neuroscience study guide (test 1) - …kupt2013comps.wikispaces.com/file/view/neuroscience.docx ·...
TRANSCRIPT

Neuroscience Study Guide (Test 1)Neurons: Structure and Function
Neurons:Dendrites-gray mater, receive info from other cellsAxon-white mater (myelinated), carries output info to presynaptic terminalPresynaptic terminal-transmit info to other cells; neurotransmitters releasedSoma cell body-gray mater, neurotransmitter produced
Membrane Channels (2 types): 1) leak-always open, allow diffusion from high to low concentration, no energy used2) gate-open in response to stimulus and close without stimulus
Modality gated-response to specific sensory infoLigand gated-open in response to neurotransmitter binding to channel receptorVoltage gated-open in response to electrical potential
Electrical Potential (3 types):1)Resting Membrane-difference in electrical charge across cell membrane at rest, no net flow of ions across membrane, typically -70 mV, maintained by Na/K pump2)Local Potential-initial change in membrane potential, all-or-none-stimuli results in action potential
temporal summation-combined effect of local potentials occurring rapidlyspatial summation-combined effect of several small local potentials at the same time
3)Action Potential-a 15 mV depolarization (-70mV to -55mV) produces action potential; 3 eventsVoltage-gate Na channels open, influx of Na; voltage-gate Na channels close; voltage-
gated K channels open and K leaves cellsAbsolute refractory period-no stimuli will result in action potentialRelative refractory period-stronger than usual stimuli will produce action potential
Postsynaptic terminal: receiving cell, contains receptorsExcitatory postsynaptic potential-depolarization, summation can lead to action potentialInhibitory postsynaptic potential-hyperpolarization, decrease chance of action potential
Presynaptic terminal: end of axon, releases neurotransmittersPresynaptic facilitation- increase neurotransmitters releasedPresynaptic inhibition- decrease neurotransmitters released
Neurotransmitters: must bind to receptors for an effectDirect effect-binds to receptor and opens ligand-gated channelsIndirect effect-binds to receptor and opens ion channel activating cascade of eventsAcetylcholine; Amino Acids-glutamate, glycine; Amines-dopamine; Peptides-endophins
Glial Cells: provide structure, transmit info, involved in neural development and repairMacroglia: Astrocytes-provide structure, regulate signaling, neural development and repair
Oligodendrocytes-produce myelin sheath in CNSSchwann cells-produce myelin sheath in PNS
Microglia: Phagocytes-repair damageNeural Stem Cells: undifferentiated precursors to both neurons and glial cells
2 areas in the brain produce neurons-subgranular zone of hippocampal dentate gyrus and subventricular zone of lateral ventricular wall
Development of Nervous SystemDevelopmental stages in utero: preembryonic (conception-2 wks), embryonic (2-8 wks), fetal (8wk-birth)
Embryonic-neural tube forms: neural plate forms in ectoderm->neural groove->neural crest(PNS)->neural tube: mantal-inner gray layer, and marginal-outer white layer

Divisions of the brain (4wks-birth):Forebrain: telencephalon and diencephalon-thalamus, hypothalamus, 3rd ventricle, basal gangliaMidbrain: mesencephalon-midbrain, cerebral aqueductHindbrain: metencephalon and myelencephalon-cerebellum, pons, 4th ventricle, medulla
Cellular-level development:2nd trimester: cell proliferation, migration, growth3rd trimester: synaptic formationLate 3rd trimester through young adulthood: mylenation
Brain Development:Blooming-proliferation of neuronsPruning-regression of neurons, neural death and axon retractionExperience expectant maturation-expects experiences and stimulationsExperience dependent maturation-experience refines brain growth
Sensory stimulation builds connections: vision, hearing, taste, smell, touch-most developed sensation
Spinal Cord and PNSSpinal cord: convey sensory info from periphery to brain, convey motor info from brain to periphery,
modify ascending and descending info; spinal cord continuous with medulla, ends at L1-2, cauda equine L2-S5 nerve roots, filum terminale-connective tissue to coccyx; dorsal and ventral rootlets form dorsal and ventral roots that combine to form spinal nerve;
Dorsal horn- sensory, contains endings of sensory neurons, interneurons, and cell bodiesLateral horn- cell bodies of preganglionic sympathetic neurons in T1-L2 spinal segmentsVentral horn- motor, cell bodies of lower motor neuronsDorsal Column-sensory tracts; Lateral Column-sensory and motor tracts; Anterior Column-motor tractsAfferent axon-carries sensory info to spinal cord; Efferent axon-carries info from spinal cordMyotome: group of muscles innervated by single spinal nerveDermatome: dermis innervated by a single spinal nerveUpper Motor Neuron: neurons with axon that descend from cerebral cortex or brain stem and end on
lower motor neuron; first pathway-neurons within CNSLower Motor Neuron: cell body in brain stem (cranial nerve) or ventral horn of spinal cord (alpha MN);
axon leaves CNS and synapses in periphery on muscles; secondary pathway-PNSReflexes: involuntary, stereotyped response to a sensory input that results in motor outputSpinal White Mater:
Sensory pathway-dorsal and lateral columnDorsal Column Pathway-conscious touch and proprioception
sensory info enters spinal cord, ascends in dorsal column to ipsilateral medulla, crosses spinal cord and ascends in medial lemniscus to contralateral
thalamusSpinothalamic pathway-conscious pain and temperature
sensory info enters spinal cord and synapses in dorsal horn, crosses contralateral spinal cord, ascends in spinothalamic tract, synapses in
thalamusSpinoreticular pathway-alerting and arousalSpinocerebellar pathway-unconscious proprioception
Motor pathways-anterior and lateral columnCorticospinal tract-voluntary movement and fine motor control
cell body in motor cortex, crosses medullary pyramid, descends in lateral column, synapses with alpha MN in ventral horn

