neuroimmunology
TRANSCRIPT

NEURO IMMUNOLOGY
Susanth MJ

NORMAL FUNCTIONS OF THE IMMUNE SYSTEM
Protect the organism against infectious agents and
prevent reinfection by maintaining immunological
memory
Wound healing
Tumor surveillance

FUNCTIONAL DIVISIONS OF IMMUNE SYSTEM
Innate Immune System
body's first line of defense against pathogens
acts nonspecifically
Adaptive Immune System
secondary, antigen-specific response
mediated by T cells and B cells

COMPONENTS OF INNATE IMMUNE SYSTEM
Skin
Phagocytes
include polymorphonuclear cells, monocytes, and
macrophages
Natural killer (NK) cells
Acute-phase proteins - C-reactive protein
Complement system

COMPONENTS OF ADAPTIVE IMMUNE SYSTEM
B cells
T cells or thymus-derived cells
CD4 T cells
CD8 T cells
Antibodies (Immunoglobulins (Igs)
APCs
macrophages, monocytes, dendritic cells, and
Langerhans cells.

CELLS OF THE IMMUNE SYSTEM
PluripotentStem Cells In
The Bone Marrow
Myeloid Lineage
Neutrophils
Basophils
Eosinophils
Macrophages
Lymphoid Lineage
T Cells
B Cells
NK Cells
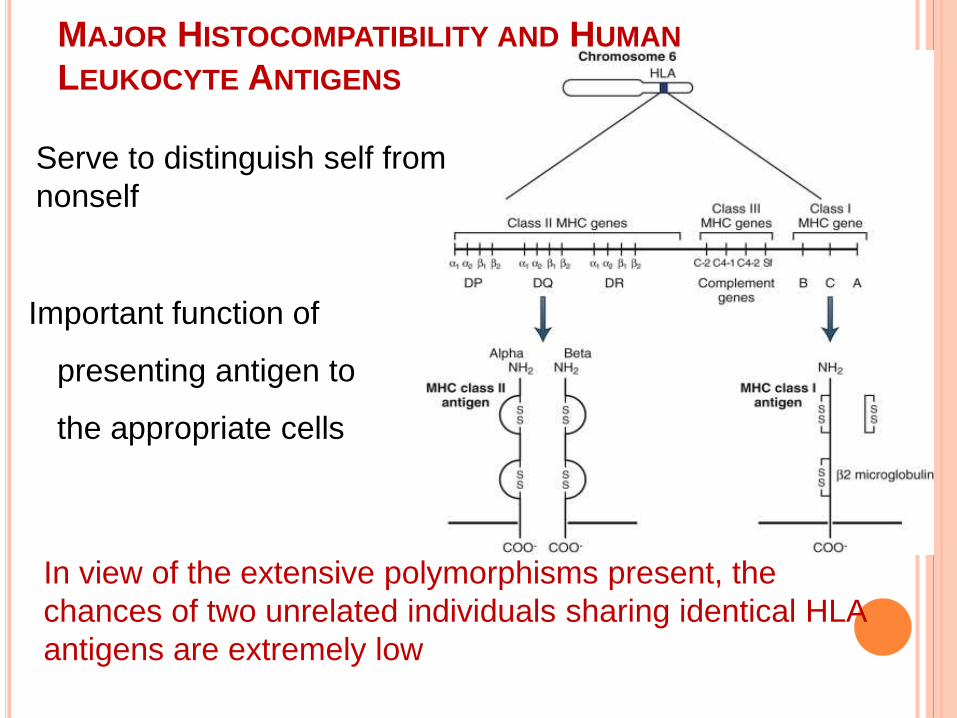
MAJOR HISTOCOMPATIBILITY AND HUMAN
LEUKOCYTE ANTIGENS
Important function of
presenting antigen to
the appropriate cells
In view of the extensive polymorphisms present, the
chances of two unrelated individuals sharing identical HLA
antigens are extremely low
Serve to distinguish self from
nonself
MHC CLASS I ANTIGENS
Expressed on all nucleated cells
Includes HLA-A, B, and C
Regulate the specificity of cytotoxic CD8 + T cells
MHC CLASS II ANTIGENS
Constitutively expressed on dendritic cells,
macrophages, and B cells
On activation expressed on T cells, endothelial
cells, and astrocytes
Includes HLA-DP, DQ, and DR
Regulate the specificity of CD 4 T-helper cells,
which in turn regulate DTH and antibody response
to foreign antigens
APCS
required to present antigen to T cells
macrophages, monocytes, dendritic cells, and
Langerhans cells
found primarily in the skin, lymph nodes, spleen,
and thymus
process antigen intracellularly and present antigen
peptide in the groove of their MHC class II
molecules

