new jersey department of human services di i i f m di...
TRANSCRIPT

New Jersey Department of Human Services Di i i f M di l A i t d H lth S iDivision of Medical Assistance and Health Services
Medicaid Utilization Reviews
Provider Orientation
2010

AgendaAgenda1. Introductions2. Overview3 Utilization Review3. Utilization Review4. Implementation Plan
Organizational Chart Recruiting Physician Panel Training Technology
5. Meeting with Current Contractor(s)6. Provider Relation
M ti ith H it l A i ti Meeting with Hospital Association Mailings/Meetings
7. Operations Review criteria – Milliman On-site vs Off-site review On-site vs Off-site review Reports Forms/Letters Delegated/Non-delegated notifications
8. QuestionsQ
11

Introductions: Permedion-HMSIntroductions: Permedion HMS Dennis Gramlich, Vice President, Permedion
Kevin Lee, Regional Vice President
David Sand MD, Chief Medical Officer
Joseph Steeger MD PhD, Medical Director
Patricia Ratwani RN, Clinical ReviewPatricia Ratwani RN, Clinical Review
Linda Freites RN, Project Manager
22
Introductions: MFD/DMAHSIntroductions: MFD/DMAHS Karen Chester RN, Regional Staff Nurse, Office of Reimbursement,
DMAHSDMAHS
Richard Hurd, Acting Chief of Staff, DMAHS
Mark Moskovitz, Deputy Director, Office of Comptroller, Medicaid
Fraud Division (MFD)
Pamela Orton RN, Healthcare Administrator, DMAHS
Jennifer Petrino, Administrator, Contract Compliance, DMAHS
33

Overview of HMSOverview of HMS Cost containment services for 37 state Medicaid agencies, CHIP,
Child Support, Pharmacy Assistance, CMS Coordination of benefits, program integrity, and other recovery and
cost savings projectscost savings projects 1,100 employees in 26 offices Multiple contracts with NJ since 1986
Oth NJ j t Other NJ projects:• Third Party Liability 1986 – Present; $1.4B Recovery • Cardiac Surgery 2009 – Present • Rx and DME Audit 2010 - Present
44
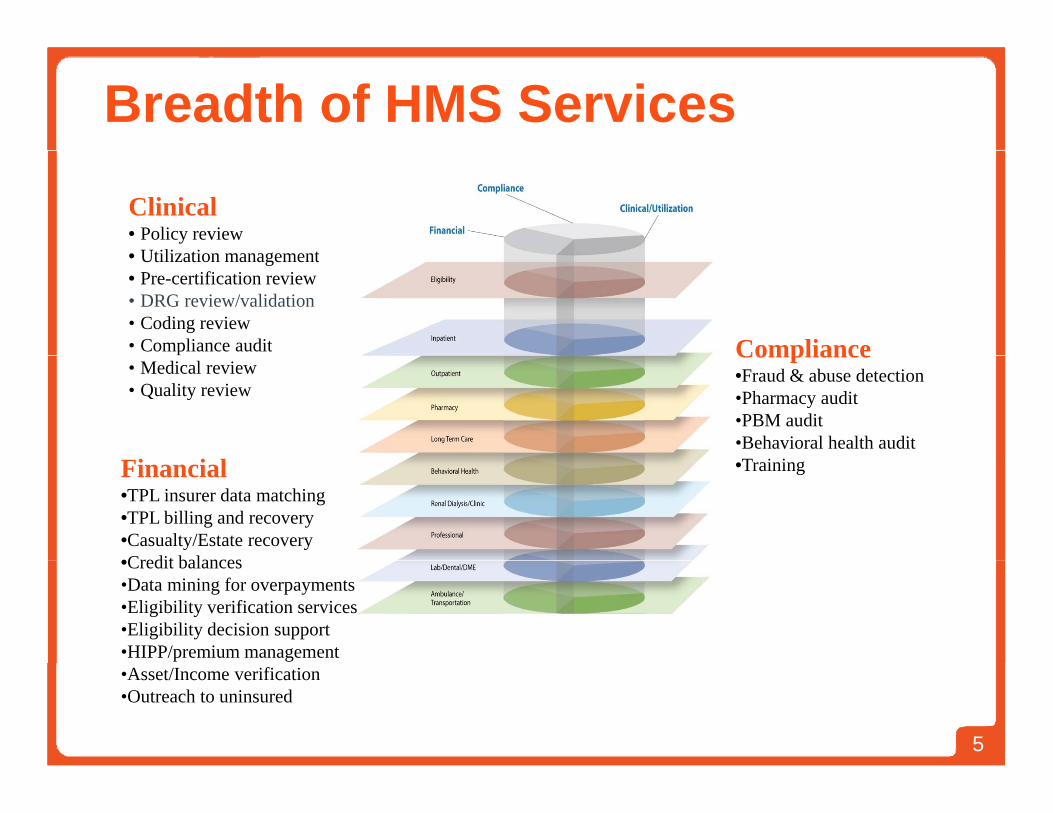
Breadth of HMS Services
Clinical• Policy review
Utili ti t• Utilization management• Pre-certification review• DRG review/validation• Coding review• Compliance audit Compliance• Medical review• Quality review
Compliance•Fraud & abuse detection•Pharmacy audit•PBM audit•Behavioral health audit
Financial•TPL insurer data matching•TPL billing and recovery•Casualty/Estate recovery•Credit balances
•Training
•Credit balances•Data mining for overpayments•Eligibility verification services•Eligibility decision support•HIPP/premium management
55
•Asset/Income verification•Outreach to uninsured

