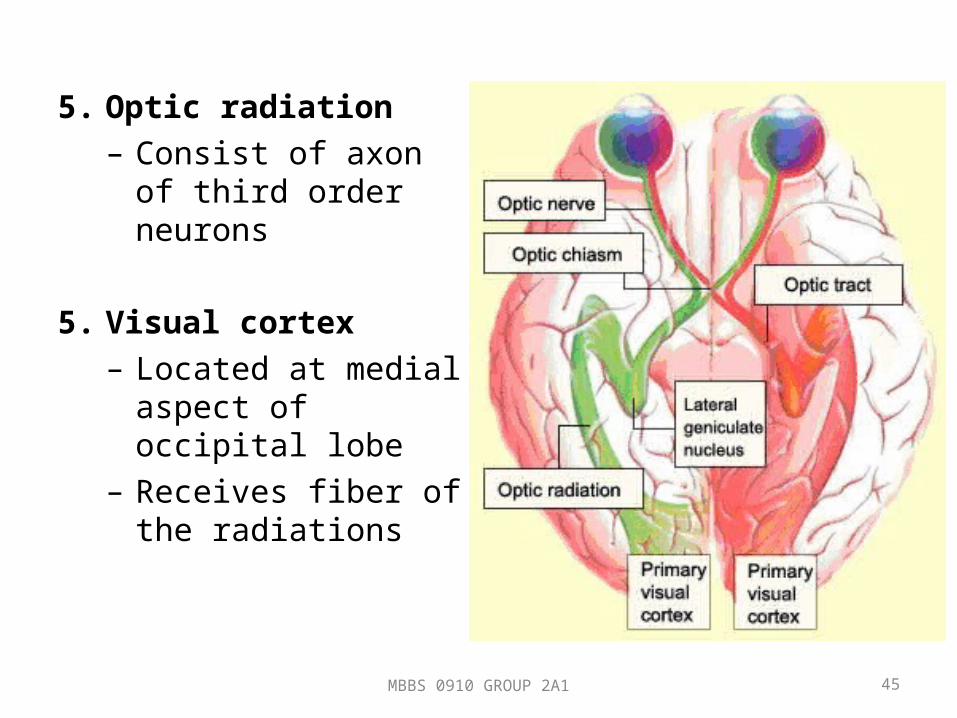
5. Optic radiation– Consist of axon of third
order neurons
5. Visual cortex– Located at medial
aspect of occipital lobe– Receives fiber of the
radiations
MBBS 0910 GROUP 2A1 45

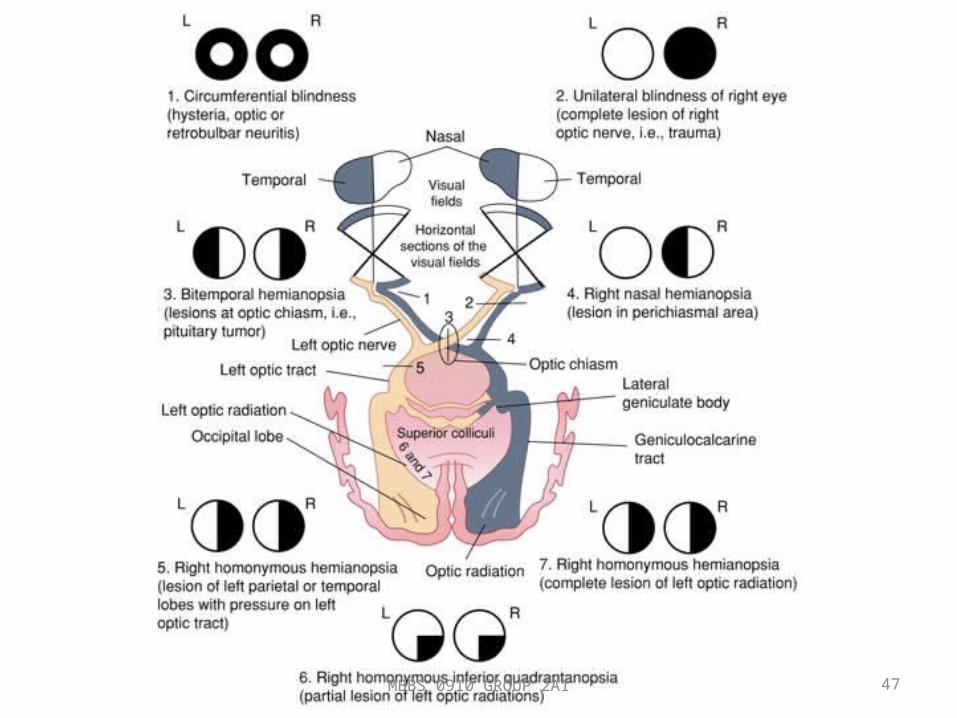
VISUAL FIELD DEFECT
MBBS 0910 GROUP 2A1 46
MBBS 0910 GROUP 2A1 47
LIGHT REFLEX PATHWAY
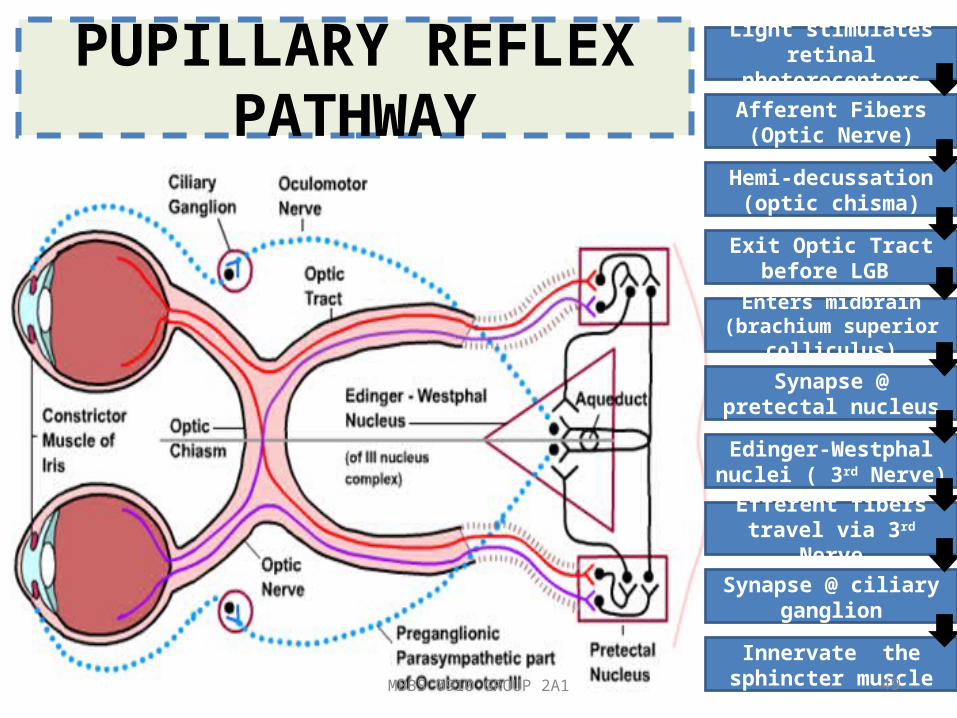
PUPILLARY REFLEX PATHWAY
Light stimulates retinal photoreceptors
Afferent Fibers (Optic Nerve)
Hemi-decussation (optic chisma)
Exit Optic Tract before LGB
Enters midbrain (brachium superior colliculus)
Synapse @ pretectal nucleus
Edinger-Westphal nuclei ( 3rd Nerve)
Efferent fibers travel via 3rd Nerve
Synapse @ ciliary ganglion
Innervate the sphincter muscleMBBS 0910 GROUP 2A1 49
MBBS 0910 GROUP 2A1 50