nhs fife woundcare guidelines · anne wilson vascular nurse and senior prescribing support nurse...
TRANSCRIPT

Approved: December 2016 For review: February 2020 Approved by NHS Fife ADTC 2016
Wound Formularyand Wound Management Guidelines
2017
Developed by the NHS Fife Wound and Skin Care Forum (WSCF) Group
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 1 27/01/2017 10:09

Area Drug and Therapeutics Committee
1
Contents Introduc on 2 Wound Defini on 4 Cavity Wounds, Packing and Probing 4 Necro c Wounds & Comprehensive wound assessment 5 Factors to consider when planning holi wound care 7 Characteris of ideal dressings & Ordering products 8 Guide to selec on of wound dressings 9 Overgranula on 10 STAR – Skin Tear Classifica on System 11 Bacterial burden and management of infec on 12 Wound cleansing guidelines 14
MONOGRAPHS FOR DRESSINGS o Barrier film 17 o Non adherent dressings 17 o Hydrocolloid dressings 18 o Foam dressings 19 o Hydrofibre dressings 20 o Hydrogel dressings 21 o Alginate dressings 22 o Deodorising dressings 23 o Silicone dressings 24 o Silicone Foam 25 o Super Absorbent Dressings 26
SPECIALISED DRESSINGS Guidance for use of Specialised dressings and therapies 27 Ropper Ladder 28
o Silver containing Dressings 29 o Prontosan Preparation 29 o Cutimed Range 30 o Honey Preparations 30 o Iodine containing Dressings 32 o Antimicrobial Alginate Gel 32 o Pain Management Dressings 33 o Foam/Fibre Dressings - Heavily Exuding Wounds 33 o Debridement product 33 o Tulle Dressings 34 o Technology Lipidocolloid (TLC) 34 o Specialist Plastic Surgery 35 o Larvae Therapy 37 o Negative Pressure Wound Therapy 37 o Wound Drainage Bags 38
Glossary of Wound Terms 39 Reading list / Resources 40 Related Policies 42 Appendix 1 – Wound Assessment Charts 43 Appendix 2 – Wound Conversion Charts 46
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 2 27/01/2017 10:09

Area Drug and Therapeutics Committee
2
Introduction
Wound care consumes a significant amount of resources in terms of wound management products and professional time. The range of wound care products currently available can be bewildering and choosing the most appropriate dressing difficult. There is no such thing as the perfect dressing, so the choice is usually a compromise, trying to achieve the optimum environment to encourage the best outcomes in the shortest time. The dressing selected will invariably change as the wound healing proceeds, adding to the number of decisions necessary. The introduction of non-medical prescribing has increased both responsibility and accountability in wound management. Prescribers must therefore ensure that the choice of dressing is based on a full and accurate assessment of all the factors which may influence healing, and not just the wound itself. These guidelines aim to assist practitioners in the assessment and management of wounds. They encourage rational, Price-effective prescribing of dressings and other materials used in wound care. Demonstrating the use of evidence based treatments, and allowing practitioners to disseminate and share best practice, will promote seamless care across all sectors. On most of the pages containing information on dressings, a 1st and 2nd choice is given. Where possible, the 1st choice dressing should be used, however there may be reasons that this is not appropriate, therefore the 2nd choice dressing may be used. Staff must be able to give a rationale for choosing a dressing out with the main pages of the guidelines and this should be documented in the patients’ notes. Other dressings, treatment choices are within the specialised dressing pages. Dressing prices (Scottish Drug Tariff, SDT January 2017) have been added to make practitioners aware of Price. More expensive dressings may still be Price effective if used in the correct manner. Practitioners are advised to contact their local Tissue Viability nurse or Podiatrist for further advice, if they have a good rationale for not using the choice of dressing given. These guidelines are based on a selection of up to date research and clinical expertise of group members. We do accept that opinions vary and point out that these guidelines are not intended to be a definitive textbook, therefore a further reading list is included.
Disclaimer
Guideline users should be mindful that, as with any clinical guideline, recommendations may not be appropriate for use in all circumstances. Clearly, a limitation of any guideline is that it simplifies clinical decision making processes and recommendations. Decisions to adopt any particular recommendations must be made by the practitioner in the light of available resources, local services, policies and protocols. The particular patient’s circumstances and wishes including consent for treatment and medical photography, available personnel and equipment, clinical experience of the practitioner and knowledge of most recent research findings must all be considered and decisions clearly documented in the patient’s notes.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 3 27/01/2017 10:09

Area Drug and Therapeutics Committee
3
Acknowledgements
The NHS Fife Wound and Skin Care Forum would like to thank the Glasgow Wound Guidelines Group, for allowing us to use some of their work, particularly in the teaching area of the Fife Guidelines. We would also like to thank Ruth Ropper, Tissue Viability Nurse in Lothian for her permission to use the Ropper Lothian Ladder for wound infection.
We would also acknowledge the contribution of both NHS Fife Community Services and NHS Fife Acute Services Division staff in the development of these Guidelines.
NHS Fife Wound and Skin Care Forum (WSCF) Guideline Group
NAME POSITION
Jane Nicoll Lead Tissue Viability Nurse, ASD (Chairperson)
Anne Barns District Charge Nurse, Path House, Kirkcaldy
Andy Cameron Senior Procurement Officer
Julia Chalmers District Charge Nurse, Balmullo Health Centre
Lynn Coyne Plastic Surgery Specialist Nurse, ASD
Antonia De Angelis Tissue Viability Nurse, ASD and Community
Katrina Deas Clinical Practice Development Officer
Fiona Dick Charge Nurse, Ward 13 VHK
Kevin Finnegan Assistant Procurement Administrator
Fiona Graham Highly Specialist Podiatrist
Tanya Hardy Senior Staff Nurse, Plastic Surgery, ASD
Joanne Koczubik Plastic Surgery Nurse, ASD
Deborah McCallum Clinical Nurse Practitioner, Plastic Surgery, ASD
Heather McKellar Senior Charge Nurse in OPD, Adamson Hospital
Gillian Meldrum Highly Specialist Podiatrist
Gillian Preston Tissue Viability Nurse, ASD
Leesa Radcliffe Community Tissue Viability Nurse, West Fife
Yvonne Robson Senior Charge Nurse, OPD, QMH
Susan Roemmele Staff Nurse, Dermatology Department, QMH
Islay Roy Plastic Surgery Nurse, ASD
Lesley Shiels Tissue Viability Nurse, Community East Fife
Mary Thomson Senior Prescribing Support Nurse
Caroline Turnbull Plastic Surgery Nurse, ASD
Catherine Ward Staff Nurse, Ward 10 VHK
Karen Whatton Senior Prescribing Support Nurse
Anne Wilson Vascular Nurse and Senior Prescribing Support Nurse
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 4 27/01/2017 10:09

Area Drug and Therapeutics Committee
4
Wound Definition
For the purposes of these guidelines, the following definitions apply -
A simple wound is one where there is damage to the epidermal layer of the skin, including discolouration due to pressure damage.
A complex /chronic wound is one which heals by granulating from the base up and requires contraction and scar tissue to close. Debridement of slough and necrotic tissue may be necessary.
It is important to note that the term chronic suggests longevity; however, many wounds e.g. diabetic foot or rheumatoid lesions may be termed chronic at the onset. A more accurate term for a chronic /complex wound would be a compromised wound. It is the underlying host response to the wound, which will determine to a great extent its ability to heal.
Cavity Wounds Providing a single definition for a cavity wound is challenging as they vary in aetiology, size, depth and position. They may present with additional challenging features such as sinus formation, fistulae, undermining or bridging (Wounds UK, Cavity Wounds Quick Guide, 2016) For the purposes of these guidelines, the following definitions apply –
A wound extending beneath the layers of the dermis, potentially exposing structures such as fascia, tendon, muscle or bone.
A wound requiring more than a simple flat dressing – wounds that require a ‘filler’ dressing.
A wound deeper than 2cm.
Packing and Probing wounds
Guidance has been requested on how best to pack a wound and how to probe a wound to measure wound depth. A literature search was conducted; unfortunately there is no evidence to support robust guidance. However the consensus of the Fife Wound and Skin Care Forum Group is as follows:
Clinicians must use their clinical judgement when deciding to pack or probe a wound.
To gauge depth use a soft cotton tipped swab to gently probe, taking care not to damage tissue or structures.
Podiatrists, please seek local advice regarding probe type.
To pack a wound with a hydrogel or alginate gel, half fill the cavity and apply secondary dressing.
To pack a wound with dressing material, the end of the wound must be established to avoid dressing material being lost within the wound, it may be more appropriate to use a gel.
Pack dressing material loosely
Clearly document how many pieces of dressing material have been inserted and removed from the wound.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 5 27/01/2017 10:09

Area Drug and Therapeutics Committee
5
Necrotic tissue
Necrotic tissue is a layer of dead tissue which can be brown/ black and or waxy in colour and is caused by an inadequate blood supply or infection. It may be soft or hard on the surface. The skin can remain intact and the necrosis can be of varying depth and it may produce an offensive smell.
Nursing staff must be cautious before attempting to remove necrotic tissue from a wound; this includes autolytic debridement with the use of hydrogels and dressing products. A full, holistic assessment of the patient must be undertaken first to ascertain any intrinsic or extrinsic factors which may cause complications if removal of necrotic tissue is initiated or necessary.
Necrosis should not be routinely removed in an ischemic area. This may cause significant
deterioration in the area.
Necrosis should not be routinely removed and at the end of life in the absence of any systemic
or local signs of infection unless required for symptomatic relief.
For example: debridement may be necessary e.g. wound is beginning to break down, a
collection of fluid is evident below the necrosis and when malodour or infection is an issue, this
must be discussed with the relevant clinicians before you attempt any form of necrotic tissue
removal.
Specialist advice should be sought when considering sharp debridement of a wound.
Mechanical or surgical removal such as sharps debridement of tissue should only be performed
by specialist practitioners.
Further information:
Guidelines For Practice, Effective Debridement in a Changing NHS – a UK Consensus, Wounds UK 2013. Available form: www.wounds-uk.com
Healthcare Improvement Scotland (2010) Tissue Viability Scottish Wound Assessment and Action Guide...\20100728_Wound_Assessment_Tool_Guide_Final SWAG.pdf
Comprehensive Wound Assessment
Recognised good practice is to assess a wound using a validated wound assessment chart (see page )
Compromised wound healing is usually a result of the patients underlying disease processes, ability to initiate an inflammatory response and fight infection. Intrinsic factors must therefore be taken into account whilst planning wound care.
Extrinsic factors at the wound bed (slough, necrotic tissue, biochemical and bacterial burden or damage to underlying structures, e.g tendon) may inhibit the healing process and wound bed preparation must be carried out to promote proliferation and epithelialisation. (See web site below).
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 6 27/01/2017 10:09

Area Drug and Therapeutics Committee
6
The condition of the surrounding skin must be considered when recognising if there are signs of infection, tracking or undermining of the wound. Consideration must be made as to whether adhesive or non-adhesive dressings should be used dependent on the vulnerability of the surrounding skin.
Address patient issues to establish if the patient/carer can be empowered to assist in their own wound care. It is important to determine if they have the ability to cope psychologically with the presence of a wound. It is important to recognise the need for adequate pain control / analgesia and this must be reviewed regularly.
It is not always possible to heal wounds due to the patients underlying aetiology (e.g. in fungating tumours or advanced disease). In this instance palliative care may be the aim, with management of symptoms in a way that is acceptable to the patient.
There should be an awareness in the non-healing compromised wound that further referral to the appropriate specialty may be required, e.g. vascular, dermatology, podiatry, plastic surgery or tissue viability.
Assessment tools have been developed by the National Association of Tissue Viability Nurses (Scotland) and the Scottish Wound Assessment and Action Guide can be accessed on-line:
..\20100728_Wound_Assessment_Tool_Guide_Final SWAG.pdf
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 7 27/01/2017 10:09

Are
a D
rug
and
Th
erap
euti
cs C
om
mit
tee
7
Fact
ors
to
Co
nsi
der
wh
en
Pla
nn
ing
Ho
listi
c W
ou
nd
Car
e
Pat
ien
t Is
sue
s (R
ela
tin
gto
wo
un
dan
dp
ers
on
al)
Pai
nO
do
ur
Exu
dat
eA
nxi
ety
Low
Sel
fEs
tee
mP
oo
rM
ob
ility
Soci
al Is
ola
tio
nLo
ss o
f e
mp
loym
en
t/in
com
eFe
elin
gvu
lne
rab
leN
eed
tob
ein
clu
de
dw
ith
the
irm
anag
em
en
t
Intr
insi
c fa
cto
rs t
hat
de
lay
he
alin
g
Co
mp
rom
ise
db
loo
dfl
ow
Oe
de
ma
Dia
bet
esP
oo
rn
utr
itio
nC
on
nec
tive
tiss
ue
dis
ord
ers
Smo
kin
g
Mal
ign
ancy
Alc
oh
ol m
isu
seD
rug
tre
atm
en
t /r
adio
the
rap
ySy
ste
mic
infe
ctio
n
Surr
ou
nd
ing
Skin
Re
dn
ess
Mac
era
tio
nD
ry /
Flak
yO
edem
ato
us
No
du
lar
Frag
ileU
nd
erm
inin
gTr
acki
ng
Co
nd
itio
no
fm
argi
ns
Sup
ple
ne
ss
Wo
un
dB
ed
He
alth
ygr
anu
lati
on
Exp
ose
dte
nd
on
or
bo
ne
Epit
hel
ialis
atio
nB
acte
rial
Bu
rden
Wet
/D
ry S
lou
ghB
ioch
emic
al im
bal
ance
Typ
e &
Co
lou
r o
f e
xud
ate
Dep
th,p
rese
nce
of
sin
us
or
fist
ula
e
Ne
cro
sis
Pre
cise
an
ato
mic
alp
osi
tio
n
Nu
trit
ion
alFa
cto
rsw
hic
hm
ayco
mp
rom
ise
wo
un
dh
eal
ing
Inab
ility
to
acce
ss f
oo
dP
oo
re
con
om
icst
atu
sR
ed
uce
d m
ob
ility
Inab
ility
to
com
mu
nic
ate
pre
fere
nce
Soci
ally
iso
late
d
Po
or
app
eti
teU
nd
erl
yin
gd
ise
ase
p
roce
ssM
ed
icat
ion
De
pre
ssio
n
Dif
ficu
lty
insw
allo
win
gSt
roke
Ne
uro
mu
scu
lar
dis
ord
ers
Un
de
rlyi
ng
mal
ign
ancy
Inab
ility
to
abso
rbad
eq
uat
e
nu
trie
nts
Gas
tro
-in
test
inal
dis
ord
ers
Mal
abso
rpti
on
syn
dro
me
Par
alyt
ic il
eu
sV
om
itin
gan
dd
iarr
ho
ea
Smal
lor
larg
eb
ow
elr
ese
ctio
n
Incr
eas
e m
eta
bo
lic d
em
and
Tra
um
aSe
psi
sR
ece
nt
surg
ery
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 8 27/01/2017 10:09

Area Drug and Therapeutics Committee
8
Characteristics of Ideal Dressings
1. Provide the optimum environment for wound healing - a moist environment - at the wound/dressing interface.
2. Allow gaseous exchange of oxygen, carbon dioxide and water vapour.
3. Provide thermal insulation - wound healing is temperature dependent.
4. Impermeable to micro-organisms (in both directions).
5. Free from particulate contaminants.
6. Non-adherent (many products are described as non-adherent but are low adherent).
7. Safe to use (non-toxic, non-sensitising, non-allergenic).
8. Acceptable to the patient.
9. High absorption characteristics (for exuding wounds).
10. Price effective.
11. Carrier for medicaments, e.g. antiseptics.
12. Capable of standardisation and evaluation.
13. Provide mechanical protection.
14. Conformable and mouldable (especially over sacrum, heels and elbows).
It is generally recognised that modern wound dressings are capable of being left on the wound bed for up to seven days, however this is dependent on exudate levels and whether there is infection present within the wound, therefore check with the instructions given within the box of dressings for further information.
Ordering Dressings
The most Price effective ordering route for both hospital and community is via the Area Distribution Centre/National Distribution Centre (ADC/NDC).
All dressings listed on the general pages of the Wound Management Guidelines are available on Drug Tariff.To order an item that is not on formulary, an Exception form must be completed and submitted to the Senior Prescribing Support Nurses ([email protected])
http://www.fifeadtc.scot.nhs.uk/formulary/woundcare-formulary/woundcare-catheter-product-request-and-exception-form.aspx
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 9 27/01/2017 10:09