About Permedion
Wholly owned subsidiary of HMS since October 2007
Designated as a QIO-like entity by CMS
Accredited by URAC for both Utilization Management and y g
Independent Review
IRO for 12 States – Commercial Insurance Appealspp
110 Employees
600 Board Certified & Licensed Physicians600 Board Certified & Licensed Physicians
66

Utilization Review ServicesExperience and Approach
7

Utilization Review Experience
Colorado South Carolina
Illinois
South Carolina
Virginia
Kentucky North Carolina
New Jersey Massachusetts
Ohio
8
Approachpp1. Review of Billing and Reimbursement Policies
• Clinical Guidelines• Audit Regulations• Data Mining Process Updated to Reflect Parameters
2 Case Selection2. Case Selection• Random Sample for Utilization Review• Random Sample for DRG Validation
3. Provider Medical Record Request• All Letters Sent to Specific Individual• Attempt to Accommodate Provider Workload Issues• Courtesy Call• On Site Reviews Scheduled for Selected Facilities• Electronic Record Intake Option
All L tt G t d/T k d i S t
9
• All Letters Generated/Tracked in System
Approach (continued)4. Clinical/Coding Review
• Medical Record Abstraction by RN• RN and Certified Coders• RN and Certified Coders• System Ensures Accurate Abstraction• Quality Review for all Cases
5 Ph i i R i5. Physician Review• Required for medical necessity or DRG change• NJ physician panel
6. Notification Letter • Clinical summary and detailed rationale• Educational guidance as appropriate
7. Reconsideration & Appeal• Reconsideration to Permedion• Clinical issues referred to 2nd specialty-matched physician
10
Clinical issues referred to 2 , specialty matched physician• Fair Hearings to State

