nhd focus on....pku
DESCRIPTION
NHD Supplement July 2016TRANSCRIPT
July 2016: Issue 116
PHENYLkETONURIA
NETWORK HEALTH DIGEST
PKU SUPPLEMENT
The Magazine for Dietitians, Nutritionists and Healthcare Professionals NHDmag.com
PKU through the life stages: from paediatric to adult obesity management
FOCUS on PKU

FOCUS ON PkU
Contents
In this issue, we spotlight Phenylketonuria (PKU), an inherited metabolic disease that causes disruption to the metabolism of the amino acid, phenylalanine (Phe). We have included articles that give a thorough overview of PKU, taking us through the life stages of this patient group. Like many chronic conditions, PKU is best managed by a multidisciplinary approach, with the dietitian taking a key role in advising the patient and their family about the essential diet required to manage the condition. Paula Hallam RD, Specialist Paediatric Dietitian in Metabolics at Great Ormond Street Hospital, gives us a fine overview of paediatric PKU management, while Heidi Chan, Practicing Adult IMD Dietitian at Guy’s and St Thomas’ Hospital, details the challenges and approaches to transitioning the young adult with an inherited metabolic disease. Louise Robertson and Sarah Howe, Specialist Dietitians in IMD at University Hospitals Birmingham NHS Foundation Trust, explore the incidence, causes and management of obesity in adults with PKU. Finally, we get a parent’s perspective from Louise Conlisk, who shares her experiences of PKU management for her young child Caitlin, through diet and Kuvan. A controversial approach to managing PKU, Kuvan is not routinely prescribed here in the UK or the Republic of Ireland; however, Louise and Caitlin have access to the medication whilst living in Australia. I talked to Louise at a PKUAI (PKU Association of Ireland) meeting earlier this year and she was keen to share Caitlin’s story with healthcare professionals and fellow parents, to shed some light on the real experience of living with PKU and using this medication. It’s a moving and informative read. Emma
FRom THe eDIToR
Welcome to our first NHD FOCUS on . . . supplement.
emma Coates - NHD editor
Advertising Richard Mair Tel 01342 824073
Phone 0845 450 2125 (local call rate) Fax 0844 774 7514
email [email protected]
www.NHDmag.com www.dieteticJOBS.co.uk
Address Suite 1 Freshfield Hall, The Square, Lewes Road, Forest Row,
East Sussex RH18 5ES
editor - Emma Coates RD
Publishing Director - Julieanne Murray
Publishing editor - Lisa Jackson
Publishing Assistant - Katie Dennis
Special Features - Ursula Arens
News - Dr Emma Derbyshire
Design - Heather Dewhurst
29 Transitioning young adults with an IMD Dealing with adolescent challenges
38 PKU: a parent’s perspective An overview of living with PKU and medical support
35 ObESITY IN ADULTS WITH PkU Maintaining a healthy PkU diet
22 PAEDIATRIC PkU Dietary management and monitoring
Louise Conlisk and her daughter Caitlin. Turn to page 38 for their story.
2 www.NHDmag.com July 2016 - Issue 116 - Supplement

Anamix Junior is the only powdered product for 1–10 year olds with PKU, MSUD, TYR, HCU, GA1, MMA/PA and IVA that contains all of the following: DHA Calcium & Vitamin D Fibre
Can be taken as: a spoonable paste or as a drink
Comes… in to promote an easier follow-on from Anamix Infant or Anamix First Spoon
and in in
in with
PKU, MSUD, TYR, HCU: 10gPE; MMA/PA, GA1: 5gPE; *IVA:
HELPING YOUR PATIENTS GET ON WITH LIFE
Something
new!

PAeDIATRIC
PKU is caused by a mutation in the gene for the enzyme phenylalanine hydroxylase (PAH). PAH is responsible for breaking down the essential amino acid phenylalanine, to tyrosine. A deficiency of PAH results in raised serum (and brain) phenylalanine levels and decreased tyrosine levels.
NeWBORN SCReeNINGIn the UK, a nationwide newborn screening programme for PKU began in 1969.2 Currently, every baby born in the UK is offered the screening test for PKU at approximately day five of life. This is commonly known as the ‘heel prick test’, which is a blood test performed by midwives. Prior to the ‘heel prick test’ there was a urine test or ‘nappy test’ that was carried out in certain areas of the UK. The screening test today also includes the following inherited meta-bolic conditions:
• Medium-chain-acyl-CoA dehydrogenase deficiency (MCADD)
• Glutaric aciduria type 1 (GA1)• Maple syrup urine disease
(MSUD)• Homocystinuria (HCU)• Isovaleric acidaemia (IVA)
As well as these disorders:• Cystic Fibrosis• Congenital hypothyroidism• Sickle cell disease
CLINICAL SeveRITIeSPKU exhibits a wide range of clinical severities, depending on the level of residual enzyme activity.1 In patients with PKU, the PAH enzyme is not functioning properly or is absent and, therefore, it cannot convert phenylalanine into tyrosine. This leads to a build-up of phenylalanine in the blood and brain, as well as a deficiency
FocUS oN PKU: PAeDIATRIc
Paula Hallam RDSpecialist Paediatric Dietitian, Metabolics, GOSH
Paula is a clinical Dietitian at Great ormond Street Hospital for children in the metabolic Team, working predominantly with children with PKU and their families. Previously, Paula held the position of Dietitian Advisor to the NSPKU for three years. She is also a Freelance Paediatric Dietitian and mum to two girls.
Phenylketonuria (PkU) is a genetically inherited condition of amino acid metabolism, with a prevalence of approximately one in 10,000 in the Uk.1 This means that each year 60-70 babies are born with PkU in the Uk.
For full article references please email info@ networkhealth group.co.uk
Figure 1: The PKU pathway
Source: University of Utah, Health Sciences, Learn Genetics: http://learn.genetics.utah.edu/content/disorders/singlegene/pku/
4 www.NHDmag.com July 2016 - Issue 116 - Supplement