EXU
DAT
E LE
VELS
EXU
DAT
E LE
VELS
EXU
DAT
E LE
VELS
EXU
DAT
E LE
VELS
EXU
DAT
E LE
VELS
LOW
LOW
LOW
LOW
LOW
MED
- H
IGH
MED
- H
IGH
MED
- H
IGH
MED
- H
IGH
MED
- H
IGH
FOR
MU
LARY
DR
ESSI
NG
SFO
RM
ULA
RY D
RES
SIN
GS
FOR
MU
LARY
DR
ESSI
NG
SFO
RM
ULA
RY D
RES
SIN
GS
FOR
MU
LARY
DR
ESSI
NG
S
Epith
elia
lisin
gIn
fect
edN
ecro
ticSl
ough
yG
ranu
latin
g
NH
S
1st C
HO
ICE
2nd
CH
OIC
E
1st C
HO
ICE
1st C
HO
ICE
1st C
HO
ICE
2nd
CH
OIC
E
IS T
HE
WO
UN
D?
AS
SE
SS
TH
E W
OU
ND
OB
JEC
TIV
ES
: To
prot
ect a
ndpr
omot
e ne
w ti
ssue
gro
wth
. O
BJE
CT
IVE
S: T
o re
duce
bac
teria
llo
ad in
wou
nds.
NB
: If s
prea
ding
infe
ctio
n (e
.g. c
ellu
litis
), sy
stem
ican
tibio
tics
will
be
requ
ired.
OB
JEC
TIV
ES
: To
rehy
drat
e es
char
.N
B: D
epen
ding
on
over
all a
ims,
it m
ayno
t be
appr
opria
te to
bre
ak n
ecro
sis
dow
n, e
.g. p
allia
tive
or v
ascu
lar w
ound
s.
OB
JEC
TIV
ES
: To
debr
ide
slou
gh,
man
age
exud
ate
leve
ls.
OB
JEC
TIV
ES
: Enc
oura
gean
giog
enes
is a
nd p
rom
ote
gran
ulat
ion
tissu
e.
Non
-adh
eren
tdr
essi
ng
OR
Thin
Hyd
ro-
collo
id
Hyd
roge
l
Non
-adh
eren
tw
ith p
ad o
rfo
am
Non
-adh
eren
tdr
essi
ng
OR
Foam
dre
ssin
g
Non
-adh
eren
tdr
essi
ng w
ithab
sorb
ent p
ad
OR
Foam
adh
esiv
e/N
on a
dhes
ive
Non
-adh
eren
tdr
essi
ng w
ithab
sorb
ent p
ad
OR
Foam
dre
ssin
g
Hyd
rofib
redr
essi
ng &
abso
rben
t pad
OR
Foam
dre
ssin
g
Hyd
roge
l and
non-
adhe
rent
dres
sing
with
pad
OR
Hyd
roco
lloid
Foam
dre
ssin
gC
onsi
der.
hydr
ogel
ifne
cros
is s
till
need
s br
oken
dow
n.
Ant
imic
robi
alim
preg
nate
d dr
essi
ng &
non
adhe
rent
dres
sing
.
Ant
imic
robi
alor
silv
erim
preg
nate
ddr
essi
ngpl
usab
sorb
ent
seco
ndar
ydr
essi
ng
Aqu
acel
Foa
m*
Ref
er to
Infe
cted
Wou
ndse
ctio
n of
Wou
nd G
uide
lines
(Rop
per L
adde
r)
1st C
HO
ICE
2nd
CH
OIC
E
1st C
HO
ICE
2nd
CH
OIC
E
1st C
HO
ICE
1st C
HO
ICE
1st C
HO
ICE
365
Isla
nddr
essi
ng
Mep
ilex
Lite
Adhe
sive
/N
on A
dhes
ive
Tega
derm
Foa
m/
Tega
derm
Foa
mad
hesi
ve
Pur
ilon
gel &
Mep
ilex
Lite
Pur
ilon
gel &
Tega
derm
Foa
m
Inad
ine
&no
n ad
here
nt p
ad
1st C
HO
ICE
2nd
CH
OIC
E
Klin
ider
m
Tega
derm
Foa
m/
Tega
derm
Foa
mad
hesi
ve
Tega
derm
Foa
m/
Tega
derm
Foa
mad
hesi
ve
Pur
ilon
gel &
Tega
derm
Foa
m/
Tega
derm
Foa
mad
hesi
ve
Tega
derm
Foa
m/
Tega
derm
Foa
mad
hesi
ve (i
fin
fect
ion
susp
ecte
d, re
fer t
oIn
fect
ed W
ound
sect
ion)
.
2nd
CH
OIC
E2n
d C
HO
ICE
2nd
CH
OIC
E
Com
feel
Plu
sU
lcer
*Aqu
acel
Foa
mad
hesi
ve/
non
adhe
sive
2nd
CH
OIC
E
Aqu
acel
Ext
ra &
Klin
ider
m
2nd
CH
OIC
EA
ctili
te a
ndno
n ad
here
ntpa
d
Urg
otul
SS
D&
Klin
ider
m
Part
ners
hip
Fife
Hea
lth
& S
ocia
l Car
e
Supp
ortin
g th
e pe
ople
of F
ife to
geth
er
REM
EMBE
R: A
full
holis
tic
asse
ssm
ent o
f the
pat
ient
mus
t be
carr
ied
out.
NA
Ultr
a pl
us36
5 Is
land
dres
sing
Aqu
acel
Ext
rapl
us K
linid
erm
Dev
elop
ed b
y N
HS
Fife
Wou
nd &
Ski
ncar
e Fo
rum
(WSC
F) J
anua
ry 2
017.
Rev
iew
Dat
e Ja
nuar
y 20
20Fo
r fur
ther
info
rmat
ion
on d
ress
ings
, ref
er to
Wou
nd F
orm
ular
y.

Area Drug and Therapeutics Committee
10
Overgranulation
An essential aspect of secondary intention wound healing is the proliferation of granulation tissue, (McGrath, 2011). Granulation incorporates a dense network of blood vessels and newly growing capillaries with an irregular upper layer created by the capillaries looping together on the wound surface. This is what gives the appearance of red lumps or granules on the wound surface. When granulation ‘over grows’ beyond the surface of the wound, this is known as overgranulation, or hypergranulation. It is clinically recognised by a soft, fleshy, friable, often shiny appearance which is raised above the level of the surrounding skin. The wound will not continue to heal as the presence of this tissue will prevent the migration of epithelial tissue across the wound bed.
The exact cause of overgranulation is unknown, (Russell 2000). It is thought to be the consequence of a reaction to foreign bodies, infection/bio burden, mechanical trauma or allergies and hypersensitivities.
The research to date to support treatment options for overgranulation is limited, (McGrath, 2011). Reported treatments attempt to treat the causative factor, and focus on reducing bacteria present, applying pressure, using non occlusive dressings and the use of steroid therapies.
It is essential that the clinician can identify the causative factor of the overgranulation, in order to make informed clinical decisions on an effective treatment. A number of treatment options exist, and for this reason, the advice of an appropriate specialist should be sought, e.g. local Tissue Viability Nurse or Plastics Nurse.
ReferencesMcGrath A (2011) Overcoming the challenge of overgranulation. Wounds UK 7(1): 42-49Russell L (2000) Understanding physiology of wound healing and how dressings help. British Journal of Nursing 9(1): 10-21Stephen – Haynes J. Wound Care Alliance UK: Achieving effective outcomes in patients with overgranulation
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 11 27/01/2017 10:09

Are
a D
rug
and
Th
erap
euti
cs C
om
mit
tee
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 12 27/01/2017 10:09

Area Drug and Therapeutics Committee
12
Bacterial Burden and Management of Infection
Bacterial burden and virulence are important factors in assessing the wound for infection. Host resistance is a major determinant in the body’s ability to fight infection and initiate an inflammatory response.This may be illustrated in the following equation:
Infection = dose x virulencehost resistance
Bacterial Burden Continuum
Bacterial Load Definition Wound Dressing
Contaminated Presence of non replicating bacteria in the wound
Topical antimicrobial and antibiotics not recommended.
Colonised Replicating bacteria adhering to the wound, with no detrimental effect to woundhealing
As above.
Critically colonised Presence of bacteria at the wound bed, whichcompromises healing but does not result in infection
Topical antimicrobial dressings can be used.In general, a two week treatment is advised. Ifno improvement in wound after this time, seek advice from local wound care specialist
Infection Invasion and multiplication ofmicro-organisms in bodytissues with overt hostresponse
If there is clinical evidence of invasiveinfection systemic antibiotics are required.Prescribe systemic antibiotic therapy inconjunction with appropriate dressing.
Wound Swabs for Microbiology
Wound infection is recognised by the presence of clinical signs of infection rather than the isolation of bacteria from a wound swab. A wound swab should only be taken when there is concern regardinginfection. They should not be taken as part of “routine practice”. Taking a wound swab will give aqualitative picture of bacteria present on the wound surface. These are most commonly colonisingbacteria and not responsible for infection. (Refer to The Adapted Ropper Lothian Ladder). N.B. Do notconfuse signs of inflammation with infection
For diabetic foot wounds consult local podiatrist for advice at an early stage as signs of infection may bemasked.
Organisms most commonly associated with soft tissue infections are S.aureus, and Group A, B, C, and GStreptococcus. The clinical presentation should be reviewed alongside the swab result to ensure themost appropriate treatment is prescribed.
Swabbing for culture and sensitivity is only recommended before antibiotics are commenced or toconfirm that the antibiotics commenced are appropriate. If a patient fails to respond to antibioticswithin 72hours, then consider re-swabbing or seek further Medical advice
The Price incurred for each Wound Swab is in excess of £35.88.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 13 27/01/2017 10:09

Area Drug and Therapeutics Committee
13
The wound bed must be cleansed prior to swabbing so as to avoid sampling slough or necrotic tissue that may only reveal surface organisms which are not causing underlying infection. Critically colonised or infected wounds can be treated with antimicrobial dressings but when significant infection is present systemic antibiotics should be commenced.
Procedure for taking a Wound Swab
Irrigate the wound with Sodium Chloride 0.9% solution.
Swab the edge of the wound adjacent to the good tissue which is inflamed. It is the organism infecting the good tissue which will be the major pathogen. This would normally tend to be nearer the edge of the wound as the tissue in the centre is more often necrotic.
The swab should be rotated between the fingers to ensure that all sides of the swab make contact with the wound.
Infected wound below, swab area as directed by arrows
Example of mostsuitable areas to swab
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 14 27/01/2017 10:09

Area Drug and Therapeutics Committee
14
Wound Cleansing Guidelines
To Clean or Not To Clean?
There is no single correct way to clean a wound or the surrounding skin, although there are a number of important considerations
Does the wound really need cleansing?
What is the safest method that causes no ill effect and maintains the wound temperature?
What is acceptable to the patient?
Simple wound cleansing procedure (e.g. suture lines, superficial breaks)
Gentle skin washing with warm tap water (e.g. showering).
A minimalist approach is recommended to reduce interference at the wound bed.
Dry surrounding skin with non woven gauze to allow adherence of wound dressing.
Compromised / complex wound cleansing procedure
Aims:
Remove excess exudate, debris or old dressing materials.
Minimize pain and trauma.
Prevent infection.
Procedure
1 Explain procedure and rationale to patient.
2 Wash hands thoroughly as per hand hygiene policy prior to and following procedure.
3 Dressing packs are not always necessary.
4 Requirements: non woven swabs, clean surface, non-sterile gloves.
5 Remove dressing as per manufacturer’s instructions.
6 Assess wound type and carry out appropriate irrigation procedure (see pages 11 and 12).
7 Dry surrounding area with non woven swabs.
8 Do not touch surface of wound with swabs.
9 Apply new dressing.
Further guidance available, wound cleansing flowchart: www.tissueviabilityscotland.org
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 15 27/01/2017 10:09

Are
a D
rug
and
Th
erap
euti
cs C
om
mit
tee
15
Wo
un
d C
lean
sin
g G
uid
elin
es
Pre
par
atio
nP
roce
du
reR
atio
nal
e
Wit
hta
pw
ate
r
Ge
ntl
esh
ow
eri
ng
of
wo
un
dar
ea
du
rin
gro
uti
ne
soci
alh
ygie
ne
Ru
nsh
ow
er f
or
thre
e m
inu
tes.
En
sure
sfr
ee
flo
win
gw
arm
cle
anw
ate
r.
Gen
tly
irri
gate
wo
un
dw
ith
war
mw
ater
usi
ng
sho
wer
hea
d.
Ensu
res
safe
rem
ova
lof
exu
dat
e, l
oo
sesl
ou
ghan
dw
ou
nd
dre
ssin
gre
sid
ue
.
Inh
ealt
hca
re p
rem
ises
, sh
ow
er s
ho
uld
be
clea
ned
wit
hge
ner
alp
urp
ose
neu
tral
det
erge
nt/
crea
m c
lean
ser
bef
ore
an
daf
ter
use
.M
ain
tain
s cl
ean
wo
rkin
ge
nvi
ron
me
nt.
Inth
e h
om
eca
rese
ttin
g p
atie
nts
ow
nh
ou
seh
old
clea
ner
sho
uld
be
use
dto
clea
nth
e sh
ow
eran
d/o
rb
ath
bef
ore
and
afte
rth
ep
roce
du
re.
Ref
erto
Infe
ctio
nC
on
tro
l Man
ual
.
Bu
cke
t lin
ed
wit
hp
oly
the
ne
bag
for
low
er
limb
sG
entl
yw
ash
limb
. D
rysk
insu
rro
un
din
g w
ou
nd
pri
or
to
app
licat
ion
of
new
dre
ssin
g. A
void
dir
ect
con
tact
wit
hw
ou
nd
bed
.
Ensu
res
safe
rem
ova
lof
exu
dat
e, l
oo
sesl
ou
ghan
dw
ou
nd
dre
ssin
gre
sid
ue
.It
inco
rpo
rate
s so
cial
hyg
ien
ein
tow
ou
nd
man
age
me
nt
pro
ced
ure
.
Inh
eal
thca
rep
rem
ise
s, b
uck
et
sho
uld
be
cle
aned
wit
hge
ne
ral
pu
rpo
sen
eu
tral
de
terg
en
t an
dw
arm
wat
er,
rin
sed
and
dri
ed
.B
uck
ets
sho
uld
be
sto
red
dry
and
inve
rte
d.
Pat
ien
tso
wn
ho
use
ho
ldcl
ean
er
sho
uld
be
use
d in
ho
me
care
sett
ing.
Re
fer
toIn
fect
ion
Co
ntr
olM
anu
al.
Mai
nta
ins
cle
anw
ork
ing
en
viro
nm
en
t.
Infe
ctio
nC
on
tro
l Man
ual
can
be
acce
ssed
via:
Intr
anet
/Su
bje
cts
/In
fect
ion
Co
ntr
ol /
Infe
ctio
nC
on
tro
lMan
ual
htt
p:/
/in
tran
et.f
ife
.sco
t.n
hs.
uk/
sub
ject
s/in
dex
.cfm
?fu
seac
tio
n=s
erv
ice.
dis
pla
y&p
agei
d=7
A5
F5B
B2
-50
56
-8C
6F-
C0
3F5
A9
FA5
92
A3
1A
&su
bje
ctid
=6C
96
5E0
A-D
B7
D-B
17
A-0
4E5
4EA
C6
A4
2E8
39
&o
bje
ctid
=6B
E80
1F1
-50
56
-8C
6F-
C0
E12
BB
07
75
8F4
62
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 16 27/01/2017 10:09
Are
a D
rug
and
Th
erap
euti
cs C
om
mit
tee
16
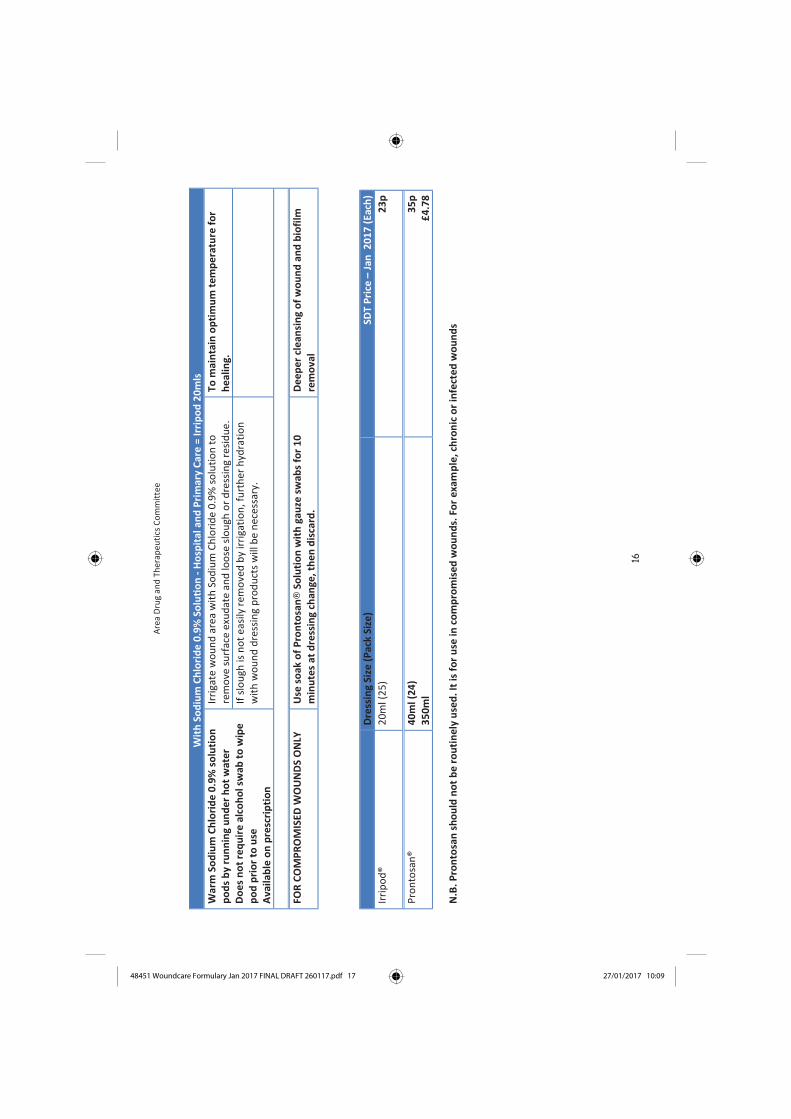
With
Sod
ium
Chl
orid
e 0.
9% S
oluti
on -
Hos
pita
l and
Prim
ary
Care
= Ir
ripod
20m
lsW
arm
Sod
ium
Ch
lori
de
0.9
%so
luti
on
po
ds
by
run
nin
gu
nd
er
ho
tw
ater
Do
es
no
tre
qu
ire
alco
ho
lsw
abto
wip
ep
od
pri
or
tou
seA
vaila
ble
on
pre
scri
pti
on
Irri
gate
wo
un
dar
ea
wit
hSo
diu
m C
hlo
rid
e0
.9%
solu
tio
nto
rem
ove
su
rfac
eex
ud
ate
and
loo
se s
lou
gho
rd
ress
ing
resi
du
e.
To
mai
nta
ino
pti
mu
mte
mp
era
ture
for
he
alin
g.
If s
lou
ghis
no
tea
sily
rem
ove
db
y ir
riga
tio
n,f
urt
her
hyd
rati
on
w
ith
wo
un
dd
ress
ing
pro
du
cts
will
be
nec
essa
ry.
Wit
hP
ron
tosa
n®
40
ml/
35
0m
l
FOR
CO
MP
RO
MIS
EDW
OU
ND
SO
NLY
Use
soak
of
Pro
nto
san®
Solu
tio
nw
ith
gau
ze s
wab
s fo
r1
0m
inu
tes
atd
ress
ing
chan
ge, t
he
nd
isca
rd.
De
ep
er
cle
ansi
ng
of
wo
un
dan
db
iofi
lmre
mo
val
Dre
ssin
gSi
ze(P
ack
Size
)SD
T P
rice
–Ja
n2
01
7(E
ach
)
Irri
po
d®
20
ml(
25
)2
3p
Pro
nto
san
®4
0m
l(2
4)
35
0m
l3
5p
£4
.78
N.B
.P
ron
tosa
nsh
ou
ldn
ot
be
rou
tin
ely
use
d.I
tis
fo
ru
se in
com
pro
mis
ed
wo
un
ds.
For
exa
mp
le, c
hro
nic
or
infe
cte
dw
ou
nd
s
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 17 27/01/2017 10:09
Area Drug and Therapeutics Committee
17
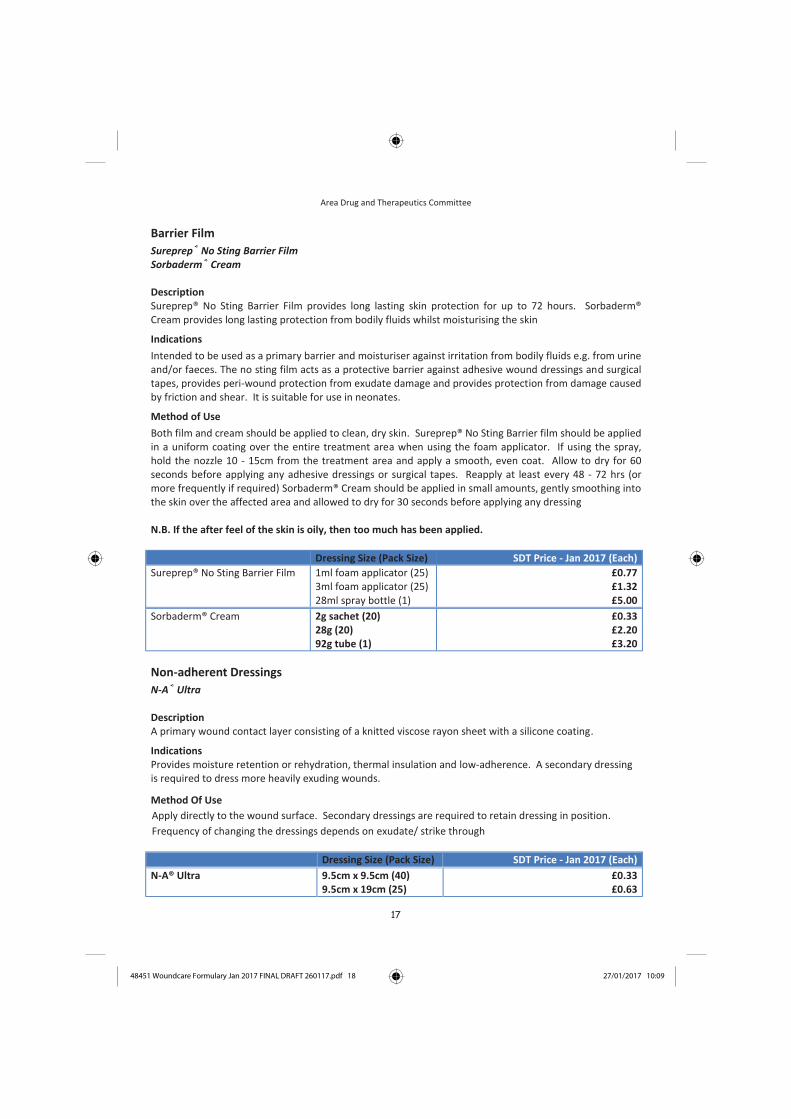
Barrier Film
Sureprep® No Sting Barrier FilmSorbaderm® Cream
DescriptionSureprep® No Sting Barrier Film provides long lasting skin protection for up to 72 hours. Sorbaderm®Cream provides long lasting protection from bodily fluids whilst moisturising the skin
Indications
Intended to be used as a primary barrier and moisturiser against irritation from bodily fluids e.g. from urineand/or faeces. The no sting film acts as a protective barrier against adhesive wound dressings and surgical tapes, provides peri-wound protection from exudate damage and provides protection from damage causedby friction and shear. It is suitable for use in neonates.
Method of Use
Both film and cream should be applied to clean, dry skin. Sureprep® No Sting Barrier film should be appliedin a uniform coating over the entire treatment area when using the foam applicator. If using the spray,hold the nozzle 10 - 15cm from the treatment area and apply a smooth, even coat. Allow to dry for 60seconds before applying any adhesive dressings or surgical tapes. Reapply at least every 48 - 72 hrs (ormore frequently if required) Sorbaderm® Cream should be applied in small amounts, gently smoothing intothe skin over the affected area and allowed to dry for 30 seconds before applying any dressing
N.B. If the after feel of the skin is oily, then too much has been applied.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Sureprep® No Sting Barrier Film 1ml foam applicator (25)3ml foam applicator (25)28ml spray bottle (1)
£0.77£1.32£5.00
Sorbaderm® Cream 2g sachet (20)28g (20)92g tube (1)
£0.33£2.20£3.20
Non-adherent Dressings
N-A® Ultra
Description A primary wound contact layer consisting of a knitted viscose rayon sheet with a silicone coating.
IndicationsProvides moisture retention or rehydration, thermal insulation and low-adherence. A secondary dressing is required to dress more heavily exuding wounds.
Method Of Use
Apply directly to the wound surface. Secondary dressings are required to retain dressing in position.
Frequency of changing the dressings depends on exudate/ strike through
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
N-A® Ultra 9.5cm x 9.5cm (40)9.5cm x 19cm (25)
£0.33£0.63
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 18 27/01/2017 10:09

