new business models and primary care contracting
TRANSCRIPT

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS1
Primary care in an Accountable Care
Organisation (ACO)
Gabrielle Darby, Unit Head, New Business Models Group, NHS England
Paul Maubach, Accountable Officer, Dudley CCG
22nd November 2017
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS2
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS
Why are GPs considering accountable models?

www.england.nhs.uk
Trends suggest demand on general practice will
continue to rise…
33
The population in England is growing and age profile is changing – proportion of the population that
is over 65 and over 85 is increasing (48.9% and 113.9% respectively) (4). The number of older
people with care needs is expected to rise more than 61% in the next 20 years.(5) The share of
clinical staff contacts taken up by patients over 85 is growing, it increased by 16% between 2010/11
and 14/15 compared to 4% for 18 – 64 year olds.(6)
Demand in general
practice has been rising
historically
A growing and ageing
population could
further increase GP
workload
Estimates of a 10.5% increase in GP and nurse consultations between 2007 and 2015(1). Between
2010/11 and 2014/15 average list size increased by 10%.(2) The average number of consultations
per patient per year from 4.2 in 2000 to 5.5 in 2008 and in the over 75s from 7.9 in 2000 to 12.3 in
2008.(3)
The number of people with three or more long-term conditions is predicted to rise from 1.9 million in
2008 to 2.9 million in 2018.(7) LTCs account for about 50% of all GP appointments.(8) Intensity
could rise as complex care needs longer appointments, Hobbs et al found that mean duration of GP
consultations increased 6.7% to 9.22 minutes between 2007 and 2014 implying the 10 min
appointment system is nearing saturation point (9).
Changing burden of ill
health could impact
both volume and
intensity of workload
At the same time
patient expectations
are rising
The majority of patients (74.1%) contacting a surgery want to access a GP and in 2017 50% of
patients had a preferred GP. A survey of medical professionals across Europe showed that patients
expect higher standards, more information, more involvement in decisions and access to the latest
treatments. Person centered care and shared decision making have implications for demand on
GP time.

www.england.nhs.uk
… and that general practice will need to adapt to
meet this demand
44
The 2015 GP Worklife survey reported the lowest overall job satisfaction reported by GPs since
2001. Reported levels of stress increased between 2012 and 2015 on all 14 stressors in the survey.
Reported levels of stress are now at their highest since the survey began in 1998.(1) A BMA 2015
poll of GPs found that 34% intended to stop working by 2020.
Attrition rates mean the
workforce may struggle
to meet demand
Stress and workload
are leading to burnout
and early retirement
During 2000 and 2010 the number of salaried GPs increased more than ten-fold (3). Two thirds of
salaried GPs work part time and in 2016 53% of the GP workforce was female. (4) NHS England
data shows a decreasing number of GP partners correlating with an increasing number of salaried
GPs (5). CfWI have modeled a range of scenarios showing that there is likely to be a demand-
supply imbalance by 2020 (6).
Nuffield / RCGP survey suggests a trend towards formal collaboration following the publication of
the Five Year Forward View with 63% of respondents saying they were in a collaboration and 44%
of respondents reporting their ‘main organization’ was formed in 2014/15 (7). NAPC now has more
than 200 Primary Care Home sites and there is real momentum behind ACS and ACO development
in the system.
Practices consolidation
and integration are
changing the provider
landscape
Technological
Innovations present an
opportunity if
harnessed early
Apps are starting to play a role in empowering service users, supporting professionals and
enabling specialist expertise to transcend geographical boundaries. We are starting to see
businesses emerging to offer online GP consultations.

