normal labour and abnormal labour
TRANSCRIPT

LABOUR
JMJ 1
CONTENTS
• Introduction• Fetal and maternal anatomy relevant to labour• The process of the labour• Physiology of the labour• Management of normal labour• Pain relief in labour• Abnormal labour• Labour in special circumstances• Induction of labour• Clinical risk management
JMJ 2
Introduction
• There is a complex interaction between the• “Powers of the uterus” –
• contractions
• “Passage” of the birth canal –• bony pelvis and the soft tissues of the pelvic floor and perineum)
• “Passenger” –• Fetus
JMJ 3
Fetal and maternal anatomy relevant to labour
• The pelvis• Pelvic brim/inlet• Pelvic mid cavity• Pelvic outlet• Pelvic floor• Perineum
• The fetal skull• Bones, sutures and frontenelles• Diameter of the skull
JMJ 4
Pelvic brim of inlet
• Is bounded
JMJ 5
Anteriorly
Posteriorly
Each sides Each sides
Symphysis pubis (joint separating the 2 pelvic bone)
• Upper margin of the pubic bone
• Ileopecteneal line• Ala of the sacrum
• Upper margin of the pubic bone
• Ileopecteneal line• Ala of the sacrum
Promontory of the sacrum
Pelvic brim of inlet
• Normal transverse diameter – 13.5 cm
• Normal AP diameter – 11cm
• Angle of the inlet normally 60º to the horizontal in the erect position
• Increased angle - delay the head entering (Afro Carribean)
JMJ 6
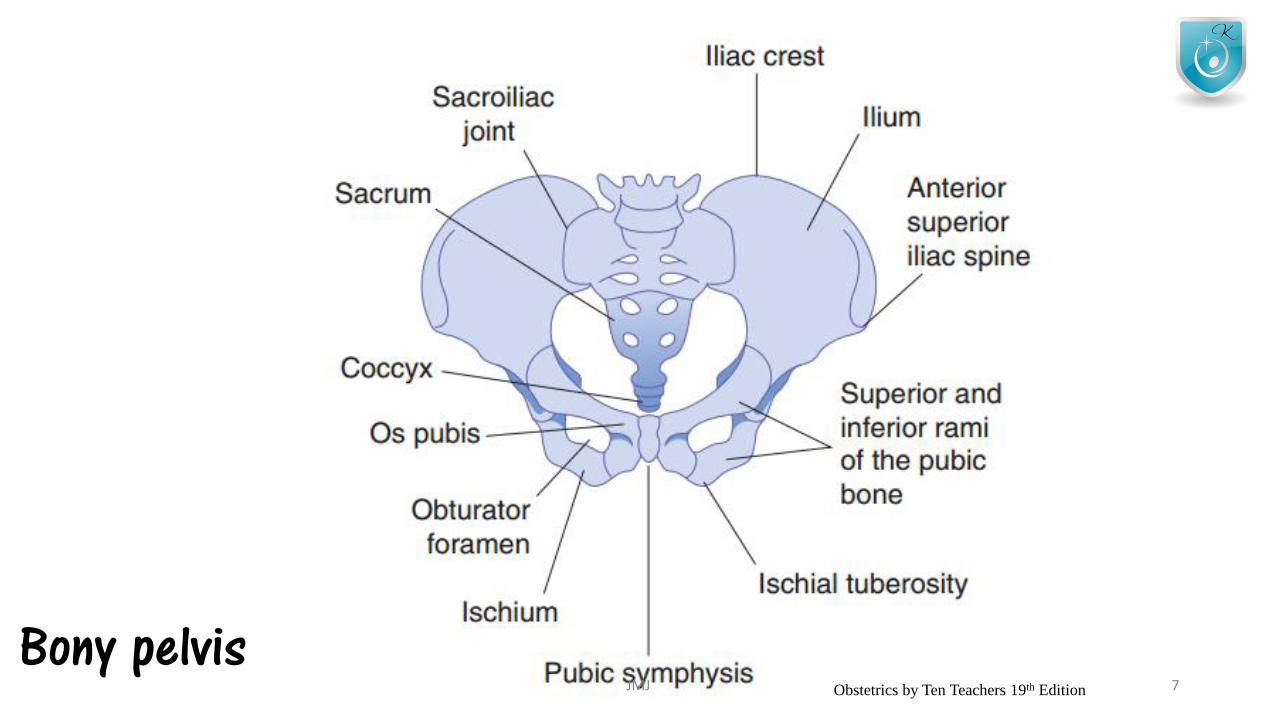
Bony pelvisJMJ 7Obstetrics by Ten Teachers 19th Edition
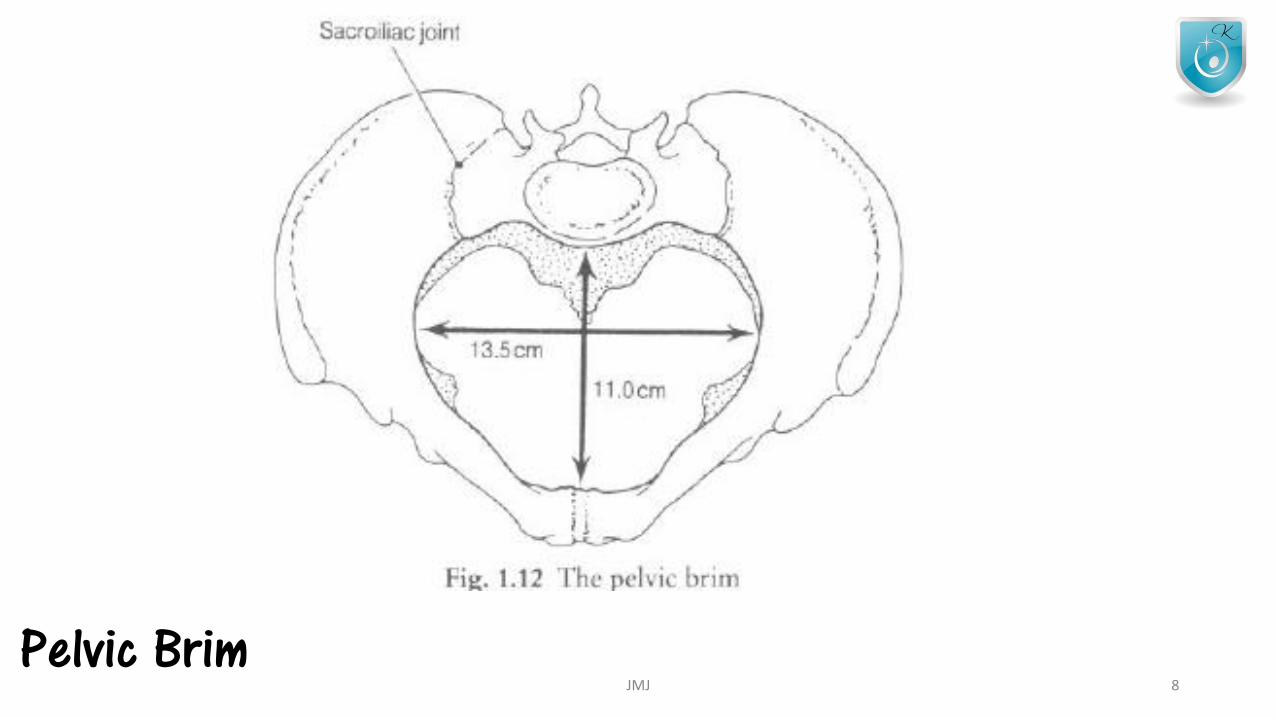
Pelvic BrimJMJ 8
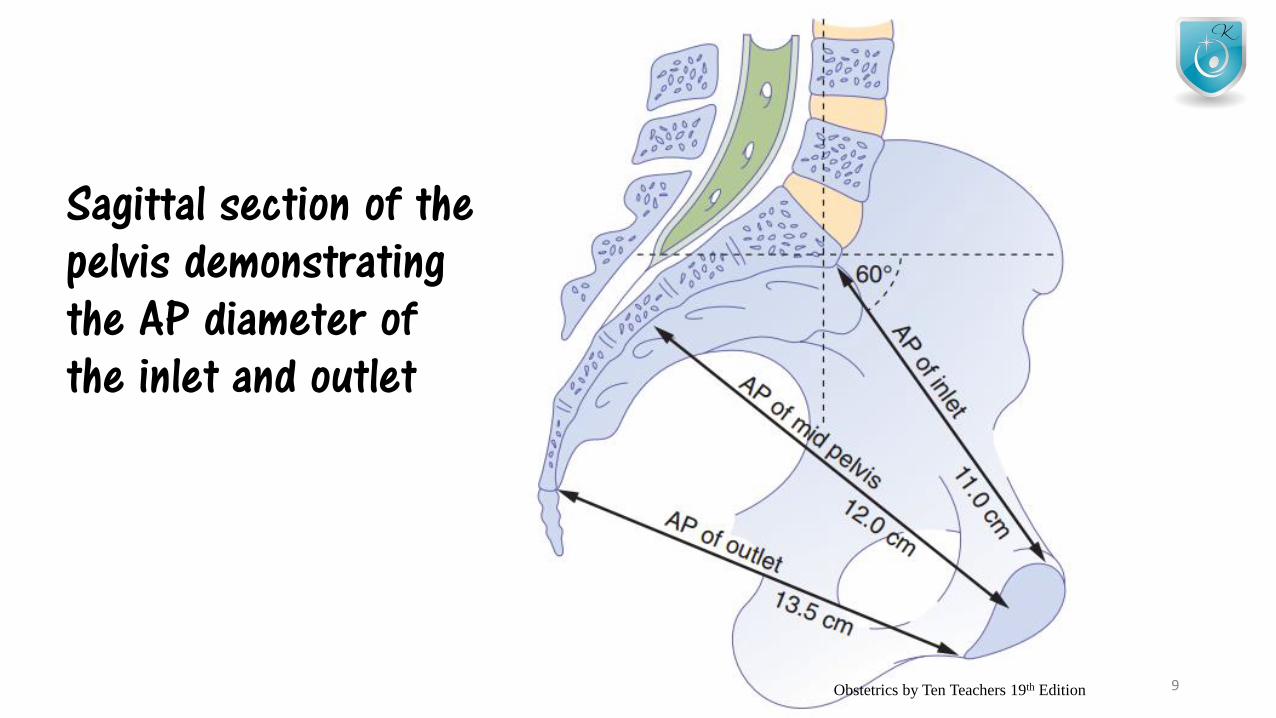
Sagittal section of the pelvis demonstrating the AP diameter of the inlet and outlet
JMJ 9Obstetrics by Ten Teachers 19th Edition
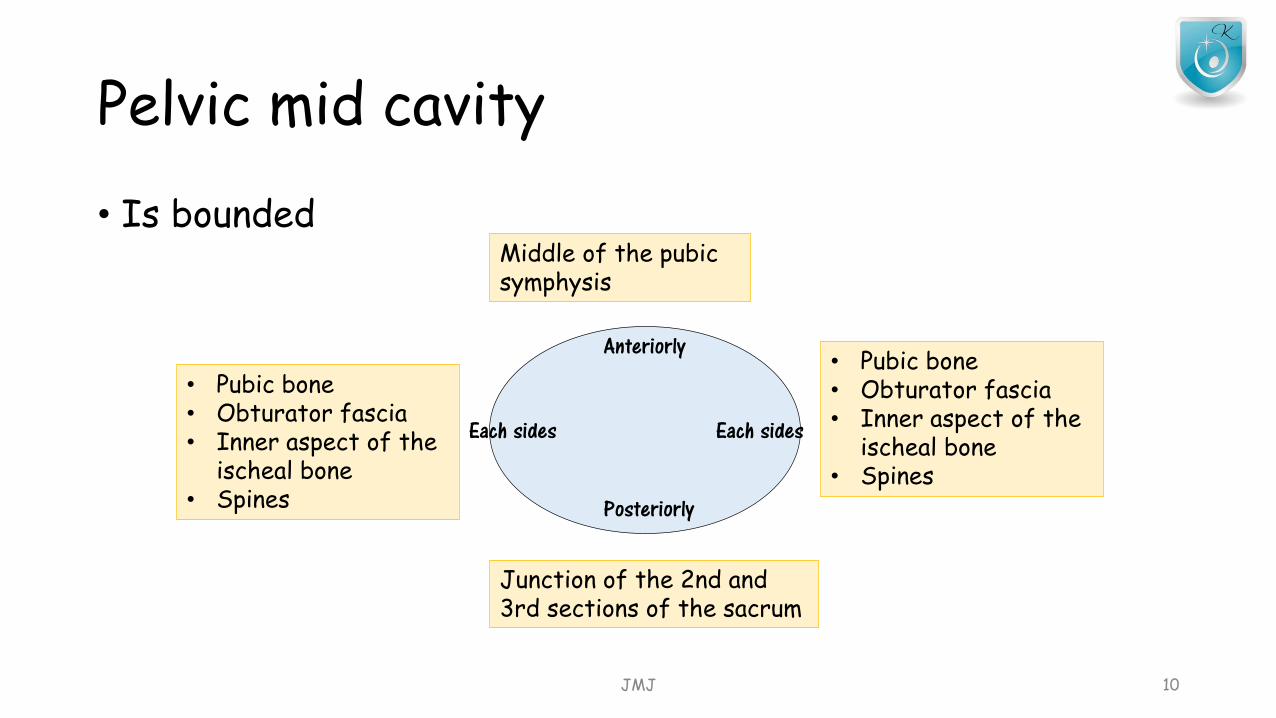
Pelvic mid cavity
• Is bounded
JMJ 10
Anteriorly
Posteriorly
Each sides Each sides
Middle of the pubic symphysis
• Pubic bone• Obturator fascia• Inner aspect of the
ischeal bone• Spines
Junction of the 2nd and 3rd sections of the sacrum
• Pubic bone• Obturator fascia• Inner aspect of the
ischeal bone• Spines
Pelvic mid cavity
• Cavity is almost round• Transverse and anterior diameter – 12 cm
• Ischeal spines are palpable vaginally • Are used as a landmarks to
• assess the descend of head on vaginal examination (station)• For providing an anesthetic block to the pudendal nerve
• Pudendal nerve passes behind and below the ischeal spine on each side
JMJ 11
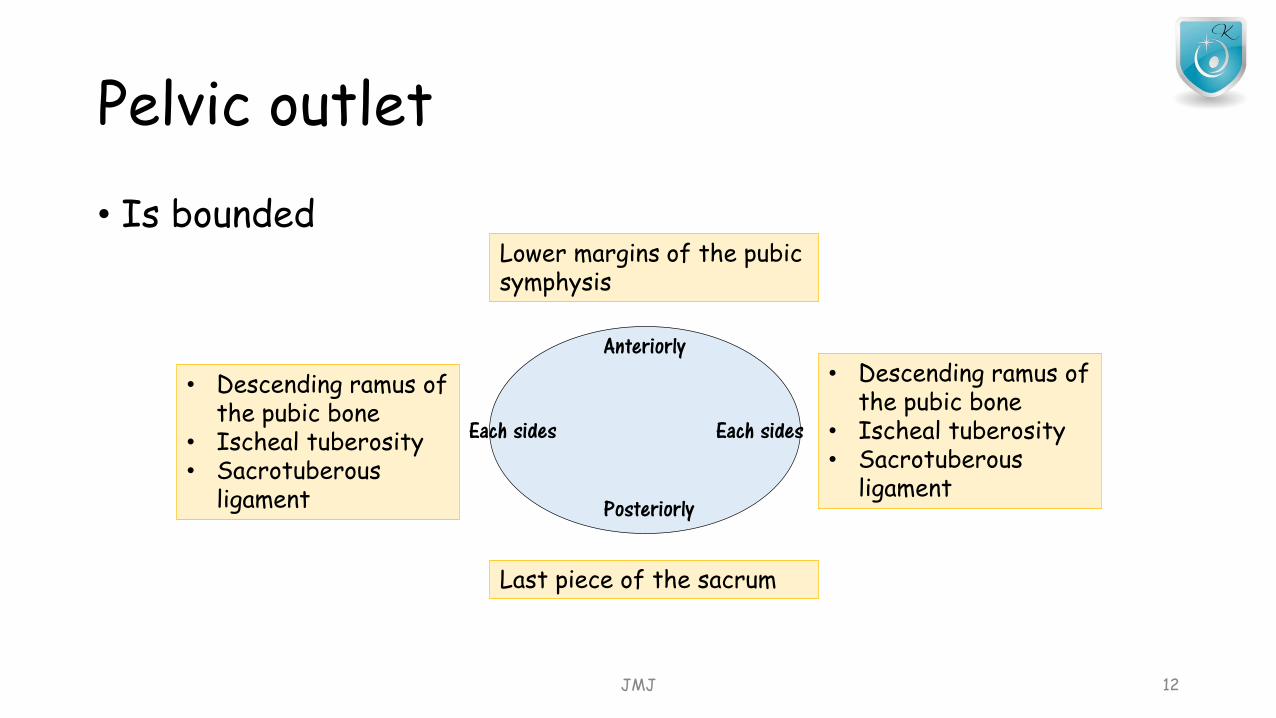
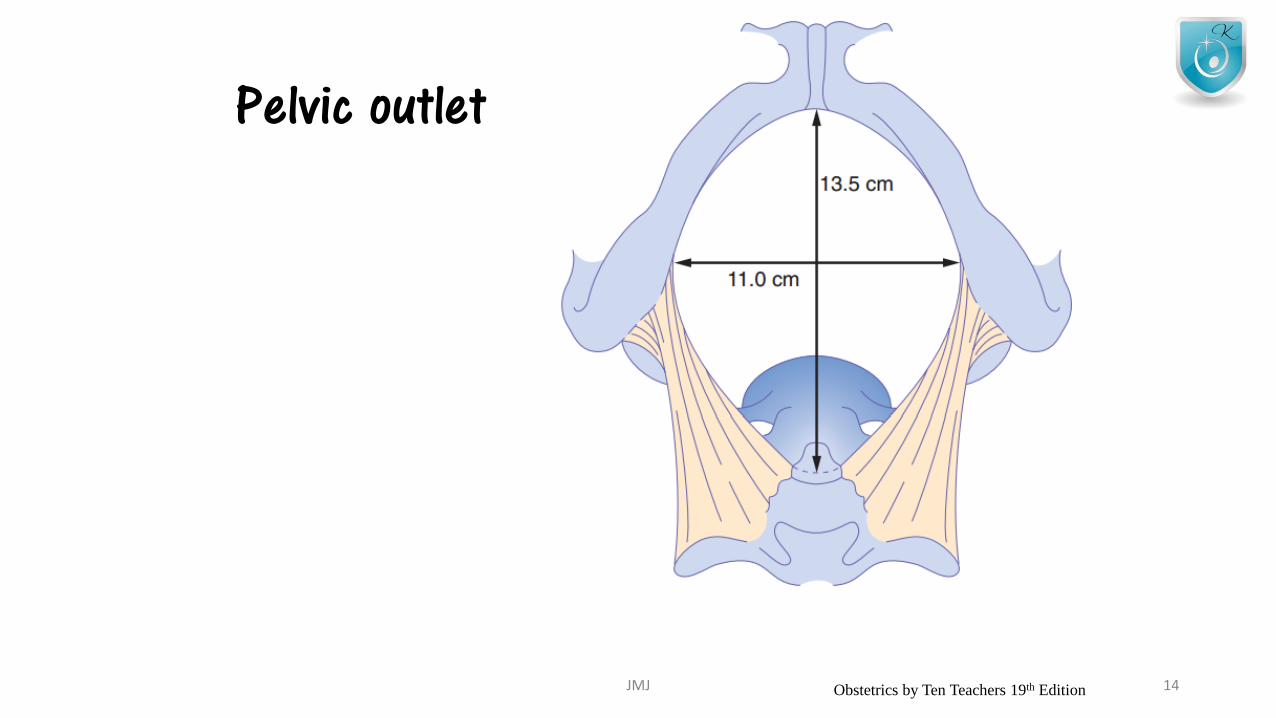
Pelvic outlet
• Is bounded
JMJ 12
Anteriorly
Posteriorly
Each sides Each sides
Lower margins of the pubic symphysis
• Descending ramus of the pubic bone
• Ischeal tuberosity• Sacrotuberous
ligament
• Descending ramus of the pubic bone
• Ischeal tuberosity• Sacrotuberous
ligament
Last piece of the sacrum
Pelvic outlet
• AP diameter – 13.5 cm• Transverse diameter – 11cm
• Transverse is the widest diameter at the inlet, but at the outlet it is the AP
• These measurements can be less in• Maternal stature• Previous pelvic fracture• Metabolic bone diseases (rickets)
• During 3rd trimester these become loosen• Pelvic ligaments at pubic symphysis• Sacroiliac joint
JMJ 13
Pelvic outlet
JMJ 14Obstetrics by Ten Teachers 19th Edition
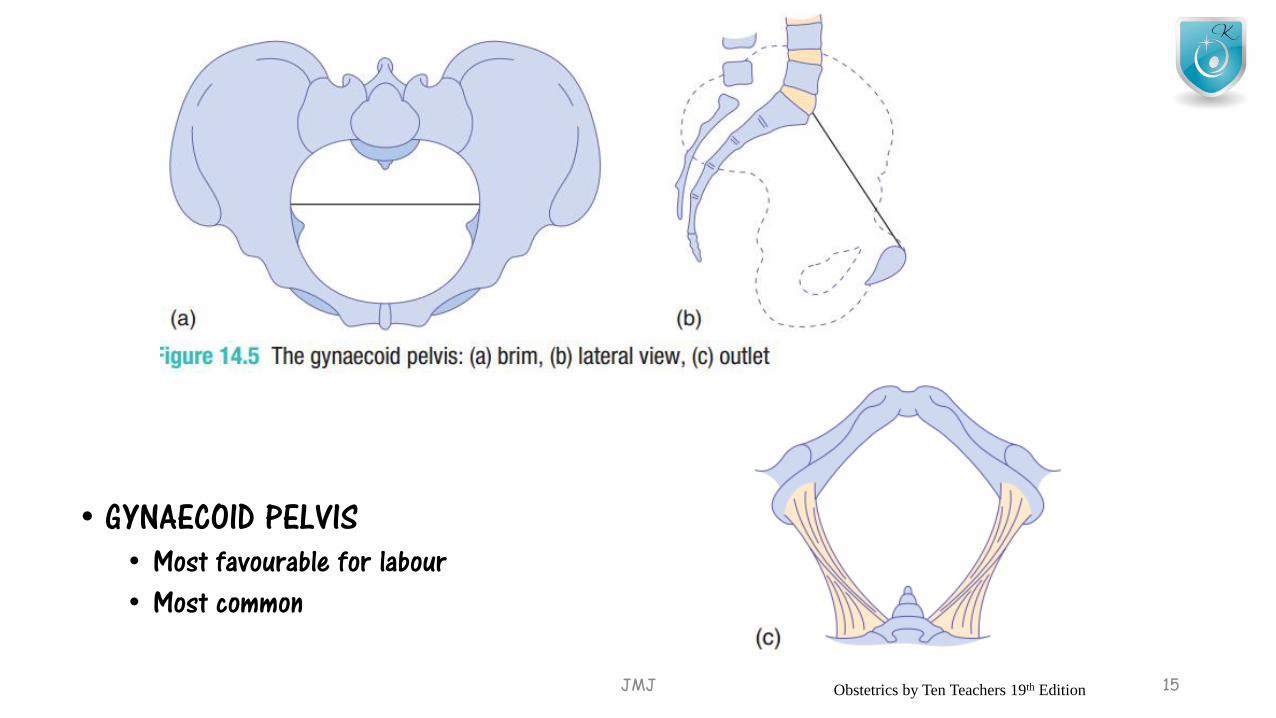
• GYNAECOID PELVIS• Most favourable for labour• Most common
JMJ 15Obstetrics by Ten Teachers 19th Edition