MONOCYTES AND MACROPHAGES
4% of the peripheral blood leukocytes
abundant cytoplasm and a kidney-shaped nucleus
Monocytes differentiate into tissue-specific
macrophages including Kupffer cells of the liver and
brain microglia

NATURAL KILLER CELLS
2.5% of peripheral blood lymphocytes
Large intracytoplasmic azurophilic granules and high
cytoplasm-to-nucleus ratio
Activated primarily in response to interferons
Involved in
Elimination of virally infected host cells
Tumor immunity
Lack immunological memory
Lack the cell surface markers present on B cells and T
cells

T LYMPHOCYTES
Originate from the thymus
respond to peptide antigens only
CD4 + T cells (T-helper (T H) cells )
expressing CD4 antigen on their cell surface
CD8 + T cells (cytotoxic T cells)
expressing CD8 on their surface
Suppressor or regulator T cells
Can express either CD4 or CD8.
Most abundantly expressed antigen in T cells is CD45

CD4 T CELLS
Recognize antigen presented in association with
MHC class II on the surface of APCs
Promote B-cell maturation and antibody production
Produce factors called cytokines to enhance the
innate or nonspecific immune response
CD8 T CELLS
Recognize antigen in association with MHC class-I
antigen on the surface of most cells
Play an important role in eliminating virus-infected
cells
Damaging target cells via the release of degrading
enzymes and cytokines

T-CELL RECEPTORS
Heterodimer consisting of two
chains stabilized by interchain
and intrachain disulfide bonds
Associated with the CD3 antigen
to form the TCR complex
Can only recognize short peptides
that are associated with MHC
molecules

B LYMPHOCYTES
Switch to other isotypes, while maintaining antigen specificity
↓
Differentiate and form mature antibody-secreting plasma cells
Acquire Ig receptors
(normally IgM )
T-cell
help
Directly (cognate
interaction)
Indirectly by secreting helper factors
(noncognate interaction)
Bone marrow
Respond to proteins, peptides,
polysaccharides, nucleic acids, lipids,
and small chemicals

IMMUNOGLOBULINS
Glycoproteins that are the
secretory product of plasma cells
Each molecule consists of light
chains (kappa [κ] or lambda [λ])
linked to two identical heavy
chains
According to heavy chain, Igs
divided into five main classes:
IgM, IgD, IgG, IgA, and IgE
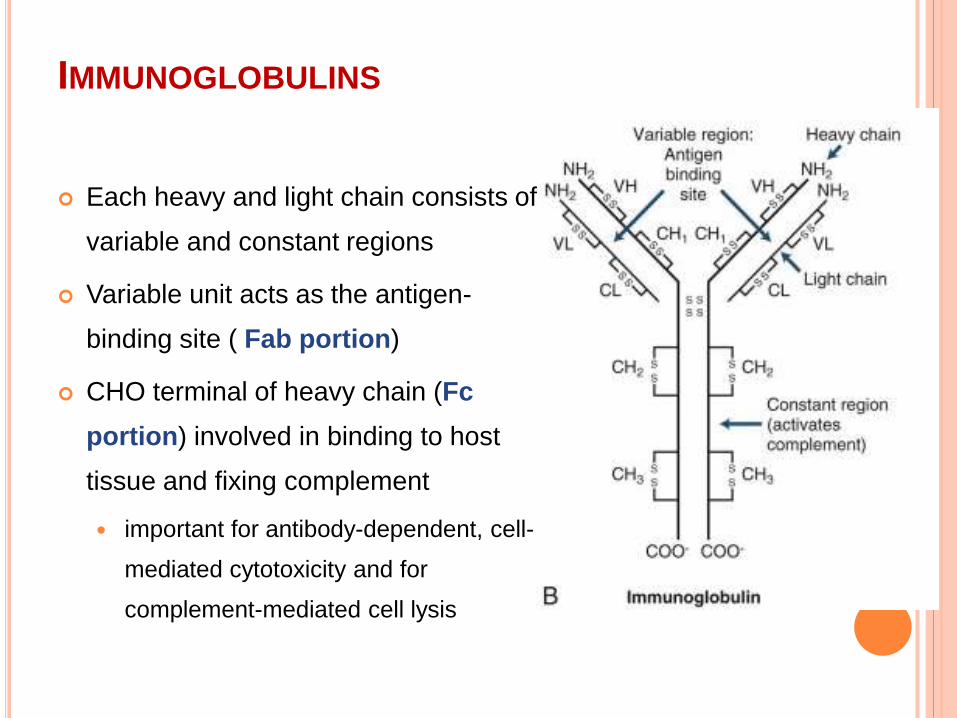
IMMUNOGLOBULINS
Each heavy and light chain consists of
variable and constant regions
Variable unit acts as the antigen-
binding site ( Fab portion)
CHO terminal of heavy chain (Fc
portion) involved in binding to host
tissue and fixing complement
important for antibody-dependent, cell-
mediated cytotoxicity and for
complement-mediated cell lysis