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS5
5
There are some common themes to the models of
collaboration which we have heard from stakeholders
De-medicalise
model Value
professional
judgment
Value GPs handling
risk and uncertainty
Maintain GP relationship
with community
Look to reduce
inappropriate specialist
referrals and build
capacity in community
Holistic care for
complex needs
Generalist equal to
specialist
Measure quality by
patient experience
Personalised decision making
Whole population
approach
Support professionals to
focus consultations on
what matters to patients
Population
segmentation and
targeted approach
Prevention – more
focus on keeping
people well
Recognise social
determinants of healthSelf-care and
patient activation
GP leading a wider
clinical team
Give flexibility for
GPs’ preferences
Strategic redistribution
of medical work
Risk concentrating
complexity in GP role
GP provides expert medical
overview like hospital
consultant
Upskill wider team
Invest in dataConnect to
community assets

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS6
These models form the corner-stone of system-wide
accountable care
• ‘Accountable care’ is a term used to describe accountability for using a defined set of
resources to provide the best possible quality of care and health outcomes for a defined
population.
• The care model, centred on general practice, is by far the most important aspect of
developing new arrangements.
• It is possible to develop a care model through collaboration but in some places
commissioners have decided that sustainable implementation of the model with clear
decision rights and a single re-deployable budget to deliver it requires a new contract, rather
than relying on goodwill.
• Some areas (particularly some of the MCP and PACS vanguards) wish to establish
contracted-for Accountable Care Organisations (ACOs)
• ACOs need to either directly encompass general practice – through sub-contracting with GP
practices or employing primary care staff (or a mix of the two) – or there needs to be a very
strong integration agreement between the ACO and local GPs.
• ACOs vary in scope. E.g. an MCP is largely based on out of hospital services, whereas a
PACS has a wider scope as it brings in acute services.

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS7
Types of accountable care models
Collaborative
change
Small scale
Primary care
network
ACO – fully
integrated
Single contract with
integrated budget (inc
core primary care)
Virtual MCP or PACS ACS
ACOs are organisations
with a new contract,
rather than collaborations Structural
change
Large scale
ACO – partially
integrated
Integrated contract
aligned with GMS/PMS
practices

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS8
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS
What is a virtual model?
• This is one of the more common approaches sites are taking
• The virtual model allows local providers and commissioners to collaborate to deliver an MCP or
PACS, a primary network or other collaboration
• The Alliance Agreement sits on top of existing contracts (such as GMS/PMS/APMS for General
Practice but does not replace existing Contracts.
• The Alliance is signed by all the participants in the virtual model, but does not overrule existing
bilateral service contracts.
• It enables integration between the providers who agree to a shared vision, operational and
resource commitments.
• It’s possible for commissioners to included as part of, or remain outside, the alliance
GMS / PMS /
APMS Contracts
Commissioners
NHS Standard
Contract
NHS Standard
Contract
NHS Standard
Contract
NHS Standard
Contract
Acute
provider
GP
practicesCommunity
provider
Mental
health
provider
Voluntary
sector
providers
ALLIANCE
AGREEMENT

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS9
Beacon Medical Group – NAPC Primary Care Home
Model Primary Care Home
Contract length Lifetime (PMS contract duration)
Population 39,000 patients across Plymouth and South Devon
ScopePrimary care, social care, public health, community
healthcare, mental health
Annual budget Total health spend for population - £46.7m
Stage of
procurementIn action, considering progress to Virtual MCP
GP integration Primary Care Home is led by the GP practice
Social care
integrationSocial care part of an integrated health and social
care provider and fully engaged.
Notes
As a rapid test site for the NAPC Primary Care Home Programme Beacon Medical Group have
developed a care model which will:
• Increase levels of health activation and community level support for our patients in partnership with
our patient groups, community pharmacy and the voluntary sector
• Provide outpatients support within our community as a practice and in conjunction with secondary
care
• Develop an integrated and flexible team around our most vulnerable patients through virtual ward,
enhanced care homes support and liaison psychiatry

