new insights in the “personalized” therapy of nscl cancer paolo marchetti oncologia medica...
TRANSCRIPT

New insights in the
“personalized” therapy of
NSCL cancer
Paolo MarchettiOncologia Medica
Azienda Ospedaliera Sant’Andrea
&IDI IRCCS
Roma
Highlights in the Management of NSCL cancer
June 13-14, 2008
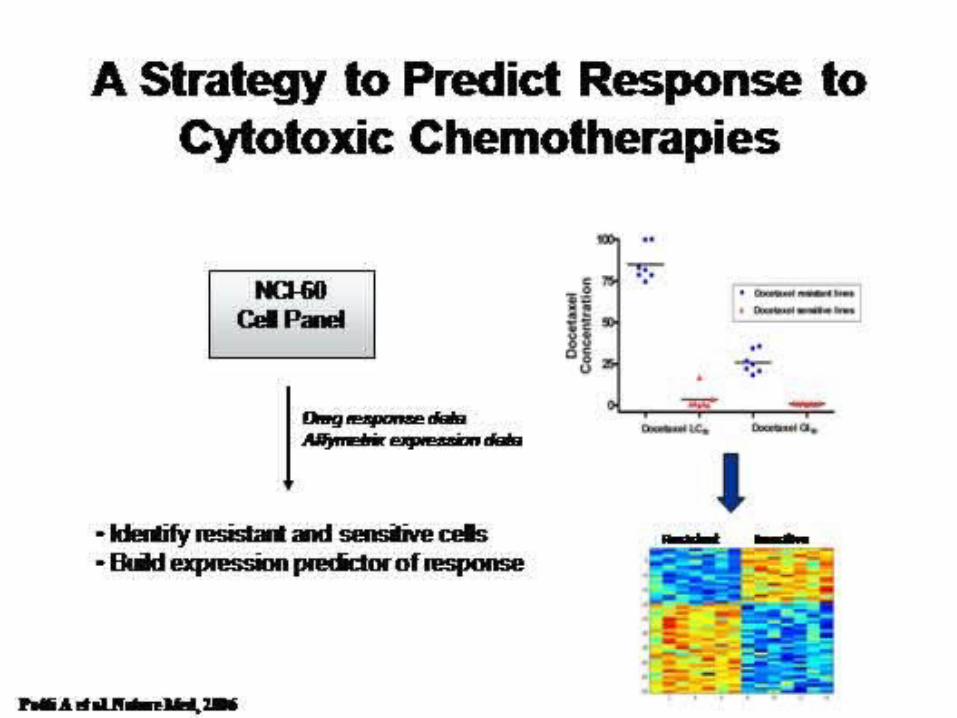
Drug sensitivityThe Clinical Problem
• Protein and/or mRNA levels of several genes are beginning to emerge as predictive markers of chemotherapeutic efficacy in NSCLC.
• Clinical benefit from approved drugs occurs in minority of patients
• Prediction of response not currently possible for most patients and drugs
• Goal:– Selection of most effective treatment– Development of new agents
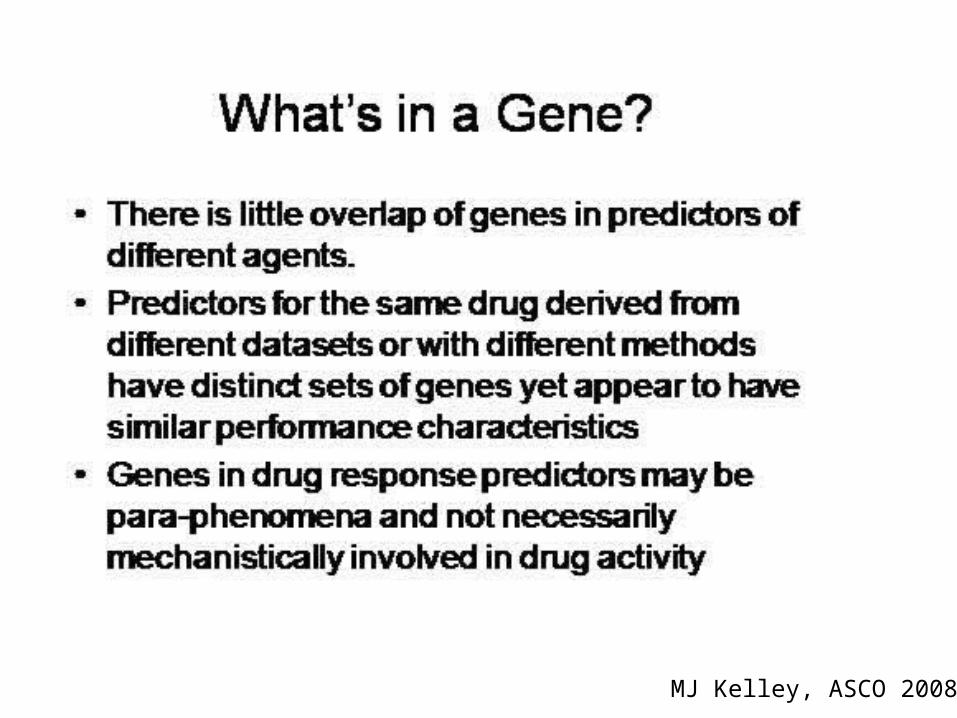
MJ Kelley, ASCO 2008