• ANDROID - TYPE• Predisposes to deep transverse arrest
JMJ 16Obstetrics by Ten Teachers 19th Edition
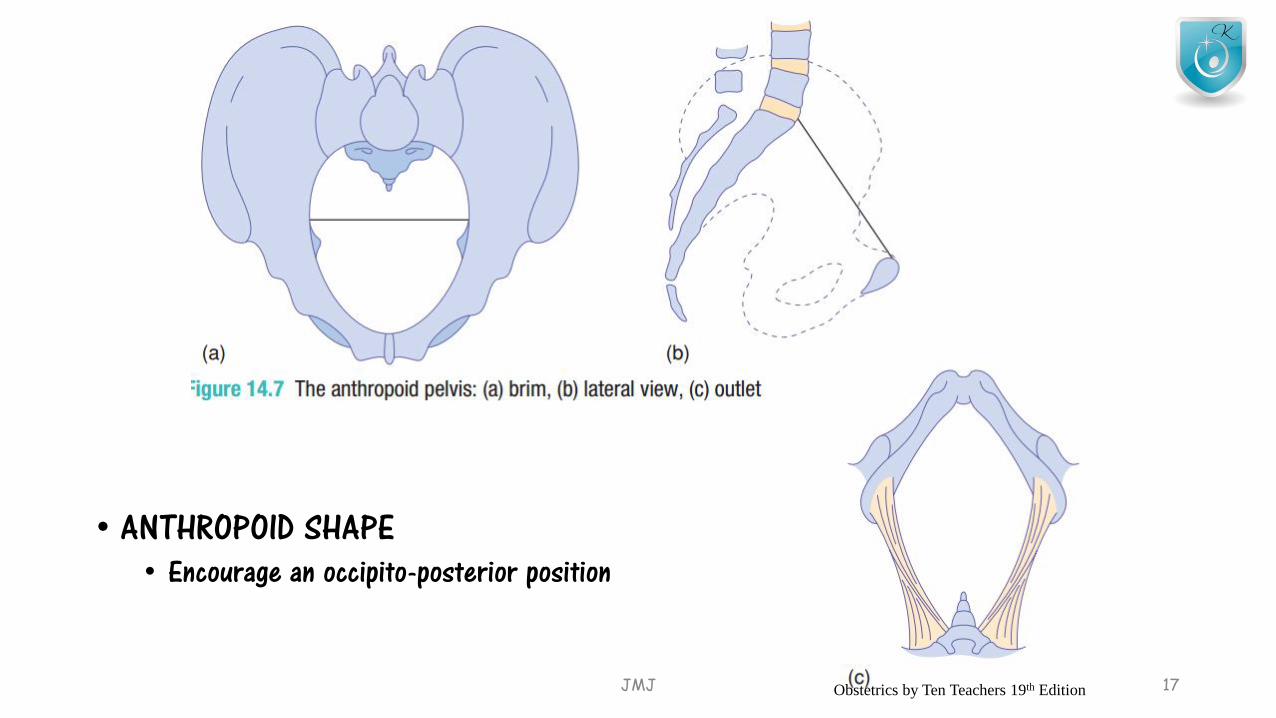
• ANTHROPOID SHAPE• Encourage an occipito-posterior position
JMJ 17Obstetrics by Ten Teachers 19th Edition
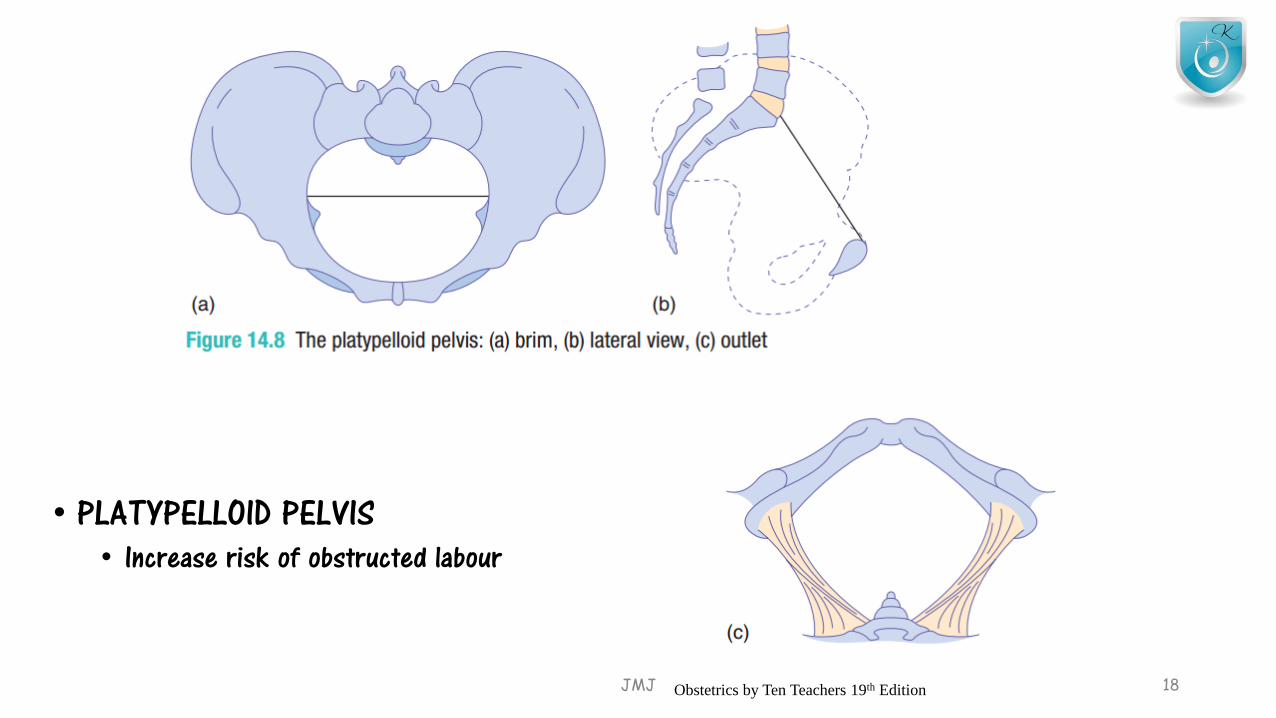
• PLATYPELLOID PELVIS• Increase risk of obstructed labour
JMJ 18Obstetrics by Ten Teachers 19th Edition
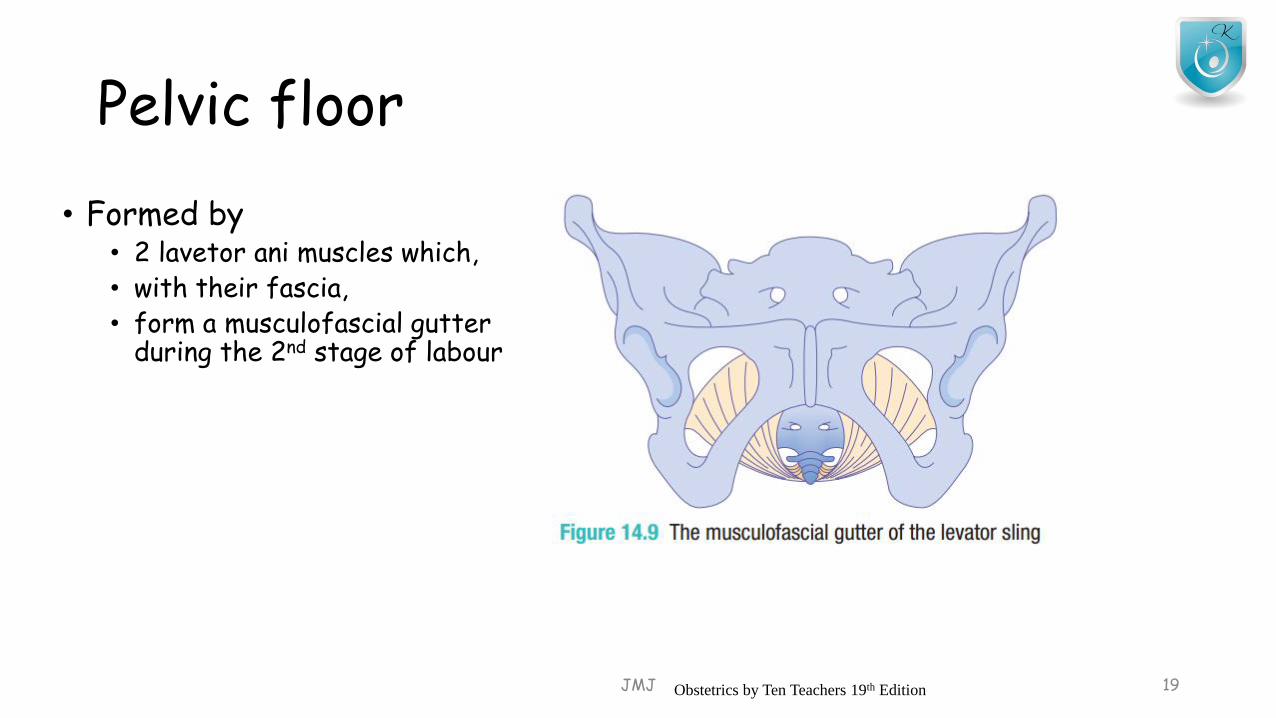
Pelvic floor
• Formed by• 2 lavetor ani muscles which,• with their fascia, • form a musculofascial gutter
during the 2nd stage of labour
JMJ 19Obstetrics by Ten Teachers 19th Edition
Perineum
• Perineal body• Is a condensation of fibrous and muscular tissue • lying between the vagina and the anus
• It receives attachments from• Posterior end of the bulbocavenous muscles• Medial ends of the superficial and deep transverse perineal muscles• Anterior fibers of the external anal sphincter
• It is always involved in a 2nd degree perineal tear
JMJ 20
JMJ 21
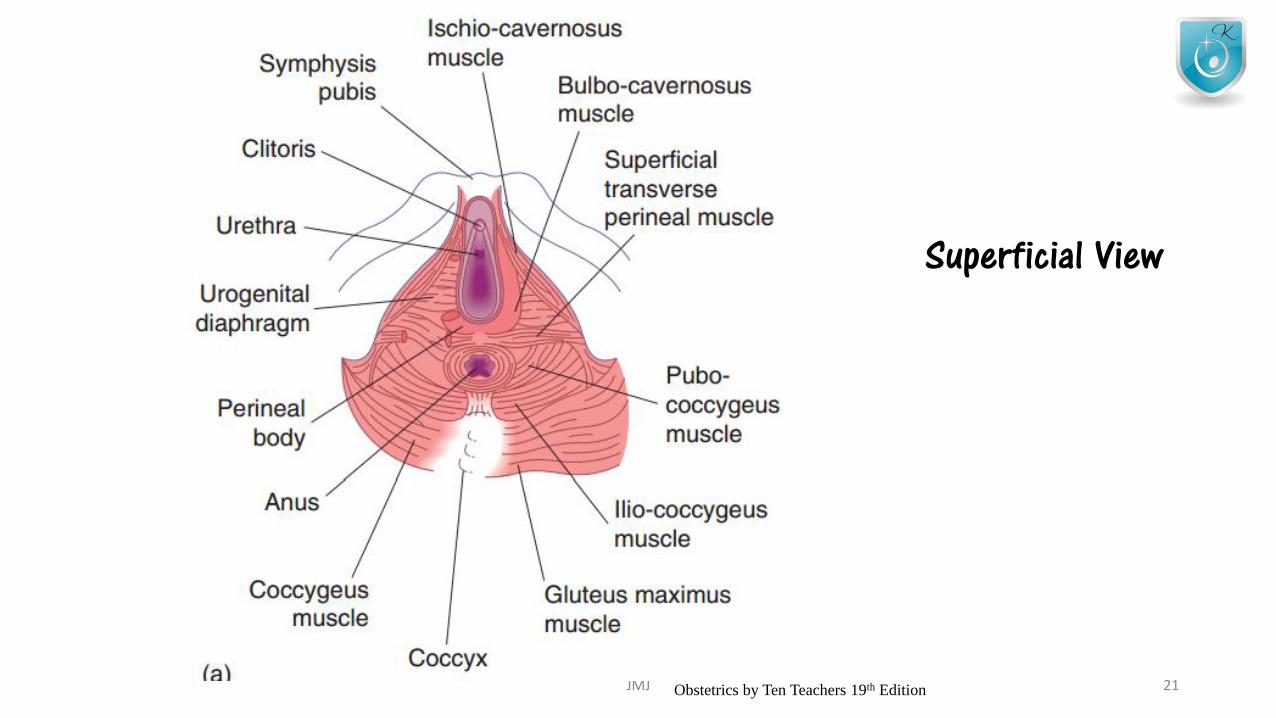
Superficial View
Obstetrics by Ten Teachers 19th Edition
JMJ 22
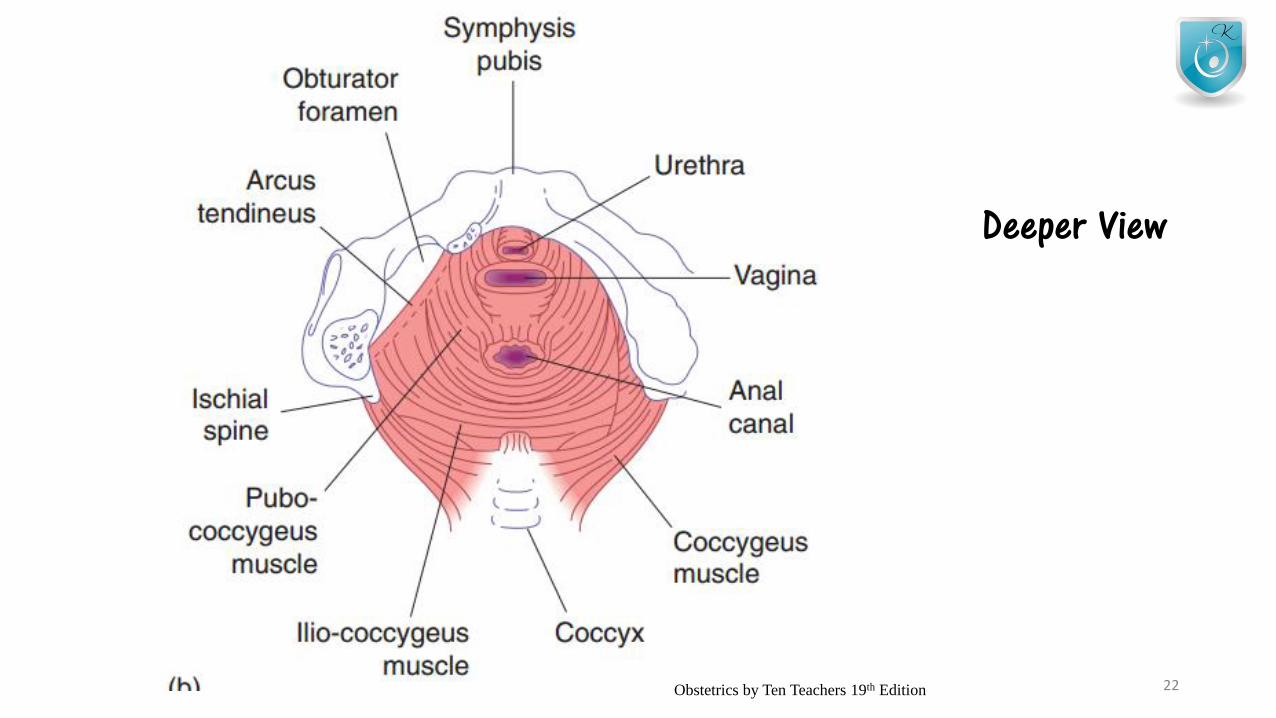
Deeper View
Obstetrics by Ten Teachers 19th Edition
Fetal skull bones, sutures, frontenelles
• Fetal skull • Vault• Face• Base
• At the time of labour, • Sutures joining the bones of the vault are
• soft, unossifed membranes
• Sutures of the face and the skull base• Firmly united
JMJ 23
JMJ 24
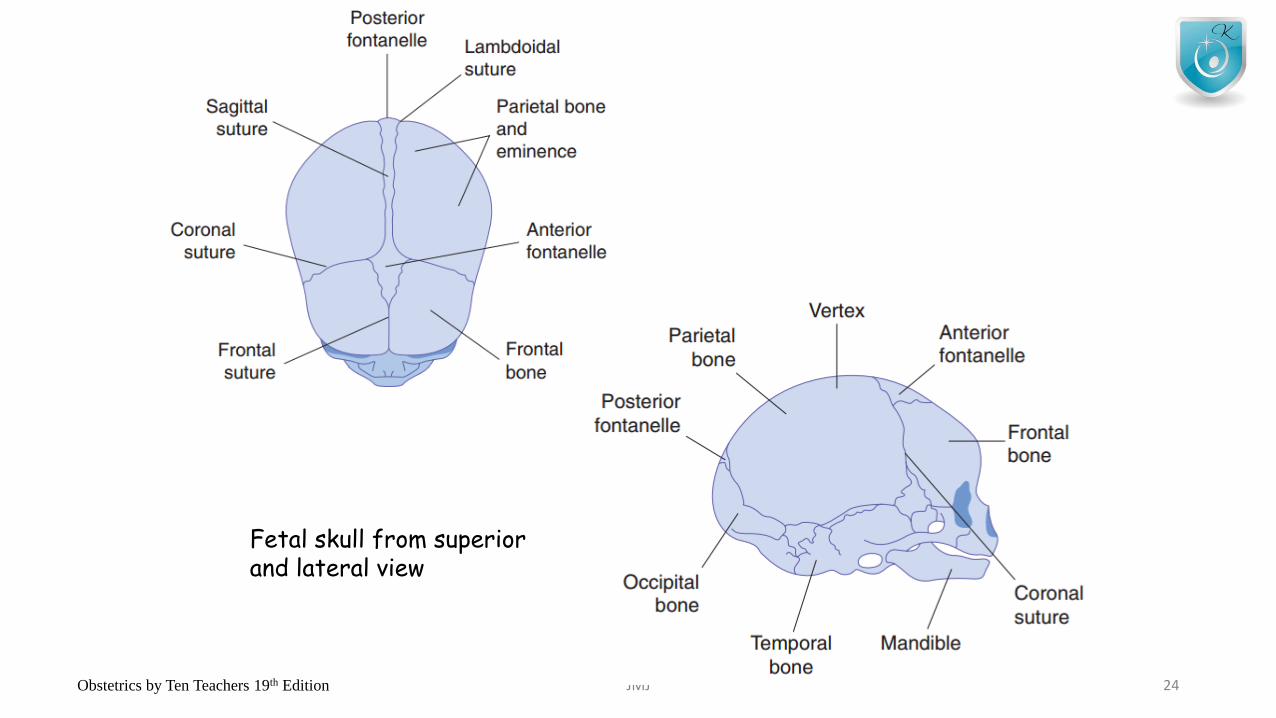
Fetal skull from superior and lateral view
Obstetrics by Ten Teachers 19th Edition
Fetal skull bones, sutures, frontenelles
• Vault is formed by• Parietal bones and parts of occipital• Frontal and temporal bones
• Between these bones there are 4 membranous sutures• Sagittal• Frontal• Coronal• Lambdoidal sutures
JMJ 25
Fetal skull bones, sutures, frontenelles
• Anterior frontenelle (bregma)• Diamond shaped• At the junction of sagittal, frontal and coronal sutures
• Posterior frontenelle• Triangular shape• Lie at the junction of the sagittal suture & lamb
• The area of the fetal skull bounded by 2 parietal eminenses& the anterior and posterior frontenelles – “vertex”
JMJ 26
Fetal skull bones, sutures, frontenelles
• Sutures allow these bones to move together and even to overlap• Paratial bones usually slides over the frontal and occipital bones• Bones are also compressible
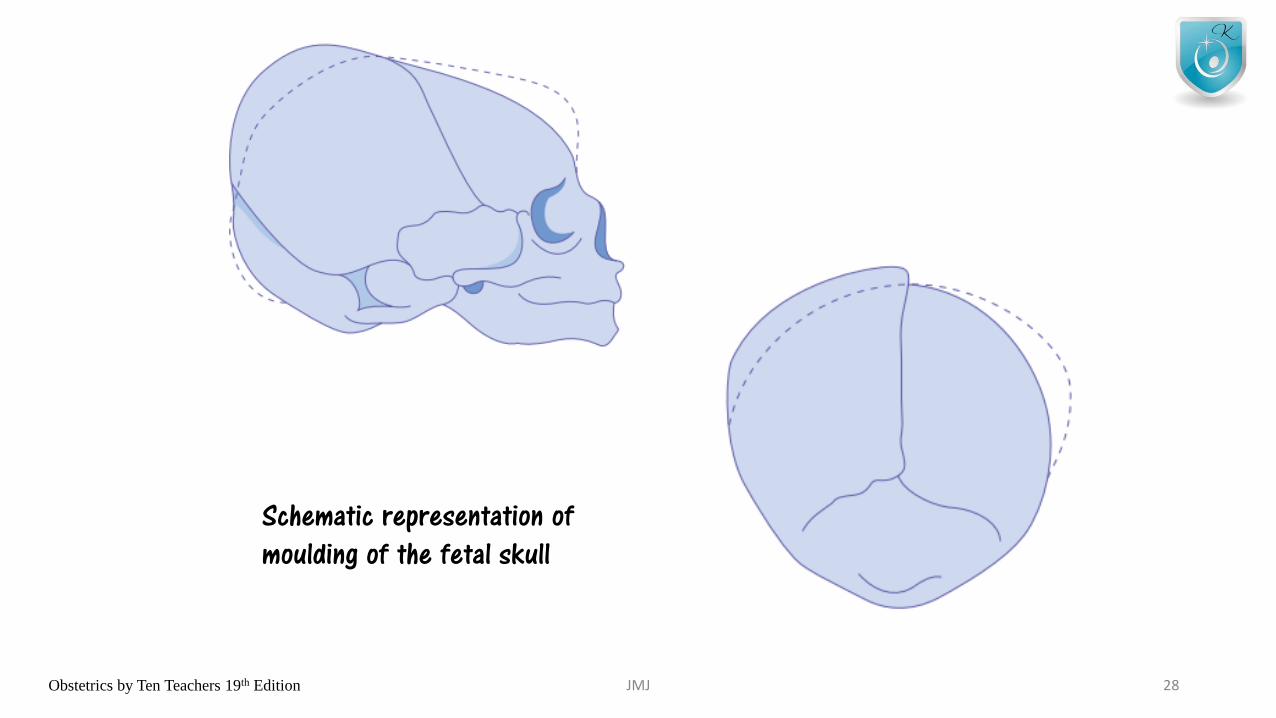
• Together these characteristics of the fetal skull allow a process called “moulding”
• Which effectively reduces the diameter of the fetal skull and • encourages progress through the bony pelvis, • without harming the underlying brain• .
JMJ 27
JMJ 28
Schematic representation ofmoulding of the fetal skull
Obstetrics by Ten Teachers 19th Edition
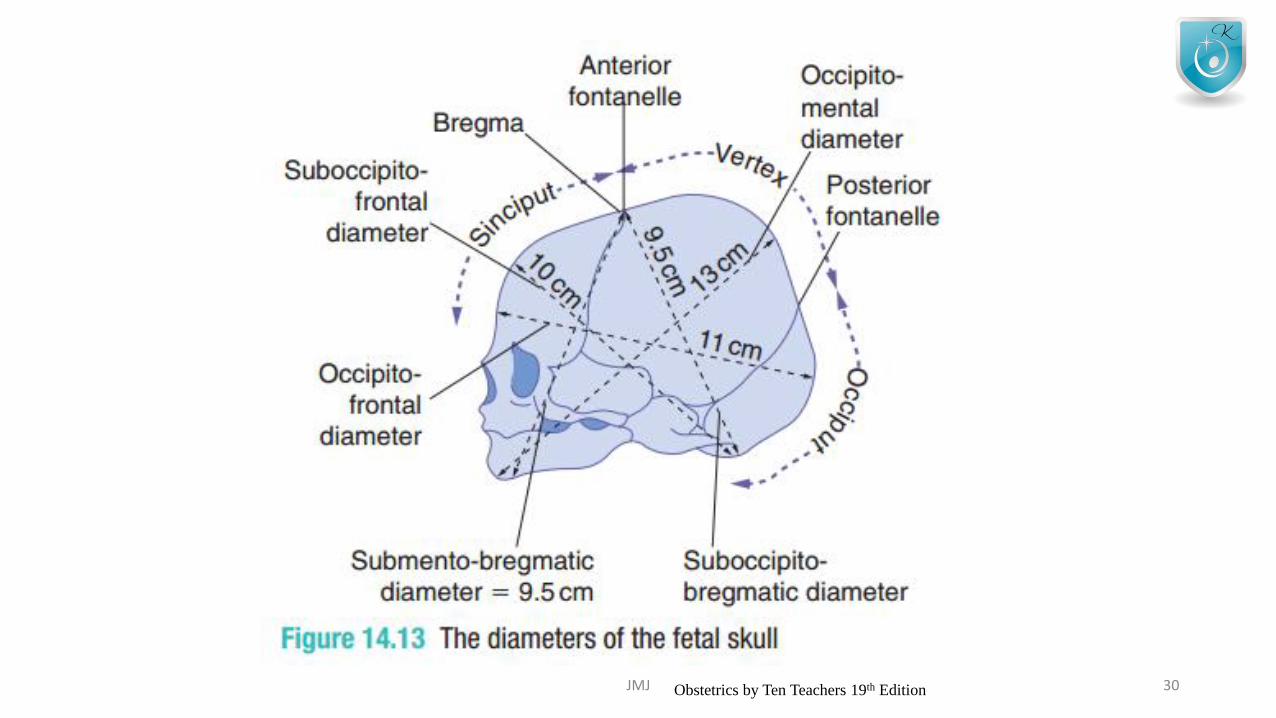
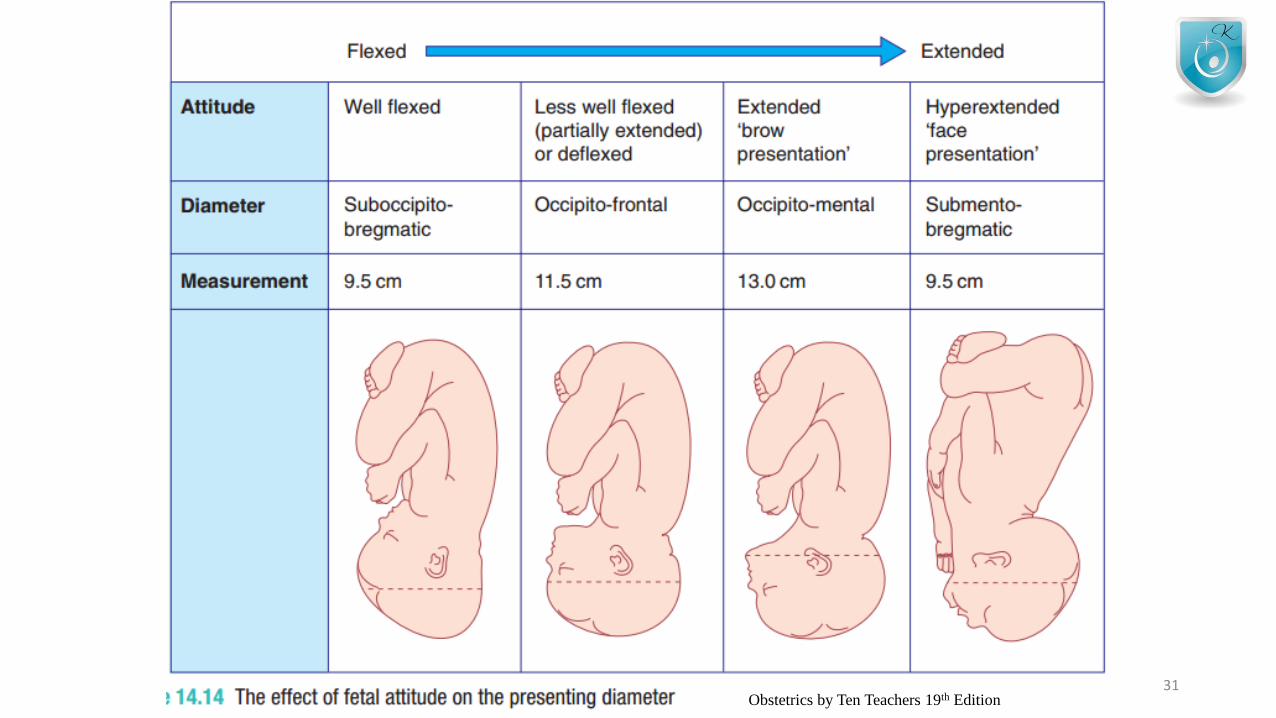
Diameter of the skull
• Fetal head- ovoid in shape
• The attitude of the head • Refers to the degree of flexion and extension at the upper cervical
spine• Different longitudinal diameters are presented to the pelvis in
labour depending on the attitude of the fetal head
JMJ 29
JMJ 30Obstetrics by Ten Teachers 19th Edition
JMJ 31Obstetrics by Ten Teachers 19th Edition
PROCESS OF LABOUR
• The onset of labour• Stages of labour
• 1st stage• 2nd stage• 3rd stage
• Duration of labour• Mechanism of labour
JMJ 32
Onset of labour
• Can be defined as• Regular contractions bringing about progressive cervical change
• Diagnosis is made retrospectively
• Following does NOT define as onset of labour• Loss of ‘show’ ( blood-stained plug of mucus passed from the
cervix)• Spontaneous rupture of membranes (SPOM)
JMJ 33
Stages of labour – 1st stage
• Time from the diagnosis of labour, to full dilatation of the cervix (10 cm)
JMJ 34
1st stage
Latent phase Active phase
JMJ 35
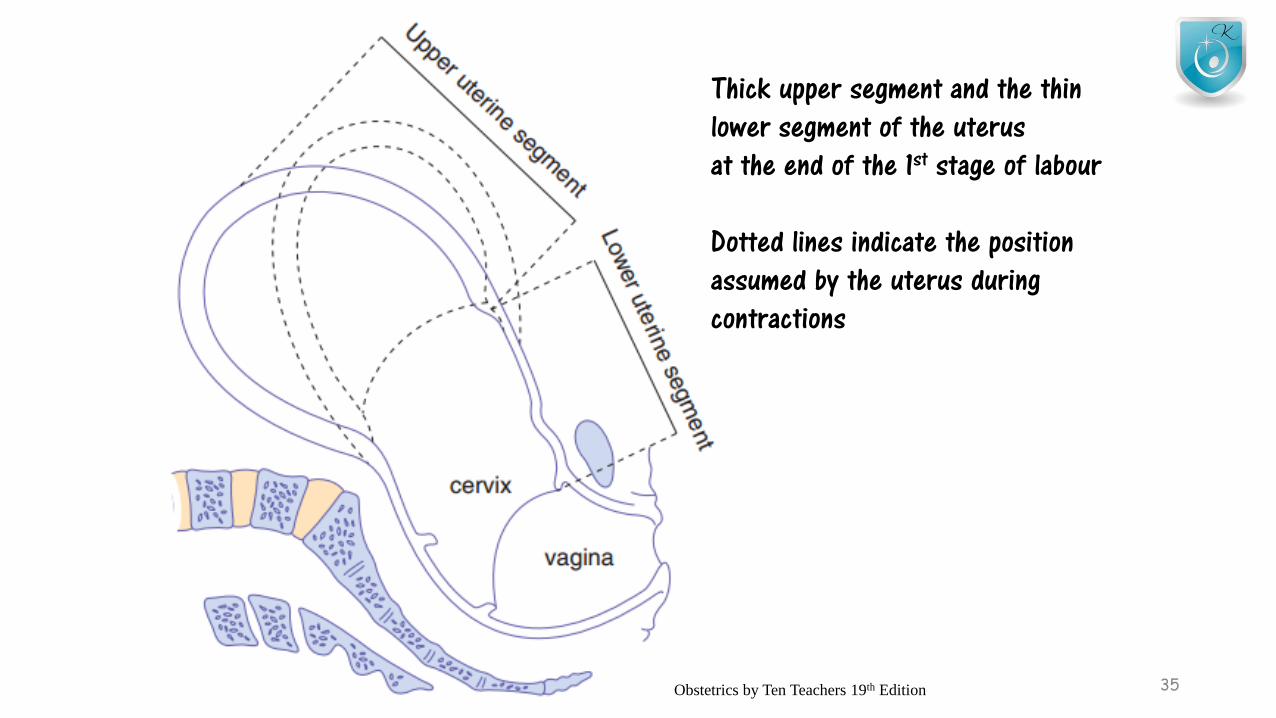
Thick upper segment and the thinlower segment of the uterus at the end of the 1st stage of labour
Dotted lines indicate the positionassumed by the uterus during contractions
Obstetrics by Ten Teachers 19th Edition
JMJ 36
Effacement • Is the process by which the cervix shortens in length as it becomes
included into the lower segment of the uterus• Begins during the weeks proceeding the onset of labour, but will
complete by the end of the latent phase.• Cervical os usually cannot begin to dilate until effacement is complete
• Effacement and dilatation should be thought of as • consecutive events in nulliparous women• Simultaneous events in multiparous women

