new employee check list - barber specialties,...
TRANSCRIPT
NEW EMPLOYEE CHECK LIST
Company Name: Client #: 1057
Employee Name: Employee #:
o Employee Enrollment Form
o Employee Acknowledgement (4 pgs)
o W-4 Form (1pg)
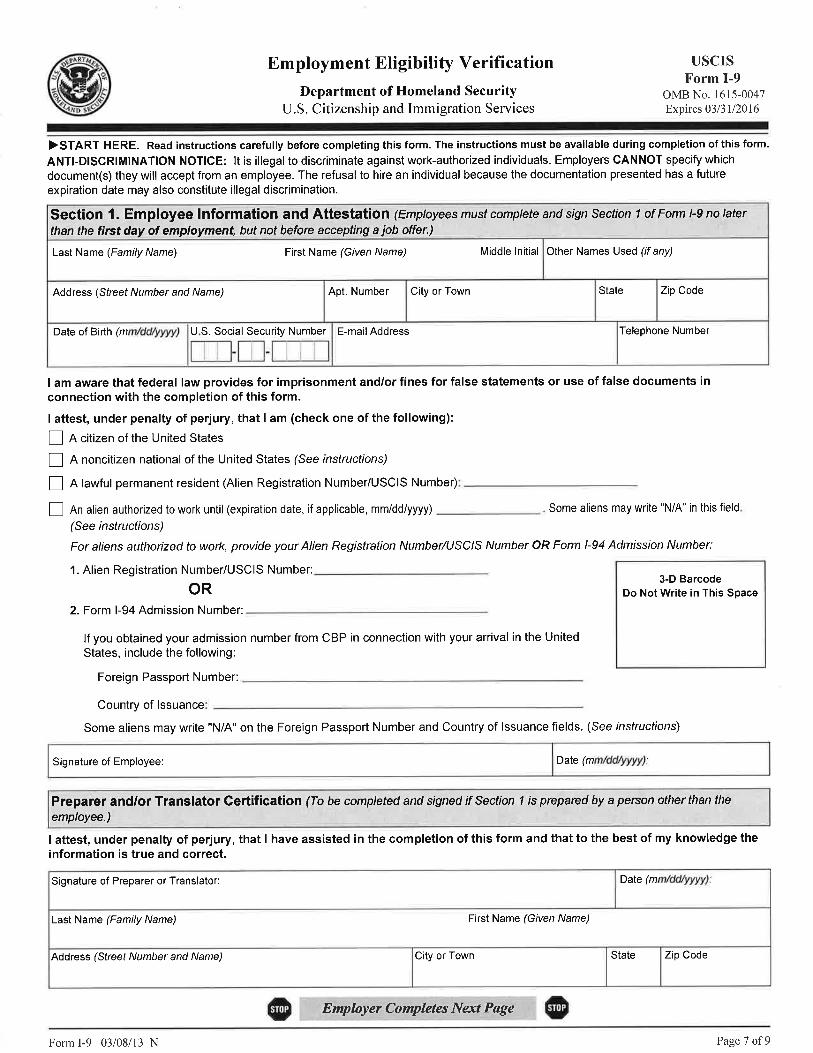
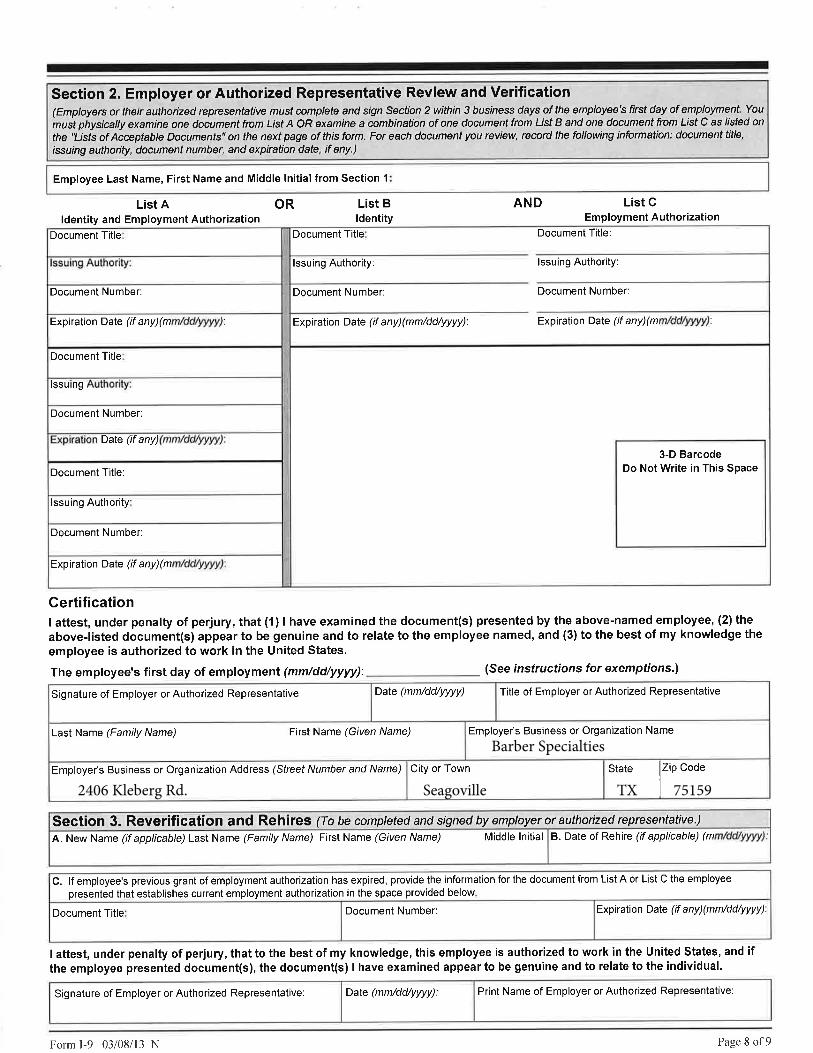
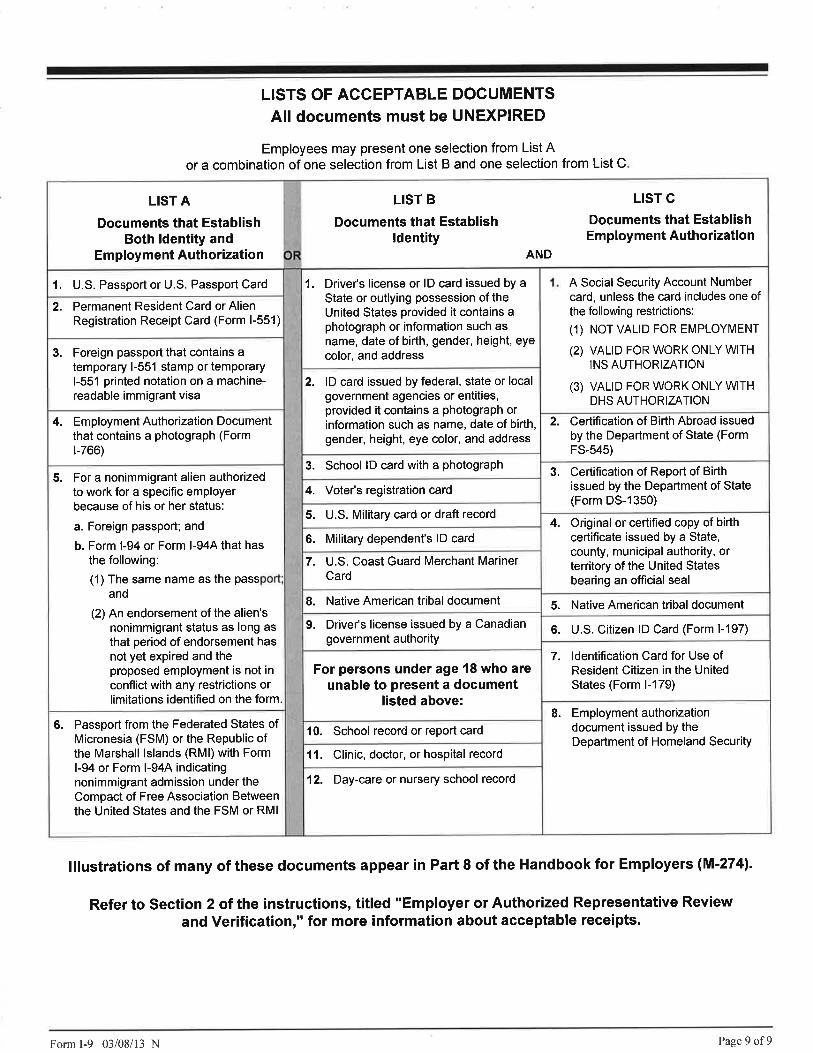
o a. I-9 Form
b. Photocopies of D.L. & SS Card, or other documents must be submitted with I-9 documents
o Direct Deposit (IF CLIENT HAS REQUESTED SERVICES AND HAS BEEN APPROVED.)
o Benefit Election Form
o Medical Health Insurance Application
o Dental & Vision Insurance Application
o Life Insurance Application
o Employee Handbook (IF REQUESTED BY CLIENT)
The following forms must be completed before an employee can be added to payroll:
Barber Specialties
The following is a list of forms that will need to be completed before we can add an employee. Please make
sure that you obtain the photo copies of the required documentation that will need to be submitted with
each I-9. If you have any questions, regarding any of the forms, please do not hesitate to contact your
Client Resources Manager. This page must also accompany the below requested documents.
Rev: 4/16/03 NEW WSE Checklist 1/1
EMPLOYEE ENROLLMENT
Client Name: Client #: 1057
Name:(Nombre) Last/Apellido First/Nombre Middle/Inicial Suffix Employee #
Social Security #:(Seguro Social)
Address:(Dirección) City/Ciudad State/Estado Zip/Coligo Postal
Date Of Birth: Home Telephone:(Fecha De Nacimiento)
Emergency
Contact Name: Emergency Phone Number:
_____________________________________________________
Vietnam Veteran: No Yes Disabled:
Ethnic Code:
KEY Effective Date: Original Hire Date:
Position: Department: Division:
Comp Code: EEO Job Class: 6. Craft Workers (skilled)