Drug sensitivityThe Clinical Problem
• Lung cancer guidelines recommend drug options as equivalent– Locally advanced NSCLC
• Cisplatin, carboplatin (--), paclitaxel, docetaxel, vinorelbine, RT + CT
– Untreated advanced NSCLC• Cisplatin, carboplatin (--), paclitaxel, docetaxel, vinorelbine,
gemcitabine, (pemetrexed), or non-platinum doublets
– Previously treted NSCLC• Docetaxel, pemetrexed, erlotinib
MJ Kelley, ASCO 2008

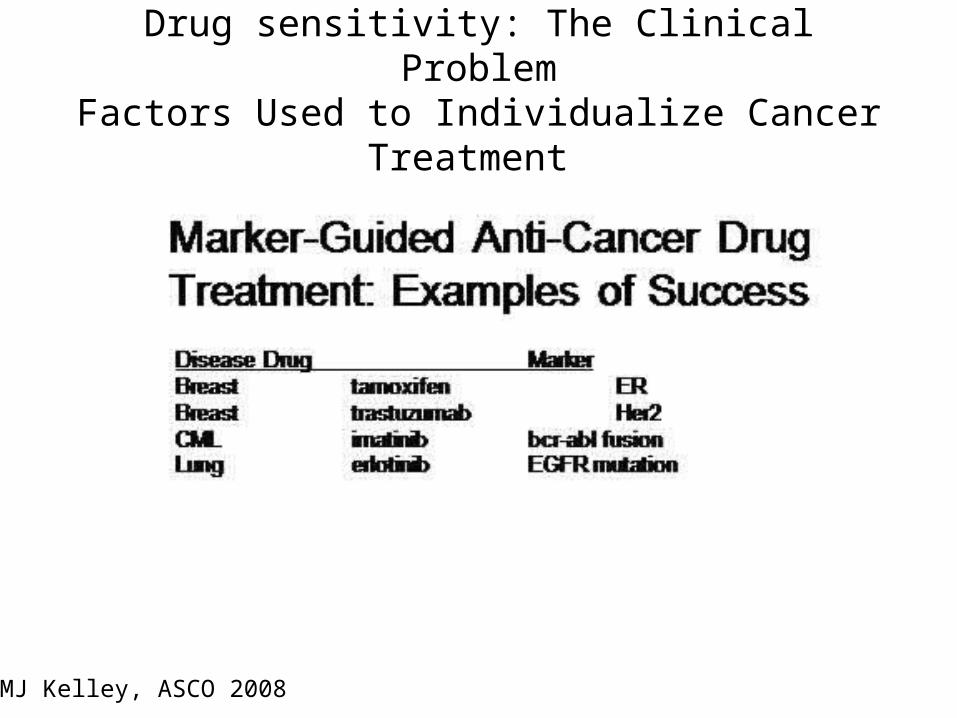
Drug sensitivity: The Clinical ProblemFactors Used to Individualize Cancer Treatment
• Patient factors– Age, sex, race– Performance status– Germline genetics (SNPs,
CNV, mutation)– Co-morbility
• Tumor factors– Size & stage– Histopathology– Biochemical functions (PET
scan)– Microenvironment
(hypoxia, angiogenesis)– Protein expression (IHC,
proteomics)– DNA alterations (mutation,
methylation, telomere length)
– RNA expression– Metabolites
MJ Kelley, ASCO 2008
Drug sensitivity: The Clinical ProblemFactors Used to Individualize Cancer Treatment
MJ Kelley, ASCO 2008

