new respiratory gating technique for whole heart cine imaging: integration of a navigator slice in...
TRANSCRIPT
Technical Note
New Respiratory Gating Technique for Whole HeartCine Imaging: Integration of a Navigator Slice inSteady State Free Precession Sequences
Sergio Uribe, PhD,1–3* Cristian Tejos, PhD,3,4 Reza Razavi, MD,1
and Tobias Schaeffter, PhD1
Purpose: To evaluate the performance of a slice navigatorsequence integrated into a b-SSFP sequence for obtainingreal time respiratory self-gated whole heart cine imaging.
Materials and Methods: In this work, we present a noveland robust approach for respiratory motion detection byintegrating a slice navigator sequence into a balancedsteady state free precession (b-SSFP) sequence, whilemaintaining the steady state. The slice navigatorsequence is integrated into consecutive repetition times(TRs) of a b-SSFP sequence to excite and read out a navi-gator slice. We performed several phantom experiments totest the performance of the slice navigator sequence.Additionally, the method was evaluated in five volunteersand compared with breathing signals obtained from con-ventional pencil beam navigator sequence. Finally, thenavigator slice was used to obtain whole heart MR cineimages.
Results: The breathing signals detected by the proposedmethod showed an excellent agreement with thoseobtained from pencil beam navigators. Moreover, the tech-nique was capable of removing respiratory motion arti-facts with minimal distortion of the steady state. Imagequality comparison showed a statistical significantimprovement from a quality score of 2.1 obtained by thenonrespiratory gated images, compared to a quality scoreof 3.4 obtained by the respiratory gated images.
Conclusion: This novel method represents a robustapproach to estimate breathing motion during SSFP
imaging. The technique was successfully applied to ac-quire whole heart artifact-free cine images.
Key Words: respiratory self-gating; whole heart imaging;k0 projectionsJ. Magn. Reson. Imaging 2011; 34:211–219.VC 2011 Wiley-Liss, Inc.
WHOLE HEART CINE imaging has become increas-ingly important as a way of simplifying cardiac MR(1,2). This approach avoids cumbersome planningduring scanning as the imaging volume can be refor-matted in any plane retrospectively. However, thesescans have long acquisition times and difficulties withrespiratory motion compensation, even when under-sampled reconstruction techniques are applied (3–7).Pencil beam navigators have been proposed to moni-tor breathing motion. In cine imaging those navigatorsare usually interleaved into steady state free preces-sion (SSFP) sequences (8), thus interrupting the ac-quisition (9). This disturbs the steady state resultingin image artifacts. Self-respiratory gating techniqueshave been proposed (10–13) to overcome this limita-tion. A common approach in those techniques is touse a respiratory navigation based on the acquisitionof k0 center points or k0 profiles (14). For this, thebreathing information is obtained from the intensitymodulation of k0 center points (11,12), or is detectedusing projections derived from the k0 profiles (10,15).However, both approaches could fail in large patients,where the signal of k0 or of k0 profiles is stronglyinfluenced by signals arising from static tissue. Thiseffect is more prominent if a phase array receive coilis used, with higher sensitivity in the region of thechest wall. In this case, the breathing signal derivedfrom k0 center points is made up of a high intensitystationary signal arising from static adipose tissuesand a small intensity modulation due to the signalarising from moving tissues (e.g., liver). Furthermore,it is difficult to define the same universal gating win-dow in different patients since the intensity of themodulation varies among patients. Additionally, thisapproach cannot provide information of the actualdisplacement in a physical magnitude (e.g., mm).
1King’s College London, Division of Imaging Sciences, BHF center,NIHR Biomedical Research Center at Guy’s and St Thomas’ NHSFoundation Trust, London, United Kingdom.2Pontificia Universidad Catolica de Chile, Radiology Department,Santiago, Chile.3Pontificia Universidad Catolica de Chile, Biomedical Imaging Center,Santiago, Chile.4Pontificia Universidad Catolica de Chile, Department of ElectricalEngineering, Santiago, Chile.
Contract grant sponsors: BHF Center of Excellence; BRC center;VRAID-PUC.
*Address reprint requests to: S.U., Pontificia Universidad Catolica deChile, Radiology Department, Santiago, Chile. E-mail: [email protected]
Received September 2, 2010; Accepted March 28, 2011.
DOI 10.1002/jmri.22625View this article online at wileyonlinelibrary.com.
JOURNAL OF MAGNETIC RESONANCE IMAGING 34:211–219 (2011)
CME
VC 2011 Wiley-Liss, Inc. 211
Similarly, projections calculated from k0 profiles areless sensitive to motion in the presence of high inten-sity signals coming from adipose background. Thus,the edges in the projection arising from moving tissueare more difficult to detect in the presence of a strongbackground. Consequently, using k0 center points, ork0 profiles, can result in inconsistent respiratory sig-nals for some patients.
In this study, we present a novel and robust tech-nique for respiratory motion detection that has beenimplemented on a clinical scanner. In this approach,the excitation of an additional slice and the readout ofits projection are integrated into a balanced steadystate free precession (b-SSFP) imaging sequence withminimal interference of the steady state. In the follow-ing, this additional slice used for motion detection isrefereed as ‘‘navigator slice.’’ The influence of high in-tensity signals arising from static tissues closed to re-ceiver coil elements is avoided by using a dedicated ori-entation of the navigator slice and using only one ofthe elements of an array coil. This approach allows theselection of a small region inside the body and there-fore the final signal incorporates moving tissues whileavoiding contamination from high intensity signal fromadipose tissue. The technique was tested in phantomexperiments and compared with information obtainedfrom a pencil beam navigator echo sequence in fivehealthy volunteers. It was then used in the same vol-unteers to obtain a self-respiratory gated whole heartcine acquisition (15) under free breathing.