2. Professions 7. Operatives (semi-skilled)
Full Time Part Time 3. Technicians 8. Laborers (unskilled)
4. Sales 9. Service Workers
5. Office and Clerical
Hourly $ (per hour)
Commission $$ or % Other Pay: Type $$
Weekly Bi-Weekly Semi Monthly Monthly
Amount Vacation Accruals: No Yes
$
$ Sick Time Accruals: No Yes
$
$
Payroll Deductions:
Type *
* If there are Child Support or Garnishments, please send a copy of the court order.
No Yes
White Black Hispanic American Indian/Alaskan Native Asian, Pacific Island
1. Officials & Managers
Tips No Yes
Normal Hours(per pay period)
Temporary Full Time Temporary Part Time
Salary (per pay period)
Month/Mes Day/Dia Year/Ano (Telefono) Area Code/Numero del AreaNumber/Numero
Street/Numero y Calle Apt. #
2. It is essential that you provide your supervisor the required identification to complete the I-9 form.
Barber Specialties
3. Key Business Solutions will be unable to continue to employ anyone that cannot provide the required identification.
Male Female
SECTION 1 - To be completed by employee
(Your name must EXACTLY match the name printed on Social Security card.)
This packet contains paperwork that is essential in processing your paychecks. Please read the information below before completing the
attached new hire paperwork.
1. Please read and complete all areas.
SECTION 2 - To be completed by Client Worksite Employer
KEY is an Equal Opportunity Employer. To help us comply with government record keeping requirements, we would appreciate
your completing the following information. You are not required to provide this information. If you choose not to provide the information, your decision will not
affect your application. This data will be kept confidential, and will only be used in accordance with applicable state and federal laws and regulations.