Targeted Therapy
• Assumes we know the target
• Assumes we know how to measure the target
• Assumes we have an agent that blocks or interferes with the target
• Assumes the agent is selective and specific for the target

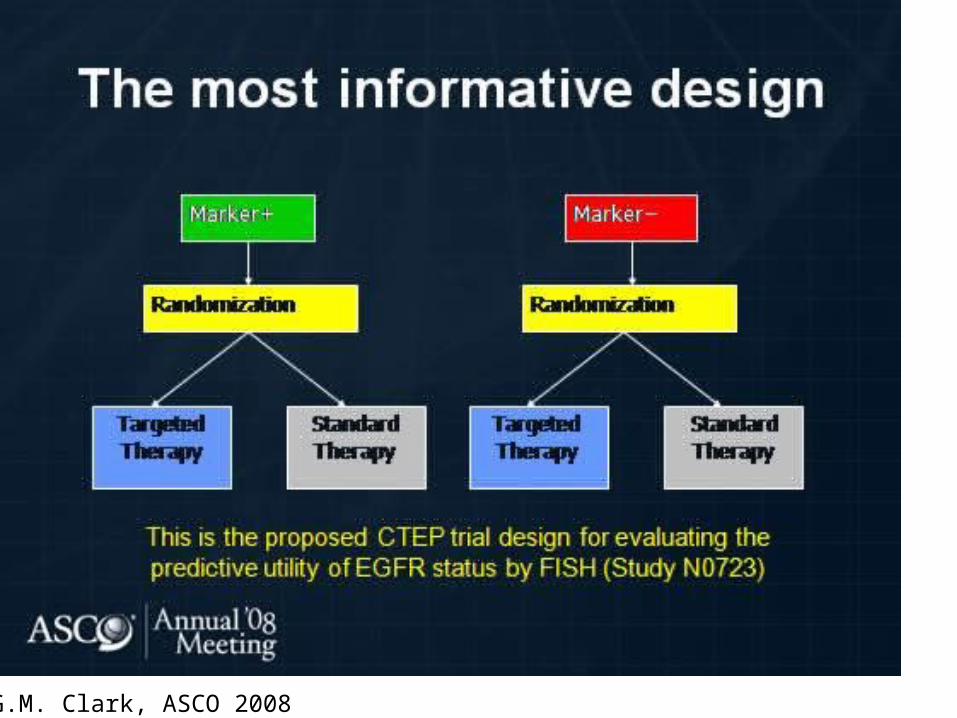
What types of clinical trials should we design?
• Prognostic vs. predictive factors.

