novel direct acting antivirals against...
TRANSCRIPT

Novel Direct Acting Antivirals against HCV
2nd Asian Conference on Hepatitis and HIV, Beijing, China
Jürgen Rockstroh, Department of Medicine I,
University of Bonn, Germany

Predictors of Mortality Among US HCV Infected Veterans
195,585 HCV Patients 202,739 HCV Negative Veterans
All cause mortality 43.9 per 1000
person-years
HCV Positive
All cause mortality 24 per 1000
person-years
Erqou S, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 453.
HCV Negative
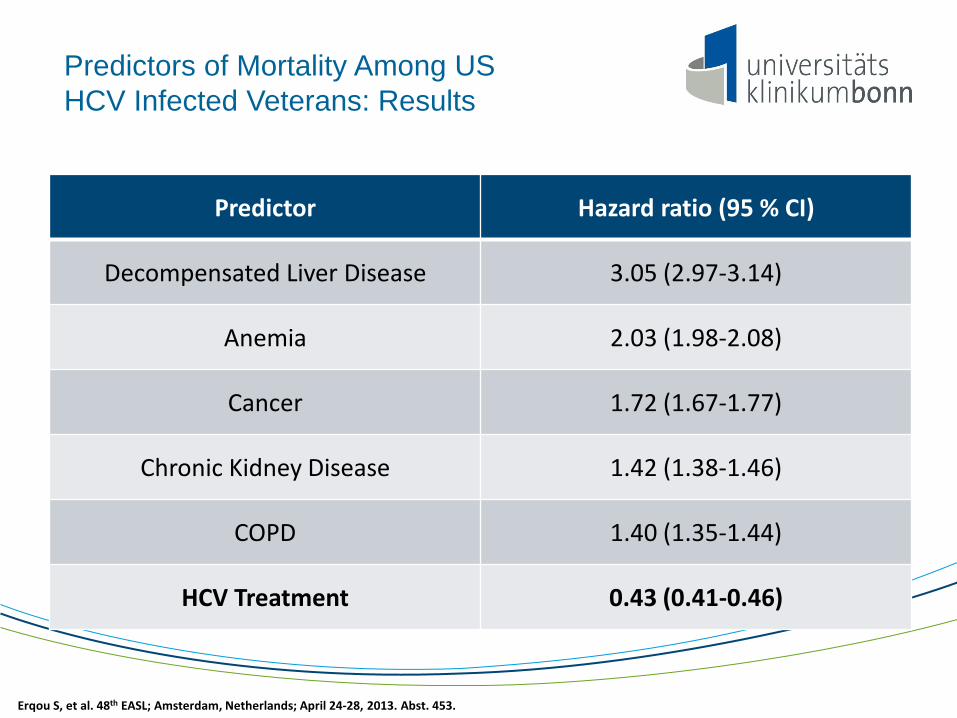
Predictors of Mortality Among US HCV Infected Veterans: Results
Predictor Hazard ratio (95 % CI)
Decompensated Liver Disease 3.05 (2.97-3.14)
Anemia 2.03 (1.98-2.08)
Cancer 1.72 (1.67-1.77)
Chronic Kidney Disease 1.42 (1.38-1.46)
COPD 1.40 (1.35-1.44)
HCV Treatment 0.43 (0.41-0.46)
Erqou S, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 453.

Treatment of HCV disease is evolving
Patients achieving SVR (%)
100
80
60
40
20
0 24 48 78 Peg-IFN IFN +
ribavirin Peg-IFN + ribavirin Weeks
IFN monotherapy
All genotypes Genotype 1 Genotypes 2 or 3
6-19 11-19 10-22
18-39 35-43
61-79
33-36
76-82
42-46
*Range of values reported; lower bar represents lower value;
Manns MP, Foster GR, Rockstroh JK, et al: Nature Reviews Drug Discovery, 2008

