nrf-gc.orgnrf-gc.org/.../2016/...3-macro-micro-of-four-brain-system… · web...
TRANSCRIPT

Review of Chapter Eight
A. Reminding ourselves of the shame factorB. Sharing our personal journal (rotating through class participants)
a. Who you are at your Best (green zone – Heart/Hand/Head)b. Who you are at your Worst (red-Hand/blue-Head/combo-Head)c. Dyadic patterns from your past family (mom/dad)d. Patterns from past to present, similarities? Differences? e. Individual Toxic Stress Patternsf. Relational Toxic Stress Patterns g. Professional dyadic stress patterns, Rupture? Repair?
C. Sharing our families a. Early Phase Assessment Form AWAKE Cycles
i. PIESii. Check boxes
iii. Toxic Stress Patternsiv. Integrating Colors with HHHv. Parallel Process
b. Graphical Displays i. PIES
ii. Toxic Stress Patternsiii. Sleep
Chapter Nine, Phase 1, Step 3: Macro and Micro Approach to the Four Brain Systems, the Four Stories and the Use of the History Worksheet and Needs Assessment
ORIENTATION TO GLOBAL CONCEPTS FOR STEP THREE
Branches to the tree. The metaphor for step three is the branches to the tree. Now, the strengths of the roots and the trunk feed into building healthy branches or there are needs that have been gathered along the way from toxic stress at the root level and poor serve and return relational processes in the trunk. Organically, the branches are a result of both the genetics and the environment – the dynamics (epigenetics) of the two interacting, beginning with the in utero environment.
1

The links between the three steps. Step One informs you if there is a toxic stress pattern that needs to be addressed. Physiological stability is the foundation to the Levels of Engagement. If there is a toxic stress pattern in an individual, dyad, or family system, there is vulnerability or constrictions in Step Two as well, that also need support. While Step One and Two inform you this family needs help, neither step one nor does step two inform you as to what all the multiple causes are that are contributing to the vulnerabilities. That is for Step Three to do! Step Three is a comprehensive approach to assessment (and intervention) that helps you organize the individual differences in each person in the family system, in a neuro-developmentally sensitive manner. As this information is gathered with the parents, the strengths and needs become a guide for use within the family. This information helps inform the parents what they can do for themselves and their children. The four brain systems also help the practitioner and parents organize all of the services they may already be receiving, as well as highlight any pieces that might be missing, so that these can be discussed collaboratively.
Multiple Uses of the Four Brain Systems. There are many layers to the use of the four brain systems. While each part of the tree has depth and breadth to it, the four brain systems are the most rich and multi-faceted. These layers can be thought of as a way to think about parallel process!
First, on a preliminary level, if you have other practitioners on your team that have been gathering information from the family, and they are free to share it with you, you can use the four brain systems to begin to organize the information you’ve gotten, right from the start. The History Worksheet is something that all practitioners across teams can share.
2

Second, the four brain systems serve as four stories. These consist of interviews that can be done in a concentrated way with a semi-structured interview or over the course of time. As one already knows, the four stories are ever emerging and ever evolving. One begins, yet, as the NRF is like a spiral staircase, one can cycle back at any time to a piece of history or knowledge that may have been hidden.
Third, the four brain systems are a way to begin to understand the global strengths and vulnerabilities of each brain network via looking at risk and protective factors. As one begins and continues to fill in the History Worksheet, the sheer numbers of risk factors can be counted to see where the strengths and vulnerabilities are weighted. In general, we say that a score of four or more is a weight that one carries within that brain system. As there are many risk factors, including the Adverse Childhood Experiences, one can see things from a Micro perspective. As we stand back and observe the sheer numbers of risk factors within each brain network, and where things are balanced or imbalanced with strengths, we shift back out the Macro level.
Fourth, they can be used to understand the families’ global needs and where in your community the resources are –including where your personal warm hand-offs are and where you need to forge new connections. This begins to look at the Macro level of community systems work. Both the Purple Wheel and the Family and Community Needs Assessment are used for looking at the big picture. What team members might you need for this case/family? Whom do you know in each of these areas of need? Whom might you want to form a connection with for future reference?
Following the global interviews of the four stories and using the History Worksheet to look at the strengths and vulnerabilities, one begins to go deeper into the four brain systems. The NRF has organized functional capacities within each brain network so that individual differences in each brain system can be assessed. The following items reflect the details of this micro level depth analysis.
Fifth, assessing functional capacities within each brain system help you take a closer look at the health or distress within a network, helping you identify and plan for services that may be needed for remediation.
Sixth, the brain systems have intervention principles embedded in them all along the way, and they are integrated into the understanding of the functional capacities.
Seventh, as each brain system’s strengths and vulnerabilities are processed, each brain system can be a guide for the cumulative, yet distributed sources of Triggers that contribute to adaptive and toxic stress response and toolkits for stress recovery. The Toolkits can be discovered on the self-regulatory side and the co-regulatory side. The process and concept of using Triggers and Toolkits can begin early on in the learning process of using the four brain systems. However, the mastery and depth of mining the four brain system for triggers and toolkits comes with the depth of these previous layers of knowledge.
Eighth, one goes back out the larger picture, revisiting looking at a community from a Macro point of view, with its systemic and leadership links – within a local area, across a state, and across state leadership lines.
3

Ninth, they are ways that we can evaluate on a meta-level, where any promising practice or evidence-based treatment is “weighted” from a neurodevelopmental landscape, so they can more judiciously be used for matching the treatment to the needs of the parents/child/family.
Layers to the Use of the Four Brain Systems & Links to Phases and WorksheetsLEARNING PHASE 1
First level A way to organize any preliminary data collected and shared with you
Phase 1 History Worksheet
Second level Four stories that are interviews in concentrated form or spread out over time
Phase 1 Four Interviews
Third level Organizes risk and protective factors, count the number of risk factors
Phase 1 History Worksheet
Fourth level Organizes individual needs and warm handoff links practitioners have or do not have in the community
Phase 1 Purple WheelFamily and Community Needs Assessment
LEARNING PHASE 2Fifth level Assesses functional capacities within each brain
system that show strengths, vulnerabilities, or often both
Phase 2 Current Functional Capacities
Sixth level Use intervention principles embedded within the four brain systems
Through all phases
In text, references to bottom-up and top-down processes
Seventh level Organizes Individualized Triggers and Toolkits for stress responses and stress recovery
Phase 2 Brain System Triggers and Toolkits
Eighth level Provides macro level view of cross-sectored links within a community, across systems of care on a state level, or national level
Phase 2 Purple WheelYellow CircleBronfenbrenner’s Layers
LEARNING PHASE 3Ninth level Meta-level map for where promising practices
and evidence based treatments are “weighted” from a neurodevelopmental perspective for matching treatments with needs
Phase 1 & 2
Material Introduced in NRF Chapter 9 & 11
GENERAL ORIENTATION TO THE FOUR BRAIN SYSTEMS, MACRO AND MICRO USE
As already mentioned, there are many uses of the four brain systems. In this Phase, I am orienting you to the use of them as a way to begin, right away, to organize individual differences in a comprehensive, yet organized and systematic fashion. This is referred to as the Micro level of using the four brain systems for individual organization. Second, I am orienting you to the four brain systems as a way to organize your family’s use of all of the community systems of care. This shift helps you look at the larger picture and begins your journey as a practitioner who is interested in holding in mind the larger picture, seeing your sector as part of a larger whole. A family in need can enter through any one of the five sectors we hold in mind. Organizing care through the four brain systems, and using a common language and shared approach with the NRF’s three steps, provides an avenue for a more efficient and effective way to service our most at-risk infants and at-risk parents.
4

