nhpp6 - thrust areas of 12th five year plan (2012 2017) i
TRANSCRIPT

1
NHPP6 - Thrust Areas of 12th
Five Year Plan (2012 – 2017)
Quadrant – I
Personal details:
Role Name Affiliation
Principal Investigator Dr. C.P. Mishra Professor Department of Community Medicine Banaras Hindu University, Varanasi Uttar Pradesh, India
Paper Coordinator Dr. Davendra Kumar Taneja Director Professor Department of Community Medicine Maulana Azad Medical College New Delhi, India
Content Writer/Author Dr. Nilanjana Ghosh
Assistant Professor Dept. of Community Medicine North Bengal Medical College Siliguri Darjeeling, India
Content Reviewer Dr. Bratati Banerjee Professor Department of Community Medicine Maulana Azad Medical College New Delhi, India
Description of Module:
Items Description of Module
Subject Name Community Medicine
Paper Name National Health Policies and Programmes
Module Name/Title Thrust areas of 12th Five year Plan (2012 – 2017)
Module Id NHPP6
Pre-requisites Knowledge on five year plans; Knowledge on health and health related problems in India
Objectives At the end of this module the students will be able to:
State the outcome indicators of 12th
five year plans
Describe the thrust areas of the 12th
Five Year Plan with special reference to Universal Health Coverage (UHC) and National Health Mission (NHM)
•
Key words Five Year Plan, Thrust area, HLEG, NHM, UHC
2
Introduction
“A good plan implemented today is better than a perfect plan implemented tomorrow”.
Growth of a nation is symbiotically linked to its health. Health cannot be achieved by curative or
preventive services alone. Health sector needs to work in coordination and with convergence of various
sectors. Thus in India, for every five years, a plan w ith monitorable and achievable targets, keeping in
mind operational feasibility, is envisaged by health planners and policy makers. However,
notwithstanding all limitations, even if all cannot be achieved, the five year plans serve as a blueprint of
what actions to be implemented and act as a backbone for health planners and health workforce.
As optimum service delivery and effective service utilization go a long way in ensuring favorable
health indicators, proper planning at national level by policy makers ensures their adequate
implementation at all the three tiers of the extensive health care delivery system of the nation.
Recommendations of the Bhore committee were delivered through the first five year plan in 1951,
subsequently Kartar Singh Committee and others followed with successful implementation of other five
year plans followed with improvisation in each plan subsequently. After the eleventh five year plan in
(2007-2011), it was seen the health indicators were not as favorable as estimated and the country faced
newer challenges as well1. Problems of out of pocket expenditure (OOP), health workforce imbalance and
issues regarding affordability and quality of health services took the centre-stage.
Thus emerged the 12th
Five year plan (2012- 2017) to further enhance and expand the initiatives of
11th
Five year plan and achieve the much desired Universal Health Coverage. Redefining policies with
increasing incentivisation of state government, paying attention to determinants of health like water and
sanitation, and increasing GDP to 2.5% are few strategies envisaged2.
Learning outcomes
At the end of this module student should be able;
To know the outcome indicators of 12th
five year plans
To know the thrust areas of the 12th
Five Year Plan with special reference to Universal Health
Coverage (UHC) and National Health Mission (NHM)
3
Main Text
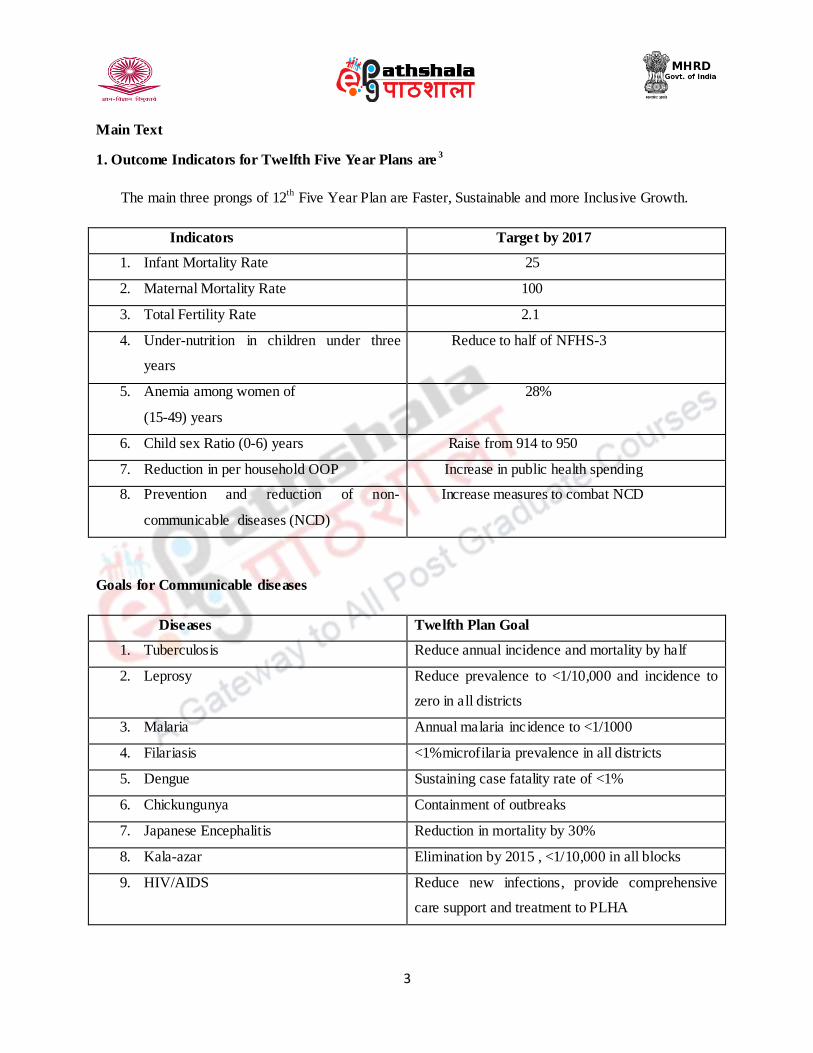
1. Outcome Indicators for Twelfth Five Year Plans are3
The main three prongs of 12th
Five Year Plan are Faster, Sustainable and more Inclusive Growth.
Indicators Target by 2017
1. Infant Mortality Rate 25
2. Maternal Mortality Rate 100
3. Total Fertility Rate 2.1
4. Under-nutrition in children under three
years
Reduce to half of NFHS-3
5. Anemia among women of
(15-49) years
28%
6. Child sex Ratio (0-6) years Raise from 914 to 950
7. Reduction in per household OOP Increase in public health spending
8. Prevention and reduction of non-
communicable diseases (NCD)
Increase measures to combat NCD
Goals for Communicable diseases
Diseases Twelfth Plan Goal
1. Tuberculosis Reduce annual incidence and mortality by half
2. Leprosy Reduce prevalence to <1/10,000 and incidence to
zero in all districts
3. Malaria Annual malaria incidence to <1/1000
4. Filariasis <1%microfilaria prevalence in all districts
5. Dengue Sustaining case fatality rate of <1%
6. Chickungunya Containment of outbreaks
7. Japanese Encephalitis Reduction in mortality by 30%
8. Kala-azar Elimination by 2015 , <1/10,000 in all blocks
9. HIV/AIDS Reduce new infections, provide comprehensive
care support and treatment to PLHA