1ST STAGE
LATENT PHASE
• Time between onset of labourand 3-4 cm dilatation
• Cervix become fully effaced
• Usually lasts between 3 – 8 hours
• Being shorter in multiparous women
ACTIVE PHASE
• Time between the end of latent phase and full dilatation (10cm)
• Usually lasting between 2-6 hours
• Shorter in multiparous women
• Cervical dilatation occurs at 1cm/hour –more in normal labour
• Abnormal – less than 0.5cm/hour
JMJ 37
2nd stage
• Time from full dilatation of the cervix to the delivery of the fetus or fetuses
JMJ 38
2nd stage
Passive phaseActive 2nd
stage
2nd STAGE
PASSIVE PHASE
• Time between full dilatation and the onset of involuntary expulsive contractions
• No maternal urge to push
• Fetal head is still relatively high in the pelvis
ACTIVE 2ND STAGE
• There is maternal urge to push
• Fetal head is low (often visible)
• Causing a reflex need to ‘bear down’
• Should last no longer than• 2hr- primiparous lady• 1hr- previous NVD
JMJ 39
Active 2nd stage
• If a woman never reaches a point of involuntary pushing, • the active 2nd stage is said to begin • when starts making voluntary active efforts • directed by her midwife.
• Active 2nd stage – lasting more than 3 hours• Associate with increase maternal and fetal morbidity
• Use of epidural anesthesia • May influence the length & management of 2nd stage of labour
JMJ 40
3rd STAGE
• Time from delivery of the fetus or fetuses until delivery of the placenta
• Placenta usually delivered within few minutes of the birth of the baby
• Lasting more than 30 minutes – Abnormal
• If women is under the ‘Physiological management’ – can last for 60 minutes
JMJ 41
Duration of labour
• Morale of most women starts to deteriorate after 6 hours in labour• After 12 hours the rates significantly accelerated
• Longer labours• Greater incidence of fetal hypoxia
• Early Artificial Rupture of Membranes (ARM)• Does shortens the length of labour,• Does not necessarily alter the outcome
• Prolonged labour• > 12 hours - nulliparous women• > 8 hours – multiparous women
JMJ 42
Mechanisms of labour
• Refers to the series of changes in
• position & attitude
• that the fetus undergoes
• during its passage through the birth canal
• Here describes on vertex presentation in a gynaecoid pelvis
JMJ 43
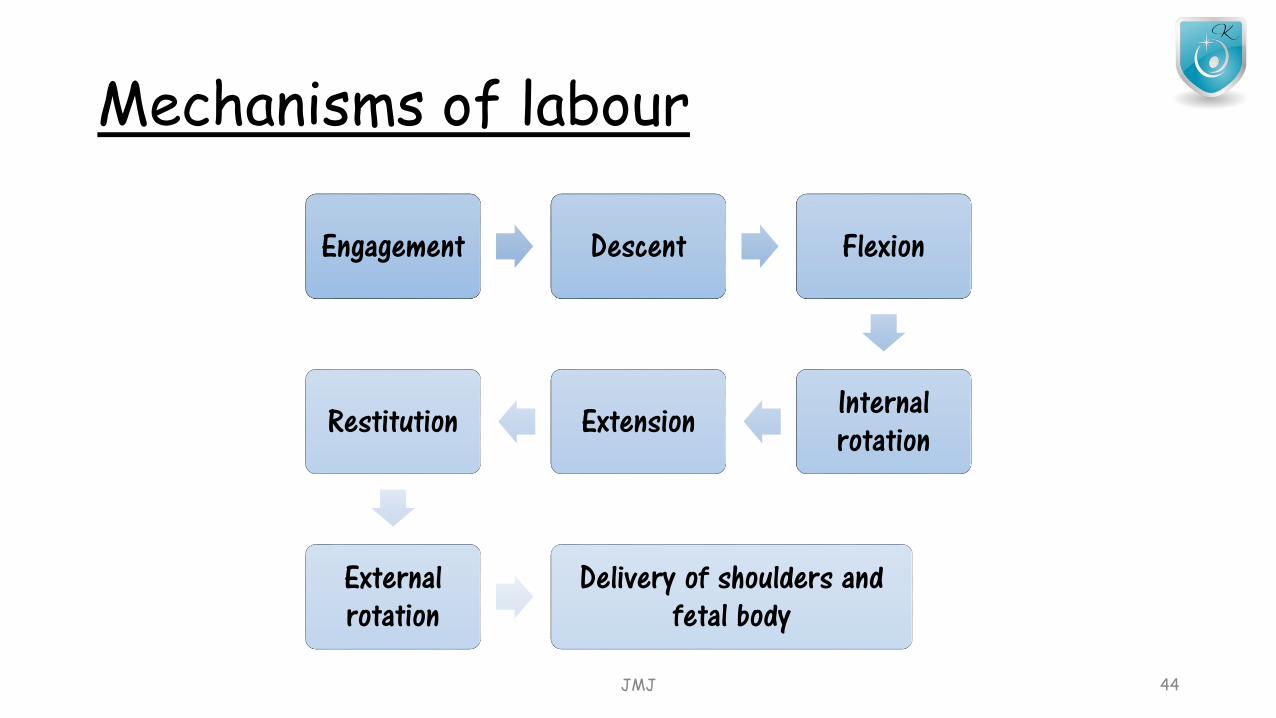
Mechanisms of labour
Engagement Descent Flexion
Internal rotationExtensionRestitution
External rotation
Delivery of shoulders and fetal body
JMJ 44
Engagement
• Head enters the pelvis – in transverse position
• Engagement is said to have occurred when, • Widest part of the presenting part has passed successfully through the
inlet
• It has occurred • In vast majority of nulliparous women prior to labour• Not so majority in multiparous women
• If more than 2/5th of fetal head is palpable abdominally – head not yet engaged
JMJ 45
Descent
• During 1st stage and 1st phase of the 2nd stage• Descent is 2ry to uterine contractions
• During Active phase of 2nd stage• Descent is helped by voluntary use of abdominal musculature &• Valsalva manoeuvre (‘Pushing’)
JMJ 46
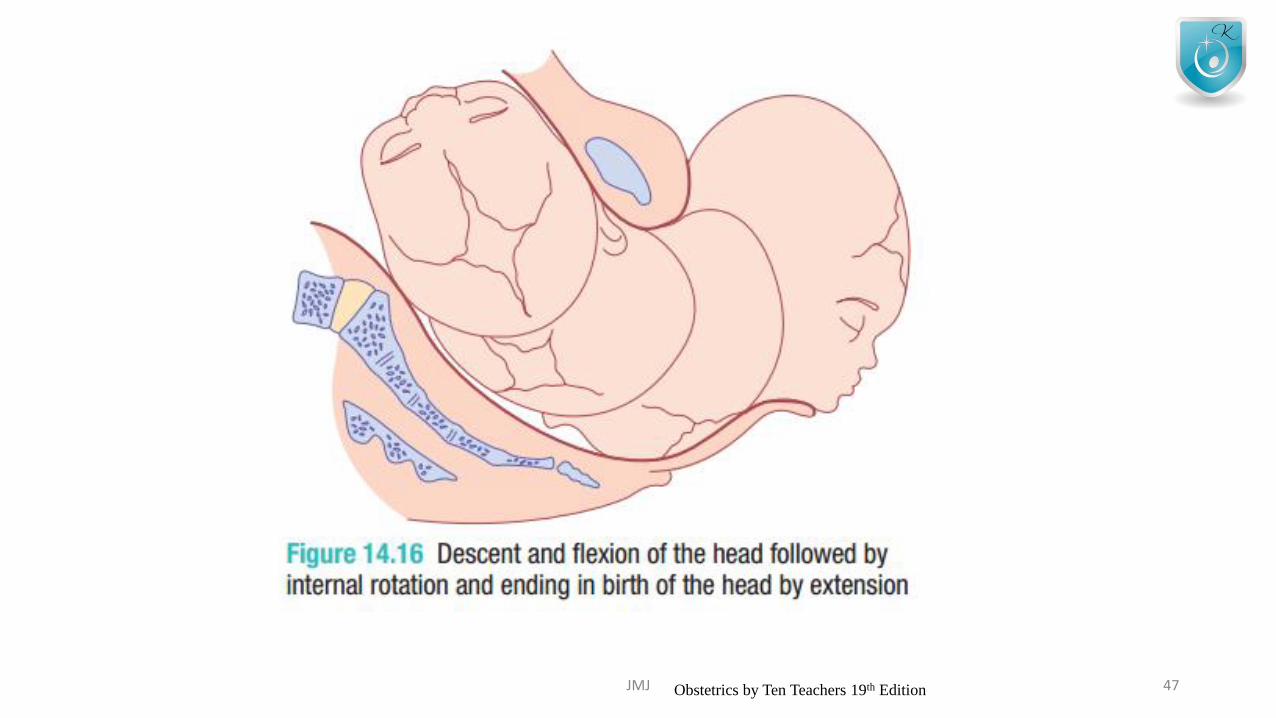
JMJ 47Obstetrics by Ten Teachers 19th Edition

