november 2014
DESCRIPTION
Our November 2014 issue of San Diego Physician looks at the Nov. 4 Proposition 46 victory, as well as infectious disease, Ebola, pertussis, vaccinating adults, and queso fresco.TRANSCRIPT
San Diego
Physicianofficial publication
of the san diego
county medical society
• “ P h y s i c i a n s U n i t e d f o r a h e a lt h y s a n d i e g o ” •
ProP. 46
soundlydefeated, 68-32%
Members: Thank
you for bringing
this victory about!
Members-to-Be:
Support your
member physician
colleagues and
your patients by
joining SDCMS-
CMA today!
sdcms.org
november 2014
On nOv. 4, The vOTerS
of California spoke loudly
and definitively, sending
the trial lawyers’ Proposi-
tion 46 to defeat by a vote
of 67% to 33%. The message
is clear: Californians sim-
ply don’t want to increase
healthcare costs and reduce
health access so trial attor-
neys can file more lawsuits.
An increase in the Medical
Injury Compensation Re-
form Act (MICRA) cap on non-economic damages has been rejected
in California again and again: 10 times in court, five times in the Leg-
islature, and now overwhelmingly by voters. This idea now has its
own dedicated spot in California’s political trash heap.
But this time we energized the membership of SDCMS and CMA
as a whole to fight the fight together, as one unified voice of medicine,
representing the patients we so deeply care about and the care that we
have committed to provide them.
Despite the trial attorney proponents’ attempt to sweeten the deal
by adding provisions that polled well — physician drug testing and
mandatory checking of a prescription database — voters said NO on
election night. As people throughout the state heard from physicians
and No-on-46 coalition members about the real intentions of the
measure’s proponents, there was resounding opposition.
One of the secret weapons of this effort was the size and diver-
sity of our coalition. We helped amass one of the largest and most
diverse campaigns in California history. The breadth of the coalition
— which includes labor, business, local government, health pro-
viders, community clinics, Planned Parenthood, ACLU, NAACP,
taxpayers, teachers, firefighters, and more — underscores just how
important affordable, accessible healthcare is to every Californian.
In addition to the groups on the ground talking to voters about the
deception and trickery behind Prop. 46, every major editorial board
in California opposed the initiative.
The Los Angeles Times said, “As worthwhile as [Proposition 46’s]
goals may be, the methods the measure would use to achieve them
are too flawed to be enacted into law.”

90%
90%
90%
90%
90%
B SAN DIEGO PHYSICIAN.OrG OctOber 2011
© 2014 NORCAL Mutual Insurance Company
Our beats in
Our heart beats in California … and has for almost 4 decades.
Since 1975 NORCAL Mutual has served healthcare professionals through-
out the Golden State. Strength, stability and innovative products are just
a few reasons why physicians continue to look to us for their medical professional
liability insurance. We provide you:
Industry-leading claims and risk solutions support 24/7
Full access to our interactive risk management library
Flexible coverage options tailored to your needs
California is important to us. So is your peace of mind. Come see how homegrown
strength can help protect your practice.
Visit heart.norcalmutual.com/ca or call your agent/broker today. 844.4NORCAL (844.466.7225)

90%
90%
90%
90%
90%

V I S I B L E
363 FEET linear frontage on Palomar Airport Road
(43,492 CARS PER DAY)
A C C E S S I B L E
1 MILE from Interstate 5(202,572 HOUSEHOLDS WITHIN
20 MINUTE DRIVE)
S T R A T E G I C
North County’s most affluent demographics
($98,614 AVG HOUSEHOLD INCOME IN A 5 MILE RADIUS)
6 0 1 0 H i d d e n Va l l e y R o a d , C a r l s b a d , C A 9 2 0 1 1
9 0 , 0 0 0 S F
CAMPUS
TRAVIS IVESAssociate DirectorLic. # [email protected]
CUSHMAN & WAKEFIELD OF SAN DIEGO, INC.CA License No. 1329963
4747 Executive Drive, 9th Floor San Diego, CA 92121
5 0 , 0 0 0 S F existing medical office building
3 9 , 0 0 0 S F proposed build-to-suit
opportunity
NORTH COUNTY’S NEWEST AND MOST COVETED MEDICAL CAMPUS
FOR MORE INFORMATION, PLEASE VISIT WWW.NORTHCOASTMEDICALPLAZA.COMOpinions expressed by authors are their own and not necessarily those of San Diego Physician or SDCMS. San Diego Physician reserves the right to edit all contributions for clarity and length as well as to reject any material submitted. Not responsible for unsolicited manuscripts. Advertising rates and informa-tion sent upon request. Acceptance of advertising in San Diego Physician in no way constitutes approval or endorsement by SDCMS of products or ser-vices advertised. San Diego Physician and SDCMS reserve the right to reject any advertising. Address all editorial communications to [email protected]. All advertising inquiries can be sent to [email protected]. San Diego Physician is published monthly on the first of the month. Subscription rates are $35.00 per year. For subscriptions, email [email protected]. [San Diego County Medical Society (SDCMS) Printed in the U.S.A.]
Volume 101, Number 11contentsNoV.
24 Soft Cheeses From Mexico: Could This Be Making Your Patients Sick? BY WILMA J. WOOTen, MD, MPh,
JeSSICA ADAM, MD, MPh, AnD JUSTIne
KOZO, MPh
26 Physician Marketplace: Classifieds
28 Work-Life Choices: What Are Yours? BY heLAne FrOneK, MD, FACP, FACPh
2 N ov em b er 2014
28feature8 Proposition 46 Soundly DefeatedBY J. STeven POCeTA, MD,
PreSIDenT, SDCMS
departments4 Briefly Noted: Calendar • New and Returning Members • Volunteer Opportunities • And More … 10 Communication Is Key to Improving Diabetic Patient Outcomes and Reducing Liability BY The DOCTOrS COMPAnY
12 Who Should Care About Ebola? BY GOnZALO BALLOn-LAnDA, MD
18 New Immunization Recommendations: Adults Getting Children’s Vaccines and Other New Approaches BY rOBerT e. PeTerS, MD, PhD, AnD
MArK h. SAWYer, MD
20 Pertussis: San Diego County Update BY erIC MCDOnALD, MD, MPh, AnD
KAren WATerS-MOnTIJO, MPh
MANAGING EDITOR: Kyle LewisEDITORIAL BOARD: Sherry L. Franklin, MD, James Santiago Grisolía, MD, Theodore M. Mazer, MD, Robert E. Peters, PhD, MD, David M. Priver, MDMARKETING & PRODUCTION MANAGER: Jennifer RohrSALES DIRECTOR: Dari PebdaniART DIRECTOR: Lisa WilliamsCOPY EDITOR: Adam Elder
SDCMS BOARD OF DIRECTORS
OFFICERSPRESIDENT: J. Steven Poceta, MDPRESIDENT-ELECT: William T-C Tseng, MD, MPH (CMA Trustee)TREASURER: Mihir Y. Parikh, MDSECRETARY: Mark W. Sornson, MDIMMEDIATE PAST PRESIDENT: Robert E. Peters, PhD, MD
GEOGRAPHIC AND GEOGRAPHIC ALTERNATE DIRECTORSEAST COUNTY: Venu Prabaker, MD, Alexandra E. Page, MD, Jay P. Mongiardo, MD, Alt: Susan Kaweski, MD (CALPAC Treasurer)HILLCREST: Gregory M. Balourdas, MD, Thomas C. Lian, MD, Alt: Thomas J. Savides, MDKEARNY MESA: Sergio R. Flores, MD, John G. Lane, MD, Alt: Anthony E. Magit, MD, Alt: Eileen R. Quintela, MDLA JOLLA: Geva E. Mannor, MD, Marc M. Sedwitz, MD, Alt: Lawrence D. Goldberg, MDNORTH COUNTY: James H. Schultz, MD, Eileen S. Natuzzi, MD, Michael A. Lobatz, MD, Alt: Anthony H. Sacks, MDSOUTH BAY: Reno D. Tiangco, MD, Michael H. Verdolin, MD, Alt: Elizabeth Lozada-Pastorio, MD
AT-LARGE DIRECTORSLawrence S. Friedman, MD, Karrar H. Ali, MD, Kosala Samarasinghe, MD, David E.J. Bazzo, MD, Stephen R. Hayden, MD, Peter O. Raudaskoski, MD, Vimal Nanavati, MD (Board Representative), Holly B. Yang, MD
AT-LARGE ALTERNATE DIRECTORSKarl E. Steinberg, MD, Jeffrey O. Leach, MD, Toluwalase A. Ajayi, MD, Phil Kumar, MD, Wayne C. Sun, MD, Kyle P. Edmonds, MD, Carl A. Powell, DO, Marcella M. Wilson, MD
OTHER VOTING MEMBERSCOMMUNICATIONS CHAIR: Sherry L. Franklin, MD (CMA Trustee)YOUNG PHYSICIAN DIRECTOR: Edwin S. Chen, MDRESIDENT PHYSICIAN DIRECTOR: Jane Bugea, MDRETIRED PHYSICIAN DIRECTOR: Rosemarie M. Johnson, MDMEDICAL STUDENT DIRECTOR: Spencer D. Fuller
OTHER NONVOTING MEMBERSYOUNG PHYSICIAN ALTERNATE DIRECTOR: Daniel D. Klaristenfeld, MDRESIDENT PHYSICIAN ALTERNATE DIRECTOR: Diana C. Gomez, MDRETIRED PHYSICIAN ALTERNATE DIRECTOR: Mitsuo Tomita, MDSDCMS FOUNDATION PRESIDENT: Albert Ray, MD (CMA Trustee, AMA Delegate)CMA SPEAKER: Theodore M. Mazer, MDCMA PAST PRESIDENTS: James T. Hay, MD (AMA Delegate), Robert E. Hertzka, MD (Legislative Committee Chair, AMA Delegate), Ralph R. Ocampo, MDCMA TRUSTEES: Robert E. Wailes, MD, Erin L. Whitaker, MDCMA SSGPF DELEGATE: James W. Ochi, MDCMA SSGPF ALTERNATE DELEGATES: Dan I. Giurgiu, MD, Ritvik Mehta, MDAMA ALTERNATE DELEGATE: Lisa S. Miller, MD
12
V I S I B L E
363 FEET linear frontage on Palomar Airport Road
(43,492 CARS PER DAY)
A C C E S S I B L E
1 MILE from Interstate 5(202,572 HOUSEHOLDS WITHIN
20 MINUTE DRIVE)
S T R A T E G I C
North County’s most affluent demographics
($98,614 AVG HOUSEHOLD INCOME IN A 5 MILE RADIUS)
6 0 1 0 H i d d e n Va l l e y R o a d , C a r l s b a d , C A 9 2 0 1 1
9 0 , 0 0 0 S F
CAMPUS
TRAVIS IVESAssociate DirectorLic. # [email protected]
CUSHMAN & WAKEFIELD OF SAN DIEGO, INC.CA License No. 1329963
4747 Executive Drive, 9th Floor San Diego, CA 92121
5 0 , 0 0 0 S F existing medical office building
3 9 , 0 0 0 S F proposed build-to-suit
opportunity
NORTH COUNTY’S NEWEST AND MOST COVETED MEDICAL CAMPUS
FOR MORE INFORMATION, PLEASE VISIT WWW.NORTHCOASTMEDICALPLAZA.COM