Orientation to bottom-up and top-down processes. Our brains are built “bottom-up” and while there is a linear progression to the brain’s development there is also a non-linear aspect to it. So, we usually think of the first couple years of life as particularly “bottom-up” because we are primarily “doing” and not “thinking” yet it is now clear that these dual tiers have a lot of intersections and influences upon each other. So, it’s not as neat and tidy as it sounds. As we develop, many behaviors are a combination of both bottom-up and top-down processes. In order to get clear on the distinctions, though, bottom-up processes are behaviors that are habitual and automatic. We do to have to talk or think about them to do them. In contrast, top-down processes are ones that are deliberate and intentional, often requiring conscious control. These require thinking and sometimes, talking. When the environment is predictable, we benefit from having fixed and automatic habits and routines in place. It would be very time consuming if every time you went to make breakfast you had to read a manual on how to do it. It’s efficient to know how to get ready for school or work through these rather rote routines. At the same time, life is also unpredictable. For these instances, we need to be able to respond to novelty with thought and flexibility. This takes more energy to do! Thus, the balance of the two is optimal. An automatic system and a thinking system are each necessary and complimentary to each other. (Deborah Budding, 2015)
Many ways of learning require bottom-up processes the NRF references as procedural learning and that is why if you are taking an NRF course, there are usually procedural learning exercises embedded in the training programs. BTW, procedural knowledge and memories are akin to “implicit” knowledge and memories. When on the ski slopes learning how to ski, one has to think but one is also doing. This means that one learns how to become “automatic” with the use of the NRF through using it and doing the exercises. When learning the NRF, one has to both do and think, very taxing indeed! However, just as learning any routine or filling out a particular paper trail, it takes practice. Over time, the practice becomes procedural and at that point, will have a lot of automaticity built in. That means you won’t have to think so hard just to get through an intake or an Early Assessment Phase Form! That gives you more energy to deal with more complex cases and curve balls that come your way.
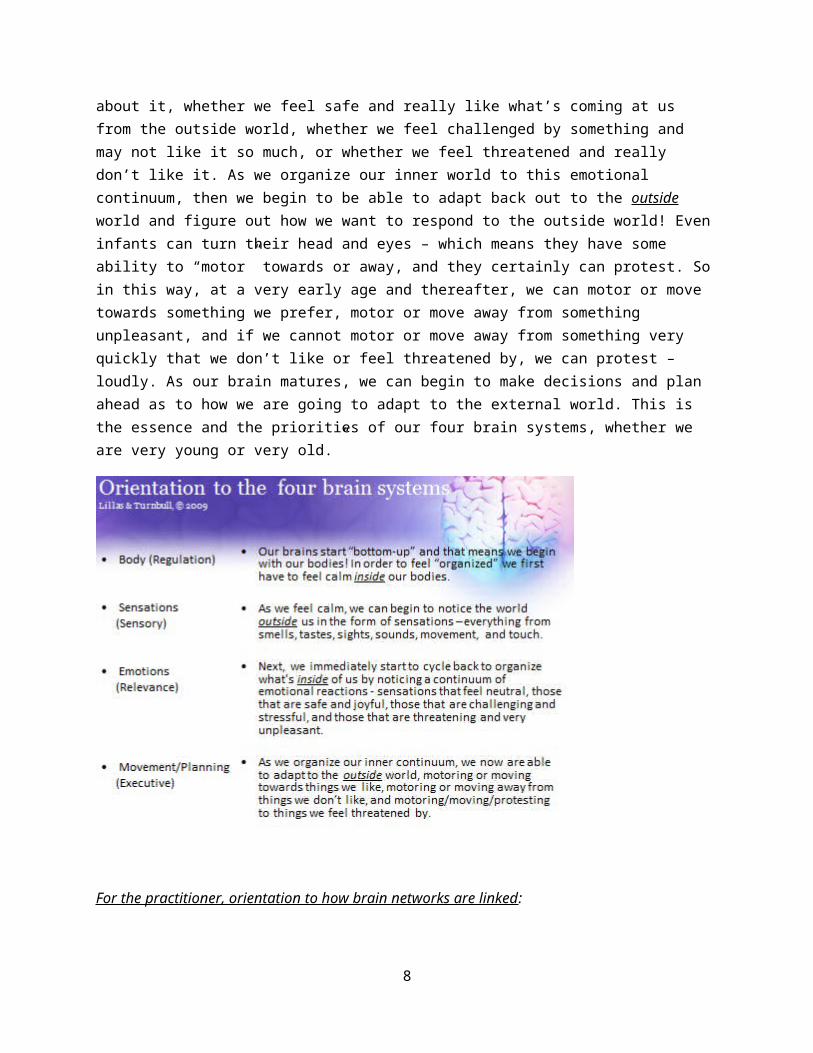
Micro level understanding of the four brain systems. The simplest way of understanding the four brain systems is often a way I might also orient a family to them or a new practitioner to the NRF. Notice that as the meaning of each brain system is told, there is a movement from the inside to the outside, back to the inside, back to the outside. So, we are moving in and out of our connections to our “internal milieu” –known our bodies, with connections to our “external milieu” –known as our outside world.
“Our brains begin “bottom-up” and that means we begin with connecting to our bodies! And in order to be at our best, we have to get calm inside our bodies to feel relaxed and present. Our infants and young children have to do this, too! As we get calm inside our bodies, we can begin to notice what’s going on outside of us. We start to notice the world around us in the form of sensations –everything from smells, tastes, sights, sounds, movement, and touch. Now, what happens next is that we immediately start to cycle back to organize what’s inside of us by noticing a continuum of emotional reactions - whether we feel neutral about something, not really registering it or caring too much about it, whether we feel safe and really like what’s coming at us from the outside world, whether we feel challenged by something and may not like it so much, or whether we feel threatened and really don’t like it. As we organize our
5
inner world to this emotional continuum, then we begin to be able to adapt back out to the outside world and figure out how we want to respond to the outside world! Even infants can turn their head and eyes – which means they have some ability to “motor” towards or away, and they certainly can protest. So in this way, at a very early age and thereafter, we can motor or move towards something we prefer, motor or move away from something unpleasant, and if we cannot motor or move away from something very quickly that we don’t like or feel threatened by, we can protest – loudly. As our brain matures, we can begin to make decisions and plan ahead as to how we are going to adapt to the external world. This is the essence and the priorities of our four brain systems, whether we are very young or very old.”
For the practitioner, orientation to how brain networks are linked:
What we’ve just walked through is one way to understand how the brain systems are linked. There are other ways as well. From this point of view, you can see in the depiction below, that the regulation and relevance systems have a lot of links to our bodies. For future reference, this is why Step One, which is our seven states of arousal and the physiology of our autonomic nervous system, which has links to all of our internal organs, covers a lot of territory in the functional behaviors for the regulation and relevance system. You can also see in the depiction below, that the sensory and executive systems have a lot of links to the outside world. Together, they are the “sensory-motor” feedback loop in taking information from the world, with how we then respond and adapt to the external world. Of course, all of these brain systems interact with each other and influence each other.
6

For the practitioner, orientation behaviors within each brain system:
As a practitioner, it’s also important to now understand that there are certain behaviors that we associate with each brain system. These multiple ways of looking at behavior allows us to be comprehensive in understanding the meaning of behavior from various lenses.
For the Regulation System, the behaviors are focused upon the 24-hour sleep-awake cycle which you are quite familiar with from Step One. As you get to know the functional capacities in the Regulation System in Phase2 you will see that you know most of them already because of the work you’ve done in Step One. The one functional capacity that is not directly related to the stress response and stress recovery process already introduced to you, is the connection one has to his or her “visceral” self. This is our link to our “interoceptive” system of sensations from inside our bodies that is further discussed in the Sensory System.
For the Sensory System, these are the behavioral reactions to all sources of sensory information that we are observant of and assessing. The focus here is on the reactions to the sensory information coming at us from the outside world, as mentioned above. However, there are subtleties that need to be noted. First, two extra sensations to our usual “external” sources of information are included in the sensory list – proprioception and vestibular. Proprioception is the input and pressure we receive on our joints and muscles. We receive passive proprioception through massage. We receive active proprioceptive input by any type of active input into our joints and muscles such as through walking, running, and jumping. Vestibular input is what we receive through our inner ears with any movement of our bodies. This is our inner balance and we are very aware of losing our vestibular stability when we get dizzy.
Secondly, sensory information we receive from inside our bodies such as pain, temperature, itch, sensual touch, and information from our internal organs – is referred to as “interoception” (ref, www.ncbi.nim.nih.gov/pubmed/12965300). The placement of “interoception” has its own functional
7
capacity in the Regulation System, due to its link with the inside of our bodies, connected to what is referred to as one’s “visceral self”. However, some NRF materials and practitioners will place both the internal and external reactions to sensations in the sensory system. Just be aware of this when communicating with other practitioners.
For the Relevance System, the behavioral links are oriented to the range of emotions and subsequent memories one builds upon over time. These two, combined, organize our meaning-making system. As an emotional continuum was mentioned in terms of experiencing the sensory world with degrees of neutrality, safety, challenge, and threat, health is defined as a balance towards a full range of positively and negatively valenced emotions, wherein the balance of safety, challenge, and threat is weighted towards adaptive stress versus toxic stress. The “relevance” system was named as such because the behaviors here pertain to what is emotionally “relevant” and meaningful to us. As we saw in the introduction to the four brain systems, our emotional reactions to sensations organize our internal worlds. These memories include “procedural” reactions that have become automatic for us without thinking, from our bottom-up capacities, and later (two to three years old on up), declarative memories that we have access to through our conscious thoughts from our top-down capacities. How we then appraise the world and ourselves emerge from our emotional histories and the quality of engagement with others.
For the Executive System, as was mentioned earlier, we begin in infancy from the bottom-up side of life to make behavioral links with movement. We can make movements towards things we love, move away from things we do not, and protest against what is dangerous to us. Again, these early movements become procedural and automatic reactions towards our external world, and organize how we adapt to it, closely linked to our relevance system. The executive system is a master juggler, receiving information from all of the other brain systems. As we develop more advanced capacities for movement and conscious thought, we have more capacities to both shift and inhibit (three years old on up) our actions, thoughts, and feelings. We can more elegantly plan ahead and make better choices as to how we adapt to our external world by making intentional decisions to move towards, away, or against experiences that arise. We have more control as to when to stay steady and on task (inhibit and sustain) and when to shift and respond to something new in our context (shift and initiate). The goal again, is to have a balance between these dynamics.
8