Why do we need new treatments ?
• Improvement of SVR
• Reduction of adverse effects
• Reduction of treatment duration
• Reduction of cost
• Non-Responders to PEG-IFN plus Ribavirin
• Difficult to treat populations
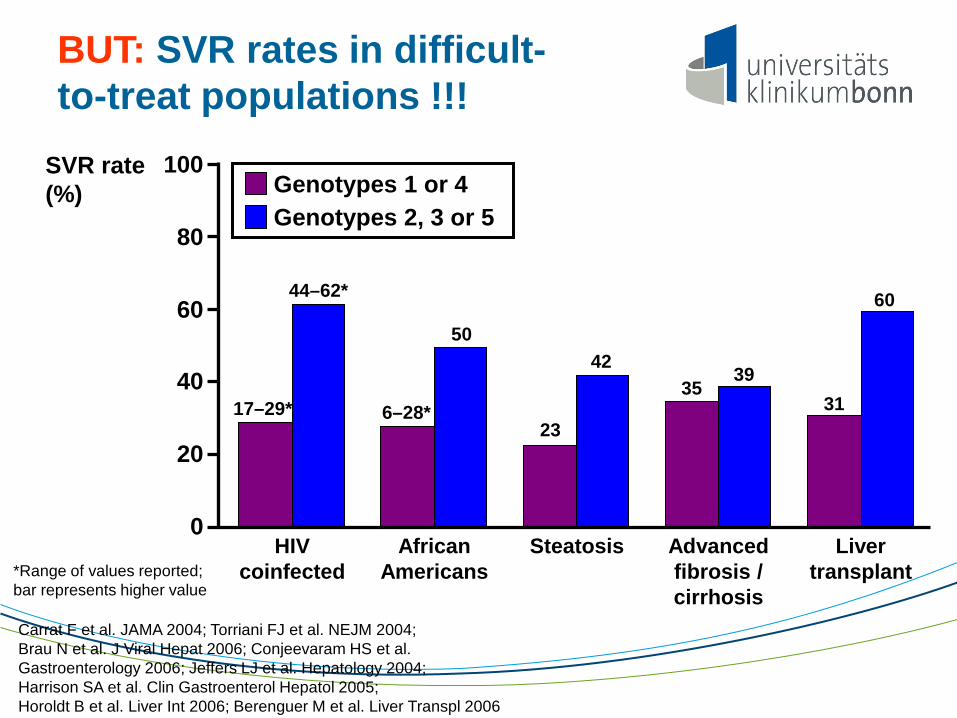
BUT: SVR rates in difficult-to-treat populations !!!
*Range of values reported; bar represents higher value Carrat F et al. JAMA 2004; Torriani FJ et al. NEJM 2004; Brau N et al. J Viral Hepat 2006; Conjeevaram HS et al. Gastroenterology 2006; Jeffers LJ et al. Hepatology 2004; Harrison SA et al. Clin Gastroenterol Hepatol 2005; Horoldt B et al. Liver Int 2006; Berenguer M et al. Liver Transpl 2006
SVR rate (%)
Advanced fibrosis / cirrhosis
HIV coinfected
African Americans
Steatosis Liver transplant
17–29* 6–28*
44–62*
50
23
42 35
39 31
60
0
20
40
60
80
100 Genotypes 1 or 4 Genotypes 2, 3 or 5
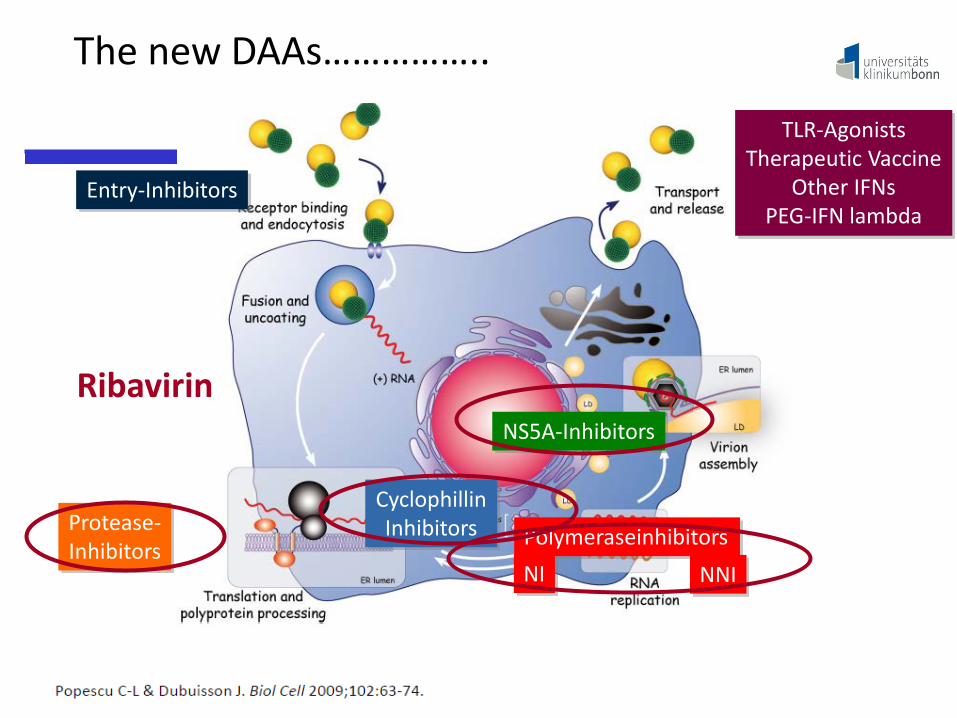
The new DAAs……………..
Protease- Inhibitors Polymeraseinhibitors
NI NNI
NS5A-Inhibitors
TLR-Agonists Therapeutic Vaccine
Other IFNs PEG-IFN lambda
Entry-Inhibitors
Cyclophillin Inhibitors
Ribavirin

HCV Protease inhibitors
»Telaprevir (licensed in US and Europe) »Boceprevir (licensed in US and Europe) »TMC 435350 (Simeprevir) (phase III) »BI 201335 (Feldaprevir) (phase III)
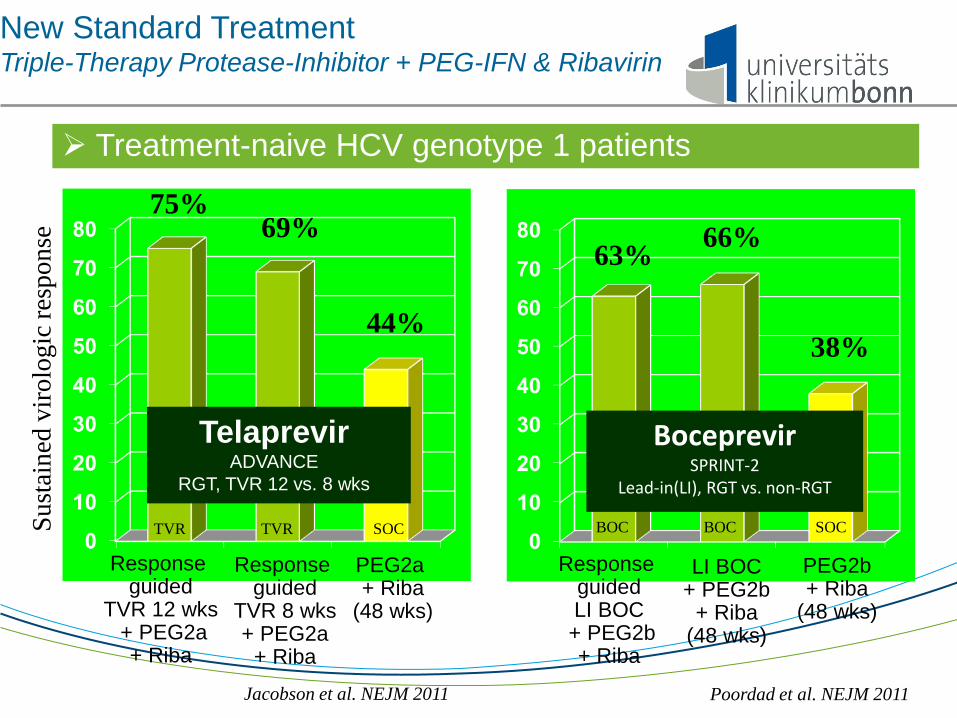
New Standard Treatment Triple-Therapy Protease-Inhibitor + PEG-IFN & Ribavirin
Jacobson et al. NEJM 2011
Sust
aine
d vi
rolo
gic
resp
onse
Response guided
TVR 12 wks + PEG2a
+ Riba
75% 69%
44%
PEG2a + Riba
(48 wks)
Response guided
TVR 8 wks + PEG2a
+ Riba
Poordad et al. NEJM 2011
Response guided LI BOC
+ PEG2b + Riba
63% 66%
38%
PEG2b + Riba
(48 wks)
LI BOC + PEG2b
+ Riba (48 wks)
TVR TVR SOC BOC BOC SOC
Telaprevir ADVANCE
RGT, TVR 12 vs. 8 wks
Boceprevir SPRINT-2
Lead-in(LI), RGT vs. non-RGT
Treatment-naive HCV genotype 1 patients

