no longer chronic subjective dizziness: new insights into ... · ©2013 mfmer | slide-1 no longer...
TRANSCRIPT
©2013 MFMER | slide-1
No Longer Chronic Subjective Dizziness:
New Insights into the Mechanisms of Persistent Vestibular Symptoms
Jeffrey P. Staab, MD, MSAssociate Professor of Psychiatry
27 April 2016
British Society of AudiologyAnnual Conference
©2013 MFMER | slide-2
Disclosures
• Commercial support
• None
• Grant support
• US National Institutes of Health
• Mayo Clinic
• Disclaimer
• Chair, Behavioral Subcommittee
• Committee for Classification Vestibular Disorders of the Bárány Society (CCBS)
• Off-label medical use
• No medications are approved by any regulatory agency to treat functional vestibular disorders.
• SSRIs/SNRIs for persistent postural-perceptual dizziness

©2013 MFMER | slide-3
Overview
1. Review history of physical & psychological interactions in patients with vestibular and balance symptoms
• 19th century observations
• 20th century symptoms and syndromes
• 21st century classification
2. Describe emerging data on pathophysiologic mechanisms
• Clinical applications – evaluation, education and treatment
3. Guiding principle
“Patients want an explanation for their suffering, but do not want to be laughed at, or worse, considered to be insane.”
- Carl Westphal, 1871

©2013 MFMER | slide-4
Die Agoraphobie (fear of marketplace)
Kuch and Swinson, Can J Psychiatry, 1992
“Patients find it impossible to cross open squares and walk along certain streets. Fear restricts their mobility, [but] they insist that they are not aware of any reasons for their anxiety. It seems to arise as an alien force as soon as a square is crossed or approached. With the anxiety, as part of one process, occurs the thought of not being able to cross and a perception of an enormous expanse of space.”
Carl Westphal, 1871
“cross squares and
walk along streets”
“Fear restricts
