nospg is asked to: approve the recommendations … final 2 contents page executive summary 3...
TRANSCRIPT
NOSCAN Review Structure and Operating Framework
NoSPG is asked to:
• Approve the recommendations within the review
Aim
To describe the review process and subsequent recommendations
Purpose
48 stakeholders interviewed with emerging issues “themed” to develop recommendations. Key
themes of the report recommendations include:
• Increased clarity of purpose and function required, both in terms of roles within the
office and for the collaboration as a whole • Improved visibility of processes needed
• Data functions and capacity should be considered as a whole across the region
• Specialist skills required to support NOSCAN should be reviewed
• Urgent need for increased collaboration to sustain services across the NoS
Conclusion
NoSPG are asked to consider the detailed recommendations and agree that these
recommendations progress to an action planning stage.
NORTH OF SCOTLAND
PLANNING GROUP
Meeting: NoSPG
Date: 18th September 2013
Item: 42/13

V0.6 FINAL
1
NORTH OF SCOTLAND CANCER NETWORK (NOSCAN) A Review of the Structure and Operating Framework July 2013
version Author / Amendments date
V0.1 JC 18/07/13
V0.2 JC / PG 24/07/13
V0.3 JC / RC 21/08/03
V0.4 JC / PK 02/09/13
V0.5 JC / PK / PG 03/09/13
V0.6 FINAL JC / RCAF 09/09/13
NORTH OF SCOTLAND PLANNING GROUP
V0.6 FINAL
2
CONTENTS
Page
EXECUTIVE SUMMARY 3
INTRODUCTION
Summary of Recommendations 3
Background 4-6
MEHODOLOGY
Methods 7
Results 7-13
Discussion 13-14
CONCLUSIONS AND RECOMMENDATIONS
Detailed recommendations 14-15
Conclusion 15
APPENDIX I - Regional Workforce comparisons 16-20
APPENDIX II - NOSCAN Review Overview 21
APPENDIX III - List of Stakeholders 22-23
APPENDIX IV – Breakdown of NOSCAN and NoSPG staff 24
Acknowledgements
The author is grateful to interviewees for giving up significant amounts of time in order to
contribute.
In developing the questions and supporting the factual elements of the review the NOSCAN
Network Manager, Peter Gent, played a central role, as did the NOSCAN Clinical Lead, Peter King.
Other members of the regional planning team contributed hugely by arranging meetings and
“scribing”. This work was primarily carried out by Margaret Barton, Martha Hay and Ruth Nisbet.

V0.6 FINAL
3
Executive Summary
NOSCAN as a collaboration of the six North of Scotland (NoS) Boards has been in existence for
11 years. The NOSCAN structure has evolved as the landscape for cancer services across
Scotland has changed.
The Scottish Government play an increasingly active role in quality performance monitoring and,
to a large degree, direct regional network activities, by setting national strategic direction and
supporting initiatives in specific areas, which often have regional aspects.
Nationally, cancer is one of the Scottish Government’s priorities, with a current focus on “Detect
Cancer Early”, development of national Quality Performance Indicators and increased scrutiny of
treatment, intervention and follow up support.
In the North of Scotland there are, currently, a range of sustainability issues including workforce
and treatment services, which will require new and innovative solutions. Short term solutions to
workforce issues are required; however a longer term view of future cancer services in the north
is urgently needed.
It is evident from this review process that NoS Boards increasingly recognise the need to work
together more, and that there is overwhelming commitment for the aims* of the NOSCAN
collaboration, ensuring the focus is on the needs of patients. With some adjustments, to
structure and process, those aims have the support of the constituent Boards and the NOSCAN
office.
* To facilitate collaborative work, across the 3 NoS Cancer Centres, for the benefit of patients.
Summary of Recommendations
• Improve longer term collaborative planning, as a matter of urgency.
• Increase clarity of purpose, commitment and structure.
• Boards should specifically address the need for a clear internal structure which supports
the aims of NOSCAN.
• Consider current MCN structures at Board and regional levels.
• Consider opportunities to streamline financial arrangements.
• Regional coordination of data and research functions should be considered.
• Increase focus on continuous improvement cycles.
• Improve communication at all levels.

V0.6 FINAL
4
INTRODUCTION
Background
Three regional cancer networks were set up across Scotland following the launch of “Scotland
Against Cancer” (Scottish Executive Health Department 2001).
The three regional cancer networks serve different populations and configurations of cancer
services (see section “regional cancer networks”). In addition they are structured in different
ways with varying levels of staffing.
NOSCAN encompasses a range of primary care, diagnostic and interventional services, including
three specialist cancer centres, supporting work across a large geographical area, carrying
specific challenges associated with remote and rural cancer pathways.
Here we consider how NOSCAN, as a collaboration of cancer services in the north, functions;
assessing whether the network, including the regional office, is appropriately structured and
sufficiently resourced, to support Board, Regional and National priorities and those affected by
cancer, across the North of Scotland.
This review is concerned primarily with the structure and operating framework of the network
and is not concerned with aspects of service delivery or sustainability, which are the subject of
other focussed work (Operational review).
The review is sponsored by the chair of NOSCAN (Mr R Carey, CEO NHS Grampian) who, on
behalf of the Regional Cancer Advisory Forum (RCAF), commissioned The Director of Regional
Planning for the North of Scotland Planning Group (NoSPG) to carry out the review.
Regional Planning Group Alignment
The South East and Tayside regional cancer network (SCAN) is managed through the regional
planning group, with the network manager reporting directly to the Director of Regional Planning.
The West of Scotland regional cancer network (WOSCAN) reports through the regional planning
group but the network manager is not line managed by the Director of Regional Planning.
In the North of Scotland the regional cancer network reports through the North of Scotland
Planning Group and the network manager has been line managed through the acute sector