New Standard Treatment Triple-Therapy Protease-Inhibitor + PEG-IFN & Ribavirin
0
20
40
60
80
100
Sust
aine
d vi
rolo
gic
resp
onse
15% 24%
REL
57%
31%
86%
TVR SOC
5%
P-NR NULL
Relapser (REL): negative at end-of-treatment but relapse thereafter Partial Non-Responder (P-NR): ≥2log wk12 but pos HCV RNA wk 24 Null-Responder (NULL): <2log wk 12
TVR SOC TVR SOC 0
20
40
60
80
100
7%
29%
REL
BOC SOC
P-NR NULL
BOC SOC
75%
52%
Bacon et al., NEJM 2011 *PROVIDE study, Vierling et al., AASLD 2011 Zeuzem et al., NEJM 2011
36%*
Treatment-experienced HCV genotype 1 patients
Telaprevir REALIZE
+/- Lead-in TVR 12 + PEG2a + Riba, 48 weeks
Boceprevir REPOND-2/PROVIDE
Lead-in (+/-RGT) BOC + PEG2b + Riba, 36/48 weeks

OPTIMIZE Study: Efficacy of TVR Dosed BID (1125mg) vs. q8h (750mg)
Buti M, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 798.
q8h
bid
CC and F0-F2
CC and F3-F4
Non-CC and F0-F2
Non-CC and F3-F4
N 79 75 29 28 183 192 79 74
SVR
12 (P
erce
ntag
e)

CUPIC: Virological response (ITT)
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
TELAPREVIR BOCEPREVIR
0
10
20
30
40
50
60
70
80
90
100
49%
Patie
nts
with
und
etec
tabl
e H
CV
RN
A (P
erce
ntag
e)
79% 81%
56%
W4 W8 W12 W24 W48 W60 W16
77 % 68 %
146 295
234 295
239 295
227 295
200 295
165 295
118 295
0
10
20
30
40
50
60
70
80
90
100
16%
51%
62% 65% 67%
W4 W8 W12 W16 W24 W48 W60
31 190
97 190
118 190
124 190
128 190
108 190
57%
79 190
40% 41%

CUPIC: SVR12 According to Prior Treatment Response
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
61/116 43/135 8/28
Relapsers
Partial responders
Null responders
53%
32% 29%
P=0.004
P=0.001
P=0.03
TELAPREVIR TELAPREVIR
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100
31 190
43/85 32/80 1/9
P=0.003
51%
40%
11%
BOCEPREVIR
Relapsers
Partial responders
Null responders

CUPIC: SVR12 Safety Findings Patients, n (% patients with at least one event) Telaprevir n=295 Boceprevir n=190
Serious adverse events (SAEs)* 535 in 160 patients (54.2%)
321 in 97 patients (51.0%)
Premature discontinuation / due to SAEs
139 (47.1%) / 63 (21.3%)
80 (42.1%)/ 27 (14.2%)
Death 7 (2.4 %) 3 (1.6%)
Infection (Grade 3/4) 27 (9.1 %) 8 (4.2%)
Hepatic decompensation (Grade ¾ ) 15 (5.1 %) 9 (4.7%)
Anemia (Grade ¾ : Hb < 8 g/dL) 38 (12.9 %) 19 (10%)
Rash (grade 3/SCAR) 16 (5.4 %)/ 2 (0.6 %) 2 (1.0%)/
EPO use / blood transfusion
168 (57 %) / 53 (18 %)
119 (62.6%) / 26 (13.7%)
GCSF use 8 (2.7 %) 13 (6.8%)
TPO use 6 (2 %) 3 (1.6%)
Fontaine H, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 60
SAEs in patients SCAR: severe cutaneous adverse reaction
Introduction to Faldaprevir
»Faldaprevir (FDV; BI 201335) is a potent and selective inhibitor of HCV NS3/4A1
»FDV has antiviral activity against HCV genotypes (GT) 1, 2, 4, 5 and 6 in vitro1
»The pharmacokinetics of FDV allow oral, once-daily administration
» In Phase II FDV + pegylated interferon α2a and ribavirin (PegIFN/RBV) demonstrated: Significantly higher sustained virological response (SVR) versus placebo2
Favourable safety and tolerability profile versus placebo2
»Three Phase III trials of FDV + PegIFN/RBV in HCV GT-1 are complete A further Phase III trial of FDV + PegIFN/RBV in HIV co-infection is ongoing FDV is also being investigated in Phase III interferon-free trials
HCV, hepatitis C virus 1. White PW, et al. Antimicrob Agents Chemother 2010;54:4611–4618; 2. Sulkowski et al Hepatology 2013 Jan 28 (epub)