Macro level understanding of the four brain systems.
The four stories and the functional behaviors within each brain system link up with now with systems of care that each have a range of diagnostic categories that they pay for. The NRF’s purple wheel is the picture often used to show these links. What is located inside the wheel are examples of functional behaviors or dynamics that are weighted towards this network that you were oriented to in this last section on the Micro level understanding of the four brain systems. What is located outside the wheel are the large systems of care that often are the one’s paying for the diagnostic categories associated with that system. The primary details organized within each brain system correlate with the unfolding of the Four Stories Interview, so they are presented to you in the section on the Engaging Parents with the Four Stories.
There are four Macro level ways of understanding the four brain systems. The NRF uses the term “weighted” to connote that there are propensities of an element whose properties are pulled towards a certain brain system. First, we will see what systems of care each brain system links up to, which will be linked with what is referred to as a The Purple Wheel. Second, where diagnostic categories are weighted within each brain system and what typically each sector pays for will be represented in a picture. Third, where disciplines are weighted within each brain system and what brain system and sector they typically work within will be depicted. Fourth, where treatment practices are weighted according to the brain system will be shown. These pictures allow you to get a Macro level view of the how the four brain systems serve us on a meta-level, giving us a link to community sectors, organizing for us diagnostic categories that are used for intervention, understanding our disciplinary matches for team building, and
9

organizing treatment perspectives that help us find matches with our family’s needs. Further details of what risk factors are within the four brain systems on a “micro” level will be covered in the section on the four story interviews and you will see in the History Worksheet.
The Regulation System is dedicated to assessing for basic needs and medical conditions, including genetic disorders. Anything that occurred during the in utero experience and any ongoing medical concerns for both the parent and child belong here. The Sensory System is dedicated to any early developmental delays and disabilities that arise. In the United States, this system is referred to as the Early Intervention, Part C funding source. The Relevance System is dedicated to the mental health needs of our families. Of course, infant mental health (IMH) that is in particular, developmental and relationship-based, is the vantage point the NRF brings to the mental health system of care. Since IMH is inter- and trans-disciplinary, the socio-emotional, relational, and mental health needs are not seen as discipline specific to mental health licenses, but essential to be distributed across all disciplines and systems of care. The Executive System is dedicated to the early care and education needs of our infants, young children, and families. Learning needs for the age-range are also viewed through developmental, relationship-based, and play-based lenses. The Child Welfare System is dedicated to working with families with abuse and neglect histories. The NRF places this system in the center of the wheel because most often, these infants and young children are involved and have needs all around this wheel. When we have a NRF community that includes child welfare, this is an awesome opportunity to build cross-sectored links with all the other systems of care that so often interface with our infants, young children, and their families. Notice that the center of the wheel includes the phrase, “prevention to detention”. The prevention teams related to child welfare are often not linked with the detention teams and even the transfer over from one system to the next is not a smooth transition. By having a common language and shared approach, these links can be improved.
10

As we know, infants, young children, and parents can enter into any one of these ports of entry. And many times, they get “lost” within a system of care and the infant, young child, or parent is only understood through this particular lens. Recall the metaphor from Chapter one as each sector or discipline can view themselves as the whole pie, rather than a piece of the pie. The Macro level goal of NRF communities is to create the links that are currently not established, so that the fragmentation is greatly reduced or eliminated.
Where diagnostic categories are weighted.
The Regulation system is weighted towards medical diagnoses, anything related to the sleep-awake cycle, and the early phase of that first year of life. Feeding, sleeping, and elimination issues are part of the core visceral self and important issues to pick up if there are concerns.
The Sensory system as linked to the Early Intervention Part C resource has typically funded speech and language delays, motor delays, and sensory processing delays up until three years of age. The larger diagnostic catchment areas they focus upon and will stay engaged with for a lifetime are Autism, epilepsy, cerebral palsy, and intellectual disabilities. These four areas definitely overlap with the medical community, so these are shared with the Regulation system. The funding sources in the United States are bifurcated at age three. Thus, there is a birth to three funding source and then a three to five year old funding source. The handoff from Early Intervention funds is to the School Districts. This is often a vulnerable space to negotiate. Often services drop off and then have to be re-visited through an IEP process with the school district. Sometimes there are rather seamless transitions where providers have worked out a system of coordination between the two funding systems.
The diagnostic label of Sensory Processing Disorder (SPD) has emerged within the sciences to be a valid diagnosis. While it’s considered to be an organic part of most youth diagnosed with Autism, it recently was established as a stand-alone diagnosis that can be separated from the Autism, [xxxxUSSF}. Despite this research, it did not make it into the DSM V that came out in May, 2013. The Diagnostic Classification System for 0-5 year olds, discussed next, did include it in their Axis I of diagnostic conditions.
As a note, any auditory-verbal or visual-spatial processing difficulties, are the origins of Learning Disabilities, that often overlap with one’s Executive System. This is another way that the Sensory/Executive systems have a lot of interconnections with each other.
The Relevance system linked with the mental health community focuses upon mental health diagnostic categories. A few are listed in the diagram below. The Diagnostic Classification System for birth to three year olds, and more recently for birth to five year olds [DC: 0-3R (xxxx) and the DC: 0-5 (xxxx)] have been developed by the national organization Zero To Three. Their approach is to identify concerns that have to do with infants in a much more nuanced manner, and later cross-walked with the DSM for billing purposes.
The Executive system, first of all, is linked with the motor capacities, so this is the bottom-up side to this brain system. Often, Part C is the funder for motor delays, so there is overlap in this regard with the
11