Relationship to
Employee: Email:__________________
Rev. 4/16/03 Employee Enrollment/Key New Employee Enrollment 1/1
EMPLOYEE ACKNOWLEDGEMENT
Rev. 5/06 KEY Employee Acknowledgment 1/4
SECTION 1: ACKNOWLEDGEMENT I accept Key Business Solutions (hereinafter called Company) as my alternative employer for Workers’ Compensation benefits and I understand and agree to my status as a leased employee of Company. I agree to conform to the rules and regulations of Company. I understand that I can leave the employment of Company with or without notice and with or without cause, and Company reserves the same rights. I understand and agree that at all times I will hold my employment as an at-will employee of Company. Upon separation of employment, I agree to contact KEY Human Resources department within 24 to 72 hours after employment has ended at 1-877-878.6463. Failure to do so may affect any claim I have for unemployment compensation. I understand and agree that, if applicable, Company may allocate tips when necessary, on the basis of “hours worked.” Tip allocation becomes necessary when total reported tips for the store are less than 8% of store sales. I understand that, if I am a tipped employee, if applicable, Company is taking a tip credit on my hourly rate of pay as permitted by law. _________Initial SECTION 2: HARASSMENT POLICY Sexual harassment is a form of sex discrimination prohibited by Title VII of the 1964 Civil Rights Act. It is the policy of this Company not to condone or permit sexual harassment. Sexual harassment includes unwelcome sexual advances or requests for sexual favors, unwelcome verbal or physical conduct of a sexual nature, or any other unwelcome sexual conduct that has the purpose or effect or unreasonably interfering with an affected person’s work performance or creating an intimidating, hostile or offensive work environment. In addition, it is sexual harassment to indicate that submission to or rejection of unwelcome sexual conduct is either explicitly or implicitly a term or condition of employment, or utilizing submission to or rejection of such conduct as a basis for an employment decision affecting the person submitting to or rejecting the conduct. Any person who after a full investigation of any allegation of sexual harassment is found to have committed an act of sexual harassment will be disciplined and, in appropriate situations, terminated from employment. Any employee who feels that he or she may have subjected to sexual harassment or to any type of discrimination or harassment prohibited by local, state, or federal law (including but limited to race, sex, color, age, religion, disability, or national origin) in the workplace must report it immediately to the Human Resources Director at Company. All allegations of sexual harassment and other types of discrimination will be investigated promptly and thoroughly and proper remedial action will be taken according to the specific circumstances of the situation. I understand that the failure to promptly report an allegation of sexual harassment or discrimination may result in the waiver of any rights, which I may have under Title VII or any other federal, state or local law. All investigations of alleged sexual harassment and other types of discrimination are strictly confidential. Federal, state and local law prohibits the taking of adverse employment action in retaliation for reporting an incident of sexual harassment or other types of discrimination. __________Initial SECTION 3: ACKNOWLEDGEMENT OF THE DRUG FREE WORKPLACE PROGRAM Testing 3.01 DEFINITION For the purpose of this policy, “drug” is defined as any alcoholic beverage, illegal inhalant, illegal drug or other substance, the use, possession, manufacture, distribution or dispensation of which is prohibited by any state or federal law or regulation and any drug or substance obtained by prescription, over-the-counter or otherwise. 3.02 TESTING PROCEDURES a). Upon The Company’s request for an employee to undergo drug testing, the employee shall execute a drug testing consent form. b). Drug testing requires that the employee submit a urine sample for laboratory analysis to detect drugs. Testing for alcohol use requires a blood sample. In addition, any other accepted and reasonable testing method may be used for alcohol or drug testing.
EMPLOYEE ACKNOWLEDGEMENT
Rev. 5/06 KEY Employee Acknowledgment 2/4
c). Testing will be conducted by a laboratory or medical facility designated by The Company. All costs for testing shall be paid by The Company. d). Refusal to submit to a drug or alcohol test shall result in the same consequences as a positive drug or alcohol screen as outlined in paragraph 3.04. 3.03 APPLICABILITY OF DRUG TESTING a). All persons applying for a position with The Company may be required to submit to a drug test as a condition of employment. b). All current and future employees must submit to a drug test upon the request of The Company under the following circumstances:
1. When special safety considerations attendant to certain jobs indicate that such testing presents a reasonable means to assure a safe working environment;
2. When the employee either sustains an injury in the course and scope of employment or contributes to or causes another employee to sustain injury in the course and scope of employment;
3. When the employee causes, indirectly or directly, damage to The Company’s property or to the property of another;
4. When the employee contributes or causes injury to any third party while the employee is in the course and scope of employment;
5. When the employee is convicted under any criminal drugs statute for a violation occurring during the course and scope of employment. If such a conviction occurs, it is the employee’s responsibility to notify The Company within five (5) days of conviction. This requirement includes any finding of guilt, guilty plea, plea of no contest or imposition of sentence or any other penalty whatsoever by any court or competent jurisdiction or otherwise in connection with any state or federal criminal statute involving the manufacture, distribution, dispensation, use or possession of any controlled substance or drug, including alcohol;
6. When The Company, in its sole discretion, determines that it is in The Company’s best interest to conduct such a drug test.
3.04 POSITIVE RESULTS a). If a test result is Positive, it shall be verified by an alternate method of testing using only the initial lab sample. The test result, if positive, shall be reported directly to the applicant. b). If the applicant or employee believes the test result is inaccurate, the applicant or employee shall have an immediate opportunity to fully and fairly explain why the applicant or employee believes the test result is inaccurate. c). If the applicant or employee refuses to contest the test results, or if The Company finds the applicant or employees explanation was unsatisfactory, the initial test result will be deemed conclusive. d). If an applicant’s positive test result is deemed conclusive, the applicant shall be refused employment by The Company. If an employee’s positive test result is deemed conclusive, the employee shall be subject to disciplinary action, up to and including termination of employment. e). The Company shall not be responsible for, and makes no representations or warranties on behalf of, the laboratory or medical facility conducting the drug test. 3.05 TREATMENT POLICY The Company encourages all employees needing treatment to voluntarily participate in any available drug assistance and or treatment programs.