Flexion
• Head may not always be completely flexed when it enters the pelvis
• When head enters then mid cavity flexion should occur
• This passive movements occurs, in part, • Due to surrounding structures • Important in minimizing the diameter of the fetal head
JMJ 48
Internal Rotation
• If head is well flexed, occiput will be the leading point• On reaching the sloping gutter of the levator ani muscles it
will be encourage to rotate anteriorly• So that the sagittal suture now lies in the AP diameter of the
pelvic outlet
• If babies head is in occipiti Posterior (OP) position-• Labour duration can be increased• May persist result in a ‘face to pubes’ delivery• Obstructed labour• Instrumental or Caesarean delivery
JMJ 49
Extension
• Following completion of the internal rotation• Occiput is underneath the symphysis pubis & • Bregma is near the lower boarder of the sacrum
• Soft tissue of perineum- still resistance, more prone to get damaged
• Well flexed head now extends,• & the occiput escapes from underneath the symphysis pubis & distends
the vulva • This is known as ‘Crowning’ of the head
• This will minimize the trauma to the soft tissues
JMJ 50
Restitution
• When head delivering – occiput is directly anterior
• As soon as it escapes from the vulva,
• the head aligns itself with the shoulders,
• which have enters the pelvis in the oblique position
• Slight rotation of the occiput through 1/8th of the circle is called ‘restitution’
JMJ 51
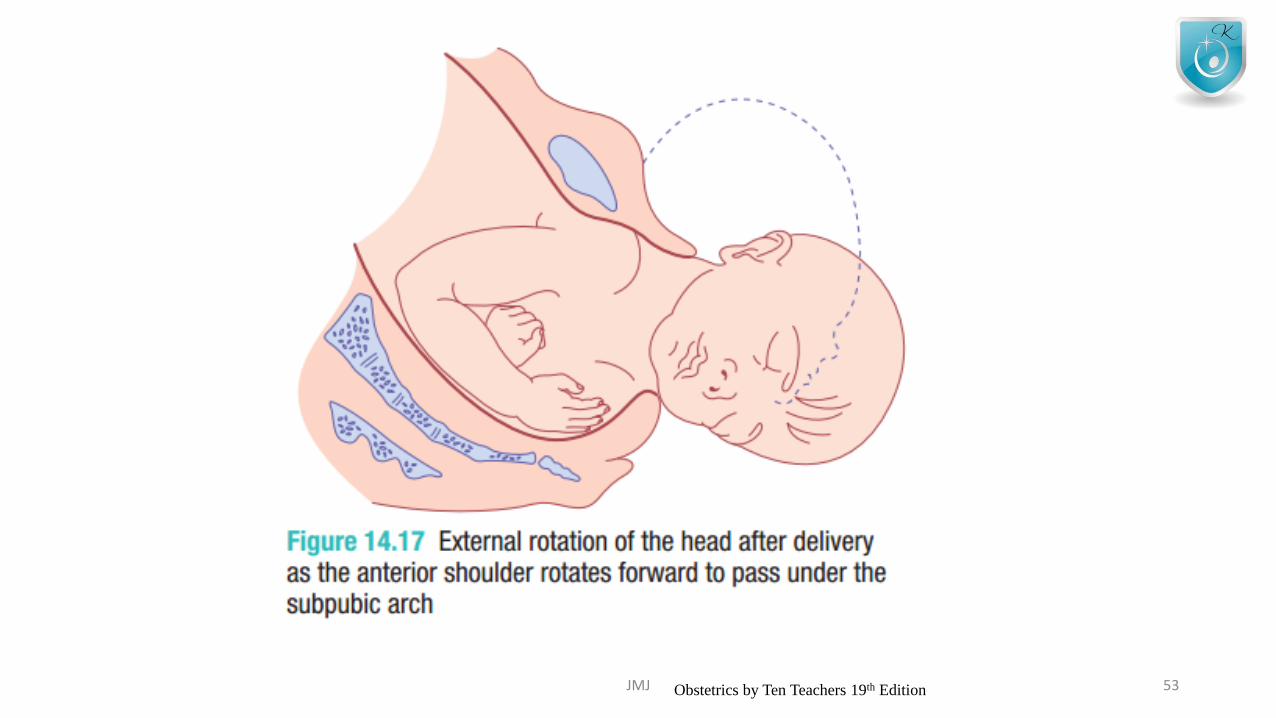
External Rotation
• In order to be delivered • Shoulders have to rotate into the direct AP plane
• When this occurs, the occiput rotates through a further 1/8th of a circle to the transverse position
JMJ 52
JMJ 53Obstetrics by Ten Teachers 19th Edition
Delivery of the shoulders and fetal body• After restitution and external rotation occurred
• Shoulders will be in AP position
• Anterior shoulder • Is under the symphysis pubis• Delivers 1st
• Rest of the body will delivered easily
JMJ 54
LABOUR Physiology of labour
JMJ 55
Physiology of labour
• Myometrium
• Cervix
• Hormonal factors
• Mechanism responsible for initiating human parturition is still unknown
JMJ 56

MYOMETRIUM
• Myometrium cells • Contains filaments of actine and myosis• Which interact and bring about contraction,• In response to increase in intracellular calcium
• Prostaglandin and oxytocin• Increase intracellular free calcium ions
• Beta adrenergic compounds, CCB• Inhibits
• Separation of actin & myosin filaments brings about relaxation of myocytes
JMJ 57
MYOMETRIUM
• Development of upper thick segment• however, unlike in any other muscle cell of the body, • this actin– myosin interaction occurs along the full length of the
filaments • so that a degree of shortening occurs • with each successive interaction.
• This progressive shortening of the uterine smooth muscle cells is called retraction and
• occurs in the cells of the upper part of the uterus.
• Retraction – results in making upper segment (thick)
JMJ 58
MYOMETRIUM
• Development of lower thin segment• It is more stretched
• This results in cervix being taken up into the lower segment of the uterus
• Cervix effaces & then dilates,
JMJ 59
JMJ 60
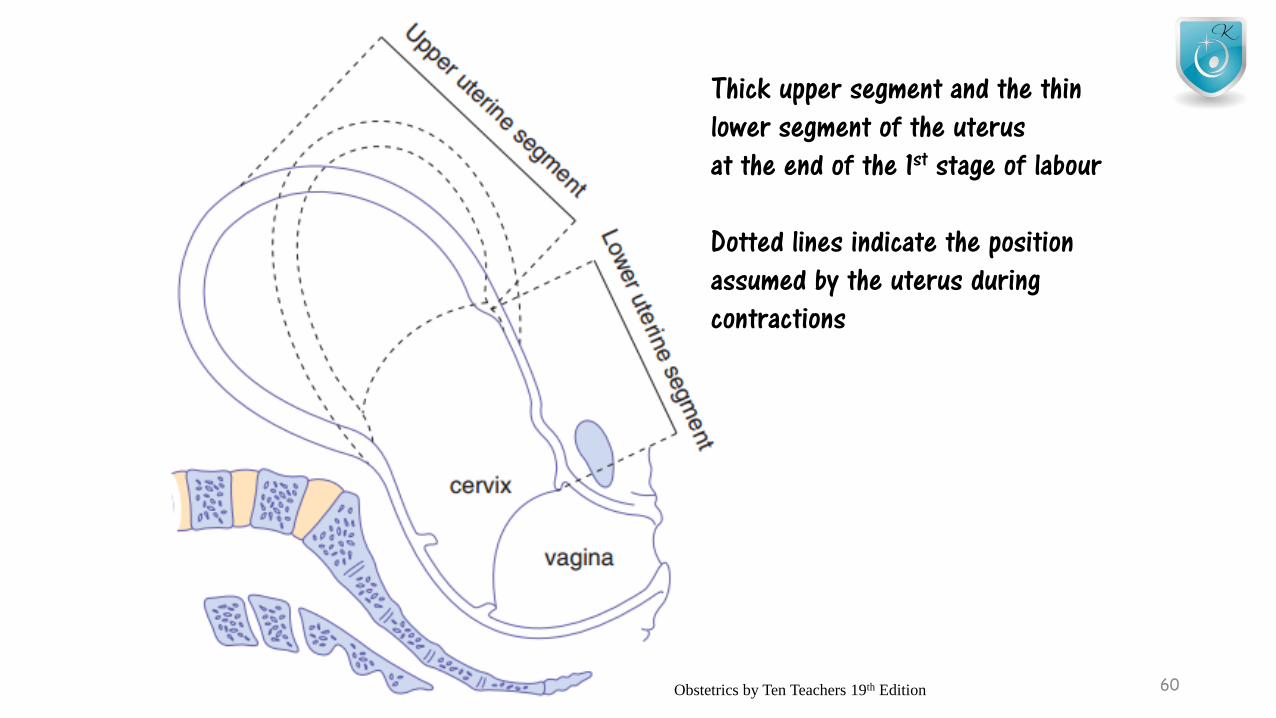
Thick upper segment and the thinlower segment of the uterus at the end of the 1st stage of labour
Dotted lines indicate the positionassumed by the uterus during contractions
Obstetrics by Ten Teachers 19th Edition
Myometrium
• Myocytes of the uterus contracts together
• Individual myometial cells are laid down in a mesh of collagen
• Cell-to-cell communication by gap junctions• These gap junctions are absent for most of the pregnancy ,
but appears at term• Prostaglandins stimulate the formation of gap junction• Beta- adrenergic - opposite
JMJ 61
Myometrium
• Uterine contractions are involuntary in nature
• Minimal extrauterine neuronal control
• Majority of labour –• occurs at intervals of 2-4 minutes
• Intensity or amplitude of the intrauterine pressure generated with each contraction averages between 30 to 60 mmHg
JMJ 62

Cervix• Contains muscles and fibroblasts,
• Separated by ‘ground substance’ made up of extracellular matrix molecule
• Under the influence of prostaglandin and other humoral mediators• There is an increase in proteotyric activity• Reduction in collagen and elastin
• Interleukins bring about a pro-inflammatory change – with significant invasion by neutrophils
• Dermatan sulphate is replaced by the more hydrophilic hyaluronic acid
• Which results in increase in water content in cervix
• This causes cervical softening or ripening,
• So that contractions, when they begin, can bring about the process of effacement and dilatation
JMJ 63
Hormonal factors• Progesterone
• Maintains uterine quiescence by,• Suppressing prostaglandin production• Inhibiting communication between myometrial cells and
preventing oxytocin release
• Oestrogen• Opposes the action of progesterone
• Prior to labour, • there is a reduction in progesterone receptors and • an increase in the concentration of oestrogen relative
to the progesterone
JMJ 64
Hormonal factors• By chorion and decidua
• Increased prostaglandin synthesis• Leading to increase in calcium influx into myometrial
cells
• Corticotrophin-releasing hormone (CRH)• Produced by placenta• Increase contractions towards term• Potentiates the action of prostaglandin & oxytocin on
myometrial contractility
• Fetal pituitary oxytocin• Fetal adrenals cortisol
JMJ 65
Stimulates the conversionof progesterone to oestrogen
LABOURMANAGEMENT OF NORMAL LABOUR
JMJ 66
History
• Details of previous births & the size of previous babies• Frequency, duration & perception of strength of the contractions
and when they began
• Whether the membranes have ruptures• Colour and amount of amniotic fluid
• Presence of abnormal vaginal discharge or bleeding• Recent activity of the fetus• Any medical issues• Special requirements (psychological needs)
JMJ 67