Area Drug and Therapeutics Committee
18
Hydrocolloid Dressings
Comfeel® Plus Transparent Duoderm® Extra Thin
DescriptionA hydrocolloid dressing is a micro granular suspension of various natural or synthetic polymers, e.g. gelatinor pectin, in an adhesive matrix. The dressings are interactive with wound exudate - by slowly absorbingfluid. They physically change to form a gel, which may be cohesive, and/or hydrophilic.
Comfeel® Plus Ulcer Absorbent hydrocolloid dressing with added alginate for absorption, a vapour-permeable film backing withbevelled edge to reduce rucking. There is a 1cm grid printed on backing to aid wound measurement.
IndicationsAids debridement in wounds covered with black necrotic tissue, suitable for softening eschar andpromoting granulation. Suitable for low to moderately exuding wounds. May also be used prophylactically on areas prone to breakdown and as a secondary dressing.
Method Of UseApply dressing of sufficient size to provide at least 2cm overlap onto intact skin. Smooth dressing intoplace - warmth of the hand improves initial adhesion. For best results aim to leave dressing in place for atleast 3 days. Dressings may be left in place for up to 7 days in low exuding wounds.
N.B. Owing to the occlusive nature of their backing hydrocolloids are not considered suitable for thetreatment of clinically infected or very heavily exuding wounds.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Comfeel® Plus Transparent 5cm x 7cm (10)5cm x 25cm (5)9cm x 14cm (10)
10cm x 10cm (10)15cm x 15cm (10)20cm x 20cm (5)
£0.66£2.53£2.39£1.25£3.27£3.34
Comfeel® Plus Ulcer 10cm x 10cm (10)15cm x 15cm (10)20cm x 20cm (5)
4cm x 6cm (10)18cm x 20cm (5)
£2.46£5.27£7.59£0.96£5.73
Duoderm® Extra Thin 5cm x 10cm (10)7.5cm x 7.5cm (5)
9cm x 15cm (10)9cm x 25cm (10)9cm x 35cm (10)
10cm x 10cm (10)15cm x 15cm (10)
£0.75£0.79£1.74£2.78£3.89£1.30£2.81
First Choice: Comfeel® Plus Transparent/Comfeel® Plus UlcerSecond Choice: Duoderm® Extra thin
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 19 27/01/2017 10:09

Area Drug and Therapeutics Committee
19
Foam Dressings
Tegaderm® Foam / Tegaderm® Foam AdhesiveTegaderm® Foam Adhesive - Heel only
Description Highly absorbent polyurethane foam dressing with semipermeable film backing layer. Foam dressings ingeneral provide thermal insulation, do not shed fibres or particles and can be cut or shaped to fit thewound (non-adhesive). They help to maintain a moist environment at the surface of the wound and are gas permeable and non adherent. Should be used on moderate to highly exuding wounds.
Tegaderm® Foam / Tegaderm® Foam Adhesive Tegaderm Foam is suitable for use in moderate to highly exuding wounds. Tegaderm Foam Adhesive is suitable for low to highly exuding wounds. Can be used on clean granulating wounds or as a secondarydressing in sloughy or necrotic wounds, can be used under compression. Adhesive version is beneficial forpatients wishing to bathe or shower. Dressing should be renewed when exudate has reached within 1cm ofthe edges of the dressing. The dressing may be left in place for 3 - 7 days depending on the level ofexudate.
Tegaderm® Foam Adhesive - Heel onlyA highly absorbent polyurethane foam dressing with semipermeable film backing layer and adhesiveborder. Comprises of four layers for high fluid absorption.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Tegaderm® Foam 8.8cm x 8.8cm (10)10cm x 10cm (10)20cm x 20cm (5)10cm x 20cm (5)10cm x 60cm (Roll)
£2.23£2.19£5.92£3.71
£12.54
Tegaderm® Foam Adhesive 6.9cm x 7.6cm (10)10cm x 11cm (10)
14.3cm x 14.3cm (10)14.3cm x 15.6cm (5)
£1.46£2.39£3.54£4.24
Tegaderm® Foam - Heel 13.9cm x 13.9cm (5) £4.22
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 20 27/01/2017 10:09
Area Drug and Therapeutics Committee
20
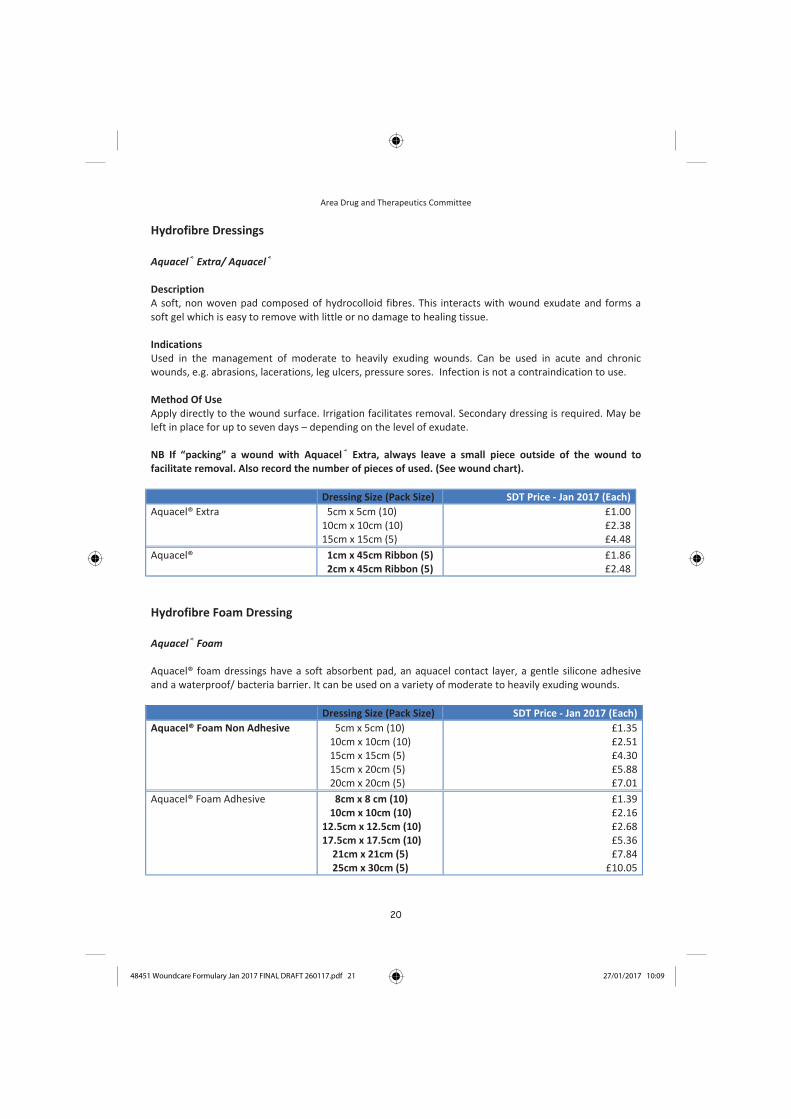
Hydrofibre Dressings
Aquacel® Extra/ Aquacel®
Description A soft, non woven pad composed of hydrocolloid fibres. This interacts with wound exudate and forms asoft gel which is easy to remove with little or no damage to healing tissue.
IndicationsUsed in the management of moderate to heavily exuding wounds. Can be used in acute and chronicwounds, e.g. abrasions, lacerations, leg ulcers, pressure sores. Infection is not a contraindication to use.
Method Of UseApply directly to the wound surface. Irrigation facilitates removal. Secondary dressing is required. May be left in place for up to seven days – depending on the level of exudate.
NB If “packing” a wound with Aquacel® Extra, always leave a small piece outside of the wound tofacilitate removal. Also record the number of pieces of used. (See wound chart).
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Aquacel® Extra 5cm x 5cm (10)10cm x 10cm (10)15cm x 15cm (5)
£1.00£2.38£4.48
Aquacel® 1cm x 45cm Ribbon (5)2cm x 45cm Ribbon (5)
£1.86£2.48
Hydrofibre Foam Dressing
Aquacel® Foam
Aquacel® foam dressings have a soft absorbent pad, an aquacel contact layer, a gentle silicone adhesiveand a waterproof/ bacteria barrier. It can be used on a variety of moderate to heavily exuding wounds.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Aquacel® Foam Non Adhesive 5cm x 5cm (10)10cm x 10cm (10)15cm x 15cm (5) 15cm x 20cm (5)20cm x 20cm (5)
£1.35£2.51£4.30£5.88£7.01
Aquacel® Foam Adhesive 8cm x 8 cm (10)10cm x 10cm (10)
12.5cm x 12.5cm (10)17.5cm x 17.5cm (10)
21cm x 21cm (5)25cm x 30cm (5)
£1.39£2.16£2.68£5.36£7.84
£10.05
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 21 27/01/2017 10:09

Area Drug and Therapeutics Committee
21
Hydrogel Dressings
First choice : Purilon®Gel
Description An amorphous gel with high water content, containing Calcium Alginate (Purilon®)
IndicationsHydrogels facilitate autolysis by rehydrating necrotic tissue and effecting debridement. They provide amoist environment which promotes healing. They are non-adherent and do not harm viable tissue orsurrounding skin. Bacterial colonisation of the wound is not a contraindication to the use of a hydrogel.
Method of UseApply the gel directly into the wound. A secondary moisture - retentive dressing is required e.g. Hydrogelshould be changed when the cover dressing leaks. Intervals should not exceed 3 days when used on sloughy or necrotic wounds or 7 days if used on clean granulating wounds.
N.B. When using in cavity wounds only half fill the cavity. Due to the effective debridement of necrotictissue, a wound being treated with gel may appear larger at first dressing change, however, this is anatural step in the healing process.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Purilon® Sterile 8g tube (10)Sterile 15g tube (10)
£1.76£2.30
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 22 27/01/2017 10:09

Area Drug and Therapeutics Committee
22
Alginate Dressings
Kaltostat®
Description The basic elements of alginates are extracted from brown seaweed (Phaeophyceae). Their clinicalcomposition means that they are highly absorbent and biodegradeable. Alginates vary in composition (calcium/sodium salts of alginic acid) and in the arrangement of fibres.
IndicationsAlginate dressings are suitable for moderate to heavily exuding wounds. They form a gel on contact withthe wound exudate, and are effective at absorbing exudate, debriding slough and encouraging granulation tissue. Where bleeding is involved, Kaltostat® may be considered as a haemostatic agent.
Method Of UseApply to the wound surface/cavity, secondary dressing required to secure. Frequency of change will depend on level of exudate.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Kaltostat® 5cm x 5cm (10)7.5cm x 12cm (10)10cm x 20cm (10)15cm x 25cm (10)
£0.96£2.10£4.12£7.08
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 23 27/01/2017 10:09

Area Drug and Therapeutics Committee
23
Deodourising Dressings
First choice : Clinisorb®Second choice : CarboFlex®
Clinisorb®
Description Clinisorb® is an activated charcoal cloth dressing, produced by carbonising and activating woven viscoserayon that is sandwiched between two layers of a nylon and viscose rayon blend. Clinisorb® has theoptimum combination of microporous activity and activated charcoal cloth weight, for significantlyreducing odour by attracting and permanently trapping bacteria. It is non-adhesive and contained in asterile peel pack.
IndicationsClinisorb® can be used to manage malodourous wounds such as fungating breast lesions, pressure ulcers,leg ulcers and diabetic foot ulcers.
Method Of UseClinisorb® can be used as a primary or secondary dressing and its soft, flexible construction can be cut to fitpractically any wound. Even unusually shaped fungating wounds on curved body sites can be easilydressed. Clinisorb® is highly effective wet or dry, can be used either side down, and can be left in place forup to one week.
CarboFlex®
Description A sterile non-adhesive dressing consisting of five layers - film layer, absorbent padding, activated charcoalcloth, film layer and absorbent wound contact layer containing Kaltostat® and Aquacel®.
IndicationsFor use in the management of malodourous acute and chronic wounds. May be used as a primary dressingfor shallow wounds or as a secondary dressing over wound fillers with deeper wounds.
Method Of UseThis dressing must not be cut to size or shape. The fibrous surface is placed directly on to the wound. Thismay be left undisturbed for up to three days depending on the level of exudate.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Clinisorb® 10cm x 10cm (10)10cm x 20cm (10)15cm x 25cm (10)
£1.91£2.54£4.09
CarboFlex® 8cm x 15cm (5) Oval10cm x 10cm (10)15cm x 20cm (5)
£3.89£3.24£7.38
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 24 27/01/2017 10:09

24
Silicone Dressings
Mepitel® One
Description A sterile transparent soft silicone wound contact layer, which is non adherent to a moist wound bed.
IndicationsFor use in a wide range of painful, chronic and traumatic wounds and wounds with compromised or fragilesurrounding skin. The soft silicone adheres gently to the surrounding skin and ensures removal withminimal trauma and pain. Mepitel®One prevents the outer dressing sticking to the wound. The porous structure of Mepitel® One allows exudate to pass to an outer absorbent dressing.
Method Of UseApply directly to the wound or wound bed. It can be cut to size or shape of wound if desired. Requires asecondary dressing which can be changed independently as the Mepitel® One can remain in place for up to10 days. Mepitel® One may offer advantages when primary dressings are required to stay in place forlonger periods, since it is adhesive on one surface only.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Mepitel® One 6cm x 7cm (5)9cm x 10cm (5)
13cm x 15cm (5)24cm x 27.5cm (5)
£1.22£2.41£4.95
£14.25
Mepilex® Lite
Description A thin absorbent foam dressing with soft silicone contact layer and film backing
IndicationsFor use on non to low exuding woumds. May also be used as a protective dressing on compromised orfragile skin.
Method of Use Apply directly to wound or wound bed. Mepilex® Lite can be easily cut to fit an individual wound andmakes it ideal for difficult to dress wounds, such as armpits, breast etc.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Mepilex® Lite 6cm x 8.5cm (5)10cm x 10cm (5)15cm x 15cm (5)20cm x 50cm (5)
£1.82£2.17£4.22
£26.60
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 25 27/01/2017 10:09