of tyrosine. Tyrosine is normally used to make other proteins as well as the pigment melanin and the neurotransmitter dopamine. Dopamine has important functions in the brain and melanin is a brown pigment, which affects the colour of the skin, hair and eyes. This is why late-treated or untreated people with PKU have pale coloured hair and skin, as well as brain damage and severe behavioural problems.3
PKU is the most common inborn error of protein metabolism1 and is inherited as an autosomal recessive condition, which means that two copies of the mutated PAH gene is required to result in a child with PKU. The carrier rate for PKU in the UK is one in 50. For two people who are both carriers, there is a one in four chance for each pregnancy, of the baby having PKU and a two in four chance of the baby being a carrier. This is illustrated in the diagram below.
THe PKU DIeTPKU is treated with a diet that is very low in phenylalanine and must be initiated by 20 days
Source: Vitaflo Introduction to PKU booklet
Figure 2: Inheritance of PKU of age.4 All naturally occurring proteins contain phenylalanine, so the diet for PKU can only contain very small amounts of natural protein. However, as phenylalanine is an essential amino acid, it must be provided in small quantities in the diet to allow for growth of the child with PKU. Additional ‘safe’ protein is provided as a protein substitute containing tyrosine and all other essential and non-essential amino acids, except phenylalanine. The amount of natural protein tolerated by each child will vary and depends on the residual enzyme activity present. There is a spectrum of severities of PKU from very mild PKU (children may tolerate 20g natural protein or more per day) to very severe PKU (children tolerate only 3.0-5.0g natural protein per day). Initially, this means a phenylalanine-free formula is given to a baby with PKU until phenylalanine levels have fallen to within a safe range. Subsequently, the phenylalanine-free formula is given in conjunction with breastfeeding, or a measured quantity of standard infant formula. A breastfeeding mum requires considerable support to continue expressing her breast milk in the initial stages of treatment.
The PKU diet consists of four main parts:1 Restriction of all sources of natural protein No meat, fish, chicken, cheese, pulses, eggs or nuts are allowed, as they are too high in protein and phenylalanine. Other foods such as bread, pasta and pastries, biscuits or cakes also contain significant amounts of protein for most people with PKU and are usually replaced by special low protein foods available on prescription.
2 Phenylalanine exchangesThese are measured quantities of foods containing some protein, such as potatoes, sweetcorn, peas, rice, baked beans, cereals and milk. 1.0g protein = 50mg phenylalanine. These foods need to be carefully weighed out at each meal. Families are taught how to read nutritional information on food labels and work out the amount of food that contains 1.0g protein or one exchange.
3 Protein substituteThis is the ‘medicine’ in the PKU diet as it is essential and makes the PKU diet nutritionally
www.NHDmag.com July 2016 - Issue 116 - Supplement 3

is the lowest calorie ready-to-feed protein substitute for PKU.We’ve added two new flavours to the range. Red - Berry Blast, and White - Caribbean Crush.
Available in 15g PE and 20g PE pack sizes. Now giving your patients even more choice.
Contact your Vitaflo representative or click here for more information.
A Nestlé Health Science Company
new new
Vitaflo International Ltd, Suite 1.11, South Harrington Building, 182 Sefton Street, Brunswick Business Park, Liverpool L3 4BQ, UK. Tel: +44 (0)151 709 9020 Web:www.vitafloweb.com PKU air is a food for special medical purposes
® Reg. Trademarks of Société des Produits Nestlé S.A. © 2015 All rights reserved. Société des Produits Nestlé S.A.
coffee fusion citrus twistberry blast caribbean crush
July 2016 NHD0716

