nine million lives - médecins sans frontières million lives is a collection of stories from the...
TRANSCRIPT


NINEMILLIONLIVES
Shortstoriesfromthefrontlinesofmedicalcrises
MEDECINSSANSFRONTIERES

PublishingDetailsNineMillionLivesbyMédecinsSansFrontières
©2015MédecinsSansFrontières
Contributors:KimComer,AdamSharp,StephenTorres,EstherClark,AnnSellberg,AbdulWassay,SteveCohen,JosineBlanksma,KellyHildebrand,AliAl-Ani,NatalieRoberts,AneBjøruFjeldsæter,BenGupta,WilliamTurner,FloraEscourrou,EmmaPedleyandAoibhinnWalsh
Themoralrightoftheauthorshasbeenasserted.Allrightsreserved.Withoutlimitingtherightsundercopyrightrestrictedabove,nopartofthispublicationmaybereproduced,storedinorintroducedintoaretrievalsystem,ortransmitted,inanyformorbyanymeans(electronic,mechanical,photocopying,recordingorotherwise),withoutthepriorwrittenpermissionofthecopyrightowner,exceptinthecaseofbriefquotationsincriticalarticlesorreviews.
MédecinsSansFrontièresAustralia
www.msf.org.au
EbookVersion1stEdition2015,ePubandMobi
Ebookcreation:Convertedfromdigitalsourcefile
Ebookfilescreatedby:AustralianeBookPublisherwww.AustralianEbookPublisher.com.au
FirstEdition:May2015

FOREWORD
NineMillionLivesisacollectionofstoriesfromtheworldofMédecinsSansFrontières,aworldwhichwouldnotexistwithoutthesupportofsomanyindividualsthatfundourwork.
Thestoriesareofhardship,injuryandillness,butalsoofcommitment,hopeand-ultimately-triumphoverthemostdifficultandchallengingcircumstancesimaginable.
Manyofthefirsthandaccountsresonatestronglywithme,butnonemoresothan“WavesofPatients”,writtenbyDrEstherSterkfollowingTyphoonHaiyaninThePhilippines.ItremindsmeofmyexperienceinHaitinotlongaftertheearthquakewhichravagedthecountryin2010.
Asourteamswenttoworkintheaftermathofthatdevastatingevent,wetreatedthewounded,distributedfood,waterandshelter,dealtwithoutbreaksofdisease,helpedwomentogivebirthandbabiestotaketheirfirstbreaths.Weevencreatedafunctioninghospitaloutofashippingcontainer.
IhadworkedwithMédecinsSansFrontièresfor13yearsatthattime,butneverhadIseensuchdevastation,norahumanitarianresponseonsuchanimmensescale.
Whetherourteamsaretreatingpatientsintheaftermathofnaturaldisasters-inplaceslikeHaiti,thePhilippinesandNepal-orrespondingtoepidemicslikethedeadlyEbolaoutbreakinWestAfrica,itisthankstothegenerosityofoursupportersthatMedécinsSansFrontièrescandelivermedicalassistancesoeffectively.
Sopleaseread,enjoyandsharethisbook.Thestoriesspeakforthemselves.
PaulMcPhunExecutiveDirectorMédecinsSansFrontièresAustralia

INTRODUCTION
NINEMILLION.That’sthenumberofpeopletreatedbyMédecinsSansFrontièresmedicalteamsaroundtheworldinayear.Itincludeswomeninlabour,childreninneedofvaccinations,thewar-wounded,patientsinjuredduringnaturaldisastersandmanyothers.Whilesomeofthemedicalemergenciesfacingthesepatientsmakethenews,manydon’t.
Thisbookgivesaglimpseintothelivesofafewdozenoftheninemillionpeoplethatwetreateachyear.Thesearethestoriesbehindtheheadlines,andtogethertheypaintacoherentpictureoftheworkofMédecinsSansFrontièresaroundtheworld.
Manychaptersarefirsthandaccountstakenfromourfieldworkers’blogs.Somearethirdpersonstoriesandothersareinterviews.Allreflectthedifficultiesofworkinginchallengingcircumstances,thecommitmentofourmedicalandlogisticalteamsandthestrengthandcourageofourpatients.
ThereisthestoryofaformerrefugeefromtheMiddleEastwhowenttoworkinSouthSudantoassistothervictimsofconflict;afirst-handaccountofthechallengesoftransportingmedicalequipmentthroughforestsanddifficultterrainintheDemocraticRepublicofCongo;andastoryaboutourteamssecuringcontinuityinhealthcareforpeoplelivinginasluminKenya.ThestoriesreflectthediversenatureofMédecinsSansFrontières’workandthepatientswetreat.
Toensurethattheirprivacyisprotected,allpatientnameshavebeenchangedthroughoutthisbook.
MédecinsSansFrontièrestreatsthevictimsofnaturaldisasters,conflict,epidemicsandothermedicalemergencies.Eachyear,millionsofpeopleareseenandtreatedbyover20,000fieldstaffinmorethan60countries.Throughthesestories,youwillmeetthedoctorsandnurses,logisticiansandfieldcoordinators,andthededicatednationalstaffwhocarryoutthiswork.Andyouwillhearabouthowthisvitalmedicalaidhelpspeopleinurgentneedeveryday.
THEPATIENTSKEEPCOMING
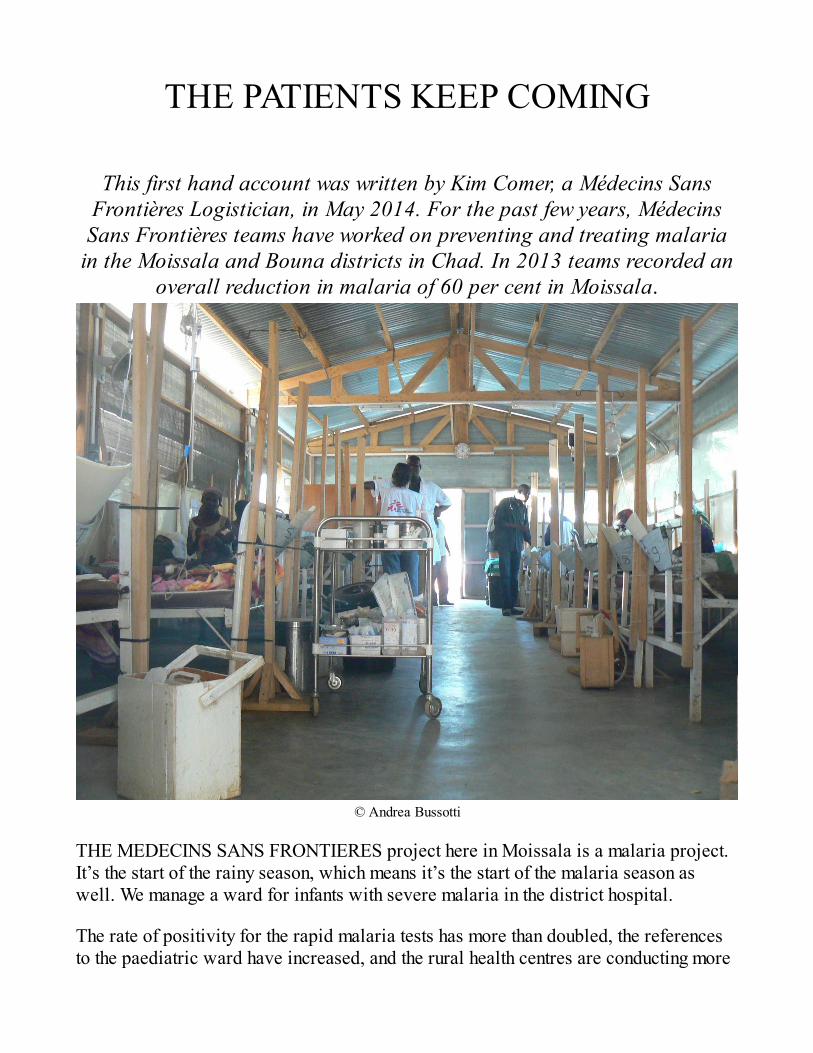
ThisfirsthandaccountwaswrittenbyKimComer,aMédecinsSansFrontièresLogistician,inMay2014.Forthepastfewyears,MédecinsSansFrontièresteamshaveworkedonpreventingandtreatingmalariaintheMoissalaandBounadistrictsinChad.In2013teamsrecordedan
overallreductioninmalariaof60percentinMoissala.
©AndreaBussotti
THEMEDECINSSANSFRONTIERESprojecthereinMoissalaisamalariaproject.It’sthestartoftherainyseason,whichmeansit’sthestartofthemalariaseasonaswell.Wemanageawardforinfantswithseveremalariainthedistricthospital.
Therateofpositivityfortherapidmalariatestshasmorethandoubled,thereferencestothepaediatricwardhaveincreased,andtheruralhealthcentresareconductingmore

consultations.Thepaediatricwardhasexpandedintooneoftheunusedbuildingsforthemalariaward,duetohighpatientvolume.Itistime.
Thelogisticsdepartmenthasbeenbusy.We’vebeenrepainting,repairingbeds,orderinginblankets,soapandmosquitonetsfordonationtoallpatients,andarrangingthefurnitureinthewards.We’rehalfwaythroughtherehabilitationofthehospital’swastearea,butithasremainedoperationalthroughout.
Ihavefourdaystoprioritiseandshuffleresourcesaround,andtogetreadyforaprovisionalopeningof30ofoureventual80beds.Thereareplentyoftrainingsanddeliveriestobedonebeforeopening,plustheusualactivityofsettingeverythingup.Thehospitalbuzzesallweekendwithlogisticalandmedicalteamsmovingeverythingintoplace,checkingequipment,photocopyingforms,hangingmosquitonets.
Mondaymorningat8amisthehoursetforopening.Afterourall-staffmeetingat7.30am,themedicsheadtotheward.Itieupsomelooseendsattheoffice(westillhaveafullrangeofexternalactivities,includingconstructingwasteareasatseveralruralhealthcentres),thenheadovertothehospital.Theteamhasdoneanincrediblejobwiththepreparations.Twenty-fivecrispbedslinethewallsofourthreerooms.Theadmissionsroomisorderedandstocked.Igreettheseveralnurses,hygienistsanddoctorswhoarethereandwetaketimetodiscussanyneedsorrequests.
Wehavenopatients.
Well,allofourindicatorswerestrong,soweknowthere’stheneedtohaveourwardopen,butasthehoursstretchbyandwedon’treceiveasinglepatient,westarttowonder.
Didwetellthehealthcentresthatwe’reopen?
Yes.
Dothepatientsknowhowtofindusatthehospital?
Yes.
Weird.
Fivedayslater,notonlyarewefull,butwe’veopenedtwonewroomswith10bedseach,andhaveafurther18newbedsinathirdbuilding.
Everybedisoccupiedwithasmallchildwithmalaria,withthemothercurledup

besidethem(mostofourpatientsareunderthreeyearsold).ThepatientsstartedarrivingonMondaynightandhaven’tstopped.Thenursesanddoctorsmovethroughthewardwithanefficientair,settingIVdripratesandtakingvitalsigns.It’sbusybutcontrolled.Theadmissionsroomismorehectic,sinceit’stheplaceforthefirstexaminationandinterventionbyourmedicalteam.Cryingchildrenanddistraughtmothersarereceivedherebeforebeingadmittedintothebusycalmofourward.
Thecommunicationbetweenthemedicalteamandthelogisticsteamisstrong,withrepairs,equipmentrequests,roomopeningsandmedicalwastemanagementallhappeningsmoothly.Thesystemsareinplace,andwecancontinuetogrowtoourcapacity.Thekitchenispreparinganddistributingmealsconsistentlyandreliably.Iturnmyattentionbacktothewasteareaandlatrinesthatarestillunderconstruction.
I’mhopingtofinishtheconstructionwithintheweek,becausearainshelterforallthemothersneedstobebuilt,andwe’relessthanamonthawayfromourfirstdistributionofmalariaprophylaxistothepopulationthroughoutthedistrict.
Andthepatientskeepcoming.