25
Silicone Foam Dressings
Allevyn® Gentle / Alleyvn ®Gentle Border Description An absorbent hydrocelluar pad sandwiched between a perforated soft gel adhesive woundcontact layer and highly permeable waterproof outer film. Alleyvn ®Gentle Border benefits from aneasy application and removal of the dressing with the ability to reposition through anadhesive technology based on the soft silicone gel in the dressing.
IndicationsDesigned for a wide range of moderate to highly exuding wounds e.g. leg, foot and pressure ulcers,traumatic wounds and secondary healing wounds.
Method of Use
During the early stages of wound management, Allevyn Gentle Border dressings should be inspected
frequently. Where the product is used on infected wounds, the infection should be inspected and treated
as per local clinical protocol.
Dressings can be left in place for up to 7 days depending on the condition of the wound and the
surrounding skin or until exudate is visible and approaches to within 1.5cm of the edge of the dressing pad,
whichever is sooner. If required, Allevyn®Gentle can be cut.
Contraindications
Do not use Allevyn® Gentle Border dressings with oxidising agents such as hypochlorite solutions (e.g.
Eusol or Hydrogen peroxide, as these can break down the absorbent polyurethane component of the
dressing. If reddening or sensitisation occurs discontinue use.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Allevyn® Gentle Border 7.5cm x 7.5cm (10)10cm x 10cm (10)
12.5cm x 12.5cm (10)15cm x 15cm (10)
17.5cm x 17.5cm (10)10cm x 20cm (10)
£1.51£2.21£2.71£4.04£5.34£3.56
Allevyn® Gentle 5cm x 5cm (10)10cm x 10cm (10)15cm x 15cm (10)10cm x 20cm (10)20cm x 20cm (10)
£1.27£2.53£4.25£4.07£6.78
Allevyn® Gentle Border Sacrum 16.8cm x 17.1cm (10)21.6cm x 23cm (10)
£4.00£5.66
Allevyn® Gentle Border Lite 5cm x 5cm (10)7.5cm x 7.5 cm (10)10cm x 10cm (10)15cm x 15cm (10)
5.5cm x 12cm (10)8cm x 15cm (10)
10cm x 20cm (10)
£0.90£1.39£2.16£3.81£1.85£3.43£3.43
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 26 27/01/2017 10:09

26
Super Absorbent Dressings
Kliniderm®
Description Super absorbent secondary dressing compromising of four layers: a hydrophillic wound contact layer, a distribution layer, a super absorbent inner core and a fluid repellent wound conact layer
IndicationsModerate to heavily exuding wounds. May be used under compression
IndicationsNot to be used on dry wounds, heavy bleeding wounds and surgical implantation. The dressing must not be cut.
Eclypse®
Description Super absorbent secondary dressing
Indications Moderate to heavily exuding wounds
IndicationsNot to be used on arterial bleeds or heavily bleeding wounds. If a wound has a potential to dry out, a nonadherent wound contact layer should be applied beforehand. Do not cut dressing.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Kliniderm® 10cm x 10cm (50)10cm x 15cm (10)20cm x 20cm (15)20cm x 30cm (10)
£0.49£0.69£0.99£1.49
Eclypse® 15cm x 15 cm (20)20cm x 30 cm (20)60cm x 40cm (10)
£0.97£2.14£8.15
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 27 27/01/2017 10:09

27
Specialised Dressings & Therapies
onthe advice of the relevant specialist, Acute or Community
Antimicrobial Dressings
Antimicrobials are agents which kill or inhibit the growth and division of micro-organisms. Commonly used in wound management are honey, iodine and silver.
There is no robust clinical evidence that dressings containing antimicrobials (e.g. silver, iodine or honey) are more effective than undedicated dressings for the prevention of wound infections.
Indiscriminate use of topical antimicrobial dressings should also be discouraged because of concerns over bacterial resistance and toxicity.
You may be asked by your local pharmacist, GP Practice or Wound Specialist Nurse to give a rationale for using these products. Please use the following tips to aid your selection.
10 Top Tips when using Antimicrobial Dressings
GENERAL POINTS
Is the wound clinically infectedo Check for signs of infectiono Don’t confuse normal signs of
inflammation with infection Systemic antibiotics are indicated in cases of
overt wound infection where classical signs are evident
Check the correct antimicrobial is chosen according to the wound exudate levels
If no improvement in wound after two weeks, review wound and antimicrobial choice
Check cautions as stated in manufacturer instructions, and BNF when using antimicrobial preparations.
SILVER DRESSINGS
Some silver products oxidise in contact with air and this may be displayed as a brown/black discolouration on the wound bed and/or surrounding skin
HONEY PRODUCTS
Patients may experience pain due to osmotic effects of dressing on wound (e.g. “drawing sensation”). Monitor pain levels, consider simple analgesia and only remove if the dressing is not tolerated.
Wound exudate may increase when using honey ointments and therefore use an appropriate absorbent secondary dressing.
IODINE PREPARATIONS
These products are rapidly deactivated by wound exudate therefore consider other antimicrobials for moderate – highly exudating wounds
All iodine products change from orange/brown to white when iodine is inactive/”used up”.
Please see Ropper Lothian Ladder on next page for further guidance
Initiation of these products should be on the advice of the relevant specialist e.g. Acute or Community Tissue Viability Nurse, Podiatry, Vascular, Plastic
Surgery or Dermatology Service.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 28 27/01/2017 10:09

28
Each stage builds on the previous signs noted
Stage 4: Overt signs of local infection and signs of systemic infection: may lead to sepsis if not treated Spreading cellulitis Pus/abscess Patient systemically unwell
e.g. confusion Pyrexia Raised white cell count/CRP Malodour of wound
Stage 4 – Treatment If systemic signs only, consider other source of infection Swab wound using standardised method Consider taking blood cultures prior to starting antibiotics Start broad spectrum systemic antibiotics* while awaiting culture
results Consider combination therapy with topical antimicrobials** e.g. in
PVD, diabetes Monitor wound progress, review wound at 2 weeks and stop
topical antimicrobials when signs of infection cease Once topical antimicrobial stopped continue with correct dressing
regime for wound/tissue type
Stage 3: Overt signs of local infection: evidence of surrounding tissue involvement, wound deteriorating Localised cellulitis Discoloured or bleeding granulation tissue Pain in or around wound Exudate: thick, haemopurulent or purulent
and/or high volumes Localised oedema Malodour
Stage 3 – Treatment Swab wound using standardized method Drain any local collections of pus/fluid Consider combination therapy with broad spectrum systemic
antibiotics* and topical antimicrobials** Monitor wound progress, review wound at 2 weeks and stop
topical antimicrobials when signs of infection cease Once topical antimicrobial stopped continue with correct dressing
regime for wound/tissue type If no progress after two weeks and/or signs of systemic infection
move to Stage 4
Stage 2: Increasing signs of infection (Critical colonisation): healing not progressing normally Exudate – high volumes Malodour Pain in or around wound Discolouration of granulation tissue Slough/Necrosis
Stage 2 – Treatment Select topical antimicrobial** Monitor wound progress, review wound 1-2 weeks If no improvement:
i. Consider swabbing wound using standardised method ii. Consider alternative topical antimicrobial**
If improved stop topical antimicrobials when signs of infection cease
Once topical antimicrobial stopped continue with correct dressing regime for wound/tissue type
If no progress after two weeks and/or increasing signs of systemic infection move to Stage 3
Stage 1: Few subtle signs: healing progressing normally
Exudate – low to moderate volume Pain – minimal Odour – minimal Slough/necrosis – minimal
Stage 1 – Treatment Promote moist wound healing using correct dressing regime for
wound/tissue type & exudate level Monitor wound progress, if no improvement in 1-2 weeks
reassess wound and dressing choice Check underlying aetiology of wound, if required refer to
appropriate specialist e.g. vascular, diabetic podiatry, tissue viability, lymphoedema etc.
If no progress after a further 1-2 weeks and/or increasing signs of infection/critical colonisation move to Stage 2
START
This guidance should be used along with clinical judgement in complex patients; in particular patients with diabetic wounds, vascular problems and immuno compromised patients may require topical antimicrobials for prophylaxis as well as treatment. *Systemic Antibiotics – Follow NHS Fife Antibiotic Guidance for the Treatment of Community Managed Infections Sept 2010. **Topical Antimicrobial – NHS Fife Joint Wound Formulary 2010. Topical antimicrobials can include honey, iodine, silver, PHMB, DACC and enzymatic products. Contact TVN team for more info if required.
References::European Wound Management Association (2005) Position Document: Identifying criteria for wound infection, MEP, London European Wound Management Association (2006) Position Document: Management of wound infection, MEP, London Best Practice Statement: Use of topical antiseptic/antimicrobial agents in wound management, Wounds UK, Aberdeen (2010) Good Practice Recommendation for Antimicrobial Use in Frail Elderly 2013
Adapted & reproduced with permission of R. Ropper, TVN CNS NHS
Lothian
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 29 27/01/2017 10:09
The Adapted Ropper Lothian Ladder Guidelines for identifying infected wounds and when to start & stop using topical antimicrobial dressings

29
Specialised Dressings & Therapies
Silver Containing Dressings
Aquacel® Ag+ RibbonAquacel® Ag+ ExtraUrgotul®SSD
Aquacel® Ag+ Ribbon/Extra
DescriptionAquacel®Ag+ Ribbon is a versatile primary dressing. The combination of Hydrofiber® Technology with ionicsilver (Ag+), enhanced with anti – biofilm technology, produces a dressing that is highly absorbent and hasfavourable gelling characteristics with the aid of broad-spectrum antimicrobial activity
IndicationsFor use in moderate to highly exuding chronic and acute wounds where there is infection or an increasedrisk of infection. Also suitable for cavity wounds
Contraindications Should not be used on patients who are sensitive to, or have had an allergic reaction to silver or sodiumcarboxymethycellulose.
Urgo®SSDDescription A non adherent, non occlusive, antibacterial contact layer. The contact layer is a polyester meshimpregnated with hydrocolloid petroleum jelly and silver sulphadiazine particles.
IndicationsFor use on non to lightly exuding wounds with signs of infection. Can be combined with an absorbent layerfor heavily exuding wounds. Can also be used in cavity wounds.
Contraindications Do not use on patients with a known sensitivity to any components of the dressing.Caution: Do not use on patients undergoing MRI scans. Avoid contact with electrodes or conductive gels
during electronic measurement procedures.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Aquacel® Ag+ Ribbon 1cm x 45cm (5)2cm x 45cm (5)
£3.12£4.76
Aquacel ® Ag+ Extra 5cm x 5cm (5)10cm x 10cm (5)15cm x 15cm (5)
2cm x 30cm (5) 4cm x 10cm (5) 4cm x 20cm (5) 4cm x 30cm (5)
£1.95£4.64£8.75
£21.71£2.83£3.69£5.52
Urgotul® SSD 10cm x 12cm (10)15cm x 20cm (10)
£3.17£8.99
Initiation of these products should be on the advice of the relevant specialistpractitioner and follow local policies for use.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 30 27/01/2017 10:09
30
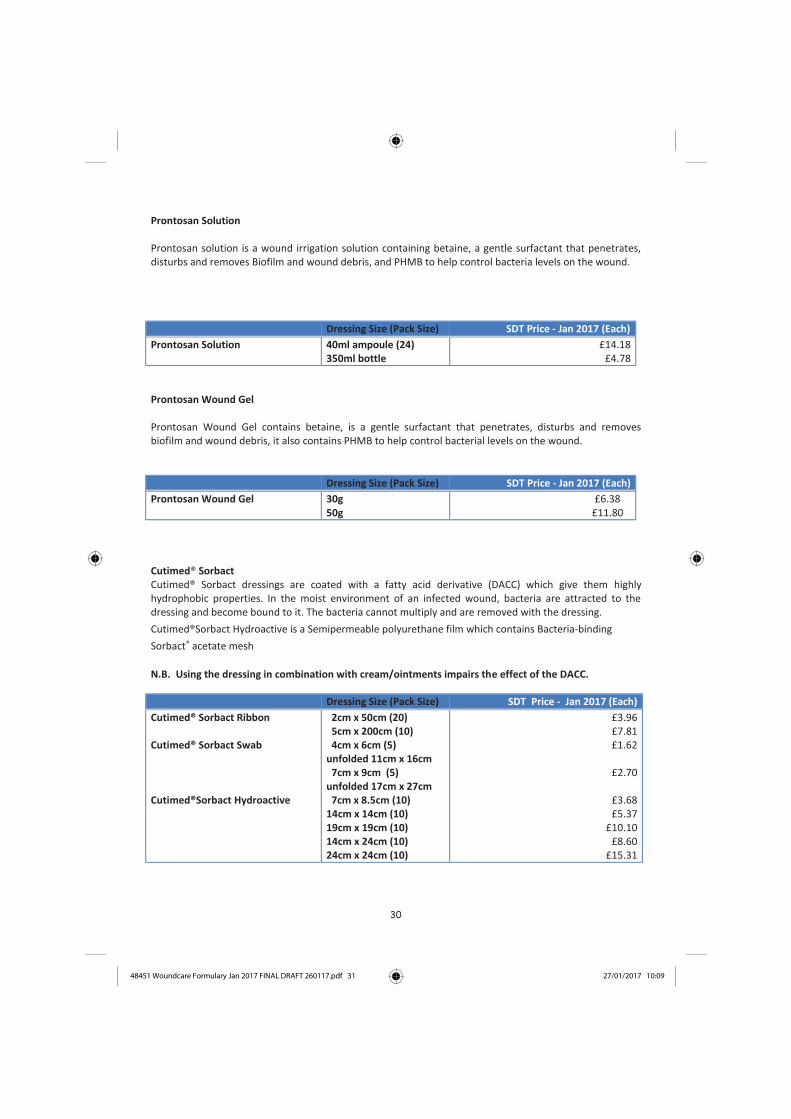
Prontosan Solution
Prontosan solution is a wound irrigation solution containing betaine, a gentle surfactant that penetrates,disturbs and removes Biofilm and wound debris, and PHMB to help control bacteria levels on the wound.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Prontosan Solution 40ml ampoule (24)350ml bottle
£14.18£4.78
Prontosan Wound Gel
Prontosan Wound Gel contains betaine, is a gentle surfactant that penetrates, disturbs and removesbiofilm and wound debris, it also contains PHMB to help control bacterial levels on the wound.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Prontosan Wound Gel 30g50g
£6.38£11.80
Cutimed® SorbactCutimed® Sorbact dressings are coated with a fatty acid derivative (DACC) which give them highlyhydrophobic properties. In the moist environment of an infected wound, bacteria are attracted to the dressing and become bound to it. The bacteria cannot multiply and are removed with the dressing.
Cutimed®Sorbact Hydroactive is a Semipermeable polyurethane film which contains Bacteria-binding
Sorbact® acetate mesh
N.B. Using the dressing in combination with cream/ointments impairs the effect of the DACC.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Cutimed® Sorbact Ribbon
Cutimed® Sorbact Swab
Cutimed®Sorbact Hydroactive
2cm x 50cm (20)5cm x 200cm (10)4cm x 6cm (5)
unfolded 11cm x 16cm7cm x 9cm (5)
unfolded 17cm x 27cm7cm x 8.5cm (10)
14cm x 14cm (10)19cm x 19cm (10)14cm x 24cm (10)24cm x 24cm (10)
£3.96£7.81£1.62
£2.70
£3.68£5.37
£10.10£8.60
£15.31
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 31 27/01/2017 10:09
31
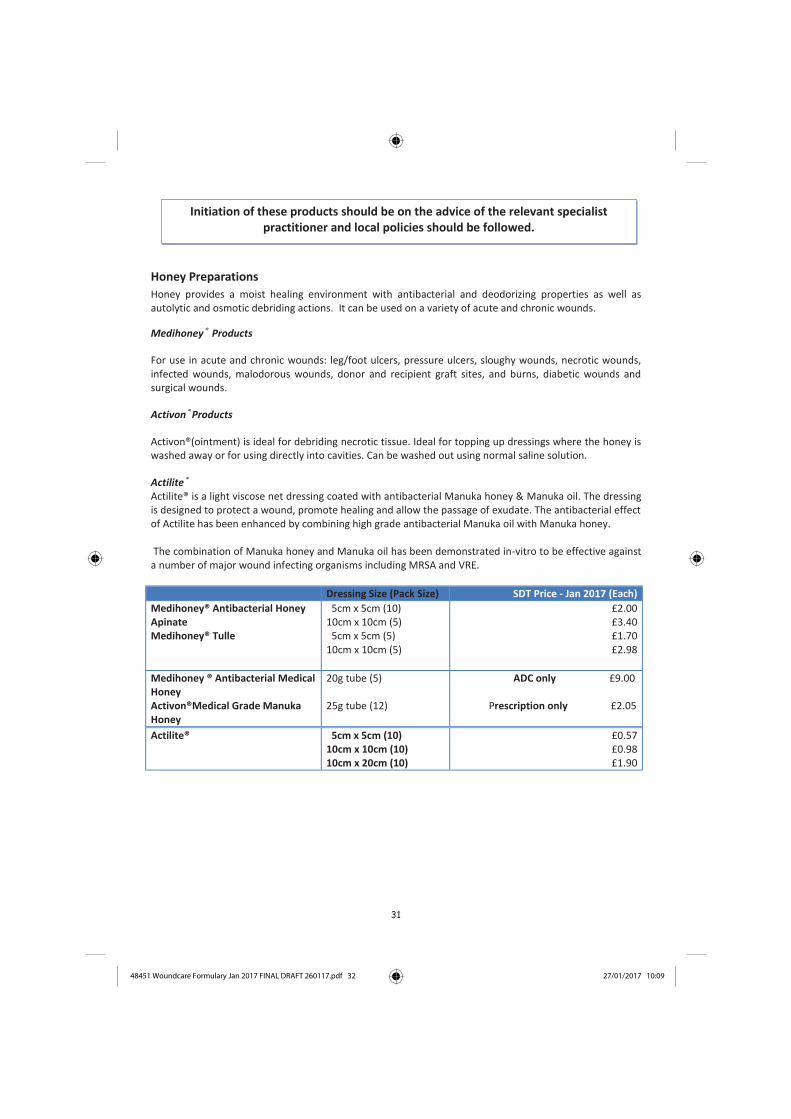
Honey Preparations
Honey provides a moist healing environment with antibacterial and deodorizing properties as well asautolytic and osmotic debriding actions. It can be used on a variety of acute and chronic wounds.
Medihoney® Products
For use in acute and chronic wounds: leg/foot ulcers, pressure ulcers, sloughy wounds, necrotic wounds,infected wounds, malodorous wounds, donor and recipient graft sites, and burns, diabetic wounds andsurgical wounds.
Activon®Products
Activon®(ointment) is ideal for debriding necrotic tissue. Ideal for topping up dressings where the honey iswashed away or for using directly into cavities. Can be washed out using normal saline solution.
Actilite®Actilite® is a light viscose net dressing coated with antibacterial Manuka honey & Manuka oil. The dressingis designed to protect a wound, promote healing and allow the passage of exudate. The antibacterial effectof Actilite has been enhanced by combining high grade antibacterial Manuka oil with Manuka honey.
The combination of Manuka honey and Manuka oil has been demonstrated in-vitro to be effective againsta number of major wound infecting organisms including MRSA and VRE.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Medihoney® Antibacterial HoneyApinateMedihoney® Tulle
5cm x 5cm (10) 10cm x 10cm (5)
5cm x 5cm (5)10cm x 10cm (5)
£2.00£3.40£1.70£2.98
Medihoney ® Antibacterial MedicalHoneyActivon®Medical Grade ManukaHoney
20g tube (5)
25g tube (12)
ADC only £9.00
Prescription only £2.05
Actilite® 5cm x 5cm (10)10cm x 10cm (10)10cm x 20cm (10)
£0.57£0.98£1.90
Initiation of these products should be on the advice of the relevant specialistpractitioner and local policies should be followed.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 32 27/01/2017 10:09