MATERIALS AND METHODS
MR Acquisition
Scanning was performed on a Philips Achieva 1.5Tesla (T) clinical scanner (Philips Medical Systems,
Best, The Netherlands) using a 32-element cardiacarray coil (two 16 array coils elements composed offour rows and four columns). A retrospectively gated,b-SSFP k-space segmented sequence was used toobtain three-dimensional (3D) cine data of the wholeheart. The 3D imaging volume was measured in sagit-tal orientation considering the read-out along the foot-head direction, the first phase encoding along anterior–posterior and the second phase encoding along theslice selection in left–right direction. To obtain the re-spiratory motion, the excitation and acquisition of thenavigator slice was integrated into the 3D cine acquisi-tion of the imaging volume. This interleaved sequenceallowed frequent measurements of the diaphragmdisplacement (i.e., every 240 ms) while maintainingthe steady state of the magnetization within the imag-ing volume. This approach was achieved by modifyinga b-SSFP sequence (Fig. 1) in the following way:
i) The excitation of an additional slice and the readout of its magnetization was integrated into twoconsecutive repetition times (TR) of a balancedSSFP imaging sequence. In particular, a shortSinc-Gaussian radio frequency (RF) -pulse wasused during the center of first TR to excite theadditional slice, whereas its projection was readout during the second TR. All additional gra-dients were balanced during each TR to maintainthe steady state of imaging volume obtained bythe SSFP sequence. The use of two consecutiveTRs for the slice navigator sequence avoids pro-longation of the original TR, which should be asshort as possible in b-SSFP sequences so that tolimit off-resonance effects. The proposedsequence allows the measurement of an addi-tional slice with arbitrary orientation while main-taining the steady state of the imaging volume.
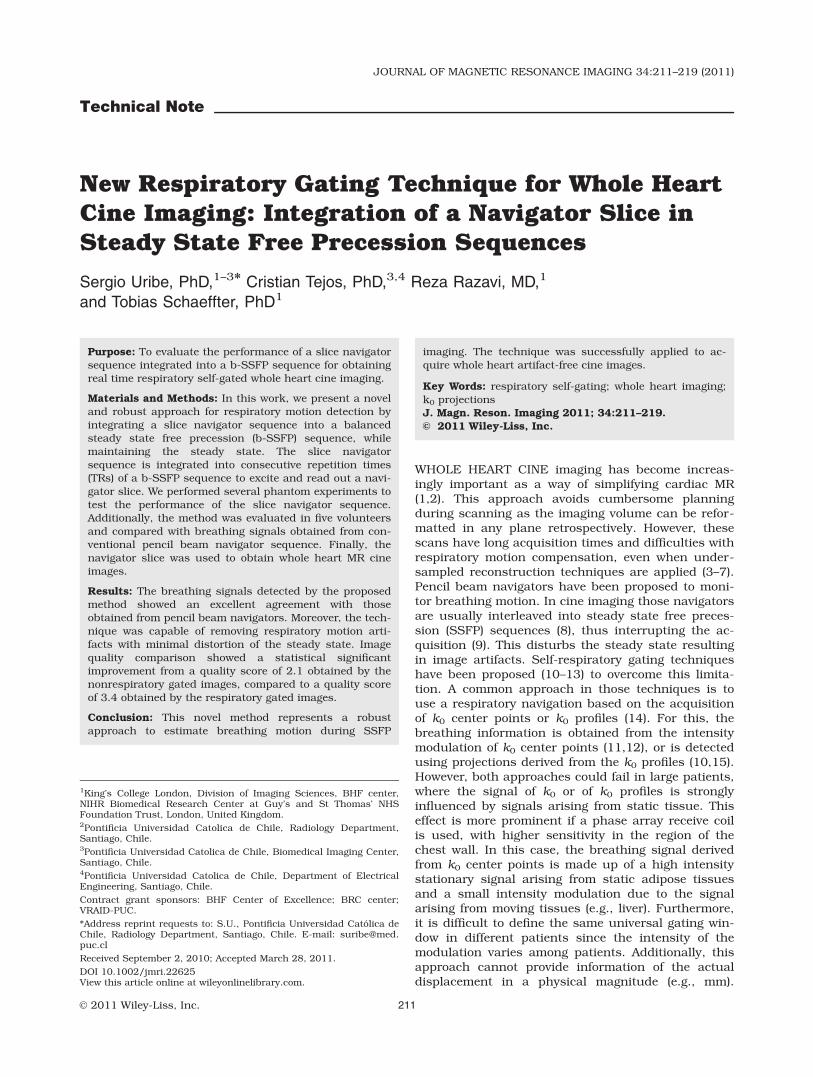
Figure 1. Integration of an additional slice navigator sequence into a b-SSFP imaging sequence. The excitation and read outof the navigator slice was performed in two subsequent TR of the imaging sequence without increasing the original TR andmaintaining the steady state of the spins in the imaging volume (Ima Vol). A dedicated coil element with a specific coil sensi-tivity (CS) and an angulated slice along the Feet Head direction allowed the restriction of the signal to a specific region, i.e.,static and fat contamination in the navigator slice projection can be avoided. The amplitude of the dephasing gradients werechosen in a way to reduce the signal of the imaging volume while having only a small effect on the navigator slice signal.