V0.6 FINAL
5
management structure in NHS Grampian. In the recent past, due to interim arrangements in
regional posts, line management of the NOSCAN manager has fallen to the interim Director of
Regional Planning and these arrangements now require clarification.
Regional Cancer Networks
Specific comparisons between each regional cancer network and the resources available to them
are detailed in Appendix 2. This comparison shows the variation in how each network resources
and manages the cancer agenda regionally, demonstrating the difficulty in assessing whether
NOSCAN is appropriately resourced or not. Each of the regional cancer network managers and
colleagues from SCT described the differences in scale and the complexities of the arrangements
across each of the three regions.
Whilst NOSCAN serves a population of 1.3m, SCAN in the south east serves circa 1.3, and
WOSCAN in the west serves 2.6.
The challenges faced by NOSCAN, which works across three cancer centres and six NHS Boards,
with circa 23% of the population of Scotland spread across half of the total land mass of
Scotland, should not be underestimated.
What is evident from these comparisons is that:
• Data management and line management arrangements are inconsistent – the other
regional cancer networks have this resource but NOSCAN does not.
• There is consistency around funding arrangements for regional MCN clinical leads in that
no clinical leads are funded in any of the regional MCN structures.
• WOSCAN host a number of national networks and initiatives – this makes comparison of
capacity and output difficult when set against the compounding factors of differences in
population and number of cancer centres.
• Funding for Regional Pharmacist posts is not consistent across the networks – Each
regional cancer network has a regional pharmacy post and these are managed and
resourced differently.

V0.6 FINAL
6
Funding Arrangements
NHS Grampian currently “hosts” NOSCAN in terms of financial management whilst NHS Tayside
play host to NoSPG financial arrangements. This may have the potential to cause ambiguity in
terms of the management of regional resources and currently relies on an excellent working
relationship between finance in NHS Grampian and NHS Tayside to run smoothly for certain
aspects.
Strategic aims of NOSCAN
NOSCAN's main objective on behalf of NoSPG (the North’s collaboration of Chief Executives and
Directors of Planning) is to promote equity of care and access to care by:
• negotiating with lead officers at SGHD and associated bodies to influence national policy;
• advocating cancer service improvement at Board and regional level;
• creating regional policies and securing adequate regional / local resources and investment to
implement them;
• planning at a regional level, those specialist cancer services appropriately provided at a level
beyond that of a single NHS Board, to the benefit of all patients across the North;
• identifying strategic gaps in services and leading national improvement projects on behalf of
NHS Scotland to rectify them;
• driving regional equitable improvements through NOSCAN wide MCN’s and sub-groups;
• creating long term regional cancer service improvement plans and directing local versions;
• delivering regional specific services and regional infrastructure;
• supporting implementation within the region at Board and service level;
• co-ordinating and integrating all cancer improvement effort in the North of Scotland;
• supporting redesign of cancer services to ensure they are delivered as efficiently as possible;
• ensuring collaboration across Scotland; and
• reporting on all of the above to NoSPG, its Boards, Scottish Cancer Taskforce and SGHD,
communicating these efforts and their outcomes to all members.
It is clear through the review process that the majority of these aims are being met. Some of
these aims have been explored further in the discussion section and specific areas have been
identified for future improvement.

V0.6 FINAL
7
Methodology
Information was gathered from the three regional cancer network managers, and collated to
allow comparisons between the resource and structure across the regions.
Thematic, qualitative information was gathered by interviewing stakeholders (Appendix 3) using
structured questions to guide discussion. Interviews were transcribed and collated in an
anonymous format.
48 people were interviewed across a list of stakeholders including executive leads, operational
service managers and clinicians, NOSCAN office staff, patient representative, tumour specific lead
clinicians and general managers (Appendix 3 – list of stakeholders interviewed).
Discussions were held with Scottish Government colleagues (Scottish Cancer Taskforce),
focussing on the strategic direction of cancer services in Scotland, before recommendations were
finalised.
Questions (Appendix 2) were developed collaboratively with the substantive - and interim -
NOSCAN Network Managers, Clinical Lead and colleagues from the other regional cancer
networks. Input was also received from Scottish Government colleagues who lead the Scottish
Cancer Taskforce (SCT).
Questions were designed to gain some insight into how NOSCAN is meeting the needs of
stakeholders from across the spectrum. They were also designed to provide an opportunity to
highlight where regional planning and working has worked well, so that success criteria could be
gauged and built upon in future work.
Questions gave interviewees the chance to provide specific suggestions for improvement and
these have been listed later in the results section.
Whilst every effort has been made to conduct interviews in an objective and standardised way,
the report author does not purport to have used a robust scientific methodology in developing
recommendations.