Rubrospinal tract-gross motor movementscell body in red nucleus, crosses immediately, synapses with alpha MN in
ventral hornReticulospinal tract-trunk movement and postural controlVestibulospinal tract-trunk movement and postural controlTectospinal tract-reflexive movement of the head
Brain Stem and Cranial NervesBrainstem: 3 main sections (superior to inferior)-midbrain, pons, medulla; Sensory, Autonamic, and Motor tracts travel in brainstem; Tectospinal, Rubrospinal, Reticulospinal, and Vestibulospinal tracts originate in brainstem
Sections: Basilar-located anterior and contains predominantly motor system structuresTegmentum-located posterior, sensory nuclei and ascending sensory tracts
Reticular formation-adjust general activity level of nervous system; cranial nerve nuclei; medial longitudinal fasciculus-eye and head movement
Tectum-additional posterior section, pretectal areaSuperior and inferior colliculi-reflexive eye and head movement
Medulla: contributes to control eye and head movements, coordinates swallowing, helps regulate cardio, respiratory, and visceral activity
Cranial Nerves: part of PNS, myelinated by Schwann cells, LMN; CN 1-2 myelinated by oligodendroglia, specialized-sensory, motor, or both (review CN)
Corticobulbar tracts-first order neuron that starts in motor areas of cerebral cortex and project to CN nuclei in brainstem; facilitates second order LMNs that innervate muscles of head and neck
ANS, Hypothalamic, Limbic SystemANS: influenced by hypothalamus, maintains homeostasis, regulates activity of internal organs and
vasculatureReceptors-Mechanoreceptors, Chemoreceptors, Nosioceptors, ThermoreceptorsAfferent pathways-info from visceral receptors enter CNS from spinal cord via dorsal roots, or
from brainstem via CN 7,9,and 10Medulla regulates HR, RR, vasoconstriction/dilation by signals to autonomic efferent neurons in SC via
vagus nucleusHypothalamus, Thalamus, and Limbic system modulate brainstem autonomic control
Hypothalamus-overseers of homeostasis and ANS; many regions of the brain supply hypothalamus with info but only olfactory and small visual system send sensory
info directly to hypothalamus; hypothalamus also regulates pituitary which produces hormones
Limbic System: emotion and memory functions; influences motor and autonomic output via emotionsComposed of: hypothalamus, nuclei of thalamus, limbic cortex, hippocampus, and amygdale
ANS Efferent Pathways: Sympathetic-cell bodies of preganglionic neurons in lateral horn T1-12
maintain optimal blood supply to organs, regulate body temperature and metabolic rate, and regulates activity of vicera; thoracolumbar outflow; ‘fight or flight’
Parasympathetic-preganglionic cell bodies in brainstem and sacral spinal cordenergy conservation and storage, decrease cardiac activity, facilitates digestion, and
regulates activity of visera; craniosacral outflow; ‘rest and digest’
Neuro Test 2
Somatosensory
Sensory information serves to:• alert organism to changes in the environment • arouse organism• discriminate different sources of stimuli• provide a map of the environment
ReceptorsSensory threshold = minimum stimulus intensity which produces a response; this intensity may shift to different levels under different conditions.
Facilitation: Increase in excitability of a neuron by presentation of multiple subthreshold stimuli, each depolarizing the neuron until the threshold is reached.
Habituation: decrease in response to a repeated, benign stimulus
Parallel Processing: Related sensory information is used by different systems for different purposes, gives a more complete view of sensory environment = enhanced performance
There are three categories of pathways related to somatosensory system function:
1. conscious relay pathways : discrimination functions. Dorsal column/Medial lemniscus (touch) & spinothalamic (sharp, localized pain) pathways; terminate in primary somatosensory cortex
2. divergent pathways : slow, aching pain. Spinoreticular pathway; terminates in midbrain & reticular formation.
3. unconscious relay pathways : movement-related; postural adjustments. Spinocerebellar pathways; terminate in cerebellum
Nocioception (pain); Spinothalamic tract. A gamma fibers, small myelinated – gives sharp pain quickly, C-fibers are small and unmyelinated, they are slow – give dull aching pain
Mechanical - pin-pricks; squeezing/pinching of skin Thermal - dangerously high/low skin temperature Analgesia: the absence of pain in response to stimuli that would normally be painful. Hyperalgesia: excessive sensitivity to painful stimuli
Thermoreception - temperature changes close to body temperature; warm receptors & cool receptors; continuous (tonic) discharges, which change rate when temperature shifts
Mechanoreception – different types: touch, light touch, vibration/pressure, steady pressure