STARTVerso1: Treatment-naïve patients
• Patients enrolled from Europe and Japan • Eligibility: Treatment naive, GT1 infection, no HBV or HIV coinfection, adult, platelets
>90,000 cells/mm3 • Criteria for response guided therapy
– Early Treatment Success (ETS): HCV RNA <25 IU/mL at Week 4 and undetectable at Week 81 – Patients with ETS in active treatment arms were eligible to stop all treatment at Week 24
• Primary endpoint: SVR 12 weeks after completion of all treatment
PegIFN/RBV Placebo + PR Observation Period
Day 1 Week 12 Week 24 Week 48 Week 72
Faldaprevir 240 mg QD + PR
Observation Period
Placebo + PR
PegIFN/RBV Observation Period
ETS
No ETS
Arm 2 (n=261)
Arm 3
(n=262)
Arm 1
(n=133)
Observation Period
Faldaprevir 120 mg QD + PR
PegIFN/RBV Observation Period
ETS
No ETS Faldaprevir 120 mg QD + PR
Placebo + PR
Ferenci P, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1416. 1 Roche COBAS® Taqman HCV/HPS assay
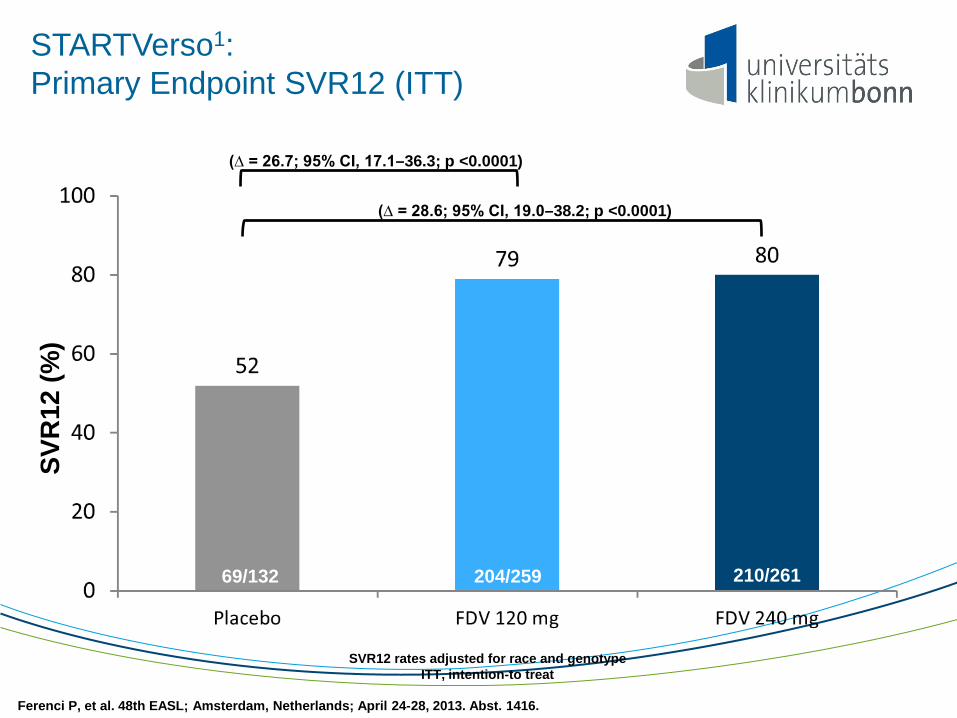
STARTVerso1: Primary Endpoint SVR12 (ITT)
(∆ = 28.6; 95% CI, 19.0–38.2; p <0.0001)
(∆ = 26.7; 95% CI, 17.1–36.3; p <0.0001)
SVR12 rates adjusted for race and genotype ITT, intention-to treat
204/259 210/261 69/132
SVR
12 (%
)
Ferenci P, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1416.
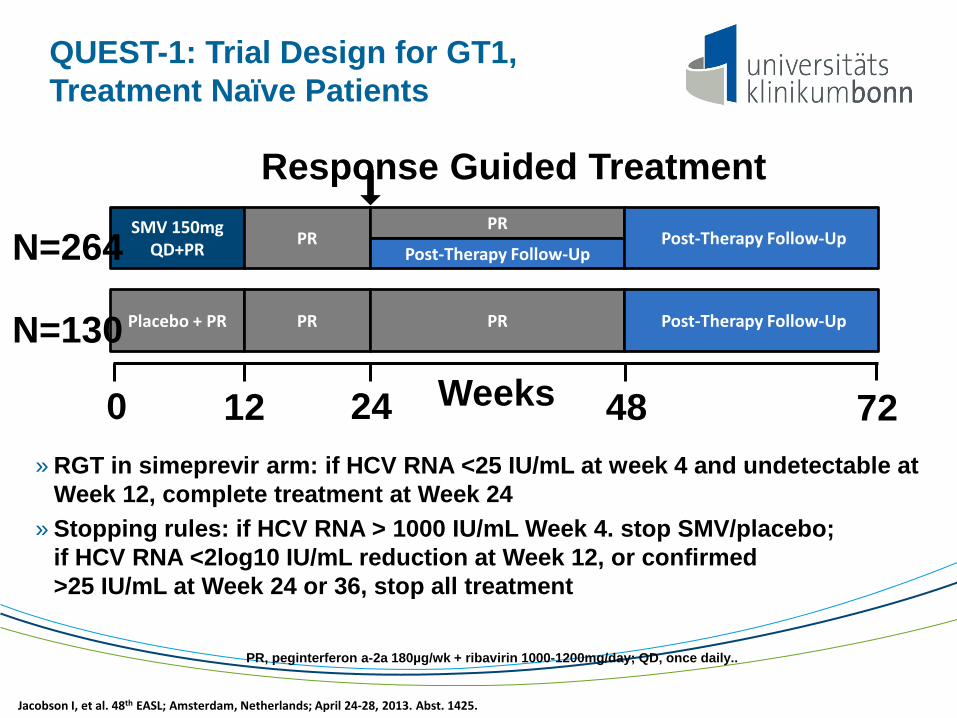
QUEST-1: Trial Design for GT1, Treatment Naïve Patients
» RGT in simeprevir arm: if HCV RNA <25 IU/mL at week 4 and undetectable at Week 12, complete treatment at Week 24