HOW DIVERSITY ACHIEVED
Diversity in variable (V) and joining (J) gene segments
of the antigen receptors
Affinity Maturation
Antigen ↔ B cells
↓
Undergo somatic mutations
↓
Increase the diversity and the
affinity of antigen binding
This phenomenon does not occur
in T cells
Isotype switching
Recombination of variable
region with new constant
region genes
↓
Other Ig types
1
2
3

HOW IT WORKSAntigens in the periphery
↓
Lymphatics or blood vessels
↓
Lymph nodes and spleen
APCs
Monocyte-macrophage
lineage and B cells
Processed intracellularly
Presented not as whole molecules but as highly
immunogenic peptides
T cells
Proliferation
Cytokine production

MOLECULES ACTIVE IN IMMUNE PROCESS
APCs
Site of antigen
presentation
Chemokines
chemoattractant peptides that regulate
leukocyte migration
Integrins
includes VCAM-1, ICAM-1,
LFA-3, CD45, and CD2
Mediates adhesion to
endothelial cells and guiding
cell traffic
L-selectins
Facilitate the rolling of leucocytes
along the surface of endothelial
cells
Function as a homing receptor to
target organs
MMPs
Proteinases secreted by inflammatory cells
digest extracellular matrix, thereby facilitating lymphocyte
entry through basement membranes including the blood-
brain barrier (BBB)
APCs APCs

ACCESSORY MOLECULES FOR T-CELL ACTIVATION
CD3
Part of the TCR complex
CD4 and CD8
Binds to MHC
class II β chainBinds to MHC
class I molecule
Accessory role in
signaling and antigen
recognition

COSTIMULATORY MOLECULES
“Second signal” to facilitate T-cell activation
Stimulatory (positive)
B7-CD28, CD40-CD154 pathways
critical for T-cell activation
Inhibitory (negative) signal
B7-CTLA4 and PD1-PD ligand

B-CELL ACTIVATION
Activation of transcription factors (c-Fos, JunB, NFκB, and c-Myc)
↓
Promote proliferation and Igsecretion
T cell dependent
Responding to peptide
antigens
T cell independent
Respond to Nonprotein
antigensCytokines from T-
helper
Induce isotype
switching
Stronger and long-
lived memory B
cells
Weak IgM
responses

INTERACTION BETWEEN B CELLS AND T-HELPER
(CD4 +) CELLS
Requires expression of MHC class II by B cells and
is antigen dependent
Occurs in the peripheral lymphoid organs
Generation of high-affinity antibody-producing B
cells and memory B cells in the germinal center of
lymphoid follicles (Affinity Maturation)
B cells T cells B7 ↔ CD28
CD40 ↔ CD154

REGULATION OF THE IMMUNE RESPONSE
Cytokines
A. Growth factors: IL-1, IL-2, IL-3, and IL-4 and
colony-stimulating factors
B. Activation factors : Interferons (α, β, and γ, which
are also antiviral)
C. Regulatory or cytotoxic factors : IL-10, IL-12, TGF-
β, Lymphotoxins, and TNF-α
D. Chemokines : IL-8, MIP-1α, and MIP-1β

CYTOKINES
IL-4 and B-cell differentiation factors
Differentiation and expansion of committed B cells to become
plasma cells
MacrophagesIL-1
T cells
IL-2 and IL-2 R •Clonal expansion of T cells
•Activation of NK cells
•Lysis of tumor cell targets
IFN-γ•Induce expression of MHC class I
and class II molecules on many
cell types including APCs
•Increases the T-cell response to
the antigen
IL-3
Hematopoietic stem cells

CYTOKINES
IFN-α and IFN-β
Both type I interferons
IFN-α by macrophages, whereas IFN-β by
fibroblasts
Inhibit viral replication
Inhibit the proliferation of lymphocytes
TGF-β
produced by T cells and macrophages
decrease cell proliferation
IL-10
Growth factor for B cells
Inhibits the production of IFN-γ
Antiinflammatory effects
CYTOKINES

CD4 + T-HELPER CELLS
T H3 cells
Secrete TGF-β
Inhibits proliferation of T cells
Inhibits activation of macrophages
T H1 cells
•IFN-γ, IL-2, and TNF-α
•Proinflammatory functions
•Mediate diseases such as MS
T H2 cells
•IL-4, IL-5, IL-6, IL-10, and IL-13
•Promote antibody production by B cells
•Enhance eosinophil functions
•Suppress cell-mediated immunity (CMI)
Cytokines of the T H1 type
may inhibit production of T H2
cytokines and vice versa