General Examination
• Body mass index
• Temperature
• Pulse
• Blood pressure
• Urine tests for• Protein / blood / ketones/ glucose
JMJ 68
Abdominal Examination
• Inspection for scars• Lie of the fetus• Presenting part
• Cephelic or breech
• If cephalic, degree of engagement• If 5/5 – do USS- to figure out the reason for high head
• OP position• Deflexed head• Placenta previa• Fibroids
• Assessment of contractions – by palpation• Can comment only on frequency and duration of contractions• Not the strength
JMJ 69
Vaginal Examination
• Examine cervix for• Dilatation• Effacement• Application of the presenting part
• Dilatation – comment by cm• If cannot feel for the cervix- fully dilated
• Length of the cervix• At 36 weeks – 3cm
• At about 4cm of dilatation, the cervix should be fully effaced
JMJ 70
Vaginal Examination
• Normal labour- presenting part is vertex
• Occiput is identified by feeling for triangular posterior frontenelle
• Normally occiput will be • Transvers (OT position)• Anterior (OA position)
JMJ 71
Vaginal Examination
• Conditions of the membranes should be noted• Copious amount of clear fluid –
• good prognosis• Heavily blood stained or meconium stained fluid –
• warning sign for fetal compromise
• Women in labour should have their,• Pulse measured – hourly• Temp, & BP – 4 hourly• Frequency of contractions – 30 minutes• Vaginal examination – 4 hourly
JMJ 72
FETAL ASSESSMENT IN LABOUR
• CTG – Cardio-toco-graphy• PARTOGRAM
JMJ 73
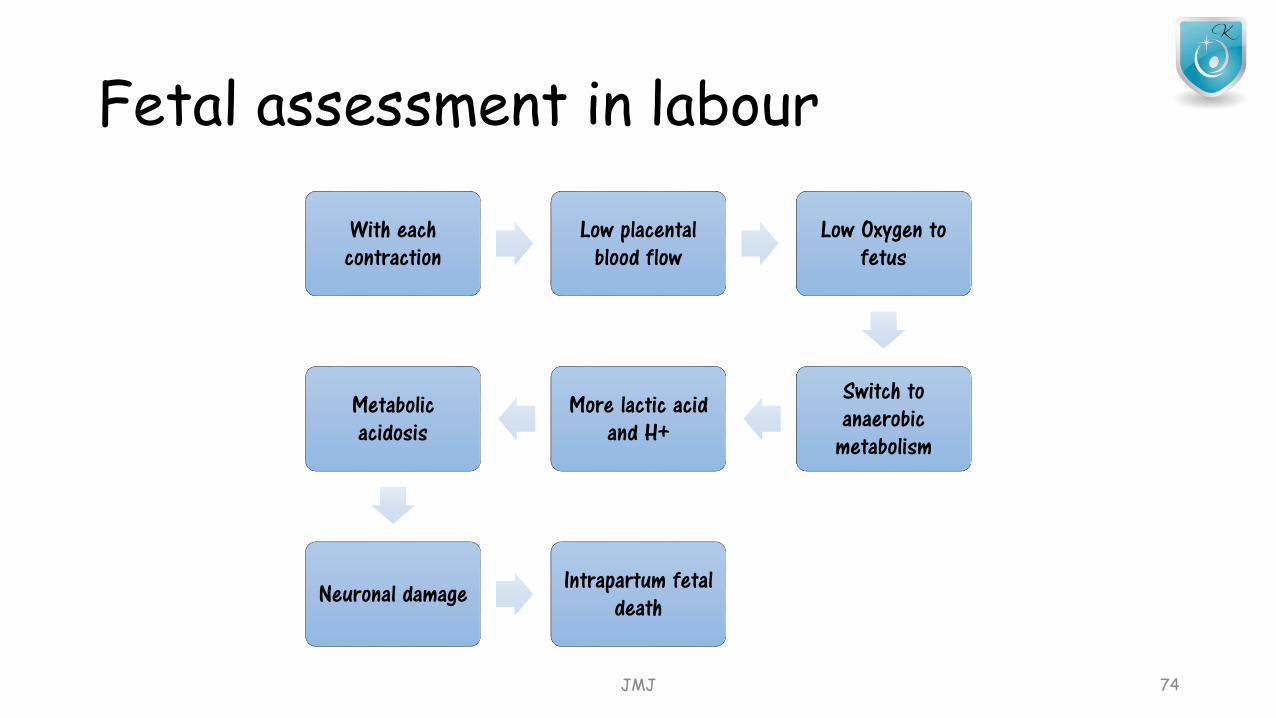
Fetal assessment in labour
With each contraction
Low placental blood flow
Low Oxygen to fetus
Switch to anaerobic
metabolism
More lactic acid and H+
Metabolic acidosis
Neuronal damage Intrapartum fetal death
JMJ 74
Passage of meconium
• Thin, very dark green or brown colour• Healthy fetus• Results of maturation of gastrointestinal physiology
• Thicker and much brighter green in colour• Intrauterine hypoxia or acidosis
JMJ 75
Fetal assessment in labour takes four forms• Observation of the colour of the liquor
• Intermittent auscultation of fetal heart using Pinardstethoscope or a hand held Doppler US
• Continuous external fetal monitoring (EFM)-by CTG
• Fetal scalp blood sampling (FBS)
JMJ 76
Fetal assessment in labour
• Women who bring labour with intermittent auscultation
• may be advised to change to continuous EFM
• if any of the following events occur during their labour• Significant meconium staining to liquor• Abnormal fetal heart rate detected by intermittent auscultation• Maternal pyrexia• Fresh vaginal bleeding• Augmentation of contractions with oxytoxin• At the request of the woman
JMJ 77
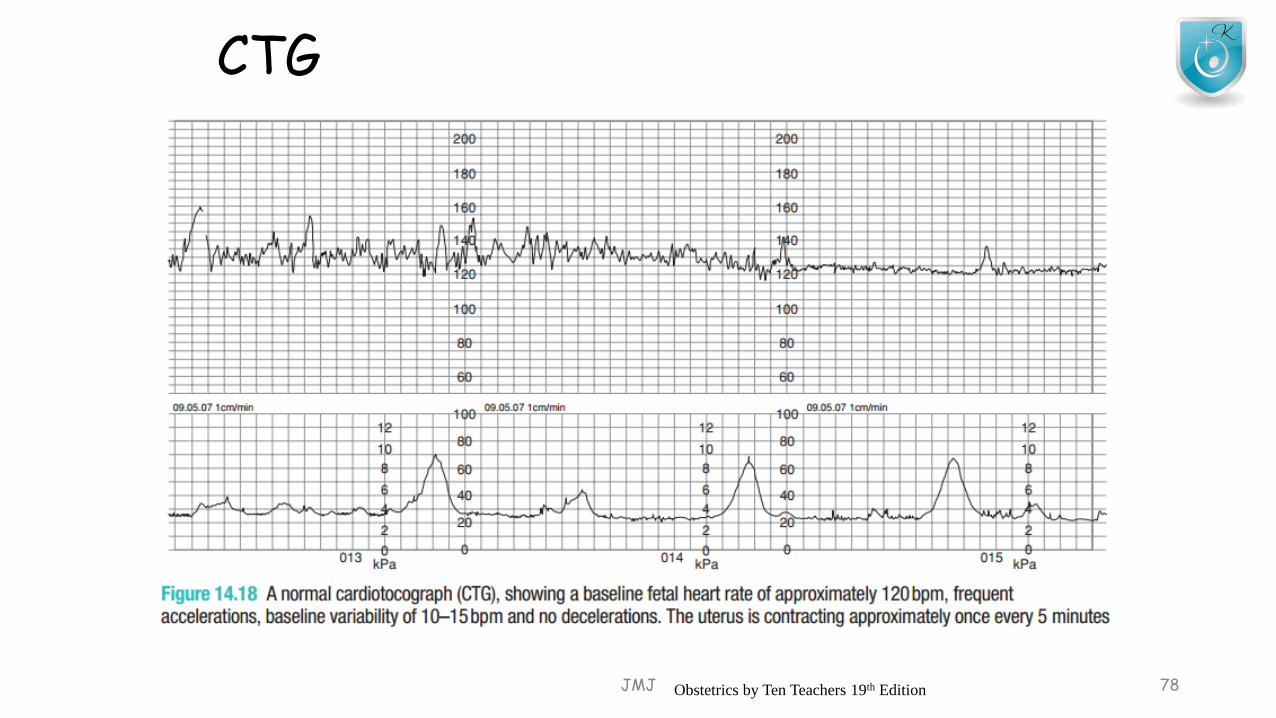
CTG
JMJ 78Obstetrics by Ten Teachers 19th Edition
CTG
• Quality is poor• Due to fetal position • Maternal obesity
• Normal parameters• Normal fetal heart rate pattern
• Baseline rate between 110-160 bpm• Baseline variability between 5 and 25 bpm• Absence of decelerations
• During 2nd stage of labour• Absence of accelerations• Presence of early decelerations tends to be normal
JMJ 79
CTG
• Each feature of CTG (baseline rate, variability, decelerations and accelerations), should be assessed each time
• Should describe as ‘reassuring’ , ‘Non-reassuring’ or ‘abnormal’ (NICE guidelines)
• If all 4 features reassuring –• Normal CTG
• If one is non-reassuring-• Suspicious CTG
• If 2 or more non-reassuring or any abnormal –• Pathological CTG
JMJ 80
Partogram
• Instance visual assessment of the rate of cervical dilatation
• Progression of the labour
• Frequency and strength of contractions
• Descent of the head in 5th palpable
• Amount and colour of the amniotic fluid draining
• Basic observation of maternal wellbeing • BP/ Pulse rate/ Temprature
JMJ 81
Management during 1st stage
JMJ 82

Key management principles of 1st stage of labour• 1st stage – timed from the Δ of labour to full dilatation of cervix
• Provision of continuity care and emotional support
• Observation of progression of labour
• Monitor fetal well being
• Adequate and appropriate pain relief
• Adequate hydration to prevent ketosis
JMJ 83
management of 1st stage of labour
• Woman in latent phase –• encourage to mobilize• Encourage and reassure them• Avoid interventions unless there is an identified risk factors• Simple analgesics preferred over NO and epidurals• No need to restrict eating and drinking (light food and clear fluid-
tolerable)• Vaginal examination – in every 4 hours
JMJ 84
management of 1st stage of labour
• Woman in active phase – (Cervical d-4cm)• Lower limit of normal progression – 1cm dilatation in every 2 hours• Descend of the fetal part
• Full dilatation may be reached, but id descent is inadequate, vaginal delivery will not occur
• During 1st stage• Membranes may be intact, ruptured spontaneously or ruptured artificially
• Maintain a partogram- maternal and fetal observations
JMJ 85
management of 1st stage of labour
• Mobility during labour is encourage (standing upright encourage the progress
• Encourage drinking water• If the woman is dehydrated- start IV fluids• To prevent ketosis, which can impair uterine contractions
• Light diet is accepted -• if no indication for GA• If they have not had pethadine or diamorphine
• Shaving and enemas are unnecessary• Antacids need only to women
• with risk factor for complications• Those who have opioid analgesia
JMJ 86
Active management of labour
• Collections of interventions
• Which are routinely recommended to
• Nulliparous women
• To maximize the chances of a normal birth
• This includes• 2 hourly vaginal examination• Early artificial rupture of membranes• Use of oxytocin augmentation if progress fell more than 2 hours
JMJ 87
Management during 2nd stage
JMJ 88
• 1st sign of the 2nd stage-• urge to push experienced by mother
• Full dilatation of cervix-• Should be confirmed by a vaginal examination, if the head is
not visible
• The women will get an expulsive reflex with each contraction, & will generally take• Deep breath, hold it and strain down (Valsalva manoeuvre
• Woman should be discourage lying supine or semi supine• Lying in the left lateral position & squatting are
particularly effective options
• Use of regional analgesia may interfere with normal urge to push
• Pushing is usually delayed for at least an hour if an epidural is in situ (‘passive phase’),
• However baby should be delivered within 4 hours after full dilatation
JMJ 89
Descent and delivery of the head
1st there is a slight general bulge as the woman strains
When head stretches the perineum, anus will begin to open
Soon after this babies head will be seen at the vulva
Between the contractions, elastic tone of the perineal muscles will push the head back into pelvic cavity
Perineal body and vulva stretches more, until fetal head is low enough to pass forward under the suprapubic arch
JMJ 90
Descent and delivery of the head… cont
When head no longer recedes between contractions (crowning) – indicated head had passed through pelvic cavity
When crowning has occur, tell woman to take rapid, shallow breaths (‘panting’)
An episiotomy cut is performed (from vaginal fourchette in a Medio lateral direction – to right)
Episiotomy is performed during –1. instrumental birth2. suspected fetal compromise
JMJ 91
Delivery of the shoulders and the rest of the body
Once fetal head is born, check whether the cord is wound tightly around the neck
If yes, cord need to clamp before delivering the rest of the body
With next contraction external rotation of the head and shoulders can be delivered
To aid delivery of the shoulders, head should be pulled gently downwards and forwards until A shoulder appears beneath the pubis
Head then lifted gradually until the P shoulder appears over the perineumbaby then swept upwards to deliver the body and legs
JMJ 92
Immediate care of the neonate
• After born, infant lies between mother’s legs • Baby will usually take 1st breath within seconds
• No need for immediate clamping of the cord• Nearly 80ml of blood will transferred from placenta to the baby, before
cord pulsation cease• Reduces the chances of neonatal anemia and iron deficiency
• Oropharyngeal aspiration is only done if necessary • After clamping & cutting cord – calculate APGAR score –
• 1 minute and • 5 minutes
JMJ 93
Immediate care of the neonate
• Immediate skin to skin contact between mother & baby• Help bonding• Promote further release of oxytocin
• Baby should be dry and cover with warm blanket• Initiation of breastfeeding – 1st ½ hour of life
• Newborn measurements – temperature, head circumference, birth weight
• 1st dose of vitamin K should be given
JMJ 94

Management during 3rd stage
JMJ 95
• Normally take 5 to 10 minutes
• Separation of placenta occurs because• Reduction of volume of uterus
• Due to uterine contractions and retraction
• Signs of separation are• Lengthening of the cord protruding from vulva• A small gush of blood from the placental bed, which normally stops
quickly due to retraction of the myometrial fibers• Rising of the uterine fundus to above the umbilicus• Fundus becomes hard & globular compared to board
JMJ 96
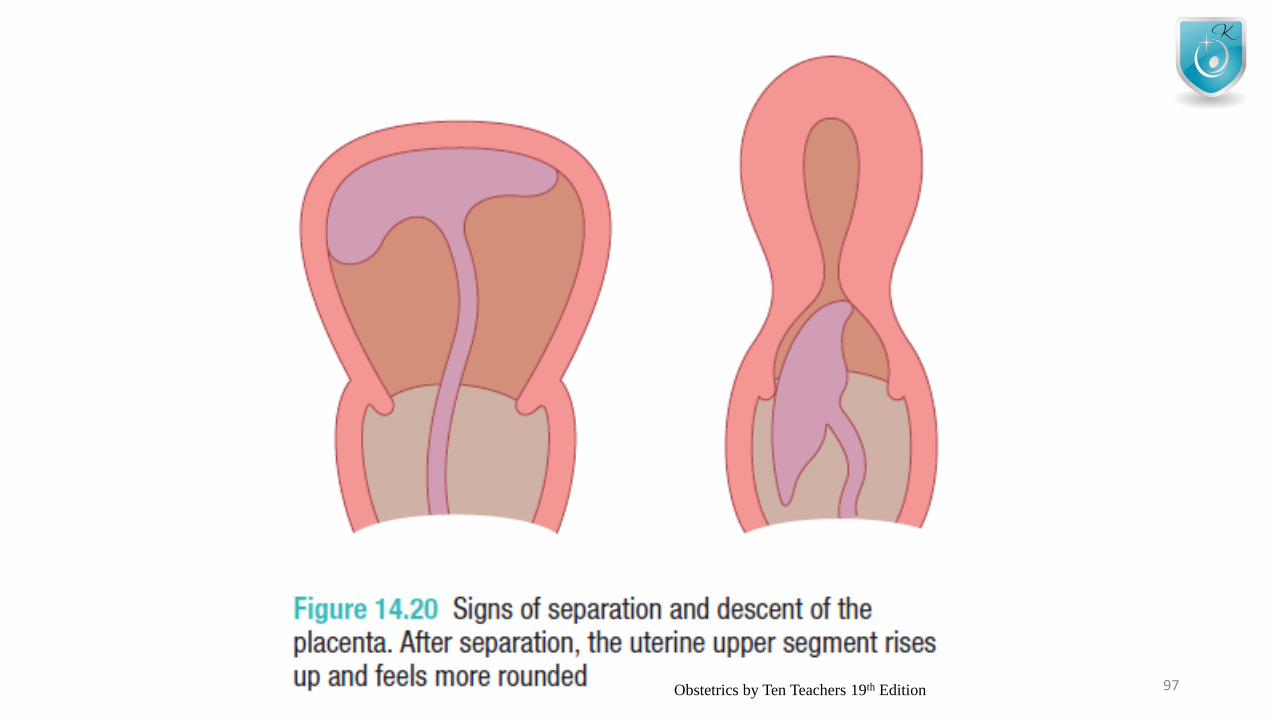
JMJ 97Obstetrics by Ten Teachers 19th Edition
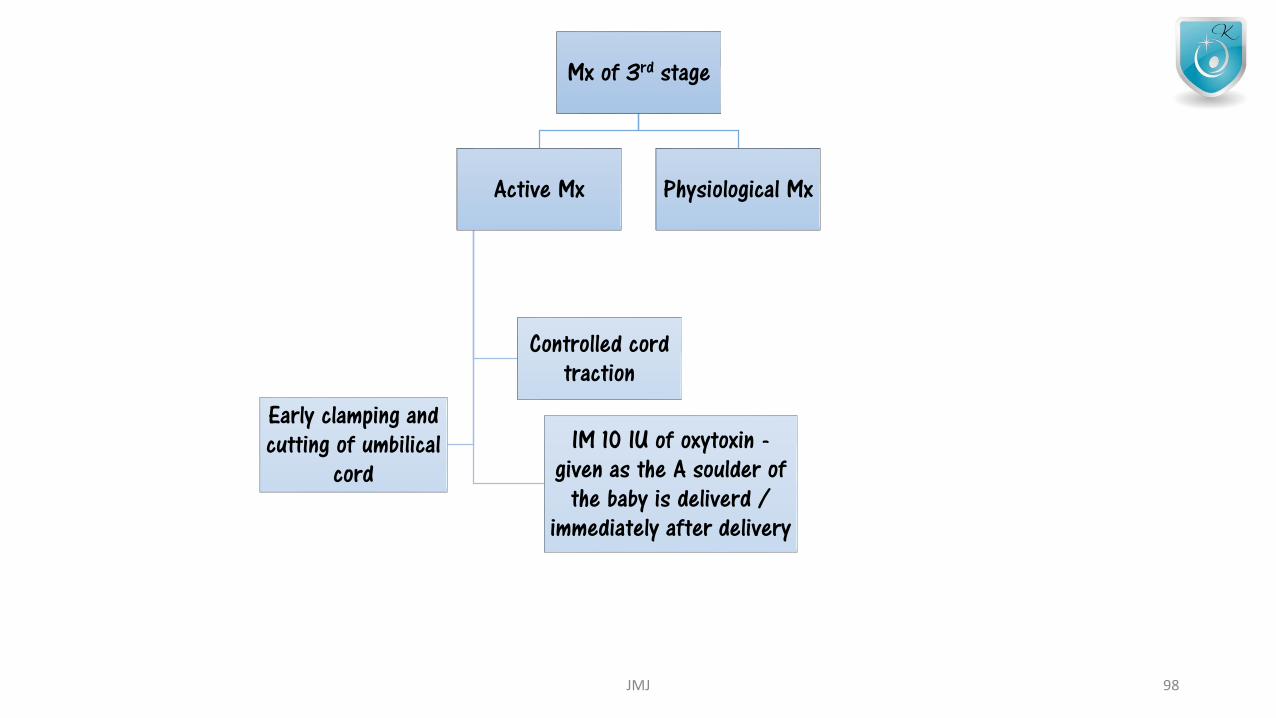
Mx of 3rd stage
Active Mx
IM 10 IU of oxytoxin -given as the A soulder of
the baby is deliverd / immediately after delivery
Early clamping and cutting of umbilical
cord
Controlled cord traction
Physiological Mx
JMJ 98
Active Management
• Recommended to all women – to reduce risk of PPH
• When signs of placental separation are recognized • Control cord traction is used
• When contractions are felt• Left hand should be moved suprapubically• & the fundus elevated with the palm facinf toward the mother• Right hand should grasp the cord• Use twisting motion
• Uterine inversion – rare complication
JMJ 99
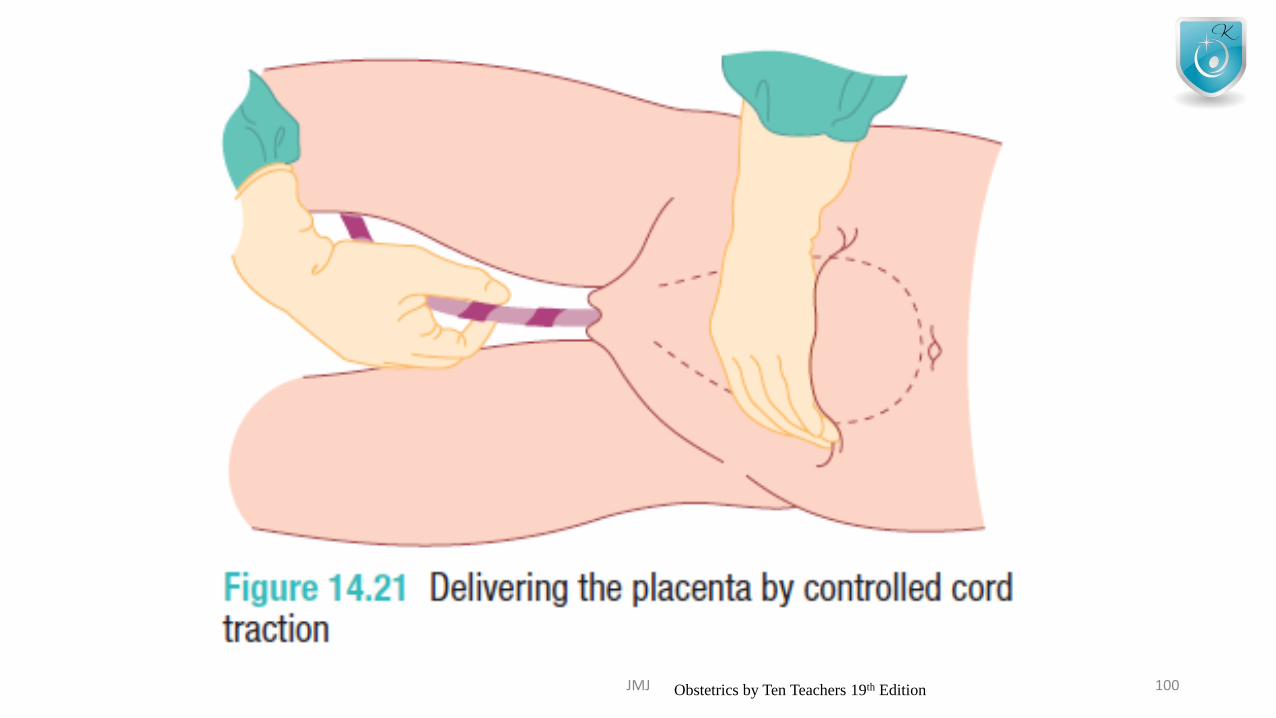
JMJ 100Obstetrics by Ten Teachers 19th Edition
Active Management
• 2% - placenta will not expelled
• If no bleeding occurs• Further attempt at controlled cord traction should be made after 10
minutes
• If that fails manual removal under GA or regional anesthesia
• Direct injection of oxytocin into the umbilical vein – may bring about delivery of the placenta
JMJ 101
Physiological Management
• Where the placenta is delivered by the maternal effort
• No uterine drugs are given to assist
• Associated with heavy bleeding
• Can wait up to 60 minutes
JMJ 102
• After completion of 3rd stage• Inspect placenta for missing cotyledons or succenturiate
lobe• If anything suspected -> manual removal (US guided)
• Inspect vulva for an tears extending into perineal muscles
JMJ 103