32
Iodine Dressings
CAUTION: Care must be taken when these dressings are used for patients with Thyroid or Renal Patients.
Inadine®A sterile low-adherent fabric dressing impregnated with 10% povidone iodine in a water soluble slowrelease base. Povidone iodine is a potent antibacterial agent with a broad spectrum of activityIt is used as a primary wound dressing providing prophylactic treatment against infections in superficialwounds and minor skin injuries. The dressing should be changed daily or when the orange/ brown colourturns to white.
lodoflex® Iodoflex is a sterile Cadexomer Iodine paste containing Iodine in an inert base. The sachet consists of thepaste sandwiched in protective gauze. Used for the topical treatment of a variety of chronic and acutewounds. When applied to the wound lodoflex® cleans and reduces' bacteria at the wound surface and isparticularly useful in highly exuding wounds.
Remove the protective gauze on both sides of the paste, lodoflex® can then be moulded into shape andapplied to the wound surface. An appropriate secondary dressing can then be applied. The dressing shouldbe changed every 72 hours.
N.B. Maximum single application is 50g; weekly maximum must not exceed 150g; treatment durationshould not exceed three months.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Inadine® 5cm x 5cm (25)9.5cm x 9.5cm (10)
33p49p
Iodoflex® 5g (5)10g (3)17g (2)
£4.13£8.25
£13.06
Antimicrobial Alginate Gel
Flaminal®
Flaminal® is an antimicrobial alginate gel, indicated for a variety of wounds. It maintains a moist woundenvironment, helps debride and restore bacterial balance. It comes in two preparations, Flaminal® Fortefor medium to heavily exuding wounds, and Flaminal® Hydro for low to moderately exuding wounds.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Flaminal® Forte 15g (5)50g (5)
£7.61£25.18
Flaminal® Hydro 15g (5)50g (5)
£7.61£25.18
N.B. Flaminal® preparations are intended for single patient use, but can be used for multiple applicationson the same patient, as this will make the product more Price effective.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 33 27/01/2017 10:09

33
Pain Management Dressing
ActiFormCool®
A transparent, non-adhesive high water content hydrogel, formed around a supporting blue polyethylenematrix. It can be particularly useful for painful wounds, e.g. leg ulcers and diabetic ulcers.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
ActiFormCool® 5cm x 6.5cm (5)10cm x 10cm (5)10cm x 15cm (5)20cm x 20cm (5)
£1.81£2.66£3.83£8.01
Foam/Fibre Dressing For Heavily Exuding Wounds
Allevyn® Life
A dressing which is a multi-layered design incorporating hydrocellular foam with a hyper-absorber lockaway core. It has a highly waterproof outer film and incorporates a mesh screen on the pad which allows the levels of exudate to be visible. This indicates when the dressing should be changed.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Alleyvn® LIfe 10cm x 10.3cm (10)12.9cm x 12.9cm (10)15.4cm x 15.4cm (10)
21cm x 21cm (10)
£1.71£2.51£3.06£6.04
Cutimed® Sorbion Sachet S
A versatile fibre dressing with high wearing comfort for highly exuding wounds. The dressing absorbs wound exudate and locks it in, creating a moist wound environment by gel formation. It provides a large capacity for wound exudate and ensures high retention of absorbed fluids.
Dressing Size (Pack Size) SDT Price – Jan 2017(Each)
Cutimed® Sorbion Sachet S 7.5cm x 7.5cm (10)10cm x 10cm (10) 20cm x 10cm (10)20cm x 20cm (10)
£1.78£2.25£3.73£7.00
Debridement Products
Debrisoft® PadDebrisoft® consists of soft, polyester fibres which are secured and knitted together. These fibres are cut ata special angle, length and thickness to ensure good effect and flexibility. The pad comes in a 10cm x 10xmsize and is used to remove slough and other debris from the wound bed to aid debridement. It can be usedon sloughy leg ulcers and surrounding skin to remove debris.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 34 27/01/2017 10:09

34
Debrisoft ® LollyComprises of monofilament polyester fibres with a blue X-ray detectable polypropylene thread. The Debrisoft ® Lolly is intended for the debridement of deep – including surgically invasive – to superficial wounds for wound bed preparation. It is used to absorb exudates, debris and keratoses during debridement.
Dressing Size (Pack Size) SDT Price -Jan 2017(Each)
Debrisoft ® Pad 10cm x 10cm (5) £6.45
Debrisoft Lolly £5.79
Tulle Dressings
Urogtul®A non adherent, non – occlusive flexible contact layer derived from Technology Lipido-Colloid (TLC
Technology). It is composed of a flexible polyester mesh impregnated with hydrocolloid and petroleumjelly particles. Can be used on acute wounds, skin abrasions and may be left for up too 7 days.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Urgotul® 5cm x 5cm (10)10cm x 10cm (10)15cm x 15cm (10)10cm x 40cm (10)15cm x 20cm (10)20cm x 30cm (5)
£1.55£3.11£6.60
£10.44£8.79
£14.13
Technology Lipidocolloid (TLC) - Urgo Dressings
Urgo® Clean Pad & Rope
Description A TLC Healing Matrix dressing which allows a pain free desloughing action, trapping and binding sloughwith its polyabsorbent fibres.It is also available as a rope which has similar absorption properties to Aquacel
IndicationsFor use in moderate to heavily exuding wounds. Change Urgo® Clean 1-2 days during the desloughingphase, then as often as required (up to 7 days)depending on levels of exudate.
Contraindications Do not use Urgo®Clean in combination with hydrogen peroxide organomercuric antiseptics orheocamidine.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Urgo® Clean Pad 6cm x 6cm(10)10cm x 10cm (10)20cm x 15cm (10)
£0.96£2.14£4.02
Urgo® Clean Rope/Probe 5cm x 40cm (10)2.5cm x 40cm (10)
£3.18£2.41
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 35 27/01/2017 10:09
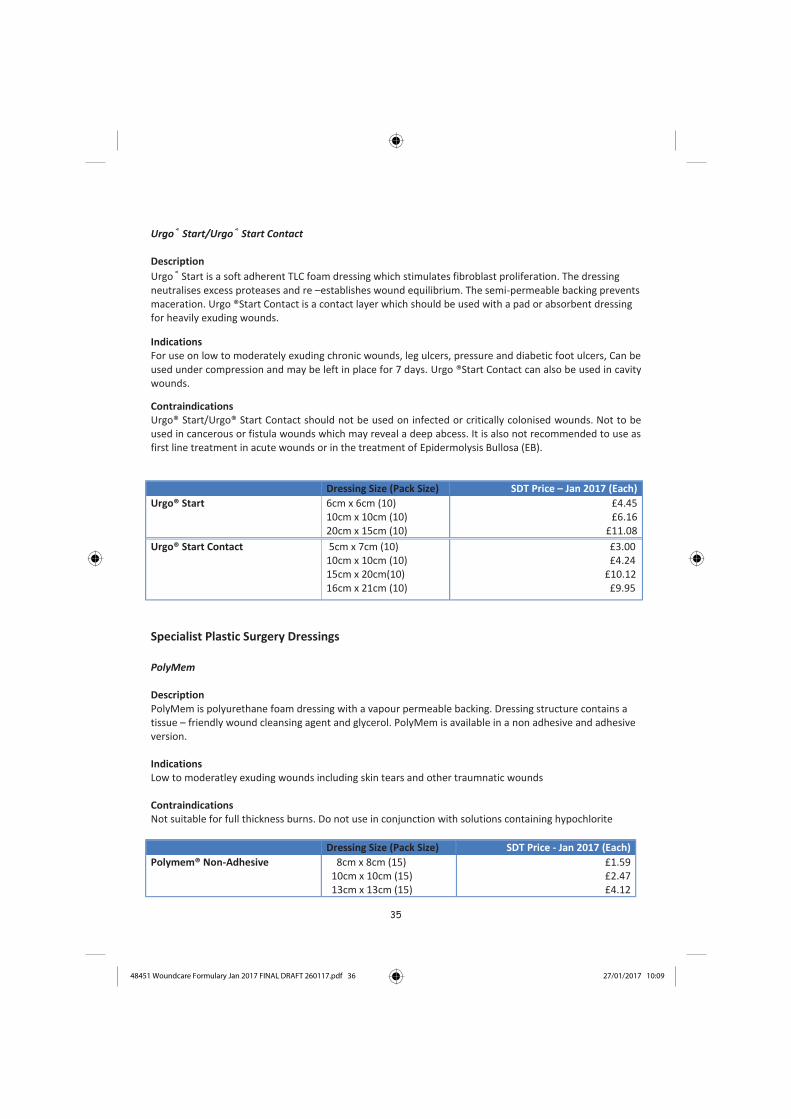
35
Urgo® Start/Urgo® Start Contact
Description
Urgo® Start is a soft adherent TLC foam dressing which stimulates fibroblast proliferation. The dressing neutralises excess proteases and re –establishes wound equilibrium. The semi-permeable backing prevents maceration. Urgo ®Start Contact is a contact layer which should be used with a pad or absorbent dressing for heavily exuding wounds.
IndicationsFor use on low to moderately exuding chronic wounds, leg ulcers, pressure and diabetic foot ulcers, Can beused under compression and may be left in place for 7 days. Urgo ®Start Contact can also be used in cavitywounds.
Contraindications Urgo® Start/Urgo® Start Contact should not be used on infected or critically colonised wounds. Not to beused in cancerous or fistula wounds which may reveal a deep abcess. It is also not recommended to use asfirst line treatment in acute wounds or in the treatment of Epidermolysis Bullosa (EB).
Dressing Size (Pack Size) SDT Price – Jan 2017 (Each)
Urgo® Start 6cm x 6cm (10)10cm x 10cm (10)20cm x 15cm (10)
£4.45£6.16
£11.08
Urgo® Start Contact 5cm x 7cm (10) 10cm x 10cm (10)15cm x 20cm(10)16cm x 21cm (10)
£3.00£4.24
£10.12£9.95
Specialist Plastic Surgery Dressings
PolyMem
Description PolyMem is polyurethane foam dressing with a vapour permeable backing. Dressing structure contains atissue – friendly wound cleansing agent and glycerol. PolyMem is available in a non adhesive and adhesiveversion.
IndicationsLow to moderatley exuding wounds including skin tears and other traumnatic wounds
Contraindications Not suitable for full thickness burns. Do not use in conjunction with solutions containing hypochlorite
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Polymem® Non-Adhesive 8cm x 8cm (15)10cm x 10cm (15)13cm x 13cm (15)
£1.59£2.47£4.12
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 36 27/01/2017 10:09
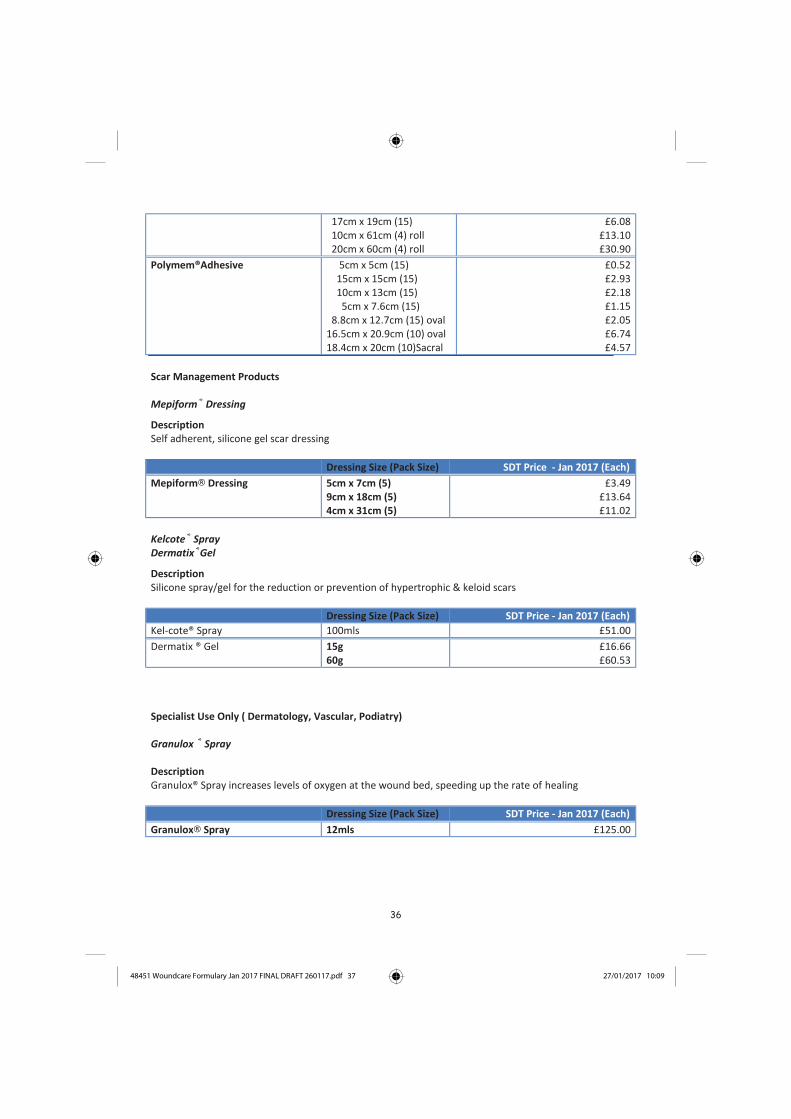
36
17cm x 19cm (15)10cm x 61cm (4) roll20cm x 60cm (4) roll
£6.08£13.10£30.90
Polymem®Adhesive 5cm x 5cm (15) 15cm x 15cm (15) 10cm x 13cm (15)5cm x 7.6cm (15)
8.8cm x 12.7cm (15) oval16.5cm x 20.9cm (10) oval18.4cm x 20cm (10)Sacral
£0.52£2.93£2.18£1.15£2.05£6.74£4.57
Scar Management Products
Mepiform® Dressing
Description Self adherent, silicone gel scar dressing
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Mepiform® Dressing 5cm x 7cm (5)9cm x 18cm (5)4cm x 31cm (5)
£3.49£13.64£11.02
Kelcote® SprayDermatix®Gel
Description Silicone spray/gel for the reduction or prevention of hypertrophic & keloid scars
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Kel-cote® Spray 100mls £51.00
Dermatix ® Gel 15g60g
£16.66£60.53
Specialist Use Only ( Dermatology, Vascular, Podiatry)
Granulox ® Spray
Description Granulox® Spray increases levels of oxygen at the wound bed, speeding up the rate of healing
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Granulox® Spray 12mls £125.00
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 37 27/01/2017 10:09

37
Larvae Therapy
Larvae reduce or eliminate odour and combat infection by ingesting and killing bacteria.Sterile larvae of the common green-bottle Lucilia Sericata are used to treat most types of sloughy, infectedor necrotic wounds. They may also reduce wound pain and stimulate the formation of granulation tissue.Larvae therapy is available on a GP10 prescription.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
BioBag® Dressing 2.5cm x 4cm (1)5cm x 6cm (1)10cm x 10cm (1)
£195.00£245.00£295.00
Negative Pressure Wound Therapy (NPWT)
Negative Pressure Wound Therapy (NPWT) is a treatment used across the wound through a dressingpositioned in the wound cavity or over a flap or graft. Excess fluid is collected in a disposable canister. NPWT helps to reduce oedema, increase blood supply and decrease bacterial colonisation. It has proven tobe effective with acute surgical wounds, pressure ulcers, chronic wounds, including diabetic feet, and skingrafts.
Patients may be discharged from the Acute Services Division into Community with NPWT in situ. Community staff should consult local policy, as permission must be granted from the Lead Nurse for hire ofunit and dressings. The NPWT pumps used (Acelity) are free of charge. Dressings and canisters areavailable on drug tariff. All pumps once discontinued must be returned to the original source. Within theAcute Services Division return units to Ward 33. For community rentals, return to Acelity.
PICO® (Disposable NPWT system)A disposable and portable system designed to kick start wound healing. It can be used on both acute andchronic wounds, diabetic or pressure ulcers, flaps and grafts and surgically closed incision sites. The packcontains one PICO® device and two PICO® dressings. Advice should be sought from the local tissue viability nurse or specialist nurse before using.
ContraindicationsContraindicated in the presence of: malignancy in the wound bed or wound margins (except in palliativecare to enhance quality of life).
Dressing Size (Pack Size) SDT Price – Jan 2017 (Each)
PICO® 10cm x 20cm (1)10cm x 30cm (1)10cm x 40cm (1)15cm x 15cm (1)15cm x 20cm (1)15cm x 30cm (1)20cm x 20cm (1)25cm x 25cm (1)
£123.50£123.50£141.61£123.50£123.50£141.61£141.61£141.61
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 38 27/01/2017 10:09

38
Wound Drainage Bag
Wound drainage bags have a central hydrocolloid island that can be cut and shaped to fit the wound. Theyare particularly useful in large abdominal wounds with high levels of exudate, where conventionaldressings would need to be changed more than twice daily.
Dressing Size (Pack Size) SDT Price - Jan 2017 (Each)
Biotrol®Draina S Fistula Mini (30)Medium (30)Large (20)
£2.59£3.88£4.77
Eakin® Wound Pouches(fold and tuck or bung closures)
Small (10)Medium (10)Large (10)Extra Large (5)
From £4.77From £6.89From £9.00
From £15.89
Other sizes/styles are available, contact companies directly for sizes and prices.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 39 27/01/2017 10:09