Approach (continued)Approach (continued)8. Collection & Recoupment
• Claim payment recouped• Provider to re-bill correctly with correct coding and/or for
appropriate setting
9. Identification of Trends• Based on errors, review• Data mining to confirm trend metrics• Data mining to confirm trend, metrics
10. Provider Education• Specific education through notification letter• Specific education through notification letter• Error trend education through provider bulletins• One-on-one interaction
11
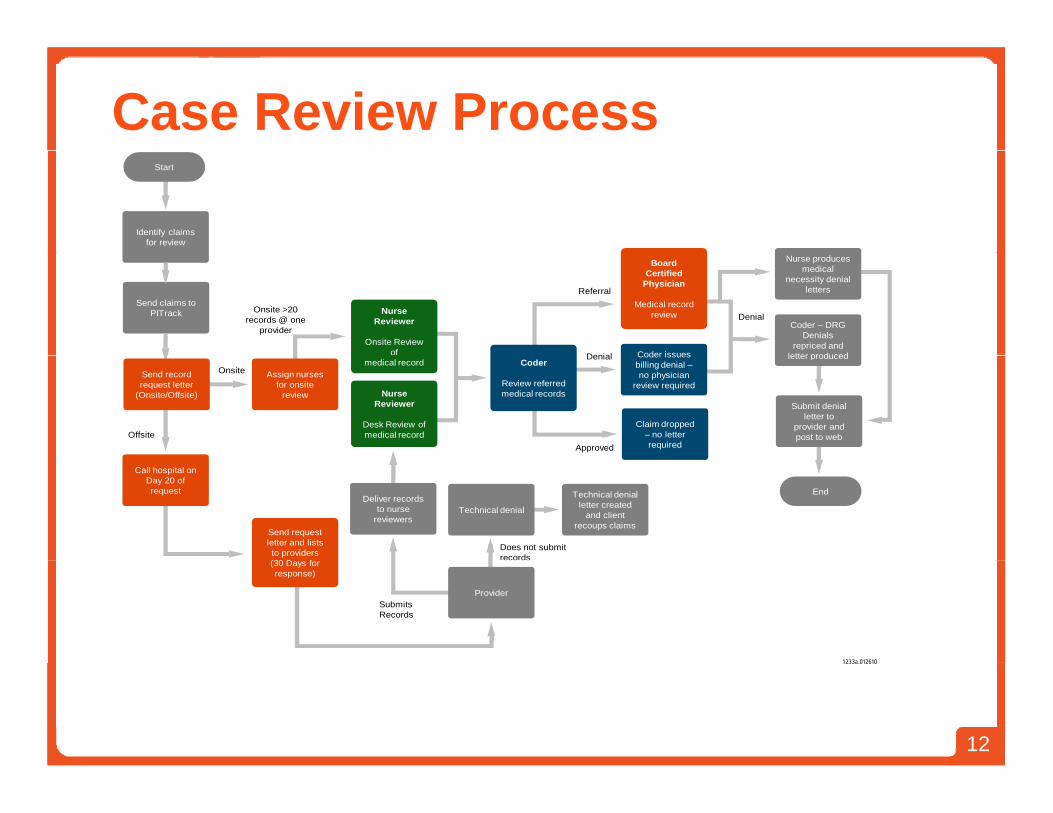
Case Review ProcessStart
Identify claims for review
Onsite >20 records @ one
provider
Send claims toPITrack Nurse
Reviewer
Onsite Review of Coder issues
Board Certified
Physician
Medical record review
Coder – DRGDenials
repriced and letter produced
Nurse produces medical
necessity denial letters
Denial
Referral
Denial
Offsite
Send record request letter
(Onsite/Offsite)
Assign nurses for onsite
review
medical record
Nurse Reviewer
Desk Review ofmedical record
Coder
Review referredmedical records
Claim dropped – no letter required
Coder issues billing denial –no physician
review required
letter produced
Submit denial letter to
provider and post to web
OnsiteDenial
Approved
End
Call hospital on Day 20 of request
Send request letter and lists to providers(30 D f
Deliver records to nurse
reviewersTechnical denial
Technical denial letter created
and client recoups claims
Does not submit records
1233a 012610
(30 Days for response)
ProviderSubmitsRecords
1233a.012610
12

Reconsideration Process
Receive appeals within 45 days of
determination letter
Board CertifiedPhysician
Medical Record Review
Start Coder/Nurse
Review chart and make determination
within 30 days of receipt of appeal
letter and additional information
Referral
Document and/orcalculate results
Written rationale documented on appeals letter
Uphold Results
OverturnResults
Appeal
Provider initiatesappeal
Send appeal results letter to Provider and
post Client letters to web
End
1232a.012610
13

ImplementationImplementationPlanPlan
1414
Implementation Plan
Approach Approach• Project Management
• Gantt Charts
• Frequent, effective communicationseque , e ec e co u ca o s
• Team approach
1515
16
17

18
Implementation PlanImplementation Plan PhasesPhases
• Transition• Facilities• Technology• Staffing• Quality Assurance• Quality Assurance• Contract Management• Training• Utilization Management Program
1919

Implementation PlanImplementation Plan
Staffing Plan: Milestones Staffing Plan: Milestones• Recruit/hire key personnel• Hire operational staffHire operational staff• Complete staff training
Training for initial hires completed by October 30, 2010
2020