T H-17 CELLS
Subset of T cells that predominantly produce IL-17
Both T H1 and T H2 cytokines suppress the
development of T H17 cells
Facilitate the recruitment of neutrophils and
participate in the response to gram-negative
organism
May also play a role in the initiation of autoimmune
disease
SELF-TOLERANCE
An organism's ability to maintain a state of
unresponsiveness to its own antigens
Maintained through three principal mechanisms
Deletion, anergy, and suppression
Categorized as either central or peripheral
tolerance
Failure lead to autoimmune disorers

SELF-TOLERANCE
Central Tolerance
In Thymus
Positive selection
TCR with no affinity to MHC will fail to receive signals
needed for maturation and will die in situ
Low affinity to MHC survive and become MHC I (CD8 +)
or MHC II (CD4 +).
Negative selection
High affinity toward self-antigen are deleted by
apoptosis

SELF-TOLERANCE
Peripheral Tolerance
For Self-reactive lymphocytes that escape central
tolerance
Maintained through clonal anergy or clonal deletion
TERMINATION OF AN IMMUNE RESPONSE
B-Cell Inhibition
Antigen-antibody complexes through binding of the
Fc receptor to the CD32 (FcγRIIB) receptor on the
surface of the B cell.
Anti-idiotypic responses
Variable regions of the Ig and the TCR can act as
antigens (idiotopes)

TERMINATION OF AN IMMUNE RESPONSE
T Cell Inhibition
a) Anergy or functional unresponsiveness
occurs when there is insufficient T-cell activation
b) Apoptosis
Repeated stimulation may lead to activation-induced cell
death through
c) Suppressor cell activity
Notably by secretion of T H2 and T H3 cytokines
ANERGY DUE TO FAILURE OF T-CELL ACTIVATION
A. Absence of signal , T cell dies because of neglect
B. Absence of costimulatory signals, the T cell
becomes anergic
Up-regulates CTLA-4
CD80 and CD86 on the
surface of APCs
C. Activated T cell
APOPTOSIS
Withdrawal of growth factors
Cytokines
TNF-α and IFN-γ, IL-2
Complete absence of either of these cytokines results in
deficient T-cell apoptosis, inability to terminate the
immune response, and uncontrolled autoimmune
disease
Exposure to corticosteroids
Activation-Induced Cell Death (AICD)

APOPTOSIS
Activation-Induced Cell Death (AICD)
Repeated exposure to antigens
Induce apoptosis via the Fas/FasL pathway
Autoreactive T lymphocyte may encounter large
doses of self-antigen in the periphery and
consequently may be deleted by AICD
Mutations in the Fas gene associated with an
autoimmune disease

REGULATORY T CELLS
Can be of the CD4 + or CD8 +subtypes
Down-regulate CD4 and CD8 T-cell responses
action by production of immunosuppressive
cytokines (T H2 or TGF-β) or through T-T cell
interactions, including the expression of CTLA-4
Important role in the control of the immune
response in autoimmune disorders, and the
function of regulatory T cells may be enhanced by
immunomodulatory therapies.

IMMUNE SYSTEM AND CENTRAL NERVOUS
SYSTEM
Immunologically privileged site because of
(1) absence of lymphatic drainage, limiting the immunological
circulation
(2) blood-brain barrier (BBB), which limits the passage of
immune cells and factors
(3) low level of expression of MHC factors, particularly MHC II
in the resident cells of the CNS
(4) low levels of potent APCs, such as Dendritic or
Langerhans cells
(5) presence of immunosuppressive factors such as TGF-β
and CD200

Because of the lack of a lymphatic system, antigens
drain along perivascular spaces
T cells must be activated before crossing the BBB
Entry is facilitated by expression of receptors for adhesion
molecules, including α4-integrin.
Neurons express MHC class I only when damaged and
in the presence of IFN-γ
Expression of MHC antigens on both microglia and
astrocytes are enhanced by the presence of cytokines,
TNF-α, and IFN-γ
IMMUNE SYSTEM AND CENTRAL NERVOUS
SYSTEM

NEUROGLIAL CELLS AND THE IMMUNE RESPONSE
Microglia and Astrocytes
Participate in immune responses within the CNS
Central role in initiating and propagating immune-
mediated diseases of the CNS