Key features of normal labour are
• Spontaneous onset• Single cephalic presentation• 37- 42 weeks gestation• No artificial interventions• unassisted spontaneous vaginal delivery• Dilatation of at least 1cm every 2 hrs in the active phase of 1st stage• An active 2nd stage of no more than 2hr primiparous woman
no more than 60 minutes in multiparous woman• 3rd stage lasting no more than 30 minutes with active management
JMJ 104
LABOUR – 02ABNORMAL LABOUR
JMJ 105
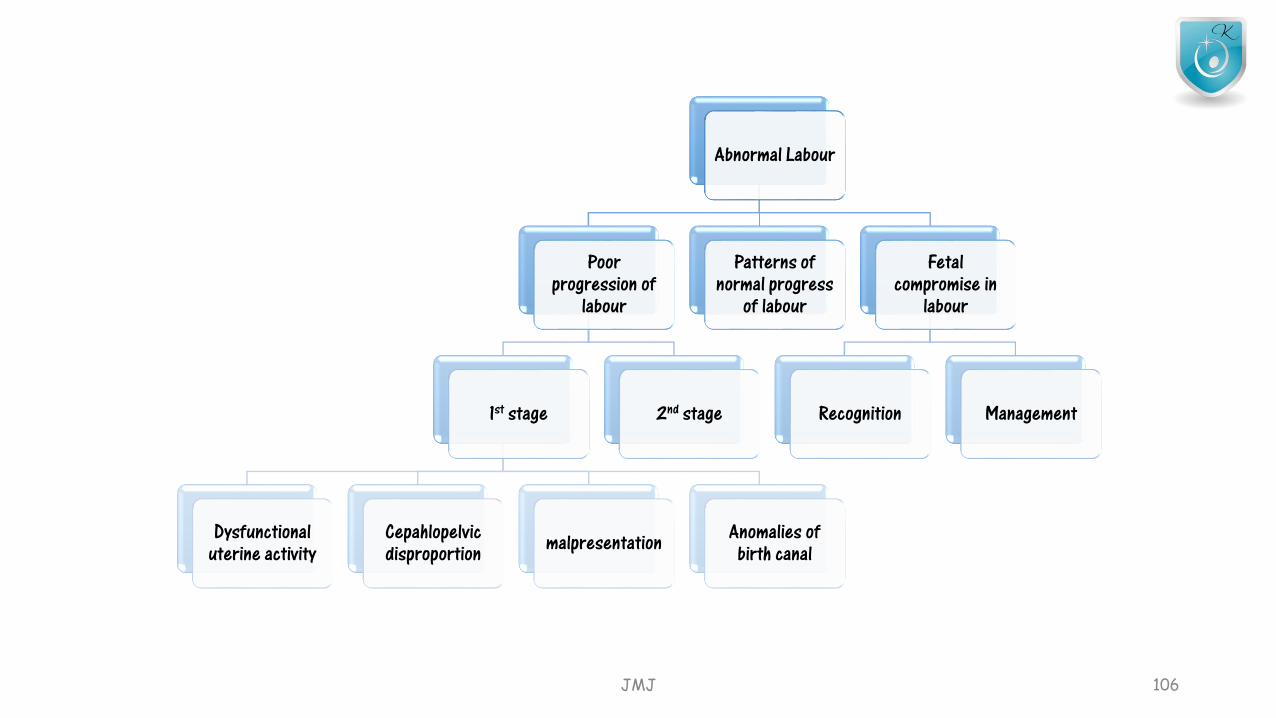
Abnormal Labour
Poor progression of
labour
1st stage
Dysfunctional uterine activity
Cepahlopelvicdisproportion malpresentation Anomalies of
birth canal
2nd stage
Patterns of normal progress
of labour
Fetal compromise in
labour
Recognition Management
JMJ 106
Poor progress of 1st stage of labour
• Defined as• Cervical dilatation of less than 2cm in 4 hours• Associate with failure of descent &• Rotation of the fetal head
• Progress dependent on 3 variabilities• Power
• The efficiency of the uterus• Passenger
• Fetus (Size, presentation, position)• Passage
• Uterus, cervix, bony pelvis
JMJ 107
Dysfunction of the uterine cavity
• Most common cause
• Common in primigravida & older women(weak contractions)
• Assessment done by• Clinical examination• External uterine tocography• Intrauterine pressure catheter (more accurate)
• Frequency of 4-5 contractions per 10 minutes- ideal
JMJ 108
Dysfunction of the uterine cavity
• When poor labour suspected• Repeat vaginal examination 2 hrly
• If confirmed• ARM
• If still poor progress till 2 hours• Oxytocin infusion- slow rate• Increase carefully in 30 minutes
• Continuous EMF• Multiparous women- less likely to experience poor progress (excepts
malposition or malpresentation)
JMJ 109
Dysfunction of the uterine cavity
• Excessive uterine contractions in a truly obstructed labour• Results in uterine rupture in multiparous women
• Augmentation with oxytocin is contraindicated
• if there are concerns regarding the condition of the fetus
• If progress fails to occur despite 4-6 hours of augmentation with oxytocin,
• a Caesarean section will usually be recommended
JMJ 110
Cephalopelvic disproportion (CPD)
• Anatomical disproportion between the fetal head and maternal pelvis• Due to
• Large head• Small pelvis• Combination of the 2
• Women with short stature (<1.60m), with a large baby in their 1st pregnancy –high risk
• Obstructive hydrocephalus – macrocephaly• Fetal thyroid & neck tumors – extension of neck• OP position – deflexion of the fetal head , presents a larger skull diameter to
the maternal pelvis
JMJ 111

Cephalopelvic disproportion (CPD)
• Cephalopelvic disproportion is suspected in labour• Progress is slow or actually arrests despite efficient uterine
contractions• The fetal head is not engaged• Vaginal examination shows sever maulding & caput formation• Head is poorly applied to the cervix
• Oxytocin can be given carefully to a primigravida with mild to moderate CPD
• Oxytosin must never be used in a multiparous women where CPD is suspected
JMJ 112
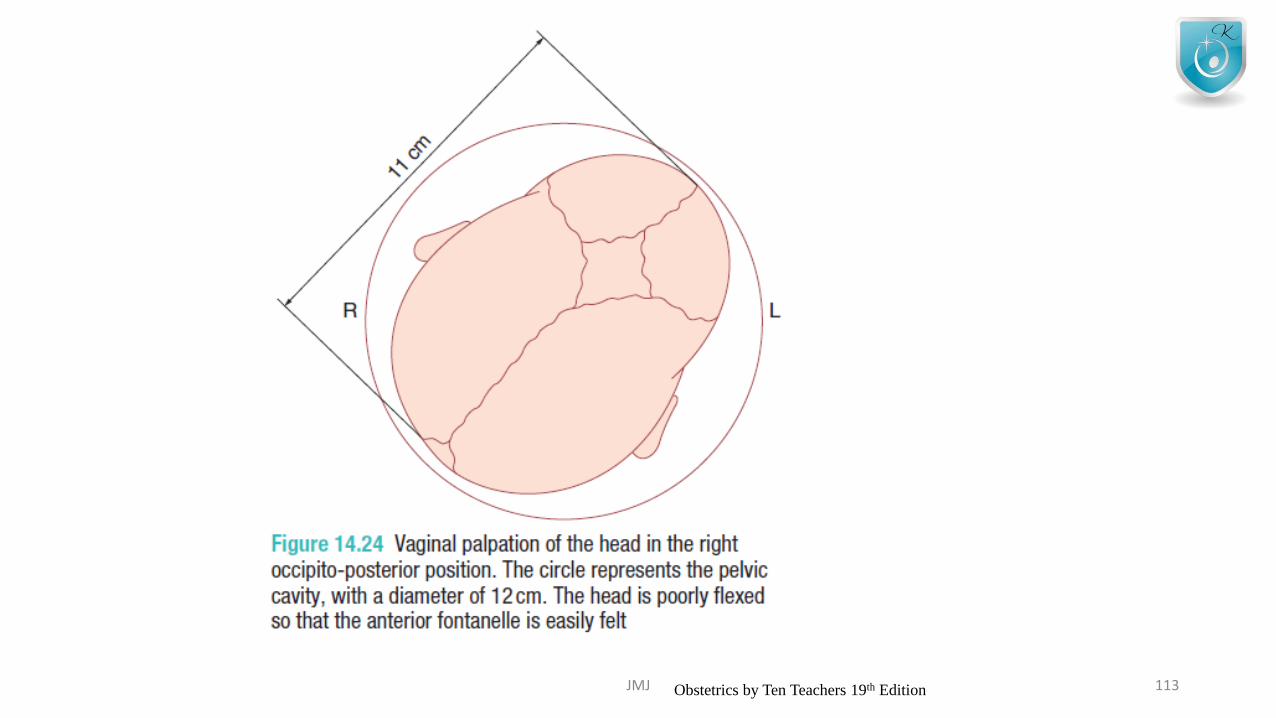
JMJ 113Obstetrics by Ten Teachers 19th Edition
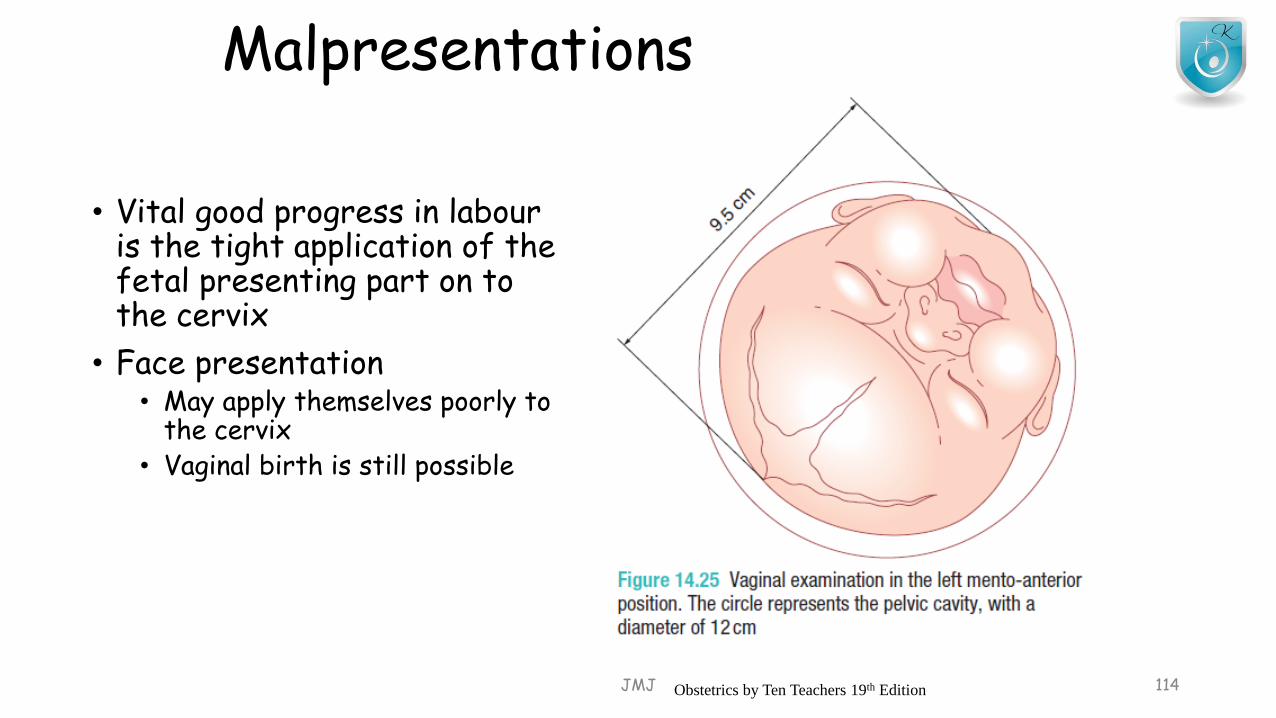
Malpresentations
• Vital good progress in labouris the tight application of the fetal presenting part on to the cervix
• Face presentation• May apply themselves poorly to
the cervix• Vaginal birth is still possible
JMJ 114Obstetrics by Ten Teachers 19th Edition
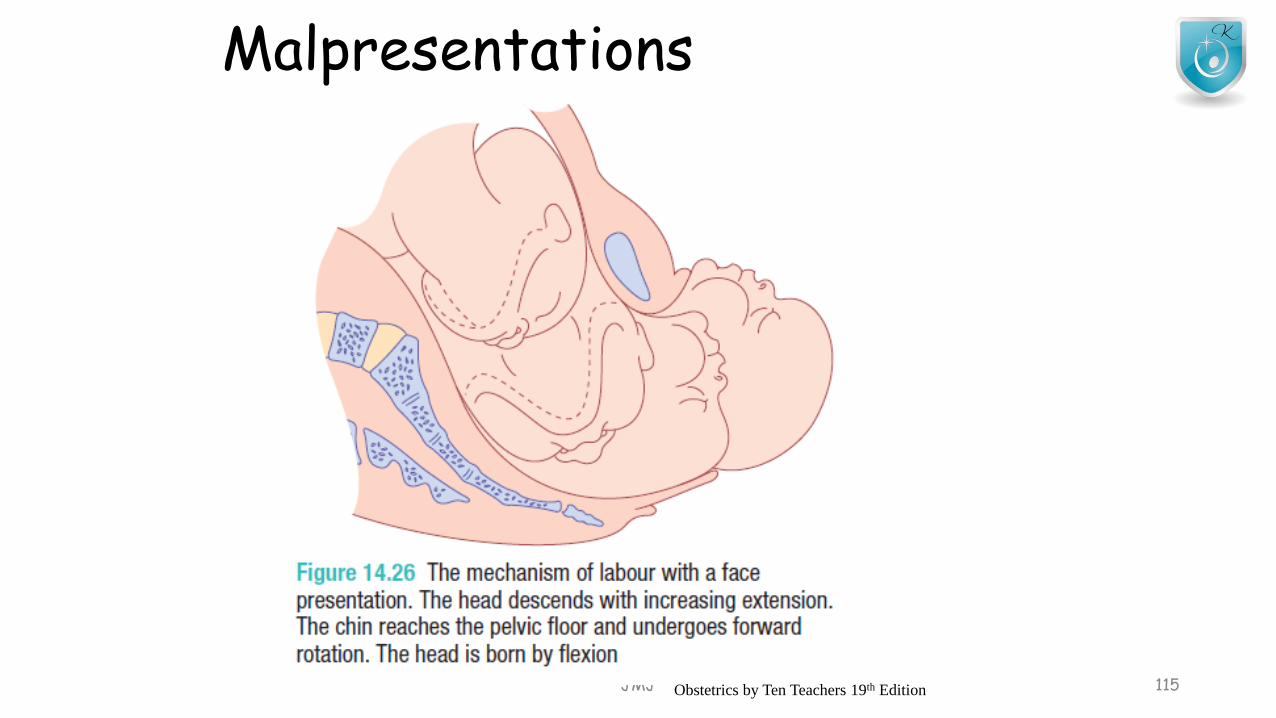
Malpresentations
JMJ 115Obstetrics by Ten Teachers 19th Edition
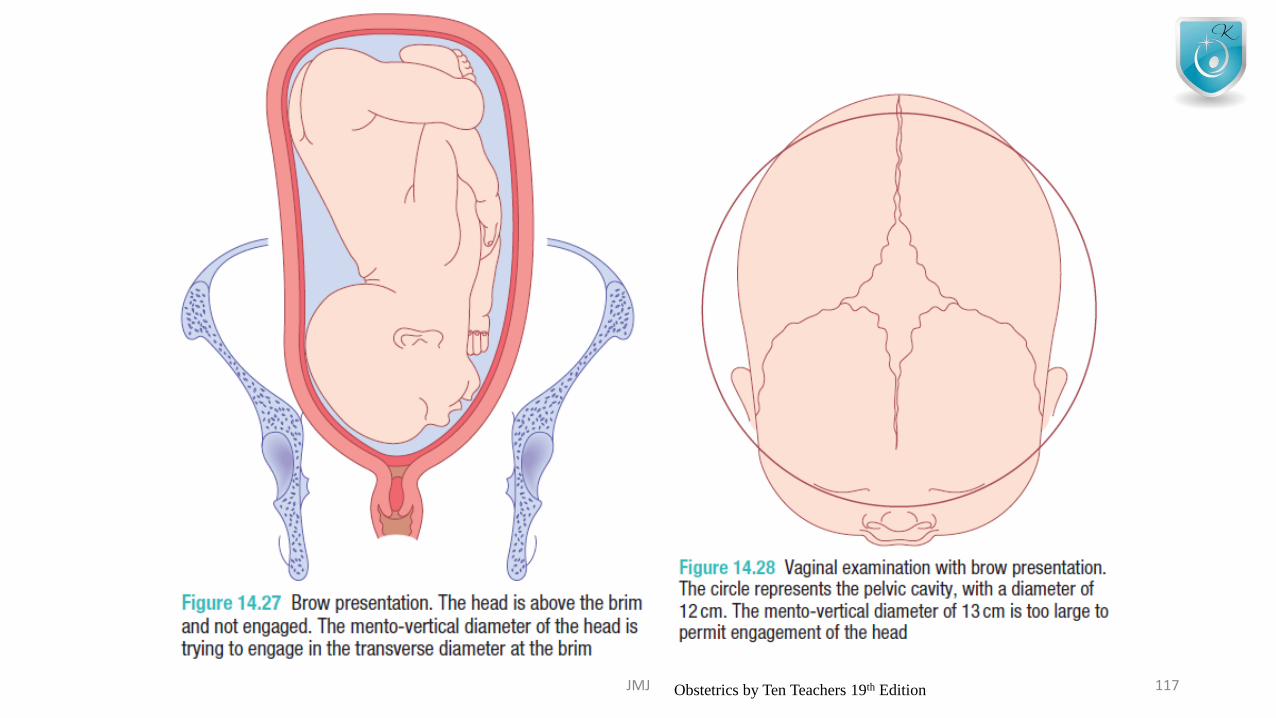
Malpresentation
• Brow presentation• Mento-verticle diameter • Too large to fit through the bony pelvis, unless flexion occurs or • hyperextension to a face presentation
• Shoulder presentation• Cannot deliver vaginally
• Malpresentations are common in women with• High parity• Risk of uterine rupture
JMJ 116
JMJ 117Obstetrics by Ten Teachers 19th Edition
Abnormalities of the birth canal
• Abnormalities of the uterus and cervix
• Unsuspeccted fibroids in the lower uterine segment –prevent descend
• Delay can caused by cervical dystocia• non-compliant cervix which effaces but fails to dilate because of
severe scarring, usually as a result of a previous cone biopsy.
JMJ 118
Poor progress in the 2nd stage of labour
• Birth is expected to take place within 3 hrs of the start of the active 2nd stage
• Delay diagnosed if delivery is not immitent after• 2 hr of pushing – nulliparous labour• 1 hour of pushing – multiparous labour
• Causes for 2nd stage delay• Abnormalities of power• Passenger• passage
JMJ 119
• 2ry uterine inertia –• common cause of 2nd stage delay• May be exacerbated by epidural analgesia
• Maternal dehydration causing ketosis• Weak uterine contractions• Tx-rehydration & IV oxytocin –if primi
• Persistent OP position – fetal head• Either head has to undergo long rotation to OA
position• Delivered in the OP position (face to pubes)
• When 2nd stage has been diagnosed,• Never start oxytocin
JMJ 120
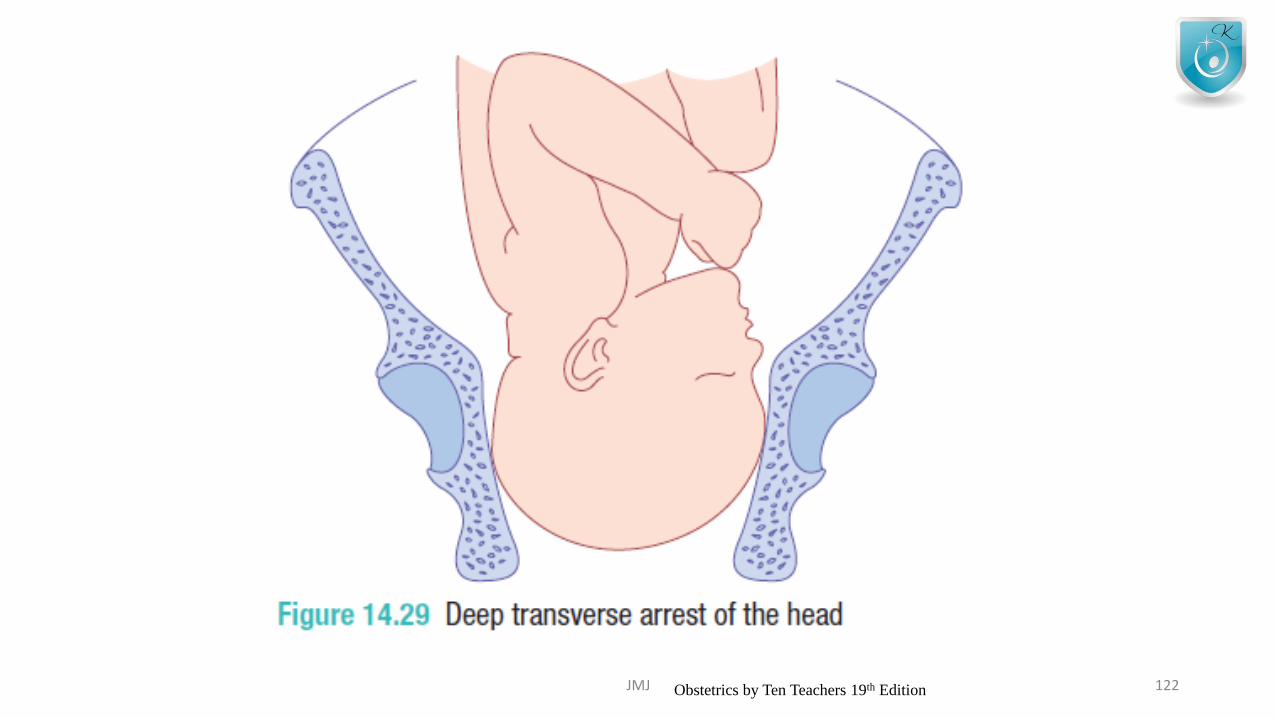
• Narrow – mid pelvis (android pelvis)• Prevents internal rotation of fetal head
• This may result in the arrest of the descent of the fetal head
• at the level of the ischial spines • in the transverse position
• “DEEP TRANSVERSE ARREST”
• Instrumental birth should be considered for prolonged 2nd stage
JMJ 121
JMJ 122Obstetrics by Ten Teachers 19th Edition
Risk factors for poor prognosis in labour• Small woman
• Big baby
• Dysfunctional uterine activity
• Malpresentation
• Malposition
• Early membrane rupture
• Soft-tissue/pelvic malformation
JMJ 123
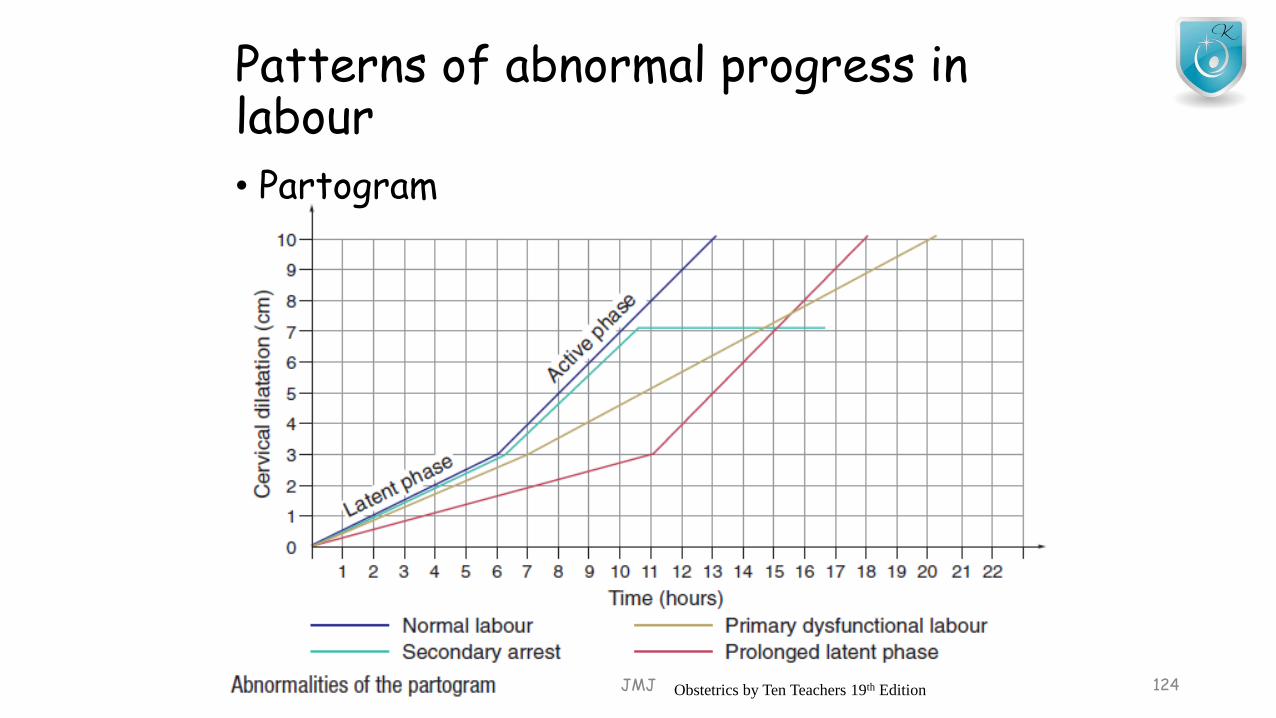
Patterns of abnormal progress in labour• Partogram
JMJ 124Obstetrics by Ten Teachers 19th Edition
• Prolonged latent phase• More common in primiparous woman
• Primary dysfunctional labour• Poor progress in the active phase of labour (<2cm
cervical dilatation/4 hourly)• Common in primi women
• 2ry arrest • When progress in the active phase of 1st stage is
initially good but then slows, • stops altogether• Typically after 7cm dilatation
JMJ 125