» Stopping rules: if HCV RNA > 1000 IU/mL Week 4. stop SMV/placebo; if HCV RNA <2log10 IU/mL reduction at Week 12, or confirmed >25 IU/mL at Week 24 or 36, stop all treatment
PR, peginterferon a-2a 180µg/wk + ribavirin 1000-1200mg/day; QD, once daily..
SMV 150mg QD+PR PR
PR
Post-Therapy Follow-Up Post-Therapy Follow-Up
Response Guided Treatment
N=264
Placebo + PR PR PR Post-Therapy Follow-Up N=130
0 12 24 48 72 Weeks
Jacobson I, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1425.
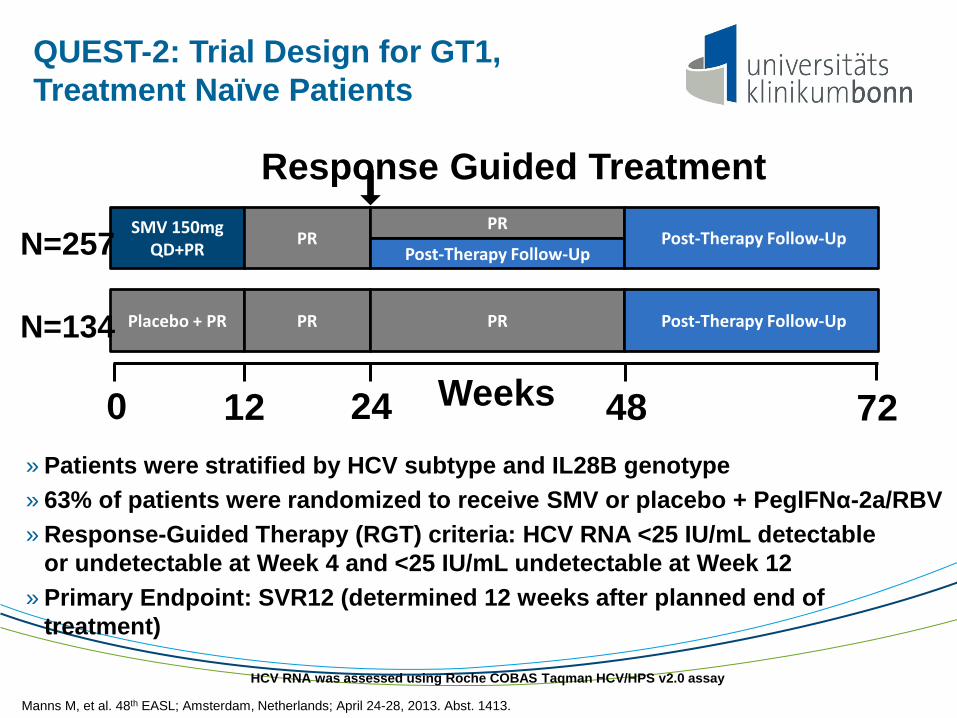
QUEST-2: Trial Design for GT1, Treatment Naïve Patients
» Patients were stratified by HCV subtype and IL28B genotype » 63% of patients were randomized to receive SMV or placebo + PeglFNα-2a/RBV » Response-Guided Therapy (RGT) criteria: HCV RNA <25 IU/mL detectable
or undetectable at Week 4 and <25 IU/mL undetectable at Week 12 » Primary Endpoint: SVR12 (determined 12 weeks after planned end of
treatment)
HCV RNA was assessed using Roche COBAS Taqman HCV/HPS v2.0 assay
SMV 150mg QD+PR PR
PR
Post-Therapy Follow-Up Post-Therapy Follow-Up
Response Guided Treatment
N=257
Placebo + PR PR PR Post-Therapy Follow-Up N=134
0 12 24 48 72 Weeks
Manns M, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1413.
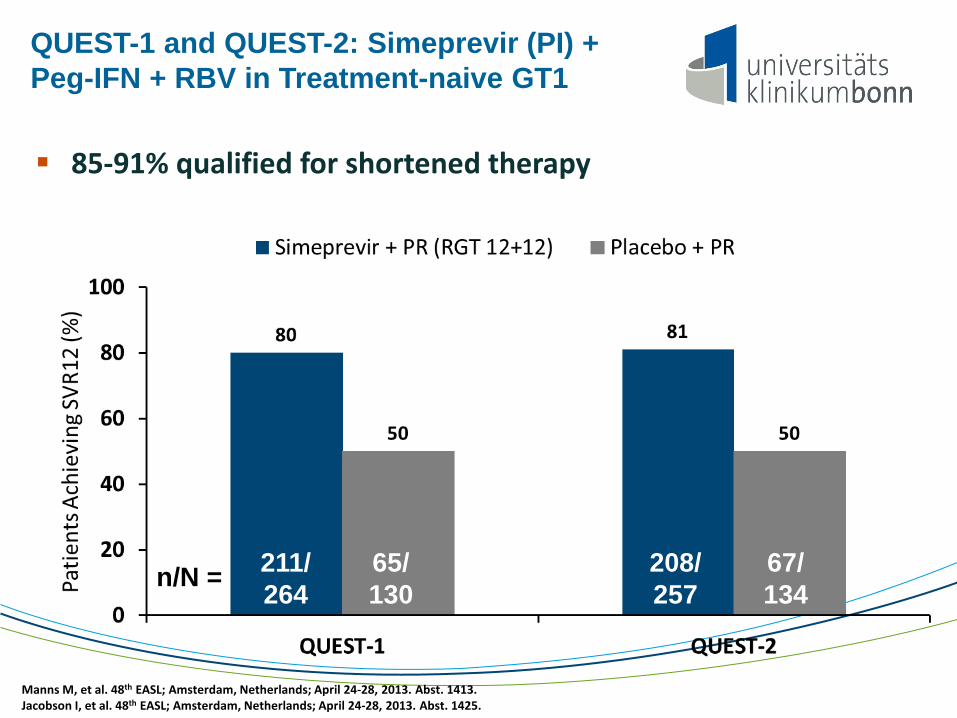
QUEST-1 and QUEST-2: Simeprevir (PI) + Peg-IFN + RBV in Treatment-naive GT1
n/N = 211/ 264
208/ 257
67/ 134
65/ 130
85-91% qualified for shortened therapy
Manns M, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1413. Jacobson I, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1425.