EMPLOYEE ACKNOWLEDGEMENT
Rev. 5/06 KEY Employee Acknowledgment 3/4
3.06 TREATMENT PROGRAMS
Company may provide each employee a list of available drug counseling, rehabilitation and/or assistance programs. The Company makes no representations or warranties express or implied, about the kind or quality of services offered by the entities, individuals contained in the list available drug treatment programs. __________Initial SECTION 4: MISCELLANEOUS PROVISIONS 4.01 COOPERATION WITH LAW ENFORCEMENT In addition, any illegal drug or other substance obtained by The Company from any employee may be turned over to a law enforcement agency, and may result in criminal prosecution. 4.02 REPORTING Each employee is responsible for promptly reporting to the appropriate Company officers any use of prescribed medication, which may affect the employee’s judgment, performance, or behavior. 4.03 OTHER PROCEDURES The Company will establish such other procedures as it finds necessary to effectively enforce this Policy. This may include a requirement that employees cooperate with personal or facility searches when there is reason to believe drugs or alcohol are present, when their performance is impaired or when their behavior is erratic. Refusing to cooperate with these procedures may cause for disciplinary action as provided in Section 2. __________Initial SECTION 5: ACCIDENTS/INJURIES PROCEDURES
The following procedures must be followed for all work related injuries: a). ALL ACCIDENTS/INJURIES must be reported to your foreman or supervisor, even is no medical attention is required. A Report of Employee Injury/Accident must be completed by the injured employee, whether or not medical attention is required. It will be placed in their medical file for future reference in case of problems.
b). A Supervisor’s Report of Accident must be completed by the supervisor, i.e. the person you report to on your assignment, at the same time the employees accident report is being filled out, regardless of whether medical attention is required. Both reports need to be faxed to the corporate office.
c). If the injury requires medical attention and is not an emergency situation, have your supervisor call the corporate office prior to going to a medical facility. In the case of an emergency, have your supervisor call and report which medical facility you are being transported to. We need to authorize treatment, arrange for proper billing, and determine that the facility follows proper procedures.
d). If an employee must be off on disability, he/she must notify their corporate office supervisor. If off for an extended period of time, the employee must go by the Company office or call at least once a week to advise of their status. Upon receiving a release to return to work, you must call the office to report your availability.
e). Anytime an employee is on light duty, the doctor’s restriction must be followed. The employee may return to regular duties only when released in writing by the doctor. It is your responsibility to tell the doctor that the company has all types of light duty work.
f). A drug screen is required for all injuries. In accordance with state law, a positive result in the same consequences as a positive drug or alcohol test.
EMPLOYEE ACKNOWLEDGEMENT
Rev. 5/06 KEY Employee Acknowledgment 4/4
g). I understand and agree to abide by the above accident procedures. I understand that any payments to me or anyone else for expenses in connection with my accident and resulting injury is not an admission of liability on the part of The Company. __________Initial RECEIPT & ACKNOWLEGEMENT OF EMPLOYEE POLICIES AND PROCEDURES Instructions: Please read the Employee Policies and Procedures carefully. If you do not understand any portion of it, ask for an explanation from Company Humans Resources Director. Please keep this policy and procedure for future reference. I, the undersigned employee, acknowledge by my signature that I have been informed that I am an assigned employee of KEY (hereinafter Company). I acknowledge that I have received, read, and had ample opportunity to understand the contents of the employee policy and procedure. I understand that this policy and procedure does not establish any contractual relationship; that its provisions, including wages, hours, benefits and terms and conditions of employment, may be changed at any time by management, and that this policy and procedure is not a guarantee of future or present employment policies. I further understand that neither this policy and procedure nor any verbal or written statement by any supervisory or managerial official of Company or any Client is an employment contract or offer of contract and that either Company or I can terminate our employment relationship at any time as I am an at-will employee of Company. Furthermore, I agree that if at any time during my employment I am subjected to any type of discrimination, including discrimination because of race, color, religion, national origin, age, sex, or disability, or if I am subjected to any type of harassment, including sexual harassment, I will immediately contact Company Human Resources Director in order to obtain assistance in the resolution of such matters. I acknowledge receipt of a copy of this policy summary. _____________________ _________________________________ _______________________________
Date Signature Printed Name
Worksite Employer Name: Barber Specialties Client #: 1057 KEY Business Solutions 7475 Skillman St. c/102 Dallas, TX 75231
Form W-4 (2016)Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes.Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2016 expires February 15, 2017. See Pub. 505, Tax Withholding and Estimated Tax.Note: If another person can claim you as a dependent on his or her tax return, you cannot claim exemption from withholding if your income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends).
Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee:• Is age 65 or older,
• Is blind, or
• Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return.
The exceptions do not apply to supplemental wages greater than $1,000,000.Basic instructions. If you are not exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations.
Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages.Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information.Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances.
Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P.Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details.Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form.Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for 2016. See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married).Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at www.irs.gov/w4.
Personal Allowances Worksheet (Keep for your records.)A Enter “1” for yourself if no one else can claim you as a dependent . . . . . . . . . . . . . . . . . . A
B Enter “1” if: { • You are single and have only one job; or• You are married, have only one job, and your spouse does not work; or . . .• Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.
} B
C Enter “1” for your spouse. But, you may choose to enter “-0-” if you are married and have either a working spouse or more than one job. (Entering “-0-” may help you avoid having too little tax withheld.) . . . . . . . . . . . . . . C
D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return . . . . . . . . D
E Enter “1” if you will file as head of household on your tax return (see conditions under Head of household above) . . E
F Enter “1” if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit . . . F
(Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.) G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information.
• If your total income will be less than $70,000 ($100,000 if married), enter “2” for each eligible child; then less “1” if you have two to four eligible children or less “2” if you have five or more eligible children. • If your total income will be between $70,000 and $84,000 ($100,000 and $119,000 if married), enter “1” for each eligible child . . G
H Add lines A through G and enter total here. (Note: This may be different from the number of exemptions you claim on your tax return.) H
For accuracy, complete all worksheets that apply.
{• If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions and Adjustments Worksheet on page 2.
• If you are single and have more than one job or are married and you and your spouse both work and the combined earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to avoid having too little tax withheld.• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
Separate here and give Form W-4 to your employer. Keep the top part for your records.
Form W-4Department of the Treasury Internal Revenue Service
Employee's Withholding Allowance Certificate Whether you are entitled to claim a certain number of allowances or exemption from withholding is
subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
OMB No. 1545-0074
20161 Your first name and middle initial Last name
Home address (number and street or rural route)
City or town, state, and ZIP code
2 Your social security number
3 Single Married Married, but withhold at higher Single rate.
Note: If married, but legally separated, or spouse is a nonresident alien, check the “Single” box.
4 If your last name differs from that shown on your social security card,
check here. You must call 1-800-772-1213 for a replacement card.