Proprioception - awareness of limb position; muscle stretch/tension; located in joints, tendons • Golgi tendon organ (GTO)
• responds to tension via passive stretch • responds to tension via active stretch
• muscle spindle • responds only to quick stretch, doesn’t do any muscle work
• Only a few of each per muscle• action is amplified to influence many muscle fibers
• Autogenic inhibition• GTO as protective system
• Therapeutic use – can use to reduce spasticity• Romberg test: stand with feet together, arms straight out to the side at 90 deg, close eyes,
and watch how they maintain their balance. Sway = positive test• Co-contraction: stable but less efficient, used when learning a new task• Reciprocal innervation: is contracting the agonist while relaxing the antagonist, learned
skill and efficient• Unconscious proprioception travels up the spinocerebellar tract and doesn’t go higher
than the cerebellum.• Voluntary movements can the travel back down the: corticobulbar – face and neck
mvmts, corticospinal – fine mvmts of the hands, corticorubrospinal – large mvmt of limbs.
Signs of Cerebellar Disease: ataxia, intention tremor, dysdiadochokinesis, poorly coordinated mvmts, problems with motor learning.
Auditory System
AnatomyThree parts make up the auditory apparatus:External ear - sound capture (auricle to tympanic membrane)Middle ear - sound amplification (ossicles – malleus, incus & stapes)Inner ear - sound (cochlea) & motion (vestibular apparatus) sensory receptors
sensory receptors - tonotopic organization,. Neural portion of the system, CN 8, enters at the junction between pons and medulla,
makes junctions in the vestibular nuclei Cochlea – middle chamber houses the organ of Corti, which contains the: auditory
receptors (inner & outer hair cells), basilar membrane, tectorial membraneHearingCan hear between 20 - 20,000 Hz, higher frequencies heard at the apex of the cochlea, lower frequencies heard at the base of the cochlea.
Intensity The amplitude of changes in sound pressure. The pressure change moves through the cochlea as a traveling wave. The positions of tectorial & basilar membranes shift positions relative to one another as pressure changes. The cilia of auditory hair cells are stretched as scala

media & basilar membrane shift position. The stretching of the stereocilia opens ion channels and activates the receptor.
Frequency The rate of pressure changes. Different auditory hair cell receptors are sensitive to different frequencies of sound (tone), with higher frequencies sensed by receptors near the oval window & lower frequencies senses by receptors nearer to the apex of the cochlea. Tonotopic organization occurs not only in the auditory receptors, but also in the auditory pathways, auditory nuclei, and auditory cortex.
After going to the 1 auditory cortex the signal will travel on to auditory association cortex: Wernicke's area area (area 22; language reception) and Broca's area (area 45; speech production).
Outputs:via cn.V (trigeminal)
protects against loud, low frequency tension of tensor tympani muscle; malleus
via cn.VII (facial) protects against loud, high frequency tension of stapedius muscle; stapes
via olivocochlear pathway enhances figure-ground discrimination adjusts length of outer hair cells
Impairments: Unilateral loss = localization deficit

Otitis media – movement of the ossicles is restricted by thick fluid in the middle ear Neural vs. conductive loss – can fix conductive, not neural Tinnitus – ringing in the ears, can occur after being exposed to loud noises Age-related frequency loss Acoustic neuroma – tumor that puts pressure on CN8, CN8 often removed with the tumor Hyperacusis – too sensitive hearing, can be addressed pharmacologically/behaviorally
Vestibular System
Only active when there are changes to the system – acceleration/deceleration
Common Impairments• Motion sickness, Meniere’s disease, Stationary nystagmus, Benign positional vertigo,
possibly related to learning disabilitiesVestibular Labyrinth:
Semicircular canals (angular acceleration) o Receptors within the canals respond to changes in angular motion. Each pair of
canals signals a change along a different angular path . Superior, Posterior, and Lateral
Macula contains 2 otolithic organs (linear acceleration & gravity) o Utricle (horizontal) o Saccule (vertical)
There is one kinocilium (larger, thicker, stiffer cilium) & many sterocilia (shorter, thinner cilia) per receptor neuron. When there are no changes in motion, the receptors are moderately active, firing at about 100 Hz. Displacement of the cupula moves the cilia and changes the polarity of the receptor. If the displacement stretches the cilia towards the kinocilium, the receptor will be depolarized (excited), and the firing rate will increase to more than 100 Hz. The receptor will be hyperpolarized (inhibited, with firing rates of less than 100 Hz) if displacement of the cupula stretches the cilia away from the kinocilium. The brain receives information from corresponding pairs of canals and compares the firing rates of each canal's receptors. This information is used to determine direction and velocity of the change in motion.
VOR PATHWAY