V0.6 FINAL
8
Interview Results
Collated interview outputs have been themed in the discussion section to support the formulation
of strategic recommendations, for consideration by the Regional Cancer Advisory Forum (RCAF).
Communication
The majority of respondents indicated that excellent communication was evident across the
network with relevant information being passed on timeously and available on the NOSCAN
website thereafter.
A significant number however indicated that there were obstacles in terms of communication
which ranged from too much information from the NOSCAN office (and no time to read it); to a
small number of respondents indicating that there was some work required around maintaining a
consistent and structured approach to communication between the NOSCAN office and
appropriate levels within Boards.
The majority of respondents indicated that they didn’t know the specifics of the NOSCAN work
plan or how it was prioritised, but in most cases felt there were appropriate mechanisms in place
to influence items on the work plan if the need arose. Generally there was a feeling that the work
plan was in the main dictated by national priorities and was in part disconnected from frontline
services.
A minority of those interviewed were concerned about a lack of inclusiveness when NOSCAN
office staff were involved with discussions at local level. On occasions discussions had taken place
with senior clinicians, with operational managers not always included appropriately.
“Links are better in local Boards when there are well functioning groups”
“A communication strategy was agreed for NOSCAN through local Boards and there are good distribution lists with a wide information sharing”
“Need some governance locally and a process to be set up”
“These are not fit for purpose”
“Engagement is highly important”
“The web site is excellent”

V0.6 FINAL
9
Structure
Respondents were generally comfortable that existing resources within the NOSCAN office was
adequate, although the majority commented that they were not sufficiently close to the day to
day running of the network office to comment in detail.
In discussion, around the team and their roles, most felt that there was fragility and unnecessary
fragmentation in data functions (audit, tracker and research teams) and a lack of regional
coordination. It was generally recognised that this fragmentation was as a result of differing
funding and line management arrangements for the various staff groups.
Board structures were reported as “patchy” in terms of meeting local needs and also the wider
needs of the network. Some reported robust local processes but the majority were either unclear
or indicated that local structures weren’t functioning well. Respondents reported varying levels of
engagement with these structures and cited this as a symptom of the lack of clarity or the
functionality of that structure.
Roles within the NOSCAN office were almost universally reported as being unclear with a number
of responses indicating that these roles had become blurred over the past 1-2 years. This lack of
clarity was around specific responsibilities of the NOSCAN office (lack of overall clarity of
purpose) but was also focussed on how combined roles between the NOSCAN office and NHS
Grampian had led to uncertainty as to when some members of staff were acting on behalf of NHS
Grampian and when they were acting on behalf of NOSCAN.
“There is a perception that loyalties exist within NOSCAN to Aberdeen”
“We have a strong network and it fits well with NOSCAN”
“When it falls down it’s because of communication at local level”
“Audit capacity is an issue across all Boards”
“We need fully functioning MCN’s which need support and we are light on this”
“WOSCAN and SCAN employ audit staff linked through the regional network. We do not have anyone with data management skills to pull the North’s
information together”
V0.6 FINAL
10
Board, Regional and National – tumour specific – MCN’s were raised by a number of respondents
as requiring some thought, perhaps rationalisation. In some areas Board MCN’s were thought to
duplicate Regional MCN activity and in others regional MCN activity was thought to be better
served by a national MCN. There was wide ranging support for the regional MCN manager role to
be focussed solely on MCN activities, to fully establish and maintain collaborative networking
opportunities across all tumour types. Respondents recognised that the MCN structure could be
improved by additional support.
There was broad recognition that national work streams would bear fruit in the fullness of time
and there was enthusiasm for the aspirations of the various national initiatives, however there
was uncertainty as to how managers and clinicians could be supported in a practical way to
engage fully with these initiatives, when there were such immediate and urgent needs around
delivering services on a day to day basis. Capacity and sustainability of frontline services being
foremost for the majority interviewed.
Few interviewees understood the relationship between NOSCAN and NoSPG and a very few
indicated that NOSCAN was on occasion viewed as a standalone entity.
Some referred to the perception of NOSCAN being “Grampian Centric” and factors alluded to
were the lead roles all being sourced from Grampian (Chair, Manager and Clinical Lead).
Most recognised that there was a clear structural role for NOSCAN and that role should be
focussed around sharing good practice, collating and presenting relevant data and facilitating
improvement work based on priorities set by the Boards and by national strategic direction (via
initiatives from SCT).