»Toxicity: Rash, Pruritis, Anaemia
»Resistence
»Pharmacokinetic profile
»Compliance
»Cost
»Benefit for non-responders ???
LIMITATIONS OF HCV PIs
Polymerase Inhibitors
• Nucleoside analogues
– Require conversion to active triphosphate form – Cause chain termination
• Non-nucleosides – Active at noncatalytic sites – Do not require triphosphate conversion

NEUTRINO Study: Design
»Open label SOF 400 mg QD + Peg-IFN-alfa-2a 180 µg/week + RBV 1000‒1200 mg/day for 12 weeks (no response-guided therapy)
»Treatment-naïve, genotype 1, 4, 5, and 6 HCV-infected patients Targeted 20% enrollment of patients with cirrhosis
»Expanded inclusion criteria No upper limit to age or BMI Opiate replacement therapy permitted Platelets ≥90,000/mm3, neutrophils ≥1500/mm3 or 1000/mm3 (blacks)
SVR12 SOF + Peg-IFN + RBV, n=327
Week 0 12 24
Lawitz E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1411.
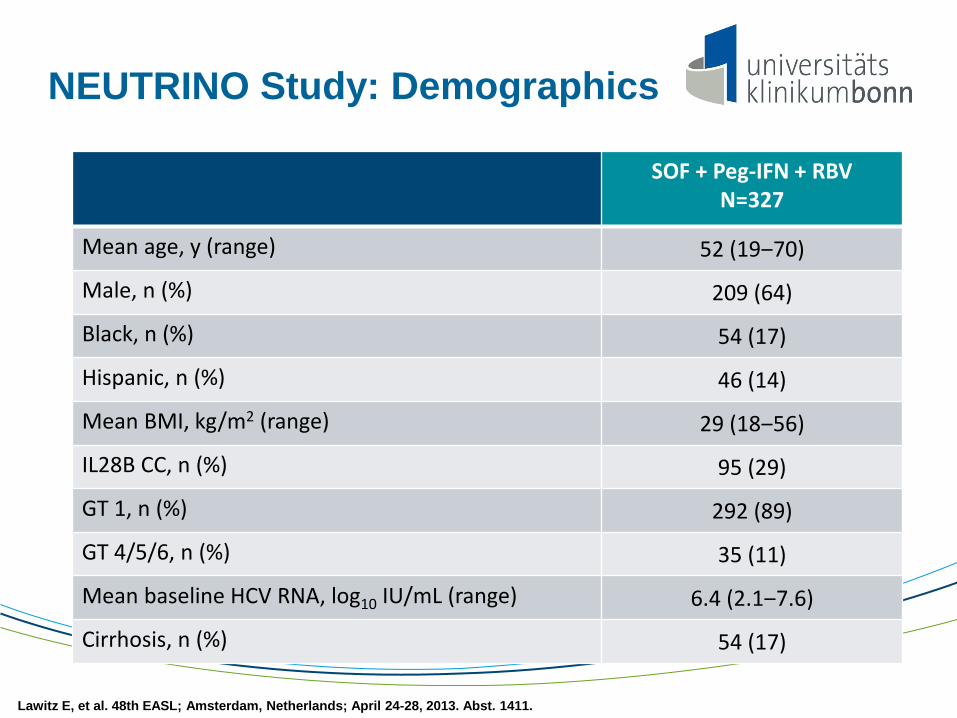
NEUTRINO Study: Demographics
SOF + Peg-IFN + RBV N=327
Mean age, y (range) 52 (19‒70)
Male, n (%) 209 (64)
Black, n (%) 54 (17)
Hispanic, n (%) 46 (14)
Mean BMI, kg/m2 (range) 29 (18‒56)
IL28B CC, n (%) 95 (29)
GT 1, n (%) 292 (89)
GT 4/5/6, n (%) 35 (11)
Mean baseline HCV RNA, log10 IU/mL (range) 6.4 (2.1‒7.6)
Cirrhosis, n (%) 54 (17)
Lawitz E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1411.

NEUTRINO Study: SVR12 by HCV Genotype
Patie
nts
with
HC
V R
NA
<LLO
Q
(%)
Overall GT 1 GT 4
Error bars represent 95% confidence intervals.
GT 5,6
295/327 261/292 27/28 7/7
Lawitz E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1411.

NEUTRINO Study: Virologic Response by Cirrhosis Status
Post-treatment On treatment
Patie
nts
with
HC
V R
NA
<LLO
Q (%
)
50/54 52/54 53/53
Week 2 Week 4 Week 12 Week 12
43/54 249/273 269/271 267/267 252/273
Error bars represent 95% confidence intervals.
Lawitz E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1411.

Week 0 12 24 36
FISSION Study: Treatment Naïve, Genotype 2 or 3 Patients
SOF + RBV n=256
Peg-IFN + RBV n=243
Mean age, y (range) 48 (20‒72) 48 (19‒77)
Male, n (%) 171 (67) 156 (64)
White, n (%) 223 (87) 212 (87)
IL28B CC, n (%) 108 (43) 106 (44)
GT 3, n (%) 183 (72) 176 (72)
Mean HCV RNA, log10 IU/mL (range) 6.0 (3.2‒8.3) 6.0 (3.2‒7.6)
Cirrhosis, n (%) 50 (20) 50 (21)
SOF + RBV*, n=256 SVR12
Peg-IFN + RBV* (SOC), n=243 SVR12
*RBV dose 1000-1200 mg/day for SOF + RBV and 800 mg/day for Peg-IFN + RBV
Gane E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 5.