Macula
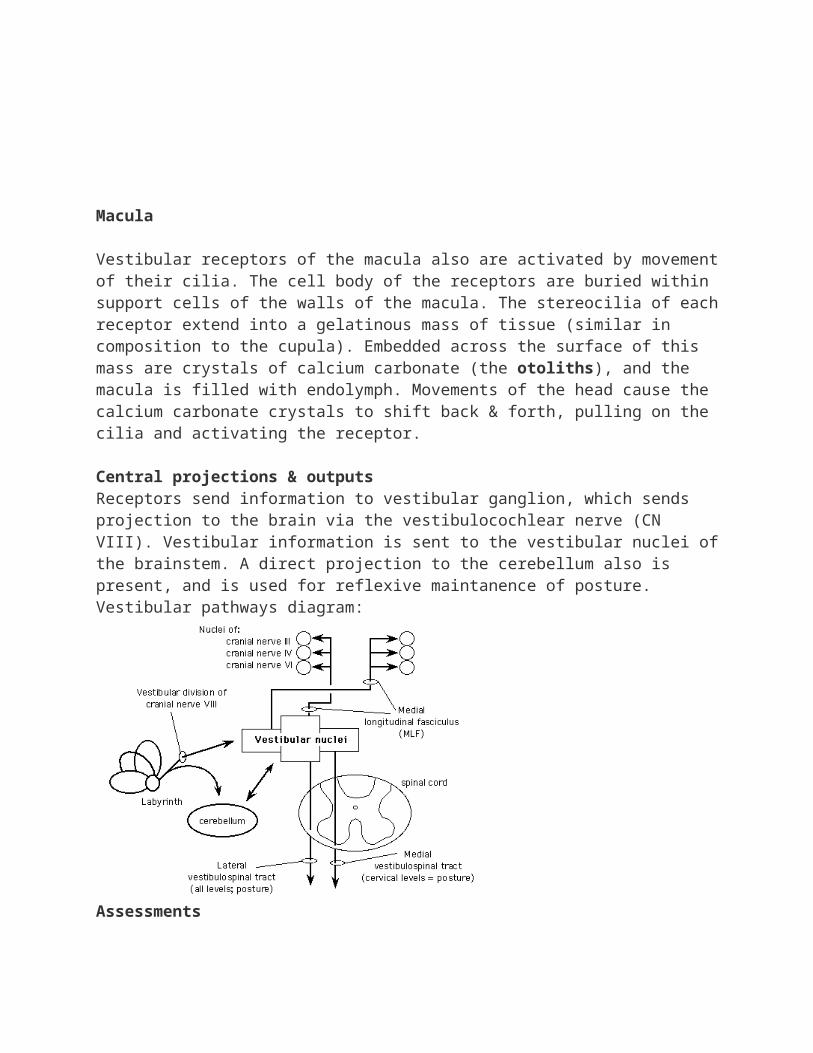
Vestibular receptors of the macula also are activated by movement of their cilia. The cell body of the receptors are buried within support cells of the walls of the macula. The stereocilia of each receptor extend into a gelatinous mass of tissue (similar in composition to the cupula). Embedded across the surface of this mass are crystals of calcium carbonate (the otoliths), and the macula is filled with endolymph. Movements of the head cause the calcium carbonate crystals to shift back & forth, pulling on the cilia and activating the receptor.
Central projections & outputsReceptors send information to vestibular ganglion, which sends projection to the brain via the vestibulocochlear nerve (CN VIII). Vestibular information is sent to the vestibular nuclei of the brainstem. A direct projection to the cerebellum also is present, and is used for reflexive maintanence of posture.Vestibular pathways diagram:
Assessments• Caloric test and VOR• Rotary chair and VOR
Visual System
Retina: photoreceptors: cones (color & bight light conditions) & rods (dim light conditions), macula & fovea , optic disk (blindspot)
Optic pathwaysOptic nerves, optic chiasm (partial crossing of fibers), optic tractsInformation sent to:
thalamus (lateral geniculate nucleus) midbrain (superior colliculus), then thalamus (pulvinar nucleus)

pretectum, hypothalamus, & accessory optic nucleiVisual reflexesSome visual reflexes occur automatically, and don't rely upon cortical processing of information
entrainment - jet-lag, seasonal affective disorder pupillary response - changes in light levels; balanced with sympathetic N.S. activity optokinetic nystagmus - picket fence, telephone poles, staring out of a bus window while
daydreaming vestibulo-ocular reflex - 'doll's eyes' reflex
The following reflexes are related to cortical function. accomodation - ciliary muscles contract, lens elongates saccades - short & very rapid shifting of eyes; reading smooth pursuit - tracking a moving object; tennis match vergence - eyes move in/out together to fixate object moving towards/away

peripheryperiphery
midline
Rightvisual field
Leftvisual field
Visual dysfunction
May occur through one or more processes:
Object agnosia – cortical problem, lack of knowing, can describe characteristics of a tennis ball but won’t be able to identify the object as a tennis ball
Prospagnosia – lower temporal lobe, specific ability to identify people’s face, even though you know this person you can’t name who they are
Blindsight – bilateral optic problem where they can’t perceive things but can avoid objects
Macular sparing - Vision, but loss of reflexive foveation, Lesion of the cortex, may not lose as much centrally as you do peripherally, b/c more of the brain is dedicated to central vision
Unilateral neglect - More than just a visual deficit, Homonomous hemianopsia ≠ unilateral neglect
Neuro Test Three
Voluntary Movement/The Motor Systems
1. Characteristics of the voluntary movement systema. Organized in the cortex to produce a PURPOSEFUL taskb. Can be varied (use of different muscle groups, intensity, direction)c. Can be improved with practice and motor learningd. Uses sensory information (M1) as well as generated internally (SMA)e. Prefrontal, SMA, PMA and M1
2. Primary Motor Cortex (M1)a. The “GO” signal to produce movementb. Low intensity stimuli elicit SIMPLE movements of SINGLE jointsc. Stimulation of M1 activates several different muscles (moves specific JOINTS rather than
specific muscle movements)d. Somatotopical organization – hands and lips are large for precision. Organization is
highly plastice. Grades how much FORCE you need to produce a movement and what DIRECTION the
movement will go 3. PMC
a. Project mainly to M1 but also to spinal cord b. Area of preparation of movement c. Requires higher stimulation to create more complex movements across multiple joints
(damage here causes more motor deficits than damage to M1) d. PMCdorsal: Projects to proximal muscles. Involved in external cues. Fires between cue
and action.