is the lowest calorie ready-to-feed protein substitute for PKU.We’ve added two new flavours to the range. Red - Berry Blast, and White - Caribbean Crush.
Available in 15g PE and 20g PE pack sizes. Now giving your patients even more choice.
Contact your Vitaflo representative or click here for more information.
A Nestlé Health Science Company
new new
Vitaflo International Ltd, Suite 1.11, South Harrington Building, 182 Sefton Street, Brunswick Business Park, Liverpool L3 4BQ, UK. Tel: +44 (0)151 709 9020 Web:www.vitafloweb.com PKU air is a food for special medical purposes
® Reg. Trademarks of Société des Produits Nestlé S.A. © 2015 All rights reserved. Société des Produits Nestlé S.A.
coffee fusion citrus twistberry blast caribbean crush
July 2016 NHD0716
PAeDIATRIC
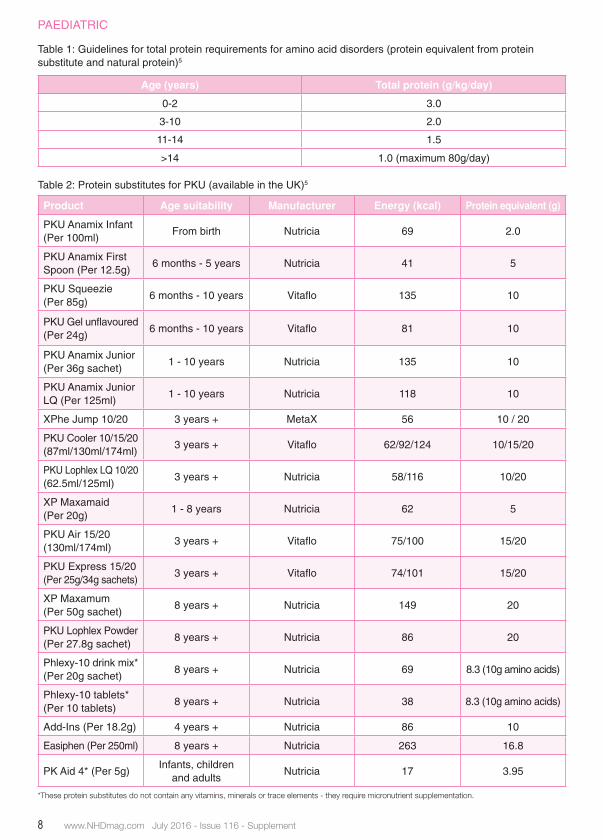
Table 1: Guidelines for total protein requirements for amino acid disorders (protein equivalent from protein substitute and natural protein)5
Age (years) Total protein (g/kg/day)
0-2 3.0
3-10 2.0
11-14 1.5
>14 1.0 (maximum 80g/day)
Table 2: Protein substitutes for PKU (available in the UK)5
Product Age suitability Manufacturer Energy (kcal) Protein equivalent (g)
PKU Anamix Infant (Per 100ml)
From birth Nutricia 69 2.0
PKU Anamix First Spoon (Per 12.5g)
6 months - 5 years Nutricia 41 5
PKU Squeezie (Per 85g)
6 months - 10 years vitaflo 135 10
PKU Gel unflavoured(Per 24g)
6 months - 10 years vitaflo 81 10
PKU Anamix Junior (Per 36g sachet)
1 - 10 years Nutricia 135 10
PKU Anamix Junior LQ (Per 125ml)
1 - 10 years Nutricia 118 10
XPhe Jump 10/20 3 years + MetaX 56 10 / 20
PKU Cooler 10/15/20(87ml/130ml/174ml)
3 years + vitaflo 62/92/124 10/15/20
PKU Lophlex LQ 10/20 (62.5ml/125ml)
3 years + Nutricia 58/116 10/20
XP Maxamaid(Per 20g)
1 - 8 years Nutricia 62 5
PKU Air 15/20(130ml/174ml)
3 years + vitaflo 75/100 15/20
PKU express 15/20(Per 25g/34g sachets)
3 years + vitaflo 74/101 15/20
XP Maxamum(Per 50g sachet)
8 years + Nutricia 149 20
PKU Lophlex Powder(Per 27.8g sachet)
8 years + Nutricia 86 20
Phlexy-10 drink mix*(Per 20g sachet)
8 years + Nutricia 69 8.3 (10g amino acids)
Phlexy-10 tablets* (Per 10 tablets)
8 years + Nutricia 38 8.3 (10g amino acids)
Add-Ins (Per 18.2g) 4 years + Nutricia 86 10
easiphen (Per 250ml) 8 years + Nutricia 263 16.8
PK Aid 4* (Per 5g) Infants, children
and adults Nutricia 17 3.95
*These protein substitutes do not contain any vitamins, minerals or trace elements - they require micronutrient supplementation.
8 www.NHDmag.com July 2016 - Issue 116 - Supplement
safe and adequate. The protein substitute contains all essential and non-essential amino acids, except phenylalanine, with added vitamins, minerals and trace elements. The protein substitute must be given every day, spread out evenly over the course of the day, usually three to four times per day In patients with amino acid disorders such as PKU, who require severe restriction of natural protein intake, the provision of a suitable protein substitute is essential for two reasons:
i) To prevent protein deficiencyii) To optimise metabolic control5
There are guidelines on the amount of total protein equivalent (from the protein substitute and from natural protein) that children with PKU should be having, according to their age, weight and severity of PKU (see Table 1). There are many PKU protein substitutes available in the UK for children with PKU (see Table 2). The protein substitutes are presented in different forms, such as powders, liquids, purees and tablets (for older children and adults). They are also available in numerous different flavours and tastes, as well as unflavoured versions.
4 ‘Free’ foods - These are low protein pre-scribable foods, as well as foods that are naturally low in phenylalanine such as some vegetables and all fruits (except passion fruit). They are called ‘free’ foods as they contain very little phenylalanine and do not need to be measured/weighed to be incorporated into the PKU diet.
WeANINGBabies with PKU can be weaned at a similar age as other children, but may benefit from weaning before six months of age.6
Weaning is commenced at around six months of age and not before four months or 17 weeks of age. In babies with PKU, there may be some advantages to starting the weaning process slightly earlier than six months.6 This is because there are many additional components to weaning a PKU baby, such
as the introduction of a more concentrated protein substitute, measuring phenylalanine exchanges and encouraging low phenylalanine ‘free’ foods.6
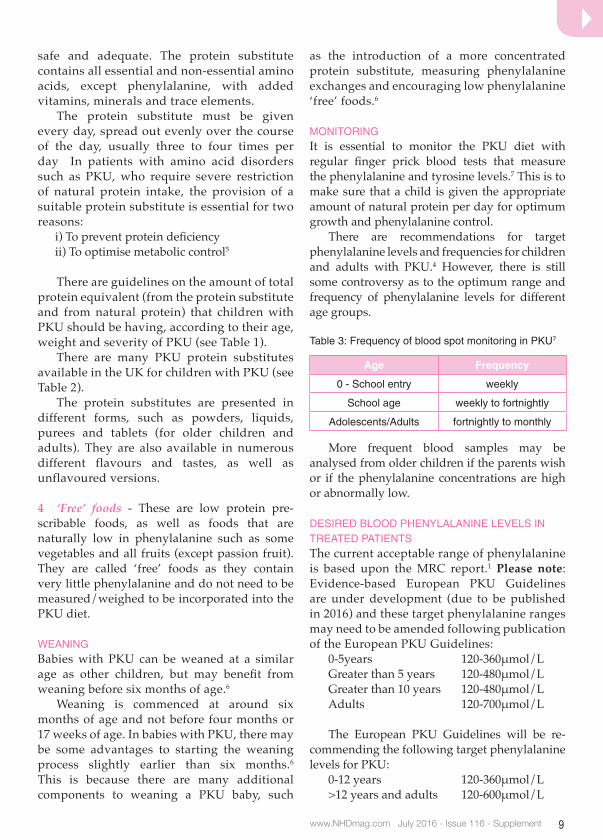
MONITORINGIt is essential to monitor the PKU diet with regular finger prick blood tests that measure the phenylalanine and tyrosine levels.7 This is to make sure that a child is given the appropriate amount of natural protein per day for optimum growth and phenylalanine control. There are recommendations for target phenylalanine levels and frequencies for children and adults with PKU.4 However, there is still some controversy as to the optimum range and frequency of phenylalanine levels for different age groups.
Table 3: Frequency of blood spot monitoring in PKU7
Age Frequency
0 - School entry weekly
School age weekly to fortnightly
Adolescents/Adults fortnightly to monthly
More frequent blood samples may be analysed from older children if the parents wish or if the phenylalanine concentrations are high or abnormally low.
DeSIReD BLOOD PHeNYLALANINe LeveLS IN TReATeD PATIeNTSThe current acceptable range of phenylalanine is based upon the MRC report.1 Please note: Evidence-based European PKU Guidelines are under development (due to be published in 2016) and these target phenylalanine ranges may need to be amended following publication of the European PKU Guidelines:
0-5years 120-360μmol/LGreater than 5 years 120-480μmol/LGreater than 10 years 120-480μmol/LAdults 120-700μmol/L
The European PKU Guidelines will be re-commending the following target phenylalanine levels for PKU:
0-12 years 120-360μmol/L >12 years and adults 120-600μmol/L
www.NHDmag.com July 2016 - Issue 116 - Supplement 9
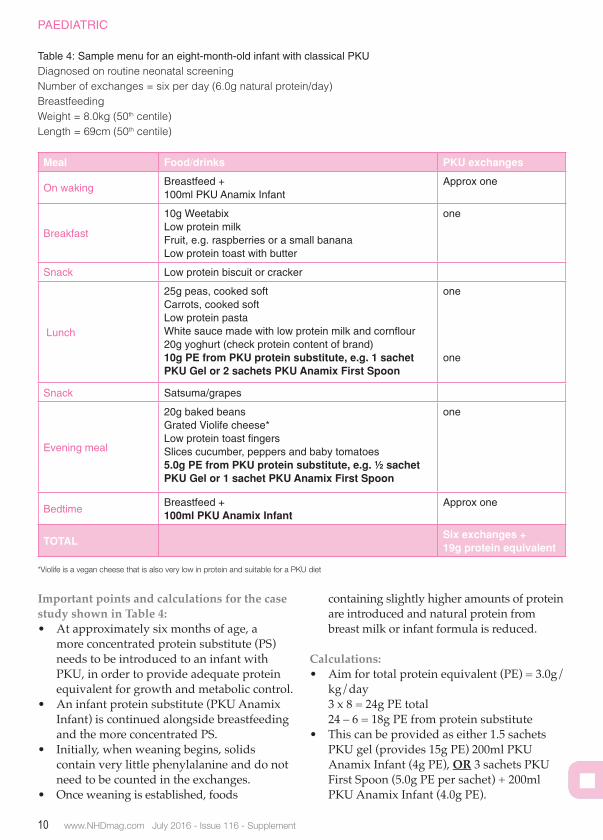
Important points and calculations for the case study shown in Table 4:• At approximately six months of age, a
more concentrated protein substitute (PS) needs to be introduced to an infant with PKU, in order to provide adequate protein equivalent for growth and metabolic control.
• An infant protein substitute (PKU Anamix Infant) is continued alongside breastfeeding and the more concentrated PS.
• Initially, when weaning begins, solids contain very little phenylalanine and do not need to be counted in the exchanges.
• Once weaning is established, foods
containing slightly higher amounts of protein are introduced and natural protein from breast milk or infant formula is reduced.
Calculations:• Aim for total protein equivalent (PE) = 3.0g/
kg/day 3 x 8 = 24g PE total 24 – 6 = 18g PE from protein substitute• This can be provided as either 1.5 sachets
PKU gel (provides 15g PE) 200ml PKU Anamix Infant (4g PE), OR 3 sachets PKU First Spoon (5.0g PE per sachet) + 200ml PKU Anamix Infant (4.0g PE).
PAeDIATRIC
Meal Food/drinks PkU exchanges
On wakingBreastfeed + 100ml PKU Anamix Infant
Approx one
Breakfast
10g WeetabixLow protein milkFruit, e.g. raspberries or a small bananaLow protein toast with butter
one
Snack Low protein biscuit or cracker
Lunch
25g peas, cooked softCarrots, cooked softLow protein pastaWhite sauce made with low protein milk and cornflour20g yoghurt (check protein content of brand)10g PE from PkU protein substitute, e.g. 1 sachet PkU gel or 2 sachets PkU Anamix First Spoon
one
one
Snack Satsuma/grapes
evening meal
20g baked beansGrated violife cheese*Low protein toast fingersSlices cucumber, peppers and baby tomatoes5.0g PE from PkU protein substitute, e.g. ½ sachet PkU gel or 1 sachet PkU Anamix First Spoon
one
Bedtime Breastfeed + 100ml PkU Anamix Infant
Approx one
TOTAL Six exchanges +19g protein equivalent
Table 4: Sample menu for an eight-month-old infant with classical PKUDiagnosed on routine neonatal screeningNumber of exchanges = six per day (6.0g natural protein/day)Breastfeedingweight = 8.0kg (50th centile)length = 69cm (50th centile)
*Violife is a vegan cheese that is also very low in protein and suitable for a PKU diet
10 www.NHDmag.com July 2016 - Issue 116 - Supplement