39
Glossary of Wound Terms
Angiogenesis Generation of new blood vessels initially seen at the base of a wound.
Autolysis Breakdown of devitalised tissue by leucocytes.
Biofilm A thin but robust layer of micro – organisms that cannot be seen by the naked eye, adhering to a solid surface and containing a community of bacteria and other organisms.
Cellulitis A spreading non-suppurative infection of the soft tissue.
Colonisation Multiplication of micro-organisms without a corresponding host reaction.
Contraction Function of the healing process in granulating wounds whereby the edges of the wound are drawn towards each other.
Debridement Removal of devitalised tissue and foreign matter from a wound.
Epithelialisation Final stage of the proliferative phase.
Eschar Scab consisting of dried serum and devitalised dermal cells.
Granulation Formulation of new tissue filling the defect which takes place during the proliferative phase of healing. The name is derived from the fact that the buds of new tissue take on the appearance of small granules.
Healing by first intention Also called Primary Intention. Wounds are closed with sutures, staples or skin glue, leaving a minimal defect.
Healing by secondary intention
Wound left open and allowed to heal by granulation.
Healing by third intention Also called Tertiary intention, or delayed closure. Wound left open often to assist drainage and closed surgically at a later date.
Infection Micro-organisms present and multiplying, producing an associated host reaction. Reaction may take various forms.
Maceration Softening or sogginess of the tissue owing to retention of excessive moisture.
Necrosis Local death of tissue. Tissue is often black/brown in colour and leathery/waxy in texture.
Overgranulation
Granulation tissue is raised above the peri-wound area.
Slough
Devitalised tissue which has yellow/white/grey hue.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 40 27/01/2017 10:09

40
Reading List
Barwell et al (2015) Diabetes Foot Infection Antibiotic Protocol
Briggs et al (2004) Principles of best practice: Minimising pain at wound dressing – related procedures. A consensus document http://www.woundsinternational.com/media/issues/79/files/content_39.pdf
Cooper R (2009) Biofilms: hard to detect, easy to under estimate, but most definitely here to stay. Wounds UK. 9 (1) p.12.
Cope G (2014) The effects of smoking on wound healing. Wounds UK Vol 10 (2)
Dow G (2003) Bacterial swabs and the chronic wound: When, how and what do they mean. Ostomy Wound Management. 49; 5A supplement: p. 8-13.
Drugs and Therapeutic bulletin (2010) Silver dressings - do they work? Dtb.bmj.com. p. 38-42.
European Wound Management Association (2004) Position Document Wound bed preparation in practice.London: MEP Ltd.
European Wound Management Association (2005) Position Document Identifying criteria for wound infection. London: MEP Ltd.
European Wound Management Association (2006) Position Document Management of wound Infection. London: MEP Ltd.
European Wound Management Association (2007) Position Document Topical Negative Pressure In wound Management. London: MEP. Ltd
European Wound Management Association (2008) Position Document Hard-to-heal wounds: A holistic approach. London: MEP Ltd.
Gottrup F, Apelqvist J et al (2013) EWMA Document: Antimicrobials and Non-healing wounds- Evidence. Controversies and suggestions. Journal of Wound Care. 22 (5 suppl): S1-S92.
Guy H (2012) The Difference Between Moisture Lesions and Pressure Ulcers. Wound Essentials. Vol. 1 p. 36-44. Available at: www.wounds-uk.com
Healthcare Improvement Scotland (2015)., Antimicrobial Wound Dressings for Chronic Wounds – HTA Report 13, Edinburgh: HIS. Available at www.healthcareimprovementscotland.org
King B (2003) A review of research investigating pain and wound care. Journal of Wound Care. 12(6) p. 219-223.
Medlin S (2012) Nutrition For Wound Healing. British Journal of Nursing (Tissue Viability Supplement) Vol, 21, No 12. S11-15.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 41 27/01/2017 10:09

41
NHS Quality Improvement Scotland (2009) Best Practice Statement. Prevention and Management of Pressure Ulcers. Available at www.healthcareimprovementscotland.org
Phillips PL, Wolcott RD, et al. (2010) Biofilms Made Easy. Wounds International 1(3). Available at www.woundsinternational.com
Strohal R, Apelqvist J, Dissemond J et al (2013) EWMA Document: Debridement. Journal of Wound Care. 22 (suppl.1) S1-S52.
Toit DF (2009) An in vitro evaluation of the cell toxicity of honey and silver dressings. Journal of Wound Care. 18 (9) p.383-399.
Yates S (2012) Differentiating Between Pressure Ulcers and Moisture Lesions. Wound Essentials. Vol 2. p.16-22. Available at www.wounds-uk.com.
White R, Cutting K (2008) Critical colonisation of chronic wounds: microbial mechanisms. Wounds UK. 4(1) P70-78.
Wounds International (2012) Appropriate use of Silver Dressings in Wounds. An expert working group consensus. London. Available to download from www.woundsinternational.com
Wounds UK (2016) Cavity Wounds, Quick Guide www.woundsuk.com
Wounds UK (2010) PHMB and its potential contribution to wound management. Wounds UK, Aberdeen. Available at www.wounds-uk.com.
Winter GD (1962) Formation of the scab and rate of epithelialisation of superficial wounds in the skin of young domestic pig. Nature 193: 293-294.
Resources/ Links
Local Tissue Viability Resource: NHS Fife Tissue Viability Webpage (Intranet)
Tissue Viability Resource: www.tissueviabilityscotland.org
Tissue Viability Resource: www.wounds-uk.com
Skin Tear Guidelines: www.tissueviabilityscotland.org
Best practice for leg ulcer management: www.legulcerforum.org
Diabetic Foot Infection Guidelines: ..\..\Desktop\Diabetic Foot Guidance Final - April 2014.pdf
Learn Pro Modules: Preventing and Managing Pressure Ulcers, CPR For Feet (NHS Education for Scotland)
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 42 27/01/2017 10:09
42
Related policies, standard operating procedures and guidance
NHS Fife Procedure for Prevention and Management of Pressure Ulcers (2016)
NHS Fife Policy for Obtaining Informed Consent (2013)
SIGN Guidelines 120. Management of Chronic Venous Leg Ulcers (August 2010)
Healthcare Improvement Scotland, Prevention and Management of Pressure Ulcer Standards, 2016 ..\..\Desktop\HIS Pressure Ulcer Standards 2016.pdf
NHS Fife Podiatry Foot Protection and Offloading Guidance 2015
NHS Fife Community Exception Form http://www.fifeadtc.scot.nhs.uk/formulary/woundcare-formulary/woundcare-catheter-product-request-and-exception-form.aspxThe lists above are not exhaustive. It is the practitioner’s responsibility to be aware of up todate policies and procedures.
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 43 27/01/2017 10:09

43
Appendix 1 – Wound Assessment Chart
Assessment Chart for Wound Management For multiple wounds complete formal wound assessment for each wound. Add Inserts as needed.
Factors which could delay healing: (Please tick relevant box)
Immobility □ Poor Nutrition □ Diabetes □ Incontinence □Respiratory / CirculatoryDisease □ Anaemia □ Medication □ Chemotherapy □
Wound Infection □ Previous History of MRSA Infection □
Inotropes □ Anti-Coagulants □ Oedema □ Steroids □
Other ………….. Allergies & Sensitivities ……………………….
Body Diagram
Front Back
Mark location with ‘X’ and number each wound
Type of Wound Total number & duration of each type of wound
Leg Ulcer …………………………………..
Surgical Wound ……………………………….
Diabetic Ulcer ………………………….…
Pressure Ulcer ………………………………..
Other, specify ………………………………
Feet Diagram
Right Left
Mark location with ‘X’ and number each wound
Date referred to:
TVN …………….Physiotherapist…………….
Podiatrist………………Dietician……………...
Other (please specify)………………………….
Assessors signature: ………………………..
Date: ………………………..…………………...
WRITE, IMPRINT OR ATTACH LABEL
Surname ……………….... CHI No ….…………..
Forenames ………………… Sex…………………..
DoB ………………..
Location……………………………………………………
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 44 27/01/2017 10:09

44
Formal Wound Assessment Complete on initial assessment and thereafter complete at every dressing change
Date of Assessment
Number of wound
Analgesia required (Refer to local pain assessment tool)
Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No
Regular/ongoing analgesia Pre-dressing only
Wound Dimensions (enter size) Length (cm/mm) Width (cm/mm) Depth (cm/mm) Or trace wound circumference Is wound tracking/undermining Photography Tissue type on wound bed ( enter percentages) Necrotic (Black)
Sloughy (Yellow/Green)
Granulating (Red)
Epithelialising (Pink)
Hypergranulating (Red)
Haematoma
Bone/tendon
Wound exudate levels/ type (tick all relevant boxes) Low Moderate High * Serous (Straw) Haemoserous (Red/Straw) Purulent (Green/Brown/Yellow)* Peri-wound skin (tick relevant boxes) Macerated (White) Oedematous * Erythema (Red)* Excoriated (Red) Fragile Dry/scaly Healthy/intact Signs of Infection * 1 or more of these signs may indicate possible infection Heat * New slough/necrosis(deteriorating wound bed)* Increasing pain* Increasing exudate* Increasing odour* Friable granulation tissue* Treatment objectives (tick relevant box) Debridement Absorption Hydration Protection Palliative / conservative Reduce bacterial load Assessors Print Initials Dressing Renewed (planned or unplanned dressing change)
Re-assessment date
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 45 27/01/2017 10:09

45
Wound Treatment Plan and Evaluation of Care
To be completed when treatment or dressing type / regime altered NB Please write clearly
Date Wound
Number Cleansing Method, Dressing Choice & Rationale
Frequency
Evaluation & Rationale for changing dressing type
Signature
Packing Yes / No (circle) Amount …………………
Packing Yes / No (circle) Amount …………………
Packing Yes / No (circle) Amount …………………
Packing Yes / No (circle) Amount …………………
Packing Yes / No (circle) Amount …………………
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 46 27/01/2017 10:09
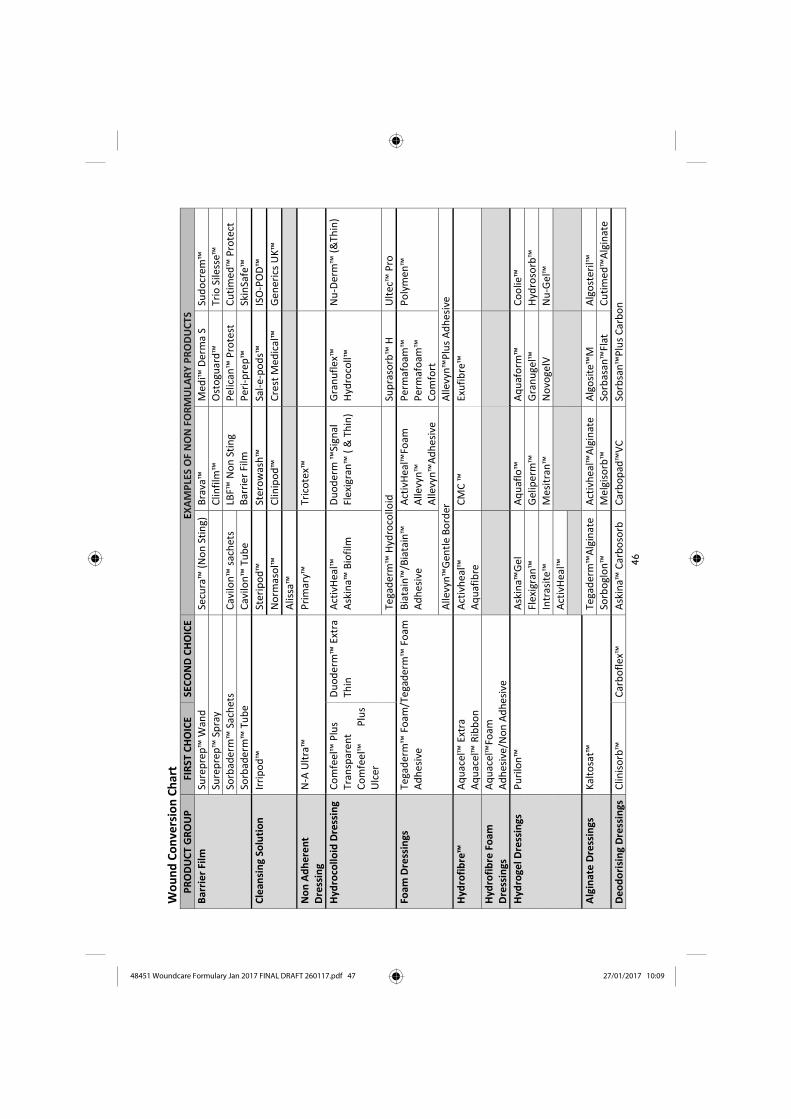
4
6
Wo
un
d C
on
vers
ion
Ch
art
PR
OD
UC
T G
RO
UP
FI
RST
CH
OIC
E SE
CO
ND
CH
OIC
E E X
AMPL
ES O
F N
ON
FO
RMU
LARY
PRO
DU
CTS
Bar
rie
r Fi
lm
Sure
pre
p™
Wan
d
Secu
ra™
(N
on
Sti
ng)
B
rava
™
Med
i™ D
erm
a S
Sud
ocr
em™
Sure
pre
p™
Sp
ray
C
linfi
lm™
O
sto
guar
d™
Tr
io S
iless
e™
Sorb
ader
m™
Sac
het
s C
avilo
n™
sac
het
s LB
F™ N
on
Sti
ng
Bar
rie
r Fi
lm
Pe
lican
™ P
rote
st
Cu
tim
ed™
Pro
tect
Sorb
ader
m™
Tu
be
Cav
ilon
™ T
ub
e P
eri
-pre
p™
Sk
inSa
fe™
Cle
ansi
ng
Solu
tio
n
Irri
po
d™
St
erip
od
™
Ster
ow
ash
™
Sal-
e-p
od
s™
ISO
-PO
D™
No
rmas
ol™
C
linip
od
™
Cre
st M
edic
al™
G
ener
ics
UK
™
Alis
sa™
No
n A
dh
ere
nt
Dre
ssin
g N
-A U
ltra
™
Pri
mar
y™
Tric
ote
x™
Hyd
roco
lloid
Dre
ssin
g C
om
fee
l™ P
lus
Tr
ansp
are
nt
Co
mfe
el™
P
lus
Ulc
er
Du
od
erm
™ E
xtra
Th
in
Act
ivH
eal™
A
skin
a™ B
iofi
lm
Du
od
erm
™Si
gnal
Fl
exi
gran
™ (
& T
hin
) G
ran
ufl
ex™
H
ydro
coll™
N
u-D
erm
™ (
&Th
in)
Tega
der
m™
Hyd
roco
lloid
Su
pra
sorb
™ H
U
ltec
™ P
ro
Foam
Dre
ssin
gs
Tega
der
m™
Fo
am/T
ega
der
m™
Fo
am
Ad
hes
ive
Bia
tain
™/B
iata
in™
A
dh
esiv
e A
ctiv
Hea
l™Fo
am
Alle
vyn
™
Alle
vyn
™A
dh
esiv
e
Pe
rmaf
oam
™
Pe
rmaf
oam
™
Co
mfo
rt
Po
lym
en™
Alle
vyn
™G
entl
e B
ord
er
Alle
vyn
™P
lus
Ad
hes
ive
Hyd
rofi
bre
™
Aq
uac
el™
Ext
ra
Aq
uac
el™
Rib
bo
n
Act
ivh
eal™
A
qu
afib
re
CM
C ™
Ex
ufi
bre
™
Hyd
rofi
bre
Fo
am
Dre
ssin
gs
Aq
uac
el™
Foam
A
dh
esiv
e/N
on
Ad
hes
ive
Hyd
roge
l Dre
ssin
gs
Pu
rilo
n™
A
skin
a™G
el
Aq
uaf
lo™
A
qu
afo
rm™
C
oo
lie™
Fle
xigr
an™
G
elip
erm
™
Gra
nu
gel™
H
ydro
sorb
™
In
tras
ite™
M
esit
ran
™
No
voge
lV
Nu
-Gel
™
Act
ivH
eal™
Alg
inat
e D
ress
ings
K
alto
sat™
Te
gad
erm
™A
lgin
ate
Act
ivh
eal™
Alg
inat
e A
lgo
site
™M
A
lgo
ster
il™
So
rbo
glo
n™
M
elgi
sorb
™
Sorb
asan
™Fl
at
Cu
tim
ed™
Alg
inat
e
De
od
ori
sin
g D
ress
ings
C
linis
orb
™
Car
bo
flex
™
Ask
ina™
Car
bo
sorb
C
arb
op
ad™
VC
So
rbsa
n™
Plu
s C
arb
on
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 47 27/01/2017 10:09

4
7
Sili
con
e D
ress
ings
A
llevy
n™
Gen
tle
Bo
rder
Ad
hes
ive
A
llevy
n™
Gen
tle
Alle
vyn
™ G
entl
e B
ord
er L
ite
Mep
itel
™O
ne
Alle
yvn
™Li
fe
Silf
lex™
Si
lon
-TSR
™
Mep
ilex™
A
skin
a™Si
lNet
M
epile
x™Tr
ansf
er
Mep
ilex™
Bo
rder
M
epit
el™
C
uti
med
™Si
ltec
Lite
Sili
con
e D
ress
ings
M
epile
x™Li
te
Alle
vyn
™ G
entl
e Li
te
Klin
ider
m™
Lite
A
dva
zorb
™ S
ilfix
Lit
e
Ad
vazo
rb™
Bo
rder
Lit
e B
iata
in™
Sili
con
e Li
te
Sup
er
Ab
sorb
en
t D
ress
ings
K
linid
erm
™
Ecly
pse
™
Fliv
aso
rb™
Ec
lyp
se™
Ad
hes
ive
Mes
orb
™
Fliv
aso
rb™
A
dh
esiv
e Ec
lyp
se™
Bo
ot
Zetu
vit™
E™-E
K
erra
max
™
Silv
er C
on
tain
ing
Dre
ssin
gs
Aq
uac
el™
Extr
a A
g+
Mel
giso
rb™
Ag
Ask
ina™
Cal
gitr
ol A
g A
ctic
oat
™Fl
ex
3
Act
ico
at™
Fle
x 7
A
ctic
oat
™M
ois
ture
A
ctis
orb
™Si
lver
A
lgis
ite™
Ag
Alle
vyn
™A
g
Bia
tian
™A
g A
trau
man
™A
g M
epile
x™A
b
Ph
ysio
tulle
™A
g
Po
lym
en™
Silv
er
Silv
erce
l™&
N/A
So
rbsa
n™
Silv
er
Urg
oce
ll™Si
lver
Urg
oso
rb™
Silv
er
Urg
otu
l™Si
lver
Te
gad
erm
™A
lgin
ate
Ag
An
tim
icro
bia
l D
ress
ings
C
uti
med
™ S
orb
act
Gel
C
uti
med
™ S
orb
act
Swab
s C
uti
med
™ S
orb
act
Hyd
roac
tive
Ho
ne
y P
rep
arat
ion
s M
edih
on
ey™
Tulle
A
ctiv
on
™ T
ulle
M
edih
on
ey™
Alg
inat
e
Act
ilite
™
A
lgiv
on
™
M
esit
ran
™
Iod
ine
Co
nta
inin
g P
rep
arat
ion
s In
adin
e™
Iod
ofl
ex™
Io
do
sorb
™
Iod
ozy
me™
O
xyzy
me™
An
tim
icro
bia
l A
lgin
ate
Gel
Fl
amin
al™
Fo
rte
Flam
inal
™H
ydro
Pai
n M
anag
em
en
t D
ress
ings
A
ctif
orm
Co
ol™
H
ydro
sro
rb™
K
erra
lire™
B
iata
in™
IBU
De
bri
de
me
nt
D
ebri
soft
Pad
™
Deb
riso
ft ™
Lo
lly
UC
S W
ipe
Tu
lle D
ress
ings
U
rgo
tul™
P
hys
iotu
lle™
P
arag
uaz
e™
Wo
un
d C
on
tact
Lay
er
Mep
itel
™
Silif
lex™
A
dap
tic™
Tou
ch
Mep
itel
™O
ne
Cu
tice
ll™
Cu
tim
ed™
Silt
ec
Ask
ina™
SilN
et
Act
ivh
eal™
48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdf 48 27/01/2017 10:09