212 Uribe et al.

ii) The sensitivity of one receive coil element was usedto select a small fraction of the additional slice over-lying the diaphragm (Fig. 1). We used a single coilelement of the 32-channel coil to receive the respi-ratory motion signal. Since the diameter of each coilelement was approximately 10 cm, it only receivessignal from a limited volume given by its sensitivityprofile. Additionally, the slice navigator was posi-tioned and oriented to intersect with this sensitivityprofile to select a ‘‘beam-shaped’’ like volume. Thisapproach reduces signal contribution from staticchest tissue.
iii) Additional dephasing gradients (16) were usedbefore and after the readout of the navigatorslice to reduce the signal contribution from theimaging volume (Fig. 1). The gradient after theread out was applied to balance the area of thegradient applied before the read out. The ampli-tude of the dephasing gradients was set to pro-duce a linear phase of 360� over the imagingvolume along the slice selection direction (right–left), resulting in a strong reduction of the imag-ing volume signal. This was achieved by settingthe area of the dephasing gradients Ag as:
u ¼ gAgDZImaVol ¼ 2p ! Ag ¼ 2p
g � DZImaVol; ½1�
where DZIma Vol is the dimension of the imagingvolume in the slice direction and g is the gyro-magnetic ratio. The thickness of the navigatorslice is usually small in comparison to the imag-ing volume DZIma Vol dimension. This will resultin a small linear phase over the navigator sliceand thus, small reduction of the projectionsignal.
iv) Finally, a gradient pairing strategy (17) of theadditional slice-navigator sequence was per-formed to reduce any eddy current effect on thesteady state of SSFP sequence. For this, theslice-navigator sequence was performed twice in4 consecutive TRs, i.e., performing two consecu-tives excitations (2 TRs) followed by two readouts (2 TRs) of the navigator slice.
Motion Measurement and Gating Strategy
The breathing motion was determined in real time byapplying a cross-correlation function (14) between anavigator slice ‘‘kernel’’ and the actual navigator sliceprojection. The ‘‘kernel’’ corresponded to a 25-voxelportion of the projection signal of the navigator slice.The size of the kernel was chosen so that it coveredareas of diaphragm and lung. The kernel wasacquired at the beginning of the scan, during a train-ing stage that lasted for about 12 s to determine theexpiratory position. The breathing motion wasobtained by determining the position (in mm) of themaximum correlation when shifting the navigatorslice kernel over 30 pixels of the navigator slice pro-jections (18). This number was selected to detect dis-placements in the range of approximately 637.5 mm.
An acceptance gating window (e.g. 6 mm) was usedfor real-time respiratory gating (19), i.e., to accept orreject k-space data during scanning. The same k-space segment was acquired several times over the R-R interval (i.e., at different cardiac phases). All thesek-space segments were accepted if all breathing sam-ples obtained from corresponding navigator slice pro-jections were within the acceptance window. In thosecases where a respiratory sample was rejected, datafrom the complete cardiac cycle were re-acquired untilall breathing signals were within the acceptancewindow.
Implementation
The slice navigator sequence and the respiratory gat-ing strategies were fully integrated into the scannersoftware. The existing real-time gating functionality ofpencil-beam navigator signals and the drift correctionalgorithms were modified for respiratory gating usingthe navigator slice signal. This allowed real-time cal-culation of the actual displacement from the projec-tion of the navigator slice, which was sent togetherwith the position of the gating window to a navigatordisplay for real-time visualization of the respiratorygating process.
Phantom Experiments
A series of tests were performed on a phantom to ana-lyze the effect of the different parts of the slice-naviga-tor sequence described above. In particular, we stud-ied the integration of the slice selective excitation andthe effect of the dephasing gradients on the quality ofthe projection signal obtained from the navigator slice.Additionally, we compared the distortion of the steadystate caused by the integration of a slice navigatorsequence with that caused by interleaving a pencilbeam navigator echo sequence. The phantom con-sisted of two bottles of doped water (see Fig. 2). Bottle1 was used as the target for the imaging volume,whereas bottle 2 was the target for the navigator slice.The bottles were set up in a way the feet-head (FH)projection of the bottle 1 (imaging volume) was differ-ent to the FH projection of the bottle 2 (navigatorslice). A 3D cine scan (TR/echo time [TR/TE] ¼ 3 ms/1.5 ms, 20 cardiac phases, flip angle 60�, resolutionof 2.5 mm3) with integration of a slice navigatorsequence every 240 ms (navigator slice flip angle 15�
and slice thickness 30 mm) was used to perform thefollowing experiments:
Improvements of the Signal Qualityin the Navigator Slice Projection
(a) To show that we can excite the navigator slice andthe imaging volume simultaneously, we performedone 3D scan in which the readout was changed alongthe slice selection direction, i.e., from foot–head (FH)to right–left (RL). This was done to obtain FH projec-tions of both bottles (see Fig. 2), i.e., to obtain thequality of slice selection profile during SSFP imaging.
Respiratory Navigation Using a Navigator Slice 213
(b) To demonstrate that the dephasing gradientscan effectively reduce the projection signal of theimaging volume while maintaining the projection sig-nal of the navigator slice, projections with the readoutalong the FH direction were obtained in 4 scans. Toevaluate the effects of the dephasing gradients on theimaging volume (see Fig. 2), bottle 2 was removedfrom the phantom for the first and second scans, andin the second scan the dephasing gradients wereswitched off. To study the effect of the dephasing gra-dients on the navigator slice projection, bottle 1 wasremoved for the third and fourth scans, and in thefourth scans the dephasing gradients were switchedoff.