UNDERNEATHALLTHEDRAMA
AdamSharpworkedinSyriawithMédecinsSansFrontièresduringtheconflictthatbeganasprotestsin2011.Herehedescribestheimpactof
MédecinsSansFrontières’workonthepeoplethathemet.
©NicoleTung
THEFIRSTAMBULANCEarrivesbeforeweareready.Itisapick-uptruckcarryingtwowoundedmenfromthefrontlines,pallidandsemi-consciouslyingonmattressesintheback.Awaveofyoungmen-volunteersfromthesurroundingvillages-surgetowardsthetruckand20handsfloateachpatientontoastretcherandinsidetotheemergencyroom.
Adoctorquicklyseesthatoneofthewoundedmenneedsimmediateabdominalsurgery.Itisamassiveinjuryandthesurgerywillbecomplicated.Theman’schancesofsurvivalarefairatbest.
Williamarrivesat6.30am,onlyminutesafterthefirstwoundedmen.Heisasurgeon

with20yearsexperiencewithMédecinsSansFrontières,heissixfootfourandhasanaturallycalmdisposition-aganglyrockinthemiddleofthehecticbuzz.Withinfiveminutesheisoperatingontheinjuredman.
Anhourlater,everyonehasarrived:90localstaff-doctors,nurses,midwives,drivers,guards,clerksand12internationalstaff-mostlymedicalprofessionals,allworkingflatout.
Idonotknowtheoutcomeforthatfirstpatientthatmorning.Ilosttrackofhim,andcountlessothers,asinjuredmenandwomencontinuedtoarrive.Thesurgicalteamworkeduntil3amthenextday-theyworkedstraightthrough-andthiscontinuedforthebestpartoftwoweeks.Williamconductedover40moresurgeriesinthefollowingdaysand,ashetoldme,thehardestdayheeverhadasasurgeonwasthatfirstone.
Buthere’sthecatch.Thisisn’tthemostimportantworkthatMédecinsSansFrontièresisdoinginSyria.Thisisnotwherethemostlivesarebeingsaved,orwherethemostsufferingisbeingalleviated,orwherethemosthumandignityisbeingdefendedandupheld.
IwishIcouldwriteproperlyaboutthepeopleIhavemet,depictingtheirstorieswiththeinterest,fidelityandsensitivitythattheydeserve.ButinsteadIwillsaythatunderneathallofthisdrama-thebombsandthebloodshedandtheheadlines-thattherearepeople,justpeople,alltryingtolivetheirlivesandcontinuefromdaytoday.
Thesepeoplewanttotendtheirland,attendschool,lookafteragedparents,orgrowuptobecomedentists,electriciansorwriters.Theywanttogivebirth,findlove,findhappiness,seeksecurityfortheirfamily,orfindanewplacetolivenowthatababyisontheway.Theywanttodoallthethingsthatpeopledoallovertheworldeveryday.Butthisisacountryatwar.
AndthisiswhereMédecinsSansFrontièresismakingadifferencebyprovidinghealthcaretopeoplewherethehealthsystemhasevaporated,maternitycareforpregnantwomen,mentalhealthservicesforthebereaved,medicationforchronicillnesses,andantibioticsforsimpleinfections.
Theprovisionofhealthcaregenuinelyhelpspeoplemaintainsomecontrolanddignityintheirlives.ThehospitalsarestaffedbydedicatedSyrians,enabledbythepresenceofMédecinsSansFrontières-theequipment,medicationsandadditionalmedicalexpertisetheybring.Sowhilemanyliveshavebeensavedonasurgicaltable,MédecinsSansFrontièresisalsocoveringperhaps90percentofallhealthneedsforacatchmentpopulationofapproximately100,000people.

ADRENALINE
DrStephenTorresisanobstetrics/gynaecologyspecialist.Hereherecountsthestoryofababyhehelpeddeliverwhenworkingwith
MédecinsSansFrontièresinSierraLeonein2012.
©MSF
I’M58YEARSOLD.Ispent22yearsinprivatepracticeaftercompletingmytraininginobstetricsandgynaecology.IhopetospendthecomingyearsworkingwithMédecinsSansFrontièresinareasofneed.
MyfirstplacementwithMédecinsSansFrontièreswasin2012attheGondamaReferralCentreinBo,SierraLeone.Thisisareferralhospitalforpregnancycomplicationsandforpaediatrics.Iwanttosharewithyouapositivestoryfrommytimethere.
Iwenttobedataround2amandsleptforacoupleofhoursbutthenIreceivedanurgentphonecall.IhurriedovertothelabouranddeliverywardasquicklyasIcouldandfoundapatientwhohadjustarrivedbyambulance,pushing,withthebaby’sbuttockshalfwaydelivered.Thiswasherfirstbabyandbasedonthesizeofthebaby’sbuttocks,itwasn’tasmallkid.Therewasn’ttimetogetherbackforacaesareansoIputmyhat,

mask,eyeshields,apron,gown,anddoubleglovesoninrecordtimeandpreparedforabreechdelivery.Ifeltprettycalmthinkingoptimistically,“Whatcouldgowrong?”Well,everythingapparently.
Thebabydelivereduptoitshipsprettyeasily.Mumpushedagainandthebabydeliveredtheumbilicalcord.That’swhentheclockstartstickinginmyhead.Fromthatpointonthebaby’sumbilicalcordisbeingcompressedbetweenthebaby’sskullandthemum’spelvicbones,effectivelycuttingoffthedeliveryofoxygentothebaby.Wehadmumkeeppushingbutthebabydidn’tbudge.Irememberbeingtoldduringmyresidencyaboutvaginalbreechdeliveries,“Keepyourhandsoffuntilthebabyhasdelivereduptothescapulas(basicallyjustbelowtheshoulders.”Ikeptthatinmindandavoidedtryingtohelpthemotherbypullingonthebabyuntilanotherminutepassedandthebaby,whohadbeenkicking,startedgoinglimp.Icouldfeelthepulseintheumbilicalcordanditwasveryslow.Iputsometractiononthebaby’shipswhilehavingthemumpullherkneesasclosetoherchestaspossibletotryandgivethebabymoreroom-butthebabywasstuck.
I’veheardhorrorstoriesaboutbabiesthatdeliveruptotheheadandthengetstuckbutthat’soneofthosethingsyoualwaysthinkwillneverhappentoyou.Buthereitwashappening.OutofoptionsIdidtheonlythingIcoulddoandreachedupintothemotherandfoundthatbotharmsweretrappedabovethebaby’shead.Iwasabletogetonefingerpastthemum’spelvicbonesandhookedaroundthebaby’srightarmneartheelbowandtriedtopullthearmdown,bendingitattheelbow,butitwouldn’tmove.Ireallydon’tknowhowmuchtimehadpassedbythen.Itmayhaveonlybeenacoupleofminutesbutitseemedlikeaneternity.Iknewthatifsomethingdidn’thappenquicklytoimprovethesituationthebabywoulddiesoIpulledashardasIcouldonthatarm.
Ieventuallymanagedtogetthebaby’sheadout.ButthebabywasaslimpasaragandIcouldnolongerfeelapulseintheumbilicalcord.
Wemovedthebabyovertotheresuscitationtableandstartedresuscitatingthebaby.Iusedthebagandmasktoforceairintothebaby’slungswhilethenursestartedchestcompressions.
Nothing.
Werolledthebabytothesideandmassageditsback,slappeditsfeet,andthencontinuedbaggingandcompressing.
Stillnothing.
Themotherwaswailing,watchingus,helpless.Andthenthebabygasped.Itwasn’t

muchanditdidn’tlastlongbutitwasenoughtogiveushopeandwekeptworking,allthewhilewatchingthebaby’sduskybluecolourstarttolightenandthenturnintoamottledpaleandthenfinallyapinkishcolour.
Whenthebabyopeneditseyesandstartedcryingeveryoneintheroomjustlookedatthepersonnexttothem,eyeswideinsomethinglikedisbelief.Ithinkwhenyou’reusedtoseeingbabiesdie,watchingonecomebackfromthedeadisespeciallymiraculous.Themotherstartedcryingandchantingandwithinaminuteortwothebabywasscreamingitslungsout.
Itcould’vegoneeitherway.IhopethatIdon’tsomedayhavetotellastorylikethatbutwithadifferentending.
IwassohypeduponadrenalineafterwardsthatIdidn’tgobacktosleep.I’dbeeninBoforthreeweeksatthattimeandwasfindingitallalittlehardtobelieve.InsomewaysitfeltlikeIhadjustarrived,butinotherwaysitfeltlikeI’dbeentherealong,longtime.

WAVESOFPATIENTS

TyphoonHaiyan–PartI
DrEstherSterkisamedicaldoctorwhoarrivedinthePhilippinestoassistinMédecinsSansFrontières’responsetoTyphoonHaiyan.EstherassessedtheimmediateneedsinsomeoftheislandswestofCebu.ShedescribesherethefirstdaysofMédecinsSansFrontières’emergency
responseandherinitialimpressionsofthesituation.
©MSF
THEEASTERNPARTofPanayIslandhasbeenheavilyaffected.Insomevillages,80percentofthehouseshavebeenpartiallyorcompletelydestroyed.Alotofrooftopsandwallshavefallenorbeentornapart.Inmanycases,thewholehousehascompletelycollapsed.Ourteamarefocusingontheisolatedvillagesalongthecoastandonthesurroundingislands.Atthemomentwedonotknowifhealthcareisaccessibleandfunctioningthere,butmedicalfacilitiesarelikelytobedestroyed.
Peopletellusthattheyneeddrinkingwater,becausethelakeshavebecomesaltysincetheseawatersurged.Intheruralareasmanypeoplehavenomeansofsubsistenceastheircropshavebeendestroyed.Usually,thoselivingonsmallislandstravelfromoneislandtoanotherbyboat,butmanyboatshavebeenruined.Sickpeoplehavenowayof

reachingthemainisland.Onbiggerislands,communitiesareworkingtocleartheroadsthatarecoveredwithfallingtrees.
ThehospitalthatwevisitedinRoxasCity,inthenorthernpartofPanay,hasbeendamagedbutisstillfunctioning.Localmedicalstaffhavedonewhattheycantocopewiththefirstwaveofpatientswhosufferedfromfracturesandwoundsduetofallingobjects.
Butithasbeenrainingalotandsurvivorshavenoshelter.Wearenowpreparingforasecondwaveofpatients.Theyarealreadyseeingcasesofrespiratoryinfectionsanddiarrhoea,andweexpectthenumberofcasestoincrease.MédecinsSansFrontièreswillfocusonsupportingthelocalmedicalfacilitieswithstaff,drugsandmedicalequipment.Wealsoplantooperatemobileclinicsinremotevillagesandsmallislands.Withthefloods,therearealotofmosquitoessoweneedtobefast.Weareworriedaboutanincreaseinmalariaanddenguecases.Leptospirosis,aparasiticdiseaseisalsoathreat,asitisendemicinthispartofthePhilippines.