Jean-Charles Soria, ASCO 2008

Jean-Charles Soria, ASCO 2008

Jean-Charles Soria, ASCO 2008

Jean-Charles Soria, ASCO 2008

Jean-Charles Soria, ASCO 2008
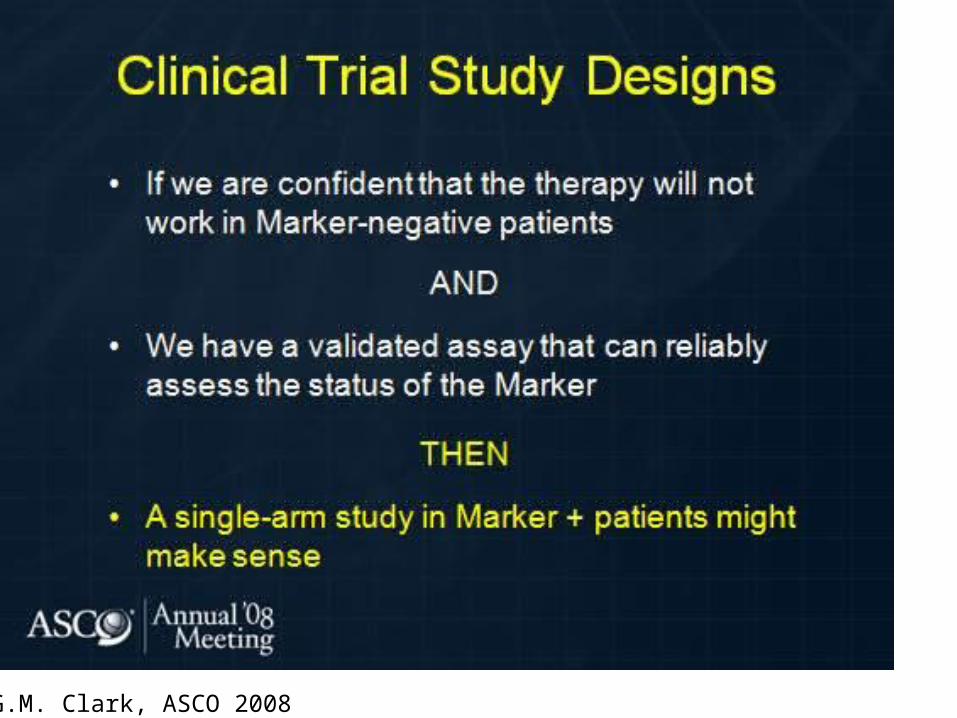
G.M. Clark, ASCO 2008
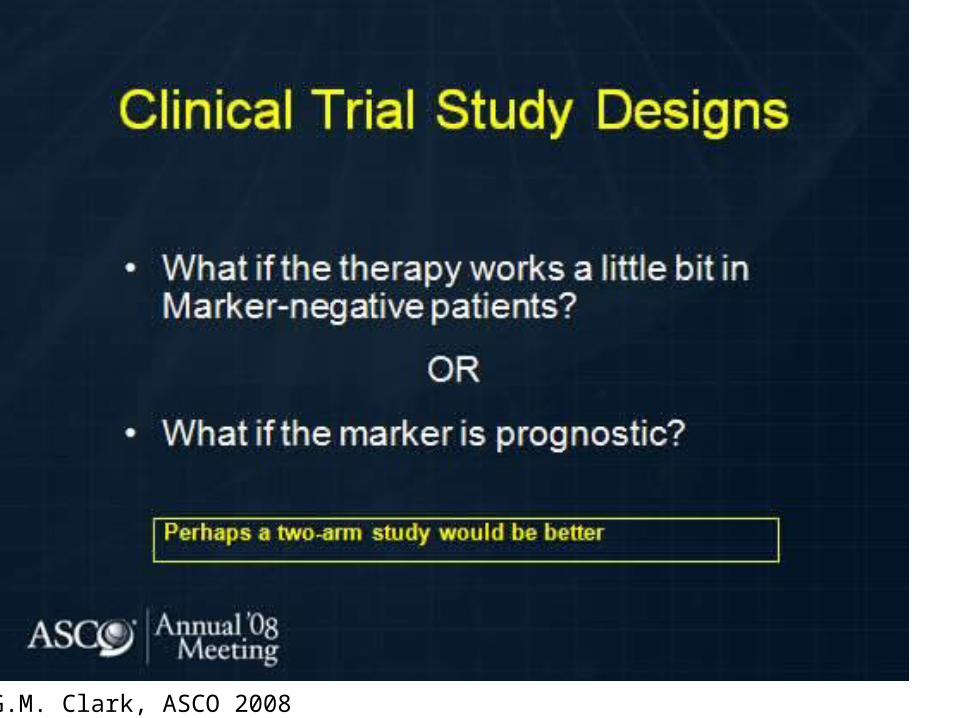
G.M. Clark, ASCO 2008