e. PMCventral: Projects to hand and digit muscles. Involved in correcting hand shape. Active if just watching an activity (“mirror cells”).
4. SMAa. Also for preparatory movement like PMCb. Involved in performing sequential movements, especially with fingers (piano) c. INTERNALLY driven movements (prepare movements from memory)d. Skilled, performance, rehearsed movements e. Involved in coordinating two sides of the body (coordination of hand movements. I.e.
monkey poking in the whole to get something out of it but can’t coordinate hands properly)
5. Output Pathways Tract Origin Crossing Point Termination/Function Other Info Damage
Lateral Corticospinal M1
(50%)
PMA
S1
Medullary Pyramids
LMN to control voluntary and fine motor movements
Difficulty with fractionated movements and changes in force and direction of movement
Ventral CS M1, PMA, S1 None LMN in cervical and thoracic segments for postural control of neck and trunk
Collaterals to brain stem to modulate vestibulospinal and reticulospinal tracts
Same as above, also loss of postural modulation
Rubrospinal Red nucleus Immediately in pons
LMN primarily of upper limb flexors for gross
Not an important tract in humans
motor control
Vestibulospinal (medial and lateral)
Vestibular nucleus
Medial project bilaterally
Lateral project ipsilaterally
Medial terminates in ventral horn on LMN of cervical and upper thoracic to stabilize head (posture)
Lateral on LMN of extensor ms to maintain balanced posture
Balance and postural problems
Tectospinal Superior colliculus
Immediately crosses
Medial part of ventral horn on LMN in cervical spine to control reflexive movement of the head
Reticulospinal Reticular formation
Medial projects ipsilat
Lateral projects bilat
Medial to LMN at all levels to facilitate postural control and limb extensor control
Lateral to LMN at all levels to control posture by facilitating flexors and inhibiting extensors
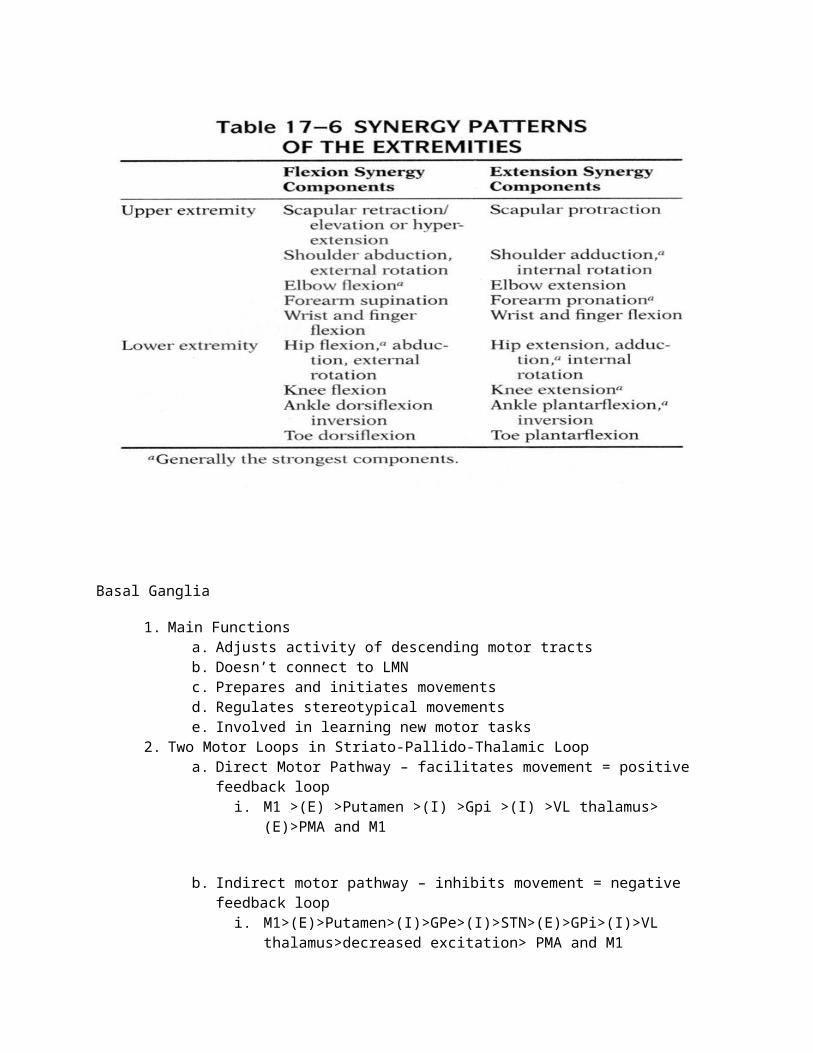
6. Synergy: pt unable to move an isolated joint without movement of entire limb

Basal Ganglia
1. Main Functions a. Adjusts activity of descending motor tracts b. Doesn’t connect to LMNc. Prepares and initiates movements d. Regulates stereotypical movements e. Involved in learning new motor tasks
2. Two Motor Loops in Striato-Pallido-Thalamic Loopa. Direct Motor Pathway – facilitates movement = positive feedback loop
i. M1 >(E) >Putamen >(I) >Gpi >(I) >VL thalamus> (E)>PMA and M1
b. Indirect motor pathway – inhibits movement = negative feedback loopi. M1>(E)>Putamen>(I)>GPe>(I)>STN>(E)>GPi>(I)>VL thalamus>decreased
excitation> PMA and M1