Additionally, the influence of the coil sensitivity wastested in (a) and (b) by comparing projectionsobtained in two different coils. These coils werelocated next to each other, in the same row but in thetwo central columns of the anterior 4 by 4 phasearray coil (see Fig. 2).
Interference of the Steady State
The interference of the steady state was comparedbetween a slice navigator and a pencil beam navigatorsequence. Three 3D scans were performed with allphase encoding gradients switched off, so that projec-tions of the imaging volume along the FH direction
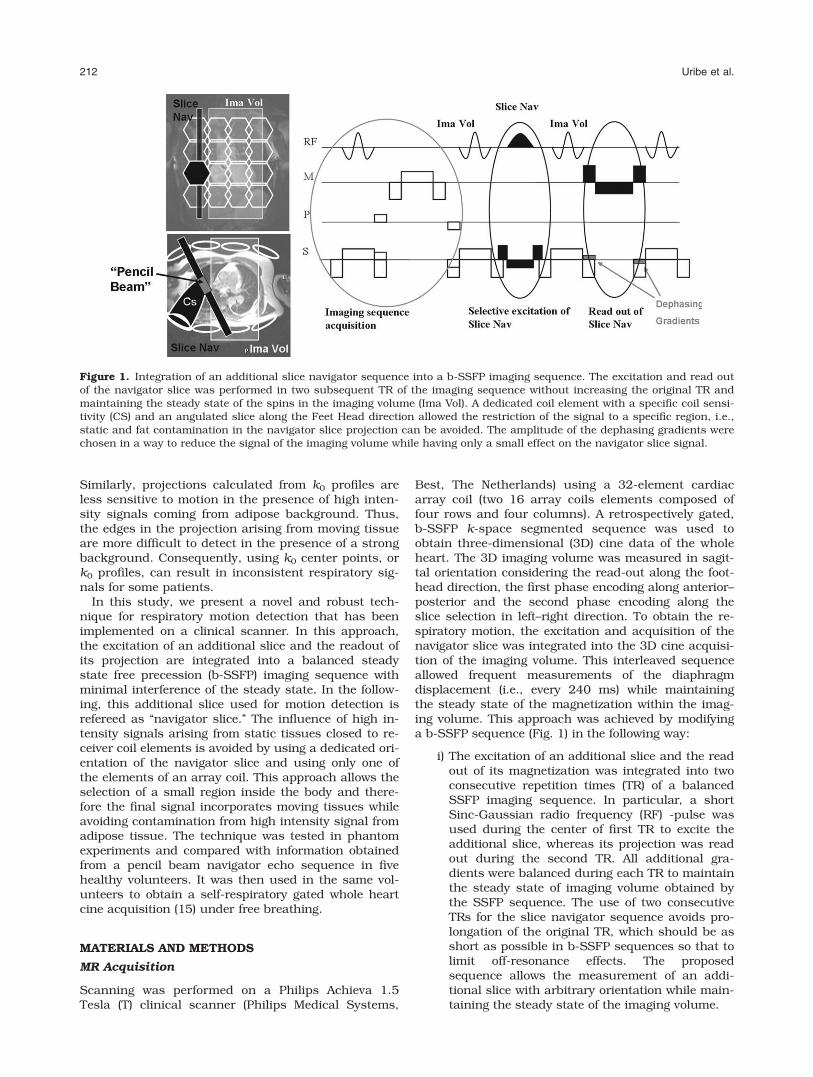
Figure 2. Phantom set up (a) and projections along the Right–Left direction for two different coils (b,c). The amplitude of theimaging volume projection varied depending on the different coil sensitivities, whereas the amplitude of the navigator sliceprojection was similar for both coils. From d to g projection along the Feet–Head direction are shown, with (dashed lines) andwithout the application of dephasing gradients (bold lines) using two different coils (coil 1, d,f; and coil 2, e,g). The dephasinggradients reduced the maximum amplitude of the imaging volume projection signal (d,e) at least three times for both coils,whereas, its effect on the navigator slice projection signal (f,g) was negligible.
214 Uribe et al.

were acquired continuously (i.e., in every TR). Thefirst scan was a standard 3D cine sequence acquiredfor reference. In the second scan the slice navigatorsequence was performed, with the slice navigatorbeing rotated 30� along the FH axis. The angulationwas chosen so that the slice navigator had a mini-mum overlap with the imaging slices inside the vol-ume of interest, while reducing signal contributionfrom static chest tissue.
Finally, in the third scan one navigator beamsequence was performed once in every cardiac cycle,immediately after the R-top detection. The flip anglein the pencil beam navigator and slice navigatorsequence was set to 30� and the diameter and thick-ness of both navigators were 20 mm.
In Vivo Experiments
Three experiments were done for evaluating differentaspects of our proposed navigator slice approach. Forthose experiments, MR-scanning was performed onfive healthy volunteers (three men and two women, 256 4 years, 70 6 20 kg, 1.70 6 0.1 m). Following asurvey scan, a SENSE reference scan was used toobtain the coil sensitivity maps of the 32-channelarray coil (7).