MICROGLIA
derived from bone marrow cells during ontogeny
three principal types of cells: perivascular,
parenchymal, and Kolmer cells, in the choroid
plexus
Activated microglia
express higher levels of MHC class II
produce higher levels of proinflammatory cytokines
including TNF-α, IL-6, and IL-1, as well as nitric
oxide and glutamate
MICROGLIA
Primary functions are immune surveillance for foreign
antigens and phagocytic scavengers of cellular debris
Participate in antigen presentation within the CNS under
certain conditions esp perivascular microglia
Role in regulating the programmed elimination of neural
cells during brain development
Enhance neuronal survival by producing neurotrophic
and antiinflammatory cytokines
Role in neuroregeneration and repair
MICROGLIA
Overactivation of microglia, possibly by microbes or other
environmental factors
↓
Chronic proinflammatory milieu in the CNS
↓
Progressive neurodegeneration.
Deleterious role in several neurodegenerative diseases: MS,
ALS, Parkinson disease and HIV-associated dementia
Strategies to down-regulate such responses are under
investigation

ASTROCYTES
role in the glia limitans at the BBB
physical support of neuronal and axonal structures
an provision of growth factors
secrete cytokines including TGF-β
critical role in converting glutamate to glutamine (
less glutamate-mediated neurotoxicity)
produce stromal-derived factor-1 (SDF-1) -
significant role in HIV-associated dementia
REGULATION OF IMMUNITY IN CNS
TGF-β produced by astrocytes and microglia down-
regulating immune responses locally
TGF-β by Neurons facilitate the differentiation of
regulatory T cells
Increased expression of Fas ligand in the CNS
compared with PNS may increase apoptosis of T
cells

REGULATION OF IMMUNITY IN CNS
Neurons expressing CD200 inhibit activation of
microglia and macrophages
Neurons expressing Fractalkine (CXCL1)
Down-regulate microglial-mediated neurotoxicity (
Parkinson disease and ALS )
Increase NK cells play (inhibitory role in CNS
inflammation esp in MS)
IS BRAIN AN IMMUNOLOGICALLY SEQUESTERED
ORGAN ?
Cells of the CNS not only respond to inflammatory
stimuli but are also capable of producing cytokines
and other inflammatory factors, often directly under
the influence of lymphocytes and is closely involved
with the systemic immune response

NEURO AUTOIMMUNE DISEASE
Results as a culmination of interactions between genetic
predisposition, environmental factors, and failure of self-tolerance
maintenance mechanisms
B-cell mediated diseases
autoantigen present
MG - antibodies to the α subunit of the acetylcholine receptor
LES - antibodies targeting calcium channels
T cell–mediated diseases
Little evidence for autoantigen
MS, inflammatory demyelinating polyneuropathy, and
polymyositis

GENETIC FACTORS IN AUTOIMMUNE DISEASES
Association between certain MHC haplotypes and
disease
MS - HLA-DR2 allele
MG - HLA-DR3
Association may be due to the ability of a particular
MHC molecule to bind and present autoantigen to the T
cell
Disease linkage tends to be more with class II genes,
suggesting a key role for T-cell autoimmunity.
Many autoimmune diseases are more frequent in
females (estrogen's effects on the immune system )

ENVIRONMENTAL FACTORS IN AUTOIMMUNE
DISEASES
Molecular mimicry
environmental antigen resembling a self-antigen elicits
an immune response to both itself and the self-antigen
Streptococcal-induced chorea, Gd1b axonal neuropathy,
Semple rabies vaccine-induced encephalomyelitis, and
the anti-Hu paraneoplastic syndrome
MS - remote infection with EBV(epitopes of EBV
resemble MBP)

ENVIRONMENTAL FACTORS IN AUTOIMMUNE
DISEASES
Epitope spreading
Once an inflammatory reaction proceeds
↓
Tissue injury expose other self-antigens that were previously
unrecognized by the immune system
↓
For unknown reasons, peripheral tolerance mechanisms fail, and
an autoimmune reaction ensues
↓
Perpetuating immune-mediated reactions and causing chronic
diseases
ENVIRONMENTAL FACTORS IN AUTOIMMUNE
DISEASES
Therapies that inhibit molecular mimicry or epitope
spreading may be useful in preventing autoimmune
diseases

MULTIPLE SCLEROSIS
Increased incidence with
HLA-DR2 (DR1501) haplotype
single nucleotide polymorphism of IL-2R and IL-7R
alleles
Inverse association between sunlight exposure and
MS
active form of vitamin D, calcitriol down-regulate
proinflammatory dendritic cells (DC) and reduce T H1
lymphocyte responses while promoting antiinflammatory
T H2 lymphocyte responses
MULTIPLE SCLEROSIS
No clear autoantigen
Immune-mediated disease rather than an autoimmune
disease
Cell-mediated immunity, primarily involving T-helper
cells, is believed to play an important role in initiating the
disease
Oligoclonal bands are commonly observed; however,
the target of these antibodies has yet to be elucidated
Activated microglia are found in progressive forms of the
disease and have been associated with axonal damage
and demyelination