mobility”
“thought of not being
able to cross”
“enormous expanse of
space”
Locomotion
Conscious motor
control
Spatial
orientation
Instinctive threat
response
“part of one process”
©2013 MFMER | slide-5
19th century
20th century
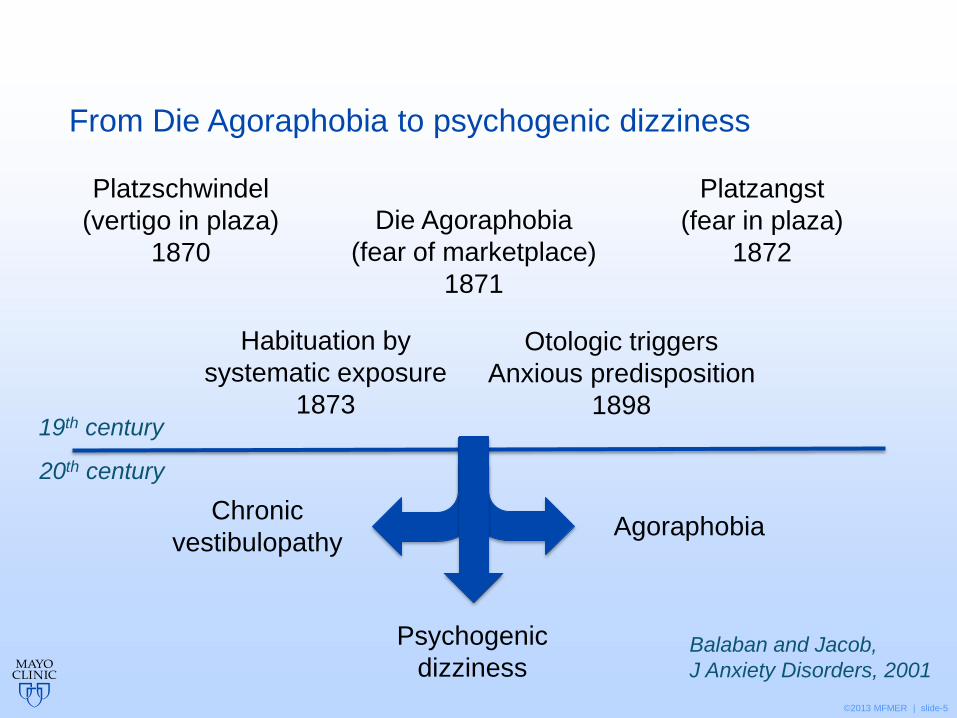
From Die Agoraphobia to psychogenic dizziness
Psychogenic
dizziness
Die Agoraphobia
(fear of marketplace)
1871
Platzschwindel
(vertigo in plaza)
1870
Platzangst
(fear in plaza)
1872
Otologic triggers
Anxious predisposition
1898
Habituation by
systematic exposure
1873
Chronic
vestibulopathyAgoraphobia
Balaban and Jacob,
J Anxiety Disorders, 2001
©2013 MFMER | slide-6
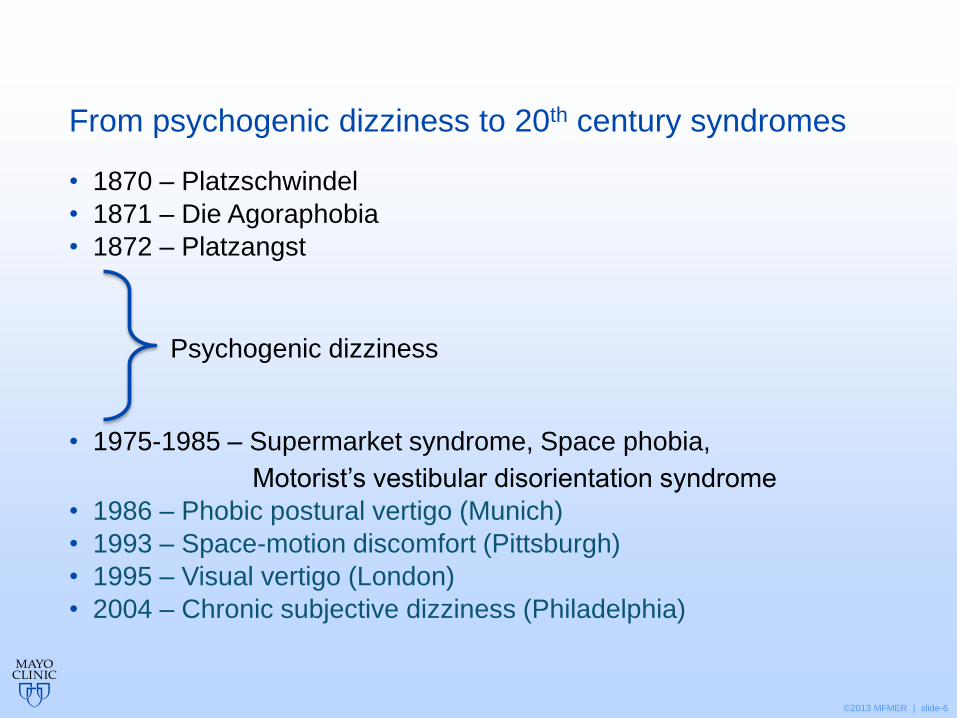
From psychogenic dizziness to 20th century syndromes
• 1870 – Platzschwindel
• 1871 – Die Agoraphobia
• 1872 – Platzangst
• 1975-1985 – Supermarket syndrome, Space phobia,
Motorist’s vestibular disorientation syndrome
• 1986 – Phobic postural vertigo (Munich)
• 1993 – Space-motion discomfort (Pittsburgh)
• 1995 – Visual vertigo (London)
• 2004 – Chronic subjective dizziness (Philadelphia)
Psychogenic dizziness
©2013 MFMER | slide-7
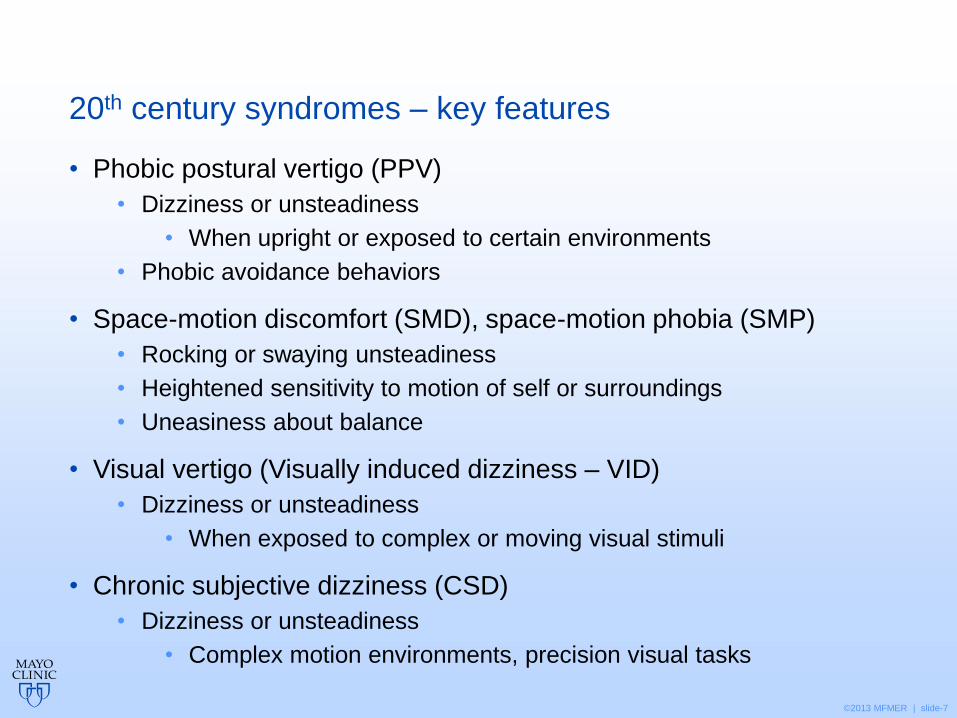
20th century syndromes – key features
• Phobic postural vertigo (PPV)
• Dizziness or unsteadiness
• When upright or exposed to certain environments
• Phobic avoidance behaviors
• Space-motion discomfort (SMD), space-motion phobia (SMP)
• Rocking or swaying unsteadiness
• Heightened sensitivity to motion of self or surroundings
• Uneasiness about balance
• Visual vertigo (Visually induced dizziness – VID)
• Dizziness or unsteadiness
• When exposed to complex or moving visual stimuli
• Chronic subjective dizziness (CSD)
• Dizziness or unsteadiness
• Complex motion environments, precision visual tasks

©2013 MFMER | slide-8
Four blind men and an elephant
a hose
a tree
a rope
a fan
©2013 MFMER | slide-9
Four research groups and a syndrome