Poor progress in labour
• Different patterns +• Insufficient uterine cavity – most common cause• Fetal malposition, malpresentation, and true CPD are other causes
• May occur in isolation or in combination with inefficient uterine contractions• ARM is a simple intervension which may shortens labour, but does not influence the overall
outcome• Use of oxytocin – relatively safe in nulliparous women• Use of oxytocin augmentation – less safe because of greater risk of uterine
hyperstimulation, fetal compromise & uterine rupture in the face of obstruction• Oxytocin does not have a significant impact on the mode of delivery, but does shorten the
length of labour
JMJ 126
Fetal compromise in labour
• Reduction in placental blood flow associated with contractions • Lead to fetal hypoxia• Eventually acidosis
• Fresh meconium staining to the amniotic fluid• Abnormal CTG
• ‘Presumed fetal compromise’ more accurate than ‘fetal distress’
JMJ 127

Risk factors for fetal compromise in labour• Placental insufficiency – fetal growth restriction and pre-eclampsia
• Prematurity
• Postmaturity
• Multiple pregnancy
• Prolonged labour
• Augmentation with oxytocin
• Uterine hyperstimulation
• Precipitated labour
• Intrapartum abruption
• Cord prolapse
• Uterine rupture / dehiscence
• Maternal diabetes
• Cholestasis of pregnancy
• Maternal pyrexia
• Chorioamnionitis
• Oligohydroamnios JMJ 128
Recognition of fetal compromise
• Meconium staining• Thick or tenacious• Dark green• Bright green• Black
• Thin & light meconium – is more likely to represent fetal gut maturity
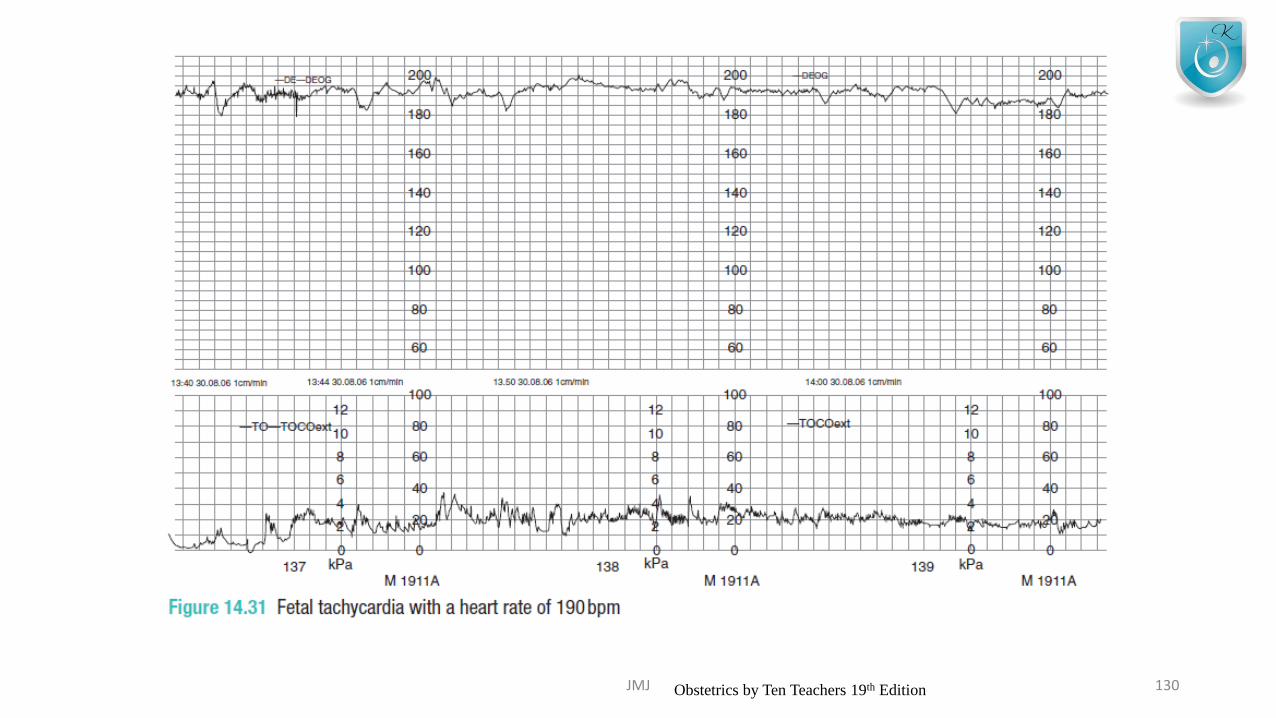
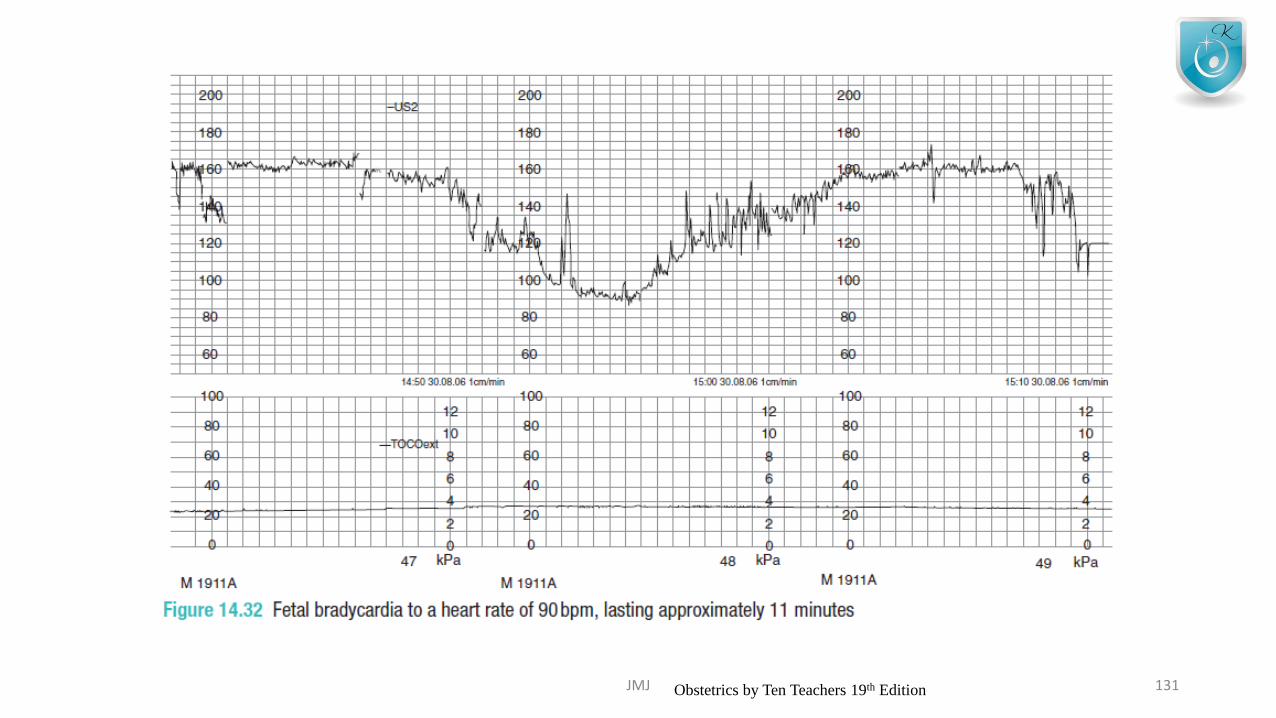
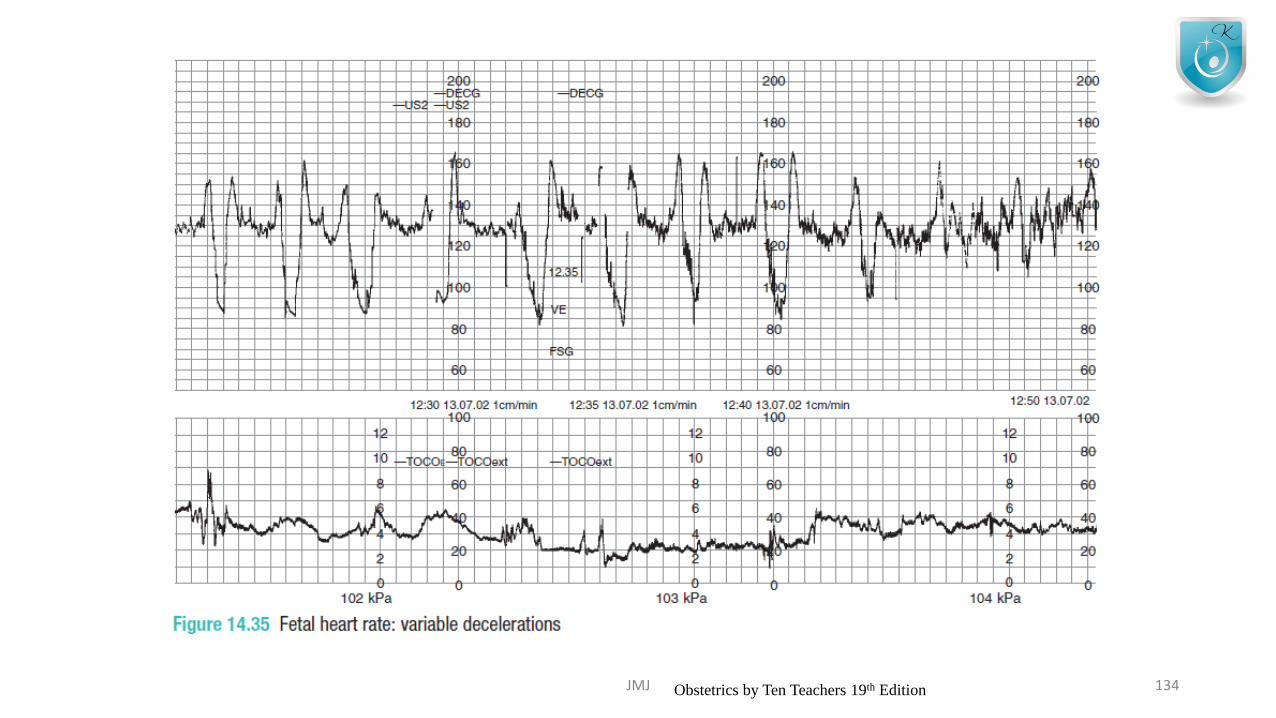
• CTG changes• Fetal tachycardia• Fetal bradycardia• Fetal heart rate deceleration
JMJ 129
JMJ 130Obstetrics by Ten Teachers 19th Edition
JMJ 131Obstetrics by Ten Teachers 19th Edition
JMJ 132Obstetrics by Ten Teachers 19th Edition