sensory system. A prominent diagnostic category in the executive system is ADD or ADHD. From the NRF’s perspective, everything else needs to be ruled-out before this diagnosis is given because inattention and hyperactivity can mean more than one thing! An experienced psychologist or neuropsychologist is often skilled at looking all the full diagnostic landscape and making this definitive diagnosis. At the same time, this diagnosis is often given by pediatricians and physicians, so this overlaps with the medical community.
As mentioned in Chapter One, these diagnostic categories are necessary and useful for funding services. However, what’s implied in this diagram is that all diagnostic categories need to be understood from the underlying dimensions of the four brain systems. We now know that the categorization of symptoms, as the DSM has done, is no longer an adequate way of understanding behavior.
Where disciplines are weighted.
Regulation: Community social workers that assist with finding resources for basic needs and physicians, nurses, and any early year practitioners are included in this brain system.
Sensory: Anyone working with early delays in speech and language, motor, and sensory domains is included in this system. Auditory and visual processing disorders originate in this brain system, so those working with auditory and visual processing delays reside here. The arenas of “processing” disorders continue to be developed. While the early origins of these can sometimes be picked up, these are
12
diagnosed later, usually in early latency, although some developmental optometrists work with younger children as well. Due to the many “auditory processing” programs that exist for some type of remediation, I often refer to an audiologist in order to sort out which actually are targeted to the need. While there is a front-end cost involved here, I consider it time and money saved down the road. While many youth I have worked with have benefited from working with developmental optometrists and auditory processing programs, these are usually frowned upon by school districts are not being “evidence-based.”
Relevance: One can see several types of practitioners listed here. This system includes any mental health license and any one qualified to provide psychotherapy. In addition, psychiatrists are qualified to prescribe medication. As stated in the text with the purple wheel, however, everyone across all levels of practitioners is able to become trained in Infant Mental Health (IMH). The designation of an Infant Mental Health Specialist, by most Endorsement standards, is someone who is Mater’s level licensed or credentialed in their discipline (e.g., Special Education Teacher) - across all disciplines. This is what makes the title of “Infant Mental Health” confusing because it sounds like it’s only dedicated to licensed mental health providers. Yet, this designation welcomes all disciplines! The Endorsement process is an important process for professional and community development. Here are two sites that link up with qualifications for this process.
There are two primary Endorsement processes that exist to my knowledge. One is located within the California tradition and the other emerges from Michigan’s long history with infant mental health. The strengths to the CA endorsement process is that this is a way for a community or a state to begin the process of having guidelines for how to become an Infant Mental Health provider at different levels. The process of putting together a portfolio and what knowledge domains are required are offered on-line without cost. http://cacenter-ecmh.org/wp/professional-development/california-compendium-of-training-guidelines-personnel-competencies-and-professional-endorsement-criteria-for-infant-family-and-early-childhood-mental-health/
The Michigan Endorsement process is a package that is purchased. The advantage of this purchase is that there is guidance the state gains in the setting up of a structure for the process of Endorsement and there is an ever-growing community that one becomes a part of. This community is now known as The Alliance for the Advancement of Infant Mental Health. At this time, there are 23 states (please check the web site as these are ever-changing numbers) and several international communities that have purchased and are implementing the endorsement package. This is supporting a national and international community of IMH practitioners to build momentum towards a professional identity with a national voice and a rich learning community. http://mi-aimh.org/alliance/ The NRF supports creating robust national and international communities that share a common understanding and investment in infants’ and parental well-being within strong relational ties.
Executive: The disciplines in this brain system are weighted towards motor, language, learning, cognitive, and executive development. As mentioned, there can be overlap with the Sensory System here. In general, the more “bottom-up” these needs are, the more they are serviced in the early years
13

through the sensory system providers (Early Intervention), and the older the child is, the more these are serviced through the School District.
Note: Home Visitors are very important practitioners that are part of NRF communities. They often are distributed around the wheel. Some are funded by Maternal-Child Health Departments, Department of Health (Regulation System), Department of Disabilities (Sensory System), Mental Health agencies (Relevance System), they can be a part of an Early Head and Head Start team (Early Care & Education System) and they can be a part of the Child Welfare System as well.
Note: Please note that Occupational Therapists are located in four out of four brain systems –regulation, sensory, relevance, and executive. First of all, OT’s began working in the mental health system, within the Relevance System. As psychiatric programs have dwindled since the 1980’s in the US, they no longer hold this strong time. Most OTs today, then, are found across the regulation, sensory, and executive (motor) domains. This is because the lines of demarcation and which part of the body different disciplines can work on, is quite discrete. OT’s can work on feeding difficulties and become certified feeding specialists (regulation); sensory processing concerns which includes sensory modulation difficulties is a primary domain; and they also work on motor planning and fine motor development both from a bottom-up aspect within sensory integration as well as a top-down capacity within the purview of daily occupation.
Where treatments are weighted. The two broad categories of where treatments lie is between bottom-up oriented, top-down oriented, or a hybrid of both. Bottom-up interventions are sensory-motor based and are everything we can do without the use of language or symbols! For the bottom-up side of things, you see the strong links here between the regulation and sensory system. Top-down interventions are
14
language based and are everything we can do with the spoken and symbolized narrative and reflections. You see the strong links here between the relevance and executive system. Many practitioners, especially mental health practitioners, are trained in top-down work. Many of the Evidence-based treatments are oriented for three to five year olds with the use of the narrative. The problem with using the chronological age as a treatment guide, is that the child may not match his chronological age with his developmental age. Thus, there are children who have language, but are not ready for top-down work. We use Step One and Step Two, along with Step Three to see where they are weighted developmentally and we always work “bottom-up” first!
Now, there are times when a practitioner is in a system of care and all they have to work with in their agency is a more top-down EBT. As one gets to know more of the subtle differences, one can see that there often are bottom-up aspects that can be found in a more top-down treatment. For example, you can see that with Trauma-Focused CBT, there is an early section of their manual that focuses on individualized relaxation and stress management. From the NRF’s point, this directly pertains to using Step One and Step Three, finding how to get to green and finding what the triggers and toolkits are for stress prevention and recovery. With Child-Parent Psychotherapy, there is an entire chapter devoted to “sensory-motor disorganization” which is all of the bottom-up issues we are dealing with in Step One and early Levels of Engagement in Step Two. Thus, one can see that the NRF assists with being able to
15

locate “bottom-up” aspects to an EBT, while providing extra guidance and support to work on these levels. By providing a neurodevelopmental landscape the NRF becomes “value-added”. In parallel fashion, one can see the top-down aspects of these and other clinical modalities. Some EBTs are only top-down in their approach and making the distinctions between bottom-up and top-down is very important in terms of carving out a clinical match with the child and parents. As one matures in the use of the Framework, it is considered an advanced phase where practitioners can map out any parenting or clinical program, accurately viewing where it is weighted from the four brain systems as well as from a Heart/Hand/Head perspective.
ORIENTATION TO THE WORKSHEETS FOR STEP THREE
Sometimes there are teams that have front-end Social Workers or Home Visitors that gather information before the secondary practitioner meets with the family. In these cases, it is possible to begin to fill out these forms ahead of time. These forms can be used at any time. As mentioned at the front end of this chapter, a Level One use of these four brain systems is to begin to organize the information you receive, right from the start, into a neurodevelopmental sequence that the NRF provides for you. However, often, the stories take time to unfold and more is revealed over time, rather than at the front-end when the working alliance is fresh and new. As trust builds over time, more details are revealed. If there is a gap in time before something is revealed, one can always place a date alongside the checked box if one wants to track the sequence of what was revealed.
Go to the History Worksheet
16

The History Worksheet has risk factors listed for each brain system. Getting to know these risk factors as you use them will help you encode and understand the organization of the four brain systems. This worksheet is upgraded on a regular basis and while this is comprehensive it is not exhaustive. This is not a worksheet that you hand to a parent or walk them through each item! These are risk factors that will emerge from the medical records you might receive, other records that are sent to you from other sectors, and the four stories interview process and subsequent ongoing conversation.
Several things help you make the best use of this:
1. There are two columns one can check. The far left box is when you and your team members are certain that this risk factor has occurred and is accurate.
2. The far right box is when you and your team members suspect that a certain risk factor may be true but it has not been revealed either due to a lack of time to inquire or the timing not being the right time to explore.
3. ACE score. The Regulation and Relevance Systems have distributed items from the Adverse Childhood Experience Score. At the bottom of the Relevance system is a box for the score of X out of 10.
4. Cumulative score. In addition, there is a box for you to place the cumulative score in each brain system box for each parent and child. Please use a separate History Worksheet for each parent and child. The ACE’s emphasis on cumulative scores is not the only one that has used this concept. The higher the score, the more, rather obvious chance there is that some vulnerability exists in this brain system.
5. Cascade effect. Thus, there is often a link with the risk factors, the functional vulnerabilities, and the need for intervention including this particular brain system’s needs.
6. Protective factors. Where are the protective factors? They are embedded in each box that is not checked. For example, if one was not exposed to any in utero toxins or born prematurely, these are protective factors, and a boost to the nervous system. Each item that is not checked off is an asset.
Go to History Worksheet Combined with Family and Community Needs Assessment
This second worksheet introduced in this Phase1 has a direct overlap with the History Worksheet. What is unique about it is that each Risk Factor segment, from each brain system, is expanded by being accompanied on the front page with 1) a needs assessment, and on the back page to reflect on the 2) community services one might need. The point of listing one’s community services is not only to make conscious links with what services exist in one’s community, but to begin to consider whom a practitioner can make warm handoffs to, or not. Warm handoffs refer to someone you actually can make a call to, you know their phone number exists (as opposed to the number being disconnected and the agency no longer is in business), and you can guide the family into their hands. Once a family makes a connection to you as the practitioner, it can be difficult to expand the team to include other members. Some families do not want to add another practitioner to the team. This is where early intervention trans-disciplinary team efforts have this as an advantage, because they take this into account. Then, additional resources can be brought along, in the role of a consultant, rather than having to shift
17