Visual vertigo
Phobic postural vertigo
Chronic
Subjective
Dizziness
Space-motion discomfort
©2013 MFMER | slide-10
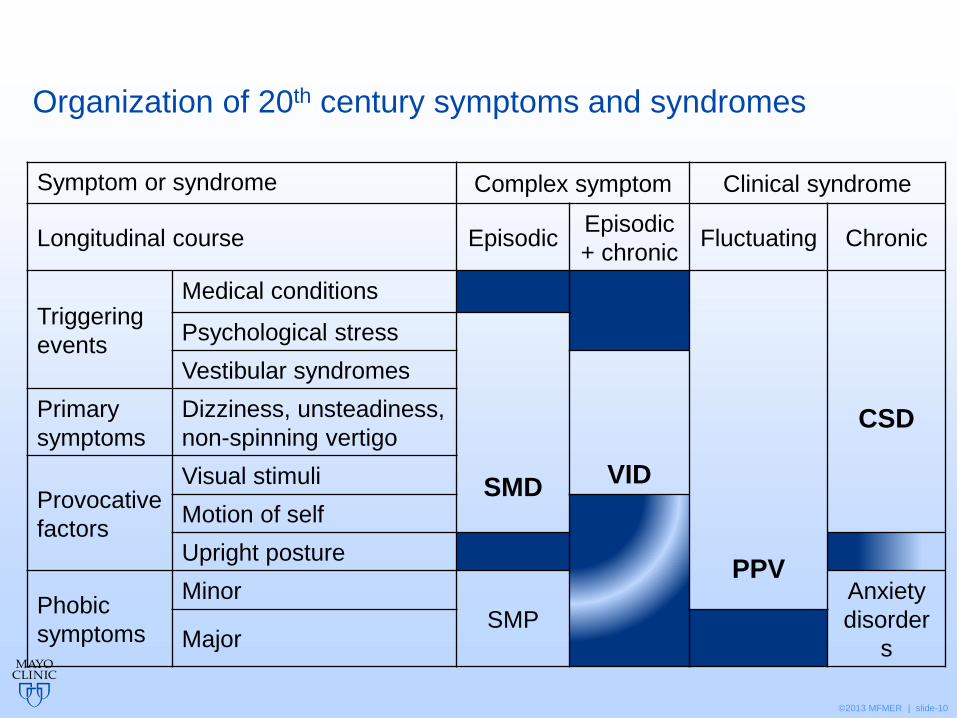
Organization of 20th century symptoms and syndromes
Symptom or syndrome Complex symptom Clinical syndrome
Longitudinal course EpisodicEpisodic
+ chronicFluctuating Chronic
Triggering
events
Medical conditions
PPV
CSD
Psychological stress
SMD
Vestibular syndromes
VID
Primary
symptoms
Dizziness, unsteadiness,
non-spinning vertigo
Provocative
factors
Visual stimuli
Motion of self
Upright posture
Phobic
symptoms
Minor
SMP
Anxiety
disorder
sMajor

©2013 MFMER | slide-11
Classification of 21st century functional vestibular disorders
Persistent postural-perceptual dizziness (PPPD)Phobic postural dizziness (PPD)
Functional vestibular disorders
Longitudinal coursePersistent with
situational provocation
Triggering
events
Vestibular syndromes
PPPD
PPD
Psychological stress
Other medical conditions
Primary
symptoms
Dizziness, unsteadiness,
non-spinning vertigo
Provocative
factors
Visual stimuli
Motion of self
Upright posture
Phobic
symptoms
Minor
Major Anxiety disorders

©2013 MFMER | slide-12
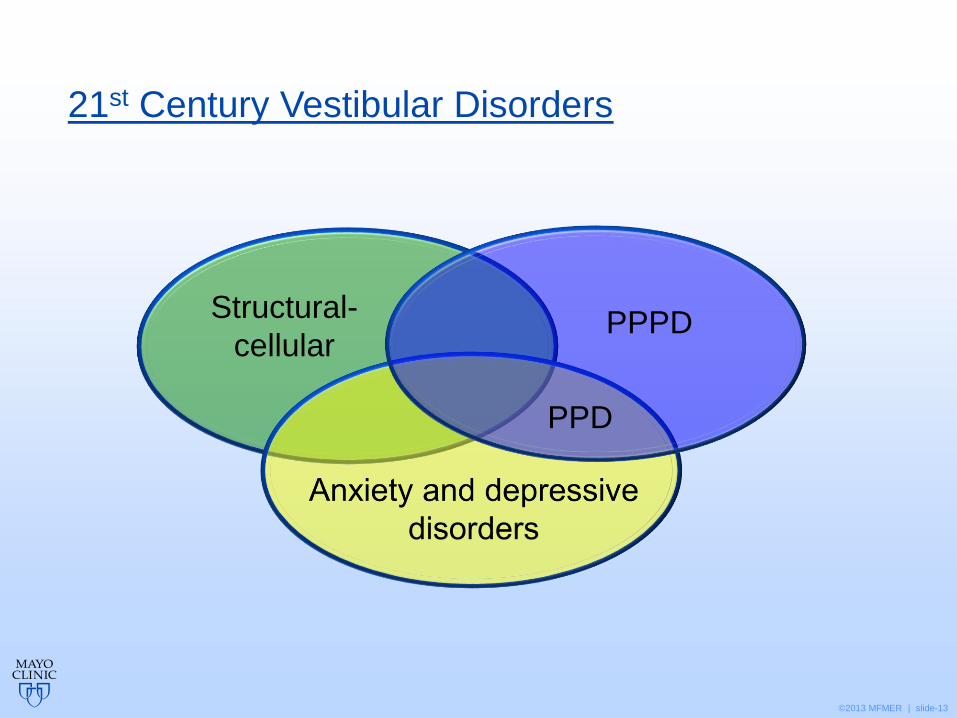
Structural-
cellularFunctional
21st Century Vestibular Disorders
Dieterich, Staab, Brandt, “Dizziness” in Hallett et al., eds.,
Functional Neurologic Disorders, in press
©2013 MFMER | slide-13
Structural-
cellularPPPD
21st Century Vestibular Disorders
PPD

©2013 MFMER | slide-14
A. One or more symptoms of dizziness, unsteadiness, or non-spinning vertigo are present on most days for 3 months or more.1,2
1. Symptoms are persistent, but wax and wane.
2. Symptoms often increase as the day progresses, but may not be active throughout the entire day.
3. Momentary flares may occur spontaneously or with sudden movements.
B. Symptoms are present without specific provocation, but are exacerbated by:3