V0.6 FINAL
11
Improvement suggestions
A summary of suggestions for improvement is included below:
• Improve communication lines at all levels
o Clarify Board communication structures
o Summarise communications to Boards where possible
o Tailor visits to suit Boards
• Review internal NOSCAN office structure
o Ensure capacity is in the right areas
• Hold regular NOSCAN meetings to develop the Continuous Improvement role
• Increase operational engagement by increased attendance by NOSCAN manager at
operational meetings within Boards
These improvements were generally based on the areas reported elsewhere in the results
section, and therefore need no further exploration here.
“Availability of figures re workload would be good; also outcomes data not yet available via audit”
“We need more work on how quality priorities can be delivered within the given
workforce or discuss what extra help is required”
“Need to see more data and research”
“opportunity to look at the future rather than crises management”
“Don't think they involve the right people - the people at the 'coal face' need to be consulted about the practicalities of a service”
“The NoS needs to operate as a region, similar to the SEoS and the WoS,
despite having 3 centres”
“we have to have infrastructure”
V0.6 FINAL
12
Sustainability
A number of specific sustainability issues emerged with overriding short term concerns around
capacity (oncology workforce and radiotherapy most specifically) and concerns around the
medium term, recognising that the three oncology centres in the north might not be able to
continue to operate as separately in future. Competition for workforce in a small “pool” was
described by many as a specific hindrance to co-operative working.
It was recognised that some tumour specific pathways were already supported by the larger
cancer centres in the central belt, however there are potentially others who may require
innovative regional solutions and different levels of support, on a more sustainable long term
basis.
There was a high level of support for a short term piece of work to support immediate
sustainability issues and recognition that a project considering the longer term requirements of
cancer patients in the NoS is required. This would need to include Board, Regional, inter Regional
and National options. Many who were interviewed suggested that realistic sustainable service
models would support recruitment across the north and that recent short term crises had the
effect of making NoS posts being perceived as less attractive to prospective applicants.
“There is no resilience in the service - if it is one person down, then that is a big problem”
“3 issues - Workforce - transport – beds”
“Increasing numbers of patients, increasing numbers of therapies, more
specialisation necessary and difficulty in delivering best modern therapy to all patients”
“it is very much fire fighting and trouble shooting”
V0.6 FINAL
13
Regional Working Exemplars
Support for regional working was evident and provided a number of examples where respondents
could clearly describe how the work had come about and what the success factors were. These
include:
• Upper GI surgery
• Gynaecological surgery
• Cross boundary support for elements of pathways delivered in remote areas
On further questioning respondents cited a number of success factors for these pieces of work,
however credible and effective clinical leadership was - by far - the most commonly described
factor.
Financial arrangements
Some respondents felt that clearer alignment with NoSPG, financial management arrangements,
would improve clarity and standardisation around regional processes. The majority of
respondents did not comment specifically on financial aspects of NOSCAN
“Good example was RARARI project which established chemo on the islands”
“The gynae network is a good example of a service that works regionally”
“Upper GI cancer services review”
“NOSCAN excels at regional project work”
“Improvements could be made by ensuring clarity around specific monies, and how network colleagues can have input into their use and reported at RCAF on
how they are spent”