4 N ov em b er 2014
//////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////
SDCMS Seminars & Webinars SDCMS.orgfor further information or to register for any of the follow-ing sdcms seminars, webinars, workshops, and courses, email [email protected].
Pain Management Strategies to Decrease Liability risk (seminar/webinar)nov 20: 11:30am–12:30pm
CMa Webinars and EventsCMAnet.org/events
Coordinated Care Initiative (CCI): What Physicians need to Know (webinar)dec 2: 12:00pm–1:00pm
Coordinated Care Initiative (CCI): What Physicians need to Know (webinar)dec 3: 6:00pm–7:00pm
CMA Solo and Small Group Practice Forum Meetingdec 4: attention physicians in practices with 1–4 members: the cma house of delegates (hod) is in san diego this year and so is the solo and small group practice forum (ssgpf) annual dinner. the ssgpf, which represents
calendar
briefly noted
your interests at cma, will be meeting at edgewater grill in seaport village on thursday, december 4, at 5:30pm. the dinner is graciously sponsored by the cooperative of american physicians. come meet your hod representatives, say thanks to california legislators who support organized medicine’s position on scope of practice, and air your own ideas. email [email protected] to rsvp.
Community Healthcare Calendarto submit a community healthcare event for possible publication, email [email protected]. events should be physician-focused and should take place in or near san diego county.
essential Tools in Serving Diverse Populationsnov 18 (scottish rite event center on camino del rio south, registration open in september)
Update in rheumatology 2014: highlights From the ACr and eULAr Meetingsdec 13 (https://cme.ucsd.edu/rheumatology/)
infectioUs disease
sdcMs convenes countywide Meeting to discuss ebola:On Monday, Oct. 20, SDCMS convened nearly 100 chiefs of staff, representatives from the County, politicians, and other infectious disease specialists to discuss Ebola, to share preparation plans for an Ebola patient, and to ask questions of each other. SDCMS has ensured all attendees now know each other and are able to easily com-municate with each other. The SDCMS GERM Commission – the Infectious Disease leaders in San Diego County — will continue to address the disease from a clinical perspective.
yoUr sdcMs foUndation
While the SDCMS Foundation is best known for the work of its Project Access San Diego (it changed the lives of 39 people at this past Oct. 25 Surgery Day), it is also involved in many other health improvement initiatives:• Its colorectal cancer screening program
assists community health centers to boost their screening rates; one of the clinics boosted from 16% to 55% in one year.
• It has provided more than 2,000 free clini-cal breast exams and mammograms to uninsured women in the past 12 months.
• Last flu season, 500 people received free flu shots; the Foundation’s goal this season is 750.
• It is launching its Jump Start for Health diabetes prevention program aimed at
pre-diabetics presenting at UC San Diego emergency department.
• Medical students and new residents at UC San Diego School of Medicine receive support from the SDCMS Foundation through small scholarships and trips to Sacramento for advocacy training.
• 360 private practice physicians received technical assistance to adopt EHRs and achieve Meaningful Use Stage 1.
• Retired physicians continue to earn CEUs and maintain professional relationships through its Retired Physicians Society.
• Newly discharged military needing assistance to navigate the healthcare system are paired with retired physi-cians through its Physician Advocates for Veterans (PAVE) program.
What Has the SDCMS Foundation Done for San Diego County Lately?

//////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////
SA N D I eGo P H YSI C I A N .o rG 5
“think SDCMS FiRSt!”
Start by contacting SDCMS at (858) 565-8888 or at
858.256.0351 • www.abs-sol.com
We can help - absolutely!
2004 - 2014
Abs
olut
e SolutionsCelebratingCelebrating
Auditing
Contracting
Credentialing
Billing Service
Business Growth
Executive Assistant
Financial Management
EHR Meaningful Use Support
Operational Management
Practice Assessment
Practice Management
Relocation Management
Technological Advances
San Diego County All Physician Directory 2014–15Published by the san diego County MediCal soCiety (sdCMs)
Delete Listing for the Following Physician:•Robertson, Cynthia A. MD
Update Listings for the Following Physicians:•Adams, Charles A. MD {p} T: 7607539500 F:
7607530785 A: 285 N El Camino Real, Suite 219, Encinitas 92024 N: 1083608533
•Brown, Douglas E. MD {cd/im} T: 8587643150 F: 8587649083 A: 3811 Valley Centre Drive, San Diego 92130 N: 1750345112
•Chahal, Nittly S. MD {im/plm} T: 6192704919 F: 7602709109 A: 7901 Frost Street, San Diego 92123 N: 1164682480
•HACKER,SCOTTALANMDMD{ors}T:6192869480F:6192869468•W:www.drscotthacker.comA:Alvarado/HelixOrthopedicsandSportsMedicine,5555ReservoirDrive,Suite104,SanDiego92120•8860CenterDrive,Suite350,LaMesa91942N:1750450805[art/knees/osm/shous]
•HOANG,VYUYENMD{pd} T:6194422560F:6194427836A:250EastChaseAvenue,Suite108,ElCajon92020N:1649575135
•KOBAYASHI,KARENNAOMIDO{obg} T:6192678313F:6194722008A:655EuclidAvenue,Suite409,NationalCity91950N:1497929517
•KOONINGS,PAULPHILIP,MD,FACOG{go/obg} T:6195282593F:6195283904W:kp.orgA:4647ZionAvenue,SanDiego92120N:1689733214
•LEV,RONEET,MD{em} T:6196863800F:8586750606A:4077FifthAvenue,Depart-mentEmergencyMedicine,SanDiego92103N:1144266123[clr/ems/pmd/pubh]
•MOSELEY,WILLIAMG.MD{u} T:6192600060F:6192996001A:3969FourthAvenue,Suite202,SanDiego92103N:1568564276
•Reddy, Sumana MD {ai} T: 6193776565 F: 6194502111 A: 8860 Center Drive, Suite 320, La Mesa 91942 N: 1053300251
•SEBRECHTS,CHRISTOPHERPAULMD{dr} T:8585650950F:8585652863W:sandi-egoimaging.comA:P.O.Box23540,SanDiego92193N:1487628558[nm]
•Shailam, Sunita MD {fp} A: 427 C Street, Suite 216, San Diego 92101 N: 1174625933
•Witczak, Izabela MD T: 7607366767 F: 7607366782 A: 150 Valpreda Road, San Marcos 92069 N: 1184735201
errata sheet✹

6 N ov em b er 2014
//////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////briefly noted
sdcMs-cMa MeMbershiP
henry S. Kane, MDchild and adolescent psychiatrycamp pendleton (760) 725-1555
Anas Kayal, MDnephrologyoceanside (858) 499-1900
Sheila M. Krishna, MDdermatologyoceanside (760) 758-5340
James e. Lamar, MD, MPhgeneral preventive medicinesan diego (639) 532-5502
John W. Love, MDemergency medicinesan diego (639) 532-5208
Fharak M. Chip, MDnephrologynational city (619) 475-4900
nicole Mau, MDdermatologyoceanside (760) 758-5340
Dan M. Meyer, MDthoracic surgeryla Jolla (858) 455-6330
Welcome New and Returning SDCMS-CMa Members!
navinder S. Sawhney, MDclinical cardiac electrophysiologyescondido (858) 657-5310
helen J. Sohn, MDgeneral surgeryla mesa (619) 462-8100
Miranda r. Sonneborn, MDfamily medicinesan diego (858) 499-2703
raymond h. Summers, MDpathologysan diego (619) 229-3135
Joseph C. Tulagan, MDpediatricsnational city (619) 382-3350
Catherine L. Worden, MDobstetrics and gynecologyescondido (760) 745-1363
henry Yuan, MDnephrologychula vista (619) 427-1144
RETURNING MEMBERS
Deidre A. Buddin, MDdermatologysan diego (858) 558-0677
Arman Faravardeh, MDnephrologyla mesa (619) 461-3880
Kristy A. Lamb, MDpsychiatryla Jolla (619) 543-6440
NEW MEMBERS
John G. Apostolides, MD, FACSplastic surgerysan diego(619) 222-3339
Christopher v. Crosby, MD, FAAD, PhDdermatologic surgeryla mesa(619) 462-1670
Sivaraman K. Gounder, MDinternal medicinesan diego(908) 361-0185
John S. hammes, MDnephrologysan diego(619) 299-2350
Shannon L. hart, DOobstetrics and gynecologyescondido(760) 745-1363
Paul W. hinshaw, DOobstetrics and gynecologyescondido(760) 745-1363
Srinivas S. Iyengar, MD, FACSophthalmologyoceanside(760) 757-1144
physician volunteers needed!Email Your Physician Volunteer Opportunities to [email protected]
VOLUNTEER PHYSICIANS WANTED FOR PROJECT ACCESS: Volunteer specialty physicians needed for the following special-ties: pulmonology, urology, neurology, and sleep study. We are seeking these specialists throughout all regions of San Diego. Commit-ment can vary by practice. The mission of Proj-ect Access is to improve community health, access to care for all, and wellness for patients and physicians through engaged volunteerism. Help us help the most vulnerable population seek care. For more information, please call Ana Seda at (858) 565-8161 or email [email protected], or visit our website at www.sdcmsf.org. [282]
FAMILY MEDICINE/GENERAL INTERNAL MEDICINE PHYSICIANS NEEDED: Excel-lent family medicine and general internal medicine community docs to serve as role models and teachers to UC San Diego first- and second-year medical students in their Ambu-latory Care Apprenticeship Program. This is a longitudinal one-afternoon-every-other-week clinical experience that extends from the be-ginning of medical school to the end of the sec-ond year, approximately 25 sessions in all. The goals are to allow students to practice history taking and physical examination skills, learn what primary care is all about, and develop a nurturing student-mentor relationship with a positive, enthusiastic practicing primary care physician in the community. Join us! Call Rusty Kallenberg, MD, at (619) 838-8047 or email [email protected]. [281]
HUMANITARIAN TEAMS NEED MEDICAL VOLUNTEERS FOR HAITI: The Seattle-King County Disaster Team is looking for physicians for one-week primary care medical clinics in rural Haiti in February and June 2015. This is a rewarding opportunity to work with the people of Haiti and provide care in a very austere environment in a medically underserved area. Seattle-King County Disaster Team — a US-based nonprofit — has been operating these clinics since 1998. It coordinates all in-country travel and logistics. Please contact Bob Downey at (619) 905-7157 or by email at [email protected] if you are interested in applying.
giving back
“”
Then indecision brings its own delays,And days are lost lamenting o’er lost days.Are you in earnest? Seize this very minute;What you can do, or dream you can, begin it.— Johann Wolfgang von Goethe, German Writer and Statesman (1749–1832)
qUote of the Month