98 82
91
62
61 71
34 30
0
20
40
60
80
100
SOF + RBV Peg-IFN + RBV
GT 2 GT 3
SVR
12 (P
erce
ntag
e)
No cirrhosis No cirrhosis Cirrhosis Cirrhosis
FISSION: SVR12 by Genotype and Cirrhosis
58/59 44/54 10/11 8/13 89/145 99/139 13/38 11/37
Gane E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 5.
Error bars represent 95% confidence intervals.
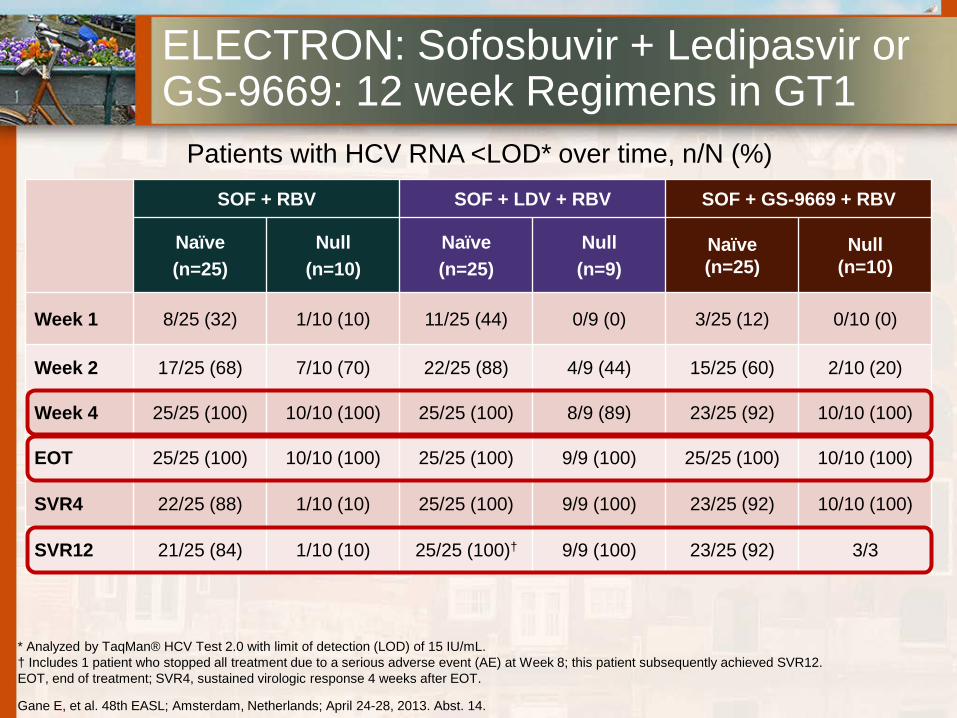
ELECTRON: Sofosbuvir + Ledipasvir or GS-9669: 12 week Regimens in GT1
SOF + RBV SOF + LDV + RBV SOF + GS-9669 + RBV
Naïve (n=25)
Null (n=10)
Naïve (n=25)
Null (n=9)
Naïve (n=25)
Null (n=10)
Week 1 8/25 (32) 1/10 (10) 11/25 (44) 0/9 (0) 3/25 (12) 0/10 (0)
Week 2 17/25 (68) 7/10 (70) 22/25 (88) 4/9 (44) 15/25 (60) 2/10 (20)
Week 4 25/25 (100) 10/10 (100) 25/25 (100) 8/9 (89) 23/25 (92) 10/10 (100)
EOT 25/25 (100) 10/10 (100) 25/25 (100) 9/9 (100) 25/25 (100) 10/10 (100)
SVR4 22/25 (88) 1/10 (10) 25/25 (100) 9/9 (100) 23/25 (92) 10/10 (100)
SVR12 21/25 (84) 1/10 (10) 25/25 (100)† 9/9 (100) 23/25 (92) 3/3
Patients with HCV RNA <LOD* over time, n/N (%)
Gane E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 14.
* Analyzed by TaqMan® HCV Test 2.0 with limit of detection (LOD) of 15 IU/mL. † Includes 1 patient who stopped all treatment due to a serious adverse event (AE) at Week 8; this patient subsequently achieved SVR12. EOT, end of treatment; SVR4, sustained virologic response 4 weeks after EOT.
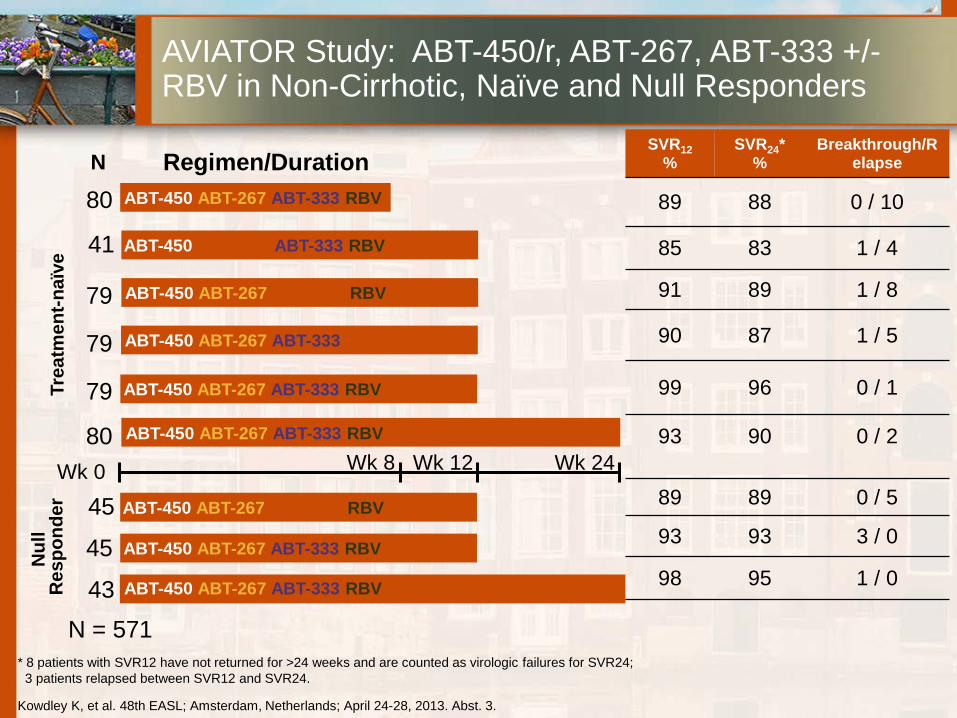
* 8 patients with SVR12 have not returned for >24 weeks and are counted as virologic failures for SVR24; 3 patients relapsed between SVR12 and SVR24.
Trea
tmen
t-naï
ve ABT-450 ABT-333 RBV
ABT-450 ABT-267 ABT-333 RBV
ABT-450 ABT-267 ABT-333 RBV
ABT-450 ABT-267 ABT-333
ABT-450 ABT-267 RBV
N ABT-450 ABT-267 ABT-333 RBV
Wk 0 Wk 8 Wk 12 Wk 24
80
79
79
79
80
41
Regimen/Duration
Nul
l R
espo
nder
ABT-450 ABT-267 RBV
ABT-450 ABT-267 ABT-333 RBV
45
45
43 ABT-450 ABT-267 ABT-333 RBV
SVR12 %
SVR24* %
Breakthrough/Relapse
89 88 0 / 10
85 83 1 / 4
91 89 1 / 8
90 87 1 / 5
99 96 0 / 1