Prinect PDF Report 3.1.098 - 1 - 01/27/2017 10:36:48 AM
Document overviewFile name: 48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdfLocation: E:\PTJobs\Jobs\48001_48500\48451_FHB Wound Care 48pp\Sy stem\Pagefiles\CurrentTitle: NHS Fife Woundcare GuidelinesCreator: Microsoft® Word 2013Producer: Microsoft® Word 2013Author: David MitchellCreation Date: 01/27/2017 09:57:55 AMModification Date: 01/27/2017 10:36:42 AMFile size: 7.2 MByte / 7378.1 KByteTrapped: UnknownOutput Intent: -PDF/X Version: -PDF Version: 1.5Number of pages: 48Media Box: 210.00 x 297.00 mmTrim Box: 148.00 x 210.00 mm
Summary Error Warning Fixed InfoDocument - 1 - -PDF/X - - - -Pages - - - -Colors - - - 42Fonts - 524 110 -Images - 18 - -Content - 6 35 -
DocumentPDF Version 1.5 is below 1.6
ColorsColor space: Device RGB (1-4,6-28,30-39,41-44,46)
FontsCourier is used inside trim box (2)CourierNewPSMT is used inside trim box (28)Arial: Font size 3.6 pt is below 6.0 pt (44)Arial: Font size 4.2 pt is below 6.0 pt (44)Arial: Font size 5.7 pt is below 6.0 pt (29,44)ArialMT: Font size 5.7 pt is below 6.0 pt (44)Calibri: Font size 2.1 pt is below 6.0 pt (30)Calibri: Font size 2.8 pt is below 6.0 pt (30)Calibri: Font size 3.6 pt is below 6.0 pt (13,18)Calibri: Font size 4.2 pt is below 6.0 pt (37)Calibri: Font size 4.9 pt is below 6.0 pt (13,18,29)Calibri: Font size 5.7 pt is below 6.0 pt (3,29,31,36)SymbolMT: Font size 5.7 pt is below 6.0 pt (29)

Prinect PDF Report 3.1.098 - 2 - 01/27/2017 10:36:48 AM
Arial,Bold: Font size 3.6 pt is below 6.0 pt (44)Arial,Bold: Font size 4.2 pt is below 6.0 pt (44)Arial,Bold: Font size 5.7 pt is below 6.0 pt (28-29,44)ComicSansMS: Font size 2.1 pt is below 6.0 pt (30)ComicSansMS: Font size 2.8 pt is below 6.0 pt (30)ComicSansMS: Font size 4.2 pt is below 6.0 pt (13)ComicSansMS: Font size 4.9 pt is below 6.0 pt (28)Arial,Italic: Font size 5.7 pt is below 6.0 pt (45)Arial-BoldMT: Font size 5.7 pt is below 6.0 pt (29)Calibri-Bold: Font size 0.3 pt is below 6.0 pt (35)Calibri-Bold: Font size 0.7 pt is below 6.0 pt (18)Calibri-Bold: Font size 2.8 pt is below 6.0 pt (30)Calibri-Bold: Font size 3.6 pt is below 6.0 pt (35)Calibri-Bold: Font size 4.2 pt is below 6.0 pt (35)Calibri-Bold: Font size 5.7 pt is below 6.0 pt (29)Arial,BoldItalic: Font size 5.7 pt is below 6.0 pt (45)Black font Arial (5.7 pt) is knockout (44)Black font Arial (8.5 pt) is knockout (6,9,13-15,28)Black font ArialMT (5.7 pt) is knockout (44)Black font Calibri (3.6 pt) is knockout (13,18)Black font Calibri (4.2 pt) is knockout (37)Black font Calibri (4.9 pt) is knockout (13,18)Black font Calibri (5.7 pt) is knockout (3,31,36)Black font Calibri (6.4 pt) is knockout (36)Black font Calibri (7.0 pt) is knockout (2,33,35)Black font Calibri (7.8 pt) is knockout (2,39)Black font Calibri (8.5 pt) is knockout (3-4,6-9,13-22,24-28,30-39,41-43)Black font Calibri (9.9 pt) is knockout (14,42)Black font Courier (7.8 pt) is knockout (2)Black font SymbolMT (8.5 pt) is knockout (6,13-15,28)Black font Arial,Bold (5.7 pt) is knockout (28,44)Black font ComicSansMS (4.2 pt) is knockout (13)Black font ComicSansMS (4.9 pt) is knockout (28)Black font ComicSansMS (6.4 pt) is knockout (2,42)Black font ComicSansMS (7.0 pt) is knockout (4,7,15-17,20,22,27,30-33,36,38,42,44)Black font ComicSansMS (7.8 pt) is knockout (31)Black font ComicSansMS (8.5 pt) is knockout (19,34)Black font Calibri-Bold (0.3 pt) is knockout (35)Black font Calibri-Bold (0.7 pt) is knockout (18)Black font Calibri-Bold (3.6 pt) is knockout (35)Black font Calibri-Bold (4.2 pt) is knockout (35)Black font Calibri-Bold (7.8 pt) is knockout (2,31,46)Black font Calibri-Bold (8.5 pt) is knockout (3-4,7-9,13-28,30-39,42-43)Black font Calibri-Bold (9.9 pt) is knockout (2-4,6,9,13-15,18,20-22,27-28,30-38,42-43)Black font Candara-Bold (8.5 pt) is knockout (17,37-38)Black font Calibri-Italic (8.5 pt) is knockout (19-20,28,33-36,38,41-42)

Prinect PDF Report 3.1.098 - 3 - 01/27/2017 10:36:48 AM
Black font CourierNewPSMT (8.5 pt) is knockout (28)Black font ComicSansMS-Bold (7.0 pt) is knockout (28)Black font ComicSansMS-Bold (7.8 pt) is knockout (14)Black font ComicSansMS-Bold (8.9 pt) is knockout (34)Black font ComicSansMS-Bold (9.9 pt) is knockout (46)Black font Calibri-BoldItalic (8.5 pt) is knockout (18-21,25,30,33-38)Black font TimesNewRoman,Bold (8.5 pt) is knockout (14,20)Black font TimesNewRoman,Bold (9.9 pt) is knockout (14)Arial: TrueType font (5-7,9,13-15,28-29,35-36,42,44,46)Tahoma: TrueType font (6,41-42)Calibri: TrueType font (1-43,45,47-48)Courier: TrueType font (2)SegoeUI: TrueType font (41)Arial,Bold: TrueType font (28-29,44-46)ComicSansMS: TrueType font (2-48)Arial,Italic: TrueType font (42,44-45)Calibri-Bold: TrueType font (1-9,11,13-44,46-48)Candara-Bold: TrueType font (17,37-38)TimesNewRoman: TrueType font (1,3-48)Calibri-Italic: TrueType font (5-6,19-21,23,28,33-36,38,41-42)CourierNewPSMT: TrueType font (28)Arial,BoldItalic: TrueType font (45)ComicSansMS-Bold: TrueType font (14,19,28,34,41,44-46)Calibri-BoldItalic: TrueType font (18-27,30,32-38)TimesNewRoman,Bold: TrueType font (14,20)Verdana-BoldItalic: TrueType font (30)ArialMT: TrueType CID font (29,44)Calibri: TrueType CID font (2-3,5-6,11,13,15,21,28-30,35-36,40-41,47-48)SymbolMT: TrueType CID font (5-7,13-15,28-29)ComicSansMS: TrueType CID font (44)Arial-BoldMT: TrueType CID font (29)Calibri-Bold: TrueType CID font (17,21,34,36,38,43-44,46-47)Calibri-Italic: TrueType CID font (28)Arial: Font is not embedded (5-7,9,13-15,28-29,35-36,42,44,46)Arial,Bold: Font is not embedded (28-29,44-46)Arial,Italic: Font is not embedded (42,44-45)TimesNewRoman: Font is not embedded (1,3-48)Arial,BoldItalic: Font is not embedded (45)TimesNewRoman,Bold: Font is not embedded (14,20)Calibri and Tahoma have the same unique identifierCalibri and Calibri have the same unique identifierCalibri and Courier have the same unique identifierCalibri and ComicSansMS have the same unique identifierComicSansMS and SegoeUI have the same unique identifierCalibri and Calibri-Bold have the same unique identifierCalibri and Candara-Bold have the same unique identifier

Prinect PDF Report 3.1.098 - 4 - 01/27/2017 10:36:48 AM
Calibri and Calibri-Italic have the same unique identifierCalibri and CourierNewPSMT have the same unique identifierCalibri and ComicSansMS-Bold have the same unique identifierCalibri and MyriadPro-Regular have the same unique identifierCalibri and Calibri-BoldItalic have the same unique identifierComicSansMS and Verdana-BoldItalic have the same unique identifier
ImagesColor image resolution 35 dpi is below 220 dpi (11,14)Color image resolution 97 dpi is below 220 dpi (11)Color image resolution 102 dpi is below 220 dpi (11)Color image resolution 136 dpi is below 220 dpi (44)Color image resolution 137 dpi is below 220 dpi (12)Color image resolution 140 dpi is below 220 dpi (44)Color image resolution 142 dpi is below 220 dpi (10)Color image resolution 150 dpi is below 220 dpi (44)Color image resolution 195 dpi is below 220 dpi (1)Color image resolution 205 dpi is below 220 dpi (14)Bitmap resolution 462 dpi is below 800 dpi (28)Images using lossy JPEG compression are present (10-12,14)1-bit image (28)4-bit image (1)
ContentTransparency is present (11,14,28,30,32,44)Line weight 0.030 mm is below hairline threshold 0.051 mm (8,13,16-27,29-39,47-48)Action, JavaScript or Annotation within printable area (6-7,9,15-16,41-43)
Additional informationColor separations: 4
CMYK
Color spacesDeviceCMYK / DeviceGray / SeparationDeviceRGB
Fonts: 37Arial TrueType / WinAnsi / embeddedArial,Bold TrueType / WinAnsi / embeddedArial,BoldItalic TrueType / WinAnsi / embeddedArial,Italic TrueType / WinAnsi / embeddedArial-BoldMT TrueType (CID) / Identity-H / embeddedArialMT TrueType (CID) / Identity-H / embeddedCalibri (4x) TrueType / WinAnsi / embedded subsetCalibri (4x) TrueType (CID) / Identity-H / embedded subsetCalibri-Bold (3x) TrueType / WinAnsi / embedded subsetCalibri-Bold TrueType (CID) / Identity-H / embedded subsetCalibri-BoldItalic TrueType / WinAnsi / embedded subset

Prinect PDF Report 3.1.098 - 5 - 01/27/2017 10:36:48 AM
Calibri-Italic TrueType / WinAnsi / embedded subsetCalibri-Italic TrueType (CID) / Identity-H / embedded subsetCandara-Bold TrueType / WinAnsi / embedded subsetComicSansMS (2x) TrueType / WinAnsi / embedded subsetComicSansMS TrueType (CID) / Identity-H / embedded subsetComicSansMS-Bold TrueType / WinAnsi / embedded subsetCourier (2x) TrueType / WinAnsi / embedded subsetCourierNewPSMT TrueType / WinAnsi / embedded subsetMyriadPro-Regular Type1 / WinAnsi / embeddedMyriadPro-Regular Type1 / WinAnsi / embedded subsetSegoeUI TrueType / WinAnsi / embedded subsetSymbolMT TrueType (CID) / Identity-H / embeddedTahoma TrueType / WinAnsi / embedded subsetTimesNewRoman TrueType / WinAnsi / embeddedTimesNewRoman,Bold TrueType / WinAnsi / embeddedVerdana-BoldItalic TrueType / WinAnsi / embedded subset

Prinect PDF Report 3.1.098 - 1 - 01/30/2017 11:54:54 AM
Document overviewFile name: 48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdfLocation: E:\PTShare\PDF StoreTitle: NHS Fife Woundcare GuidelinesCreator: Microsoft® Word 2013Producer: Microsoft® Word 2013Author: David MitchellCreation Date: 01/27/2017 09:57:55 AMModification Date: 01/30/2017 11:53:55 AMFile size: 8.5 MByte / 8667.8 KByteTrapped: NoOutput Intent: -PDF/X Version: -PDF Version: 1.6Number of pages: 48Media Box: 210.00 x 297.00 mm / 148.00 x 210.00 mmTrim Box: 148.00 x 210.00 mm
Summary Error Warning Fixed InfoDocument - - - -PDF/X - - - -Pages - - 1 -Colors - 4 - -Fonts - 511 98 -Images - 14 - -Content - 4 - -
PagesTrim box is not set directly or identical to media box (10)
ColorsColor space: Device CMYK is overprinting (26,31-32,34)
FontsCourier is used inside trim box (2)CourierNewPSMT is used inside trim box (28)Arial: Font size 3.6 pt is below 6.0 pt (44)Arial: Font size 4.2 pt is below 6.0 pt (44)Arial: Font size 5.7 pt is below 6.0 pt (29,44)ArialMT: Font size 5.5 pt is below 6.0 pt (10)ArialMT: Font size 5.7 pt is below 6.0 pt (10,44)Calibri: Font size 2.1 pt is below 6.0 pt (30)Calibri: Font size 2.8 pt is below 6.0 pt (30)Calibri: Font size 3.6 pt is below 6.0 pt (13,18)Calibri: Font size 4.2 pt is below 6.0 pt (37)Calibri: Font size 4.9 pt is below 6.0 pt (13,18,29)Calibri: Font size 5.7 pt is below 6.0 pt (3,29,31,36)SymbolMT: Font size 5.7 pt is below 6.0 pt (29)

Prinect PDF Report 3.1.098 - 2 - 01/30/2017 11:54:54 AM
Arial,Bold: Font size 3.6 pt is below 6.0 pt (44)Arial,Bold: Font size 4.2 pt is below 6.0 pt (44)Arial,Bold: Font size 5.7 pt is below 6.0 pt (28-29,44)ComicSansMS: Font size 2.1 pt is below 6.0 pt (30)ComicSansMS: Font size 2.8 pt is below 6.0 pt (30)ComicSansMS: Font size 4.2 pt is below 6.0 pt (13)ComicSansMS: Font size 4.9 pt is below 6.0 pt (28)Arial,Italic: Font size 5.7 pt is below 6.0 pt (45)Arial-BoldMT: Font size 5.5 pt is below 6.0 pt (10)Arial-BoldMT: Font size 5.7 pt is below 6.0 pt (29)Calibri-Bold: Font size 0.3 pt is below 6.0 pt (35)Calibri-Bold: Font size 0.7 pt is below 6.0 pt (18)Calibri-Bold: Font size 2.8 pt is below 6.0 pt (30)Calibri-Bold: Font size 3.6 pt is below 6.0 pt (35)Calibri-Bold: Font size 4.2 pt is below 6.0 pt (35)Calibri-Bold: Font size 5.7 pt is below 6.0 pt (29)Arial,BoldItalic: Font size 5.7 pt is below 6.0 pt (45)MyriadPro-Regular: Font size 3.7 pt is below 6.0 pt (10)Black font Arial (5.7 pt) is knockout (44)Black font Arial (8.5 pt) is knockout (6,9,13-15,28)Black font ArialMT (5.5 pt) is knockout (10)Black font ArialMT (5.7 pt) is knockout (10,44)Black font ArialMT (6.0 pt) is knockout (10)Black font Calibri (3.6 pt) is knockout (13,18)Black font Calibri (4.2 pt) is knockout (37)Black font Calibri (4.9 pt) is knockout (13,18)Black font Calibri (5.7 pt) is knockout (3,36)Black font Calibri (6.4 pt) is knockout (36)Black font Calibri (7.0 pt) is knockout (2,33,35)Black font Calibri (7.8 pt) is knockout (2,39)Black font Calibri (8.5 pt) is knockout (3-4,6-9,13-22,24-25,27-28,30,33,35-39,41-43,47)Black font Calibri (9.9 pt) is knockout (14,42)Black font Courier (7.8 pt) is knockout (2)Black font SymbolMT (8.5 pt) is knockout (6,13-15,28)Black font Arial,Bold (5.7 pt) is knockout (28,44)Black font Arial-Black (6.0 pt) is knockout (10)Black font ComicSansMS (4.2 pt) is knockout (13)Black font ComicSansMS (4.9 pt) is knockout (28)Black font ComicSansMS (6.4 pt) is knockout (2,42)Black font ComicSansMS (7.0 pt) is knockout (4,7,14-17,20,22,27,30,33,36,38,42,44)Black font ComicSansMS (8.5 pt) is knockout (19)Black font Arial-BoldMT (5.5 pt) is knockout (10)Black font Arial-BoldMT (6.0 pt) is knockout (10)Black font Arial-BoldMT (7.0 pt) is knockout (10)Black font Arial-BoldMT (8.0 pt) is knockout (10)Black font Calibri-Bold (0.3 pt) is knockout (35)