INFLATABLEHOSPITAL

TyphoonHaiyan–PartII
IntheaftermathofTyphoonHaiyan,aMédecinsSansFrontièresteamconstructedaninflatablehospitalonthedamagedseafrontofTacloban
–thePhilippinescityhardesthitbythetyphoon.
©YannLibessart
CONSISTINGOFFOURinflatabletentswithanareaof100squaremetreseachandafifthtentof45squaremetres,thehospitalcontainsanemergencyroom,awoundcareroom,apharmacy,andupto45hospitalbeds.
AdditionalcarewillbeprovidedwithinBethanyHospitaloncerepairshavebeencompletedtothedamagedsurgicalward,maternityward,neonatalunitandtheunitforsterilisingequipment.
“AlongsideFilipinoandinternationalvolunteers,weworkedhardallnight,inthe

pouringrain,sothatthehospitalwouldbeinplacethismorning,”saysYannLibessartfromMédecinsSansFrontières’emergencyteaminTacloban.“Gettingthesitereadyandinstallingthehospitalwasamajorlogisticalchallenge.FirstwehadtoclearthecourtyardandoutdoorareasofBethanyHospital–itwasatitanictask.”
OurmedicalteamsbasedintheinflatablehospitalalsoaimtosupportthefewhospitalsinTaclobanthatarestillfunctioning,andtotakeoversomeoftheworkofthefirstrescueteamstoarriveonthescene,includingsoldiers,whoarenowstartingtoleavethecity.
“Thefirstphaseoftheemergencyisnowover,”saysLaurentSury,EmergencyCoordinator,“andweexpectmainlytobetreatingpatientswithcommondiseasesorconditionsrelatedtopooraccesstohealthcare,suchaswomenwithcomplicateddeliveriesandpeoplewithchronicillnesses.Ourgoalistosupportthehealthsystemintheregionforthetimeittakestoreturntonormality.”
MédecinsSansFrontières’standaloneinflatablehospitalwasdevelopedwiththespecificpurposeofhelpingitsemergencyteamsrespondquicklytonaturaldisasters,enablingthemtoprovidepeoplewithqualityhealthcarewhiledamagedhealthfacilitiesarebeingreconstructedorrepaired.

ANUGLYDISEASE
DrAnnSellbergdescribesMédecinsSansFrontières’worktreatingchildrenwithHIVinZimbabwe,oneofthecountrieshardesthitbythe
epidemic.
©AnnSellberg
IREMEMBERTHEfirstchildIbroughttothecounsellorfordisclosure–theprocessoffindingouttheyareHIVpositive.Irememberhowhestaredatherwithbigeyeswhilesheshowedpicturesofthe‘soldiers’(theimmunesystem)andthevirus.
“InonziHIV,”shesaid,pointingattheangry-lookinggreenblob,showingitsfangs.“It’scalledHIV.”
Thechilddidn’tsaymuch;hejustkeptstaringatthepictureswiththosebigeyes,smilingbashfullyattimeswhenshewasaskinghimquestions.Towardstheendsheaskedhimtodrawapicture.Hetookhistimedrawingagirl,makingsuretofillinthe

armsandlegswithmanysmallblacklines.Ontopofherhewrote:Ebola.Thecounsellorlaughed.
“NotEbola.HIV!”Shetookhispenandscratchedoutwhathehadwritten.
“Couldyouaskhimtoexplainhispicture?”Isaid.Theboyspokewithashyvoice,butheusedmorewordsthanIhadexpected.
“Heissayingthegirlisugly,likeHIV.HewroteEbola*becausetheylearntaboutitinschool,anditisscary,likeHIV.”
Hewasanine-year-oldboyandIhadtoconvincehismothertobringhimintobetoldabouthisHIVpositivestatus.“He’stooyoung,”shesaid.“Hewon’tunderstand.”
Iexplainedtoherthatitisbetterforchildrentofindoutearly,thatitislesstraumaticandhelpsthemtoadheretotheirmedication.
“Besides,thecounsellorhaswaysofexplainingthatkidsunderstand.”Iwassurprisedathoweasyitwastoconvinceher,asthoughshewasjustwaitingforapush.
ThenexttimeIsawhimhewassmilingatme,andwedida‘givemefive’.Itwasatthesupportgroupforkidsandhewastakingeverythinginwithbigeyes.Iwashappytoseehim.Iknewthatwehadmadeadifferenceasthischildhadabetterchanceofcaringforhimselfandhisconditionwhenheknewwhathewassufferingfrom.
Thenurseshavemadeasurveyofhowmanykidshavereceiveddisclosure.Ninety-eightpercentofkidsagedfiveto10,57percentofkidsaged11to15and14percentofadolescentsaged16to20didnotknowthattheyhadHIV.Imaginethat!Achildthathasbeentakingpillsallhislife,almostreachingadulthood,maybeevenhavingsex,withoutknowingabouthisstatus.Nowondersomanyofthemarethrowingawaytheirpills,pretendingtotakethembutsecretlyhidingthemundertheirpillow.
“Wewillfocusondisclosure,”Isaidontheproject’sannualpresentationsofourplansfor2015.Itmaysoundlikeemptywords,butitisreallyhappening.Thecounsellorsarehavingdisclosurediscussionswiththecaregiversandthenursesareencouragingmoreandmorecaregiverstogowiththeirkidstothecounsellorfordisclosure.
I’mamazedathowwellitisworking.Ifwearemanagingtogetmostkidstoknowabouttheirstatus,thenwewillhavemadeahugedifferencetothispopulation.AndevenifMédecinsSansFrontièresisn’taroundinthefuture,theimpactwillstillbehere.

*Todate,nocasesofEbolahavebeenreportedinZimbabwe.

THETIMETODECIDE
MédecinsSansFrontièreshasworkedinAfghanistansince1981.InDasht-e-Barchi,MédecinsSansFrontièreshasworkedhand-in-handwith
theMinistryofPublicHealth(MoPH)tosupportthematernitydepartmentofthedistricthospital.MédecinsSansFrontièreshasalso
supportedtheMoPHinAhmadShahBabahospitalineasternKabulandBoosthospitalinLashkarGah,Helmandprovince.
©MathildeVu
ITISfourO’CLOCKinthemorning.
Awakenedbyaphonecall,theMédecinsSansFrontièresteamhurriestothematernityward.ThedistrictofDasht-e-BarchiinWestKabulissleeping,butinsidethehospitaltheurgency,anxiety,andexcitementarepalpable.

Thebrandnew42-bedmaternitywardwasanemptybuildingnottoolongago.Ninemonthslater,thelaunchoftheprojecthasbeenalittlelikeacomplicatedpregnancy.Now,acoupledaysaftertheopening,ayoungpatientsufferingfromcomplicationshasarrivedinthemiddleofthenight.
Inthedeliveryroom,Sarai-theseventeen-year-oldpatient-liesonthebed.Shehasalreadybeeninlabourformanyhours.Sheissilent,butherfaceiscontortedinpain.Herlabourisobstructedandshewillneedanemergencycaesareansectiontodeliverherbaby.
Complicationslikethisarecommon,but,inAfghanistan,thenumberofmedicalfacilitiesequippedtomanagesuchproblemsiswoefullysmall,eveninthecapital.Mostwomenandtheirfamiliescannotaffordtopayforprivatemedicalconsultationsandendupgivingbirthunassistedintheirownhomes.Inthecaseofcomplicationslikethisone,andintheabsenceoftrainedmedicalassistance,givingbirthcanbefatal.
TheteaminMédecinsSansFrontières’newmaternitywardfocusesonsuchcomplicatedbirths,andonsavingthelivesofmothersandbabieswhohavenowhereelsetogotoreceivespecialisedcare.Locatedinabuzzingmarketplacebehindagasstation,Dasht-e-Barchihospitalandthreesmallsatellitehealthcentresaretheonlyoptionsforpublichealthcareinthedistrict.
ThepopulationofthisneighbourhoodofKabulisestimatedtohavegrowntenfoldoverthepast10years,andnowhasmorethanonemillioninhabitants.ThepublicmaternityhospitalsupportedbyMédecinsSansFrontièreswillnotbeabletocatertoallthehealthneedsinthearea,buttheteamexpectstoseemorethan130complicatedcaseseachmonthoutofanestimated600normaldeliveries.
Saraiwillneedtobeoperatedonsoon.MédecinsSansFrontièresmidwifeDanielatransfershertotheoperatingtheatreteam,RenatethenurseandDianathegynaecologist.
Thelightsareblazingintheoperatingtheatre.Everythingfromtheprobetotheanaesthesiamachineisbrandnew.Inthepastweek,duringthedressrehearsal,everypieceofequipment,electricalcircuit,waterpump,andinfectioncontrolinstrumentwastested.
LaunchinganewMédecinsSansFrontièresprojectreliesheavilyonthiskindofbehind-the-scenespreparation.Thelogisticalteamworkedformonthstorehabilitatethematernitybuildingintheexistingpublichospital,strivingtoachievethehighstandardsforwhichMédecinsSansFrontièresfacilitiesareknownthroughout

Afghanistanandtheworld.
At5am,ababycries-it’saseven-poundboy.Saraiissafeandshecatchesherbreath.Shehasn’tthoughtofanameyet,but,becauseofthecareshereceived,shehastimetodecide.
Patientnamehasbeenchanged.

SURVIVINGWARANDGOINGBACK
Aftersurvivingwar,notmanypeoplewouldchoosetogobacktoaconflictzone,butthat’sexactlywhatNurseAbdulWassaydid.AsanAfghanrefugeegrowingupinPakistan,hesawfirsthandtheurgent
medicalcareMédecinsSansFrontièresdeliverstopeopleinwarzones.Afterworkingwithusnearhishome,hevolunteeredtohelpothersin
anotherconflict-torncountry-SouthSudan.
©JasonCone
I’VEBEENTHEMedicalTeamLeaderforthepast11monthshereatMédecinsSansFrontières’100-bedhospital.AfterworkingforMédecinsSansFrontièresforseveralyearsinPakistanandseeingthecriticalassistancewedeliver,IdecidedtocometoSouthSudantotreatpeoplesufferingfromtheeffectsof30yearsofwar.
LankienHospitalistheonlyoneofitskindforhundredsofmilesineverydirection.

Ourwardsarefilledwithmalnourishedchildren,expectantmotherswithcomplications,andpeoplesufferingfromtuberculosisandkala-azar,aneglectedtropicaldisease.Patientscomefromhoursaway,mostlytravellingtheruggedlandscapeonfoot.And,whenviolencebreaksoutbetweenlocalgroups,wecanfacewaveafterwaveofwoundedpatients.
ThousandsofpeoplehavebeenimpactedbythefightinginSouthSudan,andmanymen,womenandchildrenhavenowheretoturnformedicalcare.
Wenotonlyfacedthechallengeoftreatingseriousinjuries,wealsoneededtomakesurethebattlefielddidn’tmakeitswayintothehospital.WhilemycolleaguesandItriedtostopthebleeding,checkvitalsigns,andadministerIVfluidsandantibioticstostaveoffshockandinfection,Iwasalreadythinkingaboutwhatwewouldneedtodotomaintainthesafetyofourstaffandpatients.
Becauseweweretreatingpeopleonbothsidesoftheconflict,wehadtokeepourpatientsseparatedindifferentwards.Wealsorestrictedtheaccessofpeopleenteringandleavingthehospital.Butevenwiththesechanges,ourstaffstillsearchedeverypersonenteringtheinpatientcareareaforweapons,toprovideanextralayerofprotection.
ImpartialityandneutralityarecriticaltoolsformaintainingthesecurityofMédecinsSansFrontières’teamsandpatients.Andtheindependentfinancialsupportwereceivefrommembersofthepublicplaysacrucialroleinhelpingustreatanyoneneedingemergencymedicalcareinthemidstofaconflict.
Deliveringqualitymedicalcareinconflictzonesisnevereasy,butourteamshavetheexpertiseandexperiencetodowhateverittakestosavelives.