JMJ 133Obstetrics by Ten Teachers 19th Edition
JMJ 134Obstetrics by Ten Teachers 19th Edition
JMJ 135Obstetrics by Ten Teachers 19th Edition
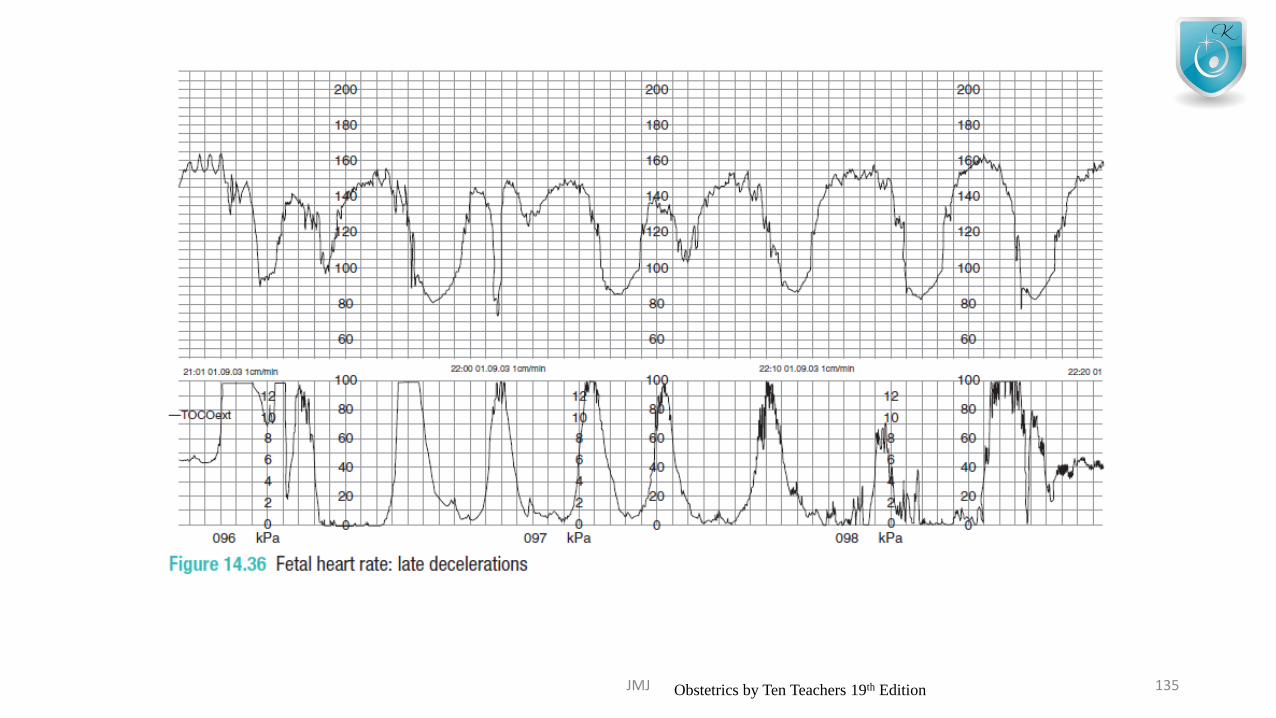
CTG signs suggestive of fetal compromise• Fetal tachycardia (>160 bpm, or a steady rise over the
course of labour)
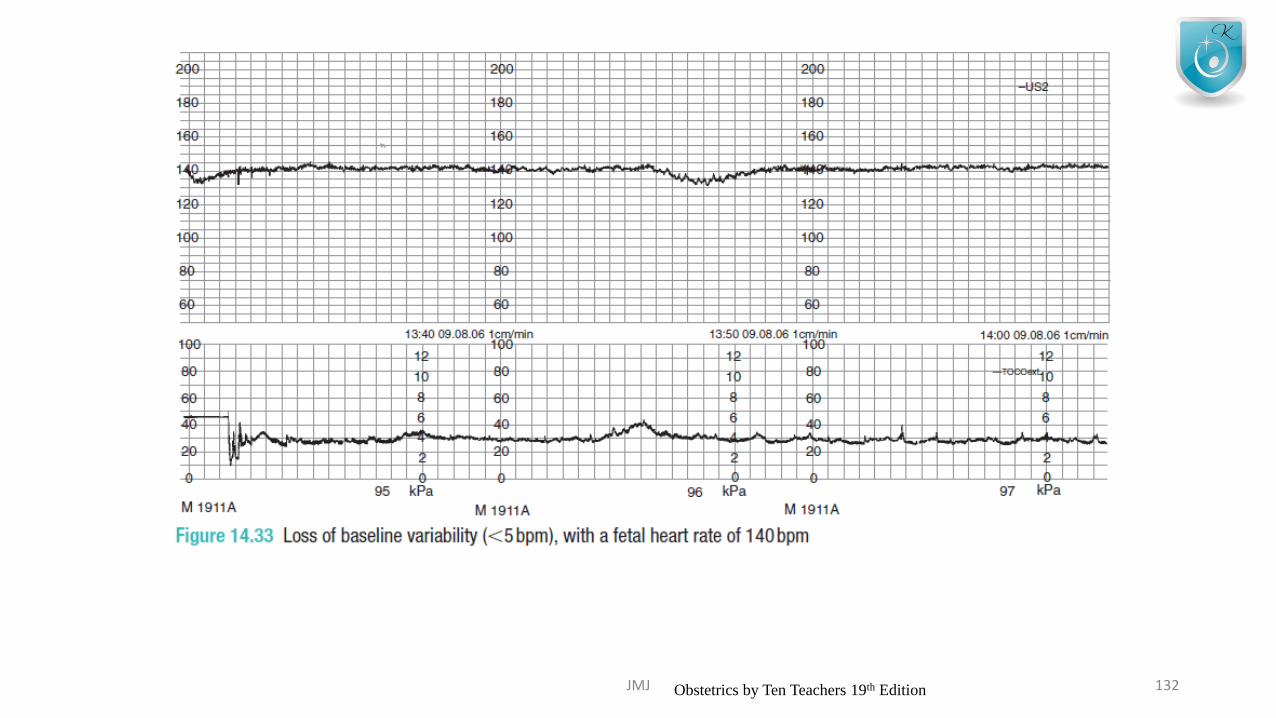
• Loss of baseline variability (<5bpm)
• Recurrent late decelerations
• Persistent variable decelerations
• Fetal tachycardia (<100 bpm for more than 3 minutes)
JMJ 136
Management of possible fetal compramise• Number of resuscitative manoeuvres
• Should be considered when a CTG is classified as ‘suspicious’
• If a CTG becomes pathological • Do immediate vaginal examination to exclude malpresentation and cord
prolapse
• If cervix is fully dilated, • Deliver baby vaginally
• If cervix is not dilated• Instrumental delivery• Caesarean section
JMJ 137
Resuscitating the fetus in labour
• Maternal dehydration and ketosis• Can corrected with IV fluids
• Maternal hypotension • 2ry to an epidural • Can be reversed by a fluid bolus• Although a vasoconstrictor such as ephedrine is occasionally necessary
• Uterine hyper stimulation• From excess oxytocin can be treated by • turning off the infusion temporarily and • using tocolytic drugs (terbutaline)
• Venocaval compression and reduced uterine blood flow • Can be eased by turning the woman into left lateral position
JMJ 138

LABOUR O3LABOUR IN SPECIAL CIRCUMSTANCES
JMJ 139
Labour
Woman with a uterine scar Malpresentation
Breech presentation
Face presentation
Brow presentation
Shoulder presentation
Multiple gestation
JMJ 140
Women with a uterine scar
• 20% deliveries are Caesarean sections
• Out of that 99% - lower segment of the uterus• Blood loss is less• Healing is better• Low risk of uterine rupture
• Upper segment C- section “ classical”
JMJ 141
Signs of uterine rupture
• Severe lower abdominal pain
• Vaginal bleeding
• Hematuria
• Cessation of contractions
• Maternal tachycardia
• Fetal compramise
JMJ 142
• Uterine rupture likely to occur• Late in 1st stage of labour• With induction or accelerated labour• In association with a large baby
• Labour after previous Caesarean section• Vaginal birth after Caesarean section
JMJ 143
VBAC after delivery
75%
C section25%
PERCENTAGE OF PERFORMING VBAC
• Contraindications for VBAC• 2 or more previous Caesarean section scars• Need for induction of labour (IOL)• Previous labour progress and outcome suggestive of CPD
• Previous classical Caesarean section• Absolute contraindication
• Previous myomectomy• Minimal danger for rupture of membranes
JMJ 144
JMJ 145

Breech presentation
• Increased risk of cord prolapse• With footing breech presentation• With flexed breech
• Increased risk of CTG abnormalities• Cord compression
• Mechanical difficulties with delivery of the shoulder &/or after coming head• Damage to visceral organs• Traction of brachial plexus• Prolonged compression of umbilical cord & asphyxia
JMJ 146
Face presentation
• 1.500 labours• Due to complete extension of fetal head• Presenting diameter(submento-bregmatic) – 9.5cm• Same diameter as suboccipito-bragmatic (vertex) presentation• Engagement of the fetal head is late & progress is also slow.
• Because facial bones do not mould
• Diagnosed by palpating nose, mouth and eyes on vaginal examination
• Forcep delivery is permitted for low mento-anterior face presentations
JMJ 147
Face presentation
• Excellent prognosis if• If chin remains meto anterior• Possible vaginal delivery• Head being delivered by flexion
• Poor prognosis if• Chin is posterior (mento-posterior position)• Extension over the perineum cannot occur• C-section is performed• Oxytocin should not be given
JMJ 148
Brow presentation
• Lesser extreme extension of the fetal neck that that with a face presentation
• can be considered a midway position between vertex and face
• 1:2000• Brow presentation –
• As a result of exaggerated extension associated with OP position
• Presenting diameter (mento-vertical) – 13.5cm• Incompatible with a vaginal delivery
JMJ 149

Brow presentation
• Diagnosed by palpating • anterior frontenelle• Supra-orbit ridges• Nose
• If this presentation persist• Delivery by Caesarian section
JMJ 150
Shoulder presentation
• 1:300
• Due to transverse oblique lie of the fetus
• Cause of this abnormal presentation include placenta Previa
• Delivery by Caesarean section
• Delay making the diagnosis have risk of• Cord prolapse• Uterine rupture
JMJ 151
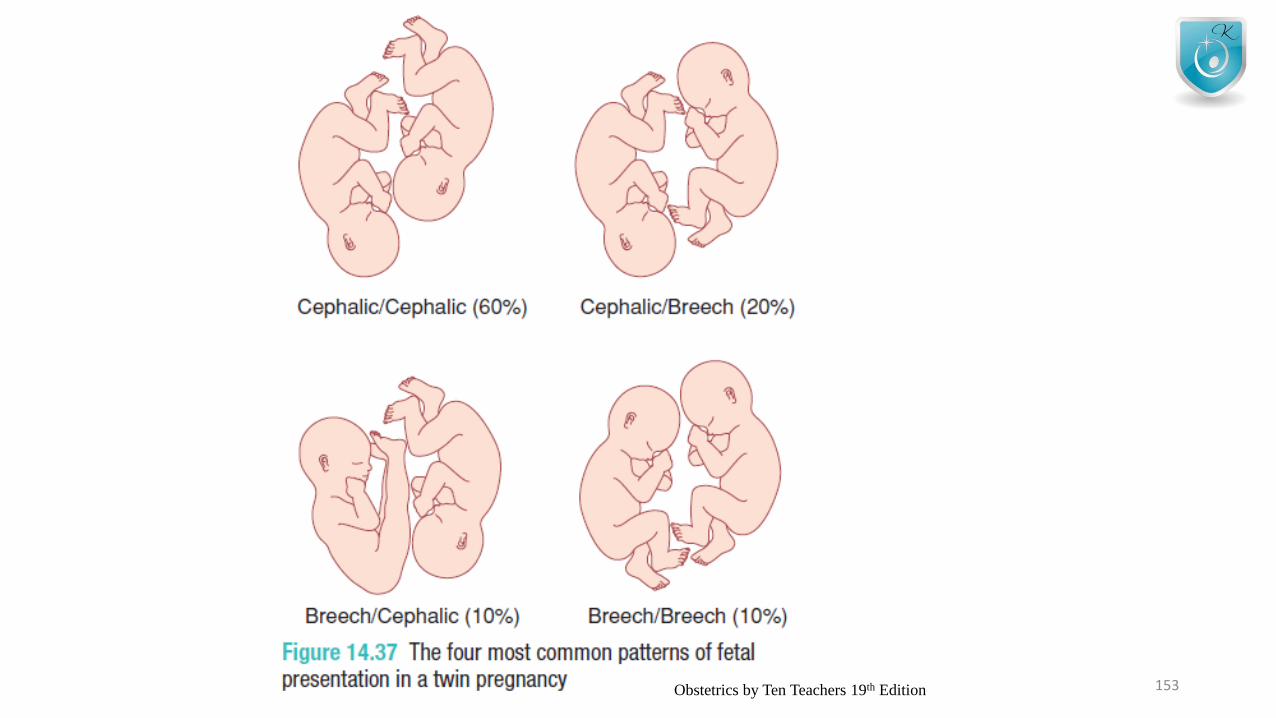
Multiple Gestation
• 1:80
• Indications for elective Caesarian section in twin pregnancy• Malpresentation of the 1st twin• Second twin larger than the 1st
• Evidence of FGR in one or both twins• Monoamniotic twins• Placenta previa• Maternal request
JMJ 152
JMJ 153Obstetrics by Ten Teachers 19th Edition
Key points• Most labours are uncomplicated and the outcomes are good.• Labour can be a hazardous journey for the baby.• Abnormalities of the uterine contractions (the ‘powers’), the fetus
(the ‘passenger’) and the pelvis and lower genital tract (the ‘passages’) can cause abnormal labour.
• The term ‘fetal distress’ is unhelpful and often misleading. If there are concerns regarding fetal well-being in labour, the term ‘presumed fetal compromise’ should be used instead.
• Augmentation of labour with oxytocin will often correct poor uterine contractions and may help to resolve fetal malposition.• Augmentation of labour with oxytocin can be dangerous in multiparous women, in those with a uterine scar, and in cases of malpresentation
JMJ 154
INDUCTION OF LABOUR
JMJ 155
Common indications for induction of labour• Prolonged pregnancy• Fetal growth restriction• Pre-eclampsia and other maternal hypertensive disorders• Deteriorating maternal illnesses• Prelabour rupture of membranes• Unexplained antepartum haemorrhage• Diabetes mellitus• Twin pregnancy continuing beyond 38 weeks• Intrahepatic cholestasis of pregnancy• Maternal iso-immunization against red cell antigens• ‘Social’ reasons
JMJ 156
induction of labour
• Recommended IOL between 41 & 42weeks
• Longer the time delay between delivery of the baby and membrane rupture• Greater risk of ascending infection (chorioamnionitis)
• Before 34 weeks• Maternal infection, fetal compromise, growth restriction
• Between 34-37
JMJ 157
Methods
• Artificial rupture of membranes
• Synthetic syntocin (Syntocinon)
• Prostaglandin PGE2• Inseted vaginally• Posterior fornix – tablet or gel• 2 doses given – 6hrs apart
• Controlled release pessery – 24hrs• Prostaglandin recommends even if the cervix is favourable
JMJ 158
Methods
• Oxytosin given IV as a dilute solution
• Mifepristone (anti-progesterone)
• Misoprostol (prostaglandin)
• Membrane sweeping - ARM
JMJ 159
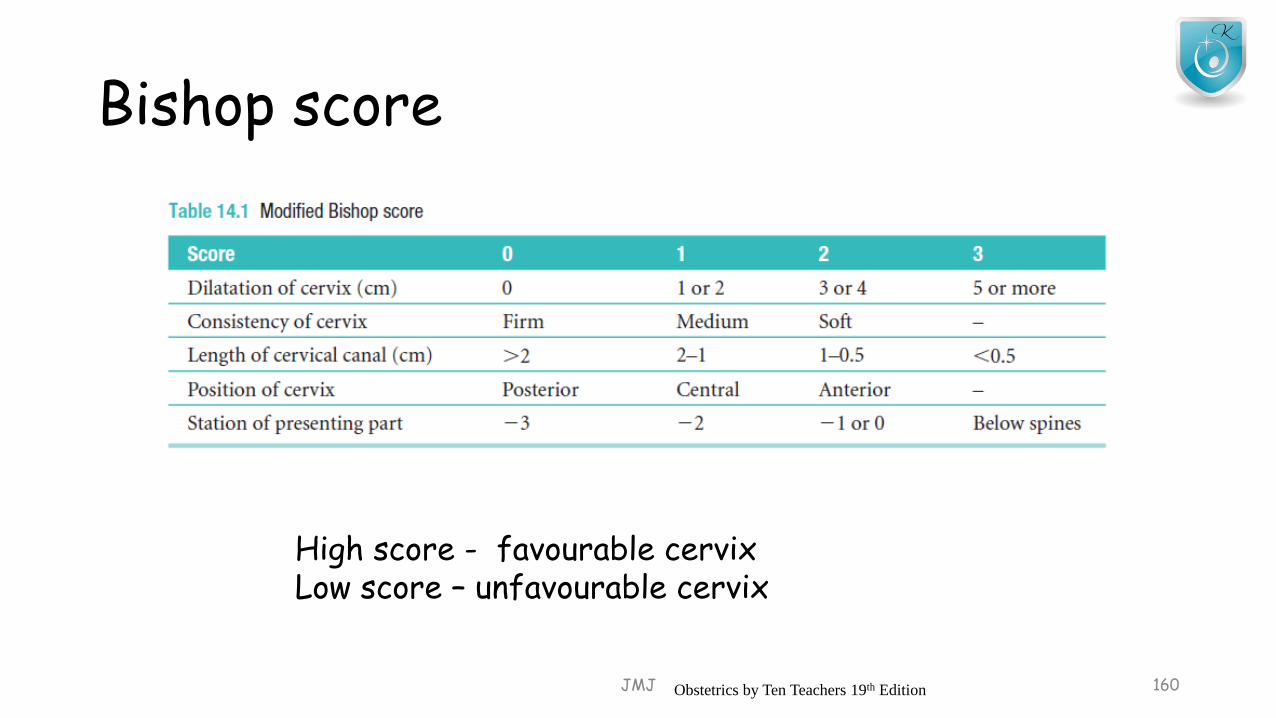
Bishop score
JMJ 160
High score - favourable cervixLow score – unfavourable cervix
Obstetrics by Ten Teachers 19th Edition
Risk of induction of labour
• Greater pain in labour
• Uterine hyperstimulation
• Cord prolapse
• Greater risk of uterine rupture during VBAC
• Failure
• Increased need for Caesarean or instrumental delivery
• Fetal compromise
JMJ 161
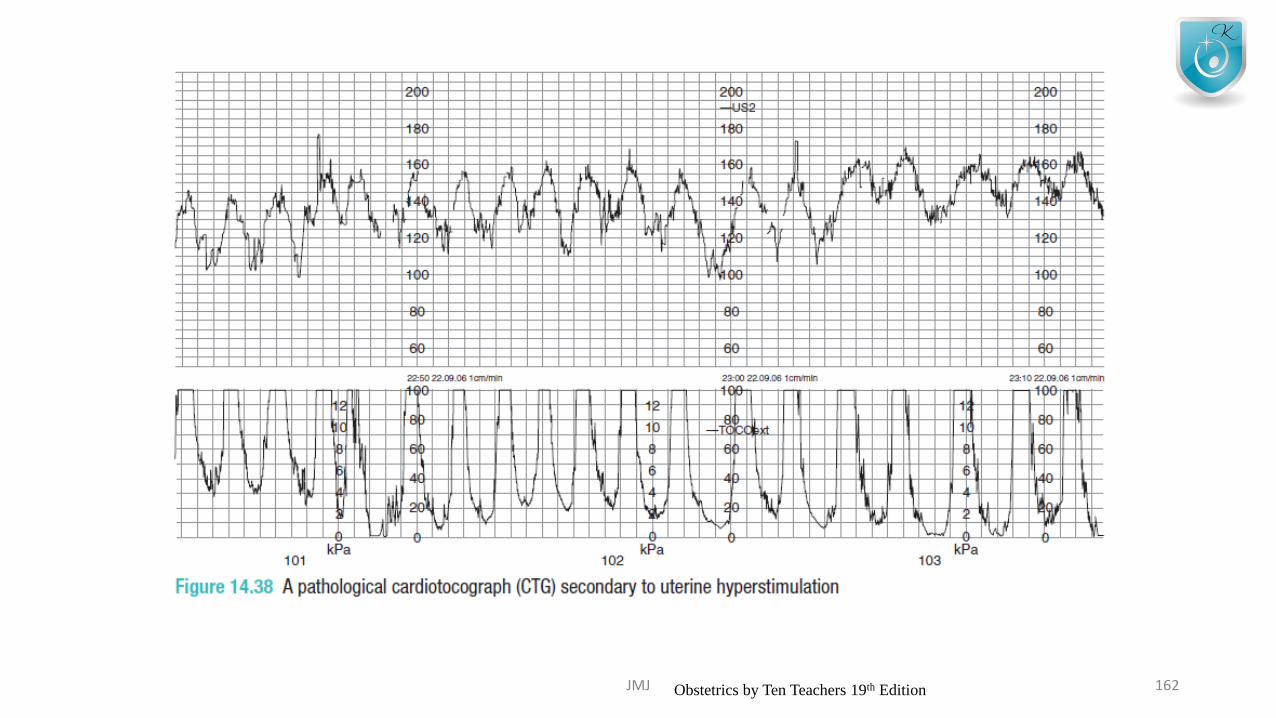
JMJ 162Obstetrics by Ten Teachers 19th Edition
Induction of labour and clinical risk management
• • Every induction of labour should have a valid indication.
• • The most common indication for induction of labour is prolonged pregnancy.
• • A high Bishop score predicts an easier induction of labour.
• • Clinical risk management aims to improve standards of intrapartum care and to reduce the number and severity of poor obstetric outcomes.
JMJ 163
THANK YOU!
JMJ 164