SA N D I eGo P H YSI C I A N .o rG 7
//////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////////giving back
As San Diego’s only provider to offer a full spectrum of treatment for advanced heart failure,
Sharp HealthCare gives you unprecedented choices to help improve your patients’ quality of life.
New techniques, such as MitraClip and TAVR, provide solutions for Level 3 and 4 heart failure
patients with few options before. You’ll work in partnership with board-certifi ed physicians
specializing in our complete range of treatments — from medical management and
transplantation to destination mechanical assist devices.
And your patients will be cared for with the leading-edge technology, skill and compassion that
are hallmarks of The Sharp Experience.
At Sharp, it’s easy to fi nd the specialist who matches your patient’s individual needs. Heart
Failure/Valve Coordinator Annette Contasti, RN, MSN, CHFN, will work with you on a referral
recommendation. Call (858) 939-5656 or email [email protected].
CORP616A ©2014 SHC
New Percutaneous Mitral Valve Repair
Now available to patients outside of clinical
trials, the MitraClip® system is a minimally
invasive alternative for degenerative mitral
regurgitation patients at prohibitive risk for
traditional surgery.
Remarkable new options for your patients with advanced heart failure
8 N ov em b er 2014
MiCra
On Nov. 4, the voters of California spoke loudly and definitively, sending the trial lawyers’ Proposition 46 to defeat by a vote of 68% to 32%. The message is clear: Californians simply don’t want to increase healthcare costs and reduce health access so trial attorneys can file more lawsuits. ¶ An increase in the Medical Injury Compensation Reform Act (MICRA) cap on non-economic damages has been rejected in California again and again: 10 times in court, five times in the Legislature, and now overwhelmingly by voters. This idea now has its own dedicated spot in California’s political trash heap.
by J. SteVeN Poceta,
mD, PreSiDeNt, SDcmS
Soundly De featedProposition 46

SA N D I eGo P H YSI C I A N .o rG 9
(858) 569-0300www.soundoffcomputing.com
TrusT
A Common sense ApproACh To InformATIon
TeChnologyTrust us to be your
Technology Business Advisor
hArdwAre sofTwAreneTworks
emr ImplemenTATIonseCurITy supporT
mAInTenAnCe
Endorsed by
But this time we energized the member-ship of SDCMS and CMA as a whole to fight the fight together, as one unified voice of medicine, representing the patients we so deeply care about and the care that we have committed to provide them.
Despite the trial attorney proponents’ attempt to sweeten the deal by adding pro-visions that polled well — physician drug testing and mandatory checking of a pre-scription database — voters said NO on elec-tion night. As people throughout the state heard from physicians and No-on-46 coali-tion members about the real intentions of the measure’s proponents, there was resound-ing opposition.
One of the secret weapons of this effort was the size and diversity of our coalition. We helped amass one of the largest and most diverse campaigns in California history. The breadth of the coalition — which includes labor, business, local government, health providers, community clinics, Planned Par-enthood, ACLU, NAACP, taxpayers, teach-ers, firefighters, and more — underscores just how important affordable, accessible healthcare is to every Californian.
In addition to the groups on the ground talking to voters about the deception and trickery behind Prop. 46, every major edito-rial board in California opposed the initiative.
The Los Angeles Times said, “As worth-while as [Proposition 46’s] goals may be, the methods the measure would use to achieve them are too flawed to be enacted into law.”
The San Francisco Chronicle decried Prop. 46, saying that the measure “overreached in a decidedly cynical way.”
The Orange County Register, U-T San Di-ego, San Jose Mercury News, Monterey Coun-ty Herald, Sacramento Bee, and dozens of other newspapers echoed these sentiments.
The efforts of the California Medical Association and the county medical asso-ciations across the state are a tremendous showing of what we can do for the future of healthcare, the quality of medicine, and the dedication to patients everywhere. Working together to spread the truth about Prop. 46, building coalitions across communities, and standing strong as one united voice are what helped carry us to victory.
This was one of the most contentious and high-stakes ballot fights in California his-tory, and we rose to the occasion. We must use this unity moving forward and showcase to our colleagues the value that the San Di-ego County Medical Society and California Medical Association bring to our great pro-fession, and stay united for whatever comes our way next.
Soundly De featedProposition 46
We energized the membership of SDCMS and
CMA as a whole to fight the fight together, as one unified voice of medicine, representing the patients we so deeply care about
and the care that we have committed to
provide them.

10 N ov em b er 2014
becaUse diabetes has the potential for serious complications and requires im-mense involvement by patients and physi-cians for successful outcomes, healthcare professionals who treat diabetic patients may be at risk for malpractice lawsuits.
In a study of claims closed from 2007 to 2013, The Doctors Company identified four common allegations made by patients with diabetes:
1. improper management of treatment: 37%2. failure or delay in diagnosis: 31%3. failure to treat: 9%4. improper management of medication
regimens: 6%Diabetic patients’ treatment is often
managed by a multidisciplinary care team, which may include a primary care physician, endocrinologist, dietician, ophthalmologist, podiatrist, and dentist. When patients file
claims, it’s not uncommon for them to name the entire care team in the complaint, alleg-ing failure to properly diagnose, supervise, monitor, and/or treat their disease.
To promote patient safety, the healthcare team should engage the patient in collabora-tive care planning and problem solving to produce an individualized care plan as well as team support when problems are encoun-tered. Other ways to promote patient safety and mitigate the risk of malpractice claims related to diabetes care are:
Communicate: Talking openly with diabetic patients about their condition and encouraging them to take an active role in decision-making enhances patient safety.
• Overcome patients’ fears about their dis-ease by taking time to answer questions.
• Discuss all associated risk factors, including weight gain. The American Medical Association and American Diabetes Association have resources available to help physicians talk to their patients about weight and diabetes.
• Provide written instructions and information about adverse effects for prescription drugs and complex pre-scription drug regimens.
• Communicate with the patient and prepare written information in the language and at the literacy level that the patient understands.
• Ask patients to repeat the information shared, not just whether they under-stand what they have been told.
Educate: Educate patients about the importance of self-management to help increase their compliance and to reduce the risk of patients attributing their injuries to substandard care. Diabetic patients should be able to articulate the importance of lab tests, medication management, diet, and exercise. Barriers to self-management, such as financial issues or lack of social support, healthcare literacy, and patient-caregiver relationships, should be assessed.
Document:Document any and all pa-tient interactions and discussions regarding the patient’s condition, including diagnosis, specialist referrals, and treatment options.
Managecare:Implement a program that ensures timely follow-up when a patient fails to schedule an appointment, misses an ap-pointment, or cancels an appointment and does not reschedule. Failure to follow up and provide intensive patient management can lead to missed or delayed diagnoses, acceler-ated disease symptoms, morbidity, and/or mortality.
risK management
communication is key to improving diabetic Patient
outcomes and reducing liability
Contributed by SDCMS-endorsed The Doctors Company. For more patient safety articles and practice tips,
visit www.thedoctors.com/patientsafety.
3 reasons to partner with us:
Exclusive specialization: We know medical office properties. It is all we do.
Extensive experience: We leverage our 35+ years of experience in healthcare real estate to assure a seemless transaction and save you money.
Optimal solutions: We will find you what you need and help you craft an ideal real estate solution.
Put our experience and expertise to work. Contact us today:
Paul Braun Chris Ross Kelly MoriartyManaging Director Vice President Associate+1 858. 410 6388 +1 858 410 6377 +1 858 410 [email protected] [email protected] [email protected]
www.us.joneslanglasalle.com/healthcare Leases ▪ Renewals ▪ Sales ▪ Strategic Planning ▪ Demographic & Patient Analysis
Helping your bottom line, one square foot at a time.