V0.6 FINAL
14
Discussion
In general stakeholders were very positive about the role of NOSCAN and although frontline
cancer services are currently under severe pressure there are clear opportunities to reduce that
pressure by working more collaboratively across the three cancer centres in the north.
A range of views were expressed throughout the interviewing process. The majority of these
were positive with a very few expressing frustration or difficulty in specific areas.
Board boundaries were sometimes cited as an obstacle to this collaborative approach by falsely
putting territorial priorities ahead of patient led priorities.
It is evident from the interviews that there is a desire to plan across the region acting more as
one regional service with support from the larger centres where appropriate. This planning
process needs to take cognisance of the co-dependencies between aspects of cancer pathways
and the location of delivery. Interviewees were mainly concerned with the care which would be
required around maintaining stability of surgical services in certain locations, by developing more
secure regional loci, potentially on a tumour specific basis.
There were a number of regional planning / working successes which demonstrated that, given
the right conditions and success factors, cross boundary arrangements can work extremely well.
There was recognition that improved non medical pathways in primary care, making more and
better use of community resources, could alleviate some of the pressures currently bearing down
on acute services.
V0.6 FINAL
15
Detailed Recommendations
• The 3 NoS cancer centres should collaborate on developing sustainable
pathways for the long term, on a shared risk basis.
There are clear opportunities within the north region, based on this approach, where some pathways will undoubtedly involve support from the larger cancer centres and
others require new ways of working across the three NoS centres. Supporting these
developments in a planned way will secure safe and robust patient care in the NoS in the
longer term.
• The strategic aims and the role / remit of NOSCAN should be clarified.
Ensuring that Boards and the NOSCAN office are clear about expected outputs from the
collaboration.
• Boards contributing to the NOSCAN collaboration should clarify internal lines
of communication. Working closely with the NOSCAN office boards should identify particular communication
needs and support, which will support smoother communication from clinical staff and
managers through to regional groups.
• Responsibilities & roles in the NOSCAN office should be clarified.
These roles should be clarified, and made explicit, in terms of supporting the aims of NOSCAN alone. This will address the perception that the function of some roles has
become “blurred” by directly and indirectly supporting operational delivery within individual Boards.
• The relationship between NOSCAN and NoSPG should be made more explicit.
Clear line management of roles, and devolved responsibilities should be detailed, including decision making and lines of reporting.
• NOSCAN financial management, at a high level, should be amalgamated with
NoSPG financial functions.
Increased standardisation of processes across regional functions will ensure financial
reporting to collaborating Boards is streamlined.
• The NOSCAN office should clarify processes for agreeing items on the regional
cancer work plan. This will ensure stakeholders are clear how the work plan is constructed and what
process is used to prioritise.
• Data and research functions across the region should be linked more
explicitly.
It is evident that data functions are fragmented and sometimes fragile across the region, and sometimes within Boards. A coordinated approach could potentially deliver better
value for money, increase flexibility and increase the clinical benefits from an ability to
describe in detail cancer pathways, across the region, on a reliable and standardised
basis.
V0.6 FINAL
16
• The NOSCAN office should develop an increased role around continuous
improvement (CI).
Services recognise the benefits of this type of activity and are keen to see NOSCAN
deliver on a broader CI agenda where they can build upon data collection cycles by
presenting data and facilitating learning.
• The NOSCAN office should facilitate improved collaboration between Boards,
the regional cancer advisory group and services.
Some support is required to promote a coordinated and transparent approach, to cancer
pathway development in the NoS. This should include appropriate escalation processes
within boards to ensure collaborative regional opportunities are not missed.
• Regional specialty resources should be reviewed in detail and considered as
part of a development plan to support current or future NOSCAN work. Although there are some mixed views, there is support for the role of regional
pharmacist. Consideration should be given to a substantive regional Pharmacist post
along with a review of other specialty skills and the ongoing need.
• NOSCAN should put in place a cyclical process to self appraise and review
processes. This should include review of lead role tenure / rotation and geographical distribution to
ensure engagement from all NoS cancer centres.
Conclusion
By keeping the patient at the centre of every planning decision, Board boundaries become less of
an obstacle and we can support sustainable pathways as close to home as possible, for the good
of patients in the north of Scotland.
This review process concludes with a series of recommendations which are presented to the
Regional Cancer Advisory Forum (RCAF) for discussion and agreement.
Implementation of these recommendations will require a series of actions, the majority of which
would be comparatively easy to achieve. Others, such as frontline service challenges will require
further extensive work but provide longer term stability and a streamlined approach to service
planning and delivery across the north.
Jim Cannon
Director Regional Planning
North of Scotland Planning Group

V0.6 FINAL
17
Appendix I
NOSCAN Review - 2013
Aims of the Review
• To describe the background to the development of NOSCAN.
• To describe current NOSCAN staffing structures and funding arrangements.
• To describe other regional cancer networks, staffing structures and arrangements.
• To assess how well current NOSCAN arrangements meet the needs of the cancer
agenda.
• To establish the likely future function of NOSCAN to best meet the cancer agenda.
• To describe how NOSCAN currently interacts with NoSPG.
• To make recommendations on future network arrangements and interactions with
NoSPG.
Purpose and General Approach
This review has been instigated by the Chair of NoSPG and the Chair of NOSCAN and should be
viewed as part of routine processes to ensure continuation of the most appropriate and effective
support to cancer services across the North of Scotland.
NOSCAN is a collaboration between NHS Boards in the North of Scotland, which exists to plan
and deliver sustainable services to the population of the North and is supported by a small team. This review seeks to assess how well the cancer agenda is being served by this collaboration,
both within Boards, across the region and nationally, but also within the network office itself.
The review will be conducted as a series of semi-structured interviews (Appendix I) with
stakeholders (Appendix II) either in person, by VC or by telephone.
Strategic Context
NOSCAN's main objective is to promote equity of care and access to care throughout the North of
Scotland by planning, at a regional level, those cancer services appropriately provided at a level
beyond that of a single NHS Board, to the benefit of all patients across the North of Scotland. In addition NOSCAN has a clear remit in areas beyond planning, for example around data collation
and reporting.
NOSCAN acts on behalf of NoSPG to improve cancer services. NoSPG has delegated authority,
through the Board Chief Executives of the collaborating NHS Boards, to act corporately to ensure
the provision of services for the population of the North of Scotland. NOSCAN is therefore
responsible for the regional planning of cancer services. This means that we must ensure that cancer services are configured to deliver the best possible care for the population of the North of
Scotland as a whole.

V0.6 FINAL
18
Scope and Accountability
As part of normal business within NoSPG, the review will be led by the Director of Regional Planning (Jim Cannon) with reference to a small review group consisting of external and internal
stakeholders. It is anticipated the review group may need to meet once or twice, however the
majority of input should be by email.
Timescales/Reporting
The review will be completed by June 2013 and will report to the NoS Regional Cancer Advisory
Forum (RCAF) and the North of Scotland Planning Group (NoSPG) thereafter.
Output
The final output of this review will contain:
• A description of the evolution of NOSCAN including a list of CEL’s which inform the work
plan.
• A clear description of the roles within the NOSCAN office:
o overview of responsibilities;
o lines of accountability;
o unfunded roles being carried out; and
o comparison with the other regional cancer network structures.
• A clear description of roles and responsibilities outwith the NOSCAN office, upon which
the work plan relies heavily:
o NHS Boards;
o Tumour specific – regional – MCN's; and
o Tumour specific – national – MCN’s.
• A description of funding arrangements including funding for roles and projects split by:
o central funding; and
o Board funding.
• A summary of stakeholders’ views on whether NOSCAN is achieving its strategic aims:
o from Board, regional (including inter-regional) and national perspectives.
• A summary of stakeholders’ views on future support required from NOSCAN.
• A clear description of how NOSCAN and NoSPG work together in terms of:
o Governance; o line management responsibility; and
o financial management.
• Options which will meet the strategic aims and Board requirements, where these are not
already being met, clearly identifying recommended options.