STORYBOOKTHERAPY
SteveCohenisaforensicpsychiatristwhowaspartoftheresponseinthePhilippinesfollowingTyphoonHaiyan.StevewaspartofMédecinsSansFrontières’MentalHealthTeamwhoprovidedoutreachcareinhard-hitregions,evacuationcentres,schools,andinpatientandoutpatient
departments.
©MSF
MEDECINSSANSFRONTIERES’programstakeamassiveamountofcoordinationandeffort,spanningseveralcontinentsinreal-time,whichinturncanbeintense,complicatedandtrying.Attendingtothepersonalneedsofthehumanitarianstaffcontinues,allwhilesourcingaplacetosetupahospital,hiringstaff,andgettingeverythingfromsurgicalamphitheatres,neonatalunits,mobileandoutreachclinics,andmentalhealthservicesupandrunning.
Attimes,thebodilyneedsareeasiertounderstandthanmentalhealthneeds.Weseeabrokenbone,hearacough,andcanmeasuretheblood-glucoselevel.Thereasonsthatapersoncomestotheattentionofmentalhealthcareprofessionalsareoftenduetoconspicuousabsencesoffunctioningathome,socially,oratworkorschool.Thisisespeciallytrueinchildren,forexampleaquietchild,decreaseinconcentrationorattention,fearfulnessatnightandsomeavoidanceofsocialplay…thesethingscouldgounrecognised.
TheelementaryschoolprogramwassetupaspartoftheTaclobanProject.Thechildren,abouttenpersession,huddleinacirclewhileoneofourstaffreadsthe

storybook,ATerribleThingHappened,byMargaretHolmes.
Thestudentscomefromtwocoastalelementaryschoolswhichwereidentifiedasthehardesthitbythetyphoon.Thenumbersarestaggering.Sixty-sevenchildrendiedinoneschool,whichrepresentsabout15percentofthetotalnumberofstudents.Wordsfailwhentryingtocapturethetragedy,andtheheartbreak.
AndthisiswhereShermantheRaccooncomesin.Somethingbadhappenedtotheyoungraccoon,andhebeginstoshowsignsoffear,stress,andacting-outbehaviour.Therearefoursessionswitheachgroup;thefirstthreeinvolvereadingthebookinthreeparts.Afterthefirstsession,thechildrenareaskedtodrawonpaperwhatShermanmaybeafraidof.Inthesecondpart,Shermanishavingsomedifficultyinschoolandwithfriendsandfamily,andtriestofindwaystocalmhimself.ThechildrenareaskedhowShermaniscopingwiththe“verybadthing,”andhowheisfindingwaystoself-sootheorpacifyhisinnerturmoil.ThefinalpartofthebookinvolvesatherapistwhoShermantalksto,andeventuallyhefeelsbetter.ThechildrenareaskedtodrawtheirthoughtsaboutShermannowthathefeelsbetter,andwhatShermanmightdowithhisre-foundhappiness.
©SteveCohen
Thechildrenexplaintooneofourfourprogramstaffthemeaningoftheirdrawings,andthethemesaretrackedthroughoutthefourweeks.Itisatherapeuticprocessonitsown,butwhensomestudentsareclearlyexhibitingadeclineinschoolfunctioning

(sometimestothepointofrefusingtoattendschool),moreintensiveworkisdone.
CaregiversandteachersareconsultedandchildrenareassessedusingatooldevelopedbyMédecinsSansFrontières.Individualtherapyisalsodonewiththechildandcaregivers.
Thewindandraincomesandthechildrenstillexhibitsomehesitancyorfear,butitpassesquicklyformost,andasongissung.Moststudentsnowrunoutsidetoplayintherain.
Over100childrenperweekparticipatedinthestorybooksessions,andfivetotenperweekhadindividualtherapy.Primaryhealthcareincludesmentalhealthcare.Ifwedon’thavestaffwhoareknowledgeableandcommittedtomentalhealthwork,eitherinadisastersettingorinalonger-termcrisissetting,wearemissingsufferingthatisidentifiableandtreatable.

MYHEARTLEAPSFORJOY
DrJosineBlanksmaworkedforMédecinsSansFrontièresinBarakahospitalineasternDemocraticRepublicofCongoforeightmonths.
Duringhertimethere,Josinetreatedhundredsofpatientsformalaria,aparasiticinfectionthatcanbefatal,particularlyinchildren.
Hereshedescribeswhatitwasliketreatingheryoungpatientsforthedisease.
©JeroenOerlemans
INTHEWARD,thenursesarealwaysbusy:movingaround,takingtemperatures,checkingtheheartratesofthelittleones,checkinghowthey’rebreathing,administeringmedicationsorputtinginadripwhenthechildrenaretooweaktoswallowpills.
Igofrombedtobedexaminingthepatients.Inchildren,malariacanrapidlybecomefatal,soit’sreallyimportantthatwepaycloseattentiontotheirsymptoms.Arethey

breathingsoftly,oraretheyshowingsignsofrespiratorydistress?Aretheylosingconsciousness,oraretheyhavingseizures?
Atthatpoint,alotofredbloodcellshavebeendestroyed,andthebrainandotherorgansarenotgettingenoughoxygen.WebringthechildrenimmediatelytotheIntensiveCareUnit(ICU),administeroxygenandgivethembloodifnecessary.We’reworkingaroundtheclock,doingeverythingwecantosavechildren’slives.
ItisthepeakofthemalariaseasonintheDemocraticRepublicofCongo(DRC).Everyday,manypatientsarriveatthehospitalwithseveremalaria.
Luckily,inmostcases,we’reabletohelpthemintime.
“Twodaysagomysondevelopedafever.He’sbeenvomiting,”aworriedyoungmothertellsme.Shecradlesherunconsciousandverypalethree-year-oldboyinherarms.
Wedoabloodtestrightaway.Mysuspicionisconfirmed:thelittleboyhasmalaria.
Wemedicatehimthroughadrip,andhegetsabloodtransfusionasthemalariaparasitehasbeenattackinghisredbloodcells.Wegivehimoxygenthroughamask,andfeedhimtherapeuticmilkthroughanasogastrictube.
Wehavedoneeverythinginourpower;nowwemustwaittoseeifhislittlebodycandefeatthedisease.I’mafraidforhislife.
WhenIwakeupthenextmorningandgotothehospital,thelittleboyisawake.Hismotherisfeedinghimporridge.Twodayslaterhe’shealthyagain,andwecandischargehim.
Onanotherday,twochildrenarriveatthehospitalsufferingfromseveremalaria.Thefive-year-oldboyhasbeendriftinginandoutofconsciousness,andthethree-year-oldgirlisinacoma.Ifeartheworst.
ButmyheartleapsforjoythenextmorningwhenIseethem:thelittlegirlisawake,lookingatmewithinterest.Theboyissittingupinbedandiseveneatingagain.
Themalariaseasonwasparticularlybadthisyear,andourhelpmakesallthedifferenceforthefamilies.TherearemanyplacesinDRCwhereMédecinsSansFrontièresistheonlyprovideroffreemedicalcare.
InDRC,myteamandIprovidelifesavingtreatmenttochildrenlikethislittleboyevery

day.AsIknowI’llbeanauntsoon,patientsuccessstorieslikethistouchmeallthemore.

SMALLMIRACLES
HereDrKellyHildebranddescribeshertimeinthePaediatricUnitsintheAweilReferralHospitalinSouthSudan.
©MSF
IHAVENOWbeenhereforsixweeksandIhaveexperiencedeverypossibleemotionfromfatigueandhopelessnesstosheerjoyandgratefulness.
OurhospitalhasbeenovercapacitysinceIarrivedaveraging120to130patientsinPaediatricsonagivenday(Ibelievethebedsarefor70to80patientsbutwehavetwinsinmanybedsandmattressesontheflooreverywhere).
Inmyneonatalunit,Iacceptverylowbirthweightinfants(1.25kilogramsandabove)withgestationalagesasearlyassixmonths.Thetetanusroomhashadfivetoeightchildrenatatime,mostlyneonatesbornathomewhogettheinfectionfromtheumbilicalcordasithasbeencutwithoutanappropriatecleantool.ThePaediatricICUisoverflowingwithmalaria,malnutritionandrespiratoryillnesses.
Thefirstweekswereextremelyhardonme.IspentalotoftimeandenergyfocusingonwhatIcouldnotdo,insteadofacknowledginghowmuchwewereaccomplishing.IwasworriedaboutgapsinmyknowledgeasIamageneralpaediatrician,notanICUdoctor(thoughIamsogratefulfortheICUtrainingIreceivedinresidency).IwasdrainingmyselfemotionallyandrealisedmentallyIwouldnotsurviveifIkepttravellingthisroute.
Twosmallmiracleshappenedformerightaroundthesametimeanditwastheturning

pointIneeded.
Duringmyfirstweekhere,amumbroughtinhertwo-week-oldbabywhoshehadgivenbirthtoathome.Thebabyhadstoppedbreastfeedingandwashavingtroublebreathing.Weplacedapulseoximeteronthechildandheroxygenlevelwasreallylow.Shehadcracklesinherlungsandaloudmurmur.Iknewshewasinheartfailure.Itoldhermumwewoulddowhatwecouldbutthechildmaynotsurvivethenight.
Westartedoxygen,gaveasmallbolusfordehydration(asmallvolumeoffluid),startedantibiotics,somemaintenancefluidsasthechildwastoosicktobreastfeedandgavediuretics.Ireallydidnotthinkthechildwouldmakeitthroughthenight,butthenextmorningthereshewasbreathingfastandretractingbutstillalive.Shenowhadoedema(swelling)andaliveredge(signsofworseningheartfailure)sofluidswerestoppedandanasogastrictubewasplaced.Themumwastaughthowtoexpressbreastmilkandhowtoplaceitinthetubeforherchild.Thepatientsurvivedfordayslikethis,herlungswerefulloffluid,allIcouldhearwerecrackles.Sheweighedlessthan1.8kilogramsandallhereffortswenttowardsbreathing(allwehadwerefivelitresofoxygenbynasalcannulatosupportbreathing).ItalkedwithhermumdailyandsheknewIhadaguardedprognosis,butIwouldcontinuetodowhatIcould.
Thenonemorning,Ididmyexaminationandtheyweregone,thecrackleswerejustgone.Iheardclearbreathsounds.ImusthavelistenedforwhatfeltlikeagesbutIcouldn’tbelievewhatIwashearing,orwasn’thearing.Overthenext10days,shecontinuedtoimprove.Shestartedbreastfeedingandthefeedingtubewasremoved.
Shecameoffoxygenandfinally,shegainedweight.Onemonthandonedaylater,Iwassendingherhome.Shestillhasamurmurandshemaygetsickagainbutfornowshe’sthriving.Itoldhermumsheismymiraclechild.(Forthemedicalpeoplemyonlyexplanationwaspersistentpulmonaryhypertensionthatslowlyimprovedwithtime.)
Mysecondsmallmiraclehappenedrightaroundthesametime.Ihavebeenstrugglingwithmalnutrition.Themortalityrateishighwhenamalnourishedchildgoesintoshockandithasbeenextremelyfrustratingforme,especiallysincemalnutritionisnotsomethingIseeathome.
Apatientwastransferredtomefromthefeedingcentrefordecompensation-asuddendeteriorationincondition-andbythetimeshearrivedshewasinshock,non-responsive,withcoolextremities,andaweakpulse.Againmyhopeforresuscitationwasnotgreatandthefluidbalancesinmalnourishedchildrencanbetricky.
Wegaveasmallbolusandstartedantibiotics.Sherespondedalittletothefluidsowe

gaveanothersmallbolusandthenplacedanasogastrictubetorehydrate.Wegavearehydrationsolutionthroughthenight.Isaidgoodnightandgavestrictinstructionstothenightstaff.Ididn’thearfromthemthatnightsoIwasnotsurewhattoexpectthenextmorning,butonceagainwhenIarrivedthereshewassittingupinbeddrinking.Iwantedtocry,Iwassohappy.
Shewasmyfirstmalnourishedchildinshocktorecover.Shecontinuedtoimproveandstartedtogainweight.
ThedaysarestillupanddownandthebaddaysarestillbadbutI’mstartingtoseeallthegoodwedohereaswellandIkeepholdingoutforsmallmiracles!