12 N ov em b er 2014
ebola?Who Should Care about
by GoNzalo balloN-laNDa, mD
infectious
disease

SA N D I eGo P H YSI C I A N .o rG 13
Consider the mother of three children who presented to the ER with fever and diarrhea, and who reported contact three weeks ear-lier with missionaries who recently returned from Liberia. Rightfully, this case triggered the rapid mobilization of considerable pub-lic health resources; however, when officials finally tracked down the missionaries in Michigan, they discovered that the mission-aries had come from Algeria, not Liberia, and therefore had posed no exposure risk.
Finally, consider also a local dental hy-gienist who recently returned from a medi-cal mission in Kenya, 3,000 miles away from the epidemic. Upon her return, her employer forbade her from working until she com-pleted the 21-day quarantine that Ebola de-mands. Each of these real-life anecdotes has engendered substantial financial, social, and emotional burdens, and each is the byprod-uct of media-fueled hysteria. FDR’s inaugu-ral address admonition rings loudest: “We have nothing to fear but fear itself.”
Nevertheless, the largest Ebola virus epi-demic in history is no laughing matter. It threatens to kill many more people in the affected areas of West Africa, and many efforts to curtail it are stymied by serious challenges. The virus kills around half of the people it infects, and we don’t know how many potential hosts are susceptible; there is a chance for severe mayhem there.
In October 1520, a great epidemic oc-curred in the Aztec capital, which was under siege by Hernán Cortés. It was caused by the smallpox virus, and the
epidemic was dubbed by the locals the huey ahuizotl (great rash). The invaders inad-
vertently introduced it. Although some ac-counts blame an African slave who belonged to one Diego de Narvaez, others attribute this to classic shifting of the blame from the part of the Spanish. Regardless of the identi-ty of the index case, this epidemic, depend-ing on the account, decimated 30–40% of the Aztec empire.
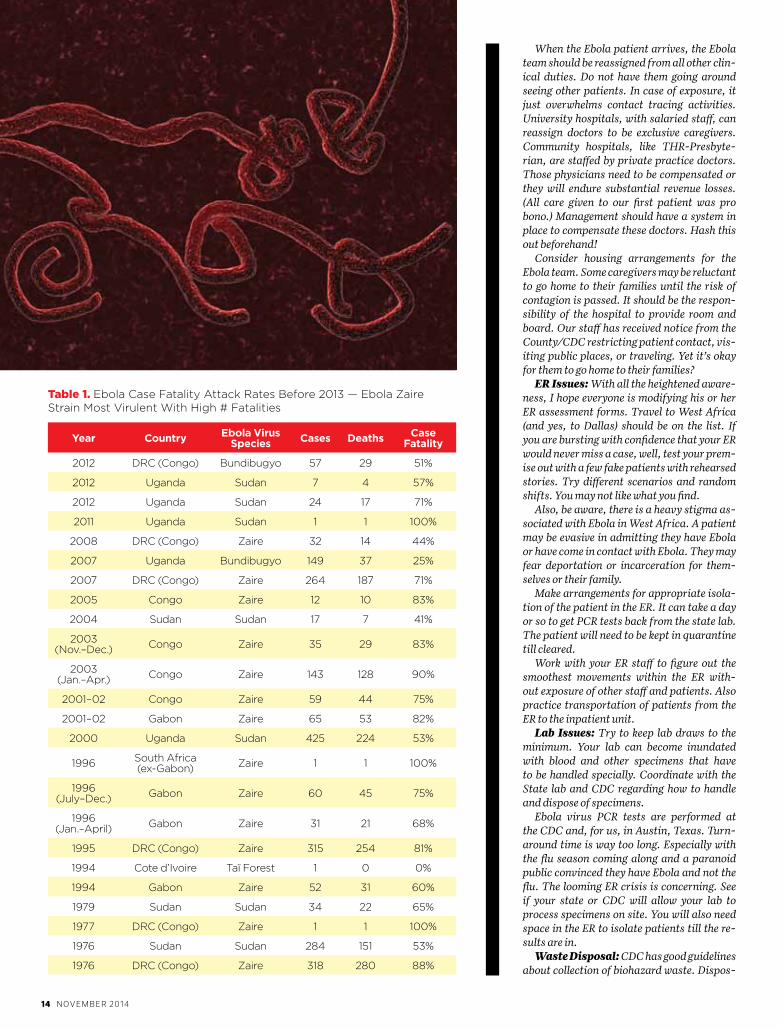
Yet this is not 1520, and Ebola is not small-pox. It is unlikely that this virus will cause havoc outside of Africa, although it could do so in other underdeveloped areas. There have been some 25 outbreaks of Ebola Hem-orrhagic Fever (EHF) in Africa since the first report in 1976 (Table 1). They have all re-solved within months.
Included below is an email from an infec-tious disease (ID) specialist in Dallas. He published it on the Emerging Infections Network (EIN) listserv to publicly share
his experience. It may give a fuller picture of caring for Ebola in the community. He writes,
I have been reading with interest all the chat-ter on EIN about managing Ebola patients. I am an ID physician at THR-Presbyterian Dallas hospital. While I did not directly care for any of the three Ebola patients, three of my partners did, and I was abreast of most of the goings on at our hospital. It has been a memo-rable and enlightening experience. I’d like to share some of our experiences in the hope that you may better prepare yourself and your in-stitution on the chance that an Ebola patient shows up in your hospital. These opinions and observations are purely my own. They do not reflect the views of our hospital, my other partners, or the CDC.
Determine First and Foremost if Your Hospital Has the Capacity to Care for an Ebola Patient: Caring for an Ebola patient is not business as usual. The toll on a hospi-tal can be substantial. Once it became known we were housing Ebola patients, our census plummeted. Elective surgeries, clinic vis-its, and deliveries disappeared. Our ER was placed on divert. We had to dedicate the entire medical ICU to house the Ebola patients. Sev-eral staff members caring for the first patient have been furloughed for three weeks from last contact. Two of my own partners are re-moved from patient contact, and a third may be too. Needless to say, the financial burden is huge, and the impact on daily operations is substantial. Talk to your senior management team and make sure they are willing to endure the cost and disruption in services.
Build a Volunteer Team Who Will Be the Exclusive Caregivers: It is impossible to train the entire hospital staff in proper isolation methods. Keep the number of con-tacts with the patient to the bare minimum. Consultants can relay their opinions (with-out direct patient contact) after doing a chart review and discussing with the primary caregivers. Goes without saying, suspend through-traffic in the isolation zone.
The volunteer team should include, at the minimum: an ID physician, ICU physician, ER physicians, respiratory techs, renal staff and dialysis techs, nurses, lab staff, radiolo-gist/techs, and environmental staff. These folks should be willing to care for the patient and ready to face the downstream effects of care. This includes the risk of getting infected, the risk of being furloughed, the risk of trans-mitting disease to their family members, the risk of social ostracism of themselves and their family. (Staff have been asked to stay away from church, children have been disin-vited from parties, etc.) I think you owe it to the staff that they fully comprehend what can happen. A few of our doctors and nurses had emotional meltdowns after they cared for the patient. Hippocratic Oath notwithstanding, you need to make sure the volunteers have the emotional fortitude to do the job.
Once this team is collected, begin practice drills. Certify that each team member is fully capable of donning and doffing their gear. No one should be allowed near the patient with-out demonstrating proficiency in correct pro-tocol. Putting on the gear is a pain. Taking it off correctly is a supreme challenge. Wear-ing it is unbearable after a while. Nurses will need frequent rotations (probably every 3–4 hours). That is about the limit one can endure under the gear.
Decide beforehand if your team will con-sider invasive procedures such as intubation, dialysis, or CPR. We performed the former two in our patient. We felt CPR would be too high a risk for staff and had our patients sign DNR orders. Practice doing the procedures in the PPE. It’s quite challenging.
ebola?
everyone should, of course — and on current evidence, everyone does. At this point, nearly every hospital and clinic has dealt with panicked patients, families, and even healthcare professionals. Consider a dentist’s office where a boy arrived for his regular tooth cleaning. When asked, he denied any recent travel, but admitted that he was originally from Sierra Leone. never mind that he was not sick, nor had he traveled or had contact with anyone who traveled — the entire office evacuated, except for a few individuals who donned hazmat suits to complete the interview.
14 N ov em b er 2014
When the Ebola patient arrives, the Ebola team should be reassigned from all other clin-ical duties. Do not have them going around seeing other patients. In case of exposure, it just overwhelms contact tracing activities. University hospitals, with salaried staff, can reassign doctors to be exclusive caregivers. Community hospitals, like THR-Presbyte-rian, are staffed by private practice doctors. Those physicians need to be compensated or they will endure substantial revenue losses. (All care given to our first patient was pro bono.) Management should have a system in place to compensate these doctors. Hash this out beforehand!
Consider housing arrangements for the Ebola team. Some caregivers may be reluctant to go home to their families until the risk of contagion is passed. It should be the respon-sibility of the hospital to provide room and board. Our staff has received notice from the County/CDC restricting patient contact, vis-iting public places, or traveling. Yet it’s okay for them to go home to their families?
ER Issues: With all the heightened aware-ness, I hope everyone is modifying his or her ER assessment forms. Travel to West Africa (and yes, to Dallas) should be on the list. If you are bursting with confidence that your ER would never miss a case, well, test your prem-ise out with a few fake patients with rehearsed stories. Try different scenarios and random shifts. You may not like what you find.
Also, be aware, there is a heavy stigma as-sociated with Ebola in West Africa. A patient may be evasive in admitting they have Ebola or have come in contact with Ebola. They may fear deportation or incarceration for them-selves or their family.
Make arrangements for appropriate isola-tion of the patient in the ER. It can take a day or so to get PCR tests back from the state lab. The patient will need to be kept in quarantine till cleared.
Work with your ER staff to figure out the smoothest movements within the ER with-out exposure of other staff and patients. Also practice transportation of patients from the ER to the inpatient unit.
Lab Issues: Try to keep lab draws to the minimum. Your lab can become inundated with blood and other specimens that have to be handled specially. Coordinate with the State lab and CDC regarding how to handle and dispose of specimens.
Ebola virus PCR tests are performed at the CDC and, for us, in Austin, Texas. Turn-around time is way too long. Especially with the flu season coming along and a paranoid public convinced they have Ebola and not the flu. The looming ER crisis is concerning. See if your state or CDC will allow your lab to process specimens on site. You will also need space in the ER to isolate patients till the re-sults are in.
Waste Disposal: CDC has good guidelines about collection of biohazard waste. Dispos-
Year Country ebola virus Species Cases Deaths Case
Fatality
2012 drc (congo) bundibugyo 57 29 51%
2012 uganda sudan 7 4 57%
2012 uganda sudan 24 17 71%
2011 uganda sudan 1 1 100%
2008 drc (congo) Zaire 32 14 44%
2007 uganda bundibugyo 149 37 25%
2007 drc (congo) Zaire 264 187 71%
2005 congo Zaire 12 10 83%
2004 sudan sudan 17 7 41%
2003 (nov.–dec.) congo Zaire 35 29 83%
2003 (Jan.–apr.) congo Zaire 143 128 90%
2001–02 congo Zaire 59 44 75%
2001–02 gabon Zaire 65 53 82%
2000 uganda sudan 425 224 53%
1996 south africa (ex-gabon) Zaire 1 1 100%
1996 (July–dec.) gabon Zaire 60 45 75%
1996 (Jan.–april) gabon Zaire 31 21 68%
1995 drc (congo) Zaire 315 254 81%
1994 cote d’ivoire taï forest 1 0 0%
1994 gabon Zaire 52 31 60%
1979 sudan sudan 34 22 65%
1977 drc (congo) Zaire 1 1 100%
1976 sudan sudan 284 151 53%
1976 drc (congo) Zaire 318 280 88%
Table 1. ebola case fatality attack rates before 2013 — ebola Zaire strain most virulent With high # fatalities
FOLLOW US ON