As some of these disorders are identified on newborn screening and treatment is optimised early, this group are surviving beyond their adolescent years and require planning for their long-term health requirements. Despite many official reports from the National Service Framework for Children,2 Royal College of Nursing3 and Royal College of Paediatrics and Child Health4 highlighting the need for a smoother transition of care, not many departments have the correct models to assist in this process. Transition is best described as the purposeful, planned movement of adolescents with chronic medical conditions from child-centred to adult-orientated health care.5 The process should acknowledge not only the medical needs of the young adult, but also their psychological, social, educational and overall wellbeing. The ultimate goal is to empower the young adult to make informed decisions in relation to their health outcomes, and support them in reaching their full potential in society.6
CHALLeNGeSThere are many factors that impede the transition process, especially as the IMD patient requires management of complex issues, such as modified diets, varying regimes of medicines, physical, mental and/or learning disability affecting daily living, access to emergency care, fertility and inheritance of their genetic condition. It is a multidisciplinary team approach often requiring community input.
A lack of engagement from the young adult and their family can make transitioning very challenging. This may be caused by their lack of understanding for the rationale behind this process. One American source reported that less than half of parents had discussed the health needs of their child with their health provider.7 There is a danger that the young adult may become lost to follow-up if there is no clear guidance regarding the transfer of their care. Within my centre, transition is a four-staged process with introduction to the adult IMD team at the third stage. Even after the fourth appointment where both teams review the young adult, patients remain under the care of the paediatric team until they have been seen solely in the adult setting. This is to prevent misunderstanding of who the care provider is between appointments, where the patient is ‘in limbo’. Miscommunication, conflict and contradictory advice must be avoided during this period so that the young adult does not feel that neither the paediatric nor the adult team are responsible for their care.8
The bond between the paediatric team and the young adult and their family will have been established from early on. The paediatric physician may have been the person who diagnosed the rare IMD condition, with the paediatric multidisciplinary team offering support to the family during the distressing initial stages of diagnosis. The team will have gone through a journey with this family; from diagnosis to schooling
TRANSITIoNING THe YoUNG ADUlT wITH AN INHeRITeD meTABolIc DISeASeInherited Metabolic Diseases (IMD) are a rare group of disorders of metabolism leading to an imbalance of chemicals. This can negatively impact organ systems which may have irreversible effects to development.1
Heidi ChanPractising Adult IMD Dietitian, Guy’s and St Thomas’ Hospital
Heidi has over a decade of continuous clinical practice in surgery, intensive care and gastroenterology with the past seven years in ImD. Her special interest is in scientific writing, particularly within ImD.
CONDITIONS & DISORDeRS
www.NHDmag.com July 2016 - Issue 116 - Supplement 11

0800 988 2488 www.mevalia.com [email protected]/mevaliauk
Taste, our secret ingredient.
EGG REPLACERLow ProteinEgg Substitute
500 g
PIP CODE: 401-7943
NEW
Job No. Stage Version
Creative PM Date
Comments
J001433 Concept 1
RH/HP EL 23/10/2015
GIVE US A CALL OR EMAIL FOR FREE SAMPLES
In partnership with
ALL YOUR FAVOURITES DELIVERED TO YOUR DOORINTRODUCING THE MEVALIA HOME DELIVERY SERVICEMevalia and Dialachemist have teamed up to bring you a greathome delivery service. Now you can have all of your favourite Mevalia products delivered straight to an address of your choice.
Dialachemist are a Lancashire based, fully General Pharmaceutical Council (GPhC) regulated online pharmacy. We are working with them to bring you this UK based home delivery service.
To register for this service you must speak to your dietitian.They can register you so you can order your favourite Mevalia products whenever you need them. You can fi nd more information about this service on our website: www.mevalia.com
J001469 - Mevalia DPS Ad_v2.indd All Pages 27/05/2016 17:41

0800 988 2488 www.mevalia.com [email protected]/mevaliauk
Taste, our secret ingredient.
EGG REPLACERLow ProteinEgg Substitute
500 g
PIP CODE: 401-7943
NEW
Job No. Stage Version
Creative PM Date
Comments
J001433 Concept 1
RH/HP EL 23/10/2015
GIVE US A CALL OR EMAIL FOR FREE SAMPLES
In partnership with
ALL YOUR FAVOURITES DELIVERED TO YOUR DOORINTRODUCING THE MEVALIA HOME DELIVERY SERVICEMevalia and Dialachemist have teamed up to bring you a greathome delivery service. Now you can have all of your favourite Mevalia products delivered straight to an address of your choice.
Dialachemist are a Lancashire based, fully General Pharmaceutical Council (GPhC) regulated online pharmacy. We are working with them to bring you this UK based home delivery service.
To register for this service you must speak to your dietitian.They can register you so you can order your favourite Mevalia products whenever you need them. You can fi nd more information about this service on our website: www.mevalia.com
J001469 - Mevalia DPS Ad_v2.indd All Pages 27/05/2016 17:41