emotional ties to another provider or to add on more services with more appointments. Sometimes, however, either there is no trans-disciplinary option or one actually needs a very specific discipline added to the team, such as a physician or a shelter for domestic violence or a substance abuse program. Please take a look and familiarize yourself with this worksheet. Begin to fill out the community agencies and services you already have warm handoff links to, or a contact number.
ORIENTATION TO ENGAGING THE PARENTS WITH STEP THREE:
ORIENTATION TO THE FOUR BRAIN SYSTEMS, THE FOUR STORIES INTERVEIWS
Orientation to the four stories. When there is space in the early assessment phase to do this, I orient the parents to the four stories, so they know what type of information may become part of the conversation over time. This is a version of how I might offer this orientation. “Now, along with each of these four brain systems are four stories. These stories are ones that we will walk through as we have time to get to know each other. The Early Story connects with what things were like before your pregnancy (OR the birth of your child if s/he was adopted or birthed in another manner besides your carrying the pregnancy), what occurred during the pregnancy, labor and delivery, time right after birth (post-partum) and the first year of life with your baby. For dads or partners, this is also about your body and if you were able to participate in the birth experience and this first year of caretaking your child. As your child grows we turn to the next phase of the story, which is your child’s Developmental Story. Here, we will consider all the ways in which infants grow so quickly, with strengths and concerns that you may have had along the way. Having a child is an emotional event, so next we will look at the Emotional Story that has occurred in your family in relationship to your child. And last, we will look at the Educational/Learning Story that has emerged with your child and where s/he is in this process. [The Educational/Learning Story can include Early Care if the infant is in a child care setting during the parents’ working hours. Now, let’s take some time and begin with the Early Story.” [For a succinct review of these Interview Guidelines, please go to the NRF Interview Question Booklet 1-30-17 located in your Chapter 9 material on the Web].
Unique order to the Interviews. The four stories follow the salient features in the History Worksheet. The italicized item(s) listed are details from that particular brain system that relate to a Functional Capacity within that brain system. Many practitioners are trained to get a developmental history from families as the first part of the Interview process. If this is the case for you, note that Step Three may be how you are traditionally taught to begin a semi-structured interview. The NRF’s difference in sequencing the interview is that it’s very focused on first working to create a paradigm shift in how behaviors are viewed by orienting parents to stress responses. Secondly, now the four stories, beginning with the early and developmental history, followed by the emotional and learning history, are organized to look for causes contributing to the stress responses. The interview has a distinct purpose and the parents are made aware of this purpose. You are beginning to look for clues as to why there is a toxic stress pattern –to empathically understand inherent vulnerabilities, to begin to organize the triggers, and the sources of resilience that can lead to toolkits for more efficient stress recovery.
18

The Use of Yourself and Cultural Awareness as You Walk Through the Four Stories. When you first walk through these four stories you might feel like you are rotely asking questions. This is not the intent but understandable if doing a developmental history is new to you! As you relax into learning how to use the four stories, the use of empathic Heart skills, the use of neurodevelopmental guidance with your Hand skills, and the use of collaborative engagement with reflective Head skills are all used in balance as you organically move in and out of these interpersonal modes. Building a working alliance is of utmost importance at the front-end of the relationship, so pacing is important. At any point, a cultural issue or a moment of trauma or oppression may emerge from any brain system. Often, this means you will switch to the Relevance system to explore it. At the same time, you will know where you are the inherent order and structure the four brain systems give you! You can always cycle back where you left off and resume walking through the other brain systems later in the session or at your next meeting.
The Early Story from the Regulation System
The Regulation System is dedicated first of all, to acknowledging any food, shelter, and clothing concerns that have to do with basic necessities. It’s pretty difficult to focus on getting to the green zone with good sleep hygiene when basic necessities are not in place. If intervention needs to begin here, the hope would be that you are trained in helping parents find community services or you have access to a social worker or case manager that has expertise with these types of services. Next, the focus is on the prenatal history, labor and delivery experience, post-partum period, and that first year of infancy. Any in utero insults, prematurity, and genetic concerns are important for this brain system since these so directly affect the integrity of the nervous system. From there, any ongoing eating, feeding, nutritional, elimination, and medical issues are contained within this brain system. When it comes to the feeding and elimination issues, this is a natural time to ask if his or her infant was a good cue sender and easy to “read.” These are some of the early bi-directional signals that can both be “sent” and “read.” This is part of the core visceral self in communicating hunger, thirst, pain, too hot, too cold, wet diaper, etc. These also are potential clues for triggers!
19

Example of an empathic heart response during an Early Story Interview. There are many potential risk factors that can occur during the early story that are traumatic or an experience of a misuse of a power-differential, where our empathic selves are activated. For example, imagine a story with a history of miscarriages before this pregnancy, wherein this pregnancy becomes viable. With renewed hope, there is a wish to have midwifery delivery at home. Despite the best plans in place, the couple is disappointed by a protracted labor that turned into being taken to the hospital for an emergency C-section due to fetal distress. During delivery, it was discovered that the cord was wrapped around the baby’s neck three times, and the baby had to be immediately taken over to a birth warmer to be given oxygen at birth, missing the immediate skin to skin contact they had hoped for. You are quietly affirming and take time to be with them in the loss of their dream. There are many parents whose longings for a particular type of labor and delivery experience are thwarted. These rough beginnings can start off an early relationship with disappointment that still may not have been processed, even a year or two later. If there were cultural differences such an immigrant family overwhelmed by the protocols of the hospital experience, or a further complication wherein the on-call physician performing the C-section had a pejorative attitude towards the midwife and the family, there would be more emotional distress to process and support.
Example of a guiding hand response during an Early Story Interview. With this part of yourself, you are listening for moments that are clues to current triggers that may be contributing to the toxic stress pattern for the child or parent or both. For example, now imagine that this infant, born with fetal distress, is six months old and is a red zone baby who tends to be inconsolable. When you ask about his cue sending signals for feeding, the parents report that all of a sudden he starts screaming when he’s hungry. There are not any obvious cues of thumb sucking ahead of time or rooting at the breast, he seems to immediately be hungry, followed by difficulty with feeding because he’s so ravenous he gulps
20

down the breast or bottle milk with such vigor that he chokes. This might be an opportune moment to wonder out loud if this is a point of distress that you might be able to work on together, to see if these moments of feeding distress can be eliminated.
Example of a collaborative head response during an Early Story Interview. Now a spirit of a collaborative process might ensue. The parents might say that they are committed to feeding him “on demand” as instructed by their midwife, and they do not want to put him on a feeding schedule. You validate how important it is to follow his cues, yet you also hear that he’s informing them of how much distress he has when he gets too hungry. This causes a host of other problems, not only from the choking, but from taking in so much air, he is in further distress after the feeding from having too much air in his belly. You wonder if there is a way to follow his lead by keeping track of his feeding rhythm for a day or so, to see what the cycle is. You explain that he may be able to really enjoy his feeding and there might be more joy between them, if they could begin the feeding, based upon his personal rhythm 10 to 15 minutes before he erupts into distress. Your collaborative spirit is working hard to both honor their concerns, while also holding the baby in mind, honoring his distress pattern. You present this as an experiment to try, with the reassurance that this is a trial and error process of learning together how to best follow his lead, while finding a way to provide more comfort and joy with the feeding process for both of them.
The Developmental Story from the Sensory System
The Sensory System is dedicated to any early developmental delays and disabilities that arise. In the United States, this system is referred to as the Early Intervention, Part C funding source. This source has typically funded speech and language delays, motor delays, and sensory processing delays up until three years of age, after which the school district becomes involved. The larger diagnostic catchment areas Part C focuses upon and will stay engaged with for a lifetime are Autism, epilepsy, cerebral palsy, and intellectual disabilities.
It is common for pediatricians and other professionals to be asking during their periodic check-ups if the parents have any concerns about delays. The use of screeners, such as the Ages and Stages Questionnaire (xxxx), can be useful to help parents actually be informed more about what are age appropriate levels of development. It is equally important to be sharing with parents the successes of a child’s developmental gains while also able to assess for delays. We are always holding the balance of resilience and strengths with any vulnerabilities or concerns. This is where the NRF supports practitioners spending time with infants and young children being present during their visits, so that they are able to observe what is developmentally occurring in terms of motor, speech and language, auditory, visual, and sensory processing and modulation, in the context of the levels of engagement. If a delay has been picked up, then asking about the form of treatment and how involved the parents are is important to find out. Many treatments do not include the parents, or some consider “family-centered” care to be a parent watching a treating practitioner behind a one-way mirror. This is not what “relationship-based” treatment is about! While the NRF is clearly developmental and relationship-biased, many communities only offer ABA services for developmental delays or disabilities. Again, the NRF practitioner is in a position to support the Levels of Engagement and to provide a bridge between
21