5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5
6 Additional amount, if any, you want withheld from each paycheck . . . . . . . . . . . . . . 6 $
7 I claim exemption from withholding for 2016, and I certify that I meet both of the following conditions for exemption.• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and
• This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.If you meet both conditions, write “Exempt” here . . . . . . . . . . . . . . . 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature
(This form is not valid unless you sign it.) Date
8 Employer’s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No. 10220Q Form W-4 (2016)
Key Business Solutions * 7475 Skillman Street Suite C/102 * Dallas, TX 75231
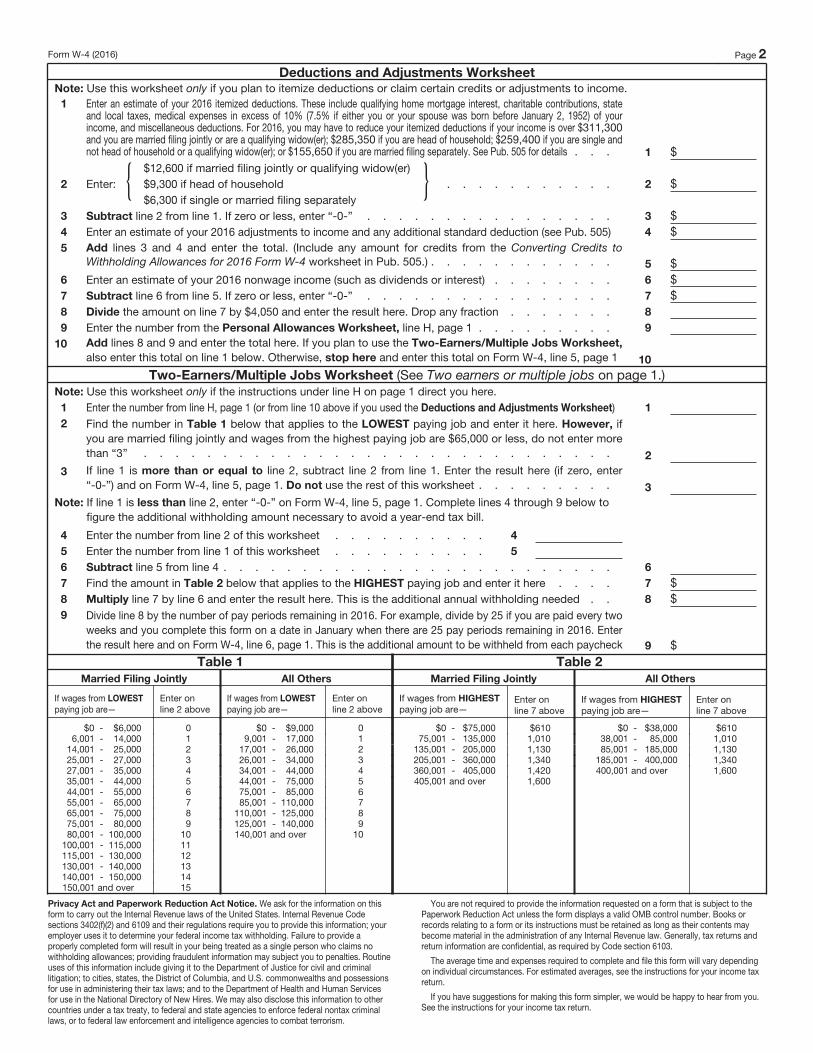
Form W-4 (2016) Page 2
Deductions and Adjustments Worksheet
Note: Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income.1 Enter an estimate of your 2016 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state
and local taxes, medical expenses in excess of 10% (7.5% if either you or your spouse was born before January 2, 1952) of your income, and miscellaneous deductions. For 2016, you may have to reduce your itemized deductions if your income is over $311,300 and you are married filing jointly or are a qualifying widow(er); $285,350 if you are head of household; $259,400 if you are single and not head of household or a qualifying widow(er); or $155,650 if you are married filing separately. See Pub. 505 for details . . . 1 $
2 Enter: { $12,600 if married filing jointly or qualifying widow(er)$9,300 if head of household . . . . . . . . . . .$6,300 if single or married filing separately
} 2 $
3 Subtract line 2 from line 1. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . 3 $4 Enter an estimate of your 2016 adjustments to income and any additional standard deduction (see Pub. 505) 4 $5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to
Withholding Allowances for 2016 Form W-4 worksheet in Pub. 505.) . . . . . . . . . . . . 5 $6 Enter an estimate of your 2016 nonwage income (such as dividends or interest) . . . . . . . . 6 $7 Subtract line 6 from line 5. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . 7 $8 Divide the amount on line 7 by $4,050 and enter the result here. Drop any fraction . . . . . . . 8
9 Enter the number from the Personal Allowances Worksheet, line H, page 1 . . . . . . . . . 9
10 Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet,
also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10
Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.)Note: Use this worksheet only if the instructions under line H on page 1 direct you here.1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than “3” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter “-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet . . . . . . . . . 3
Note: If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill.
4 Enter the number from line 2 of this worksheet . . . . . . . . . . 4
5 Enter the number from line 1 of this worksheet . . . . . . . . . . 5
6 Subtract line 5 from line 4 . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here . . . . 7 $8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed . . 8 $9 Divide line 8 by the number of pay periods remaining in 2016. For example, divide by 25 if you are paid every two
weeks and you complete this form on a date in January when there are 25 pay periods remaining in 2016. Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $
Table 1
Married Filing Jointly
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $6,000 06,001 - 14,000 1
14,001 - 25,000 225,001 - 27,000 327,001 - 35,000 435,001 - 44,000 544,001 - 55,000 655,001 - 65,000 765,001 - 75,000 875,001 - 80,000 980,001 - 100,000 10
100,001 - 115,000 11115,001 - 130,000 12130,001 - 140,000 13140,001 - 150,000 14 150,001 and over 15
All Others
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $9,000 09,001 - 17,000 1
17,001 - 26,000 226,001 - 34,000 334,001 - 44,000 444,001 - 75,000 575,001 - 85,000 685,001 - 110,000 7
110,001 - 125,000 8125,001 - 140,000 9140,001 and over 10
Table 2
Married Filing Jointly
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $75,000 $61075,001 - 135,000 1,010
135,001 - 205,000 1,130205,001 - 360,000 1,340360,001 - 405,000 1,420405,001 and over 1,600
All Others
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $38,000 $61038,001 - 85,000 1,01085,001 - 185,000 1,130
185,001 - 400,000 1,340400,001 and over 1,600
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this
form to carry out the Internal Revenue laws of the United States. Internal Revenue Code
sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism.
You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return.