FOLLOW US ON

16 N ov em b er 2014
Barry Masci, CFA, CMT, CMFC, CLU®, CFP®First Vice President – Investments11512 El Camino Real, Suite 210, San Diego, CA 92130858-720-2365 • [email protected] bmasci.wfadv.com
Wells Fargo Advisors, LLC, Member SIPC, is a registered broker-dealer and a separate non-bank affiliate of Wells Fargo & Company.© 2013 Wells Fargo Advisors, LLC. All rights reserved. 0514-03415 [74036-v4] A1272 (1194411_372510)
Investment and Insurance Products: NOT FDIC Insured NO Bank Guarantee MAY Lose Value
This is the future you weren’t thinking about 10, or 20, or 30 years ago.As a financial advisor since 1982, I have the experience, knowledge, and research to help you grow and preserve your wealth. The sooner you start, the better you can manage whatever life has in store. I can help you make it happen. If you’d like to know how, I’d be glad to talk with about your future. There’s no cost and no obligation.
Contact me today so we can begin planning together a better financial future for you.
ing of it is another matter. Do you have onsite incineration capacity or is your hospital one that subcontracts biohazard waste disposal? If the latter, then have the contractor provide input in your planning meetings. Know what your municipal, state, federal requirements are. Are there any Department of Transpor-tation restrictions to movement of hazardous material, etc.
Ebola Medicines: As you all know, there really isn’t any proven treatment for Ebola. But are you really going to stand by and not attempt to give at least one of the three ex-perimental medicines? Remember, all require an IND request from the FDA. If you have not applied for an IND request before, you are in for a shock. It can take substantial hours of your time. Usually the privilege falls upon the ID doctor caring for the patient (as though he or she has nothing better to do). Delegate the work to a colleague or recruit the hos-pital research corporation to assist in filing the request. Also work out an emergency IRB approval for these medicines and a consent form. Have this set up well in advance, or else it may delay administering the drugs.
Media: As inevitable as death and taxes. Speak the truth and with proper knowledge of the facts. Preferably someone from the direct care team — either the ID doc, or the ICU physician — should be present to answer patient care questions. Don’t leave a poor
hospital administration representative, who is not facile with the electronic records, out to the wolves. Clamp down on leaks. No cell phones or cameras. Staff will be tantalized by large sums of money to provide insider photos and details. Patient privacy is para-mount. Have your IT constantly survey the electronic records for unauthorized access to the charts.
Surrogate Decision-making: While this can be an issue even with local U.S. citizens, it can be very challenging for folks coming from West Africa. There are cultural differences in who can be a decision-maker. Patients may come from families already decimated by Ebola. Be culturally respectful. Pin down the chain of command as soon as possible. Some-one other than the patient may need to give permission for experimental treatments, di-alysis, or intubation.
These are some early observations. Ebola can easily be handled in any U.S. hospital. I am quite sure of that, even after all that has transpired here in Dallas. Both our hospital and the state and federal authorities have learned a lot in a real-time situation. I hope the CDC will come back with more pragmatic and robust suggestions for care and infection control. Maybe develop a CDC SWAT team that swoops in and verifies the local capacity of the hospital within 24 hours of confirma-tion of diagnosis.
Dr. Ballon-Landa, a 33-year member of SDCMS-CMA, is board certified in internal medicine and infectious disease and is chair of SDCMS’ Group to Eradicate Resistant Microorganisms (GERM) Commission.
There is a negligible chance that you would be the first person to come in contact with a suspected case of imported ebola. If you are, here are the steps you should take:
don protective equipment: gowns, double gloves, n95 masks, shoe booties, and full-face goggles.
call san diego county epidemiology at (858) 565-5255.
most patients will be held in ed-designated areas for isolation and observation, if nothing else. the great majority of these will turn out to be not ebola.
More information can be found at http://emergency.cdc.gov/han/han00366.asp.
1.
2.
3.

New and Refurbished Medical Equipment Sales
Calibrations and Repair Services
CBET Certified Technicians
Family Owned and Operated
Sterilizers, EKG Machines, Exam Tables, Electrosurgical Units, Anesthesia Machines, Monitors and More!
800-435-0507akwmedical.com
1990
ServingPhySicianSSince
Medical Equipment Sales • Repairs • Calibrations

18 N ov em b er 2014
infectious
disease
RECOMMENDATIONSnew immunization
adults getting children’s vaccines
and other new approaches
By Robert E. Peters, MD, PhD, and Mark H. Sawyer, MD
WWe are entering the decade of adult immunizations. Childhood immunizations have exploded over the past two decades, and immunization coverage rates for children are generally good. Now it is time to get our adult population better immunized. We can start, of course, by doing a better job of immunizing with our longstanding adult vaccines, such as influenza vaccine, pneumococcal polysaccharide vaccine, and zoster vaccine. In addition, there are now new recommendations that adults receive conjugated pneumococcal vaccine and that individuals with diabetes receive hepatitis B vaccine.

SA N D I eGo P H YSI C I A N .o rG 19
We also have a new HPV vaccine coming in 2015. For young children, there is a new pref-erence for use of the live attenuated nasal influenza vaccine this winter. Here is a quick summary of some important new immuni-zation recommendations.
The conjugated 13-valent pneumococcal vaccine (Prevnar) has been used in children for many years with great success. Not only has this vaccine reduced rates of invasive pneumococcal disease in children dramati-cally, it has also had the indirect effect of protecting adults because they are less likely to be exposed to a child carrying pneumo-coccus in their nasopharynx. Despite that, the pneumococcus still causes thousands of cases of both invasive disease and non-bac-teremic pneumonia in adults in the United
States, particularly in those 65 years of age and above. For years we have immunized seniors with the 23-valent pneumococcal polysaccharide vaccine (Pneumovax) to try to decrease these outcomes but with only modest success. In August 2014 the CDC’s Advisory Committee on Immunization Practices issued a new recommendation that we start routinely using the conjugate vaccine (Prevnar) in addition to the poly-saccharide vaccine (Pneumovax) for all in-dividuals 65 years of age and above (MMWR 2014;63:822-825). This recommendation is based on a large study recently completed in the Netherlands demonstrating signifi-cant reductions in both invasive disease and non-bacteremic pneumonia caused by the serotypes in the vaccine among those vaccinated. In order to achieve the optimal immune response, seniors should be im-munized first with the conjugate vaccine (Prevanar) starting at age 65 years, followed 6–12 months later by a booster dose with the polysaccharide vaccine (Pneumovax). For your patients who have already received the polysaccharide vaccine, the conjugate vaccine is still recommended but with a minimum of one year between the two vac-cines. This all creates a challenge for you and your staff to stock both vaccines, know the intervals between the vaccines, docu-ment carefully which vaccines have been given to each patient, and to educate your patients about the need for two different pneumococcal vaccines.
Younger adolescent and adult popula-tions at high risk for pneumococcal vaccine also benefit from this two-vaccine approach to pneumococcal vaccination (MMWR 2012;61:816-819, MMWR 2013;62:521-524). These include patients with immunocom-promising conditions such as HIV infection or malignancy, and patients with func-tional or anatomic asplenia, CSF leaks, or cochlear implants.
The other brand-new immunization rec-ommendation applies to influenza vaccine for children 2 through 8 years of age. While the recommendation continues that all chil-dren six months of age and older be immu-nized every year with influenza vaccine, for the 2 through 8 year olds there is now a stat-ed preference that they receive the live at-
tenuated (nasal) vaccine (Flumist) (MMWR 2014; 63:691-697). This recommendation is based on several studies that show better protection with the nasal vaccine for this age group. When both vaccines are avail-able, providers should give the nasal vaccine preferentially. However, it is extremely im-portant not to miss opportunities to provide influenza vaccine, so if your office only has the injectable vaccine, that should be used rather than waiting for a later opportunity to give the nasal vaccine. Also important is the fact that for older children and adults there is no clear data demonstrating that one vaccine is superior to the other, so, for these groups, you can continue to use either vaccine based on your and the patient’s preference.
The last relatively new immunization recommendation is for patients with diabe-tes who we now know are at increased risk for acquiring hepatitis B infection, mostly through inappropriate use of shared blood glucose monitoring equipment. This is a particular problem in assisted-living and long-term care facilities. Because of this newly identified risk, newly diagnosed patients with diabetes who are under 60 years of age should be getting the three-dose hepatitis B vaccine to protect them (MMWR 2011;60:1709-1711). Older patients can also be immunized, but their immune response may be less, so the target popu-lation for this recommendation is patients with newly diagnosed diabetes who are un-der 60 years of age.
More vaccines are coming. There should be a new 9-valent human papilloma virus vaccine available in 2015, which will pro-vide us a way to prevent even more cancers caused by this virus. Work is underway on other new vaccines, with a focus on adults. While we wait for these exciting develop-ments, let’s all increase our efforts to deliver the vaccines we have right now. Vaccines are one of the most cost-effective prevention strategies we have. Use them!
Dr. Peters, SDCMS-CMA member for 17 years, is board-certified in family medicine and sits on SDCMS’ GERM Commission. Dr. Sawyer is with the UCSD School of Medicine and Rady Children’s Hospital, and sits on SD-CMS’ GERM Commission as well.
The last relatively new immunization recommendation is for patients with diabetes
who we now know are at increased risk for acquiring hepatitis B infection.

20 N ov em b er 2014
SAn DIeGO AnD OTher CALIFOrnIA counties are now experiencing a pertussis epidemic that began in late 2013. The ongo-ing cases are requiring significant resources from medical providers, public health, and families as they work together to combat an illness that just a few years ago seemed a well-controlled childhood disease. Out-breaks have been reported in elementary, middle, and high schools throughout the county and the state.
For the first nine months of 2014, the San Diego County Health and Human Services Agency has confirmed 1,429 cases, with a countywide rate of 44.9 cases per 100,000. During the 2010 pertussis epidemic, 1,179 local cases were reported. Overall pertussis rates have been highest for infants less than one year of age and adolescents 10–17 years of age. Thirty San Diegans have been hospital-ized, but none have died.
As of Sept. 15, 2014, the California De-partment of Public Health (CDPH) has re-
members when new babies are born are criti-cal. Every pregnant woman should get a Tdap in the third trimester of every preg-nancy. The preferred time for pregnancy immunization is between 27 and 36 weeks of gestation, although immunization during other stages of pregnancy is safe. Pertus-sis antibodies transferred from vaccinated mothers to their infants will help protect them until they are old enough to be vacci-nated. Women should be immunized regard-less of prior Tdap history. Current data show that only 30% of pregnant women in Califor-nia are receiving Tdap vaccine.
It is important to convey to parents with newborns that the primary DTaP vaccine series is essential for reducing severe disease in young infants and should not be delayed. DTaP can be given to infants at an accelerat-ed schedule, with the first dose given as early as six weeks of age. Even one dose of DTaP may offer some protection against fatal per-tussis disease in infants.
It may be many years before a new vac-cine is available that conveys a longer lasting immunity to pertussis. As such, a “new nor-mal” of higher rates of illness may persist in San Diego, the state, and the nation for some time. However, physicians working with families and public health professionals can mitigate the current epidemic by following these recommendations:• Encourage all individuals, especially
pregnant women, to be up to date with current pertussis vaccination recom-mendations.
• Assure that all healthcare employees are immunized against pertussis with Tdap.
• Inquire about recent possible pertussis exposures in schools or community set-tings, and consider pertussis regardless of vaccination status when evaluating patients with respiratory symptoms.
• Consider pertussis regardless of age when patients present with unexplained, persistent cough illness. Pertussis symp-toms are generally milder in teens and adults, especially in those who have been vaccinated.
• Be aware that the diagnosis of pertussis can be a challenge in young infants given that the cough may be undetectable or mild and fever is usually not present. Mild ill-ness may quickly transform into respirato-ry distress and include apnea, hypoxia, or seizures. Delays in treatment may increase the risk of fatal illness in young infants, es-pecially those younger than three months of age. More information about diagnosing pertussis in young infants is available at www.cdph.ca.gov/HealthInfo/discond/Documents/CherryPertussisInYoungIn-fants2011-06-20.pdf.
infectious
disease
PERTUSSISsan diego
county updateBy Eric McDonald, MD, MPH, and
Karen Waters-Montijo, MPH
ported 8,278 cases with onset this year, with a statewide rate of 21.7 cases per 100,000. Of the reported cases statewide, 288 have been hospitalized, with 68 (24%) requiring inten-sive care. Case counts are updated every two weeks at the CDPH pertussis webpage: www.cdph.ca.gov/HealthInfo/discond/Pages/Pertussis.aspx. Sadly, one death has been reported for 2014 in an infant who was five weeks old at the time of disease onset. There were two additional deaths in 2014 with dis-ease onset in 2013. Both infants were less than two months of age when symptoms began.
Pertussis is cyclical and peaks every 3–5 years as the numbers of susceptible per-sons in the population increase due to wan-ing immunity following both vaccination and disease. Acellular pertussis vaccines in current use cause fewer reactions than the whole-cell vaccines, but they appear not to protect as long. Approximately 84% of cases reported in the current epidemic are fully immunized. Nevertheless, it is important to continue promoting the current recom-mendations for vaccine to avoid more severe impacts from pertussis.
To manage this epidemic, the focus is on preventing infant morbidity and mortal-ity. Young infants have the greatest risk for hospitalization and death from pertussis. Consequently, maternal immunization dur-ing pregnancy and immunization of family