RECONSTRUCTINGBODIES
ThisisaninterviewwithOrthopaedicSurgeonDrAliAl-AniabouttheworkhedidwithMédecinsSansFrontièresattheReconstructiveSurgeryProjectinAmman,Jordan.TheprojectservesSyrian,Iraqi,Yemeniand
Palestinianrefugees.
©EnassAbuKhalaf-Tuffaha/MSF
TellusaboutyourselfandyourroleattheAmmanproject?
MynameisDrAliAl-AniandIamfromIraq.ImovedwithmyfamilyfromIraqtoAmmanin2005becausethesecuritysituationwasverydangerousanditwasimpossibletoliveanormallife.Ibeganworkingwiththeprojectasanorthopaedicsurgeonin2007.
Whatkindofpatientsdoyousee?
Ourpatientsarevictimsofconflictintheregion.Forthefirsttwoyearsoftheproject,wereceivedonlypatientsfromIraq.In2008,weexpandedandstartedtoacceptpatientsfromothercountriesaffectedbyviolenceintheregion–we’vesincereceivedpatientsfromGaza,YemenandSyria.Themajorityofthecasesthatwedealwitharecomplex.
Whatkindofcasescanbeacceptedontheproject?
Ourselectioncriteriacoverthreespecialties:orthopaedic,maxillofacialandplasticsurgery.Manyofourpatientshaveboneinfections,requiringlengthytreatmentprocedures.Wealsoreceivepatientswhosebrokenboneshavenotfusedproperly,withorwithoutsofttissuedefect,aswellaspatientswithboneloss,nerveinjuries,andassociatedphysicaldeformitiesasalong-termconsequenceofuntreatedtrauma.
Duetothenatureofconflict-relatedinjuries,eachnewcaseisachallengeandeachwoundedpatientisincomparabletoanother.Howareyouaffectedpersonallybyyourwork?
IamasurgeonbutIamalsoahuman-beingandaffectedbywhatIseeinmywork.IfeelpainwhenIamface-to-facewithinnocentchildrenandoldermenandwomenwhoseliveshavebeenforeverchangedbyman-madeconflict.Butasasurgeon,Iaminapositiontotreatthesevulnerablepeople,tomakethemsmileandenjoyasenseofindependenceagain.Ifeelproudthatthisprojecthasrelievedthesufferingofsomanypatients–byreconstructingtheirinjuredbodiesandhelpingthemtoregainfunctionality–especiallyasthosewhoarereferredheremaynotbeabletoaffordsuchcareotherwise.
Eachpatienthastheirownstoryofalifeaffectedbywar.ButthestoryofasevenyearoldIraqiboywhowasadmittedtotheprojectin2009touchedmemost.Rahimwasonhiswaytovisithisgrandparentswhenaroadsidebombexploded.HismotherwaskilledandRahimwasbadlyinjured.Helosthisrightlegandhisleftlegwasseverelydamaged.Despitethecomplexityofthesurgeries,overthecourseofseveraloperationsthesurgicalteamwasabletoreconstructhisdamagedlegsufficientlyforthelegtobearweight,andtoattachprosthetics,sothatRahimwasabletowalkagain.
WhatdifficultiesdopatientsfacewhentheyreturntoIraq?
Themaindifficultyisaccesstofollow-uptreatmentbackhome.Thisincludespsychosocialsupportandphysiotherapy.AlthoughwetrytofinalisetreatmentinAmman,theseinjuriesoftenrequirealotoffollow-upaftersurgery,andthisisabig

challenge.
Whatareyourhopesforthefutureoftheproject?
Theprojecthasexpandedconsiderablysince2006,andwehavepositiveplansforthefuture.Wewillsoonbemovingtoanewfacilitywhichwillimprovethequalityofcareandincreasetheproject’stechnicalcapacityandscope.Itmayalsoallowustoaddnewtypesofsurgery.
Patientnamehasbeenchanged.

DAUGHTEROFTHEFLOODS
WeeksafterMalawiwasdevastatedbythelargestfloodsinlivingmemory,peoplewerestillstrugglingtogetonwiththeirlivesandpreparingasbestastheycouldforadifficultfutureahead,likethe
arrivalofanewbaby.
©RowanPybus/MSF
MARTHADIDN’TRUNwhenthefloodshit.Shedidn’trunbecausetherewasnowheretogo.Makhanga,aclusterofvillageswithapopulationof5,000,restsonwhatcanbarelybecalledahill,butisnonethelessonslightlyhighergroundthanthevastplainsofsouthMalawi.
ButtheotherreasonthatMarthadidn’trunisbecauseshewaseightmonthspregnant.
Thewatercameduringthenight.At3.00amMarthawokeup.Therewaswaterinherhouse,lickingtheblanketonwhichsheslept.
Slowly,slowly,itcreptup.Ankledeep,kneedeep…untilmidnightwhenitreachedherwindowsill.Itateupthecornfieldsthatfeedthevillage.Itcontaminatedthewellsthatsustainthefamilies.Itblanketedthelocalclinicwiththick,oozymudwhichclungto

drugs,toinstruments,toeverything.
Therewasnowheretogobutup;therewasnothingupbuttrees.Victor,Martha’shusband,hauledhisheavywifeandtheirfivechildrenupontothebranches,stilldrenchedfromtheheavyrains.
Theystayedthereforfourdays.Thebabykeptkicking.
Andthenitwastime.Earlyonemorning,13daysafterthefloodscameandwentandstoleallofherpossessions,Marthafeltthebabywasready,evenifshewasnot.
“Wewenttotheclinic,butitwasclosed.Therewasnoonetheretohelp.Iwastoldtowait,thatahelicopterwascoming,thatitcouldtakemetoanotherclinic,”sherecalls.Bythattime,Makhangavillagehadbecomeanislandcutofffromtherestofthecountry,apartfromaslowtrickleofaiddroppedfromtheair.
“Whenwelandedweweretoldtherewasawomaninadvancedlabour,butnobodytodeliverthebaby.Soitwasuptome,”saysCliveKasalu,aMalawiannurseandmidwifeworkingforMédecinsSansFrontières.Clivehadanemergencydeliverykitand14yearsexperienceunderhisbelt,sohefeltconfident.Butstill,“wehadtoimproviseabit,”hesays.
OnlypartsoftheclinichadbeencleanedupduringthethreedaysthatMédecinsSansFrontièreshadateamatworkinMakhanga.Cliveenlistedanassistantto“runupanddowntogetuswater,”whilefocusingonthesufferingmother.
Withinanhour,Marthawasengulfedbybirthingpains,sweatingandclingingtothebarebedwhileherhusbandVictor,thevillage’sheadman,waitedoutside,worrying–it’staboohereforfatherstoattendabirth.
Andthen,atnoon,Makhangahadonemorevillager:ahealthy,screaming,hungry,2.9kilogrambabygirl.
Patientnameshavebeenchanged.

ABEAUTIFULDAYINTAJIKISTAN
Rukhshonahadmultidrug-resistanttuberculosis(MDR-TB),butfollowingtreatmentinMédecinsSansFrontières’projectinTajikistan,sheisnowcured.“Thisisajoyful,memorableday”,saidproject
coordinatorBeatriceLau.“ThetreatmentforMDR-TBisextremelyhardandtakesalongtime.WeareveryproudofRukhshonathatshehas
persevered.”
©WendyMarijnissen
WHENRUKHSHONAARRIVESatherparty,sheisgreetedwarmlyandshoweredwithcongratulatorywishes.Allthepraisemakeshervisiblyuncomfortable.Nevertheless,sheisthrilledwiththepartyand,ofcourse,thereasonsforhavingit.“In2011,Iwashospitalised”,shesaid.“Ihadafever,wasnauseousandwascoughingupblood.Itmademeterriblyworried.Thatseemssolongagonow.”“Thedifferencecouldn’tbegreater,”Rukhshona’smothersaid.“Shewasveryill,shewasadifferentpersonthen.Hertreatmentwassohardandtookalotoutofher.”

PatientsreceiveaparticularlygruellingtreatmentforMDR-TB(multidrug-resistanttuberculosis),withapainfulinjectionandtakingupto20pillseveryday.Thedrugsareoftenaccompaniedwithserioussideeffects.“Igotterribleheadachesandpaininmystomachandlegs,”saysRukhshona.“Icouldbarelywalk.Iwasalsonauseousandhadtovomitoften.Ifeltsoweak.”
“AtfirstIdidnotevenknowwhatTBwas,”shecontinues.“Iwassick,butwhatdidIhave?Ididn’tknowifIcouldbetreated.Thatwasveryscary.EspeciallywhenIstartedtocoughupblood.IonlystartedtobelieveIcouldgetcuredwhenIstartedtakingmymedicationandbegantofeelalittlebetterbitbybit.”
Asateenagerwhocouldn’tgotoschool,whocouldn’tseeherfriends,Rukhshonaoftenfeltveryalone.ShefoundcomfortinthepoemsandsongsofRudaki,aPersianpoetwholivedcenturiesago,intheareawhereTajikistannowlies.“Hisversesareaboutlife,aboutrespectforpeople.Itmademeveryhappy.”
Shereceivedunconditionalsupportfromhermother,eventhoughthetreatmentwasafightforher,too.Shefoundithardtoseeherdaughtergothroughsuchhardtimes.“Shewasveryworriedaboutme,”Rukhshonasaid.“Butshewasalwaysbymyside,andhelpedmethroughthedays.Shewasveryscaredthough,andIhadtocheerherupandtellhereverythingwouldbeokay,eventhoughIwastheonewhowassick.”
Despiteherworries,Rukhshona’smotherwantedherdaughtertofinishhertreatment.“Someparentsdonotbelieveintreatment.Theirchildrendon’tsurvive,”shesaid.“I’mverygratefultoMédecinsSansFrontièresfortheircare,themedication,andtheirsupport.”
Meanwhile,thepartyisunderway.Thereisdancing,singing,andlotsoflaughter.“It’sabeautifulday,”hermothersaid.“ForMédecinsSansFrontièrestoo.Rukhshonaisproofthatpeople,children,withMDR-TBcanbecuredandhaveafuture.”Rukhshonanodsandaddressesthesmallpatientsaroundher.“IthoughtIwouldnevergetbetter,”shesaid.“ButthecareandsupportIreceivedhelpedmegetwell.I’mcurednow.Youhavetokeepbelievingthatit’spossible.”
Patientnamehasbeenchanged.

AISHA
WhenAisha’sgrandmotherbroughthertotheoutpatientpostwhereMédecinsSansFrontièresteamswereconductingoutreachactivitiesinAfar,Ethiopia,everybodythoughtshehadjustafewdaystolive.
©FaithSchwieker-Miyandazi
“IHADGIVENuphopeonmygrandchild,”saysEisa,Aisha’sgrandmother.“Ithoughtshewasgoingtodielikethethreeothersbeforeher.”
Theone-year-oldwassufferingfromsevereacutemalnutritionwhenshearrivedatouroutreachpost.Hermotherwasalsoailingandsuffersfrompsychosis.ShewasinnoconditiontotakecareofAishaandherolderbrother,leavingthegrandmotherastheirsoleguardian.

OurteamtravelledtoAfarinApril2013inresponsetoanutritionalemergency.Afarisvast,andTeru-theareathatwecover-isoneofitsmostremoteandneglectedregions.Subjecttohugesandstormsandextremetemperaturesinthedryseasonandviolentrainstormsthatfloodriversandrenderroadsimpassableduringtherainyseason,Teruisanextremelydifficultcontextinwhichtowork.
TheAfariareapastoralnomadicpeoplewhomovefromplacetoplaceinsearchofwaterandpasturefortheiranimals.Livingthiswaymakesitdifficulttoadheretotreatmentregimens,meaningthatmanypeopledefaultbeforecompletingtheprogram.Italsomakesitdifficultforourteamstofollowupwithpeoplewhodefault.
Ourinterventioncovered12Kebeles(provincialadministrativeunits),whoseinhabitantsarecompletelycutofffromhealthcare.Thedecisiontointervenewasreachedafteranassessmentrevealedanalarmingrateofsevereacutemalnutritionintheregion-26.6percentofanestimatedcatchmentpopulationof87,374peoplesufferfromthecondition.
“Mostofthecasesthatweadmitinthestabilisationcentrearesevereacutemalnutritionwithcomplications,”saysFrankKatambula,MédecinsSansFrontièresMedicalTeamLeaderinAfar.“What’smore,”headds,“mostofthesearecombinedwitheitherpneumoniaorTB.”
DespitethedifficultiesrelatedtoprovidingcareinTeru,mostcaseshavenowstabilisedandchildrenundertheageoffivecontinuetoreceivetherapeuticfood.Overall,atotalof726malnourishedchildrenwereadmittedtothetherapeuticfeedingprogramand1,154moderatelyacutemalnourishedpatients(including416pregnantandlactatingwomen)benefittedfromtheprogram.
“Intotalwehave78.2percentcuredcasesandadefaulterrateof4.5percent,whichtomeisquitegoodconsideringthataccess[tohealthcare]inthisareaisnotatalleasy,”saysJeanFrançoisSaint-Sauveur,MédecinsSansFrontièresMedicalCoordinatorinEthiopia.
Aftertwomonthsintheprogramandadmissionintothestabilisationcentrewhereshewasalsogivenspecialisedtreatmentforpneumonia,Aisha’sweightincreasedfrom3.2kilogramsto4.9kilograms.
“WhenIseethischildIfeelveryhappybecausethegrandmotherandtherestofthecommunitythoughtshewasgoingtodie,”saysNabiyuAyalew,MédecinsSansFrontièresOutreachNurse.“Butwesavedherlifeandsheisstillalive.”