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS10
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS
What is a partially integrated ACO?
• In areas procuring ACOs the most common way that GPs are looking to engage is through partial
integration, and also through some direct influence within the ACO’s governance
• In this model GPs keep their existing GMS/PMS/APMS contracts and remain separate entities from the
ACO.
• An ACO Contract is awarded for all services in scope excluding core general practice.
• Practices sign an Integration Agreement with the ACO – an agreement that sets out how the practices and
the ACO will work together to deliver the integrated care model.
• The Integration Agreement sets out their commitment to a shared vision, sharing resource and devising a
joint workforce, estates, IT and care pathway design strategy.
ACO
Commissioners
Integration Agreement
GP practice 3
GP practice 1
GP practice 2
GMS / PMS Single contract – up to 10 years
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS11
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS
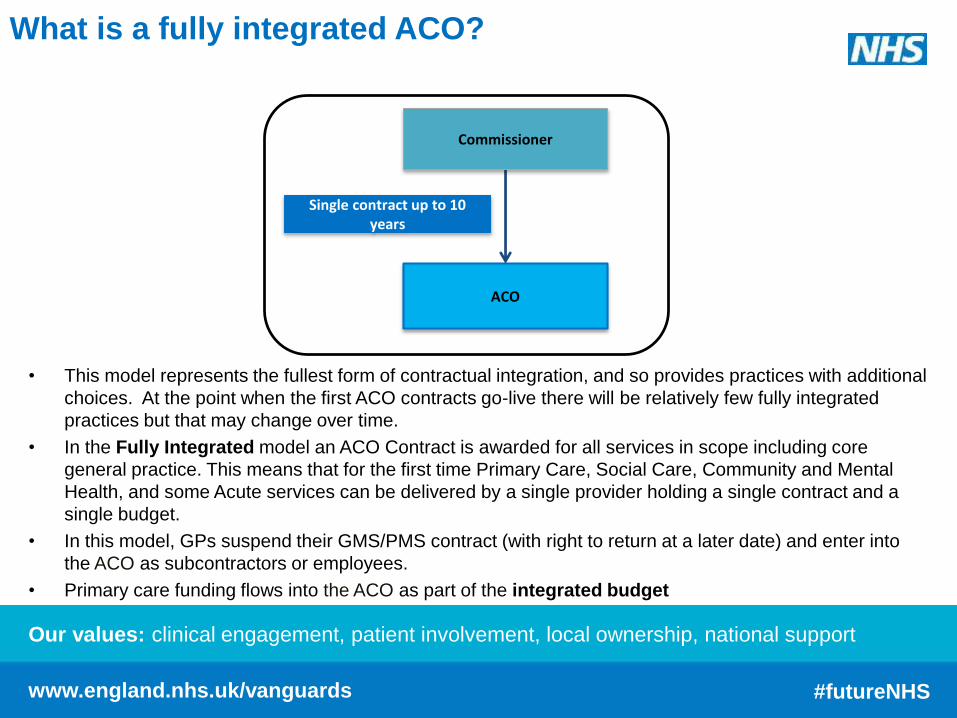
What is a fully integrated ACO?
• This model represents the fullest form of contractual integration, and so provides practices with additional
choices. At the point when the first ACO contracts go-live there will be relatively few fully integrated
practices but that may change over time.
• In the Fully Integrated model an ACO Contract is awarded for all services in scope including core
general practice. This means that for the first time Primary Care, Social Care, Community and Mental
Health, and some Acute services can be delivered by a single provider holding a single contract and a
single budget.
• In this model, GPs suspend their GMS/PMS contract (with right to return at a later date) and enter into
the ACO as subcontractors or employees.
• Primary care funding flows into the ACO as part of the integrated budget
ACO
Commissioner
Single contract up to 10 years

Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS12
Dudley case study
12
Model MCP
Contract
length10 years
Population Resident population, c.315,000 people
Scope
Community healthcare, some outpatients, UCC and out of
hours, primary care, mental health, learning disability,
intermediate care, CHC, end of life, voluntary and
community, public health, adult social care (phased)
Annual
budget>£200m
Stage of
procurementProcurement execution in progress
GP
integration
Mixed; some partial, some full. 84% of practices, covering
87% of the population, actively supportive
Social care
integration
Adult social care and public health included in scope. ASC
to be transferred over contract life
Notes
• Dudley was selected to join NHS England’s Vanguard programme in early 2015, and has since worked
with local partners and stakeholders to develop the MCP.
• The MCP will have the right to determine how the integrated budget is spent to realise a set of outcomes.
• The contract will be designed to deliver these outcomes, and some payment will be performance related.
Our values: clinical engagement, patient involvement, local ownership, national support
www.england.nhs.uk/vanguards #futureNHS13
More details can be found on the
NHS England website:
www.england.nhs.uk/new-business-
models.
england.newbusinessmodels@nhs.
net.
For further information…