G.M. Clark, ASCO 2008

G.M. Clark, ASCO 2008

G.M. Clark, ASCO 2008

G.M. Clark, ASCO 2008
G.M. Clark, ASCO 2008

Drug sensitivity: The Clinical ProblemFactors Used to Individualize Cancer Treatment
MJ Kelley, ASCO 2008
Drug sensitivity: The Clinical ProblemFactors Used to Individualize Cancer Treatment
MJ Kelley, ASCO 2008



MJ Kelley, ASCO 2008
MJ Kelley, ASCO 2008
Genes Predictive of Chemotherapeutic Efficacy in NSCLC
• ERCC1, the 5’-endonuclease of the nucleotide excision repair complex, is a molecular determinant for efficacy of platinum-based regimens.
• RRM1, the regulatory subunit of ribonucleotide reductase, is the molecular target of gemcitabine, and its expression levels are the key determinant of the efficacy of gemcitabine-based regimens.
• TS, the gatekeeper enzyme of thymidine production, has seemingly emerged as a determinant of efficacy for not only 5-FU but also for pemetrexed.
• BRCA1, the gene important for DNA damage response, appears to increase efficacy of antimicrotubulin agents such as taxanes while simultaneously mediating resistance to DNAdamaging agents such as platinum.
P.D. – 106
A RT-qPCR-BASED THREE-GENE PROGNOSTIC CLASSIFIER FOR STAGE I
NON-SMALL-CELL LUNG CANCER
Geneva – Friday, 25 April 2008
Guido Natoli, Stefania Scarpino, Annukka Pasanen, Enrico Duranti, Cecilia Pompili, Ida Paris,
Erino Rendina, Luigi Ruco, Paolo Marchetti
(University ‘La Sapienza’ – Rome, Italy)
A RT-qPCR-based three-gene prognostic classifier for Stage I NSCLC
• Despite surgery, patients with pathologic stage I disease have nearly 65% five-year survival after surgery alone and most patients relapse at distant sites.
• However, the role of adjuvant therapy remains controversial. Consequently, the recognition of indicators capable of identifying patients with stage I NSCLC at higher risk for developing recurrent disease may help clinicians to select adjuvant treatments.

A RT-qPCR-based three-gene prognostic classifier for Stage I NSCLC
• With this aim, we evaluated the significance of three genes– ERCC1, excision repair cross-complementation group 1;– LCK, lymphocyte-specific protein tyrosin kinase;– DUSP6 dual-specifity phosphatase 6
• 26 stage I completely resected NSCLC patients using reverse transcription (RT) quantitative polymerase chain reaction (qPCR) from fresh-frozen specimens.
• Then, we evaluated the association between the level of expression and relapse-free survival (RFS) and a risk index was created.

Low Risk High Risk p Test
Age (mean ± sd) 65 ± 12 66 ± 10 0.93 t test
GenderFisher’s exact Male 10 (83%) 13 (93%) 0.58
Female 2 (17%) 1 (7%)
StageFisher’s exact IA 8 (66%) 5 (36%) 0.24
IB 4 (34%) 9 (64%)
Cell type
Chi squared
Adenocarcinoma 8 (68%) 9 (64%)0.95
Squamous cell 2 (16%) 3 (18%)
Uncertain 2 (16%) 2 (18%)

0 12 24 36 48
Months
0.0
0.2
0.4
0.6
0.8
1.0
Re
lapse
-fre
e s
urv
ival
Risk.Group=0Risk.Group=1
Low Risk Group
High Risk Group
Logrank 2p = 0.0339
Kaplan–Meier estimates of relapse-free survival of 26 patients with stage I NSCLC according to the three-gene signatures (Ercc1, Lck and Dusp-6)
as measured by RT-PCR (HR = 3.8; 95% CI = 1.10-10.05)

ERCC-1 specific immunohisto-chemical staining with the use of the 8F1 antibody
Spearman’s correlation between RT-PCR and Immuno-staining to detect ERCC-1 expression: 0.49 (p = 0.01)

LCK immunohistochemical staining (polyclonal antibody) dye tumor-infiltrate instead of tumor-cells

MJ Kelley, ASCO 2008