IMMUNOPATHOGENESIS OF MS
Activation of MBP-reactive T cells predominantly T H1 via molecular
mimicry or by a superantigen presumably in the periphery
↓ VCAM-1 and its ligand, VLA-4
Cross the BBB
Reactivated T cells in the CNS
Perivascular dendritic-like cells have been shown to play a role
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage Induce B-cell activation and antibody
production that further damage myelin

IMMUNO PHARMACOTHERAPY OF MS
Activation of periperal T cells
↓ VCAM-1 and its ligand, VLA-4
Cross the BBB
↓
Reactivated T cells in the CNS
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage
B-cell activation
β-Interferon (IFN-β) •↑ IL-10 by macrophages
•↓ IL-12 by dendritic cells
•modulates adhesion molecule
expression
•↓ costimulatory molecule
expression

IMMUNO PHARMACOTHERAPY OF MS
Activation of periperal T cells
↓ VCAM-1 and its ligand, VLA-4
Cross the BBB
↓
Reactivated T cells in the CNS
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage
B-cell activation
Glatiramer acetate (GA)•bind with high affinity to the MHC
groove, leading to the generation
of GA-specific T cells
•display a T H2 bias
•down-regulation of the immune
responses

IMMUNO PHARMACOTHERAPY OF MS
Activation of periperal T cells
↓ VCAM-1
Cross the BBB
↓
Reactivated T cells in the CNS
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage
Campath-1H (Phase 2
studies)
•targets CD52 receptor
present on lymphocytes
and monocytes
•depletion of peripheral
lymphocytes
Daclizumab
•blocks the IL-2R α chain
(CD25) on T cells
•inhibits T-cell replication

IMMUNO PHARMACOTHERAPY OF MS
Activation of periperal T cells
↓ VCAM-1
Cross the BBB
↓
Reactivated T cells in the CNS
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage
CTLA4 Ig
•blocks B7-CD28
costimulatory signals on T
cells
•induce T-cell anergy in
vivo
Fingolimod•Targets sphingosine-1-
phosphate receptor, which
is necessary for
lymphocyte egress from
lymph nodes

IMMUNO PHARMACOTHERAPY OF MS
Activation of periperal T cells
↓ VCAM-1 and its ligand, VLA-4
Cross the BBB
↓
Reactivated T cells in the CNS
↓
IL-2, IFN-γ, NO and TNF-α
↓
Myelin damage
NatalizumabVLA-4 (α4β1-integrin) antibody
B-cell activation
Rituximab
antibody that primarily
targets activated B cells

Nonspecific strategies
Cyclophosphamide, Mitoxantrone, and Cladribine
depress bone marrow production of cells, including T
cells
Cyclophosphamide
inducing a cytokine switch, with a decrease in IL-12
and an increase in IL-4, IL-5, and TGF-β
IMMUNO PHARMACOTHERAPY OF MS
NEUROMYELITIS OPTICA (NMO), OR DEVIC
DISEASE
antibodies targeting the aquaporin-4 water channel
present on the surface of the glia limitans at the
BBB
Rituximab is effective
ACUTE DISSEMINATED ENCEPHALOMYELITIS
Viral or bacterial epitopes resembling myelin
antigens activate myelin-reactive T-cell clones
through molecular mimicry
30% has serum antibodies to MOG, which were
absent in MS patients
Oligoclonal bands may very rarely be present, and
these cases should be followed for the
development of MS

IMMUNE-MEDIATED NEUROPATHIES - AIDP OR
GBS
Incidence of infection has been reported to be 90%
in the 30 days before occurrence
high incidence with C. jejuni infections
autoantibodies to myelin glycolipids, including GM1,
GD1a, and GD1b
Miller-Fisher variant of GBS - GQ1b antibodies
Antibody-mediated demyelination due to
complement fixation
axonal damage - result of bystander damage
IMMUNE-MEDIATED NEUROPATHIES - CIDP
no specific autoantibodies
fewer inflammatory infiltrates
mixed demyelination and axonal changes
indirect evidence that CIDP is T-cell mediated;
however, this area is still under investigation

TREATMENT OF IMMUNE-MEDIATED
NEUROPATHIES
Plasmapheresis
short-term immunotherapy that nonspecifically removes
antibodies from the circulation
IVIG
immunomodulating agent
works in part through the presence of Fc fragments that
interact with the inhibitory Fc receptor, FcγRIIB, which is
also induced on macrophages following IVIG
administration
displace low-affinity autoantibodies from the nerve
TREATMENT OF IMMUNE-MEDIATED
NEUROPATHIES
High-dose steroids
not effective in AIDP.
CIDP responds well
Immunosuppressants such as cyclosporine A,
cyclophosphamide, and azathioprine
In refractory cases of CIDP
Future therapies for AIDP or CIDP may target
complement activation or inhibition of axonal
calpain activation.