(A) Comparisons of the performance of the cross-correlation using navigator slice projections andk0 projections with a read-out along the FHdirection. For this, two scans (with the sameimaging parameters as those used for the 3Dwhole heart scan, vide infra section C) were per-formed to acquire navigator slice projectionsand k0 projections, respectively. The k0 projec-tions were acquired as indicated in (15). In bothscans, the same coil was used to process thenavigator slice projections and k0 projections(black coil in Fig. 1).
(B) Comparison of the breathing signals measuredby a conventional pencil beam and the slice nav-igator sequence. For this, a scan was performedthat simultaneously acquired projections from anavigator pencil beam and a navigator slice. Inparticular, for each cardiac cycle, one pencilbeam navigator was performed immediately af-ter the R-top of the ECG wave. This was followedby the acquisition of multiple projections of thenavigator slice every 240 ms. Since only onepencil beam navigator was acquired for everycardiac cycle, the respiratory signal from thesedata were interpolated at the time points whenthe navigator slice data were acquired. A com-parison of both respiratory signals was thenperformed by linear regression in the fivevolunteers.
(C) Evaluation of the impact of respiratory gatingusing the navigator slice for whole heart cineimaging. In this case, two 3D SSFP cine MRIscans of the whole heart were obtained usingthe proposed real-time respiratory gatingapproach. The first scan was carried out withoutrespiratory gating and the second scan with a
gating window of 6 mm (the data were acceptedin end-expiration). The parameters used in eachscan were field of view of 280 � 280 � 145 mm,isotropic resolution of 2.5 � 2.5 � 2.5 mm3,Sense factor of 2 in the anterior posterior direc-tion, 20 cardiac phases were acquired and retro-spectively reconstructed with a temporalresolution of 40–50 ms, TR/TE ¼ 3/1.5 and aflip angle of 60�. The navigator slice wasacquired approximately every 240 ms, angula-tion of the navigator slice was 30� along the FHdirection and flip angle and thickness of thenavigator slice were 30� and 15 mm, respec-tively. The coil selected for the acquisition of thenavigator slice was positioned on the anteriorpart of the 32-channel coil. The coil was chosenas the coil further away from the imaging vol-ume and located on top of the diaphragm (blackcoil in Fig. 1).
Data from the five volunteers obtained with andwithout respiratory gating were reformatted along dif-ferent views of the heart (4Ch, Long axis, Short axis,and axial view) at representative end-systolic andend-diastolic cardiac phases. In total 80 images wereobtained, subsequently they were randomly sortedand imaged scored by two experience independentobservers (S.U., 5 years of experience in Cardiac MR,and C.B., 2 years of experience of cardiac MR). Imagequality was graded on a 4-point scale based on thevisibility of the endocardial and epicardial border(modified from McConnell et al, 19): score (i) poor: en-docardial and epicardial border poorly visible or notvisible (nondiagnostic), (ii) moderate blurring of endo-cardial and epicardial border, (iii) good endocardialand epicardial border visibility, (iv) excellent imagequality.
This study was approved by the local ethic commit-tee and informed consent was obtained from allvolunteers.
RESULTS
Phantom Experiments
Improvements of the Signal Quality in theNavigator Slice Projection
(a) Results of the selective excitation pulse of the slicenavigator sequence are shown in Figure 2b,c. Projec-tions obtained along the slice selection direction (RL)for 2 different coils are depicted. In Figure 2b,c, it ispossible to distinguish two projections, one from theimaging volume and one from the navigator slice. Thisfigure also shows that these projections were differentdepending on the sensitivity of the receiver coil.Although the projection of the imaging volume wasdifferent for coil 1 and 2, it is noticeable that the am-plitude of the navigator slice projection was similarfor both coils.
(b) The effects of the application of the dephasinggradients on the imaging volume and on the navigatorslice are also shown in Figure 2d–g. Projection alongthe FH direction demonstrated that by applying
Respiratory Navigation Using a Navigator Slice 215
dephasing gradients (dashed line in Fig. 2d,e) themaximum amplitude of the imaging volume projectionwas reduced by a factor of 3.1 for coil 1 (Fig. 2d) anda factor of 3.3 for coil 2 (Fig. 2e). However, the effect
of those gradients over the navigator slice projectionwas negligible for both coils (Fig. 2f,g). Therefore, thecontrast between the imaging volume projections andnavigator slice projections was increased by a factorof at least 3.