the more structured and sequenced approaches to delays with the more spontaneous forms of engagement, with the focus on joyful exchanges.
Example of an empathic heart response during a Developmental Story Interview. With this part of ourselves, we listen for tender spots that have to do with any identification of a delay or disability. The parents may have an emotional story about how they were told his or her child had “Autism” or they may be afraid to acknowledge to you that they have a concern. There is a whole range of parents and a wide continuum of practitioners and within these, there can be mismatches. Some parents have feared there is a developmental delay at play and someone confirming their suspicions is nothing but a relief. They are grateful that someone has been clear and concise about what the need is. Other parents may have little awareness of what is a delay, such as first-time parents, and a straightforward approach, without preparation, is a shock and very unsettling, needing help to process how the message was delivered, as well as the meaning of the message. Sharing the emotional journey is important to do with parents.
Example of a guiding hand response during a Developmental Story Interview. When using Levels of Engagement as a guide, there may be a concern that arises organically. Let’s return to the couple with the baby who was screaming when hungry. Now, progress has been made! The parents now found his rhythm and are feeding him a few minutes before he’s ravenously hungry. The feedings times are filled with quiet bliss. Now, however, you notice that with much more green zone available, he is not turning or rolling over like you would expect a six month old to be doing. You are curious and wonder out-loud about his having any tummy time on the floor. The parents have heard about tummy time, but have a natural aversion to having their baby on, what they experience as, a dirty floor. They have been through a lot of emotional turmoil just to have their baby that’s alive and they have concerns about him getting
22

ill. They prefer to keep him in a bouncy and they notice how much he loves being bounced, which makes him smile and laugh.
Example of a collaborative head response during a Developmental Story Interview. Using your collaborative spirit, which honors their concerns and your developmental concerns, you engage in a discussion with them about the dilemma. Yes, it’s great to notice that he loves to bounce! This is a source of resilience and if you are keeping track of triggers and toolkits, you place his love of movement in the toolkit side in the sensory system. You ask them if you can play them a video of what some of his other movement can look like and perhaps you go to www.pathways.com/motor and show a six month level of motor development clip to them so that they can “see” what he might be capable of. Now, perhaps you can mention that you’d like to brain storm with them about how they can keep him safe and also increase his capacity for movement. After some discussion, you ask them if Dad would be comfortable lying down on his bed and having his baby on top of his tummy, facing him. This way, you are using Dad’s body instead of the floor. Dad’s face becomes a source of playfulness while his baby is on his tummy, and they start to play together. This becomes a way to start tummy time that is organic and matches the parent’s comfort zone. Later, on another visit, you’ve found that they have bought an exercise matt that they can place on the floor and cover it with a washable blanket. This way there is more room for baby to “roam” while still being able to protect him from the floor.
The Emotional Story from the Relevance System
The Relevance System is dedicated to the mental health needs of our families. Of course, infant mental health (IMH) that is in particular, developmental and relationship-based, is the vantage point the NRF brings to the mental health system of care. Since IMH is inter- and trans-disciplinary, the socio-emotional, relational, and mental health needs are not seen as discipline specific to mental health licenses, but essential to be distributed across all disciplines and systems of care. (This has been repeated so revisit it.)
Sandwich and layer the story. It is recommended that the types of questions one inquires about the emotional story be “sandwiched” in with questions about potential strengths, with questions about potential challenges, back to questions about potential strengths or positive experiences. There are many, many questions that one can ask about the relevance system. Any many relevance system issues will occur organically. These questions are focused upon the parent’s relationship with his or her child and one is looking for consistencies, coherence, and congruence between what the parent’s narrative is, along with matches in terms of body language or potential discrepancies. Discrepancies are related to often “undigested” stories that carry loss, grief, trauma, and oppression.
Linking stories to functional capacities. As one is finding out more about the emotional story, the links to the functional behaviors in the relevance system can easily be made within yourself as the practitioner. The relevance system is about the capacity to have a full and balanced range of positively/negativey valenced feelings, a full range of positively/negatively valenced memories one can access, and a balanced appraisal of oneself and others (aware of one’s strengths and needs). The more painful, and undigested stories one has in terms of trauma and oppression, the more likely these
23

emotional experiences are now internalized. This affects one’s internal appraisal of oneself. These experiences can go in an overly negatively biased position (towards hatred of oneself or chronic deferring to others) or an overly positively biased position (towards denial of one’s needs).
Use of language. Notice that the question, second down, on the left hand side is an inquiry about “trauma” for the child yet does not have the word “trauma” in it. One has to gauge with each family what their comfort level is with the use of language. This is an ongoing dynamic to learn the language of the family and to do the best at matching, being aware of the micro-aggressions that can occur along the way.
Recall that in Step One, there was a place to ask about each parent’s reactions and reflections as to his or her child’s stress responses and what that triggered in him or her. There are follow-up questions that are more reflective. If you have not had time to get to these, this is the time to do it!
However, these questions are not about the parents’ own childhood. For those, we recommend using these questions on Resilience along with the following from COSI.
Go to Resilience Questions
COSI page 6 of 6 (add questions about five words or phrases that describe relationship with mom/dad)
Example of an empathic heart response during an Emotional Story Interview. Following our previous case, the theme of “losses” resurfaces. In addition to the two miscarriages and the unexpected traumatic birth experience, it is revealed that the mother’s brother died from Sudden Infant Death Syndrome when she was five years old. Her parents had gone to visit the neighbors –and she to play with the neighbor’s children. When her brother fell asleep in her mother’s arms, her mother placed the
24

baby boy on the adult-sized bed of the neighbor’s parents. When her mother went to check up on him an hour later, he was found dead. This tragedy shaped the rest of her childhood. Her mother went into a deep and dark depression (blue zone/detached head), her father blamed her mother (red zone/blaming hand) and both parents blamed the neighbors. She was not allowed to play with the neighbors’ children again. None of it made any logical “sense” because no one was really to blame, but the loss was too great to bear for her parents. You are sad with them and the grief in the room is palpable after all these years. You now begin to make the link that loss for this mother has a very long history of unprocessed grief, wherein an experience of disappointment may be hard to endure and to recover from.
Example of a guiding hand response during an Emotional Story Interview. As the infant has now gained core strength from his tummy time, he now is starting to cruise well beyond the safe mat and the blanket. You can feel the tension rise in the parenting couple as now the mother is more protective, having purchased a playpen to restrict his motor exploration and the father is more lenient, enjoying his son’s motor prowess and exploration. The infant cries and screams every time he is placed in the playpen. You realize that this is even more complicated then when you first began to work with the family. You understand the child’s need to move is critical (e.g., for motor reasons, for healthy exploration, for being able to be separate from parents) and that a large portion of his current stress responses are coming from not being able to move and explore novelty. You also understand the mother’s automatic protectiveness, and this being embedded in her automatic meaning-making system (relevance) from her history of loss. You wonder out loud if, just as you all found a way to have safe “tummy” time if there is a way to have safe “roaming” time, so that baby gets to strengthen his motor skills, take pride in his exploration, and mom gets to feel safe, enjoying him in a new way. This might be a teachable moment to bring out the Circle of Security, showing the parents’ hands to hold both the exploration and the coming close for connection as an ongoing, back and forth, organic model for child-rearing.
Example of a collaborative head response during an Emotional Story Interview. So, you begin the collaborative process of holding the dialectic of the “both/and”. You inquire as to all of mom’s fears and what they are about. You find out that neither parent is aware of the concept of “child proofing” and what that means. A fair amount of mom’s worries are around dangers that protection can be provided for (e.g., plug-ins for electrical outlets, locks on drawers, gates for the halls and the stairs). You suggest they explore this next week finding out about the child proofing equipment and deciding as a couple which one room of the house/apartment would be the safest room for him to explore. By suggesting the couple take their time to do research and to think about where mom feels the safest, you slow down the process and provide time for them to reflect and to collaborate as a couple. By guiding them through this process, they are learning how to work through their stress responses collaboratively –honoring everyone’s needs, and to get through to the other side as well, back to green. Your relationship with the parents becomes a parallel process experience for the couple, while also providing new experiences for the mother.
The Learning/Educational Story from the Executive System
25