4
2. Inclusive agenda for Health in the 12th
plan:
Monitoring and Evaluations
Representation in community fora with women having 50% representations
Training of health and rehabilitation professionals
Special services for poor, weak and disadvantaged population
Accessible and affordable services
Achieving Universal Health Coverage (UHC) through a model where:
- Through EHP (essential health package) clinical services at different levels are provided and
financed by the government.
- Universally providing preventive, promotive and rehabilitative health services
3. Recommendations of HLEG (High level Expert Group) on UHC emphasizing EHP at all levels
of health care with prioritization of primary health care
Universal Health Coverage Day is being observed every year, on 12th
December as a global initiative
by United Nations to ensure that every individual has access to health care without suffering from
financial hardship. On 12 December 2014, a global coalition will focus on universal health coverage to be
an important issue for the sustainable development and a priority for all nations. Universal Health
Coverage (UHC) means ensuring equitable access for all the citizens in any part of the country, regardless
of income level, social status, gender, caste or religion. It aims to provide affordable, accountable,
appropriate health service of assured quality. As such it includes promotive, preventive, curative and
rehabilitative care. India is committed to provide Universal Health Coverage for All during 12th
Plan
period (2012-2017). A High Level Expert Group (HLEG) on Universal Health Coverage (UHC) was
constituted by the Planning Commission.
The recommendations of HLEG are:
Health Financing and Financial Protection – GoI to increase GDP on health. Health services to
be provided by general taxation and OOP to be reduced. RSBY (Rashtriya Swasthya Bima
Yojna) to be implemented in full vigor.
Access to medicines, vaccines and technology – Essential drug list to be revised, expanded and
made suitable according to need. Safeguards by Indian Patents Law and TRIPS agreement.
Human resources for health – DHKI (District Knowledge Health Institutes) and Regional
Faculty Development sectors to be made operational and functional.