1. Upright posture,
2. Active or passive motion without regard to direction or position,
3. Exposure to moving visual stimuli or complex visual patterns.4
Persistent Postural and Perceptual Dizziness (PPPD)
1 Symptoms must be present for more than 15 of every 30 days. The
overwhelming majority of patients experience daily symptoms.
2 Symptoms need not be continuous, but must be present for prolonged (hours-long) periods throughout the day. Momentary symptoms alone do not fulfill this criterion.
3 Factors B.1.-3. may not be equally provocative.
4 Provocative visual stimuli may be encountered during performance of sedentary activities that require sustained visual focus.

©2013 MFMER | slide-15
C. The disorder typically begins shortly after an event that causes acute vestibular symptoms or problems with balance.5
1. Precipitating events include acute or episodic vestibular syndromes, other neurologic or medical illnesses, and acute psychological distress.
2. Symptoms usually are present from initial onset as described in criterion A, but they may occur intermittently at first, and then consolidate into a persistent course.
3. A slow, gradual onset occurs less often.
D. Symptoms cause significant distress or functional impairment.
E. Symptoms are not better attributed to another disease or disorder.6
Persistent Postural and Perceptual Dizziness (PPPD)
5 The most common precipitating events are peripheral or central vestibular conditions, vestibular migraine, panic attacks or generalized anxiety with dizziness, concussion, orthostatic intolerance, and dysrhythmias. It may not be possible to identify a specific trigger in all cases. Slow onset occurs with slowly developing triggers.6 PPPD may co-exist with other diseases or disorders. Evidence of another active illness does not necessarily exclude this diagnosis, but may indicate the presence of a comorbid condition.