3. Thalamocortical Loops – how BG influences cognition and mood a. Dorsolateral prefrontal circuit (organizing behavior, problem solving)
i. Dorsolateral prefrontal cortex>caudate> GP/SN>VA thalamus or dorsomedial nucleus
b. Lateral Orbitofrontal circuit (socially appropriate behaviors) i. Lateral Orbitofrontal cortex > caudate > GP/SN > VA or DM
c. Anterior Cingulate circuit (motivated behavior and procedural learning) i. Anterior cingulate cortex >putamen> GP/SN > Thalamus/DM
4. Basal Ganglia Diorders a. Parkinson’s – damage to substantia nigra causing loss of dopamine
i. Symptoms: rigidity, bradykinesia, masked face, shuffling gait, resting tremor, micrographia, dementia (caudate involvement later on in disease progression), retropulsion (lean back when cue to come out of flexed posture)
b. Parkinsonism disease – damage to putamen or GPc. Balism – STN damaged. Hunthington’s chorea – striatal neurons that give rise to indirect pathway are lost
i. Chorea: series of continuous, rapid movements of face tongue or limbsii. Autosomal dominant disorder due to gene defect on chromosome 4
e. Dystonia – sustained muscle contractions causing twisting and repetitive movements or abnormal posture
i. Caused by chemical dysfunction in BG or defect in descending pathways involving reciprocal inhibition of motor neurons
ii. Blepharospasm (blinking), Cervical, Oromandibular (face and jaw muscles), Dysphonia (speech), writer’s cramp
Thalamus
1. Function:

a. final processing station for sensory information before it reaches the cortexb. receives and processes all internal motor (meaning doesn’t project to a LMN
directly) systems (cerebellum, BG) 2. 4 regional zones
a. Anterior: Affectivei. Anterior Nucleus
1. Relays information from cingulated gyrus to contribute to emotional tone
ii. Dorsomedial Nucleus1. Relays information to and from prefrontal lobe to contribute to
judgment and reasoning b. Medial: Arousal
i. Intralaminar: relays arousal info from reticular formation to many areas of the brain
ii. Centromedian: sameiii. Midline: same
c. Lateral: Motori. Ventral Anterior Nucleus
1. Relays information from GP and cerebellum to premotor areas and M1 to contribute to motor planning and regulation
ii. Ventral Lateral Nucleus1. Relays information from cerebellum and GP to M1 and premotor
areas for motor output regulation d. Posterior: Sensory
i. Ventral Posterior Nucleus1. VPM and VPL
a. Relays somatosensory info to the cortex2. VPI
a. Relays vestibular info to cortexii. Pulvinar Nucleus
1. Connects all secondary sensory areas together iii. Lateral Geniculate Nucleus: visual info to primary visual cortex (17)iv. Medical Geniculate Nucleus: auditory info to primary auditory cortex (41)

3. Internal Capsule a. Anterior: affective
i. Frontopontine fibersb. Genu: motor
i. Corticorubral and corticobulbar fibers c. Posterior: motor and sensory
i. Ascending sensory fibers, auditory radiations, optic radiations, and corticospinal fibers
4. Thalamic Pain Syndrome a. Infarct in VPLb. Patients experience burning pain and dysesthesia
Cerebellum
1. Functions
a. Feedback and Feedforward information
b. Informs movement
c. Balance, Timing and Motor Learning
2. Lobes
a. Anterior

b. Posterior
c. Flocculonodular (vestibulocerebellum)
i. Sends fibers to vestibular nucleus to influence postural control/balance as well as coordinate eye and head movements (VOR)
ii. Damage: balance disorders, ataxia, loss of VOR
3. Vertical Sections (within anterior and posterior lobes)
a. Lateral hemisphere (Cerebrocerebellum)
i. Input: from the cortex
ii. Output: Dentate nucleus to VL to Premotor areas and M1
ii. Involved in planning and programming voluntary, learned, skillful movement by influencing output from the motor cortex
iv. Damage: increased reaction time, errors in movement timing
b. Paravermis (Spinocerebellum)
i. Input: from motor cortex and spinal cord
ii. Output: Interposed nucleus to VL/VA to M1 and red nucleus
iii. Adjusts limb movements on-line (compares commands from motor cortex with actual position and velocity of movement)
iv. Damage: hypotonicity, intention tremor, ataxia, pendular reflex, dysmetria
c. Vermis (Spinocerebellum)
i. Fastigal nucleus to VL to vestibular nucleus and reticular nucleus
ii. Controls extension and proximal muscles for postural control and balance
iii. Damage: ataxia, balance disorders
3. Peduncles
a. Inferior: mostly input fibers from the body. Some output to vestibular nucleus and reticular formation
b. Middle: input only from the cortex
c. Superior: output fibers to cortex and thalamus
4. Cellular Anatomy
a. Purkinje cells
i. Output from the cerebellum
ii. Receives weak input from many parallel fibers and strong input from climbing fibers
b. Climbing fibers
i. Information from higher order (cortex), teach Purkinje cells how to respond to parallel fiber inputs
ii. Synapse directly on Purkinje cells, needs only a single action potential to depolarize a Purkinje cell
iii. Each Purkinje neuron receives input from one climbing fiber
iv. Excitatory
c. Mossy fibers i. Come from spinocerebellar pathways, brainstem, reticular nuclei, pontine
nuclei, etc.ii. Synapse on Granule cells (parallel fibers), Golgi cells, Stellate cells, and
Basket cells which either make inhibitory or excitatory synapses on Purkinje cells
d. Parallel fibers (axons of Granule cells that turn parallel)i. Run along top of Purkinje cells
ii. Each Purkinje cell has about 80,000 parallel fiber synapses iii. Excitatory iv. Need synchronous activity of these fibers to depolarize Purkinje cells
5. Feedforward a. When the cerebellum predicts movements and adjusts them online b. Allow for precisely timed behaviors
Neuroscience Exam 4
Neuroplasticity – ability of neurons to change their function, chemical profile, or structure.
Types:

- Habituation: decrease in response to a repeated, benign stimulus due to a decrease in synaptic activity between sensory neuron and interneuron. Allows other types of learning to occur by letting people pay attention to important stimuli and “tune out” the unimportant.
- Experience-dependent plasticity: Use-dependent; persistent, long lasting changes in the strength of synaptic connections between neurons and within neural networks. Ex: learning to play an instrument. Long term potentiation (LTP): greater potential for neurons to produce a response. Long term depression (LTD): neurons have decreased potential to produce a response. Communication between astrocytes and neurons occur via the release of neurotransmitter by the neuron, which stimulates the release of gliotransmitters by the astrocyte.
Memory:
Working memory: things you need to remember right now (phone number etc.) Short-term memory: Remember it long enough to complete an activity (what to buy at grocery
store etc.) Long-term memory:
- Declarative: Somatic (facts) and Episodic (events)
- Non-declarative: procedural (motor skills), Priming, Classical conditioning, and Non associative learning.
Axonal injury in PNS: When axon is injured, cytoplasm leaks out and the segments retract from each other. The distal segment undergoes wallerian degeneration while glial cells pick up debris. Cell body undergoes degenerative changes, followed by regrowth of damaged axons. Recovery is slow…~ 1mm of growth/day.
CNS injury: Damage to white tracts leads to increased permeability of axons and disregulation of sodium calcium channels, causing an influx of calcium. This leads to a disruption of axonal transport and accumulation of intra-axonal components. This buildup causes axons to swell and break at site of damage.
Functional axon regeneration does not occur in CNS due to glial scars and absence of nerve growth factor.
Synapses undergo changes in 4 ways:
- recovery of synaptic effectiveness- denervation hypersensitivity- new synapses formed in hopes that any neurotransmitter released
will be caught- synaptic hypereffectiveness- if some branches are lost, the other branches become hypereffective. - Unmasking (disinhibition) of silent synapses
Cortical maps can be modified by senseory input, experience, learning and brain injury.
Neurogenesis- neural stem cells discovered in developing brain and adult brain – undifferentiated precursors to both neurons and glial cells.

Factors influencing recovery of neuronal function:
1. intensity of rehab2. type of rehab3. amount of time between the injury and initiation of rehab
Blood supply to brain – requires 50mL/min of blood for every 100g of tissue.
- 25 mL/100g puts cells in peril- 8 mL/100g kills neurons in minutes.
Brain blood supply—arteries run in pairs
1. internal carotids - branch off common carotid, enters skull through carotid canal. - branches: - anterior cerebral - to medial aspects of cortex, internal capsule and basal ganglia - middle cerebral -to lateral cortex, caudate, putamen, and anterior limb of internal capsule- opthalmic -to retina and dura- anterior choroidal -to internal capsule, thalamus, hippocampus, and basal ganglia- anterior communicating -between anterior cerebral arteries- posterior communicating -hypothalamus, thalamus, and hippocampus.
Circle of Willis – “collateral circulation”, anterior communicating, anterior cerebral, posterior communicating, and posterior cerebral arteries all join.
2. vertebral arteries - ascend from subclavians, through foramen at 6 th vertebral artery, and up through foramen magnum. Join to form basilar artery.
- branches:
- anterior spinal artery – to pyramids, medial lemniscus, medial longitudinal fasciculus, CN XII, and inferior olive
- posterior inferior cerebral artery-to spinothalamic and spinocerebellar tracts, parts of CN IX and X, vermis, and inferior cerebellum. Occlusion produces Wallenbergs syndrome.
- Posterior Spinal Artery- to fasciculus gracilis and cuneatus, spinal trigeminal nucleus, inferior cerebellar peduncle, and some of vagus N.
-Basilar artery on the ventral aspect of the pons does not have a pair. Forms at the junction of the posterior cerebral arteries and bifurcates to form vertebral arteries.
Blood Flow Deficits:
- Anterior Cerebral: contralateral hemiplegia, somatosensory loss mainly in LE, some loss of motivation and executive function.
- Middle Cerebral: contralateral hemiplegia, somatosensory loss in UE and head, aphasia, sensory association, executive function and working memory, major multisystem dysfunction possible.
- Posterior Cerebral: Hemianopsia, Weber’s syndrome, - Superior Cerebellar: ipsilateral limb and gait ataxia, contralateral loss of pain and temp, Ipsilateral
Horner’s syndrome.

- Anterior inferior cerebellar: ipsilateral loss of facial sensation, ipsilateral Horner’s syndrome, contralateral hemianesthesia.
- Posterior inferior cerebellar: Wallenberg’s Syndrome- Anterior spinal: Medial medullary syndrome- Posterior spinal: ipsilateral conscious proprioception
Vertebral Aa Compromise: extension and rotation, especially with bad posture; results in nystagmus, dizziness, nausea, blurred vision, and loss of balance.
Venous Drainage: Sinuses drain to heart via Jugular veins
- Superior sagittal sinus- Inferior sagittal sinus- Spehnoparietal sinus- Cavernous sinus- Transverse sinus- Confluence of sinuses
Meninges: 3 layers
- Dura Mater (outer)- Arachnoid mater (middle)- Pia mater (most inner)
Ventricles: filled with CSF
- 2 lateral ventricles- bordered by internal capsule- 3rd ventricle- between thalami, above hypothalamus- 4th ventricle- empties into central canal of spinal cord
Hydrocephalus: production of CSF even when flow is restricted
- Communicating- Non-communicating
Cerebral cortex
- Occipital-vision- Parietal-somatosensory- Temporal-auditory input, interpretation of speech, language on L, nonverbal on R- Frontal-judgement, reasoning, social norms
Subcortical white matter:
- Projection fibers-to/from cortex- Commissural fibers-connect homologous areas of R and L- Association fibers-connect cortical regions within one hemisphere
Primary sensory areas: receive sensory input direct from thalamus
- Vision (17)- Auditory (41/42)- Somatosensory (3,1, 2)
Secondary sensory areas:
- Visual (18,19)