2121
Implementation PlanImplementation Plan
Training Plan: Milestones Training Plan: Milestones • Revise corporate orientation programs
• Develop contract orientation program Including orientation to DMAHS Customer service trainingCustomer service training
• Develop review activity training program in
Scompliance with DMAHS regulations
• Develop position-specific training program
2222

Implementation PlanImplementation Plan
Office Space and Facilities Plan MilestonesOffice Space and Facilities Plan Milestones• Assessed Trenton, NJ office
Utilization of excess capacity
• Acquire additional space
60 – 90 days
• Complete equipment acquisitionp q p q
• Complete facilities set-up
2323
Technology Plan HMS has in-place technology and infrastructure to receive project
related data files
Technology Plan
related data files• Existing Extranet Business Partner Agreement with DHS• Existing Firewall hardware installed at DHSS• Existing high speed data lines to DHS, and to the Medicaid Fiscal g g
Intermediary, both Mercerville, NJ and Salt Lake City, Utah Data-centers
HMS receives • Paid Claim Files weekly• Paid Claim Files weekly• Provider File Quarterly
HMS has an existing Disaster Recovery Plan HMS is familiar with FD 999 Claims Adjustment Form HMS is familiar with FD-999 Claims Adjustment Form HMS is capable to implement electronic adjustments conforming to
DMAHS requirements and Fiscal Agent specifications
2424
Meeting with Current Contractor(s)g ( )
Turnover PlanTurnover Plan
Transfer Date
Clean Transfer vs. Overlap
Identify Other Action Items
2525

Provider RelationsProvider RelationsOrientation to Permedion-HMS and the
Review Program• Medical Review Process• Physician Panel• Physician Panel• Key Contacts (Project Manager, Quality
Management Supervisor)
Ongoing• Newsletter• Website• Feedback• Events• Events• One-on-one
2626
New Jersey Hospital Associationy p
Identify contactsEstablish working relationshipg pAssist with provider orientationQuarterly conferenceQuarterly conferenceWork collaboratively on provider issues
d d tiand education
2727

OperationsOperations
2828
Operations – Review CriteriaOperations Review Criteria
Milliman Care GuidelinesMilliman Care Guidelines• Evidence-based
• Used in most Permedion UR contracts
• Better fit with Medicaid population for inpatient vs
outpatient services
• Easier to use for retrospective review• Easier to use for retrospective review
29
Operations – Retrospective ReviewOperations – Retrospective Review
Sample of reviews based on number ofSample of reviews based on number of dischargesF f i b d b fFrequency of review based on number of discharges.Review of days to determine appropriate
statusQuality review
30

Operations – On-site vs. Off-siteOperations On site vs. Off site
State to determineOff-site:
• Ability to send records electronicallyy y• Less intrusion on provider operations
On-site:• Flexible in scheduling• May be intermittent
31
Operations – Forms/LettersOperations Forms/Letters
All forms and letters going to providers g g pwill:
• Be provided to DMAHS for review/approval• Contain appropriate references• Be posted to secure web page for DMAHS
accessaccess
32

MARKMARK MOSKOVITZMOSKOVITZMARK MARK MOSKOVITZMOSKOVITZ
DEPUTY DIRECTOR DEPUTY DIRECTOR MEDICAID FRAUD DIVISIONMEDICAID FRAUD DIVISIONMEDICAID FRAUD DIVISION MEDICAID FRAUD DIVISION
OFFICE OF THE STATE OFFICE OF THE STATE COMPTROLLERCOMPTROLLERCOMPTROLLERCOMPTROLLER
33

MEDICAID PROGRAMMEDICAID PROGRAMINTEGRITY AND PROTECTIONINTEGRITY AND PROTECTIONINTEGRITY AND PROTECTION INTEGRITY AND PROTECTION
ACTACT [C.30:4D[C.30:4D--53 et 53 et seqseq]]
Act that established the Office of Act that established the Office of Medicaid Inspector General in NewMedicaid Inspector General in NewMedicaid Inspector General in New Medicaid Inspector General in New JerseyJersey
Signed into law on March 16Signed into law on March 16 20072007 Signed into law on March 16, Signed into law on March 16, 20072007 OMIG consolidated into the Medicaid OMIG consolidated into the Medicaid
Fraud Division of the Comptroller’sFraud Division of the Comptroller’sFraud Division of the Comptroller s Fraud Division of the Comptroller s Office on June 30, 2010, with all the Office on June 30, 2010, with all the powers of the OMIG.powers of the OMIG.powers of the OMIG.powers of the OMIG.
34