Prinect PDF Report 3.1.098 - 3 - 01/30/2017 11:54:54 AM
Black font Calibri-Bold (0.7 pt) is knockout (18)Black font Calibri-Bold (3.6 pt) is knockout (35)Black font Calibri-Bold (4.2 pt) is knockout (35)Black font Calibri-Bold (7.8 pt) is knockout (2,46)Black font Calibri-Bold (8.5 pt) is knockout (3-4,7-9,13-25,27-28,30,33,35-39,42-43,47)Black font Calibri-Bold (9.9 pt) is knockout (2-4,6,9,13-15,18,20-22,27-28,30,33,35-38,42-...Black font Candara-Bold (8.5 pt) is knockout (17,37-38)Black font Calibri-Italic (8.5 pt) is knockout (19-20,28,33,35-36,38,41-42)Black font CourierNewPSMT (8.5 pt) is knockout (28)Black font MyriadPro-Bold (7.0 pt) is knockout (10)Black font ComicSansMS-Bold (7.0 pt) is knockout (28)Black font ComicSansMS-Bold (7.8 pt) is knockout (14)Black font ComicSansMS-Bold (9.9 pt) is knockout (46)Black font Calibri-BoldItalic (8.5 pt) is knockout (18-21,25,30,33,35-38)Black font TimesNewRoman,Bold (8.5 pt) is knockout (14,20)Black font TimesNewRoman,Bold (9.9 pt) is knockout (14)Arial: TrueType font (5-7,9,13-15,28-29,35-36,42,44,46)Tahoma: TrueType font (6,41-42)ArialMT: TrueType font (10,44)Calibri: TrueType font (1-9,11-43,45,47-48)Courier: TrueType font (2)SegoeUI: TrueType font (41)Arial,Bold: TrueType font (28-29,44-46)Arial-Black: TrueType font (10)ComicSansMS: TrueType font (2-9,12-13,15-27,29,31,33-43,45-48)Arial,Italic: TrueType font (42,44-45)Arial-BoldMT: TrueType font (10)Calibri-Bold: TrueType font (1-9,11,13-44,46-48)Candara-Bold: TrueType font (17,37-38)TimesNewRoman: TrueType font (1,3-9,11-25,27-30,32-33,35-48)Calibri-Italic: TrueType font (5-6,19-21,23,28,33-36,38,41-42)Arial,BoldItalic: TrueType font (45)ComicSansMS-Bold: TrueType font (19,41,45-46)Calibri-BoldItalic: TrueType font (18-27,30,32-38)TimesNewRoman,Bold: TrueType font (14,20)ArialMT: TrueType CID font (29,44)Calibri: TrueType CID font (2-3,5-6,13,15,21,29,35-36,40-41,47-48)SymbolMT: TrueType CID font (5-7,13-15,28-29)ComicSansMS: TrueType CID font (11,14,28,30,32,44)Arial-BoldMT: TrueType CID font (29)Calibri-Bold: TrueType CID font (17,21,34,36,38,43,46-47)CourierNewPSMT: TrueType CID font (28)ComicSansMS-Bold: TrueType CID font (14,28,44)Verdana-BoldItalic: TrueType CID font (30)Arial: Font is not embedded (5-7,9,13-15,28-29,35-36,42,44,46)Arial,Italic: Font is not embedded (42,44-45)

Prinect PDF Report 3.1.098 - 4 - 01/30/2017 11:54:54 AM
TimesNewRoman: Font is not embedded (1,3-9,11-25,27-30,32-33,35-48)Arial,BoldItalic: Font is not embedded (45)ArialMT and ArialMT have the same unique identifierCalibri and Calibri have the same unique identifierArialMT and ComicSansMS have the same unique identifierCalibri and Calibri-Bold have the same unique identifierComicSansMS and SymbolMT have the same unique identifierArial,Bold and Arial,Bold have the same unique identifierCalibri-Italic and SymbolMT have the same unique identifierArialMT and ComicSansMS-Bold have the same unique identifierCalibri-Bold and Calibri-Bold have the same unique identifierComicSansMS and ComicSansMS-Bold have the same unique identifierCalibri-Italic and Calibri-Italic have the same unique identifierCalibri-Italic and CourierNewPSMT have the same unique identifierComicSansMS and TimesNewRoman,Bold have the same unique identifierMyriadPro-Regular and MyriadPro-Regular have the same unique identifierCalibri-BoldItalic and Calibri-BoldItalic have the same unique identifierCalibri-BoldItalic and Verdana-BoldItalic have the same unique identifier
ImagesColor image resolution 96 dpi is below 220 dpi (11,14)Color image resolution 97 dpi is below 220 dpi (11)Color image resolution 102 dpi is below 220 dpi (11)Color image resolution 136 dpi is below 220 dpi (44)Color image resolution 137 dpi is below 220 dpi (12)Color image resolution 140 dpi is below 220 dpi (44)Color image resolution 150 dpi is below 220 dpi (44)Color image resolution 195 dpi is below 220 dpi (1)Color image resolution 197 dpi is below 220 dpi (10)Color image resolution 205 dpi is below 220 dpi (14)Bitmap resolution 462 dpi is below 800 dpi (28)1-bit image (28)4-bit image (1)
ContentObject requires PostScript Level 3 (14,28,30,32)
Additional informationColor separations: 4
CMYK
Color spacesDeviceCMYK / DeviceGray / Separation
Fonts: 97Arial (5x) TrueType / WinAnsi / embeddedArial,Bold (3x) TrueType / WinAnsi / embedded subsetArial,BoldItalic TrueType / WinAnsi / embedded

Prinect PDF Report 3.1.098 - 5 - 01/30/2017 11:54:54 AM
Arial,Italic (2x) TrueType / WinAnsi / embeddedArial-Black TrueType / WinAnsi / embedded subsetArial-BoldMT TrueType (CID) / Identity-H / embeddedArial-BoldMT TrueType / WinAnsi / embedded subsetArialMT TrueType (CID) / Identity-H / embeddedArialMT (2x) TrueType / WinAnsi / embedded subsetArialMT TrueType (CID) / Identity-H / embedded subsetCalibri (14x) TrueType / WinAnsi / embedded subsetCalibri (4x) TrueType (CID) / Identity-H / embedded subsetCalibri-Bold (18x) TrueType / WinAnsi / embedded subsetCalibri-Bold TrueType (CID) / Identity-H / embedded subsetCalibri-BoldItalic (4x) TrueType / WinAnsi / embedded subsetCalibri-Italic (4x) TrueType / WinAnsi / embedded subsetCandara-Bold TrueType / WinAnsi / embedded subsetComicSansMS (2x) TrueType / WinAnsi / embedded subsetComicSansMS (7x) TrueType (CID) / Identity-H / embedded subsetComicSansMS-Bold TrueType / WinAnsi / embedded subsetComicSansMS-Bold (3x) TrueType (CID) / Identity-H / embedded subsetCourier (2x) TrueType / WinAnsi / embedded subsetCourierNewPSMT TrueType (CID) / Identity-H / embedded subsetMyriadPro-Bold (2x) Type1 / WinAnsi / embedded subsetMyriadPro-Regular Type1 / WinAnsi / embeddedMyriadPro-Regular (2x) Type1 / WinAnsi / embedded subsetSegoeUI TrueType / WinAnsi / embedded subsetSymbolMT TrueType (CID) / Identity-H / embeddedSymbolMT (2x) TrueType (CID) / Identity-H / embedded subsetTahoma TrueType / WinAnsi / embedded subsetTimesNewRoman (4x) TrueType / WinAnsi / embeddedTimesNewRoman,Bold (2x) TrueType / WinAnsi / embedded subsetVerdana-BoldItalic TrueType (CID) / Identity-H / embedded subset

Prinect PDF Report 3.1.098 - 1 - 01/30/2017 02:13:50 PM
Document overviewFile name: 48451 Woundcare Formulary Jan 2017 FINAL DRAFT 260117.pdfLocation: E:\PTShare\PDF StoreTitle: NHS Fife Woundcare GuidelinesCreator: Microsoft® Word 2013Producer: Microsoft® Word 2013Author: David MitchellCreation Date: 01/27/2017 09:57:55 AMModification Date: 01/30/2017 02:11:27 PMFile size: 8.9 MByte / 9111.3 KByteTrapped: NoOutput Intent: -PDF/X Version: -PDF Version: 1.6Number of pages: 48Media Box: 210.00 x 297.00 mm / 148.00 x 210.00 mmTrim Box: 148.00 x 210.00 mm
Summary Error Warning Fixed InfoDocument - - - -PDF/X - - - -Pages - - 1 -Colors - 4 - -Fonts - 490 71 -Images - 14 - -Content - 4 - -
PagesTrim box is not set directly or identical to media box (10)
ColorsColor space: Device CMYK is overprinting (26,31-32,34)
FontsCourier is used inside trim box (2)CourierNewPSMT is used inside trim box (28)Arial: Font size 3.6 pt is below 6.0 pt (44)Arial: Font size 4.2 pt is below 6.0 pt (44)Arial: Font size 5.7 pt is below 6.0 pt (29,44)ArialMT: Font size 5.5 pt is below 6.0 pt (10)ArialMT: Font size 5.7 pt is below 6.0 pt (10,44)Calibri: Font size 2.1 pt is below 6.0 pt (30)Calibri: Font size 2.8 pt is below 6.0 pt (30)Calibri: Font size 3.6 pt is below 6.0 pt (13,18)Calibri: Font size 4.2 pt is below 6.0 pt (37)Calibri: Font size 4.9 pt is below 6.0 pt (13,18,29)Calibri: Font size 5.7 pt is below 6.0 pt (3,29,31,36)SymbolMT: Font size 5.7 pt is below 6.0 pt (29)

Prinect PDF Report 3.1.098 - 2 - 01/30/2017 02:13:50 PM
Arial,Bold: Font size 3.6 pt is below 6.0 pt (44)Arial,Bold: Font size 4.2 pt is below 6.0 pt (44)Arial,Bold: Font size 5.7 pt is below 6.0 pt (29,44)ComicSansMS: Font size 2.1 pt is below 6.0 pt (30)ComicSansMS: Font size 2.8 pt is below 6.0 pt (30)ComicSansMS: Font size 4.2 pt is below 6.0 pt (13)Arial,Italic: Font size 5.7 pt is below 6.0 pt (45)Arial-BoldMT: Font size 5.5 pt is below 6.0 pt (10)Arial-BoldMT: Font size 5.7 pt is below 6.0 pt (29)Calibri-Bold: Font size 0.3 pt is below 6.0 pt (35)Calibri-Bold: Font size 0.7 pt is below 6.0 pt (18)Calibri-Bold: Font size 2.8 pt is below 6.0 pt (30)Calibri-Bold: Font size 3.6 pt is below 6.0 pt (35)Calibri-Bold: Font size 4.2 pt is below 6.0 pt (35)Calibri-Bold: Font size 5.7 pt is below 6.0 pt (29)Arial,BoldItalic: Font size 5.7 pt is below 6.0 pt (45)MyriadPro-Regular: Font size 3.7 pt is below 6.0 pt (10)Black font Arial (5.7 pt) is knockout (44)Black font Arial (8.5 pt) is knockout (6,9,13-15)Black font ArialMT (5.5 pt) is knockout (10)Black font ArialMT (5.7 pt) is knockout (10,44)Black font ArialMT (6.0 pt) is knockout (10)Black font Calibri (3.6 pt) is knockout (13,18)Black font Calibri (4.2 pt) is knockout (37)Black font Calibri (4.9 pt) is knockout (13,18)Black font Calibri (5.7 pt) is knockout (3,36)Black font Calibri (6.4 pt) is knockout (36)Black font Calibri (7.0 pt) is knockout (2,33,35)Black font Calibri (7.8 pt) is knockout (2,39)Black font Calibri (8.5 pt) is knockout (3-4,6-9,13-16,18-22,24-25,27,30,33,35-39,41-43,47)Black font Calibri (9.9 pt) is knockout (14,42)Black font Courier (7.8 pt) is knockout (2)Black font SymbolMT (8.5 pt) is knockout (6,13-15)Black font Arial,Bold (5.7 pt) is knockout (44)Black font Arial-Black (6.0 pt) is knockout (10)Black font ComicSansMS (4.2 pt) is knockout (13)Black font ComicSansMS (6.4 pt) is knockout (2,42)Black font ComicSansMS (7.0 pt) is knockout (4,7,14-16,20,22,27,30,33,36,38,42,44)Black font ComicSansMS (8.5 pt) is knockout (19)Black font Arial-BoldMT (5.5 pt) is knockout (10)Black font Arial-BoldMT (6.0 pt) is knockout (10)Black font Arial-BoldMT (7.0 pt) is knockout (10)Black font Arial-BoldMT (8.0 pt) is knockout (10)Black font Calibri-Bold (0.3 pt) is knockout (35)Black font Calibri-Bold (0.7 pt) is knockout (18)Black font Calibri-Bold (3.6 pt) is knockout (35)

Prinect PDF Report 3.1.098 - 3 - 01/30/2017 02:13:50 PM
Black font Calibri-Bold (4.2 pt) is knockout (35)Black font Calibri-Bold (7.8 pt) is knockout (2,46)Black font Calibri-Bold (8.5 pt) is knockout (3-4,7-9,13-16,18-25,27,30,33,35-39,42-43,47)Black font Calibri-Bold (9.9 pt) is knockout (2-4,6,9,13-15,18,20-22,27,30,33,35-38,42-43)Black font Candara-Bold (8.5 pt) is knockout (37-38)Black font Calibri-Italic (8.5 pt) is knockout (19-20,33,35-36,38,41-42)Black font MyriadPro-Bold (7.0 pt) is knockout (10)Black font ComicSansMS-Bold (7.8 pt) is knockout (14)Black font ComicSansMS-Bold (9.9 pt) is knockout (46)Black font Calibri-BoldItalic (8.5 pt) is knockout (18-21,25,30,33,35-38)Black font TimesNewRoman,Bold (8.5 pt) is knockout (14,20)Black font TimesNewRoman,Bold (9.9 pt) is knockout (14)Arial: TrueType font (5-7,9,13-15,29,35-36,42,44,46)Tahoma: TrueType font (6,41-42)ArialMT: TrueType font (10,44)Calibri: TrueType font (1-9,11-43,45,47-48)Courier: TrueType font (2)SegoeUI: TrueType font (41)Arial,Bold: TrueType font (29,44-46)Arial-Black: TrueType font (10)ComicSansMS: TrueType font (2-9,12-13,15-27,29,31,33-43,45-48)Arial,Italic: TrueType font (42,44-45)Arial-BoldMT: TrueType font (10)Calibri-Bold: TrueType font (1-9,11,13-44,46-48)Candara-Bold: TrueType font (17,37-38)TimesNewRoman: TrueType font (1,3-9,11-16,18-25,27,29-30,32-33,35-48)Calibri-Italic: TrueType font (5-6,19-21,23,28,33-36,38,41-42)Arial,BoldItalic: TrueType font (45)ComicSansMS-Bold: TrueType font (19,41,45-46)Calibri-BoldItalic: TrueType font (18-27,30,32-38)TimesNewRoman,Bold: TrueType font (14,20)ArialMT: TrueType CID font (29,44)Calibri: TrueType CID font (2-3,5-6,13,15,21,29,35-36,40-41,47-48)SymbolMT: TrueType CID font (5-7,13-15,28-29)ComicSansMS: TrueType CID font (11,14,28,30,32,44)Arial-BoldMT: TrueType CID font (29)Calibri-Bold: TrueType CID font (17,21,34,36,38,43,46-47)CourierNewPSMT: TrueType CID font (28)ComicSansMS-Bold: TrueType CID font (14,44)Verdana-BoldItalic: TrueType CID font (30)Arial: Font is not embedded (5-7,9,13-15,29,35-36,42,44,46)Arial,Italic: Font is not embedded (42,44-45)TimesNewRoman: Font is not embedded (1,3-9,11-16,18-25,27,29-30,32-33,35-48)Arial,BoldItalic: Font is not embedded (45)ArialMT and ComicSansMS have the same unique identifierCalibri and Calibri-Bold have the same unique identifier

Prinect PDF Report 3.1.098 - 4 - 01/30/2017 02:13:50 PM
ComicSansMS and SymbolMT have the same unique identifierCourierNewPSMT and SymbolMT have the same unique identifierArialMT and ComicSansMS-Bold have the same unique identifierCalibri-Bold and Calibri-Bold have the same unique identifierComicSansMS and ComicSansMS-Bold have the same unique identifier
ImagesColor image resolution 96 dpi is below 220 dpi (11,14)Color image resolution 97 dpi is below 220 dpi (11)Color image resolution 102 dpi is below 220 dpi (11)Color image resolution 136 dpi is below 220 dpi (44)Color image resolution 137 dpi is below 220 dpi (12)Color image resolution 140 dpi is below 220 dpi (44)Color image resolution 150 dpi is below 220 dpi (44)Color image resolution 195 dpi is below 220 dpi (1)Color image resolution 197 dpi is below 220 dpi (10)Color image resolution 205 dpi is below 220 dpi (14)Bitmap resolution 462 dpi is below 800 dpi (28)1-bit image (28)4-bit image (1)
ContentObject requires PostScript Level 3 (14,28,30,32)
Additional informationColor separations: 4
CMYK
Color spacesDeviceCMYK / DeviceGray / Separation
Fonts: 96Arial (4x) TrueType / WinAnsi / embeddedArial,Bold (3x) TrueType / WinAnsi / embedded subsetArial,BoldItalic TrueType / WinAnsi / embeddedArial,Italic (2x) TrueType / WinAnsi / embeddedArial-Black TrueType / WinAnsi / embedded subsetArial-BoldMT TrueType (CID) / Identity-H / embeddedArial-BoldMT TrueType / WinAnsi / embedded subsetArialMT TrueType (CID) / Identity-H / embeddedArialMT (2x) TrueType / WinAnsi / embedded subsetArialMT TrueType (CID) / Identity-H / embedded subsetCalibri (14x) TrueType / WinAnsi / embedded subsetCalibri (4x) TrueType (CID) / Identity-H / embedded subsetCalibri-Bold (17x) TrueType / WinAnsi / embedded subsetCalibri-Bold (2x) TrueType (CID) / Identity-H / embedded subsetCalibri-BoldItalic (3x) TrueType / WinAnsi / embedded subsetCalibri-Italic (4x) TrueType / WinAnsi / embedded subset

Prinect PDF Report 3.1.098 - 5 - 01/30/2017 02:13:50 PM
Candara-Bold TrueType / WinAnsi / embedded subsetComicSansMS (3x) TrueType / WinAnsi / embedded subsetComicSansMS (7x) TrueType (CID) / Identity-H / embedded subsetComicSansMS-Bold TrueType / WinAnsi / embedded subsetComicSansMS-Bold (2x) TrueType (CID) / Identity-H / embedded subsetCourier (2x) TrueType / WinAnsi / embedded subsetCourierNewPSMT TrueType (CID) / Identity-H / embedded subsetMyriadPro-Bold (2x) Type1 / WinAnsi / embedded subsetMyriadPro-Regular Type1 / WinAnsi / embeddedMyriadPro-Regular (2x) Type1 / WinAnsi / embedded subsetSegoeUI TrueType / WinAnsi / embedded subsetSymbolMT TrueType (CID) / Identity-H / embeddedSymbolMT (2x) TrueType (CID) / Identity-H / embedded subsetTahoma TrueType / WinAnsi / embedded subsetTimesNewRoman (5x) TrueType / WinAnsi / embeddedTimesNewRoman,Bold (2x) TrueType / WinAnsi / embedded subsetVerdana-BoldItalic TrueType (CID) / Identity-H / embedded subset