V0.6 FINAL
19
Resources
The Director of Regional Planning will spend time working on the structured interviews and write
up of the final output and will liaise closely with the NOSCAN manager and other NOSCAN staff as appropriate, to contribute to meetings with stakeholders and also to supporting detailed work
around the current arrangements.
Jim Cannon Director of Regional Planning
Attachments: Appendix I – Interview Structure/Questions
V0.6 FINAL
20
Appendix 1
Name: Title:
Tel No: Email:
Questions Comments
1.
How does your Board agree locally, the strategic cancer
priorities, requiring regional support/development? E.g. • Department level
• Sector / Divisional level
• Planning Department / Board level (such as
strategic cancer steering groups)
2.
How do you/your Board agree locally, the appropriate representation and participation in the established regional
structures e.g. Regional Cancer Advisory Group, NCAG, tumour specific MCN’s?
• Department level
• Sector / Divisional level
• Planning Department / Board level (such as
strategic cancer steering groups)
3.
What are the current structures and systems for communication, both locally and regionally for engaging
with regional cancer initiatives and are these fit for
purpose?
Yes / No
4.
How aware of the work that is being devolved nationally
(SCT) through the regions?
5.
What are the mechanisms to enable you/your Board to
engage/ influence the Regional Cancer Work plan?
V0.6 FINAL
21
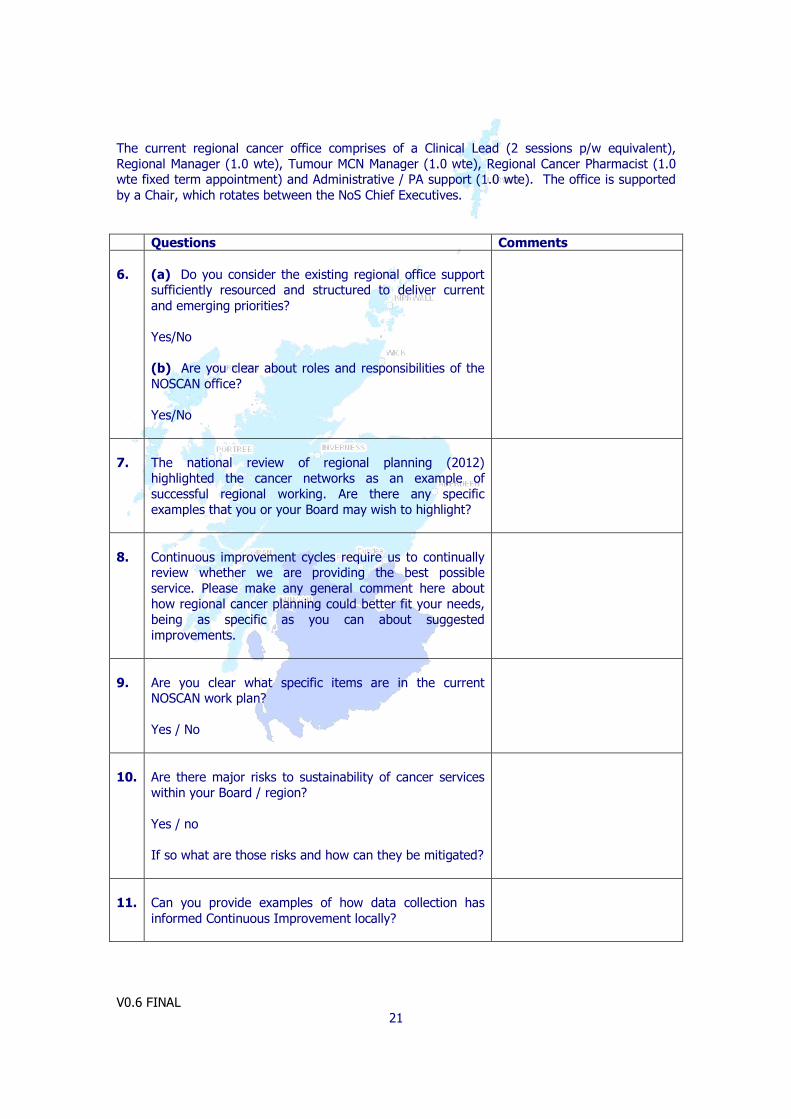
The current regional cancer office comprises of a Clinical Lead (2 sessions p/w equivalent),
Regional Manager (1.0 wte), Tumour MCN Manager (1.0 wte), Regional Cancer Pharmacist (1.0 wte fixed term appointment) and Administrative / PA support (1.0 wte). The office is supported
by a Chair, which rotates between the NoS Chief Executives.
Questions Comments
6.
(a) Do you consider the existing regional office support sufficiently resourced and structured to deliver current
and emerging priorities?
Yes/No
(b) Are you clear about roles and responsibilities of the
NOSCAN office?
Yes/No
7.
The national review of regional planning (2012)
highlighted the cancer networks as an example of
successful regional working. Are there any specific
examples that you or your Board may wish to highlight?
8.
Continuous improvement cycles require us to continually review whether we are providing the best possible
service. Please make any general comment here about
how regional cancer planning could better fit your needs,
being as specific as you can about suggested
improvements.
9.
Are you clear what specific items are in the current NOSCAN work plan?
Yes / No
10.
Are there major risks to sustainability of cancer services
within your Board / region?
Yes / no
If so what are those risks and how can they be mitigated?
11.
Can you provide examples of how data collection has
informed Continuous Improvement locally?