5
Health service Norms – National Health Package ensuring primary health care facilities for all
with special reference to urban poor.
Management and Institutional Reforms – National Health System Management Cadre to be
formed and made functional to look after the optimum utilisation of public health services.
Moreover NHRDA (National Health Regulatory and Development Authority), NDRDA (National
Drug Regulatory and Development Authority), NHPPT (National Health Promotion and
Protection Trust) also to be formed eventually.
Community Participation and Citizen Engagement – Participatory Health Councils to function
in place of existing Village Health committees.
Gender and Health - To take care of the vulnerable and disadvantaged gender beyond the
routine MCH (Maternal and Child Health) activities.
4. Other main core areas identified and strategies envisaged under the 12th
Five Year Plans are:1,2
1. Health Financing – People in India lie on the brink of poverty and sometimes death in order
to meet the medical expenses. Thus reducing the OOP burden by increasing the flexibility in
funding and providing state incentivisation is a seriously thought of measure. Moreover
outcome improvement by innovative payment methods has also been devised.
Models devised for funding are:
a. PPP (Public Private Partnership)
b. CSR (Corporate Social Responsibility) and Resource generation by facilities and
colleges
c. Cross- Subsidization of services
d. RSBY – A cashless health insurance cover of Rs. 30, 000 for a family of five , on
provision of a smart card which encompasses enlisted conditions and also alternative
health care facilities through private providers. However upward escalation of patients to
higher facilities is commonly noted.
Eligibility: Unorganized sector workers belonging to BPL category and their
family members (a family unit of five) shall be the beneficiaries under the
scheme.
Conditions included in the package are:
Hospitalization expenses up to Rs. 30,000
Over 725 predefined surgical packages

6
Maternity newborn care
Day care services
Cover all pre-existing diseases
1 day pre hospitalization and 5 days of hospitalization expenses
Transportation cost (Rs.100 per visit) with overall limit of Rs.1000 per year
Conditions excluded are:
Conditions not requiring hospitalization
Congenital external disease
Drugs and alcohol induced illness
Sterilization and Fertility issues
Vaccination, War and Nuclear invasions
Some other National Health Insurance Schemes devised are:
Employees State Insurance Scheme (ESIS)
Central Government Health Scheme (CGHS)
Aam Aadmi Bima Yojana (AABY)
Janashree Bima Yojana (JBY)
Universal Health Insurance Scheme (UHIS)
2. Regulation of health and Medical Standards –
a. Regulation of medical practice – STG (Standard Treatment Guidelines), Evidence based
management and different legislations like PCPNDT Act have been stringently enforced.
b. Drug Regulation – Essential Medicine List with pharmaco-vigilance and use of generic
names started.
c. Food Regulation – Policies newly redesigned, food surveys and FSSAI (Food Safety and
Standard Authority of India) with bio-safety have become functional.
3. National Level Health care Institutions – Up gradation of existing medical colleges and other health
care facilities, opening of more AIIMS like institutes with creation of Centers of Excellence for various
public health activities are started.