MFDMFD RESPONSIBILITIESRESPONSIBILITIESMFD MFD RESPONSIBILITIESRESPONSIBILITIES
Detect prevent and investigate fraud andDetect prevent and investigate fraud and Detect, prevent, and investigate fraud and Detect, prevent, and investigate fraud and abuseabuseRecover improperly expended MedicaidRecover improperly expended Medicaid Recover improperly expended Medicaid Recover improperly expended Medicaid fundsfundsE f M di id R l d R l tiE f M di id R l d R l ti Enforce Medicaid Rules and RegulationsEnforce Medicaid Rules and Regulations
Audit cost reports and claimsAudit cost reports and claims Review quality of care given to Review quality of care given to
beneficiaries beneficiaries
35
MFDMFD RESPONSIBILITIESRESPONSIBILITIESMFD MFD RESPONSIBILITIESRESPONSIBILITIES
Refer criminal prosecutions to theRefer criminal prosecutions to the Refer criminal prosecutions to the Refer criminal prosecutions to the Attorney General’s officeAttorney General’s office
Oversee edits to the New Jersey Medicaid Oversee edits to the New Jersey Medicaid Management Information System Management Information System (NJMMIS)(NJMMIS)
36
WU3
Slide 37
WU3 text here is too small. should break it up into two slidesWindows User, 01/31/2010

MFDMFD RESPONSIBILITIESRESPONSIBILITIESMFD MFD RESPONSIBILITIESRESPONSIBILITIES
Conduct educational programs forConduct educational programs for Conduct educational programs for Conduct educational programs for Medicaid providers, vendors, contractors, Medicaid providers, vendors, contractors, and recipientsand recipientsand recipientsand recipients
Issue a report on the MFD’s activities, as a Issue a report on the MFD’s activities, as a part of the Comptroller’s annual report topart of the Comptroller’s annual report topart of the Comptroller s annual report to part of the Comptroller s annual report to Governor and the Legislature. Governor and the Legislature. R f i f ti d id tR f i f ti d id t Refer information and evidence to Refer information and evidence to regulatory agencies and professional and regulatory agencies and professional and
ti l li i b dti l li i b doccupational licensing boards occupational licensing boards 37

KEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONS
Statute defines fraud as:Statute defines fraud as: Statute defines fraud as:Statute defines fraud as: “an intentional deception or “an intentional deception or
misrepresentation made by any personmade by any personmisrepresentation made by any personmade by any person with the knowledge that the deception with the knowledge that the deception
ldld lt ilt i th i d b fitth i d b fitcouldcould result in result in somesome unauthorized benefit unauthorized benefit to that person or another person, to that person or another person, i l di t th t tit t f di l di t th t tit t f dincluding any act that constitutes fraud including any act that constitutes fraud under applicable federal or State law.”under applicable federal or State law.”
38

KEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONS
Definition of abuse:Definition of abuse: Definition of abuse:Definition of abuse:1.1. Provider Provider practices that are practices that are inconsistentinconsistent with with
sound fiscal, business, or medical practicessound fiscal, business, or medical practicessound fiscal, business, or medical practices sound fiscal, business, or medical practices and;and;
2.2. Result Result in in unnecessary costsunnecessary costs to Medicaid to Medicaid or; or; yy ;;3.3. In In reimbursement for services that are not reimbursement for services that are not
medically necessary medically necessary oror4.4. Fail Fail to meet professionally recognized to meet professionally recognized
standards for health care. standards for health care. 5.5. The The term also includes recipient practices that term also includes recipient practices that
result in unnecessary costs to Medicaid.” result in unnecessary costs to Medicaid.” 39

KEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONSKEY DEFINITIONS
The statute defines Medicaid to includeThe statute defines Medicaid to include The statute defines Medicaid to include The statute defines Medicaid to include both the Medicaid program and the N.J. both the Medicaid program and the N.J. FamilyCare ProgramFamilyCare ProgramFamilyCare ProgramFamilyCare Program
Ch it C i l d d f t t tCh it C i l d d f t t t Charity Care is excluded from statuteCharity Care is excluded from statute
However, a separate statute, passed in However, a separate statute, passed in December 2007, gives our office power to December 2007, gives our office power to , g p, g pinvestigate charity care fraudinvestigate charity care fraud
40
ORGANIZATION OF THE MFDORGANIZATION OF THE MFDORGANIZATION OF THE MFDORGANIZATION OF THE MFD
REGULATORYREGULATORY REGULATORY REGULATORY INVESTIGATIONS INVESTIGATIONS
FISCAL INTEGRITYFISCAL INTEGRITY FISCAL INTEGRITY FISCAL INTEGRITY Audit UnitAudit Unit Third Party Liability UnitThird Party Liability Unit Data Mining UnitData Mining Unit Recovery UnitRecovery Unit
41

GOALSGOALSGOALSGOALS
Ferret out the fraud and abuse in the system, and there’s Ferret out the fraud and abuse in the system, and there’s ten billion dollars in the system. Last year, Medicaid ten billion dollars in the system. Last year, Medicaid recoveries and cost savings topped 270 million in Newrecoveries and cost savings topped 270 million in Newrecoveries and cost savings topped 270 million in New recoveries and cost savings topped 270 million in New Jersey. Jersey.
H b t dit d i h d lH b t dit d i h d l Have a robust audit program and review scheduleHave a robust audit program and review schedule--provides a deterrent effect (can’t just pay and chase).provides a deterrent effect (can’t just pay and chase).
Review provider areas that have not been reviewed in Review provider areas that have not been reviewed in quite awhile.quite awhile.
42

MFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVES
UTILIZATION AND DRG AUDITSUTILIZATION AND DRG AUDITS UTILIZATION AND DRG AUDITSUTILIZATION AND DRG AUDITS DMAHS has contracted with Permedion to DMAHS has contracted with Permedion to
conduct these auditsconduct these auditsconduct these audits.conduct these audits. Audits will begin in November.Audits will begin in November. UR Audits will include units that had beenUR Audits will include units that had been UR Audits will include units that had been UR Audits will include units that had been
omitted before, i.e. psychiatric & omitted before, i.e. psychiatric & rehabilitation.rehabilitation.
43

MFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVES
Monthly meetings with Permedion, DMAHS,Monthly meetings with Permedion, DMAHS, Monthly meetings with Permedion, DMAHS, Monthly meetings with Permedion, DMAHS, and the MFD to review audit findings, and and the MFD to review audit findings, and where there is evidence of fraud, waste, or where there is evidence of fraud, waste, or abuse, to refer them to the MFD.abuse, to refer them to the MFD.
May result in an expanded audit and/or May result in an expanded audit and/or investigation.investigation.
44

MFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVESMFD HOSPITAL INITIATIVES
COST REPORT AUDITS WILL FOCUS ON:COST REPORT AUDITS WILL FOCUS ON: COST REPORT AUDITS WILL FOCUS ON:COST REPORT AUDITS WILL FOCUS ON: Physician payments for direct patient carePhysician payments for direct patient care Administrative servicesAdministrative services Administrative services Administrative services Rental space for private officesRental space for private offices
Payments for undocumented or unnecessaryPayments for undocumented or unnecessary Payments for undocumented or unnecessary Payments for undocumented or unnecessary servicesservicesPhysician practice subsidiesPhysician practice subsidies Physician practice subsidiesPhysician practice subsidies
Physician contracts, including fair market Physician contracts, including fair market analysis of physician servicesanalysis of physician servicesanalysis of physician servicesanalysis of physician services
45

Any questions?Any questions?Any questions?Any questions?
Office location is:Office location is: P O Box 025 TrentonP O Box 025 Trenton Office location is: Office location is: P.O. Box 025, TrentonP.O. Box 025, Trenton, , N.J. N.J. 0862508625
Phone Number: (609) 826Phone Number: (609) 826--47004700 My Number: (609) 777My Number: (609) 777--41674167
Website: Website: www.nj.gov/comptroller/divisions/medicaid/index.htmlwww.nj.gov/comptroller/divisions/medicaid/index.htmlj g / p / / /j g / p / / /
46

Open Discussion and QuestionsOpe scuss o a d Quest o s
4747