Patientnamehasbeenchanged.

THESECRETBLOODBANK
DrNatalieRobertswaspartoftheMédecinsSansFrontièresteamprovidingtrainingandequipmenttohospitalsandhealthfacilitiesin
Aleppo,Syria.
©MSF
THEREISSOmuchavoidablediseaseandtraumainSyriathatweasMédecinsSansFrontièrescanreallyhelpwithandthereisreallynooneelsetheretodoit.Youcanreallyseethedifferencethatevenbasicthings,likeakitofmedicinescanmake.ThisismysecondtimeinSyria,andoverthelastweeksI’vereallynoticedtheescalationofviolence.Butyougetusedtoit.Incidentsthatinitiallymademeveryfrightened,Inowtakeforgranted.
ThefirsttimeIwasreallyscaredwaswhenaverylargemissilelandednottoofarawayfromwherewewerestaying.Wecouldfeelthewindowsofourhouseshaking.Thereweretwoofusinthehouseandwewerebothafraid.Butwithinamonth,weweregettingmissileseverynight-someverynear-andwe’dgetoutofbedandgotooursaferoombutbecomplainingthatitwascoldandoursleepwasbeinginterrupted.
Youevenstartmakingjokesaboutit,butit’sjustawayofcoping.Inreality,youneverreallylosethefear.
ThefirsttimeIvisitedoneparticularemergencydepartmentatahospitalinAleppowewerediscussingwiththestaffhowwecouldhelpthemwhennewscamethatamortarbombhadhitanearbymarket.Veryquicklywestartedtoreceivecasualties.Tenfatalitiesarrivedalmostimmediately,thenfourmore-twowhohadsustainedmassiveheadinjuries.
Insituationslikethat,it’svitalyoutriageandprioritisepatientsanditwasveryclearthatthesetwopatientswerebeyondhelp.Inthemidstofallthepanicandcrisismyrolewastopointoutthattwoeight-year-oldgirlswithshrapnelwoundswhocouldbehelpedwereourpriority.
Peoplearegratefulthatwe’rethere.Wehelpwithwhatwecan,buttheneedsarehuge.Weprovidevaccinationsandsuppliesfordialysismachines.We’vesetupabloodbankinasecretlocationwhichsuppliesallhospitalsinthearea.Peoplehavebeencomingfrom50kilometresawaytoaccessit.Itrequiredabitofwork,alotoftrainingandequipment,butit’snowupandrunning.Beforepeopleweregettingunsafeblood,bloodthathadn’tbeentestedandstoredcorrectly,butnowtheyare.Somethinglikethatisreallyeasytodo,butit’scosteffectiveanditsaveslives.
ThesufferingthatpeopleareexperiencinginSyriaisincredibleandit’sfrustratingandupsettingtoseesomanyproblemsandknowthatbecauseofsecurityorforotherreasonsyoucan’tsolveitall.ButasMédecinsSansFrontièreswedowhatwecan,andit’svitalwecontinuetohelp.

EBOLA
AneBjøruFjeldsæter,aNorwegianPsychologist,recountsherexperiencesworkingwithMédecinsSansFrontièresinSierraLeone
duringtheEbolaepidemicin2014.
©SylvainCherkaoui/Cosmos
IWASEXPECTINGtheEbolaepidemictobequitegruesomeandunlikeanythingIhadseenbefore.ButIreallydidn’texpectitsmagnitude-thisoutbreakisenormous.InSierraLeone,itkilledalotofhealthworkersbeforeMédecinsSansFrontièresevenarrived.
Notsurprisingly,medicalstaffwerereluctanttoworkwithusatfirst.They’dnevercomeacrossEbolabefore,butatleasttheyhadpreviousexperienceofpeoplesufferinganddying.Butforthenon-medicalstaff,likethehygienists-ourhospitalcleaners-it’sbeenanewanddisturbingexperience,andalargepartofmyworkinvolvesprovidingthemwithcounsellingandsupport.

Thehygienistshavethehardestjobofall,becausetheyaretheonesdealingwiththedeadbodies.Alotofthecleanersareyoung,unskilledworkers.Inanareawithanunemploymentrateof95percent,theyjumpedatthisopportunitytogetajob.
TheresaJones,19,livedinFreetownwithhersister,whereherschoolclosedaftertheEbolaalert.WhileshewastovisitinghermotherwholivesinKailahun,afriendtoldherthatMédecinsSansFrontièreshadatreatmentcentreandwaslookingforworkers.Shewentdailytothecentreforaweekandwasfinallyemployedasahygienist.Shewashesclothes,tents,patients,toilets,andalsopreparesthebodiesofthedeceasedpatientswhodidnotsurvivetheEbolavirus.
BeforejoiningMédecinsSansFrontièresshehadneverseenacorpse.Thefirsttimeshewasveryscared.Sheissadwhensheseesyoungpeoplewhohavedied.Herfriendsandfamilyareafraid,theydon’tdareapproachher,buttheyunderstandandappreciatetheworkshedoes.AtfirsttheysaidthatEbolakillsandifsheworksatthecentreshewilldie.Now,thankstoherworkatthecentre,theyknowthebasicrulestofollowtopreventcontractingthevirusthemselves.
Whileallourstaffarewelltrainedinprotectivemeasures,justknowingthatyouarepotentiallyputtingyourselfatgreatriskofcontractingthediseasecanbestressful.
Dealingwiththedeadbodiesisdisturbing;thehygienistsexperiencefeelingsofsadnessandfear,andalsodisgust.WithEbola,whenpatientsdietherecanbebleeding,vomitinganddiarrhoea.Thehygieniststellmetheyexperienceflashbacksofthingstheyhaveseenandsmelled.Evenwearingamask,youcan’tshutoutallthesmells.
Traditionally,inSierraLeone,thebodiesaretakencareofbythetribalelders.Alotofthehygienistsfeeltheyaretooyoungtobedealingwiththedead-theyfeelthey’rebeingdisrespectfuloftheirculture’straditions.Wemakesurethatoneachshiftthereisalwaysonemanandonewoman,sothatwhensomeonedies,therewillalwaysbesomeoneofthesamesextotendtothem.
Thelocalstaffalsoexperiencehugestigmafromthecommunitymakingithardforthehygieniststomaintaintheirimageofwhattheyaredoing.Wetellthem,“Youareheroes,you’redoingaveryimportantserviceforyourcommunity-it’sabsolutelyvitalthatsomeoneisdoingthisjob.”Butalthoughweseethemasheroes,thisisn’talwayshowtheyareperceivedbytheirfamilies,theirfriendsortheirvillages.
WhenwedischargeapatientwhohassurvivedEbola,itmakesanenormousdifferencetothem.Ononeoccasion,threepeoplewhohadbeencuredweredischargedfromtheisolationward,andallthehygienistsweredancingaroundtheward,deliriouslyhappy

andtakingphotographs.
Theyfindwaystomanagethestress:theytakegoodcareofeachother;whensomeoneisupset,theytalkaboutit;andtheyareveryopenaboutvoicingtheirconcernsanddifficulties.Butthefactisthatthelocalstaffhavehadtheirlivesturnedupsidedown.Forthisentiredistrict,everythingisupsidedown.

CONTINUITY
In2013,MédecinsSansFrontièresopenedanewclinicinKibera,aslumintheKenyancapitalofNairobi.Kiberaishometoaround250,000people-manyofwhomareNairobi’smostvulnerableresidents.
©PhilMoore
THEMEDECINSSANSFRONTIERESKiberaSouthclinicprovidescomprehensivemedicalcare,includinginpatientandoutpatientservices,24-hourmaternitycareandtreatmentfordiseasessuchasHIVandtuberculosis(TB),whicharecommoninKibera.
Parentsbringtheirchildrentotheclinicforessentialvaccinationsandnutritionalscreening.Victimsofsexualviolencecanalsogettreatment,supportandongoingcounselling.
InthepastyeararoundhalfofKibera’sresidentshavevisitedtheMédecinsSansFrontièresclinicformedicalcare.Theteamseesalargenumberofpatientswhoneed

treatmentforrespiratoryinfections,diarrhoealdiseasesandskindiseasesthatarecausedbythepoorhygieneandsanitationconditionsoftheslum.
Eachdayaround280peoplecomethroughthetriageroom,withthemajorityseekingtreatmentforupperandlowerrespiratorytractinfections,diarrhoealdiseases,skininfections,diabetesandhypertension.
Theclinichasa24-hourmaternitywardwhichincludesthreedeliverybedsandsixpost-natalbeds.Everyweek,around45babiesareborn.AsmanyofthelocalresidentsareHIVpositive,theclinicprovidescaretohelppreventbabiescontractingthevirusfromtheirmothers.
Chaniya,a26yearoldmothersaid,“Ihavecometobringmychildforimmunisation.AsamotherlivingwithHIVsince2008,theclinichasplayedabigroleintesting,counsellingandhelpingmetodeliverHIVnegativechildren.IhavelearntfromthestaffherethatbeingHIVpositiveisnottheendofmylife,Icanlivelonger,givebirthandbringupmychildreninahealthyway.”
Thecentreisalsoequippedwithafullyfunctioninglab,abletodobloodanalysisandtestsfortuberculosis.ThelaboratoryallowspeopletogettestedforHIVandTBandtostartontreatmentassoonaspossible.TheearlierthatpeoplereceivethecorrectdiagnosisandtreatmentforTB,thebettertheirchanceofbeingcuredandthesoonertheystopbeinginfectious.
AftermorethantwentyyearsofworkinginKibera,MédecinsSansFrontièresisplanningtohandoveritsmedicalactivitiestothelocalhealthauthoritiesin2017,andatthetimeofwriting,isworkingwiththemtomakesurethatthemedicalservicescancontinue.
Patientnameshavebeenchanged.