Interference of Steady State
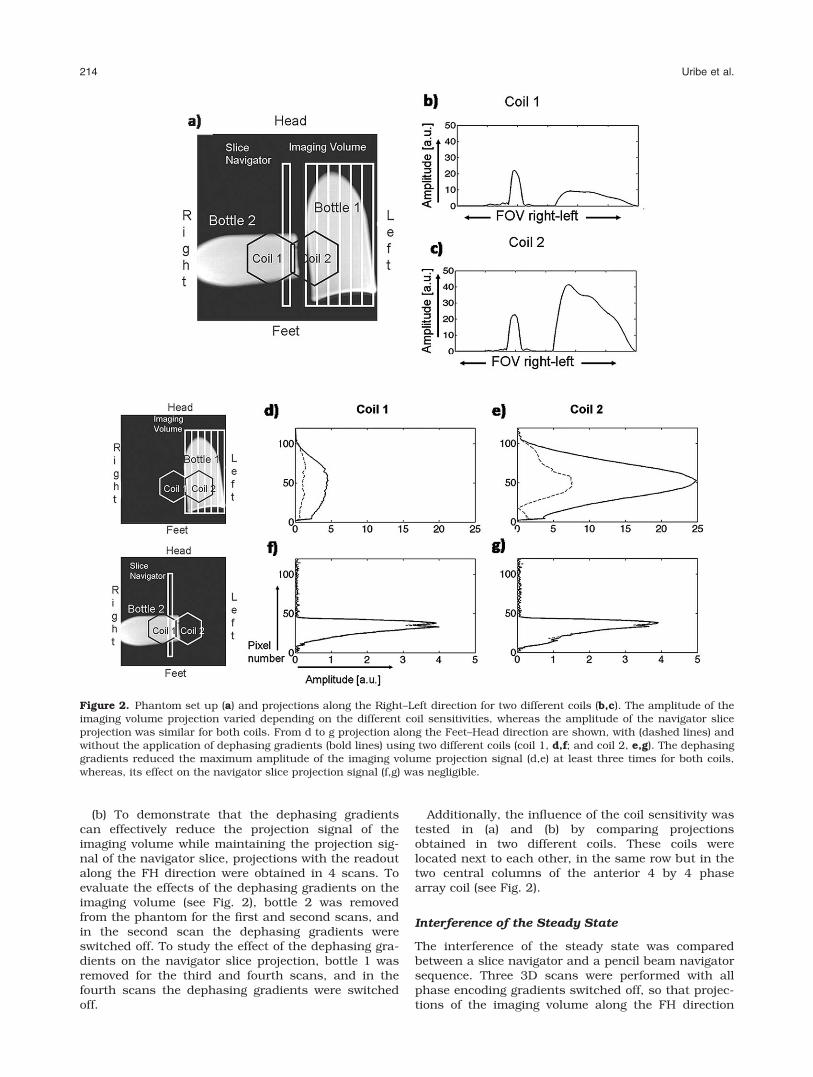
Figure 3 shows 150 k0 projections from the imagingvolume obtained immediately after the application of(a) a standard 3D SSFP scan without navigator (b) 3DSSFP scan with integration of the navigator slice and(c) 3D SSFP scan with interleaving a pencil beam navi-gator. Figure 3 also shows the amplitude of a singlepixel of the projection with time for the 3 cases (a, b,and c). It is noticeable that the distortion of the imag-ing volume projection was negligible when the extraselective excitation was applied. In contrast, the pencilbeam navigator produces a severe distortion on thesteady state. In particular, the variance of signal due tothe distortion from a pencil beam navigator was 82%higher compared to the normal scan, instead of the0.1% of increment produced by the navigator slice.
In Vivo Experiments
(a) Comparisons of the performance of the cross-cor-relation using navigator slice projections and k0
Figure 3. Left column: The 150 k0 projections from theimaging volume were continuously acquired after the appli-cation of a navigator method: (a) a standard 3D scan, (b) anavigator slice, and (c) a navigator beam. Right column: Sig-nal amplitude of a single pixel along the 150 projection sam-ples. Notice the distortion of the steady state introduced bythe application of a pencil beam navigator sequence, whereasonly minimal distortion was produced by using the slice-nav-igator sequence.
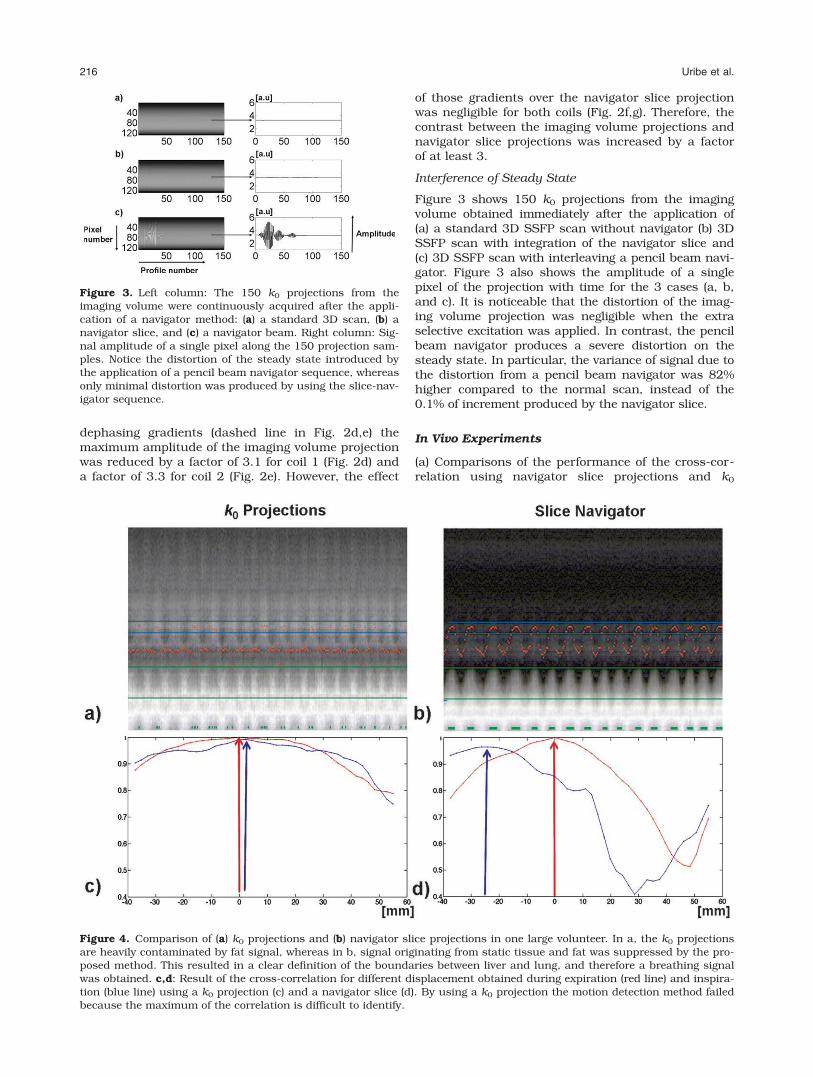
Figure 4. Comparison of (a) k0 projections and (b) navigator slice projections in one large volunteer. In a, the k0 projectionsare heavily contaminated by fat signal, whereas in b, signal originating from static tissue and fat was suppressed by the pro-posed method. This resulted in a clear definition of the boundaries between liver and lung, and therefore a breathing signalwas obtained. c,d: Result of the cross-correlation for different displacement obtained during expiration (red line) and inspira-tion (blue line) using a k0 projection (c) and a navigator slice (d). By using a k0 projection the motion detection method failedbecause the maximum of the correlation is difficult to identify.
