non-employee id # request form...c:\users\cheri\appdata\local\microsoft\windows\temporary internet...
TRANSCRIPT

NON-EMPLOYEE ID # REQUEST FORM for CONTRACTORS/TRAVELERS/PHYSICIANS
Today’s Date: FOR HR USE ONLY
Submitter: Lyndie Pfannkuche emPath ID#:
Submitter phone no: 760-837-8248 Orientation Date:
Comments: MED Student Created by:
PERSONAL INFORMATION
Last name: First: Middle: Nickname:
Address:
Social Security no.: Contact phone no.: Birth date: Sex:
POSITION INFORMATION
Start Date: [Date]
Cost Center/Department: 988-8270 / Graduate Medical Education
Job Code/Title: 5201/ Medical Student
ACCESS BADGE
Dept. and/or building access required:
Mirror the access of (name):
Security Card Acknowledgement
I understand that this security access card is used to gain access to secured areas on the campus and that if it is lost or misplaces, I am to immediately report it to the Human Resources Department (ext. 8500) or the Security Department (ext. 8200).
I also understand that this security access card must be returned to Eisenhower Medical Center upon termination or end of assignment.
Contractor Signature:
Security Name Signature: Date:
SIGNATURE
Director’s Name: Sandra Gonzales
Director’s signature: Date:
C:\Users\Cheri\AppData\Local\Microsoft\Windows\Temporary Internet Files\Content.Outlook\LTAYJW1G\Access Badge Request Med Students.doc
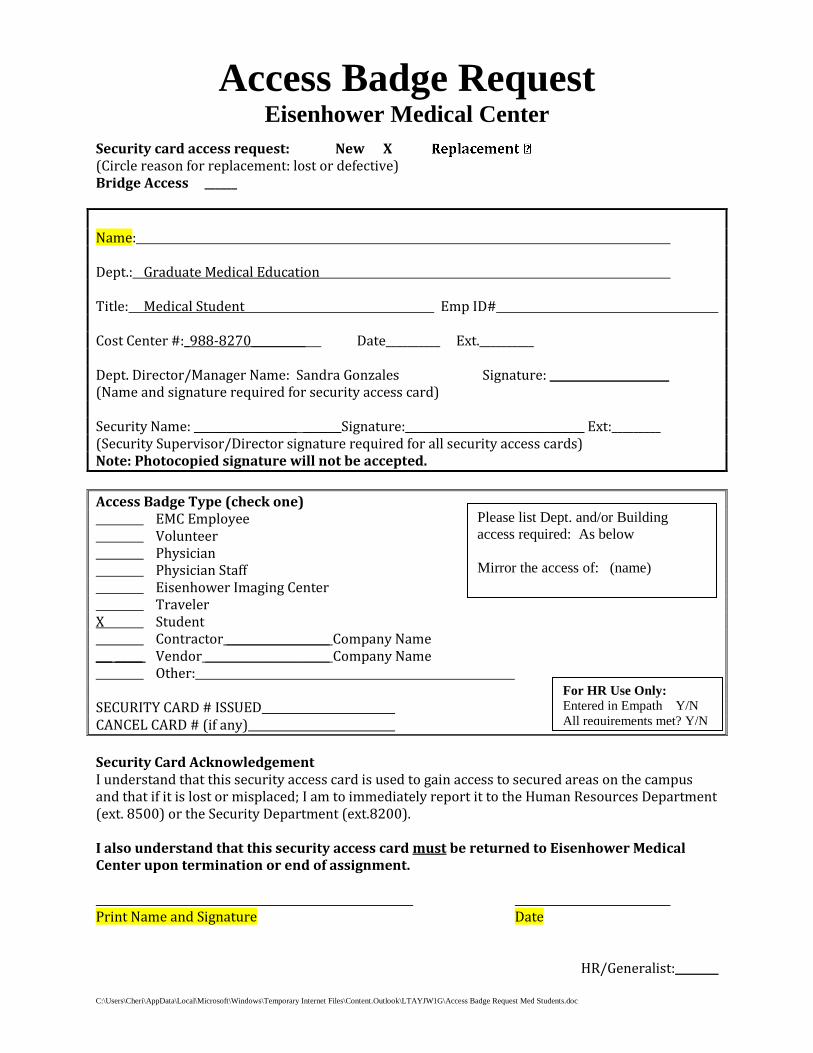
Access Badge Request Eisenhower Medical Center
Security card access request: New X (Circle reason for replacement: lost or defective) Bridge Access ______
Name: Dept.: Graduate Medical Education Title: Medical Student Emp ID# Cost Center #:_988-8270__________ Date__________ Ext.__________ Dept. Director/Manager Name: Sandra Gonzales Signature: ______________________ (Name and signature required for security access card) Security Name: ___________________ _______Signature:_________________________________ Ext:_________ (Security Supervisor/Director signature required for all security access cards) Note: Photocopied signature will not be accepted.