CHOPPED
BenGuptaisanAnaesthetist.HereherecountshistimeworkingwithMédecinsSansFrontièresinPapuaNewGuineahelpingvictimsof
violence.
I’VEBEENWORKINGasananaesthetistforMédecinsSansFrontièreshereintheSouthernHighlandsofPapuaNewGuinea(PNG)forfivemonthsalready,butthescenerystillhasthepowertoleavemebreathless.Thinkoftheword‘paradise’andyou’dprobablypicturealandscapesomethinglikethis.
Unfortunately,thisstunningscenerywasnottobethemostmemorableaspectofmyday.AsIgotbacktothehospitalaroundmidday,Max,theMédecinsSansFrontièressurgeon,cameouttomeetmewithagrimlookonhisface.
“Sorrymate,we’vegottogototheatrenow,”hesaid.“Awoman’sjustbeenbroughtin.She’sbeenchopped.”
Myheartsank.InthelocalPidginEnglish,‘chopped’meansattackedwithamachete.Irushedinsideandgotchanged.
Evenafterfivemonths,dealingwiththerepercussionsofthisviolenceonadailybasisneverfeltnormal.Ithad,however,becomedepressinglyfamiliar.AsIscrubbedup,Iwonderedhowsuchextremeandendemicviolencecouldexistinsuchanidylliclandscape,populatedbysuchfriendly,openpeople.
Lucy,oneofthelocaltheatrenurses,wasattendingtothewomanasshelayquietlyononeofthebedsoutsidetheatre.Shehadalreadyappliedpressuredressingstothewoman’sarmsandheadandwastalkingtohergently.
Despiteallthebandages,IfeltpositivewhenIsawher.ShewasalertandansweringquestionsfromLucy,asignthatsheprobablyhadn’tlosttoomuchblood.Shealsodidn’thaveanyfacialinjuriesthatwouldleaveherwithpermanentdisfigurement.
WetookherthroughtotheoperatingtheatreandIputalocalanaestheticblockintonumbherarm.Whilewewaitedforherarmtogonumb,Lucycleanedherhead-woundandchattedtoherinHuli,thelocaltriballanguage.Shetoldusherstory.
Itturnsoutshehadbeenarguingwithherbrotheraboutmoneywhen,withoutwarning,

hehadtakenamachetetoherheadandarms.
Thesurgeon,Max,beganremovingthebandagesfromhernumbarmwhileLucycontinuedtotranslate.Suddenlyhestoppedwhathewasdoing.Ilookedoverandsawthatunderneaththebandagethewoman’shandwasalmostcompletelyamputated,barelyhangingonbyatinystripofskin.
TherewasasplitsecondofsilencebeforeMaxgentlyexplainedtothewomanthatherhandcouldnotbesaved.
Wethengotonwiththejobofrepairingwhatwasleftofherforearm.Ittookusafewhours,butwemanagedtorepairmuchofthedamageandtidyupsomeofthemessthemachetehadmade.Afterthewomanhadbeenwheeledawaytotheward,wecleanedupandleftthetheatreinsilence.Noneofusfeltliketalking.
Overthefollowingweeksitwasgratifyingtoseeherslowlybutsurelymakingafullrecovery.WiththehelpoftheprofessionalpsychologicalsupportprovidedbyMédecinsSansFrontières,shealsobegantointeractmorewithstaffandevenoccasionallytosmile.
Therearenoquicksolutionsoreasyfixesfortraumalikethat,justastherearen’tanyforasocietywhereviolencehasbecomesuchanacceptedpartofdailylife.ButIhopethatbybeingthere,byprovidingmuchneededmedicalcare,wearehelpingtomakearealdifferencehere.Suchabeautifulcountryandsuchbeautifulpeopledeservethebestwecangive.
IknowthatifMédecinsSansFrontièreswasn’tinTariprovidingemergencysurgicalcare,thenalotofpeoplewhohavebeenattacked,woundedandmaimedinthisareaoverthelastfewyearswouldalmostcertainlyhavedied.

FRIDGESINTHEFOREST
ThisisafirsthandaccountfromWilliamTurnerofhistimeworkinginaMédecinsSansFrontièresmobileteaminremoteareasoftheDemocratic
RepublicofCongo.
©JohnStanmeyer
UNDERANYCIRCUMSTANCES,it’snotaneasytasktravellingalongmuddyrainforesttracksbymotorbikeandcrossingswollenriversbydugoutcanoes.Nowimaginedoingitwhilecarryingarefrigerator.ThisisexactlywhatmyteamandIdidaswemountedanexpeditiontotest40,000peopleinremotevillagesoftheDemocraticRepublicofCongo(DRC)forsleepingsickness.
ThemissiontookustothetownofBili,inthefarnorthofthecountry.BilisitsinaheavilyforestedareabetweentheriverUéléandtheborderwithCentralAfricanRepublic.Theareaisaglobalhotspotforsleepingsickness.Infact,some85percentofallsleepingsicknesscasesarefoundintheDRC.Buttheregionissoinsecureandremotethattheproblemhaslonggoneignored.

InearlyApril2013,ourMobileHAT(HumanAfricanTrypanosomiasis)TeaminstalledalaboratoryandtreatmentwardinBilihospitalandbegantestinglocalpeopleforthedisease.Oncetheentirepopulationofthetownwastested,theteamturneditsfocustoabout50othervillageslocateddeepinthesurroundingrainforest.
Theteamwasontheroadforaboutthreetofourweeksinarow.Sometimeswerodeonmotorbikestomakeourwayalongbarelyaccessiblepathsthroughtheforest.Wemovedfromvillagetovillageandsleptintentseverynight.
Thelogisticalchallengesareenormous.ItcantakeuptoamonthforsuppliestoreachBili.Smallplanes,landingonanimprovisedairstripintheforest,canbringinonlylimitedquantitiesofsupplies.Truckscarryingthecargo-whichincludessensitivetoolssuchasmicroscopesandcentrifuges-havetobeferriedacrossriversonrafts,whilemuddytracksareoftenblockedbytoppledtrees.Duringtherainyseason,manyofthevillagesarecompletelyunreachable.
Ontopofthis,thetestforsleepingsicknessiscomplex,withseveralcomponentsthathavetobekeptcoolatalltimes.Eveninthemostremoteareas,theteamstravelledwithageneratorandrefrigerators.
TheMobileHATTeamhavealsospentninemonthsinSouthSudan,anothersleepingsicknesshotspotthat’sstrugglingtoovercometheeffectsofdecadesofconflict.TheteamtargetedvillagesacrossCentralandWesternEquatoriastates,wheresleepingsicknessrateshadpreviouslybeenveryhigh.
Travellingthousandsofkilometresfromvillagetovillage,theteamscreenedmorethan60,000people.Thirty-eightconfirmedcaseswereidentifiedandtreated,indicatingthegoodnewsthattheprevalenceofsleepingsicknessintheseareashasdecreasedsignificantly.
Inadditiontoscreeningpatients,MédecinsSansFrontièreshasalsoworkedtoimproveourscreening,diagnosis,andtreatmentcapacities.Morethan200SouthSudanesestaffreceivedtrainingthattheywillbeabletoputintopracticeintheyearstocome.
Byscreeningandtreatingpeopleoverawidearea,wesavelives,firstandforemost,butwealsoreducetheprevalenceofthedisease.Eachpersontreatedisastepintherightdirection.
Butthedifficultterrain,unwieldykit,andregionalinsecurityarenottheonlychallenges.Untiltherearesimplerandmoresuitablediagnostictoolsandtreatments,anddependablefundingfornationalprograms,eliminatingthediseasewillcontinuetobeanuphillstruggle.

THEBUZZINGOFHELICOPTERS
Thisstoryshowsthemagnitudeofthefear,thepainandthesilencethataffectcommunitiesintheCaucaMountainsinColombiaand
demonstratestheirneedforpsychologicalsupporttohelpthemhealtheinvisiblewoundsandsufferingcausedbyongoingconflict.
©AnnaSurinyach
“WHENTHEFIGHTINGstarts,yousay,ohmyGod,andyourushthiswayandthatinapanictogethomeandshutyourselfinside,andthebulletswhistleoverthehouse.Thechildrenclingtoyourlegsandscreamwhentheyhearahelicopter,”saysManuela.“It’shorribletolivelikethat,andthisisthelifewearelivingherethroughouttheCaucadepartment.”
Manuelahasbeendisplacedseveraltimesbythearmedconflictbetweenarmedgroupsandthegovernmentalforcesthathasbeengoingonforthelast50yearsinColombiainvariousregionsofthecountry.

Despitethedecreaseintheamountofharassment,attacksandfighting,thepeoplecontinuetoliveinfear,painandsilenceintheCaucamountainsinthesouthofColombia.
Itisoneoftheareasinthecountrywiththemostarmedactivity.Theinhabitantsareaccustomedtothesoundofbulletsandthebuzzingofhelicopters.Theyruntohideintheirhousesorareforcedtomovetootherplaceswiththeirfamiliesuntiltheviolencestopsandtheycanreturn.
ItwasonsuchadaythatthebulletsshatteredthelivesofManuelaandherhusbandRicardooneyearago.Asusual,RicardowassowingcoffeeinhisfieldinthevillageinCauca.
“Aroundtwoo’clock,theshootingfromthefrontstarted.Weliveinbetweentwohillsandourhouseandourfieldareinthemiddlewhenthereisfighting.Welockedourselvesupinourhousetohavelunch.Forty-fiveminuteslatereverythingseemedcalmandmyhusbandwentoutsidetofeedthedog,”recallsManuelawithaseriousface.Hewashitbyabulletandfellatthefeetofhissix-year-olddaughter,whoranintothehousecrying,thinkingthatherfatherwasdead.
Thebulletenteredthroughhisfaceandexitedthroughhisribs,splittinghiscollarboneandleavinghisarmdisabledforlife.“Ican’tdothingsbymyselfanymore,nowIcan’twork.Ican’tholdanythinginmyhandforlong,”addsRicardoshyly,whileshowinghisscars.Untilthen,hehadbeenthefamilybreadwinner.Nowhecan’tevenaffordthetransporttoseethespecialist,whoisfivehoursawayfromhishouse.
Manuelaescapedthebulletsbutsufferspost-traumaticstress.“Wewereveryaffectedpsychologicallybywhathappened.Iwascryingallday.Wewerefightingandfedup.Evenourdaughterisnotwell,sheisbehindinschool,”saysManuela.
“Whenshehearsahelicoptershegoesstraighttothehouseandshetellsmetohideorshesays‘Daddy,thebadguysarecoming,’addsRicardo.Thegirlisfrightened.”
Thearmedconflicthasleftthemostdirectlyaffectedpeoplepsychologicallyscarredforyears.However,accesstomentalhealthintheseisolatedvillagesofthemountainsisnon-existent.Therearenoavailablepsychologiststodoindividualconsultationsattheprimarycarelevelnorinthemunicipalhospitals,whichareoftensix-hoursawayonunpavedroutes.
MédecinsSansFrontièrespsychologistsdobothindividualandgrouptherapysessionsinthemunicipalhospitalsandvillagesintheCaucamountains.Inthisway,thedispersedpopulationsalsohaveaccesstopsychologicalcare.

Inadditionthepsychologistsworkwiththecommunityleaders,healthpromoters,midwivesandteachersonpreventionissues.Theobjectiveistotrainthemsotheycanidentifywhichpeopleneedtobetransferredtoapsychologistorapsychiatristandsothattheycanoffersomeimmediatepsychologicalprimarycarewhenthereisanepisodeofviolence.
“Manyofthepeoplewhohavesufferedsexualviolenceorarmedconflicteventsrecently,ornotsorecently,andwhosufferpost-traumaticstresshaveneverreceivedpsychologicaltreatment,”explainsJuliana,aMédecinsSansFrontièrespsychologistwhoworksinthearea.
Paula’shusbandwaskilledin2005.AnotherresidentoftheCaucaMountains,ittookhereightyearstoseeapsychologist.SheisnowacommunityleadertrainedbyMédecinsSansFrontières.
“TheytoldmeIshouldn´tlivewiththispainandthatIcouldovercomeit.Thetherapyhasgivenmemotivationandstrengthandtrainedmetobeabletogotothecommunitiesandtellthemtheycancarryon,”saysPaula.“Idon’thavethatfearanymoreandIhavemanagedtogetoverthedeathofmyhusband.”
Patientnameshavebeenchanged.