If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
Barber Specialties
2406 Kleberg Rd. Seagoville TX 75159
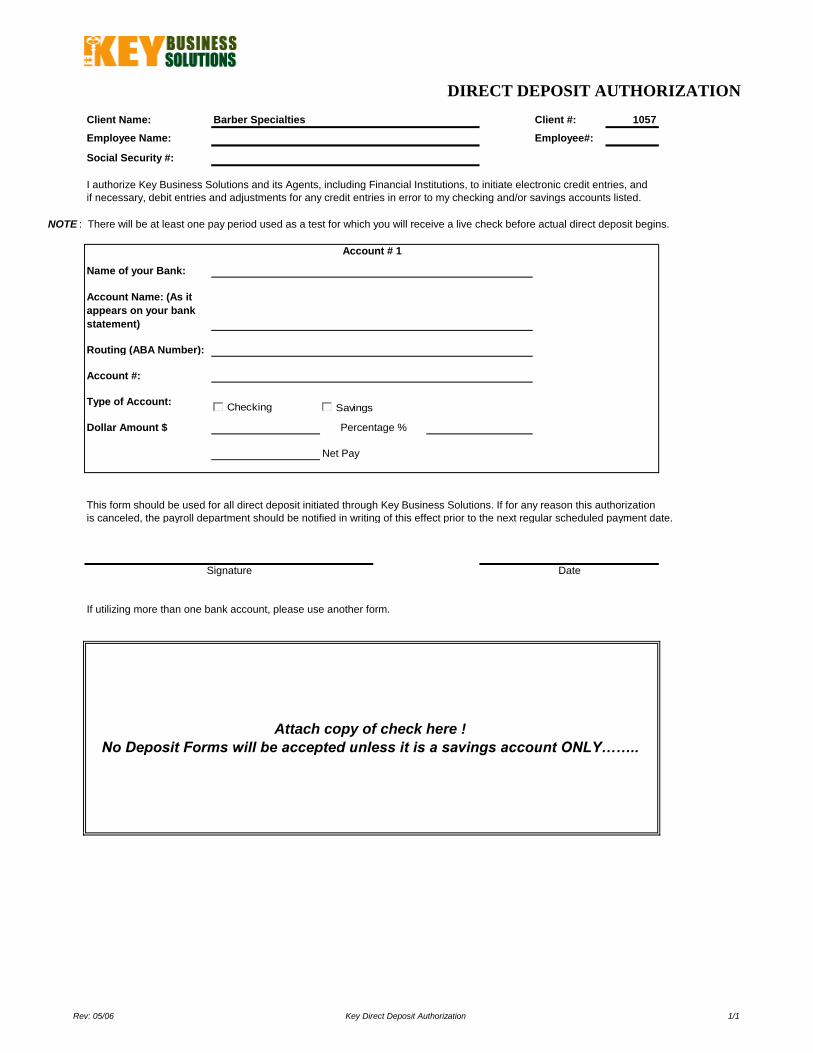
DIRECT DEPOSIT AUTHORIZATION
Client Name: Barber Specialties Client #: 1057
Employee Name: Employee#:
Social Security #:
NOTE : There will be at least one pay period used as a test for which you will receive a live check before actual direct deposit begins.
Name of your Bank:
Routing (ABA Number):
Account #:
Type of Account:
Dollar Amount $
Net Pay
This form should be used for all direct deposit initiated through Key Business Solutions. If for any reason this authorization
is canceled, the payroll department should be notified in writing of this effect prior to the next regular scheduled payment date.
If utilizing more than one bank account, please use another form.
Attach copy of check here !
No Deposit Forms will be accepted unless it is a savings account ONLY……..
I authorize Key Business Solutions and its Agents, including Financial Institutions, to initiate electronic credit entries, and
if necessary, debit entries and adjustments for any credit entries in error to my checking and/or savings accounts listed.
Percentage %
Account # 1
Signature Date
Account Name: (As it
appears on your bank
statement)
Checking Savings
Rev: 05/06 Key Direct Deposit Authorization 1/1
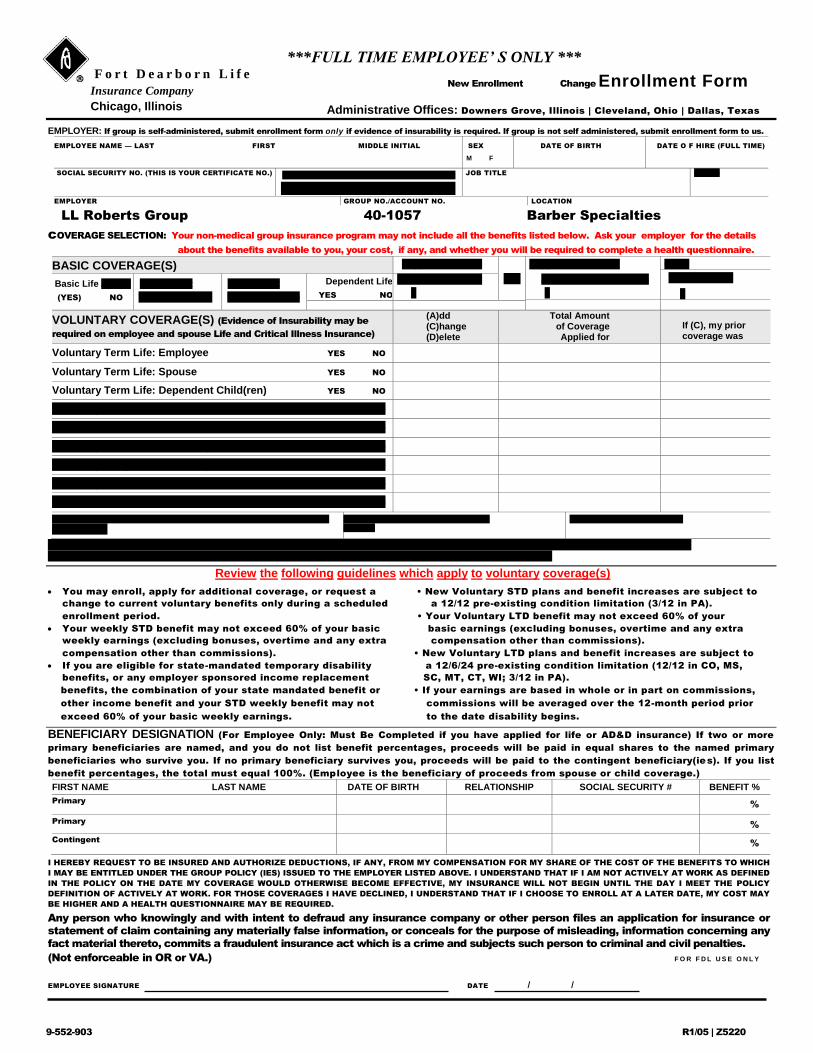
***FULL TIME EMPLOYEE’ S ONLY *** F o r t D e a r b o r n L i f e
Insurance Company
Chicago, Illinois
New Enrollment Change Enrollment Form
Administrative Offices: Downers Grove, Illinois | Cleveland, Ohio | Dallas, Texas
EMPLOYER: If group is self-administered, submit enrollment form only if evidence of insurability is required. If group is not self administered, submit enrollment form to us.