CONDITIONS & DISORDeRS
achievements, making it difficult to break the bond.7 Conversely, if this bond has not been established and oppositional behaviour occurs with non-compliance from the parent and patient, abrupt transition may appear tempting, so the young adult can then establish a fresh start with the adult team.8 However, it may result in the young adult feeling rejected by their paediatric carers and may prevent trust being established with the new care provider, the adult team. In order to see the paediatric physician, who may still be the most suitable caregivers, young adults may not wish to attend a children’s hospital, or to find themselves waiting in a room with toys. This can lead to non attendance6 due to embarrassment and disengagement as the young adult may feel that his/her needs are not being adequately met. What is the correct age for transition? Should it be when the physician feels that they are ready? Table 1 shows data from 628 respondents from the American Academy of Paediatrics to a questionnaire regarding the age at which paediatricians think transition planning should begin.7 It has been reported that some services use a cut off age range of 15 to 20 years, and some use events such as school leaving as a trigger for transition.8 A systematic review identified two studies transferring patients at aged 18 and eight studies ranging between ages 16 to 20.9 The authors suggested using tools to measure self-management and advocacy skills for preparation of transition instead of age9 to avoid inconsistency. It is clear that the timing of transition is paramount and variable; however, it should not be one event, but a series of processes. The geographical location of the adult service can be a deterrent to families who are accustomed to the paediatric location.9 Transition should not
be avoided or delayed, even with both services in close proximity. Complex IMD is managed by other teams such as cardiology, liver, renal, neurology and/or dental, which may not be at the specialist IMD centre. In my experience, it can be very stressful for the family when transferring to more than one adult specialty at one time. However, a disparity of care and access occurs when the young adult remains under local paediatric gastroenterology, for example, having accomplished a smooth transfer into adult IMD services. Another barrier to transition may be the lack of specialist adult physicians, which particularly affects IMD as this is an evolving service. Many young adults are seen by the paediatric physician, clinical nurse and dietitian as there is no adult service to refer them onto. Some IMD dietitians have a split role managing both paediatric and adult patients. The young adult will then be familiar with the existing team and there may be reluctance to transition if the staff and location remain the same. Nonetheless, adult-related topics should be explored with the young adult and patient involvement should be encouraged.
PATIeNT eXPeRIeNCeSFocus groups have been used to assess the young adult’s experience of transition. The themes recognised after transcribing their interviews from various literature of those with long-term health conditions were categorised into the following headings:• Expectations of the transition10
• Meeting the new team10
• Life decision support10
• Support from others10
• Timing10
• Physician mistrust11
Table 1: Appropriate age for transition7
Age (years)Adolescents with special needs
(%)Adolescents without special needs
(%)
<12 3 2
12-14 6 6
15-17 25 26
18-20 62 65
Don’t know 4 2
Does not total to 100% due to rounding.
www.NHDmag.com July 2016 - Issue 116 - Supplement14

• Difficulty with employers11
• Stress in personal relationships11,12
• Moving from a familiar to an unknown ward culture12
• Being prepared for transfer12
• Achieving responsibility12
One quote from a young adult which implies lack of experience and interest of the physician was the following: “Dr X is my primary doctor but he doesn’t really know anything about the disease, so I have to tell him what to do.”
Table 2: Strategies for successful transitions
Focus Intervention Rationale Strategies
Young adulteducation on their condition
Self-efficacy One-to-one teaching9
Increase confidence visual resources
Achieve responsibility12 Peer support groups
Internet based teaching
Informed decision-making Patient involvement3,4 Motivational interviewing
Agree goals on transition documents and timeline to achieve3
Personnel Named transition link3,6,9,13 Continuity of care One point of contact3,9,13
Structured transition process
Attend all transition clinics
Prepares young adultOffer a visit to the adult setting
Coherent administrative support
Prevent young adult being lost between appointments
Checklist before transfer6,8
Set transition clinics in the diary for the year
Training by Royal Colleges4 Increase awareness and skills
Mandatory within the curriculum for allied health, nurse specialist and trainees
Service Joint paediatric and adult clinic
Gradual introduction to adult services9
Adult team to attend paediatric clinics
Improve information sharing
Letters to be addressed to the young adult
Young adult clinicDiminishes feeling lost amongst general clinics
Set up young adult clinic on a different day to other clinics
Out of hours contactApproachable team offering support at times convenient to the young adult
Provide telephone contacts for emergency care
enhance follow-up Prevent consecutive non-attendance
Contact the young adult to enquire rationale for non-attendance
Include community services
Continuity of careOpen channels of communication
engagement with the General Practitioner
www.NHDmag.com July 2016 - Issue 116 - Supplement 15

CONDITIONS & DISORDeRS
Emotions during transition were also examined and coded in qualitative literature describing feelings of abandonment11 and a feeling of letting go without knowing what the future entails.12
Positive experiences around inclusion of decision-making and being treated like an adult include quotes such as:12
“At the paediatric centre they’d talk to the parents and say, ‘you must make sure your child takes medication’. At the adult centre, they tell you the benefits of it, they tell you what happens if you don’t take it and leave it in your hands, so they give you a lot of control…they do talk to you like you’re an adult; it is your decision.” “The most important thing to me when transferring to the adult clinic was that all the decisions were made with me involved and I was able to talk about what was going to happen when I saw the doctors, which I never had a chance to do in the children’s clinic.” It has been suggested that these positive experiences should be shared with paediatric patients preparing for transition11 to manage expectations.
ReCOMMeNDATIONSGeneric and disease specific transition models or programs have been described.2,8 Within my centre, a specific IMD transition model was created which can be applied for use to other chronic conditions. The Welsh IMD service identified geographical gaps in transition.13
Whichever model is adopted, the principles for successful transitions should include these valuable suggestions summarised in Table 2. Physicians in the adult services should avoid making drastic treatment changes and extensive investigations8 at the first appointment to prevent feelings of unease and to manage expectations of the young adult and their family. The physician is required to build a rapport confidently whilst engaging the young adult. Health professionals ought to be ready to invest the necessary time and support to prepare young adults to take responsibility for their own health. Allowing sufficient time for consultations, active listening by the multidisciplinary team and anticipation of young adults’ involvement may enhance their experience of themselves as valuable contributors.
CONCLUSIONLong-term outcomes of IMD patients receiving medical and dietary treatment is undefined. Therefore, transition from paediatric to adult services should be a gradual and planned process with engagement from the young adult and their family. Special consideration is required when transitioning the young adult with complex needs. Transition champions have been proposed as part of a gold standard within the skilled multidisciplinary team.8,9 The transition process should encompass a systemic outlook covering not only health, but also vocational and psychosocial aspects.9,12
References1 BritishInheritedMetabolicDiseasesGroup.www.bimdg.org.uk/site/index.aspaccessedon6.3.20162 DepartmentofHealth(2006).NationalServiceFrameworkforChildren,YoungPeopleandMaternityServices.Transition:gettingitrightforyoung
peopleImprovingthetransitionofyoungpeoplewithlong-termconditionsfromchildren’stoadulthealthservices3 Royal College of Nursing (2013). Lost in transition: moving young people between child and adult health services. London, RCN4 RoyalCollegeofPaediatrics&ChildHealth(2003).TheIntercollegiateWorkingPartyonAdolescentHealth.BridgingtheGaps:HeathCarefor
Adolescents, London, RCPCH5 Blumetal(1993).Transitionfromchild-centredtoadulthealthcaresystemsforadolescentswithchronicconditions.ApositionpaperoftheSocietyfor
Adolescent Medicine. J Adolesc Health. 14(7): 570-66 Rosen et al (2003). Transition to adult healthcare for adolescents and young adults with chronic conditions: position paper of the Society for
Adolescent Medicine. J Adolesc Health. 33(4): 309-117 McManus et al (2008). Pediatric Perspectives and Practices on Transitioning Adolescents with Special Needs to Adult Health Care. Fact Sheet No 6.
The National Alliance to Advance Adolescent Health8 VinerR(1999).Transitionfrompaediatrictoadultcare.Bridgingthegapsorpassingthebuck?ArchDisChild.81:271-2759 Crowley R et al (2011). Improving the transition between paediatric and adult healthcare: a systematic review. Arch Dis Child. 96: 548-55310TalletA(2014).Transition:aqualitativestudyofyoungadults’experiencesoftransferringfrompaediatrictoadulthealthcareservices.ArchDisChild.
99: Suppl 1 (G467)11Bemrich-StolzCJetal(2015).ExploringAdultCareExperiencesandBarrierstoTransitioninAdultPatientswithSickleCellDisease.IntJHematolTher
1(1). Doi: 10.15436/2381-1404.15.003. Epub 2015 Sep 612FegranLetal(2014).Adolescents’andyoungadults’transitionexperienceswhentransferringfrompaediatrictoadultcare:Aqualitative
metasynthesis. International Journal of Nursing Studies 51;123-13513WelshAssemblyGovernment.AllWalesInheritedMetabolicDiseaseStandardsforChildrenandYoungPeople’sSpecialisedHealthcareServices.
www.wales.nhs.uk/sites3/Documents/355/Metabolic%20Eng%20web.pdf (accessed on 13.3.2016)
www.NHDmag.com July 2016 - Issue 116 - Supplement16