SA N D I eGo P H YSI C I A N .o rG 21
(858) 259-2795 or visit www.fi rstrepublic.com New York Stock Exchange Symbol: FRC
Member FDIC and Equal Housing Lender
“ We call First Republic and instantly talk to someone who truly helps us with our account.”D O C T O R S O F F E R I N G C H A R I TA B L E S E RV I C E S ( D O C S )
Michael Halls, M.D., F.R.C.S.(C), F.A.C.S., Co-Founder (left)Munish K. Batra, M.D., F.A.C.S., Co-Founder (right)

22 N ov em b er 2014
0
50
100
150
200
250
300
JAN FEB MAR APR MAY JUNE JUL AUG SEP OCT NOV DEC
2009 2010 2011 2012 2013 2014 YTD
0
300
600
900
1200
1500
2014 YTD20132012201120102009
144
1,179
400
164
431
1,429
Table 2. county of san diego pertussis cases by episode month, 2009–2014 calendar ytd (as of 09/30/14)
Table 1. pertussis cases by calendar year of occurrence, san diego county 2009–2014 ytd (as of 09/30/14)
• Obtain a nasal aspirate (preferable) or na-sopharyngeal swab for PCR testing and/or culture when pertussis is in the differ-ential diagnosis. Serologic tests are not recommended.
• Initiate antibiotic treatment prior to obtaining test results in patients with a clinical history suggestive of pertussis or with risk factors for severe complica-tions. Azithromycin is the preferred anti-biotic because of efficacy and compliance and it is covered by Medi-Cal for both treatment and prevention of pertussis.
• Instruct all patients diagnosed with per-tussis to stay home from school or daycare until they have completed five days of an-tibiotics, and to avoid contact with infants and others susceptible to the disease.
• Provide post-exposure prophylaxis (PEP) to all household contacts, caregivers, and other persons who have had direct contact with respiratory, oral, or nasal secretions from a symptomatic case, again regard-less of vaccination status. PEP antibiotic treatment is the same as treatment for disease and should not be shortened. Additional diagnosis and treatment in-formation may be found at www.cdph.ca.gov/HealthInfo/discond /Docu-ments/CDPH_Pertussis_Quicksheet.pdf.
For further information about pertussis, Tdap vaccine, and other vaccine-preventable diseases, please contact the HHSA Immuni-zation Program at (866) 358-2966.
Dr. McDonald, SDCMS-CMA member for the past six years, has a three-year tenure with the County of San Diego and currently serves as the medical director of the HHSA Epidemiol-ogy and Immunization Services Branch (EISB) in the local health department. Ms. Waters-Montijo serves as the chief of EISB and has worked for the county for the past 12 years.


24 N ov em b er 2014
Note: The findings and conclusions in this re-port are those of the author(s) and do not nec-essarily represent the official position of the Centers for Disease Control and Prevention.
FreSh CheeSe, COMMOnLY reFerreD to as queso fresco, is a popular, traditional, but potentially harmful food product con-sumed frequently in Hispanic communities. This highly favored cheese often is made with unpasteurized milk or stored unrefrigerated during transit; consequently, it can harbor harmful bacteria that can lead to foodborne illnesses and severe consequences among
infectious
disease
By Wilma J. Wooten, MD, MPH, Jessica Adam, MD, MPH,
and Justine Kozo, MPH
persons with immunocompromised systems, pregnant women, children, persons with comorbidities, and older persons. Common bacteria isolated in these products include Salmonella, Listeria monocytogenes, and My-cobacterium bovis. Illnesses from these bac-teria can result in fever, miscarriage, tuber-culosis, and even death (1,2). The Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report estimates that the incidence of L. monocytogenes (listeriosis) is ~24 times higher among pregnant Hispanic women. In that same report, four (33%) of 12 listeriosis outbreaks were linked to Mexican-style cheeses (3). In the San Diego–Tijuana border region, considerable quantities are imported from Mexico, and this cheese is then sold or shared among families and other social networks (1,2).
During 2004, two outbreaks of Salmonella disease occurred in San Diego County, result-ing in 14 and 49 cases, respectively. The sus-pected exposure was unpasteurized cheese from Mexico, purchased from street vendors (1). In 2009, the Food and Drug Administra-tion led a three-month enforcement and edu-cation effort at the San Ysidro Port of Entry to quantify the amount of cheese imported across the border and to provide information to border crossers regarding the health risks associated with queso fresco. During that pe-riod, >65,000 pounds of cheese were assessed, the majority of which were not labeled cor-rectly or being stored at safe temperatures (4).
Recently, the County of San Diego Public Health Services (PHS) Division in Health and Human Services Agency (HHSA) partnered with CDC to investigate the health risks from unpasteurized dairy products among His-panics in San Diego and Los Angeles Counties and to identify public health messages about queso fresco for populations at risk. Activi-ties included surveys of knowledge, attitudes, and behaviors, as well as focus group feed-back about queso fresco. Preliminary findings indicate participants frequently consumed dairy products brought from Mexico. Many did not have a clear understanding of the pas-teurization process and its association with cheese safety, or that bacterial contamination of queso fresco can lead to serious illness or miscarriage. Focus group participants indi-cated that physicians are a trusted source of information and food safety messages.
Clinicians are encouraged to recognize their value as reliable sources of food safety messages and address such concerns with their patients, especially groups at high risk (e.g., pregnant women, children, and persons who are immunocompromised). Many organ-isms can cause foodborne illness; clinicians should be alert to the potential for a foodborne etiology among such patients and perform di-agnostic testing. Suspected foodborne illness
By Eric McDonald, MD, MPH, and Karen Waters-Montijo, MPH
could this be making your
patients sick?
SOFT CHEESES FROM MExICO

SA N D I eGo P H YSI C I A N .o rG 25
The San Diego County Office of Border Healththe county office of border health facilitates communication and collaboration among local, state, and federal organizations working along the u.s.–mexico border region. since its creation in 1993, the office has worked on multiple endeavors, from participating in developing a cross-border laboratory specimen transfer protocol to setting up vaccination clinics in nontraditional settings to provide care for vulnerable populations during the 2009 influenza a (h1n1) pandemic and the 2010 pertussis epidemic. the office of border health and the epidemiology and immunization services branch share space at the county health services complex on rosecrans street in san diego. additionally, personnel from the centers for disease control and prevention’s u.s.–mexico unit are located in this facility.
Special Rates for
SDCMS Members
SEOIs Your Medical PracticeOn The Map?
Search Engine Optimization - SEO
888-423-9235
Your Practice Site
888-423-9235 All-in-One Solution For Your Medical Practice
Solution21Complete Marketing Solutions
www.solution21.com
Call Now for a FREE SEO Consultation
should be reported to the local health depart-ment; clinicians should anticipate that any person with foodborne illness might be part of a more widespread disease outbreak.
The Queso fresco Task ForceThe County Office of Border Health (see sidebar), within HHSA PHS, coordinates quarterly Queso fresco Task Force meetings. Established in 2003, the Task Force’s objec-tive is to share information, discuss strategy, and provide education to the public to reduce the adverse public health impact of unpas-teurized soft cheese commonly imported from Mexico. Member organizations repre-sent different government sectors (e.g., law enforcement, ports of entry, public health, border health, and food and agriculture). For more information on this topic, please con-tact Justine Kozo, chief of the Office of Border Health, at (619) 692-6656 or at [email protected].
Dr. Wooten, SDCMS-CMA member for the past nine years, is the San Diego County pub-lic health officer and has worked for the County of San Diego for 13 years. Dr. Adam is a CDC Epidemic Intelligence Service (EIS) officer, stationed with PHS. CDC’s EIS Program is a
two-year postgraduate program of service and training in applied epidemiology (additional information is available at www.cdc.gov/eis/index.html). Ms. Kozo has been the Chief of the Office of Border Health in HHSA/PHS for the past 2 1/2 years.
References:1. Kinde H, Mikolon A, Rodriguez-Lainz A, et
al. Recovery of Salmonella, Listeria mono-cytogenes, and Mycobacterium bovis from cheese entering the United States through a noncommercial land port of entry. J Food Prot. 2007; 1:47–52.
2. Thornton AJ, Waterman SH. Crossing bor-ders: unpasteurized cheese a public health challenge for Hispanic and US–Mexico binational communities. Clin Infect Dis. 2013; 57: v–vi.
3. CDC. Vital signs: Listeria illnesses, deaths, and outbreaks — United States, 2009–2011. MMWR Morbidity and Mortality Weekly Report. 2011 Jun 10;60(22):749-55.
4. Nguyen A, Cohen N, Hongjong G, et. Al. Knowledge, attitudes, and practices among border crossers during temporary enforcement of a formal entry requirement for Mexican-style soft cheeses, 2009. J Food Prot 2014; 77:1571–8.