93 90 0 / 2
89 89 0 / 5
93 93 3 / 0
98 95 1 / 0
AVIATOR Study: ABT-450/r, ABT-267, ABT-333 +/- RBV in Non-Cirrhotic, Naïve and Null Responders
Kowdley K, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 3.
N = 571
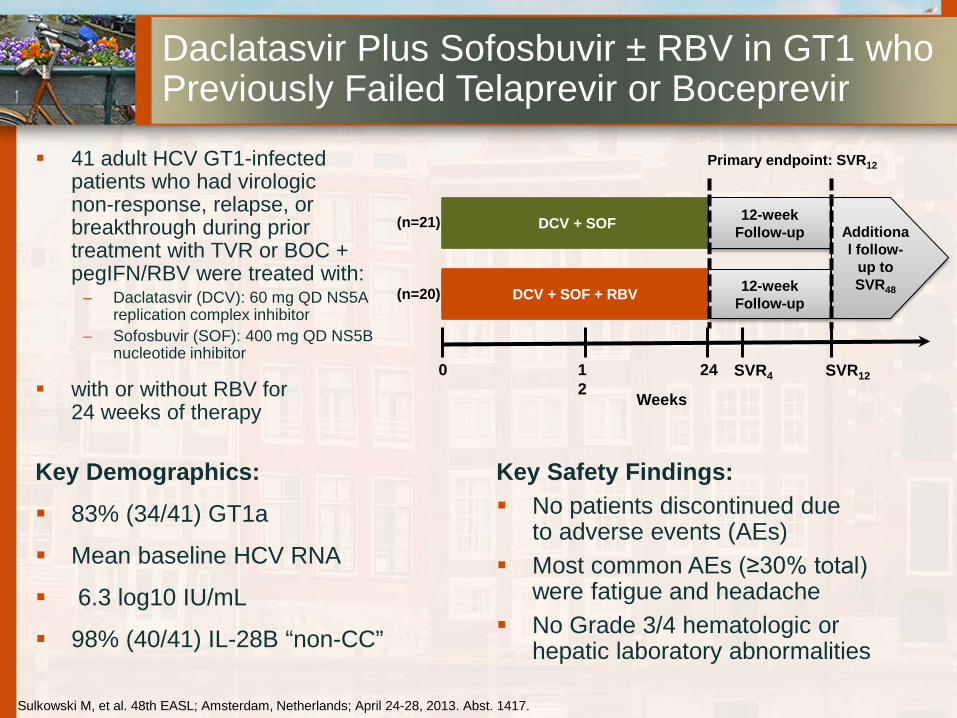
Daclatasvir Plus Sofosbuvir ± RBV in GT1 who Previously Failed Telaprevir or Boceprevir
41 adult HCV GT1-infected patients who had virologic non-response, relapse, or breakthrough during prior treatment with TVR or BOC + pegIFN/RBV were treated with:
– Daclatasvir (DCV): 60 mg QD NS5A replication complex inhibitor
– Sofosbuvir (SOF): 400 mg QD NS5B nucleotide inhibitor
with or without RBV for 24 weeks of therapy
Key Safety Findings: No patients discontinued due
to adverse events (AEs) Most common AEs (≥30% total)
were fatigue and headache No Grade 3/4 hematologic or
hepatic laboratory abnormalities
DCV + SOF
DCV + SOF + RBV 12-week Follow-up
12-week Follow-up Additiona
l follow-up to SVR48
0 12
24 SVR12
Weeks
Primary endpoint: SVR12
(n=21)
(n=20)
SVR4
Sulkowski M, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1417.
Key Demographics:
83% (34/41) GT1a
Mean baseline HCV RNA
6.3 log10 IU/mL
98% (40/41) IL-28B “non-CC”
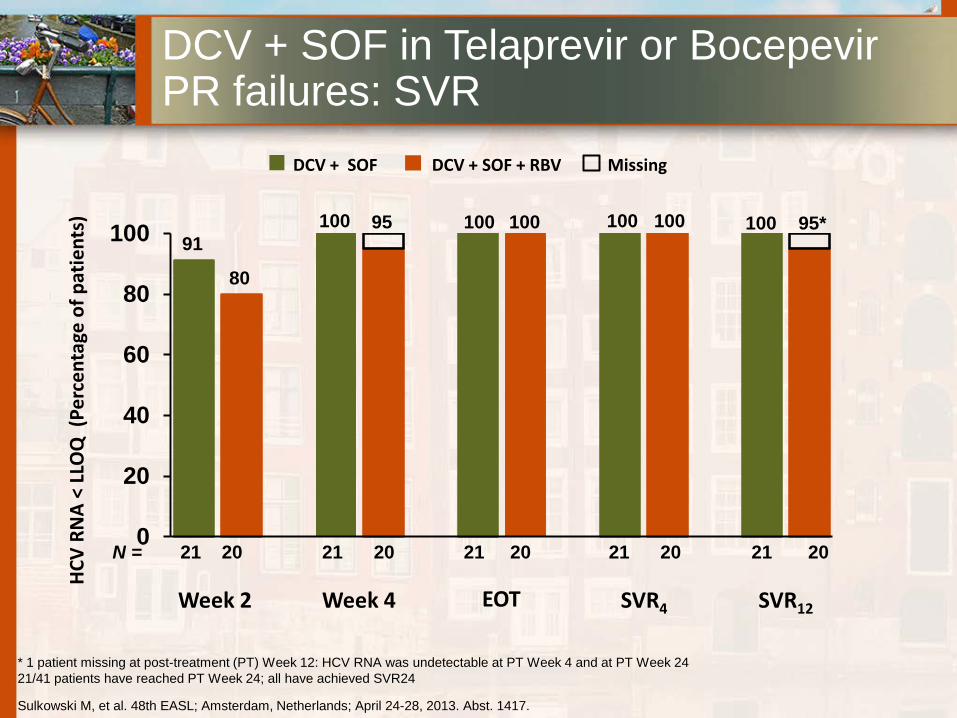
0
20
40
60
80
100
EOT
HCV
RNA
< LL
OQ
(Pe
rcen
tage
of p
atie
nts)
Week 2 SVR4
N =
Week 4
21 20
SVR12
100 100 100 100
21 20 21 20 21 20 21 20
DCV + SOF
100
91
80
95 100 95*
DCV + SOF in Telaprevir or Bocepevir PR failures: SVR
Sulkowski M, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abst. 1417.
* 1 patient missing at post-treatment (PT) Week 12: HCV RNA was undetectable at PT Week 4 and at PT Week 24 21/41 patients have reached PT Week 24; all have achieved SVR24
DCV + SOF + RBV Missing

»Triple therapy (PEG-IFN + RIBA + DAA) for GT1
»Slightly higher SVR in naive genotype 1 patients
»Shorter duration of treatment: 24 weeks
»2nd wave Pis promise better tolerability
»Simplified administration
»Additional Cost
What do the new DAAs promise for the near future ?