V0.6 FINAL
22
Appendix II Regional network comparisons
Core Regional Cancer Network Resources
NOSCAN Personnel / roles
Regional Clinical Lead (2 sessions per week)
Regional Manager (1.0 wte)
MCN Manager (1.0 wte)
Regional Cancer Pharmacist (Fixed term until June 2014) (1.0wte)
Tumour specific MCN leads x 7 (1-2 sessions per week)*
*unfunded from regional budget
PA / Administrative support (1.5 wte)
SCAN Personnel / roles
Regional Clinical Lead (2 sessions per week)
Regional Manager (1.0 wte)
MCN Manager (1.0 wte)
Modernisation Manager (1.0 wte)
Groups & Communications Co-ordinator (0.9 wte)
Information Systems Developer (0.6 wte)
Executive Assistant (1.0 wte)
Administrator (0.5 wte)
Cancer Audit Manager (1.0 wte)*
*funded by NHS Lothian,
managed by
Regional Manager
Tumour specific MCN leads x 9 (1-2 sessions per week)
WOSCAN Personnel / roles
Regional Clinical Lead (2 sessions per week)
Regional Manager (1.0 wte)
Network Service Manager (1.0 wte)
MCN Managers (2.8 wte)
Administrative support (2.0 wte)
Tumour specific MCN leads x 8 (1 session per week)*
National MCN Manager** (1.0 wte)
National MCN Administrator** (0.8 wte)
Project Managers (2.0 wte) National Quality Programme**
Administrative Support for Quality Programme (1.0 wte)**
*unfunded from regional budget
**funding to host support
national MCN / projects
NB: Regional Cancer Pharmacists substantively in position in both SCAN & WOSCAN and structurally aligned to Pharmacy services.