EMPLOYEE NAME — LAST FIRST MIDDLE INITIAL SEX
M F
DATE OF BIRTH DATE O F HIRE (FULL TIME)
SOCIAL SECURITY NO. (THIS IS YOUR CERTIFICATE NO.) EARNINGS Weekly
$ Monthly Annual
JOB TITLE CLASS
EMPLOYER GROUP NO./ACCOUNT NO. LOCATION
LL Roberts Group 40-1057 Barber Specialties
cOVERAGE SELECTION: Your non-medical group insurance program may not include all the benefits listed below. Ask your employer for the details
about the benefits available to you, your cost, if any, and whether you will be required to complete a health questionnaire.
BASIC COVERAGE(S) Supplemental Life
Del.
Supplemental AD&D Other
Yes No
$
Basic Life /AD&D
(YES) NO
STD Benefit
YES NO
LTD Benefit
YES NO
Dependent Life
YES NO
Add Change
$
Add Change Del.
$
VOLUNTARY COVERAGE(S) (Evidence of Insurability may be
required on employee and spouse Life and Critical Illness Insurance)
(A)dd (C)hange (D)elete
Total Amount of Coverage Applied for
If (C), my prior coverage was
Voluntary Term Life: Employee YES NO
Voluntary Term Life: Spouse YES NO
Voluntary Term Life: Dependent Child(ren) YES NO
Voluntary AD&D: Individual Plan YES NO
Voluntary AD&D: Family Plan YES NO
Voluntary Short-Term Disability YES NO
Voluntary Long-Term Disability YES NO
Voluntary Critical Illness with Cancer Benefit YES NO
Voluntary Critical Illness without Cancer Benefit YES NO
SPOUSE NAME — LAST FIRST M.I.
(if applicant)
SEX SPOUSE DATE OF BIRTH
M F
SPOUSE SOCIAL SECURITY #
Has Employee (if applicant) used cigarettes or other tobacco products Has Spouse (if applicant) used cigarettes or other tobacco products
in the last 2 years? YES NO in the last 2 years? YES NO
Review the following guidelines which apply to voluntary coverage(s)
You may enroll, apply for additional coverage, or request a • New Voluntary STD plans and benefit increases are subject to
change to current voluntary benefits only during a scheduled a 12/12 pre-existing condition limitation (3/12 in PA).
enrollment period. • Your Voluntary LTD benefit may not exceed 60% of your
Your weekly STD benefit may not exceed 60% of your basic basic earnings (excluding bonuses, overtime and any extra
weekly earnings (excluding bonuses, overtime and any extra compensation other than commissions).
compensation other than commissions). • New Voluntary LTD plans and benefit increases are subject to
If you are eligible for state-mandated temporary disability a 12/6/24 pre-existing condition limitation (12/12 in CO, MS,
benefits, or any employer sponsored income replacement SC, MT, CT, WI; 3/12 in PA).
benefits, the combination of your state mandated benefit or • If your earnings are based in whole or in part on commissions,
other income benefit and your STD weekly benefit may not commissions will be averaged over the 12-month period prior
exceed 60% of your basic weekly earnings. to the date disability begins.
BENEFICIARY DESIGNATION (For Employee Only: Must Be Completed if you have applied for life or AD&D insurance) If two or more
primary beneficiaries are named, and you do not list benefit percentages, proceeds will be paid in equal shares to the named primary
beneficiaries who survive you. If no primary beneficiary survives you, proceeds will be paid to the contingent beneficiary(ies). If you list
benefit percentages, the total must equal 100%. (Employee is the beneficiary of proceeds from spouse or child coverage.)
FIRST NAME LAST NAME DATE OF BIRTH RELATIONSHIP SOCIAL SECURITY # BENEFIT %
Primary %
Primary %
Contingent %
I HEREBY REQUEST TO BE INSURED AND AUTHORIZE DEDUCTIONS, IF ANY, FROM MY COMPENSATION FOR MY SHARE OF THE COST OF THE BENEFITS TO WHICH
I MAY BE ENTITLED UNDER THE GROUP POLICY (IES) ISSUED TO THE EMPLOYER LISTED ABOVE. I UNDERSTAND THAT IF I AM NOT ACTIVELY AT WORK AS DEFINED
IN THE POLICY ON THE DATE MY COVERAGE WOULD OTHERWISE BECOME EFFECTIVE, MY INSURANCE WILL NOT BEGIN UNTIL THE DAY I MEET THE POLICY
DEFINITION OF ACTIVELY AT WORK. FOR THOSE COVERAGES I HAVE DECLINED, I UNDERSTAND THAT IF I CHOOSE TO ENROLL AT A LATER DATE, MY COST MAY
BE HIGHER AND A HEALTH QUESTIONNAIRE MAY BE REQUIRED.
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or
statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any
fact material thereto, commits a fraudulent insurance act which is a crime and subjects such person to criminal and civil penalties.