©2013 MFMER | slide-16
PPPD (CSD) – Triggering events
Anxiety disorder
- panic attacks 15%
- generalized anxiety 15%
Acute vestibular syndromes
- with/without secondary anxiety 25%
Neurologic Illnesses
- migraine 20%
- traumatic brain injury 15%
- orthostatic intolerance 7%
Other Medical Conditions
- dysrhythmias, adverse drug reactions 3%
Staab & Ruckenstein,
Arch Oto-HNS, 2007
N=345
©2013 MFMER | slide-17
Pathophysiologic mechanisms – emerging data
1. High demand postural control strategy
• Stiffened – high frequency, low amplitude sway
• Lower threshold for closed loop feedback
2. Altered sensory integration
• Visual dependence
• Somatosensory dependence
3. Increased involvement of threat (anxiety) systems
• Initial process – high initial anxiety drives #1 and #2
• Sustaining mechanism – failure to readapt
©2013 MFMER | slide-18
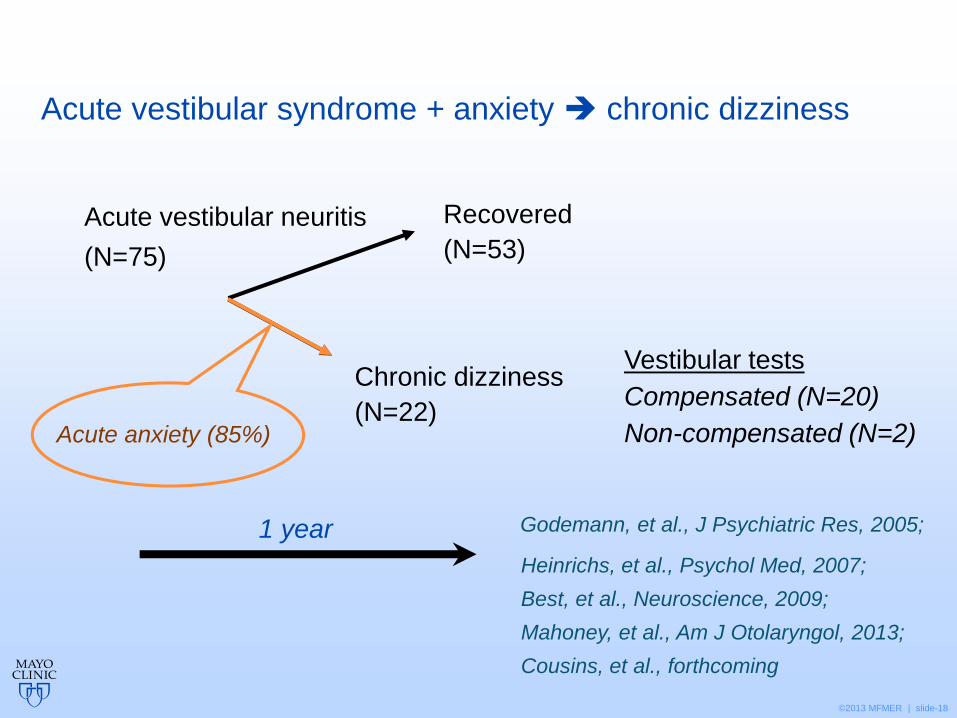
Acute vestibular neuritis
(N=75)
Vestibular tests
Compensated (N=20)
Non-compensated (N=2)
Recovered
(N=53)
Chronic dizziness
(N=22)
1 year
Heinrichs, et al., Psychol Med, 2007;
Best, et al., Neuroscience, 2009;
Mahoney, et al., Am J Otolaryngol, 2013;
Cousins, et al., forthcoming
Acute anxiety (85%)
Acute vestibular syndrome + anxiety chronic dizziness
Godemann, et al., J Psychiatric Res, 2005;
©2013 MFMER | slide-19