The Executive System is dedicated to the early care and education needs of our infants, young children, and families. Learning needs for this birth to five age range are also viewed through developmental, relationship-based, and play-based lenses.
Early executive is motor development. The early phase of the executive system is focused upon the motor capacities, strengths, and concerns. As the infant begins to move, the question becomes how s/he navigates the world. Are there strengths to motor planning, so s/he can figure out how to climb and use his or her body to walk and run? Or, is there a regular occurrence of tripping, falling, bumping, and banging into others? This may have to do with motor planning issues. The underpinnings to these may be related to how the body processes proprioceptive input (an awareness of where the body is in space), it may be related to visual-spatial concerns in how the child struggles to manage his or her visual-spatial input, or a combination of these and other processing issues.
Top-down control. The capacity for top-down control and to inhibit matures during the three to five year old range. This is why two year olds tend to roll around on the floor in motor distress (which our western culture refers to as a “tantrum”) and three year olds have more command of language and can protest with words rather than body actions. This is why “time-outs” during this age range tend to be more about punishment than learning how to inhibit and regulate one’s body. While “punishment” is a value within the behaviorally based community it is not a NRF developmental value. The NRF recommends experimenting with co-regulating “time-ins” with the parent calmly being with the child, helping them to get back to green by using the child’s sensory preferences as an option to “time-outs”. This matches the principle from Vygotsky of scaffolding a child’s development to gain body and language control over his and her stress responses. A time out, when used well, matches the child’s capacities to calm back down in a quiet and safe space and the goal of the time-out is suggested to be focused on regaining the green zone via supporting the child’s self-regulatory capacities rather than punishing the stress response. As the child does get older with more language, the “talking time” about what happened, why, what can be done differently next time, what can be learned from both parties, and the “repair” occurs after all parties are back to green. When parents and children are in a stress zone, these are not teachable moments!
Links of stories to functional capacities. The remaining questions are really about the capacity to juggle and balance two basic dynamics: the ability to initiate and shift into spontaneous behavior and the ability to inhibit and sustain behavior that supports staying on task, completing necessary routines and functions. As the capacity to juggle these two grows, then the capacity to have conscious control over these dynamics, ideally, also grows. We are making split-second decisions all the time as to whether we should check our cell phone or stay on task, which might mean staying connected to one’s child and playing with them. The juggling of the executive system continues, wherein, with maturation, there is an ability to juggle one’s thoughts with feelings, and one’s own needs with other’s needs. There is a cascade effect here where juggling one set of dynamics can help with the juggling of more.
26

Example of an empathic heart response during a Learning/Educational Story Interview. As you check in and see that this infant’s motor system is moving forward, with progress on the issue of exploration, you inquire about any future plans of having early care support from family or neighborhood resources. The parents mention this is a current battle ground between them. The mother prefers to stay at home but is feeling the fiscal need to return to work as the baby approaches one year of age. You now find out that the father’s parents are immigrants who do not approve of outside caregivers, and are happy to care for their grandson. While the mother appreciates the support, she feels controlled by her in-laws, which only further triggers her anxiety and pressure she already feels about doing a perfect job in raising her child. The grandparents want their grandson to be bilingual and the mother further feels shut out because the grandparents, while capable of speaking English with an accent, speak in their native tongue in front of her frequently. The mother increasingly suspects that they are talking about her, while in front of her, triggering her feeling shamed. The father understands the mother tongue while he speaks very little of it and is English-speaking. You explore this a bit further and he says he stopped speaking his mother tongue at a young age because of being shamed by the dominant culture. At the same time, with his head down, and with his own embarrassment, the father acknowledges that sometimes, yes, they are talking about her in front of her. He feels torn between his wife and his parents. You can feel the grid lock and take time to appreciate and verbalize the struggle. You are kind and empathic about how painful this is. You wonder what this would be like if you were in such a quandary, or if you have a parallel process experience, you acknowledge the turmoil you may be in as well.
Example of a guiding hand response during a Learning/Educational Story Interview. You are holding many things in mind at this time. For the baby, you recognize the value of learning a second language during these early years and what an advantage it is educationally to know two languages. You
27

recognize the potential resilience built-in to his having loving connections with his grandparents. You are holding in mind the mother’s painful experience of being excluded and treated as less-than by her in-laws from another culture, which feeds her internal struggle of anxiety. You are holding in mind the father’s torn loyalties between his two worlds and cultures. You wonder how much integration he has done with this being bi-cultural and how much they have discussed having such a strong cultural heritage on one hand and his having married outside his culture, which says something about his identifying with the dominant culture as well. This may be a time to talk about how our stress responses can also be related to our experiences of being included or excluded from a dominant cultural group. You explore how he may have felt excluded and shamed from the dominant culture, growing up in an immigrant family, and likewise, now his wife feels excluded and shamed by not being a part of his cultural group. Both of them share their painful experiences of being excluded.
Example of a collaborative head response during a Learning/Educational Story Interview. Now, you bring the collaborative spirit of collaborative problem solving to the experience. This dilemma is directly related to working with executive system dynamics. What type of cultural hybrid is the father? A thoughtful discussion at some point ensues. Where does he identify with his parents –accepting his cultural background with warmth (heart); where does he not accept his cultural background and standing against those values, value the dominant culture instead (hand), and where does he need to negotiate and reflect further on his own blend (head)? For the mother, what attracted her to his being from another cultural background from hers? Are there things she wants to bring into her sons life from her husband’s culture (heart)? Things she also rejects from his culture or from her dominant cultural experience (hand)? Are there pieces that need further reflection as to where to settle with creating a hybrid cultural family experience (head)? After processing, what they both could agree on was valuing the food from her husband’s culture. They both could value the gift of a second language being organically transferred to their son. And they both could agree that his parents talking in front of his wife in their native tongue, without translating or speaking in both languages, was not a value they wanted to support. They both experienced it as a way his parents were trying to have dominance over them as a couple. A plan was put in place. The father was going to express appreciation to his parents about their generous offer, while also creating a boundary with his parents about his and his wife’s experience of being disrespected, by their intentionally speaking in their native tongue rather their translating or speaking in English. From now on, he was going to translate into English in real-time what his parents were saying. They were going to see what happened with these new boundaries and go from there. The father knew this was going to be a struggle, due to his parents being disappointed with his not marrying within their own cultural group to begin with. As a practitioner, you provide support for how challenging being part of a bi-cultural experience can be and support the parents in their ability to sort out and juggle being empathic towards each other and holding each other and their child in mind. They have made great strides in recognizing each of their triggers and respectfully working towards decreasing their stress as parents.
CONSIDERING CULTURAL AWARENESS AND THE USE OF OURSELVES
28

These awareness questions came out of a dynamic effort that began with the Central Valley NRF Cohort. Please refer to the PDF version of these reflective questions within Chapter 9 for the latest version.
Please Note: the terms parents and caregivers are not gender specific nor are they biologically specific
Regulation Brain System
Cultural Reflection
1. From a cultural view, in this family, is it typical for a parent follow/read/respond to infant’s cues?
2. What is this family’s usual view of reading infant cues? Responding to infant cues?3. From a cultural view, how does this parent feed, sleep, diaper, clothe his or her baby?4. From a cultural perspective how are gender roles defined? (e.g., who earns the income/who
cooks/who cleans/who changes the diapers)5. What is this caregiver’s cultural view of prenatal care, birth, labor, delivery?6. What is this family’s cultural view of post-partum depression?7. Are there any toxic stress patterns at the personal and interpersonal levels in this family? (i.e.,
chronically in blue or combo/oversleeping; going into stress responses too quickly and too frequently)
8. What possible survival behaviors are present (i.e., adaptation to an oppressive system)? How do you, as practitioner, maintain an awareness and facilitate a dialogue regarding internalized oppression?
9. What are the systemic, institutional, and cultural barriers that create and/or support any toxic stress patterns in the family?
Parallel Process Reflection
1. Do you experience this family’s cultural values around early care as matching or aligning with your own cultural values of early care?
2. Do they remind you of anything similar to how you were raised or how you are raising or how you raised your children?
3. If there are differences in your family values, what are they?4. If there differences in your professional values, what are they? Does this cause discomfort?
Alarm? How do you communicate your discomfort? 5. Are you triggered by the family’s chronic red/blue/combo zone, any other toxic stress pattern,
or the family’s internalized oppression? If so, how (red/blue/combo zone)? Whom do you go to for reflective practice to process your stress responses?
Power Differential Reflection
1. If there is a cultural difference between your value system and the parent’s value system for feeding, sleeping, diapering, clothing their baby, how comfortable are you with the differences?
2. Are you in a dominant position as both a practitioner and culturally?
29