26 N ov em b er 2014
TO SUBMIT A CLASSIFIeD AD, email Kyle lewis at [email protected]. SDcmS members place classified ads free of charge (excepting “Services offered” ads). Nonmembers pay $150 (100-word limit) per ad per month of insertion.
classifieds and time off scheduled from November 2014 through April 2015. Email: [email protected]. Phone: (760) 510-1808. Address: 334 Via Vera Cruz, Suite 257, San Marcos, CA 92078. [277]
LOOKING FOR A PART-TIME PHYSICIAN: Well-established (and growing) family prac-tice office centrally located in the Mission Valley area is looking for a part-time physi-cian to join their practice. Must have current licensure, be board certified, and have experi-ence in family medicine. The ideal candidate would be available to work three days a week, including some Saturdays and 1–2 evenings per week. Salary to be determined based on hours and productivity. Please send current CV to [email protected]. [276]
PHYSICIANS WANTED FOR OUR GROW-ING ORGANIZATION: Full, part-time, or per-diem flexible schedules available at loca-tions throughout San Diego. A national lead-er among community health centers, Fam-ily Health Centers of San Diego is a private, nonprofit community clinic organization that is an integral part of San Diego’s healthcare safety net. Since 1970, our mission has been to provide caring, affordable, high-quality healthcare and supportive services to every-one, with a special commitment to uninsured, low-income, and medically underserved per-sons. Every member of our team plays an important role in improving the health of our patients and community. We offer an excel-lent, comprehensive benefits package that includes malpractice coverage, NHSC loan repay eligibility, and much, much more! For more information, please call Anna Jameson at (619) 906-4591 or email [email protected]. If you would like to fax your CV, fax it to (619) 876-4426. For more information and to apply, visit our website and apply online at www.fhcsd.org [046]
PRIVATE PRACTICE, PART-TIME IM/FP OPPORTUNITY: Unusual and exceptionally attractive private practice, primary care op-portunity in beautiful North San Diego Coun-ty. Well-established, collegial, single-specialty internal medicine group with >30 years in the community, exceptional office staff, and very high quality patient care set this far apart from many other situations. Option for 1–2 days/week with flexible scheduling; very at-tractive opportunity as an add-on to other part-time work. Interested in board-certified IM or FP applicants with EHR experience. Please email CV to [email protected] or call (619) 248-2324. [263]
BOARD-CERTIFIED PHYSICIANS, PHYSI-CIAN ASSISTANTS, AND NURSE PRAC-TITIONERS NEEDED FOR URGENT CARE: Part-time positions available but a full-time opportunity may be offered to the right can-didate. Must possess a current California medical license and ACLS certification. Please email or fax CV to (619) 569-2590. Visit www.DoctorsExpressSanDiego.com for more infor-mation. [229a]
PRIMARY CARE JOB OPPORTUNITY: Home Physicians (www.thehousecalldocs.com) is
PHYSICIAN POSITIONS AVAILABLE
SUPERB INTERNAL MEDICINE OPPORTU-NITY: Internist (BC, BE) coastal North County available July 2015. Single specialty seven phy-sician internal medicine group, well established and respected. With 30 years in the commu-nity, outpatient care only, minimal call, salary guarantee, income well over median range for internal medicine. Send CV to [email protected] or call (760) 846-0464. [297]
MEDICAL WEIGHT CLINIC NEEDS PART-TIME MD: Doctors Weight Clinic has an open-ing for a part-time physician in two of our locations. We have been in business for over 40 years with eight clinics. We provide FDA-approved medication, injections, and diet counseling. If this is a medical service that you would be interested in, please contact Joyce Simpson at (619) 669-1808. [292]
GENERAL, FAMILY, OR INTERNAL MEDI-CINE PHYSICIAN NEEDED IMMEDIATELY: This opening is an independent contractor po-sition. We are a house call practice located in beautiful North San Diego County. We will also provide paid training on our EMR. 8–5 Mon-day–Friday, 10–12 patients per day and on-call pager 1 week every 3 weeks, telephone call only. No rounds or hospital duties. If interest-ed please submit your CV to [email protected]. We are very anxious to fill this position and we look forward to hearing from YOU! No agencies please. [286]
RECRUITING FOR A FULL-TIME FP OR IM PHYSICIAN: San Diego Family Care is recruit-ing for a full time family practice or internal medicine physician interested in working in a federally qualified community health center (FQHC) in the Linda Vista area of San Diego. The position requires at least a 32-hour/week commitment. Must be flexible and team ori-ented. May be required to work an evening or Saturday on occasion or, if preferred, could be part of regular scheduled rotation. Sal-ary commensurate with experience and great benefits. Requirements include current Cali-fornia and DEA licenses / CPR certification, plus good standing with respective board / association. Candidates may be eligible to ap-ply for federal loan repayment. If interested, please send CV to [email protected]. [284]
PRIMARY CARE PHYSICIAN (PART TIME) (URGENT CARE — PACIFIC BEACH): We are seeking a part-time primary care physician for a well-established, busy primary care family practice / urgent care medical practice located in Pacific Beach. The candidate must be able to provide compassionate care in a fast-paced environment. Knowledge of musculoskeletal medicine and X-Ray is required. Must be able to suture and have experience with wound care. We have a state-of-the-art medical facility. Please send your CV in confidence for consid-eration to [email protected]. Compensation: excellent pay rate. [278]
CARDIOLOGIST NEEDED: To cover busy outpatient practice for periodic vacations
a fast-growing group of house-call doctors. Great pay ($140–$220+K), flexible hours, choose your own days (full or part time). No ER call or inpatient duties required. Transpor-tation and personal assistant provided. Call Chris Hunt, MD, at (619) 992-5330 or email CV to [email protected]. Visit www.thehousecalldocs.com. [037]
PHYSICIANS NEEDED: Family medicine, pedi-atrics, and OB/GYN. Vista Community Clinic, a private nonprofit outpatient clinic serving the communities of North San Diego County, has opening for part-time, per-diem positions. Must have current CA and DEA licenses. Malpractice coverage provided. Bilingual English/Spanish preferred. Forward resume to [email protected] or fax to (760) 414-3702. Visit our website at www.vistacommunityclinic.org. EEO Employer/Vet/Disabled/AA [912]
SEEKING BOARD-CERTIFIED PEDIATRI-CIAN FOR PERMANENT FOUR-DAYS-PER-WEEK POSITION: Private practice in La Mesa seeks pediatrician four days per week on partnership track. Modern office setting with a reputation for outstanding patient satisfac-tion and retention for over 15 years. A dedicat-ed triage and education nurse takes routine patient calls off your hands, and team of eight staff provides attentive support allowing you to focus on direct, quality patient care. Clinic is 24–28 patients per eight-hour day, 1-in-3 call is minimal, rounding on newborns, and occasional admission, NO delivery standby or rushing out in the night. Benefits include tail-covered liability insurance, paid holidays/vacation/sick time, professional dues, health and dental insurance, uniforms, CME, budgets, disability and life insurance. Please contact Venk at (619) 504-5830 or at [email protected]. Salary $ 102–108,000 annually (equal to $130–135,000 full-time). [778]
PRACTICES FOR SALE
DERMATOLOGY SOLO PRACTICE FOR SALE: Mature physician is retiring December 2014 after practicing 36 years in coastal San Diego County on the campus of Scripps Me-morial Hospital, Encinitas, California 92024. Professional services provided have been medical dermatology and minor dermatologic surgery. Doctor has limited his patient base to original Medicare and fee for service. New owner could add managed care and cosmetic services if desired. Office space is leased from Scripps Real Estate. Turnkey sale could be ar-ranged. Reply to email [email protected] or cell phone (760) 666-0571. [275]
OFFICE SPACE AVAILABLE
AVAILABLE IMMEDIATELY: 14ft x 12ft sunny room in a four-room office suite shared by a physician, several chiropractors, and an acu-puncturist. Located upstairs in Cardiff Town Center at the corner of San Elijo Avenue and Birmingham Drive one-half mile off I-5 and across Coast Highway 101 from San Elijo State Beach. Take advantage of Seaside Market, nu-merous restaurants, a post office, and a public library either onsite or across the street. Call (760) 436-7464. [294]
WOMEN’S HEALTH / WELLNESS OFFICE HAS SPACE AVAILABLE FOR SUBLEASE: Exam room, office, and/or shared staff op-tional. Fully furnished exam rooms available and ready for use. Location features onsite