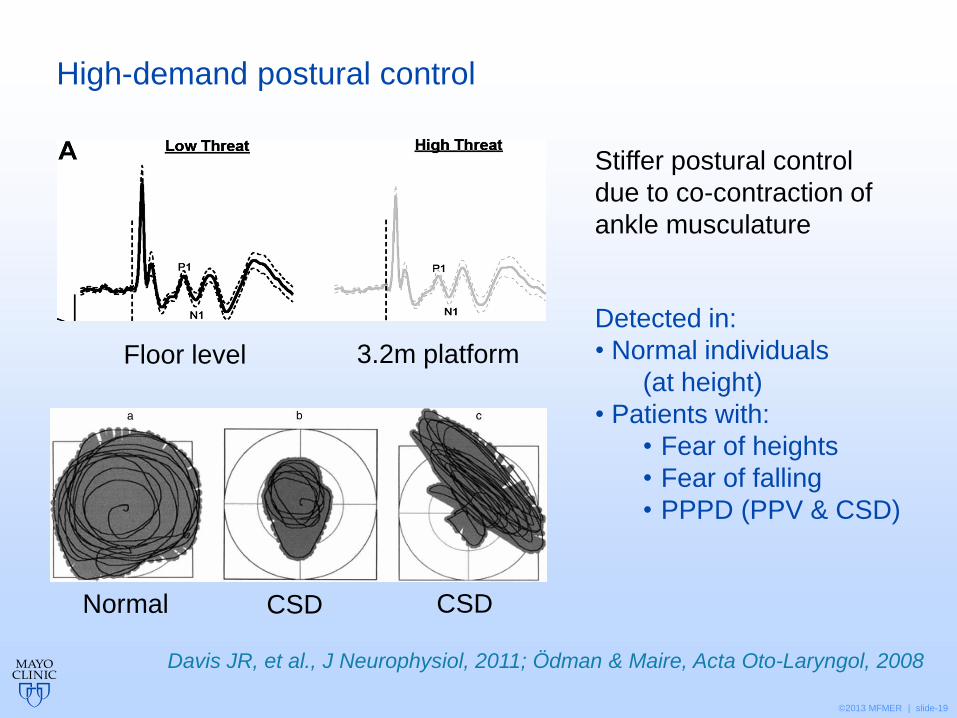
High-demand postural control
Davis JR, et al., J Neurophysiol, 2011; Ödman & Maire, Acta Oto-Laryngol, 2008
3.2m platformFloor level
Stiffer postural control
due to co-contraction of
ankle musculature
Normal CSD CSD
Detected in:
• Normal individuals
(at height)
• Patients with:
• Fear of heights
• Fear of falling
• PPPD (PPV & CSD)
©2013 MFMER | slide-20
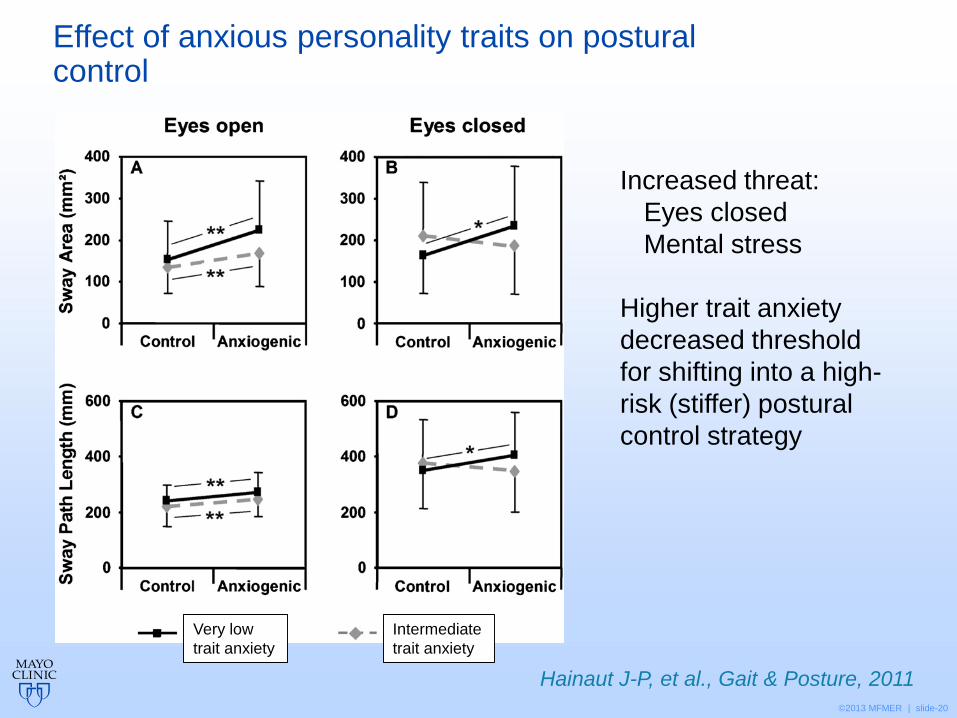
Effect of anxious personality traits on postural control
Hainaut J-P, et al., Gait & Posture, 2011
Increased threat:
Eyes closed
Mental stress
Higher trait anxiety
decreased threshold
for shifting into a high-
risk (stiffer) postural
control strategy
Very low
trait anxiety
Intermediate
trait anxiety

©2013 MFMER | slide-21
Increased visual dependence in patients with persistent dizziness handicap
Cousins, et al., PLoS 2014;
Cousins, et al., forthcoming
Prospective follow-up:
6 months after acute
vestibular neuritis
Primary predictor of
visual dependence:
Acute anxiety
©2013 MFMER | slide-22
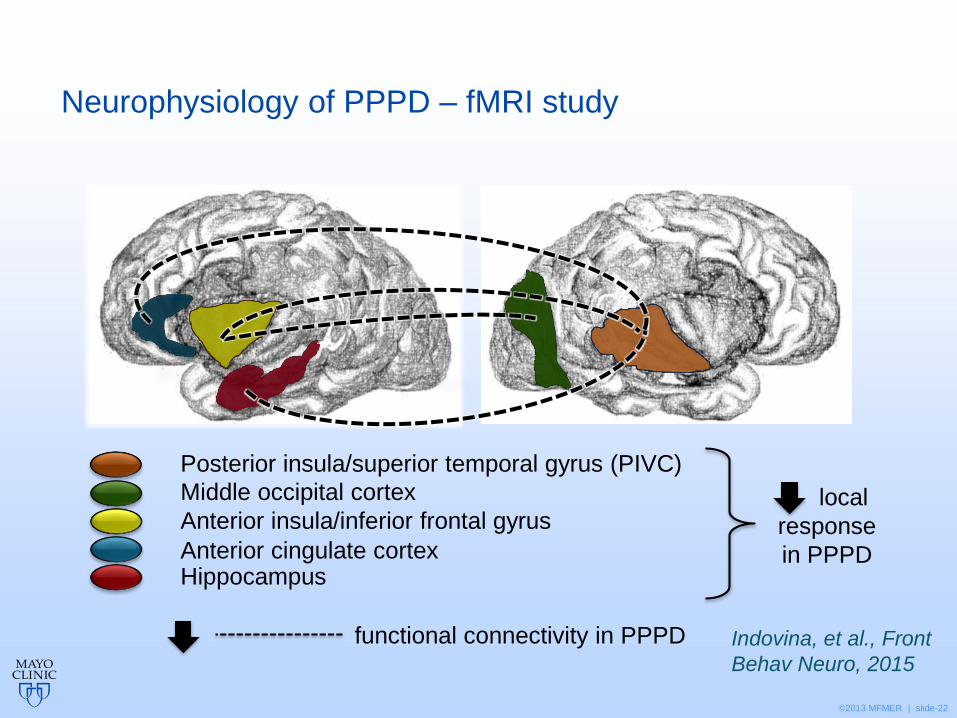
Neurophysiology of PPPD – fMRI study
Anterior insula/inferior frontal gyrus
Posterior insula/superior temporal gyrus (PIVC)
Middle occipital cortex
HippocampusAnterior cingulate cortex
local
response
in PPPD
functional connectivity in PPPD Indovina, et al., Front