3. If you are “triggered” by the cultural differences (#1 above), what stress response(s) do you have (red/blue/combo)?
4. If you are triggered by the cultural differences, how does this affect your capacity to use your heart, hand, and head skills?
5. If this family is “triggered” by the cultural differences between you and this family, what stress responses do they have (red/blue/combo)? How do you respond to their stress responses? With your heart/hand/or head?
6. If there is a professional concern that is alarming or reportable, how will this be experienced by the family in terms of dominance and your use of power? Is there any way you can prepare them or modulate that for the parents?
Sensory Brain System
Cultural Reflection
1. From a cultural perspective, when does this caregiver think infants should talk, walk?2. What is this family’s cultural view of infant‘s fine motor skills (i.e., when should infant pick up
objects toys independently)?3. What is this family’s cultural view about feeding and meals (i.e., parent’s role in feeding is
fostered, child’s independence in feeding is fostered, meals are prepared vs. child’s choices, family eats together or not, etc.)?
4. Does this family “tune-in” to processing issues, (i.e., visual spatial, auditory, olfactory, proprioception, etc.)? In other words, is this topic something this caregiver notices as part of a delay? Or an individual difference?
5. What does the family think about intervening when the child does have a developmental delay (i.e., the family may not care about the delay and sees it as part of a Western cultural bias; what if your referral sources sees denying services as parental neglect that is reportable)?
6. In terms of “matching or countering” for modulation – from a cultural perspective, can this caregiver up-regulate/down regulate? Note: Some cultural groups do not feel comfortable “down regulating” and some cultural groups find “upregulating” outside of their comfort zone.
Parallel Process Reflection
7. Do you find yourself in alignment with this family’s cultural values around early developmental milestones?
8. Do they remind you of anything similar to how you were raised or how you are raising or how you raised your children?
9. If there are differences in your family values, what are they?10. If there differences in your professional values around developmental guidelines, what are they?
Does this cause discomfort? Alarm? 11. Do you find yourself comfortable or uncomfortable around the sensory-motor climate in this
home (e.g., being an up-regulating or down-regulating type of household)? 12. Do you have any professional concerns that the sensory-motor climate is blocking regulation
and/or engagement?
30

13. Whom do you go to for reflective practice to process your concerns?
Power Differential Reflection
14. If there is a cultural difference between your value system and the parent’s value system in regards to developmental milestones and early intervention? How comfortable are you with the differences?
15. If you have not parented or parented a child with special needs in your life, do you or your clients have feelings about the validity of your input?
16. Are you in the dominant position as both a practitioner and culturally? 17. If you are “triggered” by the differences, what stress response (red/blue/combo) do you have?18. If you are triggered by the differences, how does this affect your capacity to use your heart,
hand, and head skills? 19. If the family is “triggered” by the differences, what stress responses (red/blue/combo) do they
have? How do you respond to their stress responses? With your heart/hand/or head?20. If there is a professional concern that is alarming or reportable (e.g., a provider reports neglect
for a child who needs services for motor/speech delays), how will this be experienced by the family in terms of dominance and your use of power? Is there any way you can prepare them or modulate that for the parents?
Relevance Brain System
Cultural Reflection
1. What range of feelings are valued by each parent? Ignored? Shamed? [Consider the Feeling Wheel – Peaceful, Powerful, Joyful – aspects of green? Sad – Blue; Mad – Red; Scared – Combo]
2. From a cultural perspective, how does this family feel about “approach” and “separation”? 3. Has there been an immigration history and/or familial separations?4. From a cultural perspective, how does this family feel about attachment (connection-in)
relationships? Note: Some cultural groups do not afford attachment relationships very much “power” as these relationships “come and go”.
5. Are there cultural value differences in how male versus female children are viewed and valued? 6. If there is mental health or substance abuse issues in this family – how is it viewed? Is it viewed
as “normal/typical’? Or problematic/challenging?7. Are you comfortable with families discussing or bringing up issues of mental health and/or
mental illness?
Parallel Process
31

8. From your family of origin, were there value differences in how male versus female children were viewed? Are these simpatico or different from this family?
9. Are you similar or different from this family in terms of sharing a range of feelings?10. Are you similar or different from this family in terms of sharing levels of engagement? 11. Do you feel “welcomed” in this home? How did your family welcome newcomers in your home?12. If there differences in your professional values around sharing emotions and feelings, what are
they? Does this cause discomfort? Alarm? 13. Do you find yourself comfortable or uncomfortable around the emotional climate in this home
(e.g., household of shame, rage, depression, intrusiveness)? 14. Do you have any professional concerns that the emotional climate is traumatic to this
child/spouse? 15. Whom do you go to for reflective practice to process your concerns?
Power Differential Reflection
16. Are there experiences for this caregiver/family in which they have felt excluded, discriminated against or treated poorly?
17. From a cultural perspective, what makes this caregiver feel empowered/competent?18. If there is a cultural difference between your value system and the parent’s value system in
regards to socio-emotional health and the quality of engagement in relationships? How comfortable are you with the differences?
19. If you are “triggered” by differences in socio-emotional capacities, what stress responses (red/blue/combo) do you have?
20. If you are triggered by the differences, how does this affect your capacity to use your heart, hand, and head skills?
21. If the family is “triggered” by the differences, what stress responses (red/blue/combo) do they have? How do you respond to their stress responses? With your heart/hand/ and/or head?
22. If there is a professional concern that is alarming or reportable (e.g., refusing to acknowledge abuse or neglect, domestic violence, refusal to get help), how will this be experienced by the family in terms of dominance and your use of power? Is there any way you can prepare them or modulate that for the parents?
Executive Brain System
Cultural Reflection
23. Does the family’s culture value movement and exploration (i.e., explore things orally, walking vs. being carried, being allowed to explore and move away from the parent)?
24. Does this family value dependence or independence or both? How does this family support these for their children?
25. How does this family’s cultural group view play (i.e., value or devalue)? Parent role in play? Play as a learning experience? How does this family play together?
26. In this family, who do they believe is their child’s best teacher?
32

27. From a cultural view, how does this family believe children learn the best?28. What are the culturally laden expectations around attention? Impulse control? Being on time?
Thinking about others? 29. From a cultural perspective, what do the parents think his or her child needs, in terms of skills,
to make it in life?30. From a cultural perspective do these parents have “reflective” time to think about things and to
collaborate with you? 31. From a cultural perspective, how does this family view “intervention”? What is this family’s
cultural view of seeking intervention? Medical care? Psychological care? Mental health care?
Parallel Process Reflection
32. Are you similar or different from this family in terms of sharing how learning as “play-based” is viewed?
33. Are you similar or different from this family in terms of values regarding attention, time, impulse control, and thinking about others?
34. If there differences in your professional values around any of these items, what are they? Does this cause discomfort? Alarm?
35. Do you find yourself comfortable or uncomfortable around the ability to hold his or her baby in mind in this home (e.g., parents distracted, cannot keep appointments, frequent cancellations)?
36. Do you have any professional concerns that the executive ability of the parent (i.e., to hold his or her baby in mind, to keep track of necessary schedules, appointments, and play-based learning) is dangerous to this child/spouse?
37. Whom do you go to for reflective practice to process your concerns?
Power Differential Reflection
38. Are there experiences for this caregiver/family in which they have felt excluded, discriminated against or treated poorly in terms of his or her own ability to learn and be educated?
39. From a cultural perspective, what makes this caregiver feel empowered/competent to work and to learn?
40. If there is a cultural difference between your value system and the parent’s value system in regards to learning, staying on task with schedules and appointments this child or parent needs? How comfortable are you with the differences?
41. If you are “triggered” by differences in how executive items are viewed, what stress responses (red/blue/combo) do you have?
42. If you are triggered by the differences, how does this affect your capacity to use your heart, hand, and head skills?
43. If the family is “triggered” by the differences, what stress responses (red/blue/combo) do they have? How do you respond to their stress responses? With your heart/hand/ and/or head?
44. If there is a professional concern that is alarming or reportable (e.g., refusing or inability to keep appointments for self-care or child’s needs, inability to plan ahead and follow through with
33

necessary items), how will this be experienced by the family in terms of dominance and your use of power? Is there any way you can prepare them or modulate that for the parents?
34