V0.6 FINAL
23
Appendix III
NOSCAN Review 2013 - Stakeholders
Peter King NOSCAN Lead Clinician NHS Grampian
Shelagh Bonner-Shand Interim NOSCAN Manager NOSCAN
Peter Gent NOSCAN Manager NOSCAN
Neil McLachlan NOSCAN MCN Manager NOSCAN
Mark Parsons Macmillan Regional Cancer Pharmacist NHS Grampian
Jane Tighe Cancer Centre Lead NHS Grampian
Marianne Nicolson NOSCAN MCN Lead, Lung NHS Grampian
Sami Shimi NOSCAN MCN Lead, Upper GI NHS Tayside
Dominic Culligan NOSCAN MCN Lead, Haematology NHS Grampian
To be appointed NOSCAN MCN Lead, Gynae NHS Grampian
Elizabeth Smyth NOSCAN MCN Lead, Breast NHS Grampian
Malcolm Loudon Board Clinical Lead and NOSCAN MCN Lead, Colorectal NHS Grampian
Satchi Swammi NOSCAN MCN Lead, Urology NHS Grampian
Lindsay Campbell National MCN, Hepatobiliary, Neuro-oncology & Sarcoma GG&C
Stephen Thomas Board Clinical Lead NHS Highland
Marthinus Roos Medical Director and Board Clinical Lead NHS Orkney
Gordon McFarlane Board Clinical Lead NHS Shetland
Alan Cook Interim Board Clinical Lead and Interim Cancer Centre Lead NHS Tayside
Gerte Plappert Board Clinical Lead NHS Western Isles
Lorraine Urquhart Local Cancer Services Representative/Manager NHS Grampian
Derick Macrae Local Cancer Services Representative/Manager NHS Highland
Simon Bokor-Ingram Local Cancer Services Representative/Manager NHS Shetland
Kerry Wilson Interim Local Cancer Services Representative/Manager NHS Tayside
Rachael Dunk Unit Head, Clinical Priorities Team SGHD
Evelyn Thomson Regional Manager WOSCAN
Kate McDonald Service Improvement Manager SCAN
Aileen Keel Deputy Chief Medical Officer SGHD
William Moore NoSPHN representative
V0.6 FINAL
24
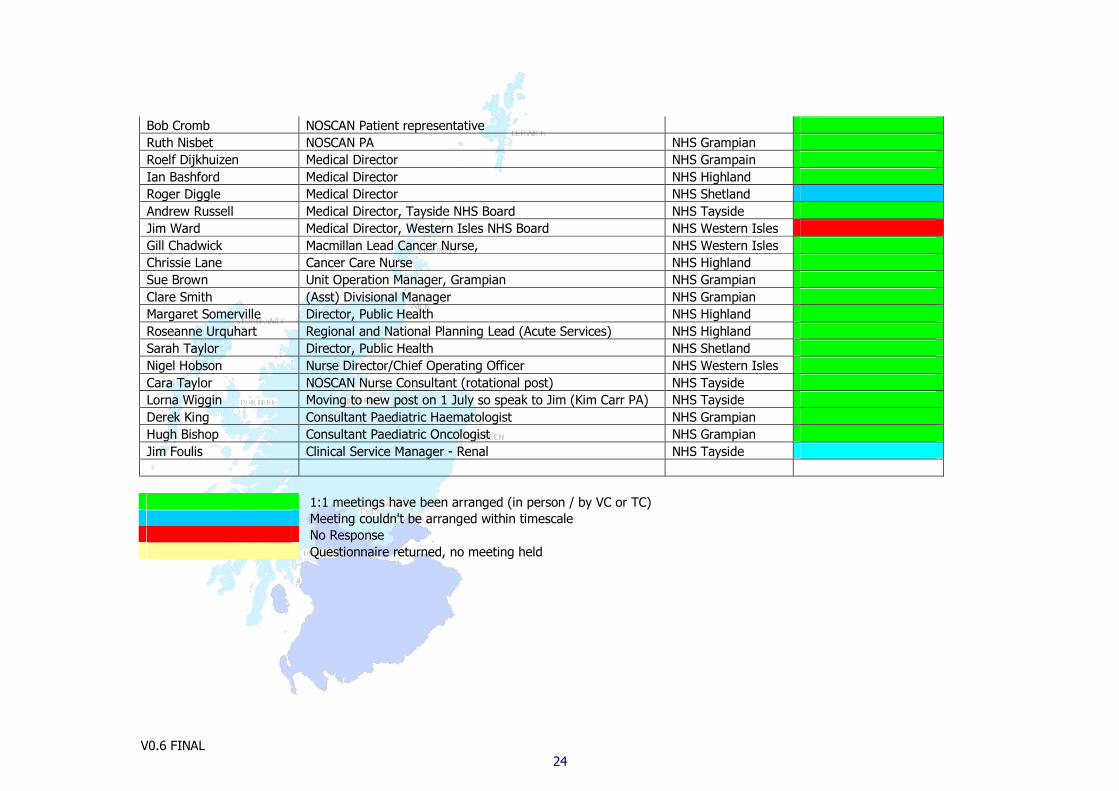
Bob Cromb NOSCAN Patient representative
Ruth Nisbet NOSCAN PA NHS Grampian
Roelf Dijkhuizen Medical Director NHS Grampain
Ian Bashford Medical Director NHS Highland
Roger Diggle Medical Director NHS Shetland
Andrew Russell Medical Director, Tayside NHS Board NHS Tayside
Jim Ward Medical Director, Western Isles NHS Board NHS Western Isles
Gill Chadwick Macmillan Lead Cancer Nurse, NHS Western Isles
Chrissie Lane Cancer Care Nurse NHS Highland
Sue Brown Unit Operation Manager, Grampian NHS Grampian
Clare Smith (Asst) Divisional Manager NHS Grampian
Margaret Somerville Director, Public Health NHS Highland
Roseanne Urquhart Regional and National Planning Lead (Acute Services) NHS Highland
Sarah Taylor Director, Public Health NHS Shetland
Nigel Hobson Nurse Director/Chief Operating Officer NHS Western Isles
Cara Taylor NOSCAN Nurse Consultant (rotational post) NHS Tayside
Lorna Wiggin Moving to new post on 1 July so speak to Jim (Kim Carr PA) NHS Tayside
Derek King Consultant Paediatric Haematologist NHS Grampian
Hugh Bishop Consultant Paediatric Oncologist NHS Grampian
Jim Foulis Clinical Service Manager - Renal NHS Tayside
1:1 meetings have been arranged (in person / by VC or TC)
Meeting couldn't be arranged within timescale
No Response
Questionnaire returned, no meeting held

V0.6 FINAL
25
Appendix IV
NOSCAN Regional Office (September 2013)
Clinical Lead 2 sessions p/w equivalent
Regional Manager 1 whole time equivalent
Tumour MCN Manager 1 whole time equivalent
Regional Cancer Pharmacist 1 whole time equivalent (fixed term appointment)
Administrative/PA support 1 whole time equivalent
NoSPG Regional Team (September 2013)
Director of Regional Planning 1 whole time equivalent
Programme Manager 1 whole time equivalent
MCN Managers (Child Health) 2.6 whole time equivalent
Project Manager (Dental, Cardiac, Workforce) 1.0 whole time equivalent
Executive Assistant 1 whole time equivalent
PA/Administrator 1 whole time equivalent