7
4. Health Workforce – NCHRH (National Commission for Human Resource for Health) encompassing
and regulating all bodies dealing with medical education and allied services to be set up. Moreover a tier
of Community Health Officers at field level to be formed along with holding CMEs (Continuing medical
education).
5. Information Technology in Health – Improved connectivity at all tiers of health care delivery
services for prompt reporting and dissemination of health related information, surveillance, repositioning
of teaching modules, telemedicine, program monitoring and maintaining registries envisaged.
6. National Health Mission – Converging urban and rural areas with special focus on urban poor the
‘Core Principles’ are:
a. Universal Coverage
b. Continuum of care
c. Achieving quality standards
d. Decentralized Planning
The priority services enlisted are: MCH, universal immunisation services, family welfare, control of
communicable and non communicable diseases, and access to medicines in all public health care
facilities. BCC and focus on public health efforts to improve governance with establishment of RKS
(Rogi Kalyan Samiti), and improving human resources, along with strengthening health system with
community participation are targeted for effective service utilisation.
Another important area is NUHM (National Urban Health Mission) in addition to NRHM
(National Rural Health Mission). The Union Cabinet gave its approval to launch a National Urban
Health Mission (NUHM) as a new sub-mission under the over-arching National Health Mission
(NHM). Under the Scheme the following proposals have been approved:
One Urban Primary Health Centre (U-PHC) for every fifty to sixty thousand population
One Urban Community Health Centre (U-CHC) for five to six U-PHCs in big cities.
One Auxiliary Nursing Midwives (ANM) for 10,000 population.
One Accredited Social Health Activist ASHA (community link worker) for 200 to 500
households.

8
The estimated cost of NUHM for 5 years period is Rs 22,507 crore with the Central
Government share of Rs 16,955 crore. This Mission will be implemented in 779 cities and towns
with more than 50,000 population and cover about 7.75 crore people.
The interventions under the sub-mission will result in
Reduction in Infant Mortality Rate (IMR)
Reduction in Maternal Mortality Ratio (MMR)
Universal access to reproductive health care
Convergence of all health related interventions.
The existing institutional mechanism and management systems created and functioning under
NRHM will be strengthened to meet the needs of NUHM. City-wise implementation plans will
be prepared based on baseline survey and felt need. Urban local bodies will be fully involved in
implementation of the scheme. NUHM aims to improve the health status of the urban population
in general, particularly the poor and other disadvantaged sections by facilitating equitable access
to quality health care, through a revamped primary public health care system, targeted outreach
services and involvement of the community and urban local bodies.
7. National AIDS Control Organisation: Integration of services at all levels with intensified
interventions for bridge population and hi-risk populations to accelerate reversal and strengthen epidemic
response are the main prongs.
8. Health research and Convergence across all sectors: mainstreaming AYUSH doctors, and
prioritising women empowerment by awareness generation and legislative measures are the cross cutting
areas.
9. Nutrition Promotion: Fed state is a healthy state. Thus many efforts to combat malnutrition and
provide balanced diet to all have been started like promoting IYCF (Infant, Young and Child Feeding
Practices), ICDS strengthening and restructuring, multi-sectoral programs to combat micronutrient
deficiencies, skilled nutrition counseling and promoting breastfeeding, 200 high burden districts special
efforts and nutrition monitoring and surveillance.
10. Drinking water and sanitation: NRDWP (National Rural Drinking water program) revised with aim
to provide at least 55lpcd of safe piped drinking water supply along with increasing coverage in rural

9
areas with building of community toilets, solid and liquid waste management and surface water
management with emphasis on water quality issues.
11. Total Sanitation Campaign – Renamed as Nirmal Bharat Abhiyan at GP level, 50%villages are
targeted to achieve the status. Child friendly toilets with recent technological inputs have been devised for
sustainable outcomes. Urban water and waste management techniques need to be improvised further.
Reviving local water bodies with groundwater recharging, water conservation strategies like recycle and
reuse strengthened.
Thus, maintaining standards and quality control, addressing national level priorities with an eye
on ethical issues will lead to successful implementation of 12th
five year plan, resulting in desired health
indicators for the nation and paving its way for progress.
Areas for health system strengthening in states2 –
1. Effective public health administration
2. Health financing
3. Health Regulation
4. Develop human resources for health
5. Health Information Systems
6. Convergence and Stewardships
7. Health services
8. NITI Aayog (National Institution for Transforming India) created on 01/01/2015 serves
as a Think Tank of the Government, replacing the Planning Commission, which aims to
involve the states in economic policy making.
Summary
The 12th
Five Year Plan (2012-2017) was formulated encompassing monitorable and achievable outcome
indicators for faster sustainable and inclusive growth. UHC Model (Universal Health Coverage) through
Essential Health Package and providing preventive services and the National Health Mission specially
designed for urban poor are the major prongs of the plan.
Some major thrust areas are reducing OOP (Out of pocket expenditure), ensuring accessibility of
vaccines, medicines and technology, meeting the staff shortage, recruiting AYUSH Doctors, multi-
sectoral convergence and coordination, women empowerment, disaster management areas, nutrition
promotion, TSC (Total Sanitation Campaign) and providing drinking water facilities. Health financing