SA N D I eGo P H YSI C I A N .o rG 27
Place your
ad here Contact Dari Pebdani
at 858-231-1231 or [email protected]
and hardwood floors. Full Ultrasound lab with tech on site, doubles as procedure room. Will sublease partial suite, one or two exam rooms, half or full day. Will consider subleasing the entire suite, totally furnished, if there is a larger group interest. Plenty of free parking. For more information, call Irene at (619) 840-2400 or at (858) 452-0306. [153]
POWAY OFFICE SPACE FOR SUBLEASE: Private exam room or rooms available for one day a week or more. Ideal for physician, chiro-practor, massage therapist. Low rates. Email inquiries to [email protected]. [173]
POWAY / RANCHO BERNARDO — OFFICE FOR SUBLEASE: Spacious, beautiful, newly renovated, 1,467SF furnished suite, on the ground floor, next to main entrance, in a busy class A medical building (Gateway), next to Pomerado Hospital, with three exam rooms, fourth large doctor’s office. Ample parking. Lab and radiology onsite. Ideal sublease / sat-ellite location, flexible days of the week. Con-tact Nerin at the office at (858) 521-0806 or at [email protected]. [873]
BUILD TO SUIT: Up to 1,900SF office space on University Avenue in vibrant La Mesa / East San Diego, across from the Joan Kroc Center. Next door to busy pediatrics practice, ideal for medical, dental, optometry, lab, radiology, or ancillary services. Comes with 12 assigned, gated parking spaces, dual restrooms, server room, lighted tower sign. Build-out allowance to $20,000 for 4–5 year lease. $3,700 per month gross (no extras), negotiable. Contact [email protected] or (619) 504-5830. [835]
SHARE OFFICE SPACE IN LA MESA JUST OFF OF LA MESA BLVD: Two exam rooms and one minor OR room with potential to share other exam rooms in building. Medi-care certified ambulatory surgery center next door. Minutes from Sharp Grossmont Hospital. Very reasonable rent. Please email [email protected] for more information. [867]
NONPHYSICIAN POSITIONS AVAILABLE
SEEKING NURSE PRACTITIONER: Internal medicine, part-time position available. Seek-ing nurse practitioner with primary care and EHR experience. Private practice located in beautiful North San Diego County, single specialty group, collegial work environment. Please contact (619) 248-2324 or email re-sume to [email protected]. [296]
PA NEEDED FOR DERMATOLOGY AND COS-METIC SURGERY PRACTICE IN ENCINITAS: Experience in general dermatology a must! Applicant must be knowledgeable in diagnos-ing and treating common dermatologic condi-tions, possess excellent interpersonal skills, be a caring and empathetic provider, and possess the highest of ethical standards. Being a team player and having a positive attitude is essen-tial for success! Please send your CV and salary history to [email protected]. We look forward to hearing from you! [290]
SEEKING PA / NP AND RN: Medical spa in the Del Mar / Solana Beach area is seeking PA / NP and RN. Should have experience with laser hair removal, IPL, CO2 laser, Botox and fillers, and sales. Positive attitude, ability to multitask, perform patient treatment, sales, consultations, effective communicator, work in a team environment, focused on client care,
billing, reception, medical assistants, poten-tial use of in-office procedure room, and a rooftop lounge. If you are interested, please reply with the heading “Space for Sublease” outlining the details of space and/or staff use desired, with your contact information, and we will contact you to set up a showing. Reply to Mrs. Kim at [email protected]. [288]
LA JOLLA (NEAR UTC) OFFICE FOR SUB-LEASE OR TO SHARE: Scripps Memorial medi-cal office building, 9834 Genesee Ave. — great location by the front of the main entrance of the hospital between I-5 and I-805. Multidisciplinary group. Excellent referral base in the office and on the hospital campus. Please call (858) 455-7535 or (858) 320-0525 and ask for the secre-tary, Sandy. [127]
3998 VISTA WAY, IN OCEANSIDE: Four medi-cal office spaces approximately 1,300–2,800SF available for lease. Close proximity to Tri-City Hospital with pedestrian walkway connected to parking lot of hospital, and ground-floor access. Lease price: $1.75+NNN. Tenant improvement al-lowance to customize the suites is available. For further information, please contact Lucia Sham-shoian at (760) 931-1134, ext. 13, or at [email protected]. [234]
SPACE AVAILABLE FOR BOARD-CERTIFIED INTERNIST interested in developing an East County practice. Contact Debbie at [email protected] or at (619) 287-7991. [283]
BANKERS HILL PRIMARY CARE / HEALTH-CARE PROFESSIONAL & RESEARCH OFFICE SPACE TO SUBLEASE: 50-year established primary care practice and clinical research of-fice, with currently two internists, have space to sublease to another primary care or prima-ry care / subspecialist, or other independent healthcare professional, to help curb overhead and, if primary care, help with acute overflow patients’ needs. Also can provide opportunity to get into clinical research. Contact Jeff at [email protected]. [265]
DEL MAR / CARMEL VALLEY MEDICAL OF-FICE FOR SUB-LEASE: Available October 2014 (4765 Carmel Mountain Rd., San Diego, CA 92130). 1,000SF. Two treatment / consul-tation rooms / office reception / photography room / break room. Unlimited patient free parking. Call (858) 481-4888 or email [email protected]. [252]
SCRIPPS XIMED MEDICAL CENTER BLDG, LA JOLLA — OFFICE SPACE TO SUBLEASE AVAILABLE: Vascular & General Surgeons have space available. One room consult office available, with one or two exam rooms, to a physician or team. Located on the campus of Scripps Memorial Hospital, The Scripps Ximed Medical Center is the office space location of choice for anyone seeking a presence in the La Jolla/UTC area. Reception and staff may be available. Complete ultrasound lab on site for scans or studies. Full-day or half-day timeslots. For more information, call Irene at (619) 840-2400. [154]
NORTH COAST HEALTH CENTER, 477 EL CAMINO REAL, ENCINITAS, OFFICE SPACE TO SUBLEASE: Well-designed office space available, 2,100SF, at the 477-D Bldg. Occupied by Vascular & General Surgeons. Excellent and central location at this large medical center. Nice third-floor window views, all new exam tables, equipment, furniture,
knowledge of lasers and laser theory, quick learner, self motivated. PA/NP will perform consultations and good faith examinations. Minimum requirements: PA, NP, RN California license. This is a part-time position, 1–2 days a week. Please email résumé / cover letter to [email protected] or fax to (858) 259-0864. [289]
NURSE PRACTITIONERS WANTED FOR OUR GROWING ORGANIZATION: See ad #046 un-der “PHYSICIAN POSITIONS AVAILABLE.”
BOARD-CERTIFIED PHYSICIANS, PHYSI-CIAN ASSISTANTS, AND NURSE PRAC-TITIONERS NEEDED FOR URGENT CARE: Part-time positions available but a full-time opportunity may be offered to the right can-didate. Must possess a current California medical license and ACLS certification. Please email or fax CV to (619) 569-2590. Visit www.DoctorsExpressSanDiego.com for more infor-mation. [229b]
NURSE PRACTITIONER: Needed for house-call physician in San Diego. Full-time, competi-tive benefits package and salary. Call (619) 992-5330 or email [email protected]. Visit www.thehousecalldocs.com. [152]
PHYSICIAN ASSISTANT OR NURSE PRAC-TITIONER: Needed for house-call physician San Diego. Part-time, flexible days / hours. Competitive compensation. Call (619) 992-5330 or email [email protected]. Visit www.thehousecalldocs.com. [038]
NONPHYSICIAN POSITIONS WANTED
RECENTLY GRADUATED CERTIFIED MEDI-CAL ASSISTANT SEEKS PART-TIME PO-SITION IN NORTH COUNTY SAN DIEGO: Experienced in wound care, plastic surgery, or-thopedics, surgical settings. Very knowledge-able, hard-working, dependable, team player, superb patient rapport, willing and eager to learn. Special interests in surgical setting or urgent care. Available afternoons or nights. Excellent references! Contact Carol at (442) 444-0621 or at [email protected]. [293]
MEDICAL EQUIPMENT
PHYSICAL THERAPY EQUIPMENT FOR SALE: Recently closed PT clinic is selling all existing equipment, therapy tables, supplies. Please email [email protected] if you are inter-ested. [291]

28 N ov em b er 2014
Work-life balance is on the minds of many physicians, as we struggle with increasing data entry, insurance report-ing requirements, and the ever-increasing knowledge we need to acquire and integrate into our practices. A Google search of “work-life balance” yields 150,000,000 entries. It’s clear that we haven’t found the answer to this dilemma! This is partly because we mistak-enly imagine that “balance” is a state of perfect equilibrium, rather than a dynamic state requiring frequent assessment of changing priorities and shifts in our activities based on those changes. Another reason balance seems elusive is that, as Jack Welch, the success-
personal & professional development
we must disappoint.The commonality of
concerns was striking — one primary care physician was surprised that specialists felt the same stress she did. This realization enhances our sense of community, diminishes our isolation, and increases our compassion for our colleagues. Another physician appreciated the guided meditation and will perhaps add this to his busy life. Meditation, or any form of mindfulness practice, has been shown to positively impact productivity and performance, decrease stress and burnout, and build resilience. Partici-pants also saw that significant shifts begin with small transi-tions and were encouraged to pick one or two changes to start. Most appreciated taking three hours to look at their lives in a safe environment in which to voice concerns and frustra-tions, where the emphasis was not on continuing to feel like a victim but on finding op-portunities for taking charge and wielding the power that we each have to create lives of greater fulfillment. Given the success of the workshop, SDCMS plans to offer it again in 2015. Look for the announce-ment in “News You Can Use” in the next few months.
Dr. Fronek, SDCMS-CMA member since 2010, is as-sistant clinical professor of
medicine at UC San Diego School of Medicine and a certified phy-sician development coach who works with physicians to gain more power in their lives and create lives of greater joy. Read her blog at helanefronekmd.wordpress.com.
ful former CEO of General Electric, likes to say, there is no such thing as work-life balance — there are work-life choices, and each choice has consequences. This places the responsibility and the power directly in our court.
For this reason, the partici-pants in SDCMS’ workshop on Work-Life Balance this past Oct. 11 began with a guided meditation to create a vision of what their balanced life would be like, and how they would be different in that ideal life. Participants noticed a variety of activities that they yearned for and found a greater sense of peace and choice in these lives, signaling the direction of the change they were seeking. This
Work-life choices
What are yours?by Helane Fronek, MD, FACP, FACPh
There is no such thing as work-life balance — there are work-life choices, and each choice has consequences.
was followed by activities to discover what creates balance — our true values — those prin-ciples or activities that make life worth living and make it our life and not someone else’s. We are often surprised at what creates the most precious events of our lives — the awe of nature, our empowerment of others, completion of a difficult task. It’s sobering to realize that these values are no longer showing up in our lives as frequently as we would like. We finished with a series of tools to help us create the lives we yearn for: communication skills, a protocol to delegate effectively, and comfortable ways to say “no” that honor our values while showing respect to those

Success.
Are You ICD-10 Ready? Get Your “ICD-10 Action Guide” FREE!
Since 1977, the Cooperative of American Physicians (CAP) has provided superior medical professional liability coverage and valuable risk and practice management programs to California’s finest physicians through its Mutual Protection Trust (MPT).
As a physician-directed organization, we understand the realities of running a medical practice these days, and are committed to supporting you with a range of programs and services that no other professional liability company offers. These include a 24-hour early intervention program, HR support, EHR consultation, a HIPAA hotline, and a robust group purchasing program, to name a few.
It’s what California’s finest physicians strive for. . .and what CAP can help you achieve.
On October 15, 2015, all medical practices must comply with new, expanded ICD-10 codes. CAP’s ICD-10 Action
Guide for Medical Practices has the answers you need to successfully make the transition.
Request your free electronic or hard copy today!
800-356-5672 CAPphysicians.com/icd10now
San Diego County Medical Society5575 Ruffin Road, Suite 250San Diego, Ca 92123
[ Return Service Requested ]
$5.95 | www.SAnDIeGOPhYSICIAn.org
1.5 tesla MRI.Make sure you’re covered.
a leaking fire suppression
system destroyed a $1,000,000
In a Los Angeles radiology practice,
For decades, The Doctors Company has provided the highest-quality medical malpractice insurance. Now, the professionals of The Doctors Company Insurance Services offer the expertise to protect your practice from risks beyond malpractice. From slips and falls to emerging threats in cyber security—and everything in between. We seek out all the best coverage at the most competitive prices. So talk to us today and see how helpful our experts can be in preparing your practice for the risks it faces right now—and those that may be right around the corner.
n Medical Malpracticen Workers’ Compensationn Health and Disabilityn Property and General Liability
n Employment Practices Liabilityn Directors and Officers/Management Liabilityn Errors and Omissions Liabilityn Billing Errors and Omissions Liability
Call our Los Angeles office at (800) 852-8872 today for a quote or a complimentary insurance assessment.
www.thedoctors.com/TDCISCA License #0677182
4082_CA_SanDiegoPhysician_Aug2013.indd 1 7/1/13 3:15 PM