Behav Neuro, 2015
©2013 MFMER | slide-23
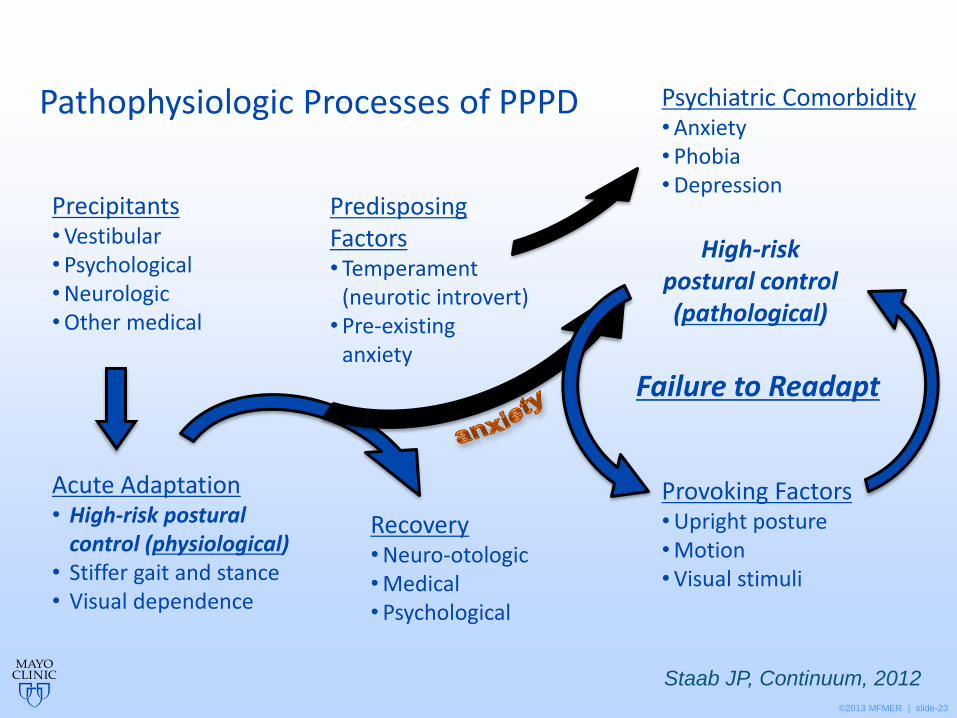
Recovery• Neuro-otologic• Medical• Psychological
Pathophysiologic Processes of PPPD
Staab JP, Continuum, 2012
Psychiatric Comorbidity• Anxiety• Phobia• Depression
Provoking Factors• Upright posture• Motion• Visual stimuli
High-risk postural control (pathological)
Failure to Readapt
Precipitants• Vestibular• Psychological• Neurologic• Other medical
Predisposing Factors• Temperament
(neurotic introvert)• Pre-existing
anxiety
Acute Adaptation• High-risk postural
control (physiological)• Stiffer gait and stance• Visual dependence
©2013 MFMER | slide-24
Treatment – Education & Physical Therapy
• Retrospective review N=26 – home exercises after 1 PT visit
• Education about the disorder
• Normal and high-risk postural control strategies
• Failure to readapt
• 22/26 – helpful or very helpful
• Vestibular habituation therapy
• Plan -- habituation exercises
• Head/body movement and visual stimuli
• Performed twice daily at home
• Follow-up at 6+ months (mean 27.5 mo)
• 14/26 – helpful or very helpful
Thompson, et al., J Vest Res, 2015
©2013 MFMER | slide-25
0
5
10
15
20
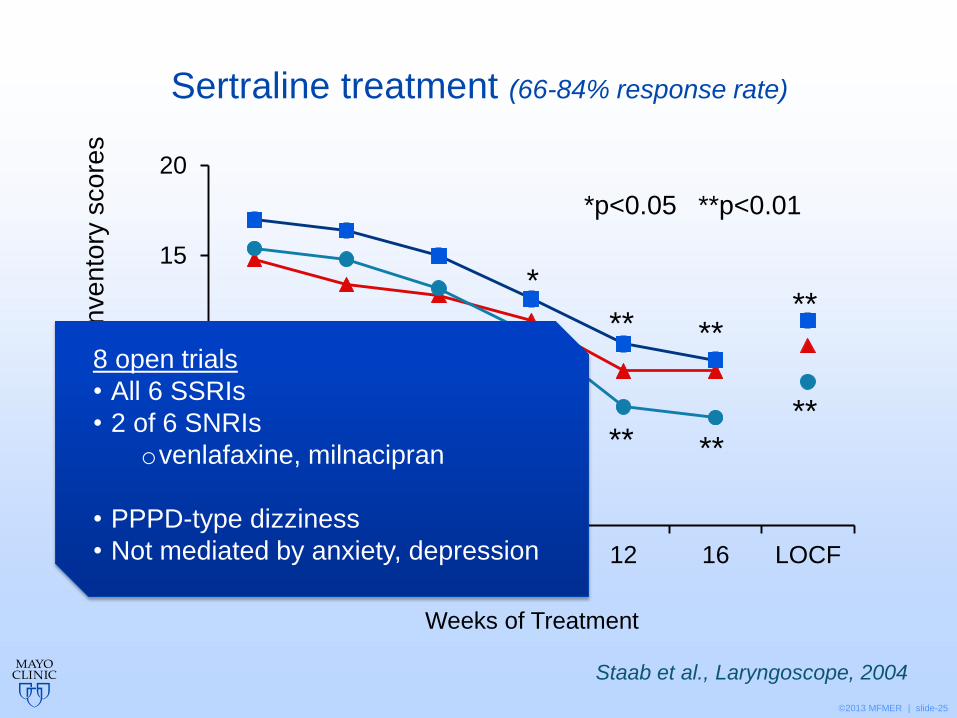
0 2 4 8 12 16 LOCF
Physical
Functional
Emotional
Sertraline treatment (66-84% response rate)D
izzin