216 Uribe et al.

projections with a read-out along the FH direction.Figure 4 shows the projections obtained with the k0
profiles (a) and the navigator slice (b) from one volun-teer (98 kg, 1.78 m). Projections from k0 profiles arecontaminated by high signal arising from static adi-pose tissue in the chest region. In contrast, the newslice navigator technique provided projections withbetter definition of edges at the border of the dia-phragm, resulting in a better detection of motion. Thecross-correlation function obtained for two respiratorymotion states (expiration and inspiration) are shownfor the data obtained by using k0-projections of theimaging volume (Fig. 4c) and using the navigator slice(Fig. 4d). The cross-correlation function of the naviga-tor slice data resulted in a narrow curve with adefined maximum at displacements 0 mm for expira-tion (red curve) and �24.2 mm for inspiration (bluecurve). However, the cross-correlation function deter-mined from k0-projections was broader with a numberof local maxima, which resulted in misleading dis-placements of 2.2 mm for inspiration (blue curve). Inparticular, the fact that side maxima have amplitudes
close to the global maximum could make the determi-nation of the displacement erroneous.
(b) Comparison of the breathing signals measuredby a conventional navigator beam and the navigatorslice. Figure 5 shows a comparison of the breathingsignal of two different volunteers obtained by a navi-gator beam and a navigator slice. Notice the goodagreement between both methods despite differentbreathing patterns. A linear regression analysis (Fig.5) showed high correlation values for all five volun-teers (see Table 1).
(c) Evaluation of the impact of respiratory gatingusing the navigator slice for whole heart cine imaging.A gating window of 6 mm resulted in a gating effi-ciency of approximately 40%. Figure 6 shows repre-sentative reformatted images of the cine acquisitionfrom one large volunteer, i.e., end-diastolic and end-systolic Short Axis (SA), four-chamber (4-CH), andaxial reformatted images. Notice the artifacts in thenongated scan, which were significantly reducedusing the proposed gating approach. In particular, therespiratory gated images provided the best visualiza-tion of the endocardial and epicardial borders with amean consensus score of 3.4, compared with thescore of 2.1 obtained by the nonrespiratory gatedimages. Additionally, the nonrespiratory gated imagesprovided 10 reformatted images with nondiagnosticvalue (at least one observer gave an score of 1),whereas all the images obtained using the slice navi-gator sequence had an score greater than 2. Further-more, a Mann-Whitney test showed the difference inimage quality to be significant P < 0.001.
Figure 5. Comparison of breathing signal obtained with the navigator beam and with the navigator slice in two representa-tive volunteers. Notice the good agreement between both techniques. Results of the linear regression between both methodsare shown in the right column.
Table 1
Linear Regression Parameters for the 5 Volunteers
Volunteer 1 2 3 4 5
Slope 1.00 0.95 0.95 1 0.92
Intercept �0.10 0.04 0.3 �0.17 0.22
Norm of the
residuals
10.159 6.45 9.99 13.48 12.99
Respiratory Navigation Using a Navigator Slice 217

DISCUSSION
We have proposed a novel and robust method to esti-mate breathing motion during b-SSFP scanning withminimal distortion of the steady state. This wasachieved by the integration of an extra navigator slicein four consecutive TRs of the b-SSFP imagingsequence. The use of a single coil element for signalreception in combination with an angulated sliceallowed selecting and positioning a beam-shaped nav-igator region. To determine the breathing motion, weused a cross-correlation measure rather than the cen-ter of mass or the correlation coefficient (10,15),allowing the determination of the diaphragm displace-ment in mm. Additional dephasing gradients wereshown to be efficient in reducing signal from theimaging volume, with minimal effect over the naviga-tor slice projection, making it more sensitive to motiondetection.
Phantom experiments showed the integration of theslice navigator in a b-SSFP sequence produces negligi-ble distortions on the steady state, which was muchless pronounced compared to the distortion caused byinterleaving pencil beam navigator sequences result-ing in the interruptions of the steady state. This isbecause the slice navigator was integrated into con-secutive TRs, i.e., RF pulses for the imaging volumewere continuously applied and therefore, the steadystate of the spin magnetization in the imaging volumewas maintained.
The methodology presented here addresses theproblem related to respiratory motion in 3D cinesequences. Respiratory motion was successfullydetermined in all volunteers with a high correlationwith the displacements obtained from pencil beamnavigator echoes.