Access Badge Type (check one) EMC Employee Volunteer Physician Physician Staff Eisenhower Imaging Center Traveler X Student Contractor ___________________ Company Name ___ _____ Vendor _______________________ Company Name Other: SECURITY CARD # ISSUED CANCEL CARD # (if any)
Security Card Acknowledgement I understand that this security access card is used to gain access to secured areas on the campus and that if it is lost or misplaced; I am to immediately report it to the Human Resources Department (ext. 8500) or the Security Department (ext.8200). I also understand that this security access card must be returned to Eisenhower Medical Center upon termination or end of assignment. Print Name and Signature Date
HR/Generalist:________
For HR Use Only:
Entered in Empath Y/N
All requirements met? Y/N
Please list Dept. and/or Building
access required: As below
Mirror the access of: (name)

CLERKSHIP/ELECTIVE APPLICATION
1. Please complete Section I of the application. Return the application to
the Eisenhower Medical Center Clerkship Coordinator along with your:
CV
Transcripts
USMLE Step score________ or COMLEX Step score_________
2. When approved, the Eisenhower Medical Center Clerkship Coordinator
will send an email confirmation to the medical school and applicant.
3. Bring the following documentation: picture ID, school ID, and
immunization records. You will be drug tested. If you are on ANY
medications which show up in a urine screening, please bring
prescription and ordering physician’s name and contact information.
Desired Elective/Clerkship: Check One
____ Ambulatory internal Medicine Elective
_____ Cardiology Elective
_____ Emergency Medicine Elective
_____ PM&R
_____ Family Medicine Clerkship
_____ Geriatrics Elective
_____ HIV Elective
_____ Nephrology Elective
_____ PM&R (Rehabilitation Medicine) Elective
_____ Sports Medicine Elective
_____ Psychiatry TMS Elective
4. Email Clerkship application to [email protected]
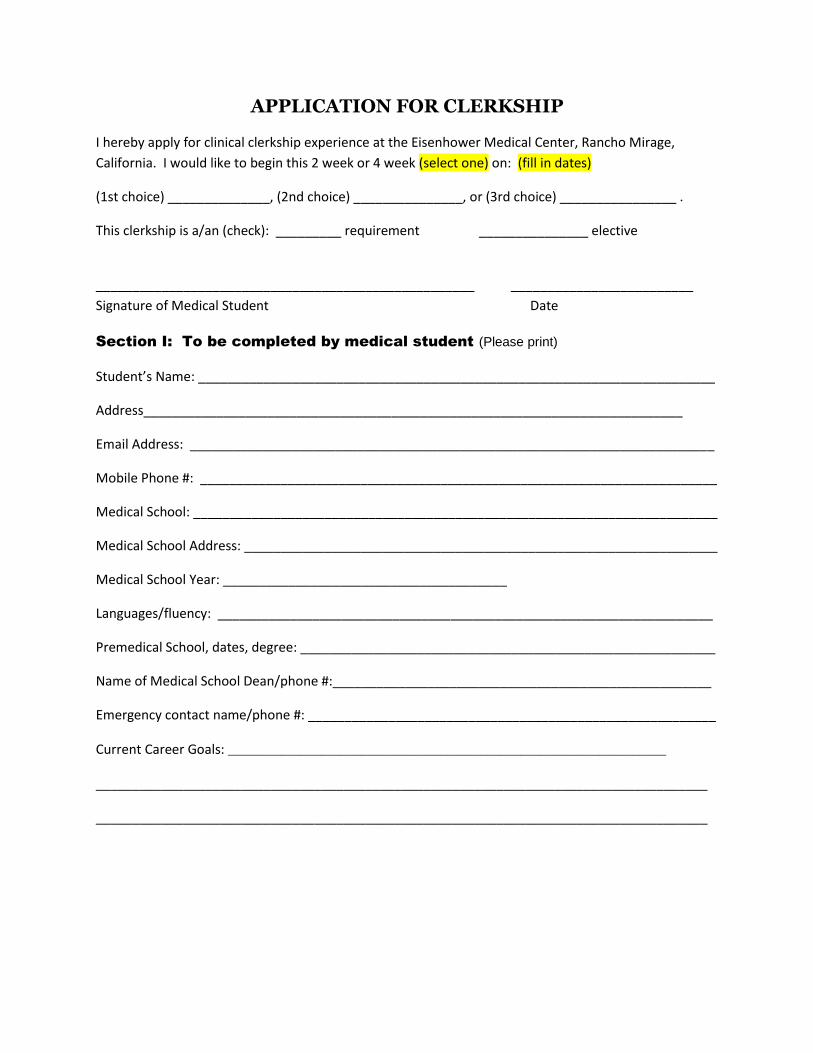
APPLICATION FOR CLERKSHIP
I hereby apply for clinical clerkship experience at the Eisenhower Medical Center, Rancho Mirage,
California. I would like to begin this 2 week or 4 week (select one) on: (fill in dates)
(1st choice) ______________, (2nd choice) _______________, or (3rd choice) ________________ .
This clerkship is a/an (check): _________ requirement _______________ elective
____________________________________________________ _________________________
Signature of Medical Student Date
Section I: To be completed by medical student (Please print)
Student’s Name: _______________________________________________________________________
Address__________________________________________________________________________
Email Address: ________________________________________________________________________
Mobile Phone #: _______________________________________________________________________
Medical School: ________________________________________________________________________
Medical School Address: _________________________________________________________________
Medical School Year: _______________________________________
Languages/fluency: ____________________________________________________________________
Premedical School, dates, degree: _________________________________________________________
Name of Medical School Dean/phone #:____________________________________________________
Emergency contact name/phone #: ________________________________________________________
Current Career Goals: __________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________