ess H
an
dic
ap
In
ve
nto
ry s
co
res
Weeks of Treatment
*p<0.05 **p<0.01
*
****
***
*
****
**
Staab et al., Laryngoscope, 2004
8 open trials
• All 6 SSRIs
• 2 of 6 SNRIs
ovenlafaxine, milnacipran
• PPPD-type dizziness
• Not mediated by anxiety, depression
©2013 MFMER | slide-26
Treatment – Psychotherapy
• Cognitive behavior therapy (CBT)
• Long-standing PPV (PPPD)
• 8-12 sessions of CBT + self-directed exposure exercises > exercises alone
• Benefits were lost at 1 year
Emerging CSD (PPPD)
• 3 sessions of CBT > wait list control
• Large benefits were maintained at 1 and 6 months follow-up.
Holmberg, et al., J Neurol, 2007;
Mahoney, et al., Am J Otolaryn, 2013

©2013 MFMER | slide-27
Conclusion – Functional vestibular disorders (PPPD and its phobic subtype PPD)
• Definition
• Distilled from clinical observations made 145 years ago
• Revived independently starting 30 years ago by 4 teams
• Formal diagnostic criteria contained in ICD-11 draft (2017)
• Treatments help
• Vestibular habituation
• SSRIs/SNRIs
• CBT done early
• Putative pathophysiologic mechanisms
• Sustained used of high-risk postural control
• Visual (somatosensory) dependence
• Mediated by anxiety-related processes
• Possibly associated with reduced higher level (cortical) integration

©2013 MFMER | slide-28
Questions & Discussion