For full article references please email info@ networkhealth group.co.uk
Newborn screening for the diagnosis of PKU and its treatment with a low phenylalanine (Phe) diet (see Table 1) is one of the major public health success stories of the last century. UK screening began in the 1960s and the heel prick screening test was introduced in 1969. Originally, it was believed that children could cease the low Phe diet once brain growth was complete. However, a growing body of evidence now suggests that people with PKU should remain on a low Phe diet for life.2 High Phe concentrations in adults have shown to affect executive functioning and organisational skills,3-5 lead to trouble with concentration,6 cause increased psychiatric symptoms,7 slower reaction times8
and low mood.6,9 It is also believed that there are many older adults in care facilities, where a PKU diagnosis was never originally given. Our screened cohort of PKU patients at University Hospitals Birmingham is now approaching middle adulthood, with the oldest patients in their 40s. In the UK, we are observing similar levels of obesity in our PKU group as the general population.12 Other countries have also found similar rates of obesity in children and adults as their general population.14-17
As our PKU adults age, we question if we will see similar rates of obesity-related co-morbidities as in the general population. Currently, there are no reported cases in the literature of PKU patients with Type 2 diabetes, but in our centre, we had a maternal PKU lady develop gestational diabetes.
The incidence of metabolic syndrome was assessed in a Portuguese PKU cohort, aged between three to 30 years.14 Although participants had a carbohydrate-rich diet, they did not have a higher incidence of overweight, obesity, central obesity or metabolic syndrome than controls. It was found that triglycerides and HDL were higher and glucose and insulin concentrations were lower than controls.14 Research into an older group of PKU adults aged between 18 to 57 years found that they had low to normal levels of cholesterol, despite 72% of the group being obese.18 Results seem to suggest that metabolic syndrome in PKU does not follow the same course as described for the general population and possibly those with PKU have a lower incidence. Further work is needed to look into the mechanisms behind this and potential consequences.
WHAT IS CAUSING THe OBeSITY?There is a lot of speculation as to what could be causing obesity in the PKU cohort. On paper, the PKU diet seems healthy; plenty of vegetables and fruit and avoidance of animal products and, therefore, saturated fat. However, due to the avoidance of natural protein, the PKU diet is higher in carbohydrate and lower in fat and fibre than the recommendations for the general population.14,19-21 Are adults on the PKU diet simply not satiated due to the composition of their diet and, therefore, do they consume more calories to make them feel fuller?
oBeSITY IN ADUlTS wITH PHeNYlKeToNURIA
Does following the recommended lifelong restrictive PkU diet bring other nutritional challenges? Problems have been reported in the literature for people with PkU, including non-optimal bone health,10 nutritional deficiencies11 and obesity.12,13
Louise Robertson Specialist Dietitian
louise and Sarah are Specialist Dietitians working with adults with inherited metabolic disorders, with PKU being their biggest cohort of patients.
WeIGHT MANAGeMeNT
Sarah Howe Specialist Dietitian
www.NHDmag.com July 2016 - Issue 116 - Supplement 17

WeIGHT MANAGeMeNT
PROTeINNatural protein promotes satiety and this is obviously restricted in the PKU diet. The protein substitute drinks required (providing all the essential amino acids excluding phenylalanine, vitamins and minerals) are based on amino acids and not whole protein, which could theoretically be less satiating. We are currently hypothesising that, due to this, people are reaching for high carbohydrate, low protein foods to feel full. These could be convenience lower protein snacks which tend to be higher in fat and sugar (crisps, chips, chocolate bars and biscuits), or low-protein prescription foods (low-protein biscuits, cakes and crackers). This may lead to overeating, especially in a non-active PKU patient.
SUGAR AND FIBReRecently, new guidelines have been released advising the general population to reduce their sugar consumption to 5% of their energy intake, to prevent excess energy intake and aim to increase fibre intake to 30g a day, thereby decreasing the risk of cardio metabolic disease and colorectal disease.22
Many of the low-protein foods on prescription, including cereals, biscuits, dessert mixes and cakes, are high in sugar. In the past, these foods have been labelled as ‘free’ due to low-protein content and, therefore, there is concern that they are freely consumed. Very much like the general population, we are advising that these foods are kept to a minimum in our adults. Another area of concern is the consumption of sugary, fizzy drinks and fruit juices in the PKU cohort. People with PKU are unable to consume aspartame due to its Phe content. This is a message that is very firmly fixed from childhood and rather than try and find a diet or no-added sugar drink with an alternative sweetener, many adults opt for full-sugar versions. These drinks provide a large quantity of sugar and calories, sabotaging any effort to lose weight. In addition, the promotion of fresh fruit juices and smoothies as a healthy drink has been a message difficult to argue. As most fresh fruit is allowed freely in the PKU diet, we have had to educate the group that consuming the whole fruit is preferable to reduce calorie and sugar intake and also increase fibre consumption.
A high-fibre intake is difficult to achieve following the PKU diet due to the higher protein content of foods containing insoluble fibre (beans, oats, nuts, wholegrain cereals, grains) and low-protein prescription foods being very low in fibre. However, the low-protein foods available on prescription are now realising the niche for fibre and are starting to include more in their products.
eXCHANGe FOODSThe choice of exchange foods could also be an issue. Many of the foods allowed as exchanges (one exchange is the equivalent of 1.0g of protein/50mg of Phe) are high-carbohydrate, for example, chips, crisps, cereal bars and potato products. Education regarding healthy exchanges and how to incorporate them into a PKU diet is important. For example, normal rice, peas and sweetcorn can be used for exchanges instead of chips, crisps, chocolate and biscuits. For adults with a higher Phe tolerance, we are now encouraging them to include foods containing moderate protein in measured quantities to fit in with allowed exchanges. These include yoghurt, soft cheese, hummus, nuts, normal low-sugar cereals, oats and even eggs for those with a higher protein intake. We believe these foods may be more satiating and reduce the need for regular snacking.
MeTABOLIC CONTROLThere may be a link between metabolic control and obesity. We found a direct correlation between BMI and Phe concentrations12 and patients in Portugal were found to have a higher prevalence of overweight and obesity in patients with poor metabolic control.14
In the USA, they found non-compliant females were more likely to be overweight or obese than compliant females, but no difference in males.23 High Phe concentrations can affect organisation skills and executive functioning,3-5 which could affect the ability to plan and cook healthy foods and order low protein foods on prescription. Patients may find it easier to rely on takeaways and convenience snack foods, but these foods are higher in protein, fat and
www.NHDmag.com July 2016 - Issue 116 - Supplement1