One disadvantage of the technique is that, to reduceeddy currents four consecutive TRs (12 ms) were nec-essary to perform one slice navigator. Since the slicenavigator was applied every 240 ms, data acquisitionwas interrupted three or four times during the cardiac
cycle (depending on the heart rate). However, this onlycorresponds to 4.8% of the R-R interval for a heartrate of 60 bpm. Furthermore, because the applicationof the slice navigators was evenly distributed over thecardiac cycle, the effect on the temporal resolutionwas negligible.
This new idea of integrating additional RF and gra-dients pulses into the steady state could lead to sev-eral other applications. For instance, it can be used tomodify tissue contrast by applying prepulses into thesteady state. Recently, it has been shown how thisidea can be use for fat suppression (20). It could bealso applied for regional saturation or spin labeling incombination with SSFP sequences.
In conclusion, this novel method represents arobust approach to estimate breathing motion duringSSFP imaging. The technique has successfully beenapplied to acquire whole heart cine images during afree-breathing scan. Motion artifacts were significantlyreduced when using the technique.
REFERENCES
1. Sorensen TS, Korperich H, Greil GF, et al. Operator-independentisotropic three-dimensional magnetic resonance imaging for mor-phology in congenital heart disease: a validation study. Circula-tion 2004;110:163–169.
2. Razavi RS, Hill DL, Muthurangu V, et al. Three-dimensional mag-netic resonance imaging of congenital cardiac anomalies. CardiolYoung 2003;13:461–465.
3. Griswold MA, Jakob PM, Heidemann RM, et al. Generalized auto-calibrating partially parallel acquisitions (GRAPPA). Magn ResonMed 2002;47:1202–1210.
4. Kozerke S, Tsao J, Razavi R, Boesiger P. Accelerating cardiac cine3D imaging using k-t BLAST. Magn Reson Med 2004;52:19–26.
5. Muthurangu V, Noble N, Boubertakh R, et al. Single breath-hold3D cine imaging: a non-angulated isotropic acquisition usingSENSE on a 32 channel system. In: Proceedings of the 9th An-nual Scientific Session of SCMR, Miami, 2005. (abstract 183).
6. Noble N, Muthurangu V, Boubertakh R, et al. Automatic refor-matting of 32-channel non-angulated cardiac volumes. In: Pro-ceedings of the 14th Annual Meeting of ISMRM, Seattle, 2006.(abstract 791).
Figure 6. Representative end-diastolic and end-systolic frame of 3D reformatted data in short axis views (SA), four chamberviews (4-CH) and axial view. Notice the reduction of motion artifacts using the proposed respiratory gating approach (bottomrow) compare to the nonrespiratory gating scan (top row).
218 Uribe et al.

7. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sen-sitivity encoding for fast MRI. Magn ResonMed 1999;42:952–962.
8. Scheffler K, Lehnhardt S. Principles and applications of balancedSSFP techniques. Eur Radiol 2003;13:2409–2418.
9. Peters DC, Nezafat R, Eggers H, Stehning C, Manning WJ. 2Dfree-breathing dual navigator-gated cardiac function validatedagainst the 2D breath-hold acquisition. J Magn Reson Imaging2008;28:773–777.
10. Stehning C, Bornert P, Nehrke K, Eggers H, Stuber M. Free-breathing whole-heart coronary MRA with 3D radial SSFP andself-navigated image reconstruction. Magn Reson Med 2005;54:476–480.
11. Brau AC, Brittain JH. Generalized self-navigated motion detec-tion technique: preliminary investigation in abdominal imaging.Magn Reson Med 2006;55:263–270.
12. Curcic J, Buehrer M, Boesiger P, Koserke S. Prospective self-gat-ing for simultaneous compensation of cardiac and respiratorymotion. In: Proceedings of the 11th Annual SCMR Scientific Ses-sions, Los Angeles, 2008. (abstract 144).
13. Lai P, Larson AC, Park J, Carr JC, Li D. Respiratory self-gatedfour-dimensional coronary MR angiography: a feasibility study.Magn Reson Med 2008;59:1378–1385.
14. Ehman RL, Felmlee JP. Adaptive technique for high-definition MRimaging of moving structures. Radiology 1989;173:255–263.
15. Uribe S, Muthurangu V, Boubertakh R, et al. Whole-heart cineMRI using real-time respiratory self-gating. Magn Reson Med 2007;57:606–613.
16. Dixon WT, Du LN, Faul DD, Gado M, Rossnick S. Projectionangiograms of blood labeled by adiabatic fast passage. MagnReson Med 1986;3:454–462.
17. Bieri O, Markl M, Scheffler K. Analysis and compensation of eddycurrents in balanced SSFP. Magn Reson Med 2005;54:129–137.
18. Foo TK, King KF. A computationally efficient method for track-ing reference position displacements for motion compensationin magnetic resonance imaging. Magn Reson Med 1999;42:548–553.
19. McConnell MV, Khasgiwala VC, Savord BJ, et al. Comparisonof respiratory suppression methods and navigator locations forMR coronary angiography. AJR Am J Roentgenol 1997;168:1369–1375.
20. Uribe S, Razavi R, Schaeffter T. Integration of magnetizationpreparation sequences into SSFP sequences: a fat saturationexample. In: Proceedings of the 16th Annual Meeting of ISMRM,Toronto, 2008. (abstract 1042).
Respiratory Navigation Using a Navigator Slice 219