10
through different models with state incentivisation is a major breakthrough designed to accomplish the
plan, along with support for AIDS control and regulation of food and drugs.
Thus ensuring effective utilization of services and adequate implementation of plans at all the three tiers
of the health care delivery system, the desirable health indicators are perceived to be achieved.
References
1. Park K. Park’s Textbook of Preventive and Social Medicine. 23th
ed. Prem nagar, Jabalpur: M/s
Banarsidas Bhanot Publishers; 2015.p.876-878.
2. Taneja D.K. Health Policies and Programmes in India.12th
ed. Banerjee B (Ed). New Delhi, Doctors Publications; 2015.pp 47-70.
3. Planning Commission. Health in Twelfth Five Year Plan (2012 – 2017),Vol III ,New Delhi, SAGE Publications India Pvt. Ltd, 1-46.

11
Quadrant III. Assessment and Evaluation
MCQs
Q.1 The core principles of NHM are all except:
a. Universal Coverage
b. Essential Health Package
c. Achieving quality standards
d. Decentralized Planning
Q.2 Under NUHM which one is not proposed:
a. One Urban Primary Health Centre (U-PHC) for every 50,000-60,000 population
b. One Urban Community Health Centre (U-CHC) for 5-6 U-PHCs in big cities.
c. One Auxiliary Nursing Midwives (ANM) for 5,000 population.
d. One ASHA (community link worker) for 200 to 500 households.
Q.3 True or False?
a) 12th
Five Year plan aims to reduce under- nutrition to one third of previous
level and MMR to 75.
b) RSBY covers insurance of Rs.30,000 and does not include congenital conditions.
Q.4 Give answers in short
a) Enlist the outcome indicators for 12th
Five Year Plan for communicable diseases.
b) Enumerate the beneficiaries of the National Urban Health Mission.
c)What are conditions not enlisted under the RSBY scheme?

12
Key to assessment
1. b. Essential Health Package
2. c. One Auxiliary Nursing Midwives (ANM) for 5,000 population.
3. a) False
b) True
4. a) 12th Five Year Plan mainly focuses on reducing IMR, MMR, Anemia and Under nutrition and has
specified targets for communicable diseases like TB, Malaria, Kala-azar, Filaria.
b) NUHM is specially designed for urban poor and vulnerable population as well as migrants.
c) RSBY does not include congenital conditions, infertility issues, immunization related conditions
primarily.

13
Quadrant IV. Did you know?
12th
Five year Plan was formulated for year (2012-2017) with a set of achievable and
monitorable goals.
RSBY – came to rescue of the distressed citizens with a package of services, an attempt
first of its kind in India.
HLEG - came up with a set of recommendations for attainment of outcome.
NUHM proposed a health care delivery structure similar to those in villages, for the
urban poor and vulnerable with ASHA as the main service providers.
Interesting facts:
World UHC Day is on 12th
December
Few core areas identified under the 12th
Five Year Plan in various domains that need to be
focused and strengthened apart from the HLEG recommendations
Core Principles of NUHM are:
Universal Coverage
Continuum of care
Achieving quality standards
Decentralized Planning
NITI Aayog is the latest addition in the list.
Glossary
DHKI: District Knowledge Health Institute
EHP: Essential Health Package
HLEG : High Level Expert Group
NHM: National Health Mission
NITI: National Institution for Transforming India
NRHM: National Rural Health Mission
NUHM: National Urban Health Mission
RSBY: Rashtriya Swasthya Bima Yojana
UHC: Universal Health Coverage

14
Study materials
Text books on National Health Programs and Policies
Textbook of Preventive Medicine
12th
Five Year plan document by Planning Commission, Government of India.
Points to ponder
Evolution of Five year plans
Goals of 12th
Five Year Plan
HLEG Recommendations for achieving UHC
Other core areas of the 12th
Five year Plan
RSBY – the prepackaged services at designated service points for beneficiaries