calories. High Phe concentrations also have a negative effect on mood,6,7,9 which could negatively affect food choices.
eXeRCISeExercise and activity in PKU is an area of little research. Anecdotally across the centres, we are getting more reports of people asking for sports nutrition advice for the PKU diet. However, we do not know if activity levels across the PKU cohort are similar to the general population. It has been speculated that those with higher blood Phe concentrations may struggle with organisation and motivation to exercise which could contribute to overweight and obesity.12 However, more work is needed in this area.
CONCLUSIONThe restricted diet for PKU is not only complex to follow but requires dedication and motivation. Research is showing a number of associated problems, including similar incidence of obesity as the general population. A dietary assessment of a PKU patient should not just be about ensuring low Phe concentrations, but to combine this with a healthy diet to prevent overweight and obesity. We need to spend time to educate patients on the myths and often firmly fixed nutritional beliefs to ensure they are following not only a low Phe diet, but a healthy satiating one as well. Overtime, we will be able to capture more data on the development of obesity levels and metabolic syndrome and understand further how to help our patients.
Table 2: Tips for a healthy diet for PKUTable 1: Low phenylalanine diet
Avoidance of all foods high in phenylalanine (found in protein), e.g. meat, fish, soya, dairy, pulses, nuts.
Protein substitutes (amino acids excluding phenylalanine) taken three to four times per day. This includes ready to drink liquids, powders made into liquids or gels, pudding styles or tablets.
Measured amounts of phenylalanine using lower protein foods, e.g. potato, rice, sweetcorn, peas, baked beans - as 50mg Phe (1.0g protein) exchanges if counting strictly or if on a relaxed diet limit to small amounts.
Plenty of low-protein foods; naturally occurring or low protein foods on prescription to provide energy and variety in diet (e.g. low protein pasta, rice, bread, flour).
vitamins and minerals are included in the newer protein substitutes, but if not additional vitamins and minerals will need to be taken.
encourage sugar-free drinks; aspartame-free, sugar-free and diet fizzy drinks and squashes.
No more than 150ml a day of fruit juice or smoothie; choose the whole fruit instead.
Increase consumption of fruit and vegetables to boost fibre intake.
To try a lower sugar protein substitute.
Aim to choose high-fibre, low-protein food options on prescription (bread, pasta, crackers).
encourage healthy exchange foods: rice, rice noodles, low sugar high-fibre breakfast cereals, oats, sweetcorn, peas, high-fibre crackers. If higher Phe tolerance: yoghurt, soft cheese, hummus, fromage frais or nuts.
encourage healthy snacks: fruit, crackers, veg and free dip. Keep snacking on low-protein cakes, biscuits, crisps and desserts to a minimum.
It has been speculated that those with higher blood Phe concentrations may struggle with organisation and motivation to exercise which could contribute to overweight and obesity.
www.NHDmag.com July 2016 - Issue 116 - Supplement 19

My husband and I are both originally from Co Galway in Ireland and moved to Melbourne almost 10 years ago. Like a lot of other people from our side of the world, the original plan was to stay a year or two in Australia, but here we still are and have now started our little family. We welcomed our beautiful healthy daughter Caitlin into the world on Valentine’s Day 2015, at the Epworth Freemason’s hospital in East Melbourne. The second day after Caitlin was born she was given a heel prick test. Blood was withdrawn from Caitlin’s heel and was tested to determine if Caitlin had any genetic disorders. Approximately nine days later we were contacted and told that our daughter had Phenylketonuria (PKU). PKU is a rare genetic disorder that prevents the normal breakdown of a protein, phenylalanine (Phe). Untreated PKU can lead to intellectual disability, seizures and other serious medical problems such as brain damage. On that first day after being told, we felt as though we had been hit by a massive blow. It was so hard to comprehend the fact that our perfect newborn baby girl had an incurable genetic illness and would never be able to eat protein freely or likely never eat meat, fish, eggs or dairy. We couldn’t comprehend what Caitlin would be able to eat. The metabolic team at the Royal Children’s Hospital, Melbourne (RCH) set up an appointment for us to come to the hospital immediately after Caitlin’s PKU diagnosis. In that initial meeting we were advised of a medication that could help stimulate the deficient enzyme to
help allow more protein into Caitlin’s diet. The medication called Kuvan,1 we were told, did not work for all patients with PKU, and as the chance of our baby being responsive to Kuvan was one in five, the odds were against us. In order for our child to be prescribed Kuvan, there needed to be a minimum 30% drop in Phe levels after a load test. We hoped and prayed that Caitlin’s levels would drop enough to be approved and given the medication.
TeSTING FOR ReSPONSIveNeSSIn order to test Caitlin’s responsiveness to this medication, the medical team inserted a tube into Caitlin’s nose and down into her stomach. Caitlin being only nine days old was too young to swallow the tablet in the normal way. It was pretty difficult to watch the medical team feed a tube through her nose. Luckily, she had an excellent response to the load test. Caitlin’s levels were periodically taken over a 24-hour period and after that time, her Phe levels had dropped from 1100+ to below 400, well in excess of the required 30% drop to be granted access to the medication. This good news helped us to accept the fact that our very young baby had PKU and gave us hope that we had something that would help us live with this chronic illness. Kuvan is not available across the whole of Australia. Currently, it is available for PKU patients in the states of Victoria and Tasmania (the states covered by the RCH in Melbourne). We thank our lucky stars every day for the fact that we live in Victoria. This was definitely the silver lining in our cloud.
PKU: A PAReNT’S PeRSPecTIVe
Having an infant diagnosed with Phenylketonuria (PkU) can be a scary and challenging experience. Louise Conlisk’s daughter Caitlin was diagnosed with the condition and here she tells us how she and her husband have been helped and supported to live with PkU.
PAeDIATRIC
For full article references please email info@ networkhealth group.co.uk
Louise ConliskSAP Consultant, eRP Consulting Company Melbourne
louise has worked as an eRP consultant for over 12 years and now lives and works in melbourne, Australia. Her interests include reading, running and time spent outdoors. Since becoming a mother, she is so ‘time-poor’ that all her interests are mostly baby-related!
20 www.NHDmag.com July 2016 - Issue 116 - Supplement