AUTOIMMUNE MYASTHENIA GRAVIS
80% to 90% - autoantibodies to the α subunit of the
acetylcholine receptor (AChR)
Thymomas occur in 10% to 15% of cases; most are in
the older age group
75% of patients will have a thymic abnormality, 85%
being thymic hyperplasia
patients with thymomas have antibodies to additional
skeletal muscle proteins such as the ryanodine receptor
and titin, as well as the neuromuscular junctional
protein, MuSK
AUTOIMMUNE MYASTHENIA GRAVIS
Both B & T cell–mediated disease
Antibodies Polyclonal and may be of any IGg
subtype
Poor correlation between serum antibody titers and
disease course and severity.
Failure of central or thymic tolerance may play an
important role
Autoreactive T cells are necessary for the disease
to occur

THERAPIES IN MG
Thymectomy
recommended for patients 15 to 65 years old, with
80% to 90% remission rate
Plasmapheresis and IVIG for acute MG
exacerbations or in preparation for surgery
Cyclosporine, Azathioprine, and Mycophenolate
Augment treatment when symptoms are not
adequately controlled

THERAPIES IN MG
Corticosteroids
used at various stages of treatment
multiple effects on the immune system, including
reducing AChR antibody levels.
Investigational therapies
Target specific molecules such as the B-cell surface
Ig or the TCR
Immunotoxins

INFLAMMATORY MUSCLE DISEASES
PM
a/w systemic autoimmune connective-tissue disorders
and viral and bacterial infections
endomysial inflammatory infiltrate containing
predominantly CD8 + T cells
DM
characterized by perifascicular atrophy
Antibody-mediated disease
IBM
mediated by CD8 + T cells

AUTOANTIBODIES IN INFLAMMATORY MUSCLE
DISEASES
Various autoantibodies directed against nuclear and
cytoplasmic cell components in up to 30%
Viruses including coxsackie B are implicated in the
pathogenesis
PM and DM patients may have anti-Jo-1 antibodies
to the viral enzyme, histidyl-tRNA synthetase

THERAPY OF INFLAMMATORY MUSCLE DISEASES
Corticosteroids
mainstay of treatment of PM and DM
IBM may be more resistant
IVIG, methotrexate, azathioprine,
cyclophosphamide, cyclosporine
Alternative treatment options
Total lymphoid or whole-body irradiation
In extreme cases
NEURODEGENERATIVE DISEASE & IMMUNITY - AD
Amyloid plaque clearance by either microglial- and
complement-mediated clearance or through direct
antibody-amyloid interactions
Immunization with amyloid-β peptide → amyloid-β-
specific antibodies, which enhanced the clearance of
amyloid plaques
patients developed meningoencephalitis, due to T-cell
responses to amyloid-β
Induction of an antibody and microglial-mediated
clearance of amyloid in the absence of a prominent T H1
response is the current goal of therapy
NEURODEGENERATIVE DISEASE & IMMUNITY - ALS
Activated microglia in areas of severe motor neuron
loss
Minocycline, which acts in part by inhibiting
microglial activation, has shown some initial
promise in the treatment of ALS

IMMUNE RESPONSE TO INFECTIOUS DISEASES
Balance the need to eliminate the pathogen and the
risk of inducing bystander damage to the delicate
and vital nervous tissues
↓
Many pathogens are not completely eliminated and
may persist to cause further symptoms.
CNS syphilis, Lyme neuroborreliosis, herpes
zoster, HIV, and Mycobacterium tuberculosis

IMMUNE RESPONSE TO INFECTIOUS DISEASES
Viral meningitis
Portal of entry is mucosal
membrane, usually the
nasopharynx
Strong local immune response
By the time the virus disseminates
to the leptomeninges, a sufficient
immune response has been
mounted in the periphery to
eliminate the pathogen
Viral encephalitis
•CNS invasion is so sudden
•Peripheral immune system has
insufficient time to react, and the
weak cns immune response is
often inadequate, resulting in a
poor outcome
Portal of entry and site of replication of the pathogen plays
a critical role