- Auditory (22)- Somatosensory (5, 7)
Association Cortices:
- Prefrontal- self awareness, executive function, problem solving- Parietotemporal- sensory integration, comprehension of communication- Limbic-emotion, motivation, memory processing
Communication: L hemisphere dominant in 94% of people
- Wernicke’s- L=comprehension of spoken language, R=interpreting nonverbal signals- Broca’s- L=instruction of language output, R=instruction for producing nonverbal communication
Disorders of Cerebral Cortex
- Agnosia-inability to recognize objects using a specific sense- Asterognosis- inability to identify objects by touch and manipulation- Visual agnosia-inability to visually recognize objects with vision intact- Prosopagnosia-inability to recognize peoples faces- Auditory agnosia- cannot recognize sounds
- L: understand speech
- R: interpret environmental sounds
- Apraxia-inability to perform movement despite intact motor cortex, sensation, and cognition- Broca’s aphasia- impairment in speaking and writing, is able to understand language- Wernicke’s aphasia-impaired language comprehension, produce sounds but has meaningless
output- Dysarthria- speech disorder due to uncoordinated or spastic muscles- Alexia: inability to comprehend spoken language- Agraphia: inability to write- Prefrontal Cortex: lack of goal-directed behavior, executive function, and initiative- Limbic:
-orbitofrontal: inappropriate risky, impulsive behavior
-temporal: outburst of physical/verbal aggression, emotionally labile
- Neglect: behave as if one side of body does not exist and will not report or respond to stimuli on contralesional side. Usually on L
Theories on aging
-Hayflick- cells can only divide so many times
-Free radical damage- oxidative stress
-alterations in the endocrine system- changes with hormones
-age related cognitive slowing- through various physiological processes, cognitive processes slow and deteriorate.
Structural age-related brain changes

- atrophy- reduced capillary density- metabolic changes
Stroke
-Central Core: 5 regions- thalamus, pons, medulla, cerebellum, reticular information: regulate basic life processes (breathing, pulse, arousal, movement, balance, etc)
-Limbic system: 3 regions-hippocampus, amygdala, hypothalamus:controls motivated behaviors, emotional status, and memory processes
-Brain cells are depended on glucose and oxygen for energy. Brain cells have severely limited storage capabilities for glucose and ATP so blood must maintain a constant supply of glucose. Normal cerebral flow 50-60mL/100g/min.
-Brain cells are destroyed after 4-6 min without oxygen
-Stroke is the 3rd leading cause of death in the US and leading cause of long-term disability worldwide.
-Etiology of stroke- atherosclerosis, heart disease, vasculitis/arteritis, trauma, tumor, infection
-Risk factors- age >55, male, African American, heredity, HTN, obesity, diabetes, smoker, high Cholesterol, excess alcohol use, heart disease, hypercoagulability, drugs
-Stroke Symptoms- trouble walking, loss of balance/coordination, trouble speaking, muscle weakness, change in alertness, sensation changes, dizziness, loss of bowel/bladder control, N/T on one side of body, mood/emotional changes, changes in eyesight
-Excitotoxicity is a key mechanism of cell and tissue destruction in cerebral ischemia
-Most important aspect of recovery is sleep. Success of rehab depends on sleep. Sleep strengthens and recovers the brain. Sleep decreases risk of another stroke.
Types of stroke: ischemic, hemorrhagic, transient, evolving, and completed, global, and focal.
Left CVA Right CVA
Aphasia Language Intact
Dysarthria Speech dysarthria
Right Homonymous hemianopsia
Sensation Left homonymous hemianopsia
Normal awareness Perception Unilateral neglect
Right side paresis Movement Left side paresis
Judgement intact, depression, Behavior Judgement impaired, denial,

slow and cautious impulsive behavior
Impaired analytical (overestimation)
Cognition Impaired analytical (underestimation)
Deficit new language info Memory Deficit new spatial info
TBI
-Primary injury- result from mechanical force acting on brain
-Secondary injury- resulting biomolecular and physiological changes that follow, progression is a major deciding factor in recovery from TBI
-Symptoms dependent on severity: cognitive deficits, poor balance/coordination, inability to walk, sensory impairments, emotional/behavioral effects
-Glutamate significantly contributes to brain cell death and dysfunction after TBI
-Blood Brain Barrier can fail as a result of TBI
-brain is highly susceptible to ischemic injury after TBI
-cerebral blood flow is often half of normal 24hrs after TBI
-brain edema is usually worse 24-48hrs post-TBI
-No successful treatment options are currently available for promoting functional recovery from TBI, although pharmacologic interventions are used to help manage TBI
-research has shown exercise can improve cognition, prevent cognitive decline, increase neurogenesis in the brain, and improve motor function.