In England, Sapropterin (Kuvan®) is not routinely commissioned and priority groups eligible for treatment with Sapropterin are the minority of pregnant women with PKU who are unable to establish adequate dietary control and achieve the target non-teratogenic range of Phe (100-300 µmol/L).2 For more information on Kuvan in the UK, see ‘More Information’ at the end of this article. One of our many questions about Kuvan was in relation to the cost. Initially we were informed that it would cost approximately $100 (approximately £50 or 64 EUR) a tablet with the amount of tablets per day increasing as the child grows. We worried about how we could afford this expense, but were relieved to hear that the cost of the medication was going to be covered by the hospital (with a minimal out-of-pocket charge to be covered by us).
STARTING THe MeDICATIONAs advised by the RCH, Caitlin did not start taking Kuvan until a few weeks after we introduced solids into her diet, which was close to when she turned seven months old. The Kuvan dosage was calculated using Caitlin’s weight and, initially, we were allowed to increase her protein by a small amount. As the weeks went by, if Caitlin’s levels were low or within range, the dietitian would on occasion recommend an increase of 0.5g to her daily protein allowance. Caitlin started on 2.0g of protein a day and now, at 15 months old, Caitlin is allowed to have 9.5g of protein daily. This is significantly more daily protein than what Caitlin would be able to have without the Kuvan medication. Caitlin is still breastfed along with bottle feeds of her PKU Anamix Infant/Gel drink. I am confident that when I stop breastfeeding, her protein intake capacity should increase. Caitlin’s current dosage is two tablets a day, one in the morning and one in the evening. Caitlin is administered Kuvan by dissolving it in a small amount of water and then mixing it with her food such as jam or apple puree which is then spoon fed to her. Caitlin normally takes the medication without any problem as she is quite used to it. On occasion, if she isn’t hungry, or is tired, it can take longer to get her to take the medicine. If we are eating out, we need to remember to bring the tablet and a small syringe to mix a small amount of water to it, so it is just a few more things to put in the baby bag.
LIvING WITH PKUAlong with the medication, the other prescriptions Caitlin currently takes are PKU Anamix Infant, PKU Anamix Gel and ProZero milk. To test Caitlin’s PHE levels, we do a blood test at home every week using a lancet to draw some blood from Caitlin’s finger to place on a Guthrie Card. The Guthrie Cards are posted to the screening laboratory at the RCH and the results are provided to us by phone each week by a dietitian from the Metabolic team. During this call, the protein allowance for the following week is also discussed. To manage Caitlin’s protein allowance, we carefully control her food intake every day and try to spread her protein allowance throughout three main meals to hopefully keep her fuller. She has 1.5 Weetabix in the morning, which works out to be 3.0g of protein, some low protein bread/pancakes/muffins for lunch and then whatever protein allowance is left over we give her for dinner. Without Kuvan, we would not be able to give Caitlin some of the regular food we currently give her, such as regular breakfast cereal, gluten-free bread and regular pasta. Caitlin goes to childcare four days a week since I returned to work. Due to her having PKU she cannot have the foods served by the kitchen at childcare, so we provide her with her own special lunch. We label all of her foods in her lunchbox with her name and the protein amounts contained in each food item, which we give to the childcare staff. They then put whatever food Caitlin doesn’t eat into a waste lunchbox. In this way we can weigh what Caitlin hasn’t eaten and accurately calculate the protein that Caitlin has consumed when not in our care.
Caitlin, leading as normal a life as possible
www.NHDmag.com July 2016 - Issue 116 - Supplement 21

PAeDIATRIC
PROS AND CONSKuvan has made a big impact on the foods we can give her. Having a higher protein allowance is of massive benefit in a lot of tangible and intangible ways. There are and will be psychological benefits, such as increased concentration levels and improvements to Caitlin’s overall behaviour. Caitlin’s quality of life is enhanced greatly, especially socially, as she can eat some ‘normal’ foods. In the future, there will be possibilities to actually eat a meal at a restaurant without having to bring Caitlin’s own food with us. All of this will contribute to a much happier, less restrictive childhood. Caitlin also does not have to eat as much of the low protein specialised PKU food due to taking Kuvan. If we need to give the tablet to Caitlin outside of our home, it isn’t too difficult; we just need to make sure that we have a little container to dissolve the tablet in. Kuvan has made going on family holidays a possibility for us too, as we can buy more foods off the shelf instead of having to bring all specialised food with us. The fact that Caitlin can have more protein in her diet is something we are very grateful for. The only real negative aspect of the medication is having to give a small child a tablet twice a day, which most of the time is fine ,but sometimes, as already mentioned, if we have a tired child on our hands it can be delicate.
SUPPORTThe RCH Metabolic team in Melbourne are truly amazing. We bring Caitlin to the Metabolic clinic at
the RCH three to four times a year. At these clinic appointments we meet with a dietitian and a doctor and go through Caitlin’s progress. We have a close relationship with the dietitians in particular and we are comfortable knowing that the management of our daughter’s condition is in very good hands. The team support us with all of the changes that happen in a young child, such as starting solids, and are extremely helpful with advice. They have provided letters for airlines when we travelled home last year, armed with a suitcase full of formula and medication. The Professor of the Metabolic department is hugely experienced in his field.
THe FUTUReWe are hopeful that Caitlin’s protein intake can continue to increase, given her levels are within range. As she grows older, we feel that she will be further enabled to reach her academic potential. Anything that helps my child live with this very restrictive condition and add more normality to her life is a massive bonus. We would love to consider moving back home to Ireland to be closer to our family, but Kuvan is not available there so moving back to Ireland for us is not an option. My biggest hope for the future is that other children with PKU are given the same opportunity as Caitlin to be given this medication. I sincerely hope too, that any health professionals or decision-makers considering whether to approve this medication for use, take into account the unquantifiable benefits in helping children with PKU lead a more normal life.
files/publications/Kuvan.pdf• NationalCentreforPharmacoeconomics,Ireland.http://www.ncpe.ie/wp-content/uploads/2009/06/Sapropterin-Kuvan-summary1.pdf
Comment from the EditorAt present, Kuvan is not considered a cost-effective alternative to dietary treatment and there is a limited amount of evidence for its effective use. The prospects for funding of Kuvan in the UK, however, are likely to improve if and when new evidence regarding clinical effectiveness is forthcoming. Professor Anita MacDonald has co-written research papers alongside other multinational metabolic healthcare professionals, which discuss this treatment and if used, how it should be monitored and managed. Click here . . . for references. In the future, greater scrutiny, stricter guidelines and increasing pressure to ensure cost-effectiveness will all be key factors in the decision-making before new medications are approved for NHS use. Continued support from UK clinical teams, sustained lobbying by patients/parents and carers, as well as by the NSPKU, will be crucial in ensuring that patients benefit from new developments in treatment. A pressure group by the name of Phedup has been formed, their website is www.phedup.co.uk - Emma
More information• NSPKU(2010).TheroleofSapropterin(Kuvan®)inthemanagementofPKUintheNHS:considerationsandprospectswww.nspku.org/sites/default/
www.NHDmag.com July 2016 - Issue 116 - Supplement22

NETWORK HEALTH DIGEST
A wealth of useful dietetic resources for all dietitians and nutritionists
Student zoneIntroducing our new resources specifically designed for students of Nutrition and Dietetics
•NHD eArticles with CPD •Live health news•dieteticJOBS.co.uk•Events and Courses•Essential links
• NHD Extra - our supplement with additional articles for subscribers
• NHD at-a-glance library of published articles
• NHD digital - view the latest issue of Network Health Digest as well as back issues
Login with your username and password to view the Subscriber zone.If you don’t have login details, you can check whether you are eligible for a FREE subscription to Network Health Digest at wwwNHDmag.com
www.NHD mag.com your essential resource
Make the most of your NHD Community!
Subscriber zone