HIV-ASSOCIATED DEMENTIA (HAD)
CD4 is the cell surface receptor for HIV and microglia
and macrophages can express low levels of CD4
may explain the propensity of HIV for CNS
HIV protein, gp120, can bind directly to CXCR4 on
neurons, resulting in neuronal signaling and apoptosis
Glial-mediated neurotoxicity plays a significant role in
the pathogenesis
production of neurotoxic factors and proinflammatory
cytokines by HIV-infected microglia and astrocytes

TUMOR IMMUNOLOGY
Tumor immunosurveillance to prevent the formation
of tumors or inhibit further growth
Main effector cells are CTLs, NK cells, and TNF-α-
producing macrophages
Tumor cells escape surveillance mechanisms by
Masking or modulating antigens on their surface
Down-regulating class I and II molecules
Expressing immunosuppressant factors.
Increased frequencies of regulatory T cells

IMMUNOTHERAPY IN TUMOURS
Therapies to exploit the body's natural tumor
immunosurveillance mechanisms
Daclizumab (Anti-CD25 Antibody)
Reduces regulatory T-cell function and enhanced host
tumor immunity
Vaccination with killed tumor cells or tumor antigens

IMMUNOTHERAPY IN TUMOURS
Therapies to exploit the body's natural tumor
immunosurveillance mechanisms
Genetic engineering to transfect tumors with plasmids
bearing genes for costimulatory molecules to enhance
the tumor APC ability
Injection of cytokines such as IL-2 and tnf-α, which
enhance lymphocyte and NK function
Dendritic cells pulsed with tumor antigens to induce NK
cell-mediated tumor killing esp in CNS gliomas

PARANEOPLASTIC SYNDROMES
Neurological syndromes arising in association with
a distant cancer
Mediated by antibodies produced by the immune
system in reaction to a tumor antigen, which cross-
react with neural tissue
Cancers associated with paraneoplastic syndromes
are generally associated with a better outcome

Antibodies Associated
malignancy
Paraneoplastic Syndrome
Anti-Hu
antibody
Small-cell
cancer of the
lung
Encephalomyelitis and/or
sensory neuropathy
Anti-Yo
antibody
Breast and
ovarian cancer
Cerebellar degeneration
Anti-Ri antibody breast and
ovarian cancer
Opsoclonus-myoclonus
syndrome
Antibodies
against VGKC
Acquired neuromyotonia, or
Isaac syndrome
Morvan syndrome,
characterized by
neuromyotonia and
insomnia

Antibodies Associated
malignancy
Paraneoplastic
Syndrome
Antibodies against
the P/Q type of
voltage-gated
calcium channels
Small-cell cancer of
the lung
Lambert-Eaton
myasthenic
syndrome
Antibodies to
glutamic acid
decarboxylase
(GAD)
Breast cancer Stiff person
syndrome

ANTIBODY-ASSOCIATED NEUROLOGICAL
SYNDROMES
Antiphospholipid (APL) syndrome, or Hughes syndrome
Chorea, strokes, bleeding, migraine headaches, and epilepsy
CNS lupus
Antibodies directed against the NR2A and NR2B subunits of
the NMDA receptor in some
Rasmussen encephalitis
Antibodies directed against glutamate receptor 3 (GluR3)
form of severe intractable epilepsy localized to one
hemisphere and partially responsive to immunotherapy

ANTIBODY-ASSOCIATED NEUROLOGICAL
SYNDROMES
Molecular mimicry mechanisms related to
streptococcal infections
Sydenham chorea
Tourette syndrome
Pediatric Autoimmune Neuropsychiatric Disorders
Associated With Streptococcal Infection (PANDAS),
which encompasses tics and obsessive-compulsive
disorder in children
IMMUNOLOGY OF CNS TRANSPLANT
Tend to have longer survival times than peripheral
grafts
Major factor in the survival is their lack of
immunogenicity in the relatively immune-privileged
site of the CNS

FACTORS THAT INFLUENCE CNS GRAFT SURVIVAL
Type of graft (xenogenic, allogeneic, genetically
modified tissue, or stem cell populations)
Location of the graft, with the periventricular areas
being the most susceptible to rejection
Presence of antigen-presenting cells within the
graft, which can be eliminated in purified grafts
Host immunosuppression

NEURAL STEM CELLS (NSCS)
Suppress disease through immunomodulatory
mechanisms in MS
can directly inhibit T-cell proliferation in response to
concanavalin A (ConA) or to MOG peptide by inducing
T-cell apoptosis; or through nitric oxide– and PGE2-
mediated T-cell suppression
Can express costimulatory molecules, CD80 and CD86,
particularly after exposure to the proinflammatory
cytokines, IFN-γ and TNF-α
SUMMARY
Field of immunology has progressed significantly in
the past 30 years
Can expect many advances in the field of
neuroimmunology, including new therapies and
better strategies for the treatment of neurological
diseases
THANK YOU