VICTORY
NurseFloraEscourroudescribesherfirstplacementwithMédecinsSansFrontièresineasternChadwhereshetookpartinameaslesvaccination
campaign.
©MSF
IARRIVEDINthecapital,N’Djamena,inmid-AprilandwiththeotherfourmembersoftheteamIsetoffontheroadtoAbéché.Thejourneywouldtaketwodaystocrossthecountryfromwesttoeast.
InAbéché,therehadbeenreportsofcasesofmeaslesforseveralmonthsandbyApril,theepidemichadreachedanalarmingscale.MeaslesisadiseasewhichisundercontrolinAustralia,butitcanleadtoseriouscomplications.Intheworst-casescenario,whenaccesstocareisinsufficient,mortalitycanclimbto20percent.Yet,

epidemicscanbeavoidedasthevaccineiseffectiveandinexpensive.ThepreviousvaccinationcampaignintheAbéchéregionhadbeencarriedoutin2009so,withthesubsequentbirths,thenumberofunprotectedchildrenhadbeensteadilyrising.
WhenwearrivedinAbéché,preparationswerealreadywellunderwayand26districthealthcentreswereapprovedtotakepartbythelocalauthorities.Wehadtwoweekstovaccinatenearly100,000children.
Ourfirsttaskwastorecruitlocalstafftohelpinthecampaign.BytheendofApril,wehadputtogetherandtrained14teamsofsixpeopleincludinganumberoflocalstudentnursescomplementedbymembersofthelocalcommunities.Eachteamhadtovaccinateanaverageof500childrenaday.
Eachmorningwemetat5amtofinalisetheroadmaps;thenthe14supervisorsarrived;afterthat,wecheckedthattheequipment,startingwiththerefrigeratedvaccines,hadbeenproperlyloadedintothejeeps;finally,theteamssetoffataround6am.
Forthefirstweek,Iwasresponsibleforsupervisingouroperations.Thedrivetothemostfar-flungvaccinationsitescouldtakeuptothreehours.Sometimesthingshadtobereorganised,suchasaskingthevillagechiefforextrasecuritypersonneltomanagethecrowds.
Onlychildrenagedbetweensixmonthsandfiveyearsreceivethejab,butmothersdon’talwaysknowtheexactageoftheirchild.Asarule,iftheyareoldenoughtohaveteeth,theyareincluded.Asanexception,childrenfromnomadiccommunitiesarevaccinatedupto15yearsofage,astheyoftenslipthroughtheroutinevaccinationprograms.
Thesecondweek,Iwasmoreinvolvedintreatingmeaslescasesthathadbeenflaggedbyourteams.Mothersdidn’talwaystaketheirchildrenwithmeaslestothevaccinationsite,forfearofcontagion.Thereisnospecifictreatmentagainstthevirus.Instead,wetacklethesymptomsoftheillnesswithantibiotics,paracetamolforthefeverandeyeointments.Nutritionalsupportisoftennecessarytoo,asmeaslesisamalnutritionriskfactor.Allthosetreatmentscanbeadministeredonthespot.
However,childrenwithcomplicationsweretakentoAbéchéhospital,whereweensuredthattheywouldreceivefreetreatment.Themostupsettingsymptomsarerespiratorydistressandconvulsions.Whenchildrenhavethesesymptoms,it’seasiertoconvincetheparentstotakethemtothehospital.Forpeopleaspoorasthosewewereworkingwith,itcantakesomepersuadingtogotoAbéchéandstayawayforseveraldays.So,evenwhenweofferedtotakeandbringbackthechildbyambulance,each

successfulnegotiationwasavictory.

GLORIOUSLYCALM
NurseEmmaPedley,describesherworkwithMédecinsSansFrontièresinCentralAfricanRepublic(CAR).MédecinsSansFrontièreshasbeen
workinginthecountrysince1997.SinceDecember2013,inresponsetothecrisis,wehavedoubledourmedicalassistanceinCARandare
runningadditionalprojectsforCentralAfricanrefugeesinneighbouringcountries.
©MSF
INADDITIONTOkeepingthehospitalandmedicalsupplysideofthingstickingover,IhavealsohadtheopportunitytotraveloutwithourmobileteamsafewtimessincecomingtoZemio,CentralAfricanRepublic(CAR).
MédecinsSansFrontièressupportsfoursmallhealthpostsacoupleofhoursalongthemainroadsleadingintoandawayfromZemio,andalargeroneinMbokwhichisawholeday’sdriveaway.Thevillageswesupportaresmallbutisolated.Malariaanddiarrhoeaarethemainkillersouthere,andit’salongwalktothehospitalinZemiowithoutthesecentres.
Ourdaystartsearly,6am,packingacarfullofequipmentandmakingsurewehaveallthenecessarysuppliestorestockthehealthposts.By7amweareonrouteoutofZemio,andthedayisalreadybeginningtogethot.
WepassfamilygroupsofPeuhl-largelynomadiccattleherderswhohavemigrated

downintoCARoverthelastfewdecadesfromChadandothernorthernAfricancountries.Wewavetothemoutofthevehiclewindowsaswepass.
Infactthewavingismoreorlessmandatory-it’spartofoursecuritybriefings,aswellasbeingcommonsensetobeentirelyfrank.MédecinsSansFrontières,bothforinformationandsafetypurposes,reliesonmaintainingcloseandfriendlyrelationswiththecommunitiesitserves.Andyouarefarmorelikelytothinkkindlyofastrangewhitefaceinacarasitpassesyouifitsmilesandwaves,thanifitignoresyou.
Thevillagesareinsmallclearingsintheforest.Noelectricityhere,nomusic,justthebackgroundnoisesofpeoplequietlygettingonwithlife-pumpingwater,sortinggrain,raisingchildren.It’sgloriouslycalmafterweeksspentatthehospitalinZemio.
MypartnerJulietakestheleadatthefirsthealthpost,deliveringrefreshertrainingondehydrationtreatmenttothestaffandgoingthroughtheirstatisticswiththem.Ipokearoundinthesmallmudwalledpharmacy,doinganinventoryandreviewingprescriptionswiththelocalpharmacist.
Afteracoupleofhourswepilebackintothecarandrattleofftothenextclinicwherewerepeattheperformanceandconsultonacoupleofcomplexandchroniccases.
Acertainhopelessfrustrationissharedbybothofusatthispoint-MédecinsSansFrontières’concernouthereisacuteandemergencycareonly,andwehavelittleornoaccesstomedicationsandtreatmentforthingslikearthritisandheartfailure.
Thereissomethingdeeplyunjustaboutseeingthedignifiedolderpeopleofthesecommunities-whohavesurvivedsomuchintheirlifetimes,yetaresomehowsoneglectedintheirlastdays.
SlowlytheshadowslengthenandthecarbeginstoslowdownaswebegintopassthroughtheoutskirtsofZemioandthehutsbecomemorecloselyspacedtogether.Thevibrantgreensoftheforestcounterparttotherichochreofthedirtroad,andinplacesdizzyinglybeautifulcloudsofenormousbutterfliesscatteroutfromtheundergrowthaswebarrelpast.
Aslonganddrainingbothphysicallyandsometimesemotionallyasthejourneysare,theyarealsoincrediblybeautiful.

QUADRUPLETS
DrAoibhinnWalshisaPaediatricianfromDublinwhowasworkingwithMédecinsSansFrontièresinTimergarainnorthwestPakistan.Hereshedescribesthelasttwodaysofhermission.MédecinsSansFrontièreshasbeenpresentinPakistansince1986,workingwithPakistanicommunities
andAfghanrefugees.
©MSF
IAMLEAVINGtheprojecthereinTimergaraintwodays.Ithasbeenalongeightmonths,andforthemajorityoftimeIhavespenthereIhavebeeninthemotherandchildhealthcentrerunbyMédecinsSansFrontièresatTimergaraDistrictHospital.
AsaPaediatrician,myjobprimarilyhasbeentocareforthebabiesborninthisdepartment,andspendingsomuchtimeherehasgivenmeinsightintothestoriesofthewomenhere,bothourstaffandpatients.Onethingthatwillforeverstaywithmeisthestrengthofthesewomen.Theytakeeverythingintheirstrideandwhenadifficultsituationarises,insteadofcomplainingtheyjustsimplyact.Ihavebeenprivilegedduringmytimeheretobearwitnesstosomeofthestoriesofthesewomen,someofthemheartbreakinglytragic,someupliftingandhopeful.Therearetoomanytorecount.HoweveronSaturdaymorningsomethinghappenedinthecentrethatwasnothingshortofmiraculousandreallymademesoproudtohavebeenpartoftheteamevenforashortperiodoftime.
Therewerefourstaffondutyfordeliveries-Gulnaz,Rabia,LubnaandAsma.Awomancameinat4am,inactivelabour,fullydilatedandreadytodeliver.Shehadone

five-year-oldboyathomeandhadpreviouslyhadtwinsdieinthefirstfewhoursoflifeaftercaesareansection.Shetoldthestaffthatshewas33weekspregnantwithquadruplets!
IcanonlyimaginethepanicanddramathatwouldhaveensuedhadthisoccurredinahospitalathomeinIreland.Multiplebirths,particularlyprematurebabies,areincrediblyhighriskforbothmotherandbabies.Ifpossiblethebabiesaredeliveredduringthedayviaaplannedcaesareansectionwithmidwives,paediatricians,obstetricians,andpaediatricnursesallpresent.Usuallythereareatleasttwomedicalstaffperbabyinthedeliveryroom.
Here,withthisnotavailableorpossible,thecentrestaffdidwhattheyalwaysdo:theytookitintheirstride.Allfourbabiesweredeliveredsafeandwellwithintwentyminutes.Twobabiesdeliveredheadfirstandtwoweredeliveredbreech(feetfirst),anothertechnicallydifficultachievement.Thenurseworkingintheneonatalwardwascalleddownandallfourbabiesweresooncosilyensconcedtogetherintheneonatalunit.
Meanwhile,themotherwenttotheoperatingtheatreasshehadexperiencedsomebleedingafterdelivery,whichistobeexpectedaftersuchadramaticdelivery.Thetotalweightofthebabiesamountingto8.2kilograms!
Icametothehospitalthenextmorningtofindthesefourbeautifulbabieswaitingforus.Seeingthelookonthemother’sfacewhenweinformedherthatallthebabieswerehealthyandstablewillbeamemoryIcarrywithmeforever.ItwillremindmeofwhythecentreissoimportanthereinTimergara.Itgivesthesewomenachancetohavetheirbabiessafely,inanenvironmentwheremotherandchildwillbegivenahighstandardofcare.Italsoleavesmeinaweofwhattheteamachieves,inaplacewithlimitedresourcesandwheretheenormousvolumeofcomplicateddeliveriescouldeasilyoverwhelmandpaniceventhemostexperiencedpeople.Insteadtheyunfailinglycontinuetotakecareoftheirmothers,sisters,auntsanddaughters,andprovethatmomentslikethebirthofthesefourbabiesarepossibleanywherewiththerightamountofknowledge,passionandskill.

©AoibhinnWalsh

CONCLUSION
Ifyouhavereadthisbookfromstarttofinish,younowhaveaninsightintotheworkofMédecinsSansFrontières.
Despiteharshterrainandclimate,riskofviolenceandillnessandanynumberofotherdifficulties,MédecinsSansFrontièresteamsdelivermedicalassistancetovulnerablepeoplearoundtheclock,aroundtheworld.
Pleasesharethisbookwithyourfriendsandfamily.
Ifyouchoosetoalsomakeadonation,yourgiftwillbeusedtodelivermedicalaidtopatientslikeRukhshona,Aisha,RahimandthemillionsofothersthatwillbeassistedbyMédecinsSansFrontièresinthecomingyear.

MEDECINSSANSFRONTIERESCHARTER
MédecinsSansFrontièresisaprivateinternationalassociation.Theassociationismadeupmainlyofdoctorsandhealthsectorworkersandisalsoopentoallotherprofessionswhichmighthelpinachievingitsaims.Allofitsmembersagreetohonorthefollowingprinciples:
• MédecinsSansFrontièresoffersassistancetopopulationsindistress,tovictimsofnaturalorman-madedisastersandtovictimsofarmedconflict,withoutdiscriminationandirrespectiveofrace,religion,creedorpoliticalaffiliation.
• MédecinsSansFrontièresobservesneutralityandimpartialityinthenameofuniversalmedicalethicsandtherighttohumanitarianassistanceanddemandsfullandunhinderedfreedomintheexerciseofitsfunctions.
• MédecinsSansFrontières’volunteersundertaketorespecttheirprofessionalcodeofethicsandtomaintaincompleteindependencefromallpolitical,economicandreligiouspowers.
Asvolunteers,membersareawareoftherisksanddangersofthemissiontheyundertake,andhavenorighttocompensationforthemselvesortheirbeneficiariesotherthanthatwhichMédecinsSansFrontièresisabletoaffordthem.