(Not enforceable in OR or VA.) F O R F D L U S E O N L Y
EMPLOYEE SIGNATURE DATE / /
9-552-903 R1/05 | Z5220
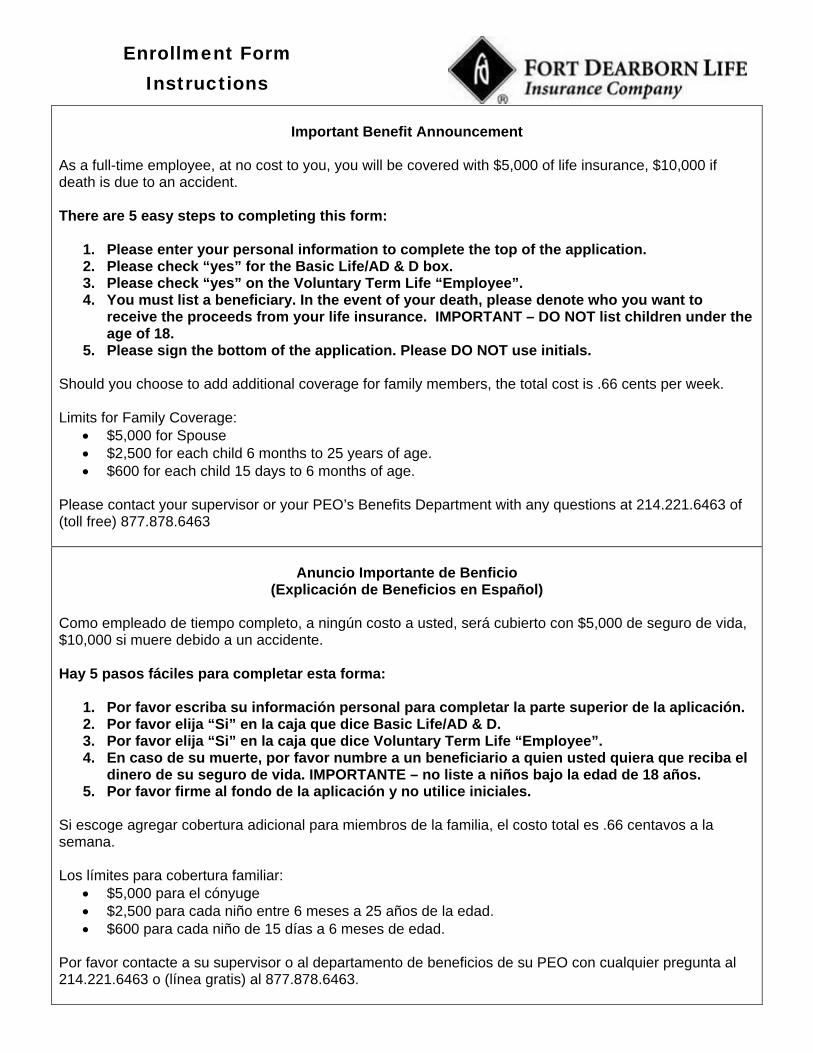
Enrollment Form Instructions
Important Benefit Announcement
As a full-time employee, at no cost to you, you will be covered with $5,000 of life insurance, $10,000 if death is due to an accident. There are 5 easy steps to completing this form:
1. Please enter your personal information to complete the top of the application. 2. Please check “yes” for the Basic Life/AD & D box. 3. Please check “yes” on the Voluntary Term Life “Employee”. 4. You must list a beneficiary. In the event of your death, please denote who you want to
receive the proceeds from your life insurance. IMPORTANT – DO NOT list children under the age of 18.
5. Please sign the bottom of the application. Please DO NOT use initials. Should you choose to add additional coverage for family members, the total cost is .66 cents per week. Limits for Family Coverage:
$5,000 for Spouse $2,500 for each child 6 months to 25 years of age. $600 for each child 15 days to 6 months of age.
Please contact your supervisor or your PEO’s Benefits Department with any questions at 214.221.6463 of (toll free) 877.878.6463
Anuncio Importante de Benficio
(Explicación de Beneficios en Español)
Como empleado de tiempo completo, a ningún costo a usted, será cubierto con $5,000 de seguro de vida, $10,000 si muere debido a un accidente. Hay 5 pasos fáciles para completar esta forma:
1. Por favor escriba su información personal para completar la parte superior de la aplicación. 2. Por favor elija “Si” en la caja que dice Basic Life/AD & D. 3. Por favor elija “Si” en la caja que dice Voluntary Term Life “Employee”. 4. En caso de su muerte, por favor numbre a un beneficiario a quien usted quiera que reciba el
dinero de su seguro de vida. IMPORTANTE – no liste a niños bajo la edad de 18 años. 5. Por favor firme al fondo de la aplicación y no utilice iniciales.
Si escoge agregar cobertura adicional para miembros de la familia, el costo total es .66 centavos a la semana. Los límites para cobertura familiar:
$5,000 para el cónyuge $2,500 para cada niño entre 6 meses a 25 años de la edad. $600 para cada niño de 15 días a 6 meses de edad.
Por favor contacte a su supervisor o al departamento de beneficios de su PEO con cualquier pregunta al 214.221.6463 o (línea gratis) al 877.878.6463.
Pre-Employment Application
Rev. 3/10 Key PreEmployment Application.doc 3 of 3
WORK HISTORY: List names of employers in order with present or last employer listed first. Account for all periods of time including military service and any periods of unemployment. If self-employed, give firm name and supply business references. Although a resume may be attached, this section must be completed. PLEASE LIST MONTH AND YEAR List Last Job First
Company Name and Address
Nature of Business
Pay Position and Duties
Reason for Leaving
Supervisor and Phone #
From $ Name
To $ Phone
From $ Name
To $ Phone
From $ Name
To $ Phone
From $ Name
To $ Phone
From $ Name
To $ Phone
List three references, not relatives or former employers. NAME ADDRESS PHONE
I certify that my answers to the foregoing questions are true and correct without any consequential omissions of any kind whatsoever. I understand that if I am employed, any false, and misleading, or otherwise incorrect statements made on this application form or during any interviews may be grounds for my immediate discharge. I hereby authorize KEY BUSINESS SOLUTIONS to contact any company or individual it deems appropriate to investigate my employment history, character and qualifications and I give my full and complete consent to their revealing any and all information they wish as a result of this investigation. In addition, I hereby waive my right to bring any cause of action against those individuals for defamation, invasion of privacy or any other reason because of their statements. I agree that, if I am employed, I will abide by all the rules and regulations of the company. I understand that the taking of drugs and alcohol tests, when given pursuant to company policy, are a condition of continued employment and refusal to take such tests when asked will be grounds for my immediate termination. I further understand that nobody at KEY BUSINESS SOLUTIONS is authorized to enter into any written or verbal employment contracts with me for any definite period of time without the express written consent of the Managing Member of KEY BUSINESS SOLUTIONS. I also understand that my employment is “at-will” and may be terminated by myself or by the company at any time for any reason or no reason at all, with or without prior notice. Signature Date / /